Back to Journals » Journal of Pain Research » Volume 12
Botulinum Toxin Type A for refractory trigeminal neuralgia in older patients: a better therapeutic effect
Authors Wu S, Lian Y, Zhang H, Chen Y, Wu C, Li S, Zheng Y, Wang Y ![]() , Cheng W, Huang Z
, Cheng W, Huang Z
Received 15 February 2019
Accepted for publication 27 May 2019
Published 17 July 2019 Volume 2019:12 Pages 2177—2186
DOI https://doi.org/10.2147/JPR.S205467
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Katherine Hanlon
Shouyi Wu,1 Yajun Lian,1 Haifeng Zhang,1 Yuan Chen,1 Chuanjie Wu,2 Shuang Li,1 Yake Zheng,1 Yuhan Wang,1 Wenchao Cheng,1 Zhi Huang1
1Department of Neurology, The First Affiliated Hospital, Zhengzhou University, Zhengzhou City, Henan Province, People’s Republic of China; 2Department of Neurosurgery, Xuanwu Hospital, Capital Medical University, Beijing, People’s Republic of China
Background: Some studies have indicated that a local injection of Botulinum Toxin Type A (BTX-A) is a promising therapy for trigeminal neuralgia (TN). However, BTX-A treatment is still ineffective for approximately 10–43% of patients. We therefore investigated which factors are associated with the therapeutic effect in BTX-A treatment of medically refractory, classical TN.
Methods: We performed a retrospective cohort study with a total of 104 patients who were receiving BTX-A injection for medically refractory classical TN between August 2013 and October 2016. A VAS score, pain attack frequency per day as well as patients’ overall response to treatment and side effects were evaluated in 104 patients with TN who were receiving BTX-A.
Results: A total of 87 patients reported successful results; 41 stated that their pain was completely controlled while 46 reported adequate pain relief, totaling 83.7%. Our study suggests that treatment success was higher in patients 50 or older (OR=3.66, 95% CI: 1.231–10.885). Univariate and multivariate analyses demonstrated that the patient’s age was independently associated with treatment outcome (OR=1.72, 95% CI: 1.063–2.282), with ≥50 years being a significant predictor of pain relief (P=0.020 and P=0.033, respectively). Seventeen patients (16.3%) reported mild side effects.
Conclusion: A local injection of BTX-A may be a safe and efficient treatment for classical TN which lasts for several months. BTX-A is a novel strategy which is particularly worth trying for particularly middle-aged and elderly patients who cannot tolerate drug side effects and may be afraid of serious complications from microvascular decompression.
Keywords: trigeminal neuralgia, Botulinum Toxin Type A, age, local injection, therapeutic effect
Introduction
Trigeminal neuralgia (TN) is characterized by touch-evoked, unilateral, brief shock-like paroxysmal pain in one or more divisions of the trigeminal nerve. In addition to the paroxysmal pain, some patients experience continuous pain.1 First line treatment is typically sodium channel blockers, either carbamazepine or oxcarbazepine.2 However, as a result of intolerable side effects, such treatment may fail. Surgical treatment microvascular decompression (MVD) then becomes the next choice if neurovascular contact has been demonstrated. However, some serious complications may occur, such as cranial nerve dysfunction, stroke or even death.2
Botulinum Toxin Type A (BTX-A) is an exotoxin which is produced by the Gram-positive bacterium Clostridium botulinum. This was initially used to treat blepharospasm and hemifacial spasm.3 More recently, BTX-A has been utilized for the relief of chronic migraine and other types of headache.4–7 In 2002, the antinociceptive effect of BTX-A in TN was reported, while its safety and effectiveness were shown by several studies.8–20 These studies indicated that local injections of BTX-A may be a promising therapy for TN.
In 2009, our group began a study of TN treatment using BTX-A. We have since established a clinical database. Through several clinical trials, our group have investigated the effects,17 safety,17 dosage,18 treatment schedule19 and long-term efficacy20 of BTX-A for treating TN. However, BTX-A treatment is still ineffective for approximately 10–43% of patients.17–20 This study aimed to investigate which factors are associated with the therapeutic effects of BTX-A treatment for TN.
Materials and methods
Subjects
We performed a retrospective cohort study. Some 142 patients received BTX-A injections for medically refractory classical TN at our institution between August 2013 and October 2016. A total of 38 patients were excluded as they had no follow-up data available. Inclusion criteria were as follows: patients must be diagnosed with classical TN according to the International Classification of Headache Disorders, version 3-beta,1 and their medical treatment must be failing either because the patient is a non-responder to one of two drugs, such as carbamazepine 400–1,200 mg/day or oxcarbazepine 900–1,800 mg/day; or because the patient cannot take those drugs due to specific counter indications; or because the patient cannot reach the therapeutic dosage due to excessive side effects.21 Exclusion criteria were as follows: patients who suffer from coagulopathy or severe heart, liver, kidney, or other organ dysfunction, or secondary TN, diagnosed by detailed physical examinations as well as CT and MRI of the cranium. In total, 104 patients were eligible and so were included in our study.
Treatment
BTX-A (100 U of clostridium botulinum type A neurotoxin complex) was acquired from the Lanzhou Biological Products Institute, People's Republic of China. BTX-A was dissolved in 2 mL of saline (0.9%) to 50 U/mL, as recommended by the manufacturer. During injections, patients lie on a bed in a supine position. After this, according to the patient’s description, BTX-A was injected intradermally at the site of pain and the trigger point using a 1 mL syringe with a 0.45×16 mm needle, while for multiple site injections, 15 mm intervals were measured between injection sites, with 5 U at each site (see Figure 1). If pain involved the oral mucosa, injections were conducted submucosally in the oral mucosa with 2.5 U at each site in the way described above. During the procedure, injections in deeper structures such as muscles were avoided to prevent unwanted effects on underlying muscles. Meanwhile, during the course of the study, the analgesics used remained unchanged and patients were prohibited from initiating therapy with a new preventive medication. In addition, patients who required “rescue” analgesic medication during the study were allowed to use their current opioid and/or non-opioid analgesics as clinically indicated. These included NSAIDs, acetaminophen and COX-2 inhibitors as well as topical analgesics.
 |
Figure 1 Schematic showing injection sites for BTX-A. The shading shows the distribution of pain and the filled circles represent BTX-A injection sites. Reproduced from Wu CJ, Lian YJ, Zheng YK, et al, Botulinum toxin type a for the treatment of trigeminal neuralgia: results from a randomized, double-blind, placebo-controlled trial, Cephalalgia (32(6)) pp. 443–450. Copyright © [2012] (SAGE Publications).17 |
Follow-up and efficacy assessment
Prior to injections, patient demographics including gender, age, duration of diseases, presence of trigger zone, side of involvement, nerve branch involved, provoking factors, frequency of TN attacks and severity of pain as well as any previous surgery were recorded. Following injections, patients were asked to complete a daily diary of their pain symptoms, including provoking factors, frequency of attacks (either spontaneous or evoked), severity of pain and side effects per 24-hr period. We used the VAS to quantify pain severity. The VAS score has 11 points on a ruler of length 10 cm, where 0 denotes “no pain” and 10 denotes “most severe pain”. Patients were also asked to evaluate pain intensity averaged over the last 24 hrs before going to bed (average daily pain score) using the VAS score. We adopted the classification that a reduction in average daily pain of <50% after treatment meant that the treatment was classified as “ineffective”, 50–75% as “effective”, >75% as “significant effectiveness” and “0” meant complete pain relief. Treatment success was defined as the percentage of patients who experienced a reduction in average daily pain score of ≥50%. A 50% threshold was chosen as it is commonly accepted in the pain literature as being reflective of effective treatment.22
Patients’ overall response to treatment was assessed using the Patient Global Impression of Change (see Table 1). In order to determine the effect of treatment, following injections, follow-up visits took place every week for 2 months and once a month thereafter for 12 months.
 |
Table 1 The Patient Global Impression of Change (PGIC) Scale |
Statistical analyses
Data are presented as mean±standard deviation or median (range) for the quantitative variables and as frequencies or percentages for the qualitative variables. We initially performed univariate logistic regression analysis to determine the relationship between the clinical predictive factors and the two outcomes (see Figure 2). Secondly, we performed stepwise regression to identify which variables should be included in the multiple regression analysis. Variables identified for univariate regression analysis were the same as those identified for stepwise regression analysis. Since our clinical experience identified toothache and side effects as two of the most important variables likely to affect outcome, we also included these in multivariate analysis. Patients were divided into two age groups (<50 years old and ≥50 years old) for analysis (see Figure 2). Normality tests were conducted on all parameters, which they did not meet. Quantitative variables were examined between the two age groups using Wilcoxon rank sum test, while qualitative variables were compared using the χ2 test or the continuity corrected χ2 test as appropriate. We selected some factors which were likely to be related to the outcome. These factors included: duration of disease, age, gender, dosage, pain intensity, frequency of TN attacks, nerve branch involved, side of involvement, side effects, toothache, hypertension, diabetes, smoking, dyslipidemia and body mass index. SPSS version 17.0 was used for statistical evaluation, while P<0.05 was considered statistically significant.
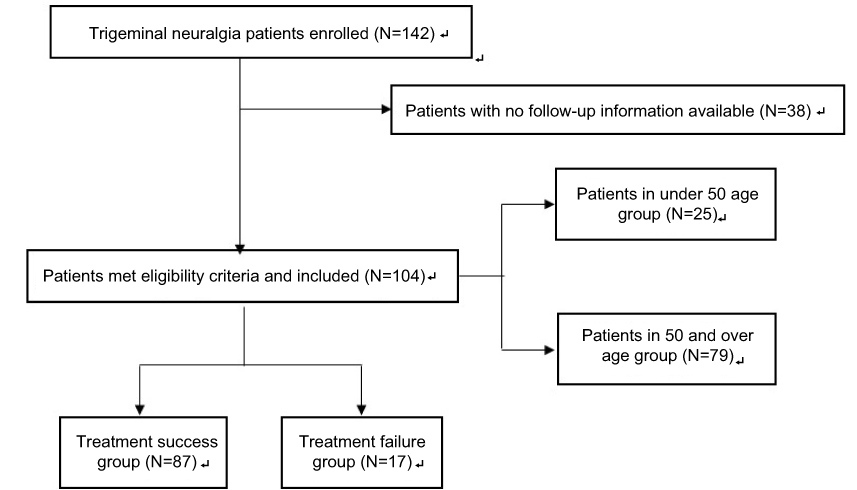 |
Figure 2 Flow diagram. |
Results
Patient characteristics
A total of 104 patients were included in the study. Patient characteristics can be seen in Table 2. Some 57.7% (n=60) were female and 68.26% (n=71) were right. The cohort’s age was 59.21±12.05 years (range: 33–93). Disease duration was 76.23±56.18 months (range: 12–300). Average daily pain score was 8.40±1.50 (range: 6–10). Average frequency of TN attacks per day was 24.90±27.70 (range: 4–120). Dosage was 59.62±21.69 U (range: 25–120). Five patients had previously undergone radiofrequency ablation, while 10 had previously undergone MVD.
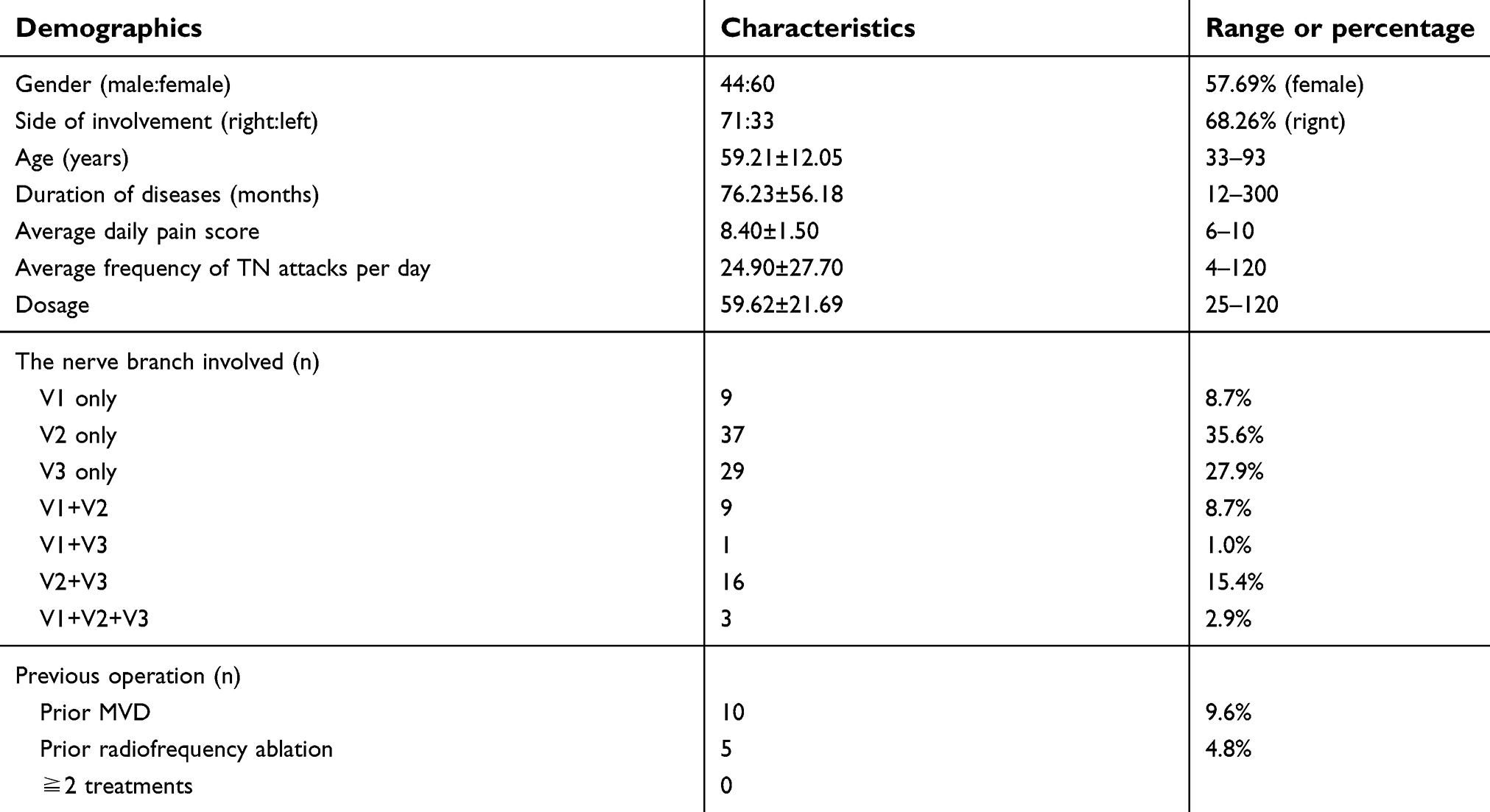 |
Table 2 Patient demographics |
Efficacy results
A total of 87 patients reported successful results after a median latency period of 8 days (range: 1–49); 41 stated that their pain was completely controlled, while 46 reported adequate pain relief, totaling 83.7%. Some 17 reported treatment failure; nine reported only mild improvement, seven no change, while one reported getting worse, totaling 7.7%. Among the 87 patients who experienced complete or adequate pain relief, the time to peak efficacy ranged from 7 to 112 days.
Univariate analysis using logistic regression demonstrated that patients’ ages were independently associated with treatment outcome (OR=1.72, 95% CI: 1.063–2.282, see Table 3). Treatment success rates were higher in patients 50 years or older (OR=3.66, 95% CI: 1.231–10.885, see Table 3). Univariate and multivariate analysis demonstrated that an age of ≥50 years was a significant predictor for pain relief (P=0.020 and P=0.033, see Table 3).
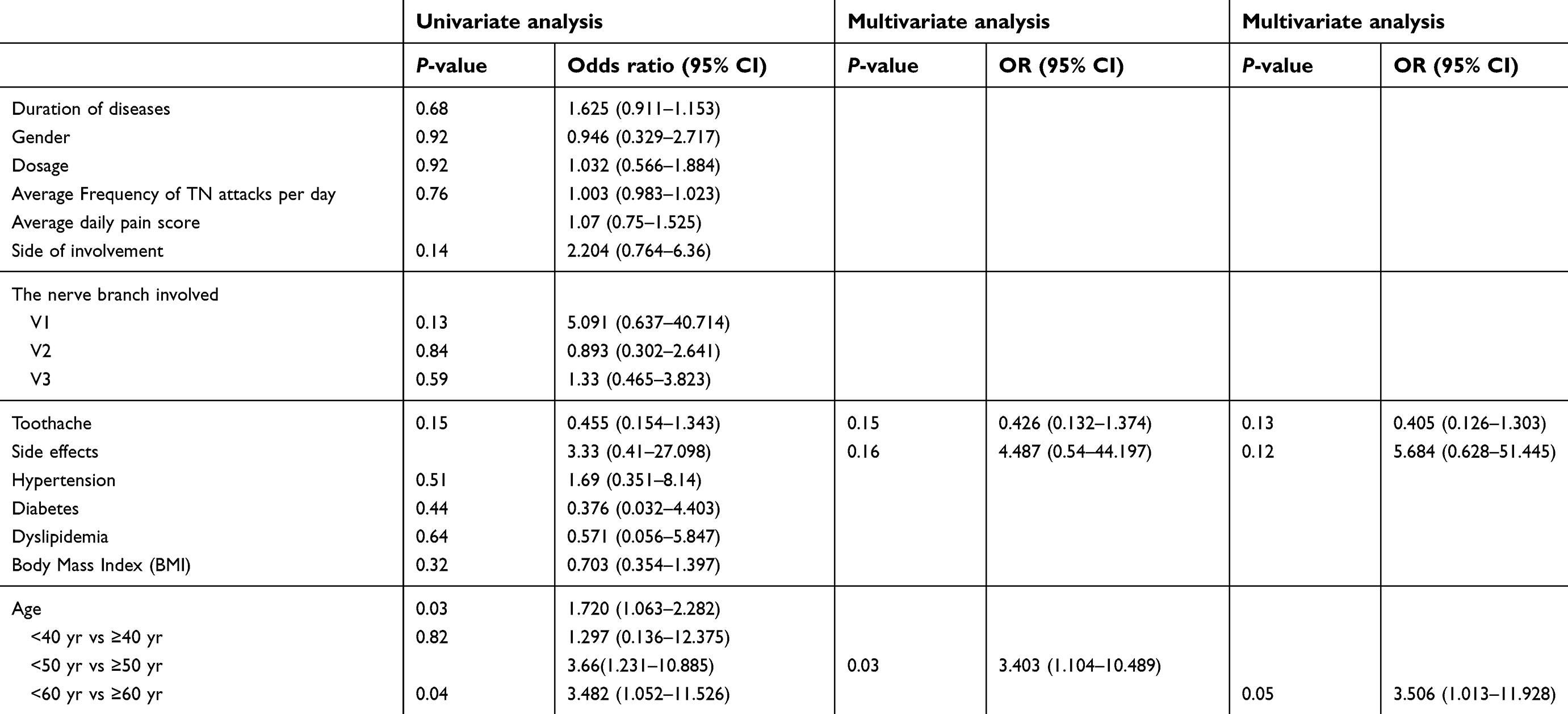 |
Table 3 Factors of outcomes after BTX-A for trigeminal neuralgia |
Logistic regression analysis demonstrated that patients in the older age group showed a greater improvement in average daily pain score following treatment with BTX-A than younger patients. The under 50 (younger) age group included 25 patients, while 79 patients were in the 50 and over (older) age group. The mean age of all patients was 59.21 years, 43.04 in the younger group and 64.33 in the older group (P<0.000, Wilcoxon rank sum test, see Table 5). No other demographic or clinical predictive variables were significant between the two groups (see Table 5). In addition, in the 50 and over group, the mean improvement in average daily pain score was 6.922 at most recent follow-up, while in the under 50 group, this was 4.976 (P=0.008 Wilcoxon rank sum test, see Figure 3A). When patients were split into good pain control and poor pain control groups, with good pain control defined as Patient Global Impression of Change (PGIC) Scale 1 or 2 and poor pain control defined as PGIC Scale 3–7, 83.3% of the older group were shown to have good pain control, while 57.3% of the younger group had good pain control at most recent follow-up (P=0.034, continuity corrected χ2 test, see Figure 3B).
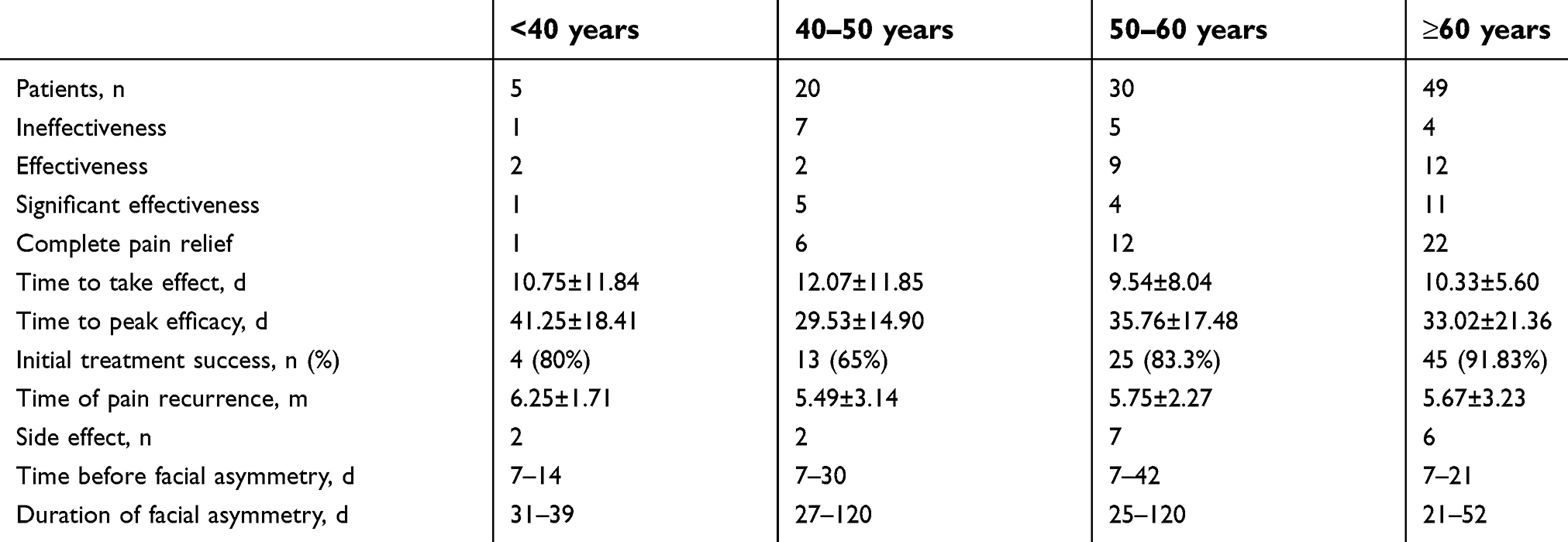 |
Table 4 Outcomes among different age groups of patients who underwent BTX-A for trigeminal neuralgia |
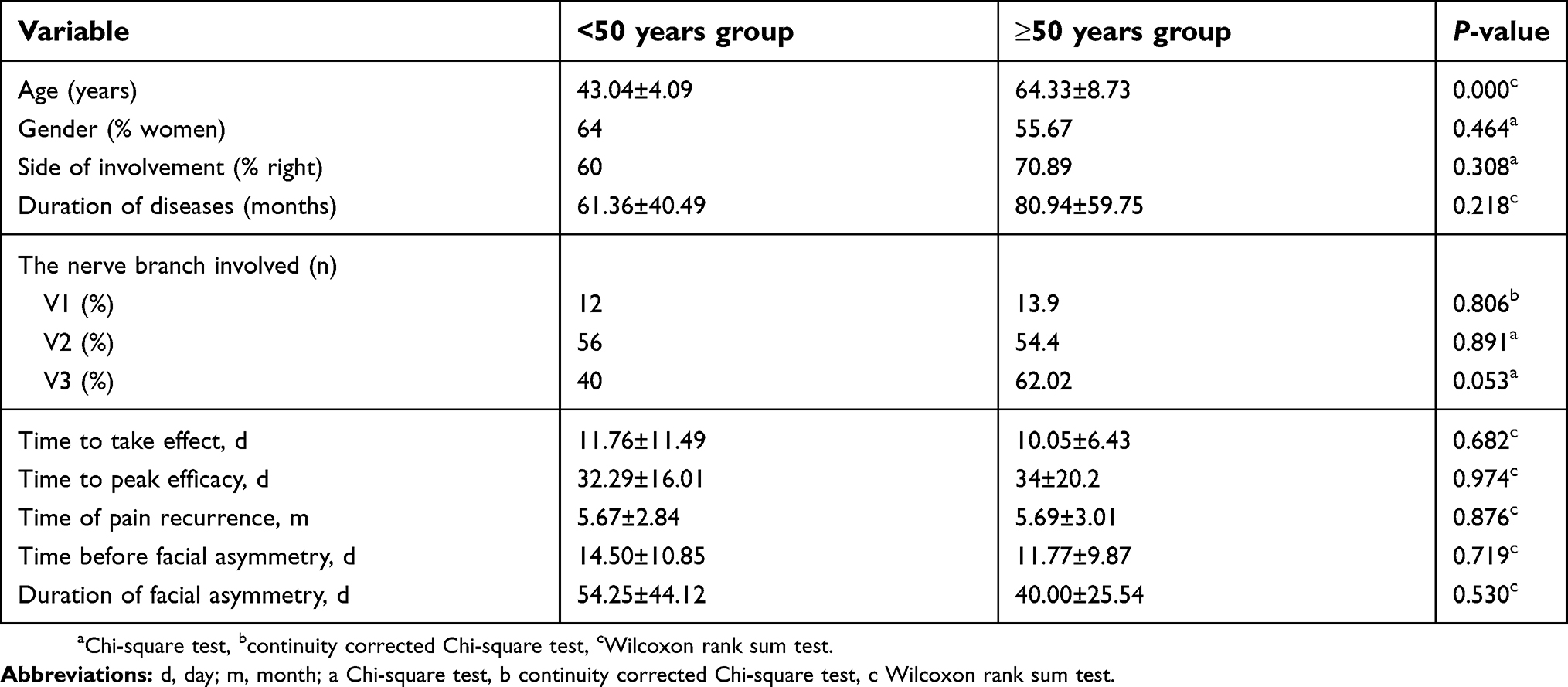 |
Table 5 Comparison of demographics and outcomes in trigeminal neuralgia patients with <50 years vs ≥50 years |
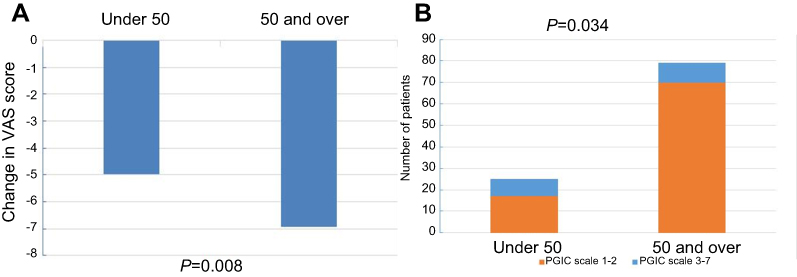 |
Figure 3 TN pain outcome after BTX-A in patients under50 compared to patients 50 and over. (A) Patients in the older age group had a significantly greater improvement in average daily pain score following BTX-A treatment. (B) There was a significantly greater proportion of patients in the older age group with PGICscale1-2. |
Table 4 lists clinical outcomes stratified by age. Higher treatment success rates were observed in older patients: <40 years (80%), 40–50 years (65%), 50–60 years (83.3%), ≥60 years (91.83%). We found the mean onset time – that is, the time to take effect – was 10.91 days while the time to peak effect was 33.15 days. In the younger group, the mean onset time was 11.76 days while the time to peak effect was 32.29 days. In contrast, the mean effect time for the older group was 10.05 days, while the time to peak effect was 34 days. There was no significant difference in the time to take effect and the time to peak effect between two groups (P>0.05 Wilcoxon rank sum test, see Table 5).
Time of pain recurrence varied with age: <40 years (6.25 months), 40–50 years (5.49 months), 50–60 years (5.57 months), ≥60 years (5.67 months). We found that time of pain recurrence was 5.68 months (see Table 4). For the younger group, time of pain recurrence was 5.67 months. In contrast, for the older group, time of pain recurrence was 5.69 months. There was no significant difference in the time of pain recurrence between the two groups (P>0.05 Wilcoxon rank sum test, Table 5).
Safety and tolerability
Following a median latency period of 7.5 days (range: 7–42 days), 17 patients (16.3%) demonstrated facial asymmetry at the injection sites and this asymmetry was resolved at a range of 21–120 days. In the younger group, time before facial asymmetry was 14.5 days while duration of facial asymmetry was 54.25 days. For the older group, the time before facial asymmetry was 11.78 days while the duration of facial asymmetry was 40 days. We found no significant difference between two age groups (P>0.05, Wilcoxon rank sum test, Table 5).
Discussion
This study suggests that patients’ age may be associated with the outcome of BTX-A treatment. The success rate of this treatment is higher for patients who are aged 50 or older. Despite this, there were no significant differences between time of pain recurrence, time to take effect and time to peak effect for older or younger patients.
BTX-A has been utilized for the relief of many pains, including chronic migraine and other types of headache,4–7 and neuropathic pain including postherpetic neuralgia,23 diabetic neuropathic pain24,25 and occipital neuralgia.26 The application of BTX-A for relieving TN was first reported in 2002.8 Several studies have indicated that local injections of BTX-A may be efficient and safe for TN and have investigated the effects,17 safety,17 dosage,18 treatment schedule19 and long-term efficacy20 of BTX-A for the treatment of TN. At present, no study has investigated the relationship between outcome and age in the BTX-A treatment. However, some studies on MVD surgery have focused on the relationship between outcome and age, showing that in younger groups, the outcome is unfortunately not as good as that reported for the older population.27,28 Older patients have a greater proportion of arteriosclerosis. Following the gradual development of arteriosclerosis gradually, vessel shape and conformation may change, leading to neurovascular compression.29 This may explain the relationship between outcome and age. We also reported that patients aged 50 or older have a better therapeutic effect for the BTX-A treatment of TN. This may be explained by different underlying pathophysiological mechanisms in TN in different age groups. Future research into pathogenesis may provide a more comprehensive understanding. Meanwhile, there is a significantly greater proportion of patients in the older group with PGIC Scale 1–2, who are therefore showing a greater improvement. However, time of pain recurrence showed no significant difference between the two age groups. The younger cohort had a smaller sample size, which may help to explain the lack of significant difference between the two age groups.
Some studies have reported that pain relief was observed several minutes after injection,17 although this is more frequently observed several days or as long as 60 days after injection.20 Similarly, our study indicates that the mean time to take effect is 10.91 days while the peak effect time is 33.15 days. We also found that the time to take effect and peak effect time showed no significant difference. In contrast, Micheli reported that the effect of BTX-A for treating TN is consistent with its relaxation of muscle tension.8 Commonly, BTX-A can relax muscle tension for 3–6months. In our study, time of pain recurrence was 5.68 months. However, a 14-month follow-up study involving 88 patients with TN has suggested that BTX-A can relieve pain for longer than it can relax muscle tension.23 However, each of these studies had different inclusion criteria, which may have led to the different outcomes.
We observed only mild, local side effects. Seventeen patients (16.3%) demonstrated facial asymmetry at injection sites; facial asymmetry occurred mainly due to the blocking of neuromuscular transmission through decreased acetylcholine release. Several studies have also reported similar outcomes.9–20
The antinociceptive mechanism of BTX-A in TN therapy remains unclear. Recent studies30 have suggested that BTX-A may relieve pain through inhibition of the release of neurotransmitters at the peripheral endings of sensory nerves, including glutamate, substance p and calcitonin gene-related peptide. Additionally, axonal transport between sensory nerves and central sensory regions, pain-sensing trans-membrane receptors such as transient receptor potential to neuronal plasma membranes as well as selective inhibition of meningeal nociceptors are also relevant for BTX-A antinociceptive activity.30
The average age of onset for classic TN is 53 years.31 In addition, a systematic review has shown that there are higher rates of death, stroke and thromboembolic events following MVD surgery for elderly patients.28 Our study demonstrates that the patient’s age may be associated with BTX-A treatment outcome. The success rate of the treatment is higher for patients who are 50 years or older. Given the serious complications in elderly patients, we suggest that BTX-A may be a novel strategy for middle-aged and elderly patients who cannot tolerate drug side effects and who may be afraid of serious complications following MVD surgery.
Limitations
There are some limitations to our study, such as its small sample size and retrospective design. As a result of the latter, there was a relatively high number of patients whom we had to exclude as we could not obtain follow-up data. In addition, this research is a single-center study, which may introduce biases related to patient selection and treatment. All patients were from the Han ethnic group, meaning the results may be not generalizable to other populations. An advantage of our study is the relatively long follow-up duration. Future research into the mechanisms of TN will provide a more comprehensive understanding of the use of BTX-A for the clinical management of TN.
Conclusion
Local injections of BTX-A may be efficient and safe for TN treatment which lasts several months. This could be a novel strategy for some patients, particularly middle-aged and elderly people who cannot tolerate drug side effects and feel afraid of serious complications following MVD.
Ethics approval and informed consent
The study protocol was approved by the Ethics Committee of Zhengzhou University (Zhengzhou, People's Republic of China). All patients provided written informed consent to participate in the study.
Acknowledgments
This study was funded by the National Natural Science Foundation of China (81371438), the National Natural Science Foundation of China (81771397) and a project of the Henan Health Department (201203006).
Author contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work
Disclosure
The authors report no conflicts of interest in this work.
References
1. Headache Classification Committee of the International Headache Society (IHS). International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia. 2013;33(9):629–808.
2. Cruccu G, Gronseth G, Alksne J, et al.; for American Academy of Neurology Society; for European Federation of Neurological Society. AAN-EFNS guidelines on trigeminal neuralgia management. Eur J Neurol. 2008;15(10):1013–1028. doi:10.1111/j.1468-1331.2008.02131.x
3. Wu CJ, Shen JH, Chen Y, Lian YJ. Comparison of two different formulations of botulinum toxin A for the treatment of blepharospasm and hemifacial spasm. Turk Neurosurg. 2011;21(4):625–629.
4. Aurora SK, Dodick DW, Turkel CC, et al. OnabotulinumtoxinA for treatment of chronic migraine: results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 1 trial. Cephalalgia. 2010;30(7):793–803. doi:10.1177/0333102410364676
5. Diener HC, Dodick DW, Aurora SK, et al. OnabotulinumtoxinA for treatment of chronic migraine: results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 2 trial. Cephalalgia. 2010;30(7):804–814. doi:10.1177/0333102410364677
6. Negro A, Curto M, Lionetto L, Giamberardino MA, Martelletti P. Chronic migraine treatment: from OnabotulinumtoxinA onwards. Expert Rev Neurother. 2016;16(10):1217–1227. doi:10.1080/14737175.2016.1200973
7. Sandrini G, De Icco R, Tassorelli C, Smania N, Tamburin S. Botulinum neurotoxin type A for the treatment of pain: not just in migraine and trigeminal neuralgia. J Headache Pain. 2017;18(1):38. doi:10.1186/s10194-017-0744-z
8. Micheli F, Scorticati MC, Raina G. Beneficial effects of Botulinum Toxin Type A for patients with painful tic convulsif. Clin Neuropharmacol. 2002;25(5):260–262. doi:10.1097/00002826-200209000-00006
9. Borodic GE, Acquadro MA. The use of botulinum toxin for the treatment of chronic facial pain. J Pain. 2002;3(1):21–27.
10. Allam N, Brasil-Neto JP, Brown G, Tomaz C. Injections of botulinum Toxin Type A produce pain alleviation in intractable trigeminal neuralgia. Clin J Pain. 2005;21(2):182–184. doi:10.1097/00002508-200503000-00010
11. Türk U, Ilhan S, Alp R, Sur H. Botulinum toxin and intractable trigeminal neuralgia. Clin Neuropharmacol. 2005;28(4):161–162. doi:10.1097/01.wnf.0000172497.24770.b0
12. Piovesan EJ, Teive HG, Kowacs PA, et al. An open study of Botulinum-A Toxin treatment of trigeminal neuralgia. Neurology. 2005;65(8):1306–1308. doi:10.1212/01.wnl.0000180940.98815.74
13. Zuniga C, Diaz S, Piedimonte F, Micheli F. Beneficial effects of Botulinum Toxin Type A in trigeminal neuralgia. Arq Neuropsiquiatr. 2008;66(3A):500–503. doi:10.1590/S0004-282X2008000400012
14. Ngeow WC, Nair R. Injection of Botulinum Toxin Type A (BOTOX) into trigger zone of trigeminal neuralgia as a means to control pain. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109(3):e47–e50. doi:10.1016/j.tripleo.2009.03.021
15. Bohluli B, Motamedi MH, Bagheri SC, et al. Use of Botulinum Toxin A for drug-refractory trigeminal neuralgia: preliminary report. Oral Surg Oral Med Oral PatholOral Radiol Endod. 2011;111(1):47–50. doi:10.1016/j.tripleo.2010.04.043
16. Lunde HM, Torkildsen O, Bo L, et al. Botulinum toxin as monotherapy in symptomatic trigeminal neuralgia. Headache. 2016;56(6):1035–1039. doi:10.1111/head.12791
17. Wu CJ, Lian YJ, Zheng YK, et al. Botulinum Toxin Type A for the treatment of trigeminal neuralgia: results from a randomized, double-blind, placebo-controlled trial. Cephalalgia. 2012;32(6):443–450. doi:10.1177/0333102412441721
18. Zhang H, Lian Y, Ma Y, et al. Two doses of Botulinum Toxin Type A for the treatment of trigeminal neuralgia: observation of therapeutic effect from a randomized, double-blind, placebo-controlled trial. J Headache Pain. 2014;15:65. doi:10.1186/1129-2377-15-65
19. Zhang H, Lian Y, Xie N, Chen C, Zheng Y. Single-dose botulinum Toxin Type A compared with repeated-dose for treatment of trigeminal neuralgia: a pilot study. J Headache Pain. 2017;18(1):81. doi:10.1186/s10194-017-0793-3
20. Li S, Lian YJ, Chen Y, et al. Therapeutic effect of Botulinum Toxin-A in 88 patients with trigeminal neuralgia with 14-month follow-up. J Headache Pain. 2014;15:43. doi:10.1186/1129-2377-15-43
21. Cruccu G, Truini A. Refractory trigeminal neuralgia. Non-surgical treatment options. CNS Drugs. 2013;27(2):91–96. doi:10.1007/s40263-012-0023-0
22. Dworkin RH, Turk DC, Wyrwich KW, et al. Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. J Pain. 2008;9(2):105–121. doi:10.1016/j.jpain.2007.09.005
23. Apalla Z, Sotiriou E, Lallas A, Lazaridou E, Ioannides D. Botulinum toxin a in postherpetic neuralgia: a parallel, randomized, double-blind,single-dose, placebo-controlled trial. Clin J Pain. 2013;29(10):857–864. doi:10.1097/AJP.0b013e31827a72d2
24. Chen WT, Yuan RY, Chiang SC, et al. OnabotulinumtoxinA improvestactile and mechanical pain perception in painful diabetic polyneuropathy. Clin J Pain. 2013;29(4):305–310. doi:10.1097/AJP.0b013e318255c132
25. Yuan RY, Sheu JJ, Yu JM, et al. Botulinum toxin for diabetic neuropathic pain: a randomized double-blind crossover trial. Neurology. 2009;72(17):1473–1478. doi:10.1212/WNL.0b013e3181a9fad1
26. Taylor M, Silva S, Cottrell C. Botulinum Toxin Type-A (BOTOX) in the treatment of occipital neuralgia: a pilot study. Headache. 2008;48(10):1476–1481. doi:10.1111/j.1526-4610.2008.01089.x
27. Bahgat D, Ray DK, Raslan AM, McCartney S, Burchiel KJ. Trigeminal neuralgia in young adults. J Neurosurg. 2011;114(5):1306–1331. doi:10.3171/2010.10.JNS10781
28. Phan K, Rao PJ, Dexter M. Microvascular decompression for elderly patients with trigeminal neuralgia. J Clin Neurosci. 2016;29:7–14. doi:10.1016/j.jocn.2015.11.027
29. Chakravarthi PS, Ghanta R, Kattimani V. Microvascular decompression treatment for trigeminal neuralgia. J Craniofac Surg. 2011;22(3):894–898. doi:10.1097/SCS.0b013e31821a07b7
30. Luvisetto S, Gazerani P, Cianchetti C, Pavone F. Botulinum Toxin Type A as a therapeutic agent against headache and related disorders. Toxins. 2015;7(9):3818–3844. doi:10.3390/toxins7093818
31. Mueller D, Obermann M, Yoon MS, et al. Prevalence of trigeminal neuralgia and persistent idiopathic facial pain: a population-based study. Cephalalgia. 2011;31(15):1542–1548. doi:10.1177/0333102411424619
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.