Back to Journals » Clinical Interventions in Aging » Volume 17
Bone-Mounted Robotic System in Minimally Invasive Spinal Surgery for Osteoporosis Patients: Clinical and Radiological Outcomes
Authors Su YF ![]() , Tsai TH, Lieu AS, Lin CL, Chang CH, Tsai CY, Su HY
, Tsai TH, Lieu AS, Lin CL, Chang CH, Tsai CY, Su HY ![]()
Received 29 January 2022
Accepted for publication 11 April 2022
Published 22 April 2022 Volume 2022:17 Pages 589—599
DOI https://doi.org/10.2147/CIA.S359538
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Yu-Feng Su,1,2 Tai-Hsin Tsai,1,3 Ann-Shung Lieu,1,3,4 Chih-Lung Lin,1– 3 Chih-Hui Chang,1,2 Cheng-Yu Tsai,4– 6 Hui-Yuan Su1,3
1Division of Neurosurgery, Department of Surgery, Kaohsiung Medical University, Kaohsiung, Taiwan; 2Graduate Institute of Clinical Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan; 3Graduate Institute of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan; 4Faculty of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan; 5Ph.D. Program in Environmental and Occupational Medicine, College of Medicine, Kaohsiung Medical University and National Health Research Institutes, Kaohsiung, Taiwan; 6Post Baccalaureate Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan
Correspondence: Cheng-Yu Tsai; Hui-Yuan Su, Division of Neurosurgery, Department of Surgery, Kaohsiung Medical University Hospital, Kaohsiung Medical University, No. 100 Tzyou 1st Road, Kaohsiung, 80708, Taiwan, Tel +886-7-3215049, Fax +886-7-3215039, Email [email protected]; [email protected]
Purpose: Severe complications, including screw loosening events and low fusion rates, in spinal fusion surgery using the traditional open method are problematic. This retrospective study aimed to evaluate the rate of screw loosening and the clinical outcomes of bone-mounted miniature robot-assisted pedicle screw placement in patients treated for degenerative spinal disease.
Patients and Methods: Data were collected from the medical records of 118 patients (mean age, 69 years). Differences in clinical outcomes, including the Oswestry disability index, visual analog scale score, screw loosening rate, cage fusion rate, and complications, were evaluated among different bone mineral densities.
Results: The screw loosening and cage fusion rates for all patients, normal bone mineral density, osteopenia, and osteoporosis groups were 12%, 8.6%, 13.1%, and 14%, respectively, and 85.3%, 93%, 82.5%, and 81.4%, respectively. There was a higher screw loosening rate and a lower cage fusion rate in the osteopenia and osteoporosis groups than in the normal bone density group. The accuracy of the screw placement was 97.3%. There were no statistically significant differences in the Oswestry disability index and visual analog scale scores, and no major complications for dural tear or vascular or visceral injury.
Conclusion: Our study demonstrated an acceptable screw loosening rate in patients with osteoporosis compared to that in patients with normal bone mineral density. The robotic system resulted in accurate screw placement in patients with osteoporosis.
Keywords: robotic surgery, screw loosening rate, spinal fixation, spinal fusion, spinal fusion rate
Introduction
Pedicle screw insertion is an essential step for spinal fusion surgery and can offer strength for cage fusion. However, insertion of the transpedicle screw is associated with several complications such as screw loosening, screw pullout, and breakage. Screw loosening is a common complication, varying from less than 1% to 15% in non-osteoporotic patients and up to 60% in osteoporotic subjects.1,2 The rate of screw loosening is significantly related to low bone quality in osteopenia and osteoporotic bones.3 Various solutions have been suggested to reduce such events, including the use of conical pedicle screws, increase in the diameter and length of screws, use of expandable or coated pedicle screws, application of a cannulated pedicle screw for bone cement augmentation, and different screw insertion techniques such as bicortical fixation and cortical bone screw trajectory.4
High screw loosening rate up to 54% was reported in open spine surgery by free-hand placement of pedicle screw.5 For free-hand techniques, screw malposition rate of up to 29% is reported in the literature. A study using human lumbar vertebrae proved that lateral violation of the pedicle attenuated the biomechanical strength of the redirection screw, and the biomechanical data were correlated with bone mineral density.6 Robot-assisted spine surgery has recently emerged as a viable tool to enable less invasive and higher-precision surgery.7 Many studies have demonstrated that robot-assisted screw placement results in greater accuracy than conventional pedicle screw placement.8–11 Most studies concerning robotic spinal surgery have discussed the accuracy of spinal instrumentation,12 radiation exposure,12 accessibility, cost-effectiveness, decrease in complication rate, and the learning curve for the surgeon.13–17 However, the screw loosening rate, spinal fusion rate, and functional outcomes in spinal surgery with the assistance of a robotic system have rarely been discussed, especially in patients with osteoporosis.
Screw loosening events and cage nonunion remain major complications in osteoporosis patients undergoing spinal fixation and fusion surgery. To solve this problem, many new methods have been introduced, including minimally invasive surgery with the assistance of a robotic system.18 We hypothesize that robot-assisted spine surgery can improve the accuracy of pedicle screw placement, which can reduce the screw loosening rate and further increase the cage fusion rate. This study aimed to evaluate the clinical benefits of using a robotic system in patients with osteoporosis who underwent minimally invasive spinal fixation and fusion surgery.
Materials and Methods
Study Sources
This retrospective study evaluated the rate of screw loosening and the clinical outcomes of spinal fusion surgery with bone-mounted miniature robot-assisted pedicle screw insertion in patients with osteoporosis. Between May 2013 and April 2016, 208 consecutive patients with degenerative spine disease underwent surgery for minimally invasive spinal fixation and fusion with bone-mounted miniature robot-assisted pedicle screw insertion. A total of 118 patients with a mean age of 69 years (range, 50–91 years) (Table 1) were included in this study according to the inclusion and exclusion criteria. Of these, 88 were women, and 33 were men. Bone mineral density (BMD) was evaluated preoperatively by dual-energy X-ray absorptiometry (DEXA) (Hologic QDR-4500SL, Waltham, MA) in all patients. The flowchart of the study design is shown in Figure 1. This retrospective study was approved by the institutional review board and ethics committee of Kaohsiung Medical University Hospital. Informed consent was obtained from all patients. This case series is reported in accordance with the PROCESS guidelines.19
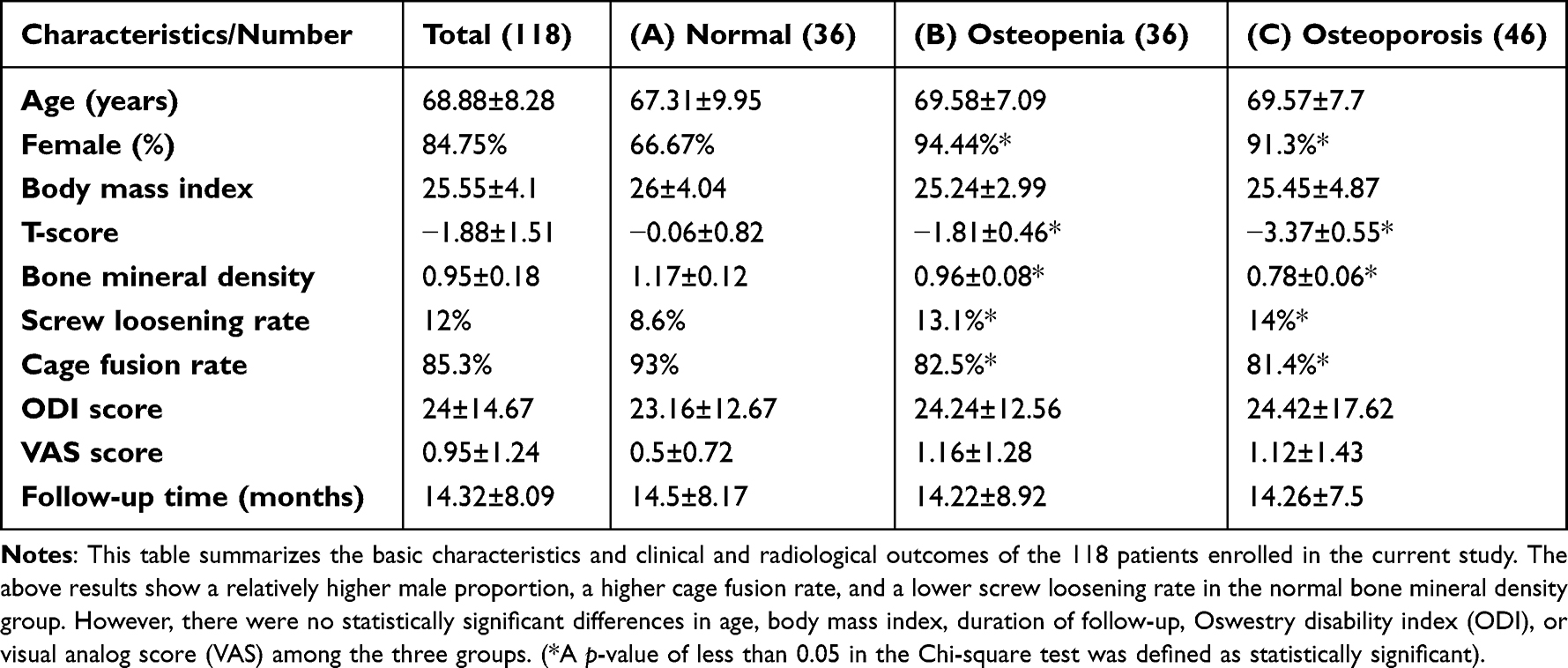 |
Table 1 Clinical Characteristics and the Clinical and Radiological Outcomes of 118 Patients with Robot-Guided Pedicle Screw Placement |
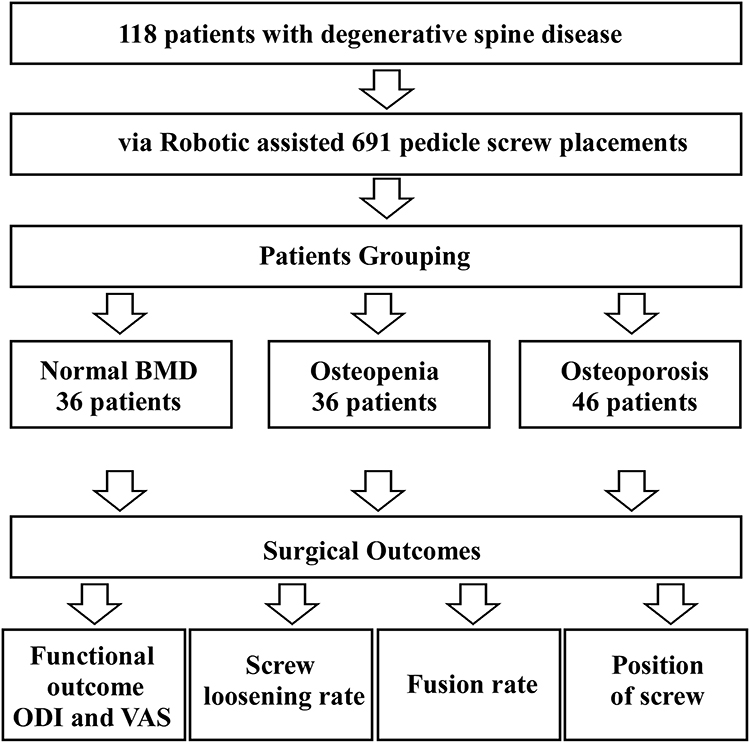 |
Figure 1 Flowchart of the study. In total, 118 patients diagnosed with degenerative spine disease were enrolled in this retrospective study, and all patients underwent spinal fixation and fusion through minimally invasive surgery with the assistance of a robotic system. They were classified into three groups: normal, osteopenia, and osteoporosis, according to the World Health Organization’s diagnostic criteria for osteoporosis. There were 36 patients in the normal group, 36 in the osteopenia group, and 46 in the osteoporosis group. After the operation, the surgical outcomes were evaluated, including the ODI (Oswestry disability index), VAS (visual analog score), screw loosening rate, and spinal fusion rate. |
Selection of Participants
The inclusion criteria consisted of: (1) patients diagnosed with degenerative spine disease, such as degenerative spondylolisthesis, disc herniation, and spinal stenosis; (2) all patients evaluated by DEXA measurement of the spine to determine the BMD; (3) all patients with back pain and varying neurological deficits such as radiation pain, numbness, and weakness, refractory to conservative treatment for six months; and (4) all patients undergoing pedicle screw fixation with the assistance of the bone-mounted miniature robotic system followed by minimally invasive surgery-transforaminal lumbar interbody fusion or posterior lumbar interbody fusion.
The exclusion criteria were as follows: (1) spinal malignancy, (2) spinal infection, (3) not undergoing examination with DEXA, and (4) use of cement augmentation for fixation of the screws.
Patients Grouping
The patients were grouped according to the World Health Organization’s diagnostic criteria into normal BMD, osteopenia, and osteoporosis, if the patient’s T-score was greater than −1.0 (T-score > −1.0 SD, standard deviation), equal or less than −1.0 and equal or greater than −2.5 (−1.0 SD ≥T-score ≥ −2.5 SD), or less than −2.5 (T-score < −2.5 SD), respectively.20 All patients were categorized into three groups: the normal BMD group (36 patients), osteopenia group (36 patients), and osteoporosis group (46 patients).
Surgical Techniques
There were six surgeons participating in the surgeries. All the surgeons had experiences of 50 or more cases before participating in this study. All procedures were performed by the same surgical team, with prone positioning required for robotic-assisted pedicle screw placement. The Renaissance robotic system procedures included preoperative planning, mounting, registration, robot assembly, drilling execution, Kirschner wire (K-wire) insertion, and cannulated screw insertion. Insertion of the guided K-wire along the preoperatively scheduled trajectory was assisted by the Renaissance robotic system. After the insertion of the guided K-wire, the instruments of the Renaissance robotic system, including the mounting framework and robotic arm, were removed. The pedicle screw was then placed through a guided K-wire. Minimally invasive surgery means avoidance of muscular destruction during pedicle screw placement through the guided K-wire. Then we inserted the cage by trans-foraminal or posterior lumbar interbody access for cage placement. In this study, the Medtronic pedicle screw system (ReBorn Essence lumbar fixation system cannulated polyaxial screw) or DePuy Spine System (VIPER lumbar fixation system cannulated polyaxial screw) was used.
The screws were inserted along the guided K-wire and placed by the robotic arm, with screw diameters varying from 4.5 to 7.5 mm. Spinal fusion surgery was performed by transforaminal interbody fusion or posterior lumbar interbody fusion, with interbody fusion using Capstone (Medtronic Sofamor Danek) or Zimmer Biomet trabecular metal cages. Autologous bone from the resected lamina was placed in the interbody space to supplement the bone fusion. The surgical procedures for K-wire insertion, with the assistance of the Renaissance robotic system, are shown in Figures 2 and 3.
 |
Figure 2 The procedures of robotic surgery. The surgical technique was combined with a secondary registration during surgery to increase the accuracy of pedicle screw placement, guided with a bone-mounted miniature robot system. (A and B) Preoperative planning: preoperative computed tomography images are converted to three-dimensional reconstruction images, and the best trajectory and appropriate size of screw, including the diameter and length, are decided on the working station of the robotic system. (C) Attachment to the patient’s spine: The bone-mounted frame is applied and fixed on the patient’s spine firmly. (D) Robot packaging and initiation: The robot is attached to the bone-mounted frame. Appropriate channel for the robot attachment is decided by the system, allowing the robotic arm to operate according to the preoperative plan. Drilling implementation: A guiding tube is inserted to the entry point of the pedicle screw along the trajectory decided by the robotic arm. Drilling along the guiding tube is subsequently performed by a surgeon, and then a Kirschner-wire is inserted along the drilling tract. |
 |
Figure 3 Secondary registration. (A) Anteroposterior view of the guided pin inserted with assistance of the robotic system. (B) Oblique view of the guided pin inserted with assistance of the robotic system. (C and D) Secondary registration (Reregistration): After implantation of the Kirschner-wire, anteroposterior and oblique radiographic plain films are obtained again. Using the same system, registration with the preoperative computed tomography images is again performed. Then, the deviation of the guided pins is evaluated compared with the original trajectory designed by the robotic system preoperatively. |
Surgical Outcomes
Clinical outcomes, including the Oswestry disability index (ODI), visual analog scale (VAS), screw loosening rate, cage fusion rate, position of the screw, and complications, were evaluated with a mean follow-up period of 14 months (range: 4–42 months). There were two observers participating in the study and not being aware of the characteristics of every individual. They evaluated screw position and bone fusion independently. When encountering different results of screw position and bone fusion, the third observer was consulted to make the final decision.
Functional Outcomes
Patients’ functional outcomes were assessed using the VAS and the ODI scoring system.
Accuracy of the K-Wire Placement
The accuracy of K-wire placement was assessed with an intraoperative robotic grading system, a technique developed by Dr. Tsai, which has yet to be validated.21–23
Position of the Screw Placement
The position and accuracy of screw placement were assessed on immediate postoperative and follow-up radiographs by using a technique developed in the literature.24
Screw Loosening and Bone Non-Union
Screw loosening and bone nonunion were checked on a plain roentgenogram during postoperative follow-up. Anteroposterior, lateral, and flexion-extension lumbosacral X-ray plain films were obtained to evaluate pedicle screw loosening and position. Screw loosening events were defined as a clear zone around a pedicle screw on anteroposterior or lateral radiographs when the radiolucency was 1 mm or wider at the bone-screw interface.1
Bone fusion was determined on lateral radiographs when: (1) clear trabecular bone bridging across the segment to be fused was seen; (2) translation of 3 mm or less and an angulation of 5° or less on full flexion-extension lateral radiographs; and (3) continuous bone growth connecting the vertebral bodies was seen.25–27
Complications
Complications included displacement of the screws, broken screws, bending screws, fractured pedicles, dural tears, and vascular and visceral problems.
Statistical Analysis
Statistical analysis was performed using SPSS software (version 19.0; SPSS, Inc., Chicago, IL, USA), and the data are presented as mean±SD. An independent t-test was performed to evaluate variables including age, body mass index, follow-up time, T-score, BMD, screw loosening rate, cage fusion rate, postoperative ODI, and VAS, while a chi-square test was performed to evaluate sex among the groups with different bone densities. Statistical significance was set at p< 0.05.
Results
Clinical Characteristics
The T-scores and bone mineral densities of the three groups (normal BMD, osteopenia, and osteoporosis) are shown in Table 1. The average T-scores of the normal, osteopenia, and osteoporosis groups were −0.06±0.82, −1.81±0.46, and −3.37±0.55 SD, respectively, and the BMD measures of the normal, osteopenia, and osteoporosis groups were 1.17±0.12, 0.96±0.08, and 0.78±0.06 gm/cm3, respectively. There were no significant differences in the clinical characteristics among the normal, osteopenia, and osteoporosis patients in terms of age, body mass index, and duration of follow-up. The results showed a higher proportion of female patients in the osteopenia and osteoporosis groups than in the normal BMD group. All three groups were compared with a statistically significant p-value of less than 0.05. Statistically significant differences were observed among the three groups (Table 1).
Surgical Outcomes
Functional Outcomes
The ODI and VAS scores were evaluated at the final follow-up visit. The average ODI scores of the normal, osteopenia, and osteoporosis patient groups were 23.16±12.67, 24.24±12.56, and 24.42±17.62, respectively, with the average VASs of these groups being 0.5±0.72, 1.16±1.28, and 1.12±1.43, respectively. There were no statistically significant differences in the ODI and VAS scores among the three groups (Table 1).
Screw Loosening
A total of 691 pedicle screws were inserted to achieve spinal stabilization. Fourteen (2.02%), 619 (89.58%), and 58 (8.39%) screws were placed at the thoracic, lumbar, and sacral spinal levels, respectively. The screw loosening rates were 83/691 (12%) in all groups, 19/221 (8.6%) in the normal group, 28/214 (13.1%) in the osteopenia group, and 36/256 (14%) in the osteoporosis group. The screw loosening rate was higher in the osteopenia and osteoporosis groups than that in the normal bone density group (p<0.05).
Bone Fusion
In our study, 190 spinal segments underwent cage fusion. The total spinal fusion rate was 162/190 (85.3%). There was no significant difference in the fusion levels among the normal, osteopenia, and osteoporosis groups. The fusion rates of the three different groups were as follows: 53/57 (93%) in the normal group, 52/63 (82.5%) in the osteopenia group, and 57/70 (81.4%) in the osteoporosis group. There was a lower cage fusion rate in the osteopenia and osteoporosis groups than that in the normal bone density group (p<0.05).
Position of the Screw
The distribution of the postoperative position of screw placement was examined using radiographs, with displacement classified into four groups: superior, inferior, medial, and lateral. The accuracies of the three different groups were as follows: 217/221, 98.2% in the normal group; 202/214, 94.4% in the osteopenia group; and 253/256, 98.8% in the osteoporosis group. The accuracy of the screw placement in all the three groups was 97.3% (672/691).
Complications
In total, four cases were encountered due to mechanical complications, including two broken screws and two fractured pedicles. There were no major complications of dural tear or vascular or visceral injuries.
Discussion
Several factors might affect the stability of pedicle screw placement, including bone quality or density, screw design, and surgical technique.28 Several biomechanical studies have demonstrated a high correlation between bone density and stability of pedicle screw in vitro.29–32 In the literature, screw loosening rates ranging from 13.2% to 54.7% have been reported.5,33–37 The spinal loosening rate in open spinal surgery for single level posterolateral fusion and fixation is 18.3%.38 In contrast to a single level, a very high screw loosening rate of 54.7% was reported in cases that received multi-level fusion surgery for degenerative disease of the lumbar spine.5 In osteoporosis, screw loosening rates of 22.2% in patients undergoing surgery for transforaminal lumbar interbody fusion and 32.3% in cases undergoing surgery for posterior lumbar interbody fusion have been reported.2,39 Multi-level spinal instruments and osteoporosis seem to be risk factors predisposing to screw loosening events.3,5 The total screw loosening rate in our study was 12%, and that for osteoporotic patients was 14%, which is lower than the rates of 22.2% and 32.3% in osteoporotic patients undergoing transforaminal lumbar interbody fusion and posterior lumbar interbody fusion, respectively, reported in the literature. Our study showed significant differences in screw loosening rates between the normal, osteopenia, and osteoporosis groups. BMD is thought to be a crucial factor influencing the development of screw loosening events in pedicle screw fixation, and some authors have reported a threshold for BMD that determines the result of screw loosening events. It might predispose an increase in screw loosening rate if BMD is below the value of such an established threshold.32,35,40 Although low BMD is still a risk factor for screw loosening, as shown in the results of our study, minimally invasive surgery accompanied with robotic assistance seems to improve the screw loosening rate in osteoporosis compared with the results of the literature.
The interface between the cancellous bone and the screw is another factor that influences screw stability. Pedicle screws achieve fixation by anchoring the cancellous bone inside the pedicles of the vertebrae rather than in the cortical bone of the pedicles.41 Bone remodeling is most prominent on the cancellous bone surfaces. Excessive remodeling poses a risk to bone strength as it destabilizes bone and introduces stress concentrators.42 In general, the maximal anchoring surface on the cancellous bone is very important for screw stability due to compromised cancellous bone in an osteoporotic group. We hypothesize that excellent accuracy of pedicle screw placement could attenuate cortical violation and increase the interface between the pedicle screw and the cancellous bone in the osteoporosis group.
The present study shows that the Renaissance robotic system offers high accuracy in pedicle screw placement. The accuracy in related studies has been reported to range from 85% to 100%.13 Devito et al reviewed 3271 pedicle screw placements in 635 patients from 14 medical centers and reported an accuracy of 98.3%.43 Kantelhardt et al compared pedicle screw placements performed manually with those in which the Renaissance robotic system was used and reported higher accuracy in a group of patients who underwent robotic spinal surgery.44 Le et al found that robot-assisted procedures are more accurate and have higher fusion rates than fluoroscopy-assisted procedures.8 The Renaissance robotic system can guide the surgeon to choose a better intraoperative pedicle screw trajectory safely and efficiently.21–23 According to the system used by Kou et al, the intraoperative accuracy of the screw is up to 98.74%. Taken together, the robotic system offers high accuracy in pedicle screw placement during surgery and prevents repeated tapping procedures.
Our study found significant differences in the screw loosening rates between the normal, osteopenia, and osteoporosis groups. Low bone mineral density is a predisposing factor for screw loosening events,32,35,40 as also demonstrated in our study. However, our osteoporotic group presented a relatively low screw loosening rate compared to that reported in the literature. There are several possible explanations for these results. We infer that the low screw loosening rate in the osteoporosis group might be attributed to the excellent accuracy of screw placement, which attenuates cortical violation of the pedicle and reduction of muscular destruction in minimally invasive surgery.
Three hypotheses are proposed to explain how stability can be enhanced by increasing the accuracy of screw placement. First, the precise trajectory confirms the maximal anchoring surface between the screw and cancellous bone, and better pullout forces were determined for screws implanted with less cortical violation in the trajectory tract.45 A larger anchoring surface on the osteoporotic cancellous bone indicates higher stability of the transpedicle screw. Second, a guided K-wire was inserted into the pedicle with assistance from the robotic arm before performing the transpedicle screw. The robotic system requires fewer tapping events using an electronic drill to insert the guided pins into the pedicles, with the minimum number of tapping events to the pedicles guaranteeing less destruction of the pedicles. Finally, we replaced any malpositioned pins with the assistance of the robotic system after the secondary registration. The severity of pedicle destruction after replacement of these guided pins with the assistance of the robotic arm was less than that caused by repositioning by the trocar using the freehand method. Repeated tapping with a trocar on the pedicle worsened the destruction of the cancellous bone of the pedicle. Pedicle screw tracts were not overly tapped or repeatedly augmented using the robotic system. Less destruction of the cancellous bone of the pedicle seemed to contribute to the higher stability of the transpedicle screws, especially in the osteoporotic group.
In addition to the excellent accuracy of pedicle screw placement, minimally invasive spinal surgery is considered a key factor in reducing the screw loosening rate in osteoporosis patients. Minimally invasive spinal surgery has low screw loosening rates of 0–7.14% and high fusion rates of 94.8–100%.45–48 In the literature, less paraspinal muscle degeneration is noted in the operation of minimally invasive transforaminal lumbar interbody fusion than in conventional open surgery.49 The increased cross-sectional area of the multifidus and the psoas major muscle after spinal stabilization exercise enhances spinal stability and reduces pain in degenerative disc disease.50 Therefore, minimally invasive spinal surgery can reduce excessive spinal tissue damage related to surgery, thereby reducing the screw loosening rate and increasing the cage fusion rate. Moreover, previous literature also reported that patients with osteoporosis who cannot tolerate traditional open surgery may be treated with percutaneous posterior fixation techniques.51 Taken together, minimally invasive spinal fusion surgery was performed after the insertion of guided pins with the assistance of a robotic system. In addition to the precise position of the transpedicle screw, preserved paraspinal muscle might be another reason for the relatively low screw loosening rate in patients with osteoporosis. In our study, we performed minimally invasive surgery accompanied by the assistance of a robotic system to place the pedicle screw percutaneously and preserve the paraspinal muscle group. Cage fusion was achieved by transforaminal lumbar interbody fusion or posterior lumbar interbody fusion.
This study had several limitations. This was not a prospective study, and the sample size of the patient group was small. In addition, the follow-up period was too short to confirm definitive loosening and fusion rates. However, this report represents the clinical outcomes of minimally invasive spinal surgery with the assistance of a robotic system in patients with osteoporosis. A larger prospective clinical trial with a longer follow-up period will be performed in the future.
Conclusion
Accurate placement of the transpedicle screws with robotic assistance and less paraspinal muscle destruction in surgeries for degenerative spine disease could be the main factors lowering the screw loosening rate, especially in patients with osteoporosis. A more accurate trajectory of the pedicle screws leads to a stronger anchoring force in the cancellous bone, which plays a key role in fixation with the transpedicle screws. Although osteoporosis is a risk factor, our study demonstrated an acceptable screw loosening rate in osteoporosis patients compared with patients with normal BMD, and the robotic system offered an excellent result in patients with osteoporosis. Accordingly, the bone-mounted robotic system could serve as an effective surgical choice for spinal fixation and fusion surgery in patients with osteoporosis.
Acknowledgments
The authors received no specific funding for this work.
Ethics Approval and Informed Consent
This retrospective study is approved by the institutional review board and ethics committee of Kaohsiung Medical University Hospital. Informed consent is obtained from all patients. The study is complied with the Declaration of Helsinki.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Galbusera F, Volkheimer D, Reitmaier S, et al. Pedicle screw loosening: a clinically relevant complication? Eur Spine J. 2015;24:1005–1016. doi:10.1007/s00586-015-3768-6
2. Rometsch E, Spruit M, Zigler JE, et al. Screw-related complications after instrumentation of the osteoporotic spine: a systematic literature review with meta-analysis. Glob Spine J. 2020;10:69–88. doi:10.1177/2192568218818164
3. Bredow J, Boese CK, Werner CML, et al. Predictive validity of preoperative CT scans and the risk of pedicle screw loosening in spinal surgery. Arch Orth Trauma Surg. 2016;136:1063–1067. doi:10.1007/s00402-016-2487-8
4. Goldstein CL, Brodke DS, Choma TJ. Surgical management of spinal conditions in the elderly osteoporotic spine. Neurosurg. 2015;77(Suppl 4):S98–S107. doi:10.1227/neu.0000000000000948
5. Röllinghoff M, Schlüter-Brust K, Groos D, et al. Mid-range outcomes in 64 consecutive cases of multilevel fusion for degenerative diseases of the lumbar spine. Orth Rev. 2010;2:e3. doi:10.4081/or.2010.e3
6. Stauff MP, Freedman BA, Kim JH, et al. The effect of pedicle screw redirection after lateral wall breach–a biomechanical study using human lumbar vertebrae. Spine J. 2014;14(1):98–103. doi:10.1016/j.spinee.2013.03.028
7. Vadalà G, De Salvatore S, Ambrosio L, et al. Robotic spine surgery and augmented reality systems: a state of the art. Neurospine. 2020;17:88–100. doi:10.14245/ns.2040060.030
8. Le X, Tian W, Shi Z, et al. Robot-assisted versus fluoroscopy-assisted cortical bone trajectory screw instrumentation in lumbar spinal surgery: a matched-cohort comparison. World Neurosurg. 2018;120:e745–e751. doi:10.1016/j.wneu.2018.08.157
9. Lonjon N, Chan-Seng E, Costalat V, Bonnafoux B, Vassal M, Boetto J. Robot-assisted spine surgery: feasibility study through a prospective case-matched analysis. Eur Spine J. 2016;25:947–955. doi:10.1007/s00586-015-3758-8
10. Keric N, Doenitz C, Haj A, et al. Evaluation of robot-guided minimally invasive implantation of 2067 pedicle screws. Neurosurg Focus. 2017;42:E11. doi:10.3171/2017.2.focus16552
11. Schatlo B, Molliqaj G, Cuvinciuc V, Kotowski M, Schaller K, Tessitore E. Safety and accuracy of robot-assisted versus fluoroscopy-guided pedicle screw insertion for degenerative diseases of the lumbar spine: a matched cohort comparison. J Neurosurg Spine. 2014;20:636–643. doi:10.3171/2014.3.spine13714
12. Molliqaj G, Schatlo B, Alaid A, et al. Accuracy of robot-guided versus freehand fluoroscopy-assisted pedicle screw insertion in thoracolumbar spinal surgery. Neurosurg Focus. 2017;4:E14. doi:10.3171/2017.3.focus179
13. Joseph JR, Smith BW, Liu X, Park P. Current applications of robotics in spine surgery: a systematic review of the literature. Neurosurg Focus. 2017;42:E2. doi:10.3171/2017.2.focus16544
14. Hu X, Ohnmeiss DD, Lieberman IH. Robotic-assisted pedicle screw placement: lessons learned from the first 102 patients. Eur Spine J. 2013;22:661–666. doi:10.1007/s00586-012-2499-1
15. Schatlo B, Martinez R, Alaid A, et al. Unskilled unawareness and the learning curve in robotic spine surgery. Acta Neurochirurgica. 2015;157:
16. Fiani B, Quadri SA, Ramakrishnan V, Berman B, Khan Y, Siddiqi J. Retrospective review on accuracy: a pilot study of robotically guided thoracolumbar/sacral pedicle screws versus fluoroscopy-guided and computerized tomography stealth-guided screws. Cureus. 2017;9(7):e1437. doi:10.7759/cureus.1437
17. Fiani B, Quadri SA, Farooqui M, et al. Impact of robot-assisted spine surgery on health care quality and neurosurgical economics: a systemic review. Neurosurg Rev. 2020;43(1):17–25. doi:10.1007/s10143-018-0971-z
18. D’Souza M, Gendreau J, Feng A, Kim LH, Ho AL, Veeravagu A. Robotic-assisted spine surgery: history, efficacy, cost, and future trends. Rob Surg. 2019;6:9–23. doi:10.2147/rsrr.s190720
19. Agha RA, Sohrabi C, Mathew G, et al. The PROCESS 2020 guideline: updating consensus Preferred Reporting Of CasESeries in Surgery (PROCESS) guidelines. Int J Surg. 2020;84:231–235. doi:10.1016/j.ijsu.2020.11.005
20. Kanis JA, Melton LJ 3rd, Christiansen C, Johnston CC, Khaltaev N. The diagnosis of osteoporosis. J Bone Miner Res. 1994;9:1137–1141. doi:10.1002/jbmr.5650090802
21. Kuo KL, Su YF, Wu CH, et al. Assessing the intraoperative accuracy of pedicle screw placement by using a bone-mounted miniature robot system through secondary registration. PLoS One. 2016;11:e0153235. doi:10.1371/journal.pone.0153235
22. Tsai TH, Tzou RD, Su YF, Wu CH, Tsai CY, Lin CL. Pedicle screw placement accuracy of bone-mounted miniature robot system. Medicine. 2017;96:e5835. doi:10.1097/md.0000000000005835
23. Tsai TH, Wu DS, Su YF, Wu CH, Lin CL. A retrospective study to validate an intraoperative robotic classification system for assessing the accuracy of Kirschner wire (K-wire) placements with postoperative computed tomography classification system for assessing the accuracy of pedicle screw placements. Medicine. 2016;95:e4834. doi:10.1097/md.0000000000004834
24. Lonstein JE, Denis F, Perra JH, Pinto MR, Smith MD, Winter RB. Complications associated with pedicle screws. J Bone Joint Surg. 1999;81:1519–1528. doi:10.2106/00004623-199911000-00003
25. Burkus JK, Foley K, Haid RW, LeHuec JC. Surgical Interbody Research Group–radiographic assessment of interbody fusion devices: fusion criteria for anterior lumbar interbody surgery. Neurosurg Focus. 2001;10:E11. doi:10.3171/foc.2001.10.4.12
26. Lee CS, Kang KC, Chung SS, Park WH, Shin WJ, Seo YG. How does back muscle strength change after posterior lumbar interbody fusion? J Neurosurg Spine. 2017;26:163–170. doi:10.3171/2016.7.spine151132
27. Wu ZX, Gong FT, Liu L, et al. A comparative study on screw loosening in osteoporotic lumbar spine fusion between expandable and conventional pedicle screws. Arch Orth Trauma Surg. 2012;132:471–476. doi:10.1007/s00402-011-1439-6
28. Kuhns CA, Reiter M, Pfeiffer F, Choma TJ. Surgical strategies to improve fixation in the osteoporotic spine: the effects of tapping, cement augmentation, and screw trajectory. Global Spine J. 2014;4:47–54. doi:10.1055/s-0033-1361588
29. Carlson GD, Abitbol JJ, Anderson DR, et al. Screw fixation in the human sacrum. An in vitro study of the biomechanics of fixation. Spine. 1992;17:S196–S203. doi:10.1097/00007632-199206001-00023
30. Coe JD, Warden KE, Herzig MA, McAfee PC. Influence of bone mineral density on the fixation of thoracolumbar implants. A comparative study of transpedicular screws, laminar hooks, and spinous process wires. Spine. 1990;15:902–907. doi:10.1097/00007632-199009000-00012
31. Soshi S, Shiba R, Kondo H, Murota K. An experimental study on transpedicular screw fixation in relation to osteoporosis of the lumbar spine. Spine. 1991;16:1335–1341. doi:10.1097/00007632-199111000-00015
32. Wittenberg RH, Shea M, Swartz DE, Lee KS, White AA, Hayes WC. Importance of bone mineral density in instrumented spine fusions. Spine. 1991;16:647–652. doi:10.1097/00007632-199106000-00009
33. Ozawa T, Takahashi K, Yamagata M, et al. Insertional torque of the lumbar pedicle screw during surgery. J Orth Sci. 2005;10:133–136. doi:10.1007/s00776-004-0883-3
34. Glaser J, Stanley M, Sayre H, Woody J, Found E, Spratt K. A 10-year follow-up evaluation of lumbar spine fusion with pedicle screw fixation. Spine. 2003;28:1390–1395. doi:10.1097/01.brs.0000067112.15753.ad
35. Pihlajämaki H, Myllynen P, Böstman O. Complications of transpedicular lumbosacral fixation for non-traumatic disorders. J Bone Joint Surg. 1997;79:183–189. doi:10.1302/0301-620x.79b2.7224
36. Ohlin A, Karlsson M, Düppe H, Hasserius R, Redlund-Johnell I. Complications after transpedicular stabilization of the spine. A survivorship analysis of 163 cases. Spine. 1994;19:2774–2779. doi:10.1097/00007632-199412150-00007
37. Soini J, Laine T, Pohjolainen T, Hurri H, Alaranta H. Spondylodesis augmented by transpedicular fixation in the treatment of olisthetic and degenerative conditions of the lumbar spine. Clin Orth Relat Res. 1993;1993:111–116.
38. Kim DH, Hwang RW, Lee GH, et al. Comparing rates of early pedicle screw loosening in posterolateral lumbar fusion with and without transforaminal lumbar interbody fusion. Spine J. 2020;20:1438–1445. doi:10.1016/j.spinee.2020.04.021
39. Cho JH, Hwang CJ, Kim H, Joo YS, Lee DH, Lee CS. Effect of osteoporosis on the clinical and radiological outcomes following one-level posterior lumbar interbody fusion. J Orth Sci. 2018;23:870–877. doi:10.1016/j.jos.2018.06.009
40. Okuyama K, Abe E, Suzuki T, Tamura Y, Chiba M, Sato K. Influence of bone mineral density on pedicle screw fixation: a study of pedicle screw fixation augmenting posterior lumbar interbody fusion in elderly patients. Spine J. 2001;1:402–407. doi:10.1016/s1529-9430(01)00078-x
41. Langdahl B, Ferrari S, Dempster DW. Bone modeling and remodeling: potential as therapeutic targets for the treatment of osteoporosis. Ther Adv Musculoskeletal Dis. 2016;8:225–235. doi:10.1177/1759720x16670154
42. Defino HL, Vendrame JR. Role of cortical and cancellous bone of the vertebral pedicle in implant fixation. Eur Spine J. 2001;10:325–333. doi:10.1007/s005860000232
43. Devito DP, Kaplan L, Dietl R, et al. Clinical acceptance and accuracy assessment of spinal implants guided with SpineAssist surgical robot: retrospective study. Spine. 2010;35:2109–2115. doi:10.1097/BRS.0b013e3181d323ab
44. Kantelhardt SR, Martinez R, Baerwinkel S, Burger R, Giese A, Rohde V. Perioperative course and accuracy of screw positioning in conventional, open robotic-guided and percutaneous robotic-guided, pedicle screw placement. Eur Spine J. 2011;20:860–868. doi:10.1007/s00586-011-1729-2
45. Wang HW, Hu YC, Wu ZY, et al. Minimally invasive transforaminal lumbar interbody fusion and unilateral fixation for degenerative lumbar disease. Orth Surg. 2017;9:277–283. doi:10.1111/os.12345
46. Elmekaty M, Kotani Y, Mehy EE, et al. Clinical and radiological comparison between three different minimally invasive surgical fusion techniques for single-level lumbar isthmic and degenerative spondylolisthesis: minimally invasive surgical posterolateral fusion versus minimally invasive surgical transforaminal lumbar interbody fusion versus midline lumbar fusion. Asian Spine J. 2018;12:870–879. doi:10.31616/asj.2018.12.5.870
47. Bin Abd Razak HR, Dhoke P, Tay KS, Yeo W, Yue WM. Single-level minimally invasive transforaminal lumbar interbody fusion provides sustained improvements in clinical and radiological outcomes up to 5 years postoperatively in patients with neurogenic symptoms secondary to spondylolisthesis. Asian Spine J. 2017;11:204–212. doi:10.4184/asj.2017.11.2.204
48. Lin GX, Sharma S, Rui G, Song MS, Kim JS. Minimally invasive transforaminal lumbar interbody fusion with intraoperative fluoroscopy for disc space preparation: analysis of fusion rate and clinical results. Op Neurosurg. 2020;19:557–566. doi:10.1093/ons/opaa178
49. Fu CJ, Chen WC, Lu ML, Cheng CH, Niu CC. Comparison of paraspinal muscle degeneration and decompression effect between conventional open and minimal invasive approaches for posterior lumbar spine surgery. Sci Rep. 2020;10:14635. doi:10.1038/s41598-020-71515-8
50. Kim S, Kim H, Chung J. Effects of spinal stabilization exercise on the cross-sectional areas of the lumbar multifidus and psoas major muscles, pain intensity, and lumbar muscle strength of patients with degenerative disc disease. J Phys Ther Sci. 2014;26:579–582. doi:10.1589/jpts.26.579
51. Gazzeri R, Panagiotopoulos K, Princiotto S, Agrillo U. Spontaneous spinal arthrodesis in stand-alone percutaneous pedicle screw fixation without in situ fusion in patients with lumbar segmental instability: long-term clinical, radiologic, and functional outcomes. World Neurosurg. 2018;110:e1040–e1048. doi:10.1016/j.wneu.2017.11.159
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.