Back to Journals » Psychology Research and Behavior Management » Volume 16
Body Dissatisfaction and Restricted Diet in Chinese Adolescents: A Longitudinal Analysis
Authors Zhang T, Wang K, Gu T, Zhang Y, Zhang X
Received 12 June 2023
Accepted for publication 19 September 2023
Published 27 September 2023 Volume 2023:16 Pages 4003—4013
DOI https://doi.org/10.2147/PRBM.S423196
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Igor Elman
Tianyu Zhang,1 Kunyan Wang,1 Tingyu Gu,1 Yali Zhang,2 Xiangkui Zhang1
1School of Psychology, Northeast Normal University, Changchun, 130024, People’s Republic of China; 2College of Education, Hebei Normal University, Shijiazhuang, 050024, People’s Republic of China
Correspondence: Xiangkui Zhang, Email [email protected]
Background/Objective: Body dissatisfaction and restricted diet frequently co-occur among adolescents. However, the exact temporal relationship between the two is unclear. Furthermore, most relevant studies concentrate on Western cultural backgrounds, with only a few investigations conducted in many non-Western developing countries, including China. Therefore, this study aimed to investigate the mutual relationship between body dissatisfaction and restricted diet among Chinese adolescents.
Patients/Methods: We recruited a sample of 672 middle school students from China (358 females, mean age = 14.33± 0.94) and collected self-reported measures of body dissatisfaction and restricted diet at three-time points (with a five-month interval between each). We used cross-lagged models to examine the bidirectional relationship between body dissatisfaction and restricted diet.
Results: (1) Both cross-sectional and cross-lagged correlation analysis showed positive correlation between body dissatisfaction and restricted diet (r=0.29– 0.36; r=0.25– 0.35, Ps< 0.001); (2) The cross-lagged effect of body dissatisfaction on restricted diet was significant (β=0.09, 0.13, Ps< 0.01), and vice versa (β=0.20, 0.18, Ps< 0.001); (3) The differences in the associations between body dissatisfaction and restricted diet across gender were found.
Conclusion/Implications: There is a bidirectional relationship between adolescents’ body dissatisfaction and restricted diet. Our findings enrich the existing literature on body image and dietary health, thereby contributing to the reduction of negative body image and disordered eating among adolescents.
Keywords: adolescents, body dissatisfaction, restricted diet, longitudinal, cross-lagged
Introduction
Restricted diet is a crucial area of study in the field of obesity psychology and eating disorder research. Polivy, Heatherton, and Herman (1988) defined it as the chronic behavior of tightly controlling one’s diet for the purpose of managing weight.1 In recent years, owing to the widespread acceptance of the “thin is beautiful” notion, people have become more strict in their aspirations for body shape and appearance. A growing number of adolescents attempt to modify and regulate their body shape through dieting. Chen et al study suggested that the prevalence of various degrees of dieting has surpassed 70%,2 signifying a noteworthy and widespread concern. Although a restricted diet appears to get quick results in losing weight, it results in a rebound of weight in the long run, as well as a range of psychological and behavioral problems (such as anxiety, depression, anorexia nervosa, and bulimia nervosa), or even premature mortality.3–5 Thus, it is imperative to investigate the origins and ramifications of a restricted diet. However, research in this field has largely centered on Western cultural backgrounds, with few empirical studies conducted in developing countries, such as China.6 Consequently, further inquiry is required, specifically to elucidate the probable predictor variables of restricted diet in non-Western cultural milieus.
To further comprehend the underlying reasons for restricted diet and facilitate better prevention and control, extensive research has investigated risk factors associated with restricted diet. Among these factors, body dissatisfaction has been a particularly noteworthy concern.7 Negative body image belongs to a personal emotional level, referring to unpleasant emotional experiences towards one’s physical self, such as dissatisfaction with one’s weight or body shape.8 Currently, two different perceptions exist when exploring the relationship between body dissatisfaction and restricted diet. The first viewpoint suggests that body dissatisfaction may be the cause of restricted diet and exacerbate them.9,10 The other perspective posits that body dissatisfaction may be a consequence of restricted diet, resulting from excessive restricted diet.11,12
However, current research has placed more emphasis on the impact of body dissatisfaction on restricted diet, to some extent neglecting the role that restricted diet plays in body dissatisfaction. This is unfavorable in clarifying the reciprocal relation between variables. Moreover, existing empirical studies on body dissatisfaction and restricted diet in adolescents have mostly used cross-sectional sampling, failing to reveal how the two develop and change over time. With these in mind, we believe it is necessary to utilize longitudinal tracking and lagged cross-lagged analysis to shed light on the above issues.
The Role of Body Dissatisfaction in Restricted Diet
Body dissatisfaction may be the causal factor for the adoption of a restricted diet style, which may reinforce restricted diet behaviors. The Tripartite Influence Model proposed by Thompson et al suggests that sociocultural factors, such as appearance-related pressures from the media, family, peers, or significant others, may cause social comparison and internalization of thin ideals, which in turn may trigger individual body image concerns (eg, body dissatisfaction).13 These negative body image concerns increase the likelihood that adolescents will perceive restricted diet as a normative behavior under environmental pressure. As a result, they may engage in restricted diet and other abnormal eating behaviors. Cross-sectional studies have shown that the unrealistic standards for attractiveness set by modern society mean that the vast majority of individuals do not match these standards. Consequently, adolescents experience dissatisfaction with their appearance and this can lead to participation in extreme appearance management behaviors.14 Other studies have revealed a significant association between body dissatisfaction and restricted diet. Individuals who are perceived as overweight are more prone to experiencing body image concerns, resulting in unhealthy weight control behaviors like engaging in dieting.15 In addition, the theory of emotional eating also strengthens the association between body dissatisfaction and restricted diet.16 Body dissatisfaction, as an emotional experience of bodily displeasure, increases an individual’s desire for thinness and fear of weight gain. This process creates cognitive discrepancies between the individual’s ideal and actual body images, which contribute significantly to adverse eating behaviors.
Although previous studies have shown a positive correlation between body dissatisfaction and restricted diet, they mostly treated body dissatisfaction as a risk factor and restricted diet as the outcome variable, neglecting the bidirectional relationship between them, as previously mentioned. Additionally, research in this area has mainly been limited to Western cultural contexts, and little is known about body dissatisfaction and restricted diet in the Chinese cultural context. Therefore, we believe that understanding the manifestation and temporal changes of both across cultures is crucial.
The Role of Restricted Diet in Body Dissatisfaction
In contrast to the above view, an alternative viewpoint suggests that body dissatisfaction may also be a consequence of restricted diet. The Goal Conflict Model of Eating17 suggests that the behavior of restrained eaters is regulated by conflicting pleasure and dieting goals. If goals such as dieting are repressed while pleasure-seeking goals are prioritized, it can result in failed attempts at restricting food intake or overeating and subsequent weight gain. Body-sensitive adolescents who fail to reach their weight-related goals and experience unexpected weight gain can easily feel dissatisfied. This view is similar to the findings of some empirical studies. For instance, research has shown that endeavors to modify or sustain body shape through measures like dieting and excessive exercising could exacerbate body dissatisfaction and even cause more severe body image issues in young women.18 Furthermore, studies have indicated that dieting is linked with a higher occurrence of psychological problems, such as body dissatisfaction and depression.19
Nevertheless, as we know, research on restricted diet as a risk factor for body dissatisfaction is limited, mostly considered within a comprehensive model, with few studies on the direct pathway. A recent longitudinal study conducted by Withnell and Bodell (2023) expanded the horizon of this research area, reporting a positive association between weight suppression and body dissatisfaction.20 It is worth noting that the study selected undergraduate students as participants, and the sample was relatively diverse and reflective of the broader campus population. However, we believe that selecting adolescent participants would be more appropriate. As mentioned earlier, adolescents are more susceptible to unhealthy weight control behaviors. Additionally, adolescence marks a peak period of physical growth and maturation, during which self-image and body concerns reach unprecedented levels. The profound physiological changes impact psychological development and create a state of imbalance, thus increasing the likelihood of body dissatisfaction.21 In addition, the study conducted three follow-ups within six months, which resulted in some valuable findings. Based on these results, we suggest that extending the follow-up duration and measurement intervals may provide a deeper understanding of the temporal relationship between restricted diet and body dissatisfaction.
Body Dissatisfaction and Restricted Diet in the Chinese Context
Body dissatisfaction and restricted diet have typically been viewed as problems that affect women living in developed Western countries. Because of this, Previous research has been focused mainly on female populations in the West.22 However, evidence points to body dissatisfaction and eating disorders gradually increasing worldwide, particularly in the cultural context of China, where these issues are prevalent among young people.23 Puberty may heighten appearance concerns and diminish well-being as adolescents experience changes to their body weight and shape and mood (Lewis-Smith, Bray, Salmon, and Slater, 2020).24 A study that examined body weight and shape satisfaction among more than 9000 normal-weight Chinese children between the ages of 3 and 15 found that only 46.5% of boys and 43.0% of girls were satisfied with their body shape.25 It is important to note that adolescents exhibit a higher preference for thinness compared to children. A study by Fan et al of 1026 high school students found that 34.49% of boys and 52.83% of girls considered themselves to be overweight, whereas in reality only 21.63% of boys and 9.79% of girls met the criteria for being overweight or obese.26 This perception of body dissatisfaction can be the cause of eating disorders, low self-esteem, and negative affect.27
Although several studies have investigated the antecedent and outcome variables of body dissatisfaction and restricted diet among Chinese adolescents,28,29 it remains to be examined whether a bidirectional relationship exists between these two variables. Considering the prevalent, widespread, and severe nature of these concerns in China, it is crucial to fill this research gap.
Current Study
The present study aims to investigate the potential relationship between body dissatisfaction and restricted diet among Chinese adolescents, in order to provide some guidance for interventions in the area of body image and eating disorders among adolescents, so as to enhance the well-being of Chinese adolescents and promote their physical and mental health development. According to the Tripartite Influence Model, the Goal Conflict Model of Eating, and existing empirical evidence, we hypothesized that body dissatisfaction and restricted diet are reciprocally related. More specifically, prior body dissatisfaction significantly predicts subsequent restricted diet, and vice versa. The proposed conceptual model is shown in Figure 1. In addition, gender differences in body dissatisfaction and restricted diet constitute a focal point of our investigation. Given the pervasive influence of societal values and mainstream media on the subject, previous research has predominantly focused on young girls in the context of body dissatisfaction and restricted diet. However, recent studies have found that adolescent boys also experience body dissatisfaction and possess more complex motives for wanting to be thin, with the occurrence of restricted diet steadily increasing over time.30,31 Therefore, exploring this issue may provide more targeted strategies for interventions to address body dissatisfaction and restricted diet among adolescents. As an exploratory analysis, no specific hypothesis was made.
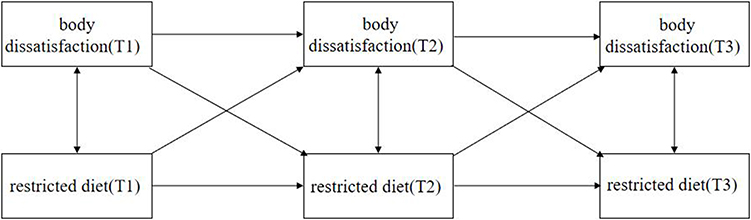 |
Figure 1 Proposed model of the relationships between body dissatisfaction and restricted diet. |
Method
Participants and Procedure
In this study, participants from two middle schools located in Jilin Province, China, were recruited by cluster sampling to conduct a follow-up study at three different time points (five months between each time point). The initial test (T1) was done in September at the start of the autumn term, and a total of 762 adolescents took part in it. The second measurement (T2) was carried out in January, at the close of the autumn term. The third measurement (T3) was performed in June, at the end of the spring Term. Twenty-seven and sixty-three subjects were lost at T2 and T3, respectively, due to dropouts, transfers, illnesses, or incomplete data. This study analyzed sample loss rates, taking into consideration the significance of sample size in longitudinal follow-up studies. The results showed no significant differences between the participants who continued the test and those who dropped out at the T1 period regarding variables such as body dissatisfaction and restricted diet, which suggests that there was no structured attrition of subjects in this study (ts < 1.96, ps > 0.05). Furthermore, this study used G*power 3.1 software (Faul et al, 2007) to estimate the sample size. The software recommended 193 subjects to achieve 80% statistical test power, based on α = 0.05 and the related effect size r = 0.20, which was satisfied by the sample size in this study. Out of the 672 participants who stayed in the study, 314 (46.7%) were male and 358 (53.3%) were female. Among them, 237 were in the seventh grade (35.3%), 265 were in the eighth grade (39.4%), and 170 were in the ninth grade (25.3%). The mean age at baseline was 14.3 years (SD = 1.1, range 12–17).
The Ethics Committee of Northeast Normal University, School of Psychology approved this study (No: 2020036). All procedures involving human participants followed the ethical standards mandated by relevant institutions, the National Research Committee, and the 1964 Helsinki Declaration, along with subsequent amendments or equivalent ethical standards. The survey was advertised as an investigation into body image and healthy eating. Informed consent was gained from all participants and one of their parents before data collection. The investigation was administered by trained graduate research assistants. Participants were asked to fill out paper-and-pencil scales regarding demographic items, Eating Disorders Inventory, and the Dutch Eating Behavior Questionnaire in their classrooms. All questionnaires were tested under unified instruction in groups and were collected immediately. The participants were free to withdraw from the study at any time. After completing the survey, the participants were given a study stationery set as compensation for their participation. The same process was adhered to for both T2 and T3 data collection.
Measures
Body Dissatisfaction
The nine-item body dissatisfaction subscale from the Eating Disorder Inventory-3 (EDI-BD) was used to assess body dissatisfaction.32 Items are rated on a 6-point Likert scale ranging from 1 “Never” to 6 “Always”, with higher total scores implying higher levels of body dissatisfaction. A representative item was “I think that my stomach is too big.” The eight-factor structure and good psychometric properties of the EDI-3 have been confirmed in clinical and non-clinical Chinese populations.33 In the present study, The Cronbach’s α was 0.82, 0.85, and 0.82, respectively.
Restricted Diet
Restricted diet was assessed with the Restrained Eating subscale of the Dutch Eating Behavior Questionnaire.34 This scale has good reliability and validity in the Chinese participant population.35 Participants responded to 10 items, using a 5-point scale ranging from 1 (never) to 5 (very often). An example item was “Do you deliberately eat less in order not to become heavier?” An aggregate score was calculated and higher score meant higher level of restricted diet. In the present study, The Cronbach’s α was 0.85, 0.88, and 0.89, respectively.
Data Analysis
The data analysis was performed using SPSS 24.0. A mixed design analysis of variance was conducted to investigate the stability and gender differences in adolescent body dissatisfaction and restricted diet. Correlation analysis was used to investigate the cross-sectional and longitudinal relationship between body dissatisfaction and restricted diet. A cross-lagged model was constructed using Amos 23.0 to analyze the reciprocal relation between body dissatisfaction and restricted diet.
Results
Preliminary Analyses of Body Dissatisfaction and Restricted Diet
Table 1 displays the results of descriptive statistics for male and female subjects on the main variables. Moreover, A 2×3 mixed-design ANOVA was conducted with gender and measurement time as independent variables and body dissatisfaction as the dependent variable. The results showed that the main effects of gender (F (1, 670) =1.10, P=0.30) and measurement time (F (2, 669) =2.34, P=0.10), as well as their interaction (F (2, 669) =0.47, P=0.63) were not significant. Subsequently, a similar analysis was then conducted with restricted diet as the dependent variable. The results showed a significant main effect of gender (F (1, 670) =18.41, P<0.05, ηp2=0.027), with females (M=23.01, SD=0.37) scoring significantly higher on restricted diet than males (M=20.69, SD=0.40). The main effect of measurement time was also significant (F (2, 669) =8.32, P<0.05), with scores for T1 (M=22.42, SD=8.34) significantly higher than T3 (M=21.31, SD=8.20), and scores for T2 (M=22.05, SD=8.10) significantly higher than T3 (M=21.31, SD=8.20). The interaction between measurement time and gender was not significant (F (2, 669) =1.15, P=0.32).
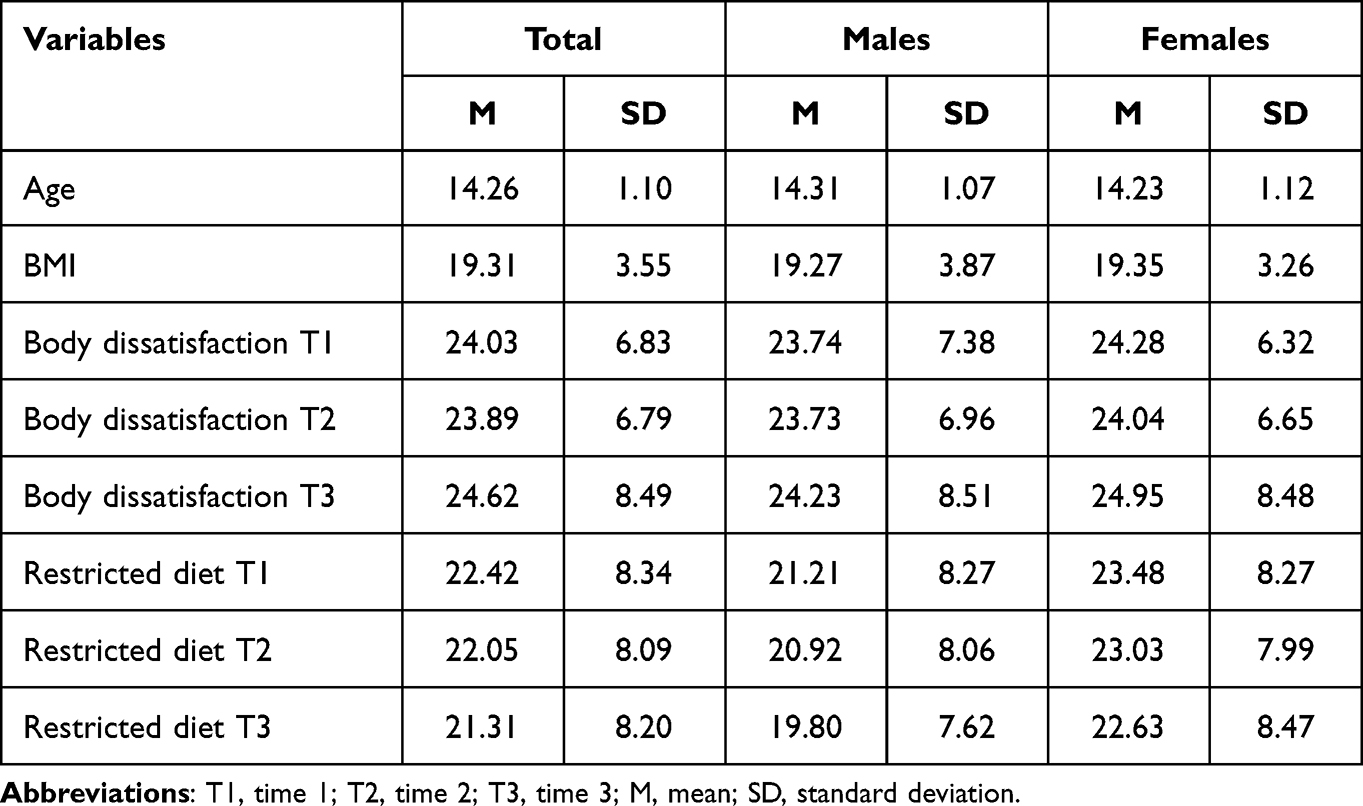 |
Table 1 Descriptive Statistics of Main Study Variables |
Further, Table 2 displays the Pearson correlation coefficients for the three measurements. The significant correlation coefficients for the three instances of body dissatisfaction ranged from 0.28 to 0.43, and for the three instances of restricted diet, the significant coefficients ranged from 0.58 to 0.67. The concurrent correlation between body dissatisfaction and restricted diet was significant, with a coefficient ranging from 0.29 to 0.36. The sequential correlation between body dissatisfaction and restricted diet was also significant, with coefficients ranging from 0.25 to 0.35.
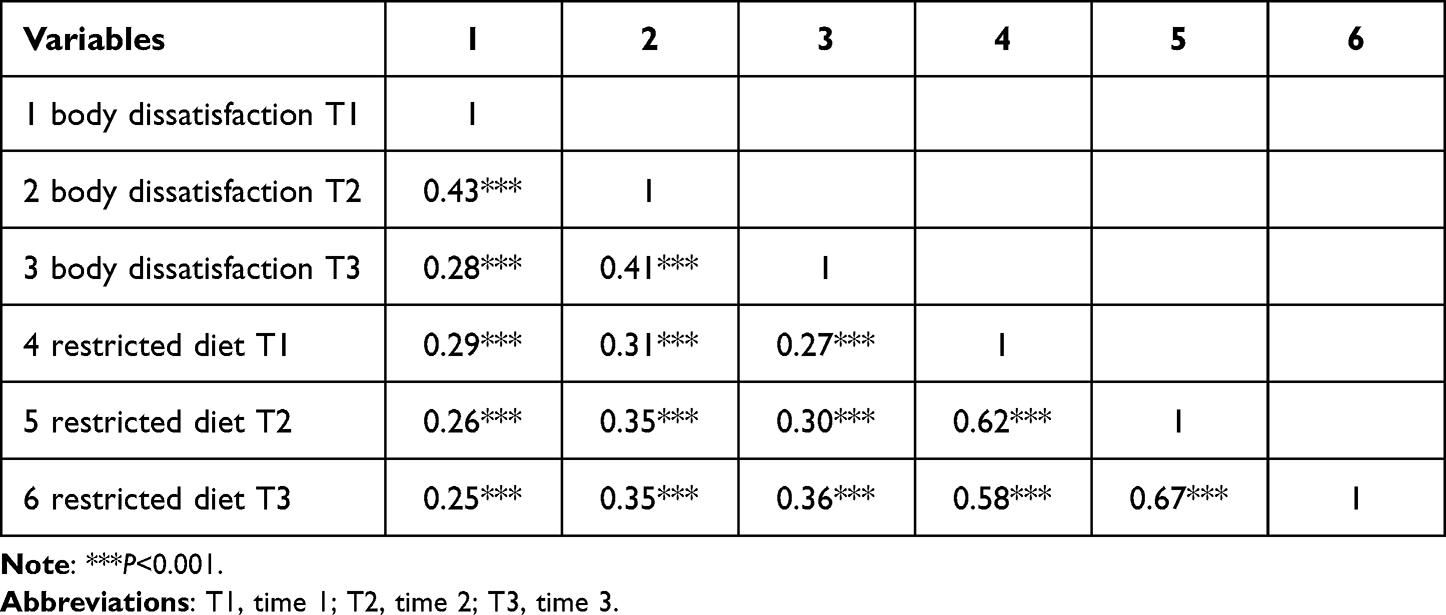 |
Table 2 Correlations Between Body Dissatisfaction and Restricted Diet |
Cross-Lagged Path Analyses of Body Dissatisfaction and Restricted Diet
Based on the correlation analysis, a cross-lagged model was constructed, with body mass index (BMI) as the control variable. As presented in Figure 2. Previous body dissatisfaction significantly predicts subsequent restricted diet, while previous restricted diet significantly predicts subsequent body dissatisfaction.
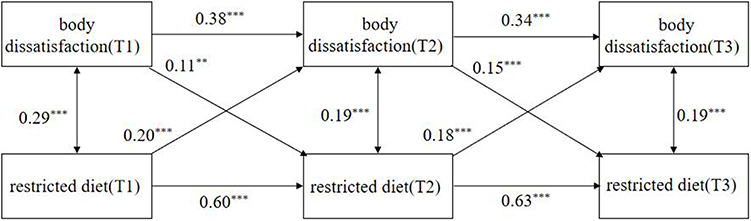 |
Figure 2 Results for the bi-directional effects between body dissatisfaction and restricted diet. Abbreviations: T1, time 1; T2, time 2; T3, time 3. Note: ***P<0.001, **P<0.01. |
To explore gender differences within the cross-lagged model, we conducted a gender-specific multi-group analysis. Initially, we developed a flexible model that allowed the parameters to differ based on gender. Subsequently, we designed a model with equivalent structural weights, where the autoregressive path coefficients and cross-lagged regression path coefficients were the same for both genders. By employing a chi-squared test, we found that the equal path constraint significantly affected the model (Δχ2 (10) = 39.48, P<0.001), indicating that gender differences are prominent in the cross-lagged model when analyzing the correlation between restricted diet and adolescent body dissatisfaction. Moreover, further analyses revealed that there existed significant gender differences in the path coefficients linking restricted diet at Time 1 and body dissatisfaction at Time 2. Specifically, the coefficients for males and females were 0.28 and 0.10, respectively (Ps<0.001). Conversely, other cross-lagged regression paths did not have a significant impact.
Discussion
To our knowledge, the present study is the first to investigate the interrelationship between body dissatisfaction and restricted diet in Chinese adolescents. To this end, we created a cross-lagged model with 672 adolescents measured at 3 time points, each 5 months apart. Consistent with our hypothesis, body dissatisfaction and restricted diet among Chinese adolescents were reciprocally related. This finding supports the idea that body dissatisfaction is a critical risk factor for restricted diet and creatively identifies the possibility that restricted diet may also lead to body dissatisfaction. This idea is similar to the findings of a study on a group of Western subjects. Adolescents from Eastern and Western cultures are becoming increasingly similar due to acculturation, particularly in terms of values and aesthetics. As a result, the differences between these cultures are diminishing, causing adolescents from distinct cultures to become more alike in specific cognitive and behavioral aspects, including body satisfaction or dietary patterns.36 Therefore, in addition to mental health education, body image education should be considered a crucial element in encouraging adolescents to develop accurate views on health and aesthetics and promote a positive lifestyle, thereby improving their physical and mental health and well-being37.
In the present study, adolescents’ previous body dissatisfaction significantly predicted the subsequent restricted diet. The results further compensate for cross-sectional studies38,39 by showing that negative evaluations of the figure are more likely to induce subsequent restricted diet attitudes or behaviors. This pattern of results may be explained by the Tripartite Influence Model. That is, the external pressures of thinness and ideal beauty from a social and cultural environment, along with the mental burden of excessive concern for the body, may result in internal psychological biases (ie, body dissatisfaction), which in turn induce unhealthy weight control behaviors (ie, restricted diet).40 Furthermore, for individuals with a high body dissatisfaction bias, their engagement in restricted diet may also result from stereotypical and overemphasized evaluations of information such as weight and body size. It has been found that individuals’ attitudes toward specific behaviors and perceived sense of behavioral control determine their intention to act.41 Accordingly, at the attitudinal level, adolescents with body dissatisfaction place more emphasis on the importance of body shape and the value of maintaining weight and will hold positive attitudes toward restricted diet; in terms of perceived behavioral control, restricted diet does not require dependence on the cooperation of others, is less difficult to implement, experiences a greater sense of control. As a result, those with negative body image are more likely to regulate their weight by abstaining from eating.
In a similar way, adolescents’ previous restricted diet significantly and positively predicted subsequent body dissatisfaction. The results support and extend previous findings for undergraduate students.42 It is shown that adolescents using restricted diet for a long period of time are more dissatisfied with their bodies than other adolescents. This is consistent with the basic idea of The Goal Conflict Model of Eating, and one possible explanation is that adolescents on restricted diet, when activating a dieting goal for weight control, continuously compare their long-term goal with their perceived current state. When the gap between the two is not decreased, the desire for the “thin ideal” is suppressed, resulting in a sudden decrease in psychological resources. This can trigger strong emotional turmoil and negative psychological states, including irrational perceptions of one’s body size and weight.43 Another possible explanation is that adolescents’ control over eating makes them more sensitive to food cues. They may struggle with food acquisition or suppression, especially when the hedonic goal of eating is activated. If this results in overeating, it can lead to weight gain, disappointment with eating behaviors, and denial of their physical self.44 This process is similar to rumination, which passively and repeatedly focuses adolescents’ attention on negative states that may arise and causes them to constantly indulge in thoughts about weight problems (eg, restricted diet is painful and will only make me fatter, etc.), which in turn induces and exacerbates body image concerns.45
To test whether there were gender differences in the cross-lagged model, we further did a cross-gender multicohort analysis. In general, there were more similarities than differences between adolescent males and females when assessing the relationship between body dissatisfaction and restricted diet. This is similar to existing findings, such as a study examining the correlation between symptoms of depression and eating disorders. The associations exhibited a similar pattern for both male and female adolescents, with gender having minimal effect on the connection.46 However, the only difference is that there is a significant gender difference on the pathway from restricted diet T1 to body dissatisfaction T2, for which we propose the explanation that it may be that boys and girls face different body image pressures during early adolescence. In the case of girls, increased fat takes them away from the slim ideal and they prefer to lose weight. In contrast, changes induced by puberty bring boys closer to the larger, more muscular ideal, as evidenced by the fact that adolescent boys can be divided into those who want to lose weight and those who want to gain weight. These changes may influence the relationship between weight suppression and body dissatisfaction among boys and girls in early adolescence.46 Future research should differentiate in detail between the two motivations in boys and investigate the longitudinal relationship between these different motivations and body dissatisfaction.
In addition, we analyzed the stability and gender differences of body dissatisfaction and restricted diet. The ANOVA results showed that the time main effect of body dissatisfaction was not significant, indicating that body dissatisfaction showed some stability across time. The stability of study variables through adolescence suggests that these attitudes and behaviors are established in early adolescence. This supports the argument that prevention programs should be targeted at preadolescence. The gender main effect of body dissatisfaction was not significant, suggesting a convergence of body dissatisfaction across both genders. This is contrary to the results of some previous studies.47 Possible reasons for this are that adolescents are in adolescence development, which is most characterized by vigorous physiological growth and rapid changes. During this period, adolescents’ body image is particularly vulnerable and can magnify the potential gap between the real body self and the ideal body self, resulting in relatively stable levels of body dissatisfaction throughout puberty.48 For example, in a review of the literature on changes in body image, it was shown that body dissatisfaction did not vary significantly across ages because adolescents’ bodies were generally far from ideal, resulting in low levels of body evaluation.49 Moreover, in sociocultural stereotypes, men have traditionally been perceived as having fewer problems with body image, thus focusing more on women in existing research.50 Indeed, according to The Tripartite Influence Model, given the influence of sociocultural factors, adolescent groups of different ages or genders have the same exposure to information related to the importance of appearance and the unrealistic thin ideal, and consequently, the participation in upward comparisons is also largely similar, thus the interpretation of external information and the evaluation of body satisfaction is likely to converge progressively between individuals,51 This finding is consistent with earlier research indicating equal levels of weight dissatisfaction in boys and girls at ages 13, 15, and 18.52
The ANOVA results showed a significant time main effect of restricted diet, indicating that there is a dynamic change in the level of restricted diet among adolescents over time. Similarly, the study also found a significant gender main effect, with girls having higher levels of restricted diet than boys. This finding is consistent with previous research.53 Our explanation for this is that, on the one hand, it is related to the ideal body size standard. Females promote thinness as beauty, while males often boast muscularity rather than just thinness. This leads to different role expectations and subsequently different behavioral performances.54 At the same time, adolescent girls and boys may be exposed to gender-specific content through media and thus respond to content in different ways.55 For example, males are likely to regulate their weight by adopting a more multifaceted approach involving exercise and fitness, compared to females who maintain body stability through a single, long-term controlled diet. On the other hand, related to the experience of sexual objectification, it has been found that women experience more sexual objectification compared to men. According to The Objectification theory, when individuals adopt a third-party observer perspective to examine or evaluate themselves, they exhibit frequent bodily surveillance and are more likely to internalize the ubiquitous sexual objectification messages in the mind and externalize them through actions. As a result, the risk of a restricted diet is significantly increased.56
Limitations and Implications
Although this study used a longitudinal design, which to some extent compensated for the lack of cross-sectional studies. Some limitations in the present study should be addressed. First, the sample in this study focused only on Chinese adolescents, and the results of the study cannot be generalized to other samples. Future studies should consider other populations, such as middle-aged, elderly, gay, or clinical populations. Second, the sample for this study primarily consisted of middle school students in a province in northeastern China. Due to regional and grade-level differences, there may be differences in body dissatisfaction and restricted diet among adolescents in varying regions and grade levels. Therefore, caution should be taken when extrapolating the results of this study to adolescents across other regions and grade levels. Third, The sample size of this study was small, and some subjects were unable to participate in all three surveys due to objective reasons, resulting in sample loss, thus reducing the stability and representativeness of this study to some extent. Also, the data were based on self-report measures for both body dissatisfaction and restricted diet, which are prone to social desirability effects, and this may affect the results to some extent. Future studies should increase the sample size and use more diverse methods to obtain more robust results. Fourth, this study did not differentiate between types of body dissatisfaction but only measured the overall level of body dissatisfaction of the subjects. Future studies could focus on different dimensions of body dissatisfaction, such as “slim and proportionate for women” and “strong and powerful for men”. At the same time, previous work has suggested that facial appearance may be a culturally specific factor associated with the risk of eating disorders in China compared to weight and body size in Western countries,57 and future research could further examine the inter-predictive relationship between facial dissatisfaction and restricted diet. Finally, this study constructed a three-wave cross-lagged model. However, the duration of follow-up remained short and the number of follow-ups needs to be increased. Although longitudinal studies provide more nuanced information regarding the relationship between body dissatisfaction and restricted diet compared to cross-sectional studies and two-wave measures. Unfortunately, it only stops at exploring the direct association between the two without further exploring the underlying mechanisms, and longitudinal mediators or moderating variables could be invoked in the future to explore the complex mechanisms involved.
Despite its limitations, the present study has several strengths. Given the increasing prevalence of body dissatisfaction and restricted diet among Chinese adolescents,58 there are few studies examining the interrelationship between the two. Thus, this study recruited a sample of Chinese adolescents of both genders and constructed a three-wave cross-lagged model to examine the inter-predictive relationship between body dissatisfaction and restricted diet, thus filling a research gap in the Chinese context. We found that body dissatisfaction and restricted diet among Chinese adolescents were actually “symbiotic relationships” in that they were mutually predictive. The internalization of media ideals and unconscious social comparisons of appearance, influenced by cultural communication in the mass media and the evaluations of others, may reinforce adolescents’ lack of confidence in their appearance or excessive demands for body goals, leading them to adopt restricted diets to regulate their weight. Failure to meet the ideal standards of physical appearance can increase self-denial and worsen body dissatisfaction.
Additionally, the findings of this study have important practical implications for reducing adolescents’ body dissatisfaction and restricted diet, which can help promote the development of a healthy self in adolescents. In terms of the findings of this study, to prevent and intervene in adolescents’ restricted diet, mental health and clinical workers can improve adolescents’ pathological perceptions, emotions, and behaviors about their bodies through professional psychological training such as Intervention on Cognitive-oriented59 and body functionality-based writing intervention.60 At the same time, the government and relevant education departments can host lectures and distribute health education materials to raise awareness about positive body image and proper dietary concepts among young people. Joint school mental health centers can also follow up on children’s health status mechanisms. Furthermore, it is also important to warn young people not to rely on controlled diets to lose weight and mold figure, which may not lead to beauty once and for all, but rather create an intertwined cycle of “restricted diet-body dissatisfaction-restricted diet”.
Conclusion
The present study found that there is a reciprocal longitudinal relationship between body dissatisfaction and restricted diet in Chinese adolescents, and there are some gender differences. These findings not only fill in the research gap regarding body dissatisfaction and restricted diet in the Chinese context but also have important practical implications for reducing body dissatisfaction and restricted diet among adolescents. As a result of the societal disparagement of overweight and the glorification of underweight, many—perhaps most—adolescents express dissatisfaction with their weight and shape. The more intense this dissatisfaction, the more likely that one will undertake attempts to change appearance through various forms of body management behavior (ie, making an effort to lose weight to look thinner). Our findings serve as a reminder that young people should embrace their bodies and not blindly pursue a single aesthetic standard, let alone try to maintain their weight through dieting.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Polivy J, Heatherton TF, Herman CP. Self-esteem, restraint, and eating behavior. J Abnorm Psychol. 1988;97(3):354–356. doi:10.1037/0021-843X.97.3.354
2. Chen G, Guo G, Wu S, et al. Effect of weight-related teasing on dieting in a sample of high school students: mediating effect of body dissatisfaction and moderating effect of gender. Clin Psychol. 2019;27:108–112. doi:10.16128/j.cnki.1005-3611.2019.01.022
3. Elran-Barak R, Sztainer M, Goldschmidt AB, et al. Dietary restriction behaviors and binge eating in anorexia nervosa, bulimia nervosa and binge eating disorder: trans-diagnostic examination of the restraint model. Eat Behav. 2015;18:192–196. doi:10.1016/j.eatbeh.2015.05.012
4. Rawana JS, McPhie ML, Hassibi B. Eating-and weight-related factors associated with depressive symptoms in emerging adulthood. Eat Behav. 2016;22:101–108. doi:10.1016/j.eatbeh.2016.04.002
5. McGrath-Hanna NK, Greene DM, Tavernier RJ, et al. Diet and mental health in the Arctic: is diet an important risk factor for mental health in circumpolar peoples?-a review. Int J Circumpolar Health. 2003;62(3):228–241. doi:10.3402/ijch.v62i3.17560
6. Day S, Bussey K, Trompeter N, et al. The impact of teasing and bullying victimization on disordered eating and body image disturbance among adolescents: a systematic review. Trauma Violence Abuse. 2022;23(3):985–1006. doi:10.1177/1524838020985534
7. Gerbasi ME, Richards LK, Thomas JJ, et al. Globalization and eating disorder risk: peer influence, perceived social norms, and adolescent disordered eating in Fiji. Int J Eat Disord. 2014;47(7):727–737. doi:10.1002/eat.22349
8. Cash TF, Deagle EA. The nature and extent of body‐image disturbances in anorexia nervosa and bulimia nervosa: a meta‐analysis. Int J Eat Disord. 1997;22(2):107–126. doi:10.1002/(SICI)1098-108X(199709)22:2<107::AID-EAT1>3.0.CO;2-J
9. Bucchianeri MM, Fernandes N, Loth K, et al. Body dissatisfaction: do associations with disordered eating and psychological well-being differ across race/ethnicity in adolescent girls and boys? Cult Divers Ethn Minor. 2016;22(1):137–146. doi:10.1037/cdp0000036
10. Lantz EL, Gaspar ME, DiTore R, et al. Conceptualizing body dissatisfaction in eating disorders within a self-discrepancy framework: a review of evidence. Eat Weight Disord. 2018;23(3):275–291. doi:10.1007/s40519-018-0483-4
11. Fairburn CG, Cooper Z, Shafran R. Cognitive behaviour therapy for eating disorders: a “transdiagnostic” theory and treatment. Behav Res Ther. 2003;41(5):509–528. doi:10.1016/S0005-7967(02)00088-8
12. Neumark-Sztainer D, Paxton SJ, Hannan PJ, et al. Does body satisfaction matter? Five-year longitudinal associations between body satisfaction and health behaviors in adolescent females and males. J Adolesc Health. 2006;39(2):244–251. doi:10.1016/j.jadohealth.2005.12.001
13. Thompson JK, Heinberg LJ, Altabe M, et al. Exacting beauty: theory, assessment, and treatment of body image disturbance. Am Psychol Assoc. 1999. doi:10.1037/10312-000
14. Laporta-Herrero I, Jáuregui-Lobera I, Barajas-Iglesias B, et al. Body dissatisfaction in adolescents with eating disorders. Eat Weight Disord. 2018;23(3):339–347. doi:10.1007/s40519-016-0353-x
15. Zhang T, Zhang X. Eating disorders among adolescents: The form and mechanism of peer influence. Adv Psychol Sci. 2019;27(4):657–665. doi:10.3724/SP.J.1042.2019.00657
16. Fox JRE, Froom K. Eating disorders: a basic emotion perspective. Clin Psychol Psychother. 2009;16(4):328–335. doi:10.1002/cpp.622
17. Stroebe W, Mensink W, Aarts H, et al. Why dieters fail: testing the goal conflict model of eating. J Exp Soc Psychol. 2008;44(1):26–36. doi:10.1016/j.jesp.2007.01.005
18. Crow S, Eisenberg ME, Story M, et al. Psychosocial and behavioral correlates of dieting among overweight and non-overweight adolescents. J Adolesc Health. 2006;38(5):569–574. doi:10.1016/j.jadohealth.2005.05.019
19. Liu K, Liang X. The effect of adolescent concerning about weight-loss diet on body image. China Health Psychol. 2012;20(2):246–247. doi:10.13342/j.cnki.cjhp.2012.02.018
20. Withnell SJ, Bodell LP. Does suppressing weight improve body satisfaction? A longitudinal analysis in undergraduate men and women. Body Image. 2023;45:126–132. doi:10.1016/j.bodyim.2023.01.011
21. Burnette CB, Simpson CC, Mazzeo SE. Exploring gender differences in the link between weight suppression and eating pathology. Eat Behav. 2017;27:17–22. doi:10.1016/j.eatbeh.2017.10.001
22. Kennedy MA, Templeton L, Gandhi A, et al. Asian body image satisfaction: ethnic and gender differences across Chinese, Indo-Asian, and European-descent students. Eat Disord. 2004;12(4):321–336. doi:10.1080/10640260490521415
23. Sun S, He J, Fan X, et al. Chinese media coverage of eating disorders: disorder representations and patient profiles. Int J Eat Disord. 2020;53(1):113–122. doi:10.1002/eat.23154
24. Lewis-Smith H, Bray I, Salmon D, et al. Prospective pathways to depressive symptoms and disordered eating in adolescence: a 7-year longitudinal cohort study. J Youth Adolesc. 2020;49(10):2060–2074. doi:10.1007/s10964-020-01291-1
25. Li Y, Hu X, Ma W, et al. Body image perceptions among Chinese children and adolescents. Body Image. 2005;2(2):91–103. doi:10.1016/j.bodyim.2005.04.001
26. Fan ZT, Yu XY, Yu CR, et al. Weight control behaviors and their association with real and perceived weight status among 1026 first year high school students in Lanzhou. Chin J Child Health Care. 2020;28(9):1051–1054. doi:10.11852/zgetbjzz2019-1708
27. Barnhart WR, Cui T, Cui S, et al. Examining appearance pressures, thinness and muscularity internalizations, and social comparisons as correlates of drive for muscularity and thinness-oriented disordered eating in Chinese heterosexual men and women: testing an integrated model. Body Image. 2022;43:429–439. doi:10.1016/j.bodyim.2022.10.005
28. Chen H, Gao X, Jackson T. Predictive models for understanding body dissatisfaction among young males and females in China. Behav Res Ther. 2007;45(6):1345–1356. doi:10.1016/j.brat.2006.09.015
29. Ma J, Wang K, Thompson JK. Translation and psychometric properties of the Chinese version of the Sociocultural Attitudes Towards Appearance Questionnaire-4 (SATAQ-4) in college students. Body Image. 2023;45:172–182. doi:10.1016/j.bodyim.2023.02.011
30. Mitchison D, Hay P, Slewa-Younan S, et al. The changing demographic profile of eating disorder behaviors in the community. BMC Public Health. 2014;14(1):1–9. doi:10.1186/1471-2458-14-943
31. Van Dyne A, Washington N, Villodas M, et al. Racial and ethnic disparities in weight loss behaviors among US college students. Psychol Res Behav Manag. 2023;Volume 16:857–873. doi:10.2147/PRBM.S395357
32. Garner DM, Olmstead MP, Polivy J. Development and validation of a multidimensional eating disorder inventory for anorexia nervosa and bulimia. Int J Eat Disord. 1983;2(2):15–34. doi:10.1002/1098-108X(198321)2:2<15::AID-EAT2260020203>3.0.CO;2-6
33. Fan Y, Li Y, Liu A, et al. Associations between body mass index, weight control concerns and behaviors, and eating disorder symptoms among non-clinical Chinese adolescents. BMC Public Health. 2010;10(1):1–12. doi:10.1186/1471-2458-10-314
34. Van Strien T, Frijters ER, Bergers PA, et al. The Dutch Eating Behavior Questionnaire (DEBQ) for assessment of restrained, emotional, and external eating behavior. Int J Eat Disord. 1986;5(2):295–315. doi:10.1002/1098-108X(198602)5:2<295::AID-EAT2260050209>3.0.CO;2-T
35. Liu X, Yang K, Liu Y, et al. Cross-lagged analysis of body shame, abnormal eating behavior and eating disorder tendency among adolescents. Chin J Sch Health. 2023;44(1):76–80. doi:10.16835/j.cnki.1000-9817.2023.01.017
36. Warren CS, Akoury LM. Emphasizing the “cultural” in sociocultural: a systematic review of research on thin-ideal internalization, acculturation, and eating pathology in us ethnic minorities. Psychol Res Behav Manag. 2020;Volume 13:319–330. doi:10.2147/PRBM.S204274
37. Liu K, Zhang J, Liu S, et al. Parental stress on children’s appearance, body dissatisfaction, and eating behaviours in Chinese children: a pathway analysis. Psychol Res Behav Manag. 2023;Volume 16:363–372. doi:10.2147/PRBM.S395628
38. Chisuwa N, O’Dea JA. Body image and eating disorders amongst Japanese adolescents. A review of the literature. Appetite. 2010;54(1):5–15. doi:10.1016/j.appet.2009.11.008
39. Woelders CS, Larsen JK, Scholte HJ, et al. Friendship group influences on body dissatisfaction and dieting among adolescent girls: a prospective study. J Adolesc Health. 2010;47(5):456–462. doi:10.1016/j.jadohealth.2010.03.006
40. Rodgers RF, Paxton SJ, McLean SA. A biopsychosocial model of body image concerns and disordered eating in early adolescent girls. J Youth Adolesc. 2014;43:814–823. doi:10.1007/s10964-013-0013-7
41. Ajzen I. The theory of planned behavior. Organ Behav Hum Decis. 1991;50(2):179–211. doi:10.1016/0749-5978(91)90020-T
42. Azzouzi N, Ahid S, Bragazzi NL, et al. Eating disorders among Moroccan medical students: cognition and behavior. Psychol Res Behav Manag. 2019:129–135. doi:10.2147/PRBM.S165114
43. Presnell K, Bearman SK, Stice E. Risk factors for body dissatisfaction in adolescent boys and girls: a prospective study. Int J Eat Disord. 2004;36(4):389–401. doi:10.1002/eat.20045
44. Hollitt S, Kemps E, Tiggemann M, et al. Components of attentional bias for food cues among restrained eaters. Appetite. 2010;54(2):309–313. doi:10.1016/j.appet.2009.12.005
45. Etu SF, Gray JJ. A preliminary investigation of the relationship between induced rumination and state body image dissatisfaction and anxiety. Body Image. 2010;7(1):82–85. doi:10.1016/j.bodyim.2009.09.004
46. Kenny B, Fuller-Tyszkiewicz M, Moodie M, et al. Bi-directional associations between depressive symptoms and eating disorder symptoms in early adolescence. Body Image. 2022;42:246–256. doi:10.1016/j.bodyim.2022.06.012
47. Kostanski M, Fisher A, Gullone E. Current conceptualisation of body image dissatisfaction: have we got it wrong? J Child Psychol Psychiatry. 2004;45(7):1317–1325. doi:10.1111/j.1469-7610.2004.00315.x
48. Zhang Y, Li T, Yao R, et al. Comparison of body-image dissatisfaction among Chinese children and adolescents at different pubertal development stages. Psychol Res Behav Manag. 2020:555–562. doi:10.2147/PRBM.S242645
49. Tiggemann M. Body image across the adult life span: stability and change. Body Image. 2004;1(1):29–41. doi:10.1016/S1740-1445(03)00002-0
50. De Vries DA, Peter J, De Graaf H, et al. Adolescents’ social network site use, peer appearance-related feedback, and body dissatisfaction: testing a mediation model. J Youth Adolesc. 2016;45:211–224. doi:10.1007/s10964-015-0266-4
51. Dumas AA, Desroches S. Women’s use of social media: what is the evidence about their impact on weight management and body image? Curr Obes Rep. 2019;8:18–32. doi:10.1007/s13679-019-0324-4
52. Rosenblum GD, Lewis M. The relations among body image, physical attractiveness, and body mass in adolescence. Child Dev. 1999;70(1):50–64. doi:10.1111/1467-8624.00005
53. Mitchison D, Mond J. Epidemiology of eating disorders, eating disordered behaviour, and body image disturbance in males: a narrative review. J Eat Disord. 2015;3(1):1–9. doi:10.1186/s40337-015-0058-y
54. Zhao Z, Huang XS, Wang W, et al. Review on research of gender differences and influencing factors in eating disorder. China J Health Psychol. 2017;25:792–797. doi:10.13342/j.cnki.cjhp.2017.05.040
55. Rodgers RF, Slater A, Gordon CS, et al. A biopsychosocial model of social media use and body image concerns, disordered eating, and muscle-building behaviors among adolescent girls and boys. J Youth Adolesc. 2020;49:399–409. doi:10.1007/s10964-019-01190-0
56. Fredrickson BL, Roberts TA. Objectification theory: toward understanding women’s lived experiences and mental health risks. Psychol Women Q. 1997;21(2):173–206. doi:10.1111/j.1471-6402.1997.tb00108.x
57. Jackson T, Chen H. Identifying the eating disorder symptomatic in China: the role of sociocultural factors and culturally defined appearance concerns. J Psychosom Res. 2007;62(2):241–249. doi:10.1016/j.jpsychores.2006.09.010
58. Xiong S, Xu Y, Zhang B, et al. Patterns of restrained eating in Chinese adolescents’ interpersonal contexts: a latent profile analysis. Curr Psychol. 2022:1–11. doi:10.1007/s12144-022-02748-1
59. Pan C, Chen H, Jiang X, et al. Intervention on cognition-orientated body dissatisfaction in adolescent girls. Psychol Dev Educ. 2010;26(2):169–175. doi:10.16187/j.cnki.issn1001-4918.2010.02.009
60. Zeng Y, Li Y, Wang Y. The effect and mechanism of functionality-based writing intervention on improving body image in Chinese female college students. Chin J Clin Psychol. 2021;29(2):414–418. doi:10.16128/j.cnki.1005-3611.2021.02.040
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.