Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Blood Eosinophil Stability Predicts Clinical Outcomes in Hospitalized Patients with Acute Exacerbations of COPD
Authors Guan L ![]() , Li J
, Li J ![]() , Liang L
, Liang L ![]() , Tong Z
, Tong Z ![]()
Received 19 May 2025
Accepted for publication 12 August 2025
Published 22 August 2025 Volume 2025:20 Pages 2913—2923
DOI https://doi.org/10.2147/COPD.S536911
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Fanny Wai San Ko
Lujia Guan,1,* Jiachen Li,2,* Lirong Liang,2 Zhaohui Tong1
1Department of Respiratory and Critical Care Medicine, Beijing Research Center for Respiratory Infectious Diseases, Beijing Institute of Respiratory Medicine and Beijing Chao Yang Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Evidence-Based Medicine Center, Beijing Institute of Respiratory Medicine and Beijing Chao-Yang Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lirong Liang, Evidence-Based Medicine Center, Beijing Institute of Respiratory Medicine and Beijing Chao-Yang Hospital, Capital Medical University, 8 Gongren Tiyuchang Nanlua, Chaoyang District, Beijing, People’s Republic of China, 100020, Email [email protected] Zhaohui Tong, Department of Clinical Epidemiology, Beijing Research Center for Respiratory Infectious Diseases, Beijing Institute of Respiratory Medicine and Beijing Chao Yang Hospital, Capital Medical University, 8 Gongren Tiyuchang Nanlua, Chaoyang District, Beijing, 100020, People’s Republic of China, Email [email protected]
Background and Objective: Blood eosinophil (EOS) levels are considered a potential biomarker for acute exacerbation of chronic obstructive pulmonary disease (AECOPD) management, but the impact of EOS stability during hospitalization on outcomes is unclear. This study examined the relationship between EOS stability and clinical outcomes in these patients.
Methods: A retrospective analysis was conducted on 2105 AECOPD patients hospitalized at Beijing Chao-Yang Hospital from 2013 to 2022. Patients were classified into four groups according to EOS counts (2%) at admission and discharge: persistent high, decreased, increased, and persistent low. Clinical characteristics and outcomes were compared between EOS stability groups. Multivariable logistic regression was used to evaluate the association between EOS stability and adverse hospital outcomes. Cox regression analysis was performed to assess the risk of AECOPD-related readmission within three years. Receiver operating characteristic (ROC) curves and nomograms were used to evaluate the predictive performance of the models.
Results: There were 586 (27.8%), 154 (7.3%), 593 (28.2%), and 772 (36.7%) patients in the persistent high, decreased, increased, and persistent low groups, respectively. Multivariable logistic regression analysis showed that the persistent high EOS group had a significantly lower risk of adverse hospital outcomes compared to the persistent low EOS group (aOR: 0.77, 95% CI: 0.59– 0.99, P = 0.040). The nomogram developed based on the multivariate model demonstrated good predictive accuracy for adverse hospital outcomes, with an AUC of 0.67, and was well-calibrated. Cox regression analysis revealed that the persistent high EOS group had a higher risk of AECOPD-related readmission within three years compared to the persistent low EOS group (aHR: 1.38, 95% CI: 1.13– 1.68, P = 0.001).
Conclusion: Blood eosinophil stability during hospitalization is associated with AECOPD prognosis and may help guide inpatient treatment and identify patients at higher risk of future readmission.
Keywords: acute exacerbation of chronic obstructive pulmonary disease, eosinophil, adverse hospital outcome
Introduction
Chronic obstructive pulmonary disease (COPD) is a highly heterogeneous lung condition characterized by persistent respiratory symptoms and airflow limitation due to airway and alveolar abnormalities.1 COPD is the third leading cause of death worldwide, responsible for approximately 3 million deaths annually,2 with nearly 90% of these occurring in low- and middle-income countries.3 Acute exacerbation of COPD (AECOPD) worsens respiratory symptoms, accelerates disease progression, and increases comorbidity and mortality.4 Studies have shown that 22–40% of COPD patients experience at least one acute exacerbation, with 9–16% experiencing multiple exacerbations.5 AECOPD also represents the largest component of the socioeconomic burden associated with COPD.
Blood eosinophils (EOS) are considered a potential clinical biomarker for identifying specific AECOPD phenotypes,6 guiding glucocorticoid therapy,7 and predicting exacerbation risk.8 However, existing research on the ability of EOS to predict the prognosis of AECOPD exacerbations remains controversial.9–11 Previous studies typically used a single EOS measurement at admission to predict clinical outcomes, which may not fully capture the dynamic changes in EOS during exacerbations.12 Multiple studies have shown that persistent high EOS levels during stable periods are associated with reduced mortality.13,14 However, EOS levels can fluctuate during exacerbations due to disease progression and medical interventions. This suggests that short-term EOS stability may be a more accurate predictor of outcomes than a single measurement.15 Our previous work found that elevated EOS at admission was associated with shorter hospital stays in AECOPD patients.7 Still, the relationship between EOS changes during hospitalization and clinical outcomes remains unclear. Only one small sample size cohort study involving 530 patients has suggested a potential link between EOS changes and AECOPD outcomes, but more evidence is needed to confirm these findings.16
In this large-sample study, we examined changes in EOS levels during AECOPD and their impact on clinical outcomes, such as mortality, ICU admission, and AECOPD readmission within three years after discharge. These findings could improve risk stratification and AECOPD management in clinical practice.
Materials and Methods
Study Design and Patients
This retrospective study included patients admitted to our Hospital for AECOPD from March 2013 to March 2022. Inclusion criteria were as follows: (1) age ≥40 years; (2) primary discharge diagnosis of acute exacerbation of COPD [International Classification of Diseases (ICD)-10 code J44]; (3) a hospital stay of at least 24 hours; (4) two EOS measurements obtained during hospitalization—one within 24 hours of admission and the other at the time of discharge. Exclusion criteria were as follows: (1) comorbid asthma, allergic diseases, autoimmune diseases, hematologic diseases, or malignancies; (2) hospital stay ≥40 days; (3) for patients with multiple hospitalizations during the study period, only the first hospitalization was included. This study is a retrospective cohort study, and the protocol was approved by the Ethics Committee of Hospital.
Data Collection
Data were retrieved from a validated electronic medical record (EMR) platform established by the Beijing Institute of Respiratory Medicine and Beijing Chao-Yang Hospital.17 This respiratory-focused big data platform integrates structured records from over 4 million cases since 2013, with rigorous quality control and linkage to citywide hospital discharge databases.18,19 Patients in this study were admitted to the Department of Respiratory and Critical Care Medicine, the Emergency Department, or the General Medicine Department. Information included demographic characteristics, smoking status, exacerbation in the previous year, comorbidity, laboratory tests, treatment and clinical outcomes. Clinical outcomes assessed during the hospitalization included in-hospital death, use of invasive mechanical ventilation (IMV), transfer to the intensive care unit (ICU), length of stay (LOS), and total hospitalization costs. AECOPD-related readmissions were tracked for up to three years following discharge. Adverse hospital outcomes were defined as transfer to ICU, use of IMV, in-hospital mortality, and LOS >14 days.
EOS stability during hospitalization was classified into four groups based on the initial and final EOS counts: (1) persistent high group: both initial and final EOS counts ≥ 2%; (2) persistent low group: both initial and final EOS counts < 2%; (3) decreased group: initial EOS count ≥ 2% but final EOS count < 2%; (4) increased group: initial EOS count <2% but final EOS count ≥ 2%. This classification method follows previous studies that evaluated eosinophil stability across multiple time points.12,20
Statistical Analysis
Categorical variables were expressed as counts and percentages, compared using chi-square or Fisher’s exact tests. Continuous variables with non-normal distributions were reported as medians and interquartile ranges (IQR) and analyzed using the Kruskal–Wallis test. Patients with missing data were excluded. Univariate regression identified variables for multivariable logistic regression, which analyzed the association between EOS stability and adverse hospital outcomes, using the persistent low EOS group as a reference to calculate odds ratios (OR) and 95% confidence intervals (CI). Receiver operating characteristic (ROC) curves and area under the curve (AUC) values assessed predictive model performance, compared using the DeLong test. Nomograms were developed based on the models. Multivariate Cox regression predicted AECOPD readmission risk within three years, with subgroup analyses by age, gender, smoking, Charlson comorbidity index, and prior-year exacerbations. Statistical analyses were performed using R 4.3.1, with significance set at p < 0.05.
Results
Study Population
As shown in Figure 1, 7039 patients aged ≥40 years with a primary discharge diagnosis of AECOPD were identified. After exclusions, 2105 patients were included in the final analysis. The number of patients enrolled each year is shown in Table S1.
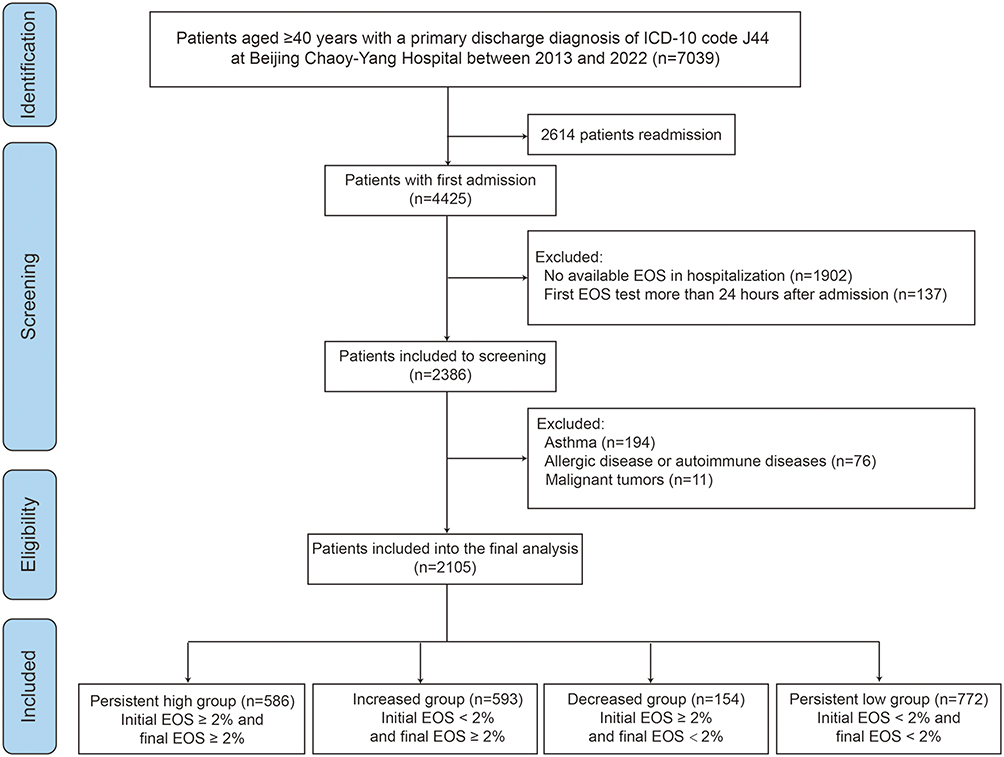 |
Figure 1 Study flow. |
Clinical Characteristics of AECOPD Patients with Different EOS Stability Groups
The numbers of patients in the persistent high, decreased, increased, and persistent low EOS groups were 586 (27.8%), 154 (7.3%), 593 (28.2%), and 772 (36.7%), respectively. Overall, 35.1% had an initial EOS count ≥2%, while 64.9% had a initial EOS count <2%. Stable EOS levels (persistent high/low) were observed in 64.5% of patients, while 35.5% showed unstable levels. The decreased group’s median EOS dropped from 3.05 (2.30–4.10) % to 0.80 (0.10–1.40) %, while the increased group rose from 0.50 (0.00–1.20) % to 3.00 (2.40–4.10) %, was shown in Table 1.
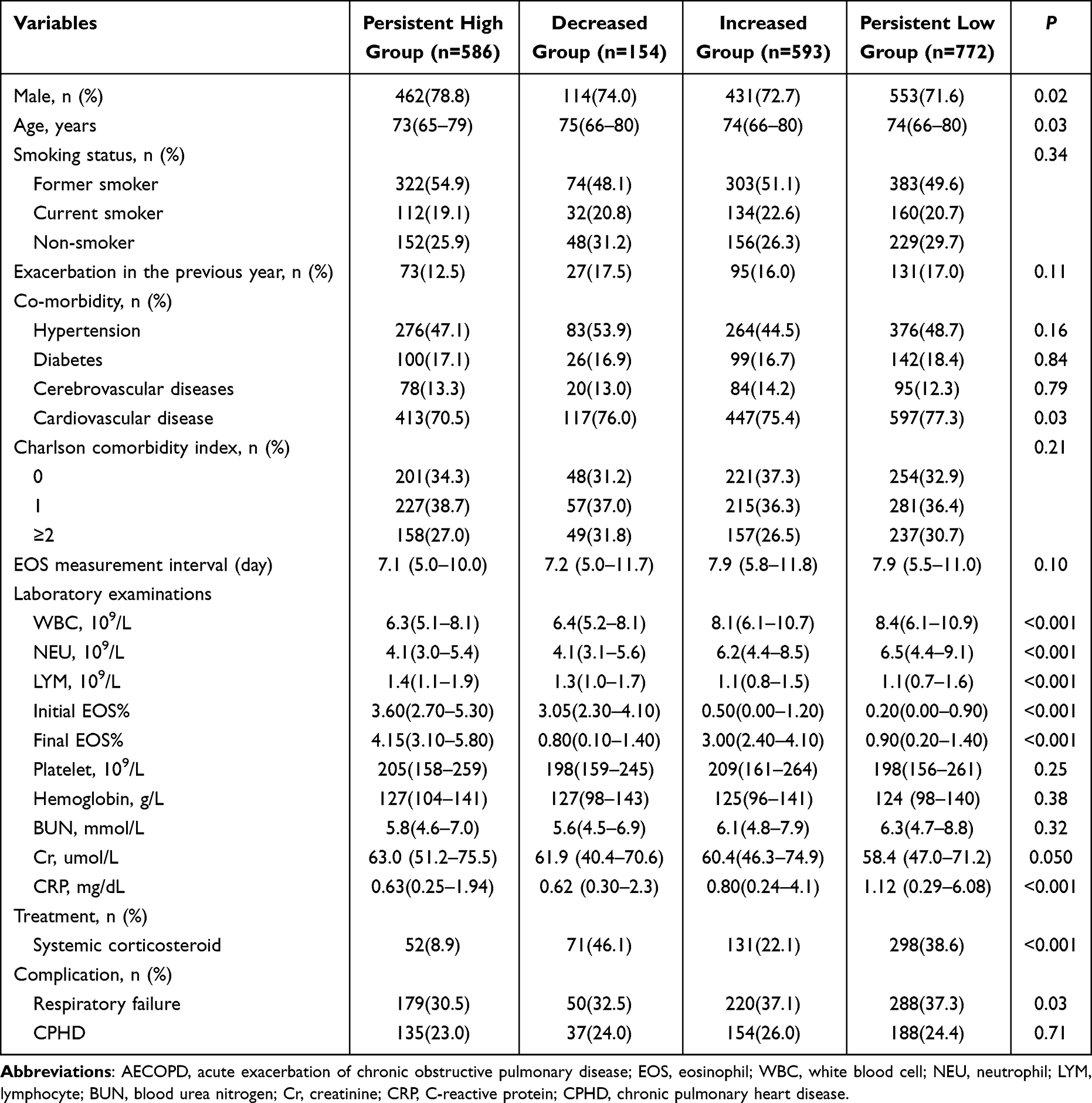 |
Table 1 Baseline Characteristics of Patients with AECOPD Stratified by EOS Stability |
The persistent high EOS group had a higher proportion of males (78.8%) and a lower median age (P<0.05). Cardiovascular disease prevalence was lowest in this group (70.5%, P=0.03), with no differences in smoking status or prior exacerbations. White blood cell, neutrophil counts, and CRP were significantly lower in the persistent high group compared to increased and persistent low groups, while lymphocyte counts were higher (P<0.001). Respiratory failure was less frequent in the persistent high group (P=0.03), and systemic corticosteroid use was lower. Systemic corticosteroid use varied significantly among groups, with the highest proportion observed in the decreased group (46.1%) and the lowest in the persistent high group (8.9%) (P < 0.001).
Clinical Outcomes and Prognostic of AECOPD Patients with Different EOS Stability Groups
The persistent high EOS group consistently had the lowest rates in these categories, including a 2.9% ICU transfer rate, 1.7% IMV use, 27.8% LOS > 14 days, and 0.2% in-hospital mortality. Total hospital costs were highest in the persistent low EOS group compared to the persistent high EOS group (P< 0.001). Adverse hospital outcomes were most frequent in the decreased EOS group (41.6%), followed by the persistent low EOS group (40.5%) (P<0.001). No significant differences were found in post-discharge AECOPD readmission within three years among the groups (P = 0.21), although the persistent low EOS group had a lower readmission rate (34.5%) compared to the other groups, as shown in Table 2.
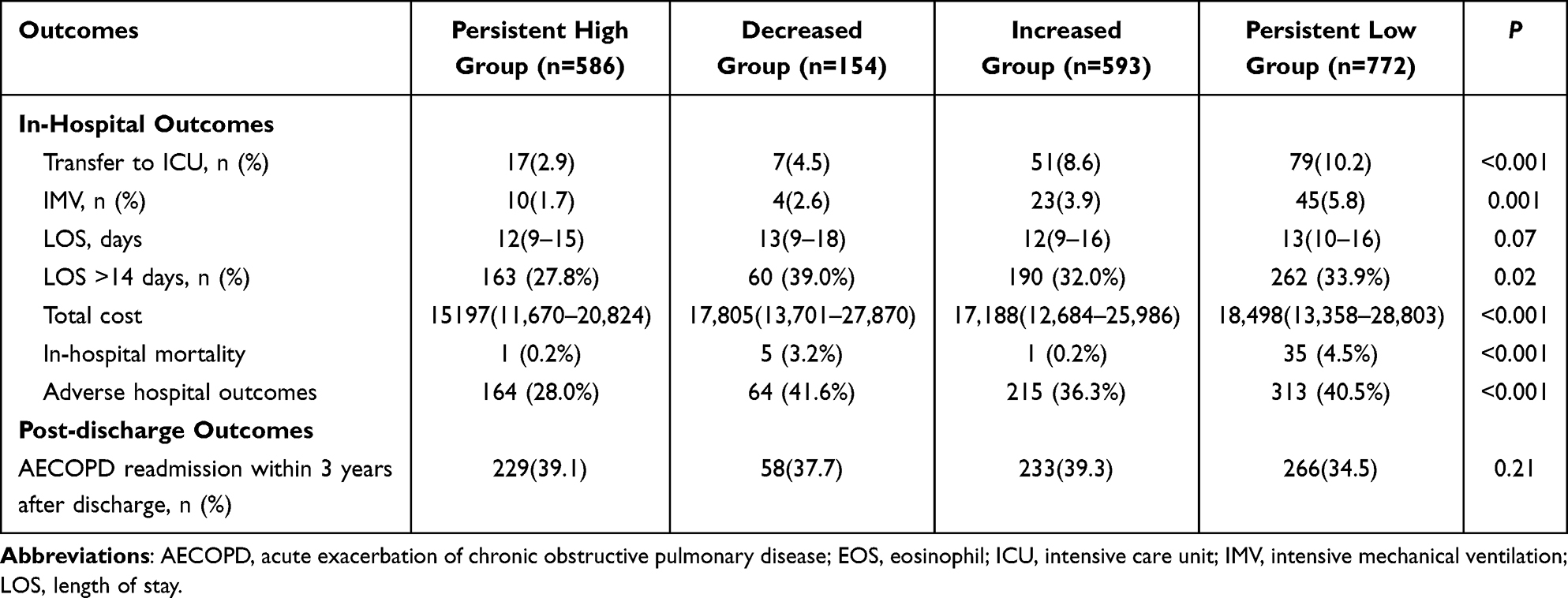 |
Table 2 Comparison of Clinical Outcomes Among AECOPD Patients with Different EOS Stability |
Predictive Factors for Adverse Hospital Outcomes in AECOPD Patients
Multivariate logistic regression analysis (Table 3) shows that the persistent high EOS group had lower odds of adverse hospital outcomes, compared to the persistent low EOS group (adjusted OR: 0.77, 95% CI: 0.59–0.99, P = 0.040). No significant differences were found for the decreased or increased EOS groups. Age (adjusted OR: 1.01, 95% CI: 1.00–1.02, P = 0.05) and hemoglobin (adjusted OR: 1.01, 95% CI: 1.00–1.02, P = 0.082) slightly increased the risk. Current smokers had lower odds than non-smokers (adjusted OR: 0.65, 95% CI: 0.48–0.88, P = 0.006). Risk factors included a history of exacerbations (adjusted OR: 1.78, 95% CI: 1.39–2.30, P = 0.006), Charlson index ≥2 (adjusted OR: 2.04, 95% CI: 1.61–2.30, P < 0.001), respiratory failure (adjusted OR: 1.76, 95% CI: 1.44–2.15, P < 0.001), and corticosteroid use (adjusted OR: 1.34, 95% CI: 1.10–1.70, P = 0.005). Higher lymphocyte counts were protective (adjusted OR: 0.84, 95% CI: 0.73–0.97, P = 0.022).
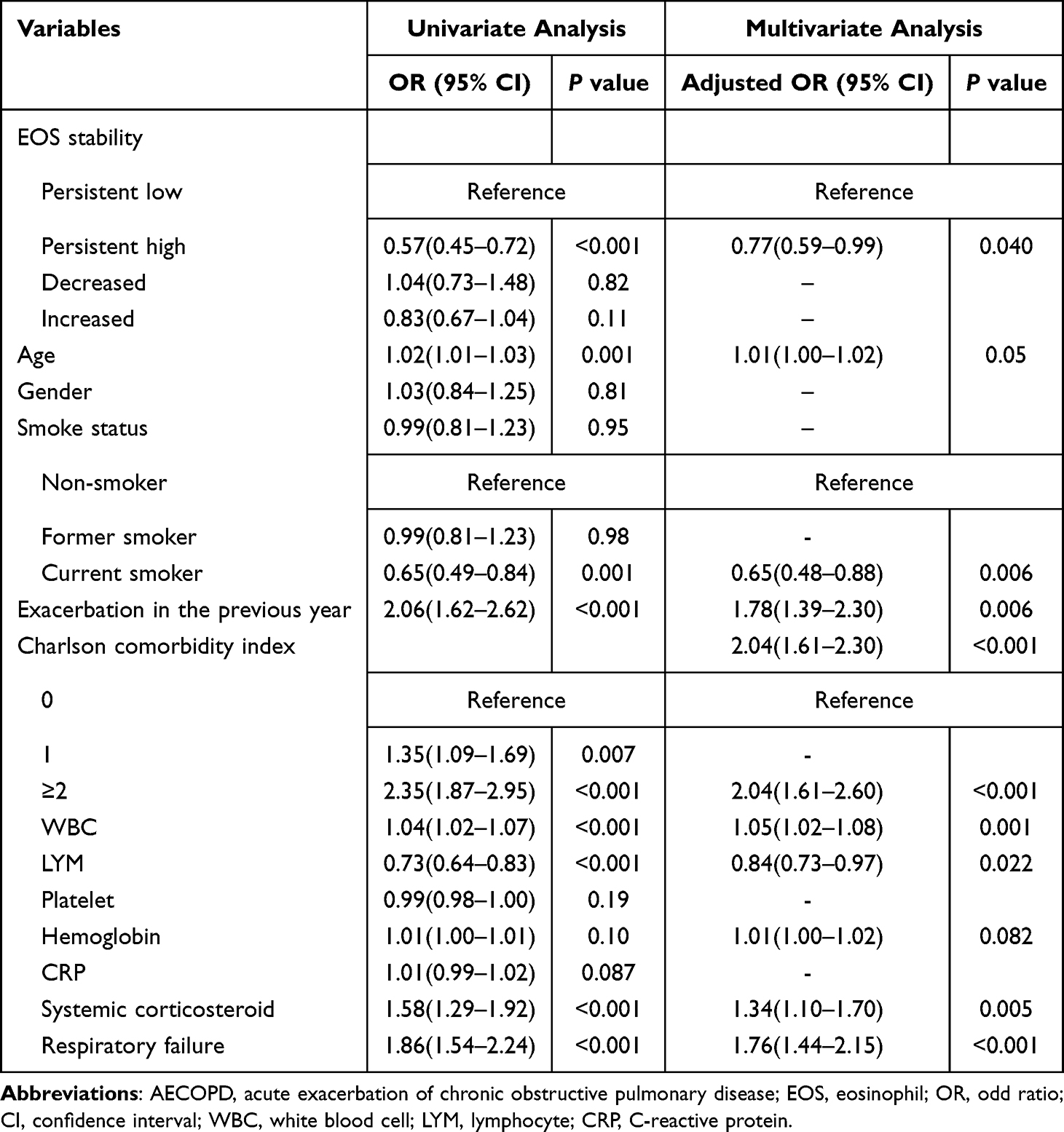 |
Table 3 The Predicting Factors for Adverse Hospital Outcomes Among Patients with AECOPD |
Predictive Models for Adverse Hospital Outcomes: AUC and ROC Analysis
Table S2 illustrates the predictive performance of models using EOS stability for adverse hospital outcomes in AECOPD patients. Model 1, including EOS stability, age, and smoking status, had an AUC of 0.59 (95% CI: 0.57–0.62). Adding exacerbation history and Charlson index in Model 2 increased the AUC to 0.64 (95% CI: 0.62–0.67). Model 3, which included corticosteroid use and respiratory failure, improved the AUC to 0.66 (95% CI: 0.64–0.69). Model 4, incorporating WBC, lymphocyte count, and hemoglobin, achieved the highest AUC of 0.67 (95% CI: 0.65–0.70). The ROC curve for Model 4 showed moderate discrimination, with the DeLong test confirming stepwise improvement. A nomogram derived from ten predictors (Figure S1) performed well, with Hosmer‒Lemeshow test P = 0.938.
The Risk of AECOPD Readmission in Different EOS Stability Groups
Table S3 and Figure 2 show that after adjusting for baseline characteristics (age, smoking status, exacerbations in the previous year, Charlson comorbidity index), systemic corticosteroid, respiratory failure, and laboratory tests, both the persistent high (adjusted HR: 1.38, 95% CI: 1.13–1.68) and increased EOS groups (adjusted HR: 1.25, 95% CI: 1.05–1.50) were associated with a higher risk of AECOPD rehospitalization, while no significant difference was observed in the decreased EOS group (adjusted HR: 1.08, 95% CI: 0.81–1.45).
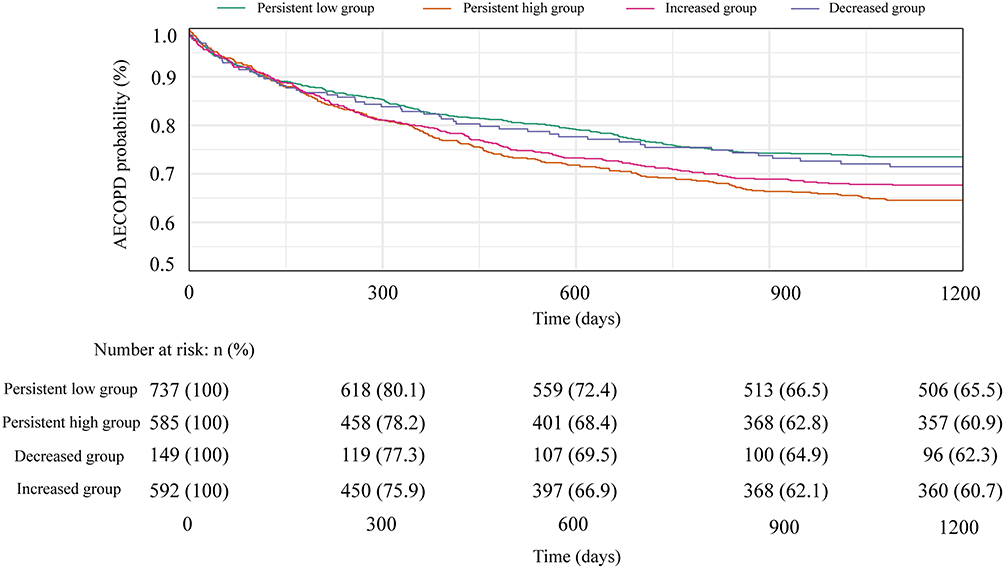 |
Figure 2 Cox proportional hazards analysis curve for AECOPD readmission by eosinophil stability groups. |
Subgroup Analysis
Table S4 shows the subgroup analysis of persistent high EOS and AECOPD readmission risk within three years. Patients aged ≥65 (HR: 1.46, 95% CI: 1.17–1.81, P = 0.001), males (HR: 1.47, 95% CI: 1.17–1.85, P <0.001), former smokers (HR: 1.54, 95% CI: 1.17–2.02, P = 0.001), those with a Charlson index <2 (HR: 1.31, 95% CI: 1.03–1.65, P = 0.03), or a history of exacerbations (HR: 1.29, 95% CI: 1.04–1.63, P = 0.02) had higher readmission risks. Persistent high EOS was associated with increased readmission risk, regardless of corticosteroid use. No significant interaction effects were observed.
Discussion
This large-sample retrospective cohort study based on EMR details the changes in EOS levels and their association with clinical outcomes in hospitalized patients with AECOPD. The results showed that more than 30% of patients did not maintain stable EOS levels during hospitalization, exhibiting either increasing or decreasing trends. Patients with persistent high EOS exhibited better hospital outcomes, including lower ICU transfer rates, reduced mortality, fewer instances of IMV, and lower total costs. However, our observations revealed that the risk of readmission due to AECOPD within three years after discharge was significantly higher in the persistent high and increased EOS groups, while there were no significant differences in the decreased EOS group compared to the persistent low EOS group.
Given the significant heterogeneity in COPD, with various phenotypes and pathophysiological mechanisms,21 precise clinical phenotyping can help clinicians assess risk and implement personalized treatment plans. Bafadhel et al classified acute exacerbation events into four phenotypes based on etiology and inflammatory markers: bacterial, viral, eosinophilic, and paucigranulocytic.22 Increased EOS levels identify the eosinophilic phenotype and are a key, treatable trait in COPD.23 The Global Initiative for Chronic Obstructive Lung Disease (GOLD) recommends using EOS levels as a biomarker to guide corticosteroid therapy in acute exacerbations.24 In our study, we selected an EOS threshold of ≥2%, and the results showed that 35.1% of AECOPD patients had an initial EOS exceeding 2% upon admission, which is consistent with prior research.25,26
However, the high EOS phenotype may not be stable and can fluctuate due to various factors. Accurate assessment of EOS stability is crucial for clinical evaluation and personalized corticosteroid treatment. In stable COPD patients, EOS levels can be influenced by factors like allergies, obesity, medications, and smoking, leading to fluctuations.27 The PROMISE-COPD and ECLIPSE studies indicated significant variability in EOS throughout the stable COPD course.12,28 Previous studies have explored the long-term stability of EOS in COPD patients and its association with outcomes.14,29 Our prior research also suggested that patients with consistently high EOS levels at admission had reduced all-cause mortality after discharge.30 However, during a single acute exacerbation, EOS levels can fluctuate with disease progression and treatment effects. Current research on EOS stability in AECOPD is limited. A similar study16 selected a threshold of 300 cells/μL for eosinophil level, which is relatively high in Chinese populations.31 As a result, the eosinophil distribution in their cohort was more concentrated in the lower range, with 71.9% of patients in the persistent low EOS group and only 10.9% in the persistent high EOS group. In contrast, our study adopted a 2% blood eosinophil percentage as the cutoff to differentiate eosinophilic and non-eosinophilic groups, based on previous research demonstrating its sensitivity in detecting eosinophilic airway inflammation and its relevance to eosinophil-driven exacerbations.22,32 This relative threshold allowed us to capture fluctuations in eosinophil levels and resulted in a more balanced distribution across the EOS trajectory groups.7
Previous studies have shown that patients with high EOS levels at admission tend to have better clinical outcomes,32,33 a trend that was even more pronounced in the persistent high EOS group in our study. We also found that these patients had lower rates of adverse hospital outcomes and reduced hospitalization costs. Consistent with previous studies, which demonstrated that AECOPD patients with lung infections tend to have elevated peripheral neutrophil counts and reduced EOS and lymphocyte levels,34,35 our study observed that patients with EOS counts below 2% exhibited higher WBC, lower lymphocyte counts, and elevated CRP levels, indicating increased susceptibility to infection. Additionally, these patients had a higher incidence of respiratory failure and more frequent use of systemic corticosteroids, reflecting greater disease severity, as noted in other studies.33,36 Interestingly, patients in the decreasing group—those with elevated EOS at admission but decreased at discharge—appeared to diverge from the typical eosinophilic phenotype and demonstrated worse in-hospital outcomes. This suggests that a subgroup of patients with initially high EOS but poor response to treatment may exist, and this warrants further investigation. Further multivariate logistic regression analysis of adverse hospital outcomes revealed that, compared to the persistent low group, only the persistent high EOS group emerged as a protective factor. This finding could explain why many earlier studies, which focused solely on a single EOS level at admission without accounting for EOS variability,9 failed to show consistent associations between eosinophil levels and clinical outcomes. A comprehensive assessment of the risk of adverse outcomes during hospitalization in AECOPD patients based on eosinophil stability is crucial. By integrating previously identified risk factors (baseline characteristics, severity assessments, and hospitalization details),37 we constructed a nomogram to predict adverse hospital outcomes. This model exhibits high predictive power and precision, providing a robust tool for evaluating patient risk and informing personalized treatment strategies.
The role of eosinophils in predicting readmission after discharge in AECOPD patients remains debated. Some studies link high eosinophil levels with increased rehospitalization risk38, while others find no strong association.10 Many previous studies have not accounted for eosinophil levels at discharge, which may overlook critical insights. In our cohort, patients with elevated eosinophils at discharge-both in the persistent and increasing eosinophil groups-demonstrated a heightened risk of rehospitalization. Interestingly, further subgroup analysis of the persistent high eosinophil group showed that these patients had an elevated risk of exacerbation, independent of corticosteroid use during hospitalization. This finding indicates that eosinophil-driven inflammation may not have been fully controlled, leaving patients in a pro-inflammatory state post-discharge.39
In our cohort, systemic corticosteroid use varied across eosinophil stability groups, with a higher proportion in the persistent low group. Although current guidelines suggest that eosinophilic AECOPD patients may benefit more from corticosteroids,7,40 in clinical practice in China, treatment decisions are often based on physician judgment and symptom severity rather than blood eosinophil counts.33,36 Regarding the observed eosinophil increase at discharge in some patients, this may reflect either the intrinsic eosinophilic inflammation phenotype of COPD or a rebound effect after corticosteroid withdrawal. The CORTICO-COP trial, for example, demonstrated a rebound increase in blood eosinophils between days 3 and 5 following the initiation of corticosteroid treatment.15 Additionally, Citgez et al reported that corticosteroid use did not significantly impact eosinophil categorization stability during subsequent AECOPD episodes. To more precisely delineate the impact of treatment on eosinophil dynamics, future studies incorporating prospective designs, standardized treatment protocols, and serial eosinophil monitoring are warranted.
Beyond eosinophils, the association between systemic inflammation and disease severity in AECOPD patients has also been explored through other hematologic biomarkers. One of the most studied markers is the neutrophil-to-lymphocyte ratio (NLR), which has been proposed as a reliable indicator of systemic inflammatory burden. Shao et al41 reported that NLR measured at admission was significantly associated with adverse clinical outcomes and the risk of readmission in patients with AECOPD. However, their analysis was based solely on static, single-time-point measurements, which may overlook important dynamic inflammatory changes during hospitalization. Jiang et al42 subsequently highlighted not only the prognostic relevance of NLR stability, suggesting that the trajectory of inflammatory markers may better reflect disease progression than absolute values. Nevertheless, their outcome assessment was limited to in-hospital events, without consideration of longer-term outcomes such as post-discharge readmission. In contrast, our study focused on the stability of EOS levels during hospitalization and developed a four-group trajectory model based on changes between admission and discharge (persistent high, persistent low, increased, decreased). Our work incorporates a larger sample, longer follow-up, broader outcome assessment, and a dynamic modeling approach—together underscoring the clinical relevance of inflammatory phenotype stability in AECOPD risk stratification.
This study has limitations. First, being a single-center study, its representativeness is limited. Second, as a retrospective study, pre-hospital treatment records for acute exacerbations are often missing, precluding the assessment of pre-hospital corticosteroid treatment. Finally, although the changes in EOS percentage among the increase and decrease groups were ≥0.3%, there is no established consensus on the minimal clinically meaningful change or the threshold for defining eosinophil stability. Further research is warranted to evaluate the prognostic value of more detailed eosinophil trajectories using repeated measurements and standardized definitions.
Conclusions
Our findings reveal that the stability of blood eosinophil levels during hospitalization holds prognostic significance in AECOPD. Early-phase eosinophil changes may guide acute treatment decisions, while discharge eosinophil levels could help predict long-term outcomes such as readmission risk. These findings support incorporating eosinophil dynamics into individualized AECOPD management strategies.
Abbreviations
COPD, chronic obstructive pulmonary disease; AECOPD, acute exacerbation of chronic obstructive pulmonary disease; EOS, eosinophil; EMR, Electronic medical record; IMV, invasive mechanical ventilation; ICU, intensive care unit; LOS, length of stay; IQR, interquartile ranges; OR, odds ratio; CI, confidence interval; GOLD, The Global Initiative for Chronic Obstructive Lung Disease.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author ([email protected]) on reasonable requests.
Ethical Approval and Informed Consent
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Beijing Chao-Yang Hospital (No. 2023-ke-749). This retrospective study used de-identified data, and the requirement for consent to participate was waived by the Ethics Committee of Beijing Chao-Yang Hospital.
Acknowledgments
We appreciate the data collection team from the Beijing Municipal Health Big Data and Policy Research Centre.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Beijing Municipal Administration of Hospitals Incubating Program (PX2020014); Beijing Municipal Science & Technology Commission (Z201100005520028 and Z201100005520029); Beijing Key Specialists in Major Epidemic Prevention and Control; Clinical Research Incubation Project, Beijing Chao-Yang Hospital, Capital Medical University (CYFH202210); Financial Budgeting Project of Beijing Institute of Respiratory Medicine (Ysbz2023002); Clinical Research Incubation Project, Beijing Chao-Yang Hospital, Capital Medical University (CYFH202210); Beijing Municipal Science & Technology Commission (Z231100004623008).
Disclosure
The authors have no competing interests to declare.
References
1. Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. Lancet. 2022;399(10342):2227–2242. doi:10.1016/s0140-6736(22)00470-6
2. Papaioannou AI, Hillas G, Loukides S, Vassilakopoulos T. Mortality prevention as the centre of COPD management. ERJ Open Res. 2024;10(3):00850–2023. doi:10.1183/23120541.00850-2023
3. Vos T, Allen C, Arora M, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the global burden of disease study 2015. Lancet. 2016;388(10053):1545–1602. doi:10.1016/s0140-6736(16)31678-6
4. MacLeod M, Papi A, Contoli M, et al. Chronic obstructive pulmonary disease exacerbation fundamentals: diagnosis, treatment, prevention and disease impact. Respirology. 2021;26(6):532–551. doi:10.1111/resp.14041
5. Gayle A, Dickinson S, Morris K, Poole C, Mathioudakis AG, Vestbo J. What is the impact of GOLD 2017 recommendations in primary care? - a descriptive study of patient classifications, treatment burden and costs. Int J Chronic Obstr. 2018;13:3485–3492. doi:10.2147/copd.S173664
6. Bafadhel M, McKenna S, Terry S, et al. Blood eosinophils to direct corticosteroid treatment of exacerbations of chronic obstructive pulmonary disease: a randomized placebo-controlled trial. Am J Respir Crit Care Med. 2012;186(1):48–55. doi:10.1164/rccm.201108-1553OC.
7. Li J, Liang L, Feng L, et al. The prognostic value of blood eosinophil level in AECOPD is influenced by corticosteroid treatment during hospitalization. J Inflamm Res. 2023;16:3233–3243. doi:10.2147/jir.S421605
8. Zeiger RS, Tran TN, Butler RK, et al. Relationship of blood eosinophil count to exacerbations in chronic obstructive pulmonary disease. J Allergy Clin Immunol Pract. 2018;6(3):944–954.e5. doi:10.1016/j.jaip.2017.10.004
9. Yu S, Zhang J, Fang Q, Tong Z. Blood eosinophil levels and prognosis of hospitalized patients with acute exacerbation of chronic obstructive pulmonary disease. Am J Med Sci. 2021;362(1):56–62. doi:10.1016/j.amjms.2021.02.013
10. Csoma B, Bikov A, Tóth F, Losonczy G, Müller V, Lázár Z. Blood eosinophils on hospital admission for COPD exacerbation do not predict the recurrence of moderate and severe relapses. ERJ Open Res. 2021;7(1). doi:10.1183/23120541.00543-2020
11. You Y, Shi GC. Blood eosinophils and clinical outcome of acute exacerbations of chronic obstructive pulmonary disease: a systematic review and meta-analysis. Resp Inter Rev Thoracic Dis. 2021;100(3):228–237. doi:10.1159/000510516
12. Schumann DM, Tamm M, Kostikas K, Stolz D. Stability of the blood eosinophilic phenotype in stable and exacerbated COPD. Chest. 2019;156(3):456–465. doi:10.1016/j.chest.2019.04.012
13. Shin SH, Park HY, Kang D, et al. Serial blood eosinophils and clinical outcome in patients with chronic obstructive pulmonary disease. Respir Res. 2018;19(1):134. doi:10.1186/s12931-018-0840-x.
14. Casanova C, Celli BR, de-Torres JP, et al. Prevalence of persistent blood eosinophilia: relation to outcomes in patients with COPD. Europ Resp J. 2017;50(5):1701162. doi:10.1183/13993003.01162-2017
15. Sivapalan P, Lapperre TS, Janner J, et al. Eosinophil-guided corticosteroid therapy in patients admitted to hospital with COPD exacerbation (CORTICO-COP): a multicentre, randomised, controlled, open-label, non-inferiority trial. Lancet Respir Med. 2019;7(8):699–709. doi:10.1016/s2213-2600(19)30176-6
16. Cui Y, Zhang W, Ma Y, Zhan Z, Chen Y. Stability of blood eosinophils in acute exacerbation of chronic obstructive pulmonary disease and its relationship to clinical outcomes: a prospective cohort study. Respir Res. 2021;22(1):301. doi:10.1186/s12931-021-01888-5
17. Zhao Q, Li J, Liang L. Establishment and application of the data quality control system of an electronic medical record-based big data platform for respiratory diseases. J Med Inform. 2022;7(43):55–60.
18. Feng L, Li J, Qian Z, et al. Comprehensive nomograms using routine biomarkers beyond eosinophil levels: enhancing predictability of corticosteroid treatment outcomes in AECOPD. J Inflamm Res. 2024;17:1511–1526. doi:10.2147/jir.S450447
19. Li J, Zuo Y, Feng L, et al. Association of blood eosinophils with corticosteroid treatment failure stratified by smoking status among inpatients with AECOPD. BMJ Open Respir Res. 2024;11(1). doi:10.1136/bmjresp-2023-001634
20. Citgez E, van der Palen J, van der Valk P, Kerstjens HAM, Brusse-Keizer M. Stability in eosinophil categorisation during subsequent severe exacerbations of COPD. BMJ Open Respir Res. 2021;8(1). doi:10.1136/bmjresp-2021-000960
21. Stockley RA, Halpin DMG, Celli BR, Singh D. Chronic obstructive pulmonary disease biomarkers and their interpretation. Am J Respir Crit Care Med. 2019;199(10):1195–1204. doi:10.1164/rccm.201810-1860SO
22. Bafadhel M, McKenna S, Terry S, et al. Acute exacerbations of chronic obstructive pulmonary disease: identification of biologic clusters and their biomarkers. Am J Respir Crit Care Med. 2011;184(6):662–671. doi:10.1164/rccm.201104-0597OC.
23. Cardoso J, Ferreira AJ, Guimaraes M, Oliveira AS, Simao P, Sucena M. Treatable traits in COPD - a proposed approach. Int J Chronic Obstr. 2021;16:3167–3182. doi:10.2147/COPD.S330817
24. Agustí A, Celli BR, Criner GJ, et al. Global initiative for chronic obstructive lung disease 2023 report: GOLD executive summary. Europ Resp J. 2023;61(4):2300239. doi:10.1183/13993003.00239-2023
25. Greulich T, Tüffers J, Mager S, et al. High eosinophil blood counts are associated with a shorter length of hospital stay in exacerbated COPD patients - a retrospective analysis. Respir Res. 2020;21(1):106. doi:10.1186/s12931-020-01365-5.
26. Ko FWS, Chan KP, Ngai J, et al. Blood eosinophil count as a predictor of hospital length of stay in COPD exacerbations. Respirology. 2020;25(3):259–266. doi:10.1111/resp.13660
27. Chipps BE, Jarjour N, Calhoun WJ, et al. A comprehensive analysis of the stability of blood eosinophil levels. Ann Am Thoracic Soc. 2021;18(12):1978–1987. doi:10.1513/AnnalsATS.202010-1249OC
28. Singh D, Kolsum U, Brightling CE, Locantore N, Agusti A, Tal-Singer R. Eosinophilic inflammation in COPD: prevalence and clinical characteristics. Eur Respir J. 2014;44(6):1697–1700. doi:10.1183/09031936.00162414
29. Gong Y, Sun H. Stability of blood eosinophils in COPD with multiple acute exacerbations within 1 year and its relationship with prognosis. Int J Chronic Obstr. 2022;17:3123–3128. doi:10.2147/COPD.S392660
30. Zhang Y, Liang LR, Zhang S, et al. Blood eosinophilia and its stability in hospitalized COPD exacerbations are associated with lower risk of all-cause mortality. Int J Chronic Obstr. 2020;15:1123–1134. doi:10.2147/copd.S245056
31. Zheng DL, Wang HM, Liu YC, et al. The distribution of blood eosinophils and the related clinical characteristics in chronic obCOPD patients. Zhonghua Jie He He Hu Xi Za Zhi. 2021;44(3):218–224. doi:10.3760/cma.j.cn112147-20200617-00715.
32. Ko FWS, Chan KP, Ngai J, et al. Blood eosinophil count as a predictor of hospital length of stay in COPD exacerbations. Respirology. 2020;25(3):259–266. doi:10.1111/resp.13660
33. Cui Y, Zhan Z, Zeng Z, et al. Blood eosinophils and clinical outcomes in patients with acute exacerbation of chronic obstructive pulmonary disease: a propensity score matching analysis of real-world data in China. Front Med Lausanne. 2021;8:653777. doi:10.3389/fmed.2021.653777
34. Mou S, Zhang W, Deng Y, Tang Z, Jiang D. Comparison of CRP, procalcitonin, neutrophil counts, eosinophil counts, sTREM-1, and OPN between pneumonic and nonpneumonic exacerbations in COPD patients. Can Respir J. 2022;2022:7609083. doi:10.1155/2022/7609083
35. Gao S, Duan Y, Chen J, Wang J. Evaluation of blood markers at admission for predicting community acquired pneumonia in chronic obstructive pulmonary disease. Copd. 2021;18(5):557–566. doi:10.1080/15412555.2021.1976739
36. Pu J, Yi Q, Luo Y, et al. Blood eosinophils and clinical outcomes in inpatients with acute exacerbation of chronic obstructive pulmonary disease: a prospective cohort study. Int J Chron Obstruct Pulmon Dis. 2023;18:169–179. doi:10.2147/copd.S396311
37. Cao Y, Xing Z, Long H, et al. Predictors of mortality in COPD exacerbation cases presenting to the respiratory intensive care unit. Respir Res. 2021;22(1):77. doi:10.1186/s12931-021-01657-4
38. Hegewald MJ, Horne BD, Trudo F, et al. Blood eosinophil count and hospital readmission in patients with acute exacerbation of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2020;15:2629–2641. doi:10.2147/copd.S251115
39. David B, Bafadhel M, Koenderman L, De Soyza A. Eosinophilic inflammation in COPD: from an inflammatory marker to a treatable trait. Thorax. 2021;76(2):188–195. doi:10.1136/thoraxjnl-2020-215167
40. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease report; 2024. Availble from: https://goldcopd.org/2024-gold-report/.
41. Shao S, Zhang Z, Feng L, Liang L, Tong Z. Association of blood inflammatory biomarkers with clinical outcomes in patients with AECOPD: an 8-year retrospective study in Beijing. Int J Chron Obstruct Pulmon Dis. 2023;18:1783–1802. doi:10.2147/copd.S416869
42. Jiang M, Yang Y, Wang H. Stability of neutrophil to lymphocyte ratio in acute exacerbation of chronic obstructive pulmonary disease and its relationship with clinical outcomes: a retrospective cohort study. Int J Chron Obstruct Pulmon Dis. 2024;19:2431–2441. doi:10.2147/copd.S487063
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.