Back to Journals » OncoTargets and Therapy » Volume 19
Bladder-Preserving Platforms for BCG-Unresponsive Non-Muscle-Invasive Bladder Cancer
Received 2 April 2026
Accepted for publication 5 June 2026
Published 15 June 2026 Volume 2026:19 614003
DOI https://doi.org/10.2147/OTT.S614003
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr John Maher
Kaiyuan Zhang, Yanche Ren
Department of Urology, the First Hospital of China Medical University, Shenyang, Liaoning, People’s Republic of China
Correspondence: Yanche Ren, Department of Urology, the First Hospital of China Medical University, No. 155 Nanjing North Street, Heping District, Shenyang, Liaoning, 110001, People’s Republic of China, Email [email protected]
Abstract: Bacillus Calmette Guerin (BCG)-unresponsive high-risk non-muscle-invasive bladder cancer (NMIBC) remains a difficult clinical setting in which radical cystectomy offers the most reliable oncologic control but is not feasible or acceptable for many patients. This review examines contemporary bladder-preserving strategies, with emphasis on biologic intravesical platforms, device-assisted drug-delivery systems, systemic immunotherapy, and pragmatic intravesical chemotherapy alternatives. These approaches should not be viewed as interchangeable. Biologic platforms seek to restore or intensify local antitumor immunity, whereas device-assisted strategies aim to overcome the pharmacokinetic limitations of conventional intravesical therapy by improving residence time, exposure, or tissue penetration. Across platforms, clinically meaningful activity has been reported, but current evidence remains constrained by single-arm study designs, heterogeneous eligibility criteria, non-equivalent endpoints, and variable follow-up maturity. As a result, available data support expansion of bladder-preserving options but do not establish a definitive treatment hierarchy. In clinical practice, differences in durability, toxicity, treatment burden, BCG dependence, device requirements, access, and biomarker eligibility may be as important as initial response rates. The central challenge is therefore shifting from whether bladder preservation is possible to how available options should be selected, sequenced, and integrated for individual patients. More harmonized comparative evidence, mature post-failure data, and clinically deployable biomarker frameworks will be needed to guide future treatment allocation.
Keywords: non-muscle-invasive bladder cancer, Bacillus Calmette Guerin, Bacillus Calmette Guerin-unresponsive, bladder preservation, intravesical therapy, device-assisted drug delivery
Introduction
Bladder cancer is among the most frequently diagnosed malignancies worldwide.1 Approximately three quarters of newly diagnosed cases are non–muscle-invasive.2 Within non-muscle-invasive bladder cancer (NMIBC), high-risk disease remains a major clinical problem because recurrence and progression continue despite transurethral resection followed by intravesical Bacillus Calmette Guerin (BCG), which remains the benchmark adjuvant bladder-preserving therapy.3 Nevertheless, a substantial subset of patients develop persistent, recurrent, or early relapsing high-grade disease despite adequate BCG exposure. The formalization of BCG-unresponsive disease was therefore an important advance, providing a more uniform clinical and trial framework for evaluating novel bladder-preserving therapies.4,5
Radical cystectomy remains the preferred oncologic standard for this population.6,7 However, that recommendation sits in constant tension with real-world practice. Cystectomy offers excellent cancer control, but at the cost of substantial perioperative morbidity, non-trivial mortality in selected patients, and permanent effects on urinary, sexual, and psychosocial function.8,9 Many patients are medically unfit for cystectomy, whereas others are technically operable but reluctant to accept the consequences of immediate bladder removal. The central clinical question in BCG-unresponsive NMIBC is therefore not whether cystectomy remains the reference treatment, but which patients can reasonably pursue bladder preservation without compromising oncologic safety. This question is especially relevant when adverse pathological features are present. High-risk histologic variants and poorly differentiated components, including plasmacytoid, sarcomatoid, and micropapillary features, may increase the risk of BCG failure and alter the risk-benefit balance of bladder-preserving salvage. Although robust variant-specific estimates of BCG-unresponsive disease frequency remain limited, available NMIBC data suggest that these features should be treated as risk-modifying factors rather than as a homogeneous contraindication to bladder preservation, with interpretation depending on histologic subtype, tumor burden, completeness of resection, and patient fitness for cystectomy.
Recent advances in intravesical therapy have evolved along two broads, partly overlapping lines. One seeks to restore or amplify local antitumor immunity through gene-based, viral, or cytokine-mediated strategies. The other seeks to improve drug delivery by prolonging dwell time, sustaining effective intravesical exposure, or enhancing urothelial penetration. This distinction is clinically useful because post-BCG treatment failure reflects both biologic resistance and the pharmacokinetic limitations of conventional intravesical instillation.
The need for such a framework has become more pressing as recent long-term follow-up, regulatory reports, and late-phase studies have expanded the bladder-preserving landscape beyond older salvage approaches. However, these data have also created a practical interpretive problem: available platforms differ in mechanism, disease phenotype, endpoint definition, response assessment, treatment burden, follow-up maturity, BCG dependence, and biomarker requirements. The resulting unmet need is not simply for additional active agents, but for a clinically usable way to distinguish, contextualize, and eventually sequence non-equivalent bladder-preserving strategies. This review therefore organizes contemporary platforms according to their biologic and pharmacokinetic rationale, summarizes recent evidence, and highlights the methodological and clinical factors that should guide treatment interpretation.
Biological and Pharmacokinetic Bases of BCG Failure
Key Vulnerable Nodes in BCG-Mediated Immune Activation
The antitumor activity of intravesical BCG is initiated by urothelial attachment and internalization, followed by activation of innate immune pathways and subsequent recruitment of adaptive antitumor immunity.3 A further mechanistic dimension that has gained increasing attention is trained immunity, whereby BCG induces epigenetic and metabolic reprogramming of innate immune cells, resulting in a heightened secondary response state.10 In bladder cancer, available human data support the biological relevance of this phenomenon, but its exact contribution to durable oncologic benefit remains incompletely defined.11
BCG failure can arise from disruption of these early immunologic steps. Reduced attachment or internalization may blunt initial immune priming, and experimental data support a role for fibronectin-mediated binding in this process.12 Similarly, inadequate innate activation or inefficient antigen presentation may limit transition to effective adaptive antitumor immunity.8 These biological vulnerabilities help explain why subsequent intravesical platform development has focused either on restoring local immune priming or on augmenting downstream effector-cell function.
Immune Escape Mechanisms in BCG-Unresponsive Tumors
Immune escape after BCG failure appears biologically heterogeneous rather than mechanistically uniform. Paired tumor analyses indicate that relapse after BCG can follow at least two immune-evasion trajectories: HLA-I downregulation associated with a myeloid-immunosuppressive, EMT-skewed microenvironment, or maintenance/upregulation of HLA-I within an inflamed, checkpoint-enriched state.13 This heterogeneity argues against reducing BCG failure to a single escape axis and instead supports mechanistically differentiated platform development.
Among candidate checkpoint pathways, the PD-1/PD-L1 axis is among the best supported in this setting. Baseline PD-L1 positivity has been associated with subsequent BCG nonresponse.14 In KEYNOTE-057 cohort A, pembrolizumab monotherapy achieved a 3-month complete response rate of 41% in patients with carcinoma in situ (CIS)-containing BCG-unresponsive disease.15 Taken together, these data support biological relevance of the pathway, but also indicate that PD-1 blockade alone is insufficient for durable disease control in a substantial proportion of patients. Recent translational work has also linked poor BCG response to a pretreatment B-cell–rich microenvironment characterized by tumor-adjacent tertiary lymphoid structures, atypical B-cell programs, and local immune-exhaustion signals.16 These findings extend the biology of BCG failure beyond a purely T-cell checkpoint framework and support continued exploration of combination or multi-compartment immune strategies.
Pharmacokinetic Limitations of Conventional Intravesical Instillation
Beyond immune escape, conventional intravesical instillation is limited by fundamental delivery constraints. Effective local exposure is brief because dwell time is typically restricted to 1–2 h and the instilled solution is subsequently lost with voiding; ongoing urine production may further reduce intravesical drug concentration.17 In parallel, the urothelium forms a high-resistance barrier, with the umbrella-cell apical surface and tight-junction architecture restricting trans urothelial transport into deeper tissue compartments.18 These constraints have driven the development of engineering-based intravesical platforms designed either to prolong intravesical residence and stabilize local exposure or to enhance permeability and local drug effect.2,17
From a therapeutic-design standpoint, failure of bladder-preserving treatment after adequate BCG can be understood along two nonexclusive axes: biologic failure, characterized by insufficient immune activation or subsequent immune evasion, and delivery failure, characterized by inadequate residence time, urine-mediated dilution, and limited trans urothelial penetration. Much of the current intravesical pipeline can be interpreted within this framework, with biologic platforms intended to intensify local antitumor immunity and engineering platforms intended to optimize local drug exposure.
Biologic Intravesical Instillation Platforms
Biologic intravesical platforms are developed on the premise that at least some post-BCG failures reflect inadequate local immune reactivation rather than residual tumor burden alone.3 Despite sharing this general objective, these agents differ substantially in mechanism. Nadofaragene firadenovec provides local interferon-based gene transfer, cretostimogene grenadenorepvec combines selective viral oncolysis with GM-CSF–mediated immune stimulation, and nogapendekin alfa inbakicept is intended to strengthen residual responsiveness to BCG rather than replace it. These agents are better understood as mechanistically distinct immunologic bladder-preserving strategies within the same clinical setting.
Non-Replicating Adenoviral Gene Therapy: Nadofaragene Firadenovec (Adstiladrin)
Nadofaragene firadenovec is a non-replicating adenoviral vector carrying the human interferon alfa-2b gene and is administered intravesically once every three months. After intravesical transduction of urothelial cells, enhanced by the surfactant excipient Syn3, the urothelium becomes a local source of IFN-α2b, thereby providing local type I interferon signaling within the bladder after BCG failure.19,20
Among biologic intravesical agents, nadofaragene firadenovec has one of the most mature peer-reviewed evidence bases and the most developed long-term follow-up. In the pivotal Phase 3 CS-003 study, 53.4% of patients with CIS with or without papillary disease achieved complete response within 3 months, and among initial responders, 46% maintained complete response at 12 months, with a median response duration of 9.7 months.20 Five-year follow-up from the same phase 3 program provides unusually mature outcome data for this setting, with 60-month overall survival of 76% in the CIS cohort and 86% in the Ta/T1 cohort, 60-month cystectomy-free survival of 49% overall, and clinical progression to muscle-invasive disease in only five patients.21
The safety profile has remained favorable. In the 5-year follow-up analysis, most study drug–related adverse events were grade 1 or 2, grade 3 events occurred in 3.8% of patients, and no grade 4 or 5 study drug–related adverse events were reported.21 On this basis, nadofaragene firadenovec received FDA approval in December 2022 for adult patients with high-risk BCG-unresponsive NMIBC with CIS with or without papillary tumors, becoming the first approved gene therapy for bladder cancer.22
Its main limitation is durability rather than initial activity. Despite meaningful early complete response rates, durable long-term high-grade recurrence-free control is maintained in only a minority of patients.21 Higher post-treatment antiadenoviral antibody titers were associated with greater response durability in a planned secondary analysis, but this signal remains hypothesis-generating rather than practice-changing.23 Clinically, nadofaragene firadenovec is best positioned as a low-frequency outpatient bladder-preserving option with regulatory maturity and unusually mature follow-up, although combination strategies with chemotherapy or checkpoint blockade remain under evaluation to address limited long-term disease control.21–23
Oncolytic Adenoviral Immunotherapy: Cretostimogene Grenadenorepvec (CG0070)
Cretostimogene grenadenorepvec is a conditionally replicating serotype 5 oncolytic adenovirus engineered for preferential replication in bladder cancer cells with dysregulated Rb–E2F signaling and for local GM-CSF expression.24 Unlike non-replicating gene delivery, this platform couples tumor-selective viral replication with local immune stimulation: replication-associated tumor cell lysis can promote release of tumor antigens and danger-associated signals, while the GM-CSF transgene is intended to enhance antigen presentation and downstream antitumor immunity.25 Clinically, cretostimogene is more appropriately framed as an intravesical oncolytic immunotherapy platform than as a conventional gene-delivery product, because its activity depends on both selective viral lysis and immune activation.
In practical terms, the platform is designed to do more than transduce urothelial tissue. Its therapeutic logic is sequential and immunobiologic: tumor-selective viral replication produces direct oncolysis, while virus-driven inflammatory signaling together with GM-CSF expression is intended to convert local tumor destruction into broader immune priming. Recent reviews of oncolytic virus therapy therefore characterize agents such as cretostimogene through three coupled functions—selective replication, direct oncolysis, and immune activation—rather than as conventional gene-delivery products.
Clinically, cretostimogene is among the most advanced investigational intravesical agents in this setting, but the peer-reviewed monotherapy record remains less mature than that of approved platforms.26 Later-stage monotherapy updates have been encouraging, yet precise statements regarding complete response rate, durability, or papillary-only activity should still await full peer-reviewed reporting of the registrational dataset.
In the peer-reviewed literature available to date, tolerability has generally been acceptable and adverse events have been dominated by local urinary symptoms.27 However, it would be too strong to characterize cretostimogene-based therapy as free of grade 3 treatment-related toxicity, because grade 3 treatment-related adverse events have been reported in the Phase 2 CORE-001 study; that study also used weekly induction with protocol-defined re-induction and maintenance, supporting a relatively intensive but still workable intravesical schedule.28 Regulatory positioning should be described cautiously until the registrational monotherapy dataset is fully published in a peer-reviewed format.
The key limitation at present is the maturity of the evidence rather than the coherence of the biologic rationale. Cretostimogene has a strong mechanistic basis and encouraging clinical signals, but its comparative position among bladder-preserving platforms should remain provisional until mature peer-reviewed monotherapy data become available. By contrast, combination treatment with pembrolizumab is already supported by a full peer-reviewed phase 2 publication, in which the 12-month and 24-month complete response rates were 57.1% and 51.4%, respectively, in CIS-containing BCG-unresponsive NMIBC.28 Whether Rb–E2F dysregulation can evolve from a biologic selection principle into a clinically useful predictive biomarker remains unproven.
IL-15 Receptor Agonist–Based BCG Potentiation: Nogapendekin Alfa Inbakicept (NAI/N-803, Anktiva) Plus BCG
Nogapendekin alfa inbakicept (NAI, N-803) is an IL-15 receptor agonist complex that activates NK cells and CD8-positive T cells while showing limited stimulation of regulatory T cells in preclinical systems.29 Unlike nadofaragene firadenovec and cretostimogene grenadenorepvec, however, NAI is not best viewed as a BCG-independent intravesical platform. Rather, its clinical role is to potentiate residual BCG responsiveness and reinforce local antitumor immunity.
In the FDA-reviewed efficacy population of the CIS-containing cohort, NAI plus BCG achieved a complete response rate of 62% (48/77); among complete responders, 58% and 40% maintained response for at least 12 and 24 months, respectively. In the monotherapy cohort, NAI alone was stopped early for futility, with a complete response rate of 20% and only one durable complete response lasting at least 6 months. Pharmacokinetic analyses showed systemic NAI exposure below the limit of quantitation after intravesical administration, and these data supported FDA approval of NAI plus BCG for BCG-unresponsive NMIBC with CIS, with or without papillary tumors.29
In papillary-only disease, the 12-, 24-, and 36-month disease-free survival rates were 58.2%, 52.1%, and 38.2%, respectively, and the 36-month cystectomy avoidance rate was 81.8%; most treatment-related adverse events were grade 1–2, with 3% grade 3 and no grade 4–5 events.30 Taken together, the available evidence indicates that the clinically meaningful activity of this platform is a property of the NAI–BCG combination rather than of NAI monotherapy. Its main clinical attraction is that it extends the utility of an established BCG backbone; however, broader deployment remains contingent on reliable BCG access.
Device-Assisted Delivery Platforms
If biologic intravesical therapies primarily attempt to restore or amplify antitumor immunity, device-assisted platforms address a different therapeutic problem: the physical inefficiency of conventional intravesical drug delivery. Their clinical rationale lies in prolonging drug exposure, stabilizing local drug concentration, or improving tissue penetration across the urothelial barrier. Accordingly, their value lies less in molecular novelty than in whether improved exposure or penetration can be translated into meaningful antitumor activity, rather than in whether they replicate the immune-restorative logic of biologic therapies.
Intravesical Gemcitabine-Releasing System: TAR-200
TAR-200 is a gemcitabine-releasing intravesical drug-delivery system developed to sustain local drug exposure within the bladder.26 Its rationale is pharmacokinetic rather than mechanistically novel: by prolonging intravesical residence time and mitigating the concentration variability inherent to conventional instillation, it is intended to improve delivery of an established cytotoxic agent across a biologically restrictive urothelial environment.17 In this respect, TAR-200 is conceptually distinct from immune-restorative intravesical therapies, because its therapeutic logic lies in optimizing local exposure rather than reprogramming antitumor immunity.
In the phase IIb SunRISe-1 study, TAR-200 monotherapy achieved a centrally confirmed complete response rate of 82.4% in BCG-unresponsive CIS with or without papillary disease, with a median time to response of 2.8 months and a median duration of response of 25.8 months. In the papillary-only cohort, the 12-month disease-free survival rate was 70.2%.31 These results indicate substantial clinical activity. However, because SunRISe-1 did not include a comparator arm using conventional gemcitabine instillation, the incremental therapeutic contribution of sustained-release delivery cannot be quantified directly.
Although the complete response rate was numerically higher with TAR-200 monotherapy than with TAR-200 plus cetrelimab (82.4% vs 67.9%), SunRISe-1 was a phase IIb parallel-cohort study and did not support formal between-cohort efficacy comparisons.31 These data do not show that PD-1 blockade diminished activity; rather, the published dataset has not demonstrated a clear added-value signal sufficient to justify the additional complexity and toxicity of combination treatment.
Safety was dominated by lower urinary tract and device-related adverse events, most of which were low grade; in the CIS monotherapy cohort, grade ≥3 treatment-related adverse events occurred in 12.9%, serious treatment-related adverse events in 5.9%, and discontinuation because of treatment-related adverse events in 3.5%.31 Taken together, TAR-200 currently stands as the most clinically advanced exposure-engineered intravesical platform. Its significance lies in showing that sustained local delivery of a familiar cytotoxic agent can produce substantial activity and encouraging durability without reliance on a novel molecular target. At the same time, its comparative place in therapy remains unresolved because direct comparisons against conventional intravesical gemcitabine and other contemporary bladder-preserving options are lacking, and repeated device exchanges remain integral to treatment burden and real-world acceptability.26,31,32
Targeted Intravesical FGFR Inhibition: TAR-210
TAR-210 is an investigational intravesical erdafitinib-releasing platform being evaluated in FGFR-altered NMIBC. Its rationale is to combine molecular selection with sustained intravesical drug delivery in order to deliver FGFR inhibition locally while potentially reducing reliance on systemic therapy.
Clinical support for FGFR-directed therapy in NMIBC currently comes from oral erdafitinib rather than from TAR-210 itself. In BCG-treated, papillary-only high-risk disease harboring FGFR3/2 alterations, oral erdafitinib prolonged recurrence-free survival versus intravesical chemotherapy.33 Final analyses also suggested activity in CIS-containing and intermediate-risk cohorts.34 By contrast, direct peer-reviewed clinical evidence for TAR-210 remains limited, and the platform is therefore better viewed as an investigational biomarker-selected, device-assisted intravesical approach rather than an established bladder-preserving option.
The appeal of this strategy lies in its biologic selectivity. Its trade-offs are narrower eligibility and a practical dependence on routine, reliable molecular testing. For now, TAR-210 is best viewed as a precision-oriented investigational platform whose eventual place in therapy will depend on mature peer-reviewed data on efficacy, durability, and comparative value.
Hyperthermic Intravesical Chemotherapy
Chemohyperthermia combines intravesical chemotherapy—most commonly mitomycin C—with controlled bladder heating to enhance drug penetration and augment local cytotoxicity.35 Unlike TAR-200 and TAR-210, which are designed to prolong intravesical exposure, chemohyperthermia seeks to intensify tissue penetration and pharmacologic effect during the instillation itself. It therefore belongs within the same device-assisted framework of pharmacokinetic optimization, albeit through transient heat-enabled delivery rather than sustained release.2
Interpretation of chemohyperthermia requires explicit separation of platforms rather than pooled discussion under a single label. Radiofrequency-induced thermo-chemotherapy and recirculating conductive HIVEC share the goal of heat-enabled pharmacologic intensification, but they differ in heat generation, temperature control, drug-circulation dynamics, treatment schedule, and practical delivery. These differences are not merely technical details; they may influence tissue penetration, tolerability, and ultimately clinical outcome. For that reason, chemohyperthermia should be approached as a family of device-dependent modalities rather than as one standardized intervention.2,26
The HYMN trial remains particularly important because it showed that radiofrequency-induced chemohyperthermia did not improve overall disease-free survival over standard second-line intravesical management in patients with recurrence after prior BCG, with less favorable results in CIS-containing disease.36 However, that result should be interpreted as a negative trial for a specific platform in a specific post-BCG context, not as a universal refutation of all heat-assisted intravesical chemotherapy. At the same time, encouraging noncomparative experiences with other systems, including HIVEC-based approaches, are not sufficient to establish a standard of care. The most balanced conclusion is therefore that chemohyperthermia remains mechanistically credible and clinically relevant, but its role after BCG failure must be defined at the device level rather than inferred from cross-platform generalization.
At present, chemohyperthermia is best positioned as a pragmatic but nonstandard bladder-preserving strategy rather than as a validated post-BCG standard. Its attraction lies in combining an established intravesical chemotherapy backbone with device-mediated pharmacokinetic enhancement, but its eventual place in treatment algorithms will depend on stronger device-specific comparative evidence, more mature outcome reporting, and better real-world data on implementation and tolerability.26
Benchmarks, Pragmatic Alternatives, and Emerging Strategies
Pembrolizumab: The Systemic Immunotherapy Benchmark
Pembrolizumab, a humanized anti–PD-1 monoclonal antibody, received FDA approval in January 2020 for patients with BCG-unresponsive high-risk NMIBC with CIS, with or without papillary tumors, who were ineligible for or declined radical cystectomy, on the basis of KEYNOTE-057 cohort A. In the peer-reviewed cohort A report, 39 of 96 evaluable patients (40.6%; 95% CI 30.7–51.1) achieved complete response at 3 months after a median follow-up of 36.4 months; median duration of response was 16.2 months, and 46% of responders remained in response for at least 12 months.15 Cohort B enrolled 132 patients with papillary-only BCG-unresponsive disease and reported a 12-month disease free survival (DFS) rate of 43.5% (95% CI: 34.9–51.9%) with a median DFS of 7.7 months.37
As a systemically administered therapy, pembrolizumab carries an inherently different risk profile from intravesical agents. In the published KEYNOTE-057 reports, grade 3–4 treatment-related adverse events occurred in 13% of cohort A and 14% of cohort B; immune-related toxicities included thyroid dysfunction, colitis, adrenal insufficiency, and pneumonitis, and no treatment-related deaths were reported in the peer-reviewed cohort publications.15,37 Economic analyses have raised affordability concerns, but their conclusions are strongly model- and pathway-dependent rather than uniformly unfavorable to pembrolizumab.38
For treatment selection, pembrolizumab is more appropriately considered a systemic bladder-preserving option than a like-for-like comparator to intravesical platforms. Cross-trial comparisons with bladder-confined therapies therefore remain inherently limited and should be interpreted cautiously.32
Intravesical Chemotherapy Optimization: Sequential Gemcitabine and Docetaxel
Among conventional intravesical chemotherapy regimens, sequential gemcitabine followed by docetaxel has emerged as a pragmatic bladder-preserving salvage option supported mainly by retrospective multicenter evidence. In a multi-institutional study of 276 patients with recurrent NMIBC previously treated with BCG, the 1-year and 2-year high-grade recurrence-free survival rates were 65% and 52%, respectively, with generally acceptable tolerability.39 Although that cohort was not limited to strictly BCG-unresponsive disease and the evidence base remains nonrandomized, more recent comparative analyses in patients meeting BCG-unresponsive criteria suggest that gemcitabine-docetaxel may reduce progression relative to additional salvage BCG.40 Separate cohort-level comparisons in high-risk treatment-naïve disease have also reported lower recurrence and high-grade recurrence rates, together with less induction discontinuation, than BCG.41 These data do not elevate gemcitabine-docetaxel above approved post-BCG agents in evidentiary hierarchy, but they do support its continued relevance as a low-cost, reproducible, and globally deployable comparator within contemporary bladder-preserving algorithms.
Emerging Investigational Intravesical Strategies
Several other intravesical approaches remain at an earlier stage of clinical development. In a phase 2 study, oportuzumab monatox induced complete response in 44% of patients, but only 16% remained disease free at last follow-up, underscoring the limited durability observed to date.42 Preclinical development is also ongoing for mucoadhesive nanoparticles, thermosensitive hydrogels, and liposomal formulations intended to prolong intravesical residence and enhance tissue penetration.17 Photodynamic therapy has shown antitumor activity in selected BCG-refractory or BCG-intolerant cohorts, but procedural complexity and specialized equipment requirements continue to limit broader adoption. Taken together, these approaches remain less clinically mature than the leading late-phase biologic and device-assisted platforms discussed above. More broadly, systematic appraisal of post-BCG clinical and preclinical pipelines indicates that many investigational strategies remain early phase, single arm, and difficult to compare directly, which should temper enthusiasm based on pipeline breadth alone.43
Clinical Interpretation Across Platforms and Implications for Treatment Selection
In clinical practice, treatment selection should begin with disease phenotype and patient-level suitability rather than with nominal response rates alone. Key considerations include CIS-containing versus papillary-only disease, tumor burden, completeness of resection, variant histology or other adverse pathological features, fitness for radical cystectomy, patient preference, tolerance for systemic immune-related toxicity, ability to comply with repeated intravesical visits or device exchanges, BCG availability, molecular eligibility such as FGFR alteration status, and the consequences of delayed definitive surgery. These factors do not generate a fixed algorithm, but they provide a practical framework for matching non-equivalent bladder-preserving platforms to individual clinical contexts. A concise summary of selected bladder-preserving platforms, including mechanism, regulatory or investigational status, key efficacy endpoints, toxicity profile, and practical considerations, is provided in Table 1.
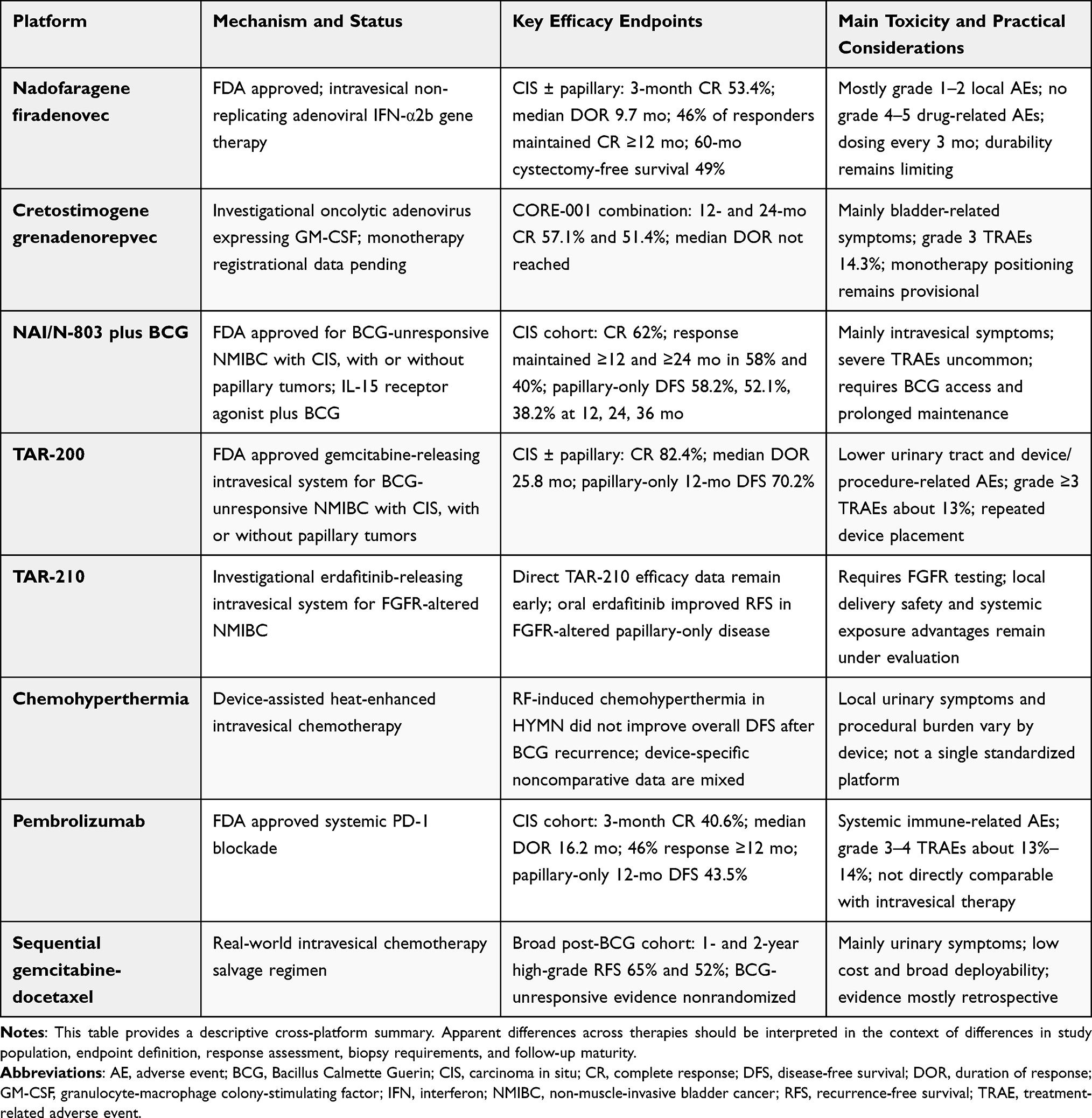 |
Table 1 Selected Bladder-Preserving Platforms for BCG-Unresponsive High-Risk NMIBC |
Methodological Challenges in Cross-Trial Efficacy Comparisons
Cross-platform efficacy comparisons remain fundamentally limited by the absence of randomized head-to-head trials.32 For the principal approved and late-stage bladder-preserving platforms, the available evidence is derived predominantly from single-arm registration studies, which does not permit a defensible efficacy hierarchy across agents.44 Nevertheless, recent studies provide useful comparative perspectives when interpreted descriptively rather than as direct evidence of superiority. For example, updated data for nadofaragene firadenovec, pembrolizumab, NAI plus BCG, TAR-200, and sequential gemcitabine-docetaxel allow comparison across clinically relevant domains such as CIS-containing versus papillary-only disease, complete response, DOR, DFS or recurrence-free survival, cystectomy avoidance, toxicity profile, visit burden, BCG dependence, and follow-up maturity.15,20,21,29–31,37,40 These comparisons are most informative when they clarify how platforms differ in clinical positioning rather than when they are used to rank efficacy numerically.
Indirect comparisons are further undermined by between-study differences in enrolled disease phenotype, stringency of BCG-unresponsive definitions, endpoint selection, response adjudication, and follow-up maturity.45 Differences in response confirmation are particularly important: pivotal studies varied in the timing and use of protocol-mandated biopsies and in whether response was adjudicated locally or centrally, so observed differences in complete response or durability may partly reflect assessment intensity rather than treatment effect alone.22,29,31 A recent contemporary review reached a similar conclusion, estimating broadly moderate aggregate activity across salvage strategies but finding heterogeneity too substantial for any defensible ranking of contemporary agents46. Thus, the most balanced use of recent comparative evidence is to support patient- and platform-level contextualization, not to imply a validated treatment hierarchy.
Interpreting Efficacy Across Non-Comparable Studies
In this setting, cross-trial reading should remain descriptive rather than hierarchical, with interpretation anchored to disease phenotype, endpoint construction, and follow-up maturity rather than to nominal response rates alone.44,45 Among CIS-containing cohorts with peer-reviewed efficacy data, several platforms have shown clinically meaningful activity, with especially strong initial complete response reported for TAR-200, while NAI plus BCG, nadofaragene firadenovec, and pembrolizumab have also demonstrated meaningful activity in this disease state.15,20,29,31 Cretostimogene monotherapy also remains promising, but its quantitative placement should remain provisional until mature peer-reviewed monotherapy data are available. Differences in biopsy mandates, endpoint construction, and follow-up maturity further limit any inference about relative superiority.32,45 Durability comparisons require even greater caution, because the commonly cited 12-month metrics are derived from non-equivalent denominators and definitions. TAR-200 reported a 12-month CR rate of 45.9% from treatment initiation and duration of response (DOR) ≥12 months in 52.9% of responders; nadofaragene maintained response at 12 months in 45.5% of initial complete responders; pembrolizumab maintained response for at least 12 months in 46% of responders; and NAI plus BCG maintained response for at least 12 months in 58% of responders.15,20,29,31 The same caution applies to median DOR, which is influenced not only by antitumor activity but also by differences in response assessment, censoring, and durability definitions across studies.32,45 Peer-reviewed reports support a median DOR of 25.8 months for TAR-200, 9.7 months for nadofaragene firadenovec, and 16.2 months for pembrolizumab.15,20,31 For NAI plus BCG, the most robust peer-reviewed emphasis remains durability among responders rather than a directly comparable median DOR estimate.29 Quantitative placement of cretostimogene monotherapy should therefore remain provisional until mature peer-reviewed monotherapy data are available.26
In papillary-only cohorts, the currently peer-reviewed 12-month DFS rates are 70.2% for TAR-200, 58.2% for NAI plus BCG, and 43.5% for pembrolizumab.30,31,37 Cretostimogene should not yet be assigned a like-for-like 12-month monotherapy estimate in this setting, and a 9-month figure should not be used as a surrogate 12-month comparator.26 Long-term outcome maturity remains greatest for nadofaragene firadenovec: in the 5-year phase 3 follow-up, 60-month overall survival was 80% overall and 60-month cystectomy-free survival was 49% overall.21 Comparable peer-reviewed long-term survival follow-up is not yet available for the other platforms.
Safety Profile Differentiation
Safety differences across platforms are clinically relevant and broadly reflect route of exposure and device dependence. Peer-reviewed data indicate that cretostimogene-based therapy is generally well tolerated, with adverse events predominantly consisting of transient local urinary symptoms; in the phase 2 CORE-001 combination study, grade 3 treatment-related adverse events occurred in 14.3% of patients.28 Nadofaragene firadenovec also has a favorable long-term safety profile, with grade 3 study drug-related adverse events reported in 3.8% of patients and no grade 4 or 5 events in the 5-year phase 3 follow-up.21 NAI plus BCG likewise appears to retain a predominantly intravesical toxicity pattern; the FDA approval summary described its safety as consistent with expected intravesical toxicities, and systemic N-803 exposure after intravesical administration was below the limit of quantitation.29 For TAR-200, grade ≥3 treatment-related adverse events were reported in 12.9% of the CIS cohort and 13.5% of the papillary-only cohort in SunRISe-1; the adverse-event profile was dominated overall by lower urinary tract and device/procedure-related events.31 Pembrolizumab remains qualitatively distinct because systemic immune-related toxicity is integral to its risk profile; in KEYNOTE-057, grade 3–4 treatment-related adverse events occurred in 13% of the CIS-containing cohort and 14% of the papillary-only cohort, and immune-mediated events included thyroid dysfunction, colitis, adrenal insufficiency, and pneumonitis.15,37 These proportions should still be interpreted descriptively rather than comparatively, because follow-up length, adverse-event capture intensity, treatment schedule, and the inclusion of device- or procedure-related events are not uniform across studies.
Administration Convenience and Patient Burden
Administration burden also differs substantially across platforms and should be weighed alongside efficacy and safety. Nadofaragene firadenovec is administered intravesically once every 3 months and therefore imposes a relatively low visit frequency.20 TAR-200 requires repeated brief office-based procedures, with administration every 3 weeks through month 6 and then every 12 weeks through month 24.31 In CORE-001, cretostimogene was administered weekly for 6 weeks, with re-induction at month 3 permitted for persistent CIS or high-grade Ta, followed in complete responders by three weekly maintenance instillations at months 3, 6, 9, 12, and 18.28 NAI plus BCG is likewise schedule-intensive: the approved regimen consists of weekly induction for 6 weeks, an additional induction course when needed, and weekly-for-3-weeks maintenance at months 4, 7, 10, 13, and 19, with optional further maintenance at months 25, 31, and 37 in ongoing complete responders.29 Accordingly, treatment selection is influenced not only by efficacy and safety, but also by visit frequency, device handling, and the feasibility of prolonged maintenance.
Combination Strategies: Early Evidence and Paradoxes
Early data on combination strategies remain heterogeneous. In the phase 2 CORE-001 trial, cretostimogene plus pembrolizumab showed encouraging activity in CIS-containing BCG-unresponsive NMIBC, consistent with—but not proving—the biologic rationale for combining oncolytic immunotherapy with PD-1 blockade.28 By contrast, SunRISe-1 did not provide a clear efficacy advantage for TAR-200 plus cetrelimab over TAR-200 monotherapy; however, because this was a parallel-cohort phase IIb study rather than a randomized head-to-head comparison, formal between-cohort superiority or inferiority cannot be concluded.31 Accordingly, the currently available dataset does not establish a clear incremental benefit for adding PD-1 blockade to a highly active local delivery platform, whereas additional toxicity remains pertinent to the overall risk-benefit balance.31 Additional randomized studies and biomarker-informed combination trials are needed before these regimens can be positioned with confidence.45
Toward Biomarker-Guided Treatment Selection
No prospectively validated biomarker has yet entered routine clinical use for selecting among bladder-preserving therapies after BCG-unresponsive disease.32 FGFR2/3 alteration status currently provides the clearest biomarker-defined entry point for intravesical precision therapy, but its clinical role remains investigational rather than established across approved intravesical options.33 Rb–E2F pathway dysregulation has biologic relevance as a determinant of cretostimogene replicative selectivity, but it has not been prospectively validated as a clinical predictive biomarker.24 PD-L1 expression is biologically relevant in this setting, but it has not become a prospectively validated treatment-selection biomarker in NMIBC.14 Beyond FGFR-directed enrichment, platform-specific predictive markers for the major non-targeted intravesical options remain exploratory.32 Transcriptomic subtype frameworks may ultimately refine treatment selection, but their use for assigning specific post-BCG intravesical therapies remains unvalidated.32,46 Any move toward biomarker-guided allocation will also require clinically implementable urine-based workflows and standardized assay pathways, not merely exploratory molecular associations.47
Future treatment selection is more likely to emerge from integrated tissue and urine-based molecular frameworks than from any single immunohistochemical marker. In particular, the BCG response subtype 3 (BRS3) phenotype has been linked to an epithelial-to-mesenchymal transition/basal program, an immunosuppressive microenvironment, enrichment among tumors recurring after BCG, and poorer progression outcomes than BRS1/2. Complementing tissue-based subtyping, field-effect-informed urinary tumor DNA approaches have recently shown that molecular response classes can distinguish surgery responders, BCG responders, and nonresponders, suggesting that biologically distinct treatment-sensitive states may be detectable noninvasively. In the post-BCG salvage setting, urinary minimal residual disease assessment after nadofaragene induction has already shown prognostic value for recurrence-free survival. These developments do not yet justify routine biomarker-driven assignment of a specific approved platform, but they make a purely empiric, one-size-fits-all sequencing strategy increasingly difficult to defend.46,48,49
Global Access and Cost Considerations
Economic and implementation issues deserve greater attention as bladder-preserving treatment becomes more diversified. Available cost-effectiveness analyses suggest that apparent value is highly scenario dependent rather than fixed across agents: gemcitabine-docetaxel performed favorably in several modeled settings, whereas HIVEC also appeared cost-effective under selected assumptions.38,50 These findings support caution against universal economic rankings across health systems, because conclusions vary according to treatment pathway, willingness-to-pay threshold, reimbursement context, and assumptions regarding the timing of radical cystectomy.
Access should also be viewed as an oncologic systems issue rather than a narrow pricing issue. The BCG shortage era showed that treatment-supply disruption can be associated with higher recurrence, progression, cystectomy use, and overall costs.51 In parallel, long-term observational data indicate that progression in high-risk NMIBC is linked to substantially greater downstream expenditure, underscoring that short-term acquisition cost alone is an incomplete measure of value.52 Thus, future comparative work should assess not only efficacy and durability, but also implementation burden, treatment availability, pathway consistency, and the clinical consequences of delayed disease control. Real-world positioning of these therapies is also shaped by regulatory approvals, local availability, and practice environment as much as by efficacy alone.6,7
Conclusion
Bladder-preserving treatment for BCG-unresponsive NMIBC has evolved from a limited salvage setting into a diversified landscape of non-equivalent therapeutic platforms. Biologic intravesical strategies, device-assisted delivery systems, systemic immunotherapy, and optimized intravesical chemotherapy differ not only in efficacy signals, but also in mechanism, durability, toxicity, treatment burden, access, dependence on BCG supply, and biomarker requirements. These differences are clinically important because treatment selection increasingly requires platform-level judgment rather than simple substitution among available agents.
Current evidence supports the expanding role of bladder preservation but does not establish a definitive treatment hierarchy. Most available data come from single-arm studies with heterogeneous eligibility criteria, endpoint definitions, response-assessment protocols, and follow-up maturity, making nominal cross-trial comparisons insufficient for determining relative efficacy. Radical cystectomy therefore remains the oncologic reference standard, particularly for patients with adverse disease features or a low likelihood of durable bladder control. For patients pursuing bladder preservation, contemporary options should be interpreted as differently positioned tools whose use depends on disease phenotype, patient fitness and preference, expected treatment burden, toxicity profile, access, and the consequences of delayed definitive therapy.
Future progress will require more interpretable evidence rather than additional isolated activity signals alone. Harmonized trial design, mature durability and post-failure sequencing data, real-world implementation studies, and clinically deployable biomarker frameworks will be essential for moving beyond empiric treatment selection. Until such evidence becomes available, bladder-preserving therapies should be selected through individualized clinical reasoning rather than treated as rank-ordered substitutes.
Declaration of Generative AI Use
Authors declare no AI use during the preparation of this work.
Abbreviations
BCG, Bacillus Calmette Guerin; NMIBC, non-muscle-invasive bladder cancer; CIS, carcinoma in situ; NAI, Nogapendekin alfa inbakicept; DOR, duration of response; DFS, disease free survival; BRS3, BCG response subtype 3.
Author Contributions
Both authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding.
Disclosure
The authors declare no competing interests.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–14. doi:10.3322/caac.21660
2. Tan WS, Kelly JD. Intravesical device-assisted therapies for non-muscle-invasive bladder cancer. Nat Rev Urol. 2018;15:667–685. doi:10.1038/s41585-018-0092-z
3. Pettenati C, Ingersoll MA. Mechanisms of BCG immunotherapy and its outlook for bladder cancer. Nat Rev Urol. 2018;15:615–625. doi:10.1038/s41585-018-0055-4
4. Kamat AM, Sylvester RJ, Böhle A, et al. Definitions, end points, and clinical trial designs for non-muscle-invasive bladder cancer: recommendations from the international bladder cancer group. J Clin Oncol. 2016;34:1935–1944. doi:10.1200/jco.2015.64.4070
5. Kamat AM, Colombel M, Sundi D, et al. BCG-unresponsive non-muscle-invasive bladder cancer: recommendations from the IBCG. Nat Rev Urol. 2017;14:244–255. doi:10.1038/nrurol.2017.16
6. Babjuk M, Burger M, Capoun O, et al. European association of urology guidelines on non-muscle-invasive bladder cancer (Ta, T1, and Carcinoma in Situ). Eur Urol. 2022;81:75–94. doi:10.1016/j.eururo.2021.08.010
7. Holzbeierlein JM, Bixler BR, Buckley DI, et al. Diagnosis and treatment of non-muscle invasive bladder cancer: AUA/SUO guideline: 2024 amendment. J Urol. 2024;211:533–538. doi:10.1097/ju.0000000000003846
8. Stein JP, Lieskovsky G, Cote R, et al. Radical cystectomy in the treatment of invasive bladder cancer: long-term results in 1054 patients. J Clin Oncol. 2001;19:666–675. doi:10.1200/jco.2001.19.3.666
9. Clements MB, Atkinson TM, Dalbagni GM, et al. Health-related quality of life for patients undergoing radical cystectomy: results of a large prospective cohort. Eur Urol. 2022;81:294–304. doi:10.1016/j.eururo.2021.09.018
10. Netea MG, Domínguez-Andrés J, Barreiro LB, et al. Defining trained immunity and its role in health and disease. Nat Rev Immunol. 2020;20:375–388. doi:10.1038/s41577-020-0285-6
11. van Puffelen JH, Novakovic B, van Emst L, et al. Intravesical BCG in patients with non-muscle invasive bladder cancer induces trained immunity and decreases respiratory infections. J Immunother Cancer. 2023;11. doi:10.1136/jitc-2022-005518
12. Ratliff TL, Kavoussi LR, Catalona WJ. Role of fibronectin in intravesical BCG therapy for superficial bladder cancer. J Urol. 1988;139:410–414. doi:10.1016/s0022-5347(17)42445-1
13. Rouanne M, Adam J, Radulescu C, et al. BCG therapy downregulates HLA-I on malignant cells to subvert antitumor immune responses in bladder cancer. J Clin Invest. 2022;132. doi:10.1172/jci145666
14. Kates M, Matoso A, Choi W, et al. Adaptive immune resistance to intravesical BCG in non-muscle invasive bladder cancer: implications for prospective BCG-unresponsive trials. Clin Cancer Res. 2020;26:882–891. doi:10.1158/1078-0432.Ccr-19-1920
15. Balar AV, Kamat AM, Kulkarni GS, et al. Pembrolizumab monotherapy for the treatment of high-risk non-muscle-invasive bladder cancer unresponsive to BCG (KEYNOTE-057): an open-label, single-arm, multicentre, phase 2 study. Lancet Oncol. 2021;22:919–930. doi:10.1016/s1470-2045(21)00147-9
16. Yolmo P, Rahimi S, Chenard S, et al. Atypical B cells promote cancer progression and poor response to bacillus calmette-guérin in non-muscle invasive bladder cancer. Cancer Immunol Res. 2024;12:1320–1339. doi:10.1158/2326-6066.Cir-23-1114
17. Li ZA, Wen KC, Liu JH, Zhang C, Zhang F, Li FQ. Strategies for intravesical drug delivery: from bladder physiological barriers and potential transport mechanisms. Acta Pharm Sin B. 2024;14:4738–4755. doi:10.1016/j.apsb.2024.07.003
18. Dalghi MG, Montalbetti N, Carattino MD, Apodaca G. The urothelium: life in a liquid environment. Physiol Rev. 2020;100:1621–1705. doi:10.1152/physrev.00041.2019
19. Shore ND, Boorjian SA, Canter DJ, et al. Intravesical rAd-IFNα/Syn3 for patients with high-grade, bacillus calmette-guerin-refractory or relapsed non-muscle-invasive bladder cancer: a phase II randomized study. J Clin Oncol. 2017;35:3410–3416. doi:10.1200/jco.2017.72.3064
20. Boorjian SA, Alemozaffar M, Konety BR, et al. Intravesical nadofaragene firadenovec gene therapy for BCG-unresponsive non-muscle-invasive bladder cancer: a single-arm, open-label, repeat-dose clinical trial. Lancet Oncol. 2021;22:107–117. doi:10.1016/s1470-2045(20)30540-4
21. Narayan VM, Boorjian SA, Alemozaffar M, et al. Efficacy of intravesical nadofaragene firadenovec for patients with bacillus calmette-guérin-unresponsive nonmuscle-invasive bladder cancer: 5-year follow-up from a phase 3 trial. J Urol. 2024;212:74–86. doi:10.1097/ju.0000000000004020
22. Colbert L, Jia Y, Sharma A, et al. FDA approval summary: nadofaragene firadenovec-vncg for bacillus calmette-guérin-unresponsive non-muscle-invasive bladder cancer. Clin Cancer Res. 2025;31:1182–1185. doi:10.1158/1078-0432.Ccr-24-2812
23. Mitra AP, Narayan VM, Mokkapati S, et al. Antiadenovirus antibodies predict response durability to nadofaragene firadenovec therapy in BCG-unresponsive non-muscle-invasive bladder cancer: secondary analysis of a phase 3 clinical trial. Eur Urol. 2022;81:223–228. doi:10.1016/j.eururo.2021.12.009
24. Ramesh N, Ge Y, Ennist DL, et al. CG0070, a conditionally replicating granulocyte macrophage colony-stimulating factor--armed oncolytic adenovirus for the treatment of bladder cancer. Clin Cancer Res. 2006;12:305–313. doi:10.1158/1078-0432.Ccr-05-1059
25. Li R, Zhang J, Gilbert SM, Conejo-Garcia J, Mulé JJ. Using oncolytic viruses to ignite the tumour immune microenvironment in bladder cancer. Nat Rev Urol. 2021;18:543–555. doi:10.1038/s41585-021-00483-z
26. Ghodoussipour S, Bivalacqua T, Bryan RT, et al. A systematic review of novel intravesical approaches for the treatment of patients with non-muscle-invasive bladder cancer. Eur Urol. 2025;88:33–55. doi:10.1016/j.eururo.2025.02.010
27. Burke JM, Lamm DL, Meng MV, et al. A first in human Phase 1 study of CG0070, a GM-CSF expressing oncolytic adenovirus, for the treatment of nonmuscle invasive bladder cancer. J Urol. 2012;188:2391–2397. doi:10.1016/j.juro.2012.07.097
28. Li R, Shah PH, Stewart TF, et al. Oncolytic adenoviral therapy plus pembrolizumab in BCG-unresponsive non-muscle-invasive bladder cancer: the phase 2 CORE-001 trial. Nat Med. 2024;30:2216–2223. doi:10.1038/s41591-024-03025-3
29. Heiss BL, Chang E, Joeng HK, et al. FDA approval summary: nogapendekin Alfa Inbakicept-pmln with BCG for BCG-unresponsive carcinoma in situ. Clin Cancer Res. 2025;31:4223–4229. doi:10.1158/1078-0432.Ccr-25-1231
30. Chang SS, Chamie K, Kramolowsky E, et al. Prolonged progression-free survival, disease-free survival, and cystectomy avoidance with IL-15 receptor lymphocyte-stimulating agent NAI plus Bacillus Calmette-Guérin in Bacillus Calmette-Guérin-unresponsive papillary-only nonmuscle-invasive bladder cancer. J Urol. 2026;215:44–56. doi:10.1097/ju.0000000000004782
31. Daneshmand S, Van der Heijden MS, Jacob JM, et al. TAR-200 for Bacillus Calmette-Guérin-unresponsive high-risk non-muscle-invasive bladder cancer: results from the phase IIb SunRISe-1 study. J Clin Oncol. 2025;43:3578–3588. doi:10.1200/jco-25-01651
32. Li R, Hensley PJ, Gupta S, et al. Bladder-sparing therapy for Bacillus Calmette-Guérin-unresponsive non-muscle-invasive bladder cancer: international bladder cancer group recommendations for optimal sequencing and patient selection. Eur Urol. 2024;86:516–527. doi:10.1016/j.eururo.2024.08.001
33. Catto JWF, Tran B, Rouprêt M, et al. Erdafitinib in BCG-treated high-risk non-muscle-invasive bladder cancer. Ann Oncol. 2024;35:98–106. doi:10.1016/j.annonc.2023.09.3116
34. Daneshmand S, Zaucha R, Catto JWF, et al. Erdafitinib in patients with high- and intermediate-risk non-muscle-invasive bladder cancer: final analysis of THOR-2 study. Eur Urol. 2026;89:165–173. doi:10.1016/j.eururo.2025.09.4152
35. Lammers RJ, Witjes JA, Inman BA, et al. The role of a combined regimen with intravesical chemotherapy and hyperthermia in the management of non-muscle-invasive bladder cancer: a systematic review. Eur Urol. 2011;60:81–93. doi:10.1016/j.eururo.2011.04.023
36. Tan WS, Panchal A, Buckley L, et al. Radiofrequency-induced thermo-chemotherapy effect versus a second course of Bacillus Calmette-Guérin or institutional standard in patients with recurrence of non-muscle-invasive bladder cancer following induction or maintenance Bacillus Calmette-Guérin Therapy (HYMN): a Phase III, open-label, randomised controlled trial. Eur Urol. 2019;75:63–71. doi:10.1016/j.eururo.2018.09.005
37. Necchi A, Roumiguié M, Kamat AM, et al. Pembrolizumab monotherapy for high-risk non-muscle-invasive bladder cancer without carcinoma in situ and unresponsive to BCG (KEYNOTE-057): a single-arm, multicentre, phase 2 trial. Lancet Oncol. 2024;25:720–730. doi:10.1016/s1470-2045(24)00178-5
38. Myers AA, Talwar R, Duan Z, et al. Cost-effectiveness analysis of treatments for Bacillus Calmette-Guérin-unresponsive carcinoma in situ of the bladder. Eur Urol. 2026;89:151–162. doi:10.1016/j.eururo.2025.09.4137
39. Steinberg RL, Thomas LJ, Brooks N, et al. Multi-institution evaluation of sequential gemcitabine and docetaxel as rescue therapy for nonmuscle invasive bladder cancer. J Urol. 2020;203:902–909. doi:10.1097/ju.0000000000000688
40. Taylor J, Kamat AM, Annapureddy D, et al. Oncologic outcomes of sequential intravesical gemcitabine and docetaxel compared with bacillus calmette-guérin in patients with Bacillus Calmette-Guérin-Unresponsive non-muscle invasive bladder cancer. Eur Urol Oncol. 2025;8:469–476. doi:10.1016/j.euo.2024.12.005
41. McElree IM, Steinberg RL, Mott SL, O’Donnell MA, Packiam VT. Comparison of sequential intravesical gemcitabine and docetaxel vs Bacillus Calmette-Guérin for the treatment of patients with high-risk non-muscle-invasive bladder cancer. JAMA Netw Open. 2023;6:e230849. doi:10.1001/jamanetworkopen.2023.0849
42. Kowalski M, Guindon J, Brazas L, et al. A phase II study of oportuzumab monatox: an immunotoxin therapy for patients with noninvasive urothelial carcinoma in situ previously treated with bacillus Calmette-Guérin. J Urol. 2012;188:1712–1718. doi:10.1016/j.juro.2012.07.020
43. Nazmifar M, Williams C, Naser-Tavakolian A, et al. Clinical and preclinical therapies for bladder cancer following bacillus calmette-guérin failure. J Urol. 2023;209:32–48. doi:10.1097/ju.0000000000002957
44. Li R, Sundi D, Zhang J, et al. Systematic review of the therapeutic efficacy of bladder-preserving treatments for non-muscle-invasive bladder cancer following intravesical Bacillus Calmette-Guérin. Eur Urol. 2020;78:387–399. doi:10.1016/j.eururo.2020.02.012
45. Roumiguié M, Kamat AM, Bivalacqua TJ, et al. International bladder cancer group consensus statement on clinical trial design for patients with Bacillus Calmette-Guérin-exposed high-risk non-muscle-invasive bladder cancer. Eur Urol. 2022;82:34–46. doi:10.1016/j.eururo.2021.12.005
46. de Jong FC, Laajala TD, Hoedemaeker RF, et al. Non-muscle-invasive bladder cancer molecular subtypes predict differential response to intravesical Bacillus Calmette-Guérin. Sci Transl Med. 2023;15:eabn4118. doi:10.1126/scitranslmed.abn4118
47. Liedberg F, Mariappan P, Gontero P. Clinical implementation of urinary biomarkers for surveillance of Non-muscle-invasive Bladder Cancer (NMIBC): considerations from the European association of urology NMIBC guideline panel. Eur Urol Oncol. 2025;8:234–236. doi:10.1016/j.euo.2024.09.011
48. Shi WY, Liu KJ, Esfahani MS, et al. Field-effect-informed urine liquid biopsy for bladder cancer. Cell. 2026;189:1024–1038.e1029. doi:10.1016/j.cell.2025.12.054
49. Narayan VM, Tholomier C, Mokkapati S, et al. Minimal residual disease detection with urine-derived DNA is prognostic for recurrence-free survival in Bacillus Calmette-Guérin-unresponsive non-muscle-invasive bladder cancer treated with nadofaragene firadenovec. Eur Urol Oncol. 2025;8:425–434. doi:10.1016/j.euo.2024.09.016
50. Rieger C, Schlüchtermann J, Storz E, Kastner L, Pfister D, Heidenreich A. Cost-effectiveness analysis of different treatment modalities in BCG-unresponsive NMIBC. BJU Int. 2024;134:582–588. doi:10.1111/bju.16332
51. Ourfali S, Ohannessian R, Fassi-Fehri H, Pages A, Badet L, Colombel M. Recurrence rate and cost consequence of the shortage of Bacillus Calmette-Guérin connaught strain for bladder cancer patients. Eur Urol Focus. 2021;7:111–116. doi:10.1016/j.euf.2019.04.002
52. Williams SB, Howard LE, Foster ML, et al. Estimated costs and long-term outcomes of patients with high-risk non-muscle-invasive bladder cancer treated with Bacillus Calmette-Guérin in the veterans affairs health system. JAMA Netw Open. 2021;4:e213800. doi:10.1001/jamanetworkopen.2021.3800
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Experimental and New Approaches for Bladder Preservation in Intermediate and High-Risk Non-Muscle-Invasive Bladder Cancer (NMIBC)
Avilez ND, Capibaribe DM, Reis LO
Research and Reports in Urology 2024, 16:89-113
Published Date: 6 April 2024