Back to Journals » Clinical Interventions in Aging » Volume 16
Bisphosphonates May Reduce Intraoperative Blood Loss in Surgery for Metastatic Spinal Disease: A Retrospective Cohort Study
Authors Zhang HR ![]() , Zhao YL, Qiao RQ, Li JK, Hu YC
, Zhao YL, Qiao RQ, Li JK, Hu YC
Received 19 August 2021
Accepted for publication 9 October 2021
Published 1 November 2021 Volume 2021:16 Pages 1943—1953
DOI https://doi.org/10.2147/CIA.S324975
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Hao-Ran Zhang,1,* Yun-Long Zhao,1,* Rui-Qi Qiao,2 Ji-Kai Li,2 Yong-Cheng Hu1
1Department of Bone Tumor, Tianjin Hospital, Tianjin, People’s Republic of China; 2Graduate School, Tianjin Medical University, Tianjin, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yong-Cheng Hu
Department of Bone Tumor, Tianjin Hospital, 406 Jiefang Southern Road, Tianjin, People’s Republic of China
Email [email protected]
Purpose: This study was undertaken to investigate the relationship between bisphosphonate use and intraoperative blood loss following surgery for metastatic spinal disease.
Methods: We retrospectively analyzed cancer patients who were treated by metastatic spinal tumor surgery at our institution. Recorded data included intraoperative blood loss, timing and duration of bisphosphonate use, and other important confounding factors. We showed the results of crude model, minimally adjusted model, and fully adjusted model to fully observe the effects of bisphosphonates under different adjustment strategies. The timing and duration of bisphosphonate exposure were assessed and statistical results were tested to identify a trend.
Results: A total of 467 patients were treated by metastatic spinal tumor surgery, with or without bisphosphonate treatments. In all adjustment strategies, intraoperative blood loss was lower in patients using bisphosphonates than in patients without bisphosphonate treatments. In the fully adjusted model, the effect size, confidence interval, and p value were − 246.4, − 447.0 to − 45.8, and 0.017, respectively. In terms of duration, all three models showed the same duration–response relationship: a longer duration of bisphosphonate use accurately predicted a smaller amount of blood loss (p for trend < 0.001). We observed an interaction between operative time and bisphosphonate use, the effect size in the bottom tertile group was significantly smaller than that in the other two groups.
Conclusion: We found that the preoperative use of bisphosphonates could reduce the amount of intraoperative blood loss during metastatic spinal tumor surgery, especially for surgery with longer operative time.
Keywords: metastatic spinal disease, intraoperative blood loss, bisphosphonate, surgery
Introduction
As cancer patients live longer and various diagnostic measures continue to improve, the incidence of metastatic spinal disease in the population is increasing. The spine is the third most common site of cancer metastases, second only to the lung and liver.1–3 The treatment of spinal metastases requires multidisciplinary collaboration, including surgery, radiotherapy and chemotherapy. In a randomized controlled trial conducted by Patchell et al in 2005,4 patients were randomly divided into two groups: surgical decompression plus radiotherapy or radiotherapy alone, to explore the importance of surgery in the treatment of spinal metastases. The results showed that the clinical outcome of patients receiving surgical decompression combined with radiotherapy was better than that of patients receiving radiotherapy alone. The publication of this landmark article confirms the role of surgery in the management of spinal metastases. The purposes of surgery are to relieve the symptoms of spinal cord compression, restore and maintain spinal stability, and improve the life expectancy and quality of life of cancer patients as much as possible.
However, metastatic spinal tumor surgery is a challenging operation, often accompanied by a huge amount of blood loss during surgery and a very long operative time. A meta-analysis of blood loss during spinal tumor surgery and metastatic spinal tumor surgery revealed a pooled estimate of blood loss of 2180 mL.5 Therefore, it is important to accurately identify the influencing factors of intraoperative blood loss and make corresponding preventive measures in time. Previous literature reported that type of primary tumor, surgical method, operation time, preoperative embolization, tumor location and instrumentation and decompression levels can affect the amount of blood loss during the operation.6–8 Unfortunately, few studies have focused on the effects of bisphosphonate on intraoperative blood loss, and more attention has been paid to the effects of bisphosphonate on pain relief and prevention of skeletal related events.9–11 To our knowledge, only one cohort study explored the association between bisphosphonate and blood loss.12 However, this study had a small sample size and did not adjust for important confounding variables. What is more notable is that the patients enrolled in this study were given bisphosphonates only 2–5 days before surgery. In fact, a part of patients will receive bisphosphonates via oral or intravenous infusion a few months before surgery, therefore it is necessary to explore the timing and duration of bisphosphonate use.
The purpose of this study is to assess the correlation between bisphosphonate use and intraoperative blood loss during metastatic spinal tumor surgery. We hypothesized that the use of bisphosphonates could reduce the amount of intraoperative blood loss, and the longer the duration, the more significant the effect would be.
Materials and Methods
Patients
We retrospectively analyzed 467 cancer patients who underwent metastatic spinal tumor surgery at our institution between 2009 and 2019. The indications for surgery were worsening neurological function, existing or potential spinal instability, pain that cannot be alleviated, or a combination of these factors. The exclusion criteria were as follows: a history of previous surgery for spinal metastases, a history of radiation therapy, a history of preoperative embolization, minimally invasive surgery for spinal metastases, and surgery for sacral metastases. This study received ethical approval from the institutional review board (2019-089) and each patient obtained informed consent.
Recorded Data
We obtained the required data by searching medical records and hospital electronic records. The recorded data included demographic characteristics, primary tumor type, comorbidity index, location and number of metastatic tumors, preoperative Frankel score, timing and duration of bisphosphonate use, and intraoperative details, including surgical type and approach, instrumentation and decompression levels, operative time and amount of blood loss.
At least 1 week before surgery, we would stop giving patients antiplatelet and anticoagulant drugs to avoid prolonged coagulation time and bleeding time during the surgery. Prior to surgery, routine blood and biochemical tests were performed. If the patient had an abnormal blood parameter, appropriate adjustment measures would be taken to normalize it or surgery would be delayed until the normal state appears.
The comorbidity index was measured and calculated according to the method published by Charlson et al.13 According to Kumar et al’s classification of spinal metastases,6 we divided the primary tumor types into three groups: highly vascularized, moderately vascularized, and hematologic metastases. We believed that such classification could improve statistical power and more clearly determine the differences between the three groups. The neurological status of cancer patient before surgery was evaluated according to the Frankel score: patients with A-C grade were considered to be nonambulatory, and patients with D-E grade retained walking function.14 The surgical methods we used varied according to the location and size of metastatic tumors and can be divided into three categories in general: palliative instrumentation and decompression (type 1), subtotal corpectomy (type 2), and total en bloc spondylectomy (type 3).15 Reconstruction and stabilization procedures were performed via pedicle screws, titanium mesh, bone cement, and bone graft fusion alone or with various combinations.
The intraoperative blood loss in this study was obtained from the anesthetist’s medical records and records of intraoperative fluid management. In general, anesthetist calculated the amount of blood loss during the operation by adding the amount of blood collected in suction bottles and weighing all wound swabs.
The timing and duration of bisphosphonate exposure were assessed by examining medical records and electronic prescriptions. Depending on whether bisphosphonate was used, study population were classified as ever users and never users. The ever users were patients who had at least one record of bisphosphonate use. According to the timing of use, ever users were further subdivided into past use (if the latest record ended more than 1 month before the date of surgery), recent use (if the latest record ended between 1 week and 1 month before the date of surgery), and current use (if the latest record lasted through the date of surgery or ended within 1 week before surgery). In order to more fully assess the effects of bisphosphonate on intraoperative blood loss, the study population was divided into four subgroups based on the cumulative duration of treatment: no use, less than 1 week, 1 week to 1 month, and more than 1 month.
Statistical Analysis
Continuous data were expressed as mean ± standard deviation and categorical data were expressed in frequency or as a percentage. The Student’s t-tests (continuous variables) and chi-square tests (categorical variables) were used to confirm any statistical differences between means and proportions. Univariate linear regression model was used to evaluate the correlation between bisphosphonate use and intraoperative blood loss. According to the recommendations of The Strengthening the Reporting of Observational Studies in Epidemiology statement,16 we showed the results of crude model, minimally adjusted model, and fully adjusted model to fully observe the effects of bisphosphonates under different adjustment strategies. The principle for determining covariates that need to be adjusted is as follows: when added to the model, changed the corresponding effect size by at least 10%.17 The timing and duration of bisphosphonate exposure were assessed and statistical results were tested to identify a trend. Tests for trend were performed by entering the median of each category of bisphosphonate exposure as a continuous data in the models. Exploratory subgroup analysis using the hierarchical linear regression model is essential for identifying special populations. Likelihood ratio tests were used to examine effect modifiers and interactions of subgroups.18 A p value of less than 0.05 (two-sided) represented a statistically significant difference. All statistical analyses were performed using R version 3.5.2 for Windows (R Foundation for Statistical Computing, Vienna, Austria) and GraphPad Prism 8 Software (GraphPad Software Inc., San Diego, CA).
Results
Baseline Characteristics
A total of 467 patients were treated by metastatic spinal tumor surgery, with or without bisphosphonate treatment. Table 1 summarizes the participants’ baseline characteristics and surgical details. There were 257 male patients (55.0%) and 210 female patients (45.0%) with a mean age of 58.4 ± 10.7 years. Before surgery, 325 patients (69.6%) had not used bisphosphonate drugs, while the remaining 142 patients (30.4%) had ever used them. There were 78 cases of highly vascularized metastases (16.7%), 346 cases of moderately vascularized metastases (74.1%), and 43 cases of hematologic metastases (9.2%). In terms of tumor location, thoracic metastases were the most common type (229 cases, 49.0%), followed by lumbar metastases (180 cases, 38.5%) and cervical metastases (58 cases, 12.4%). Eighty-one patients (17.3%) underwent palliative instrumentation and decompression, 361 patients (77.3%) underwent subtotal corpectomy, and only 25 patients (5.4%) underwent total en bloc spondylectomy.
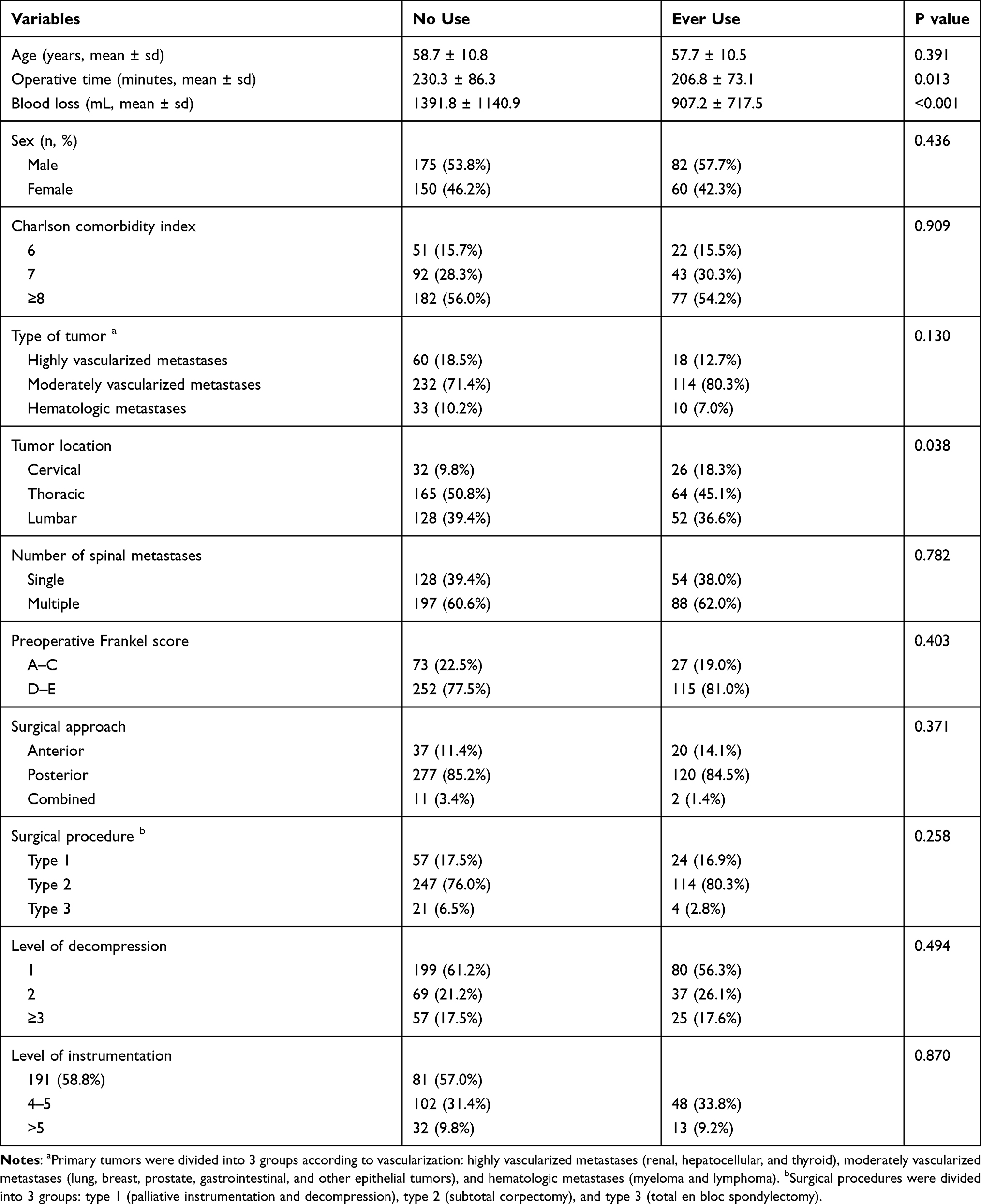 |
Table 1 Baseline Characteristics of Participants |
Compared with patients who had not used bisphosphonates, the ever users had shorter operative time (p = 0.013) and a higher proportion of cervical metastases (p = 0.038). There were no significant differences in the remaining clinical characteristics between the two groups.
Univariate Analysis
Thirteen potential influencing factors were analyzed individually to identify the relationship with intraoperative blood loss. The results of univariate linear regression analysis are shown in Table 2. We noted that type of tumor (p < 0.001), tumor location (p < 0.001), operative time (p < 0.001), surgical approach (p = 0.005), surgical type (p < 0.001), and bisphosphonate use (p < 0.001) were significantly associated with intraoperative blood loss. The remaining variables including sex (p = 0.372), age (p = 0.608), Charlson comorbidity index (p = 0.283), number of spinal metastases (p = 0.789), preoperative Frankel score (p = 0.704), level of decompression (p = 0.716), and level of instrumentation (p = 0.152) were not related to intraoperative blood loss. Using a box plot to qualitatively show the relationship between bisphosphonate use and intraoperative blood loss, we could find that the difference was also significant (Figure 1).
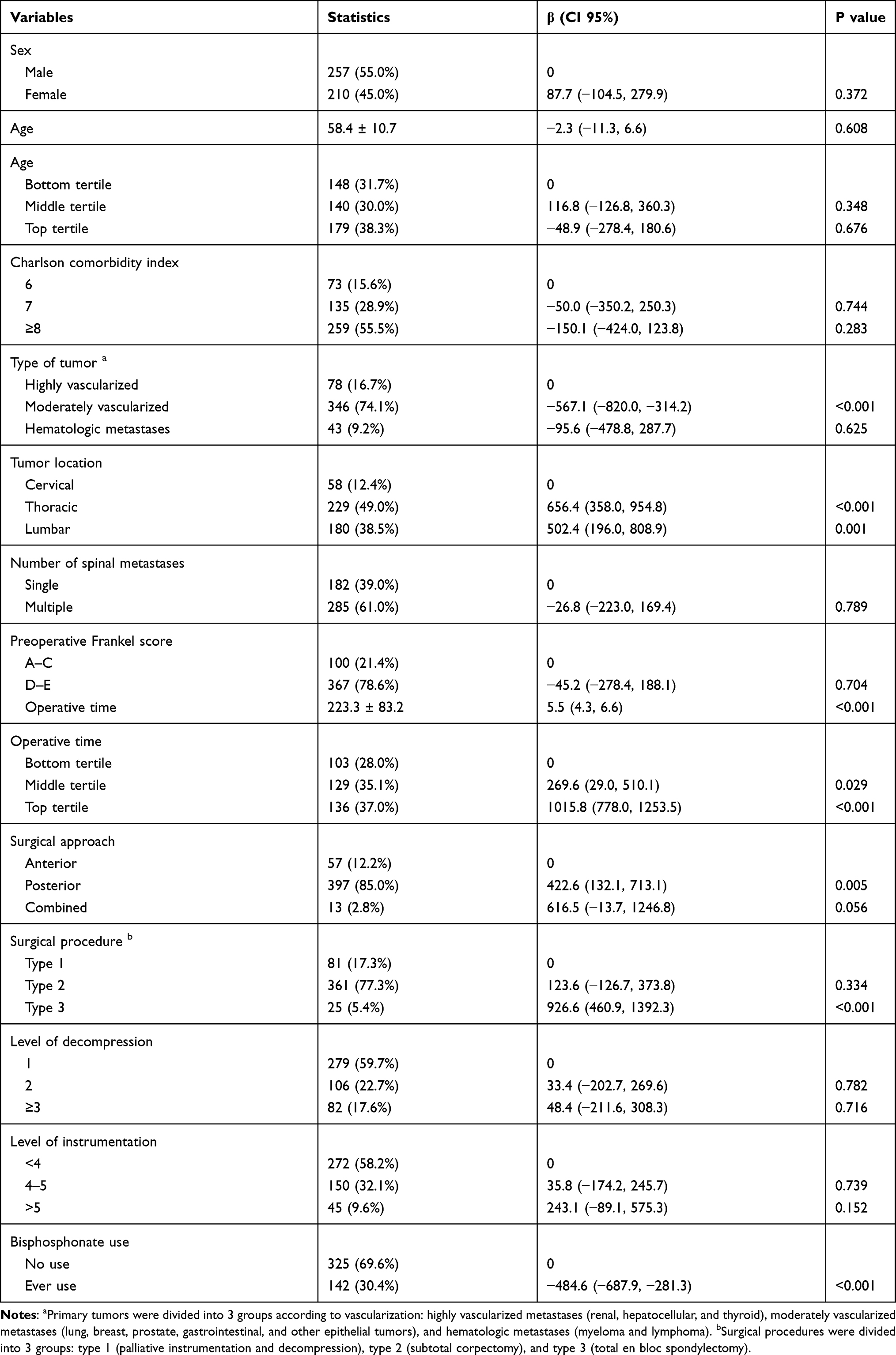 |
Table 2 Effects of Risk Factors on Blood Loss by Univariate Analysis |
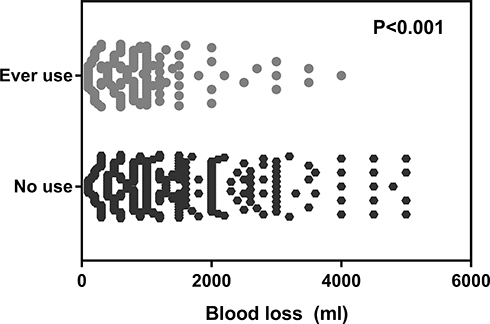 |
Figure 1 The intraoperative blood loss in patients with bisphosphonate treatments and patients without bisphosphonate treatments. There was a significant difference in the intraoperative blood loss between the two groups (p < 0.001). |
Multivariate Analysis
We used multivariate linear regression models to assess the correlations between bisphosphonates and intraoperative blood loss. In order to compare the differences between several adjustment strategies, we listed the crude model, minimally adjusted model, and fully adjusted model at the same time in Table 3. In all adjustment strategies, intraoperative blood loss was lower in patients using bisphosphonates than in patients without bisphosphonate treatments. In the fully adjusted model, the effect size, confidence interval, and p value were −246.4, −447.0 to −45.8, and 0.017, respectively.
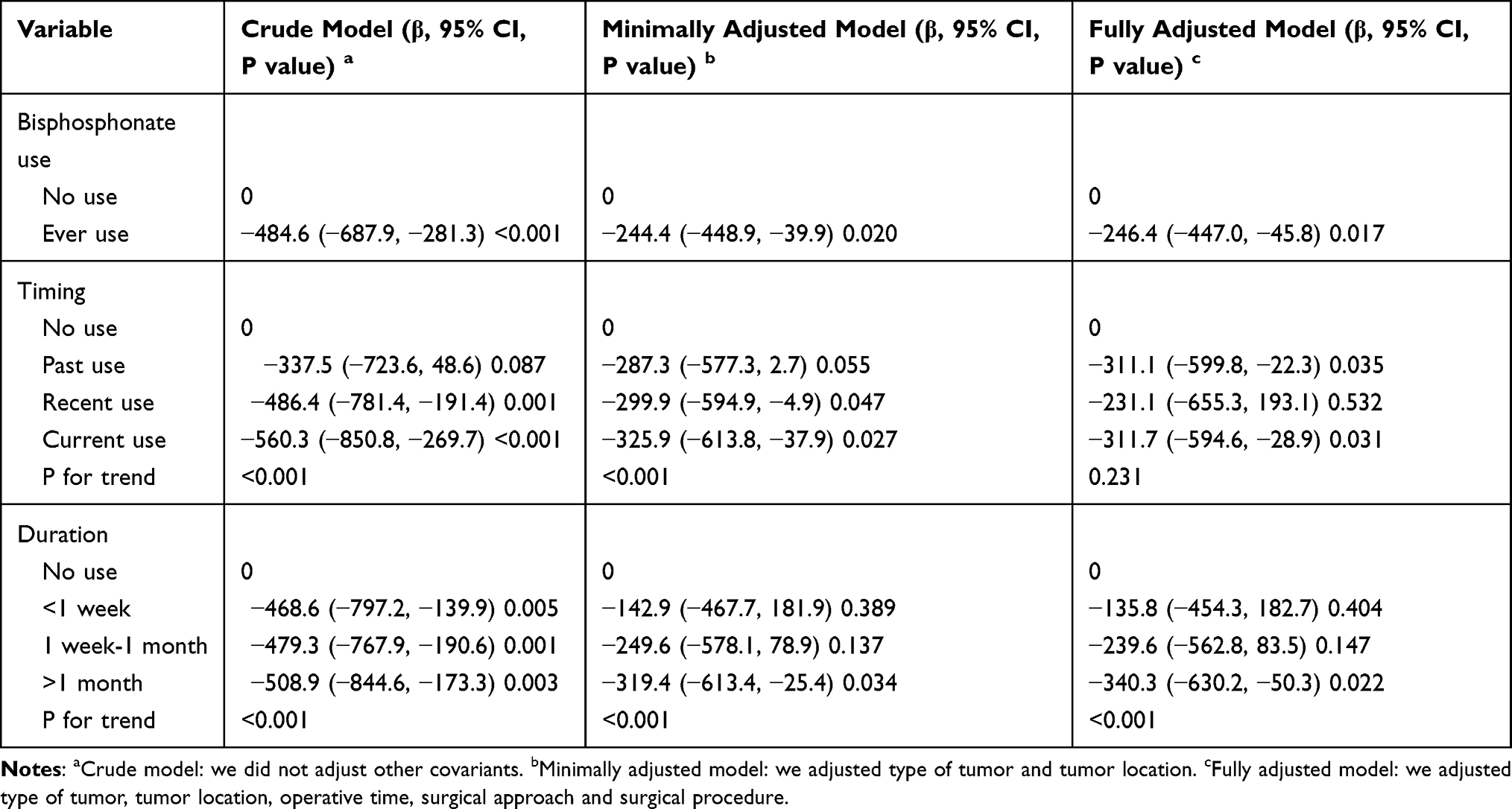 |
Table 3 Association of Any Bisphosphonate Use with the Amount of Blood Loss |
For sensitivity analysis, further analyses were performed according to the timing and duration of bisphosphonate use. In terms of timing, the crude model and minimally adjusted model showed that the closer the date of the most recent bisphosphonate use to the date of surgery, the more obvious the effect of reducing intraoperative blood loss was, and this trend was significant (p for trend <0.001). However, this trend had changed in the fully adjusted model, and the past use group and current use group seemed to have similar effects (p for trend = 0.231). In terms of duration, all three models showed the same duration–response relationship: a longer duration of bisphosphonate use accurately predicted a smaller amount of blood loss, and the longer the duration was, the more significant the effect would be (p for trend <0.001).
Subgroup Analysis
As shown in Table 4, the interaction test showed that the operative time was marginally significant (p for interaction = 0.053). The interaction test did not show statistical significance in terms of sex, age, Charlson comorbidity index, type of tumor, tumor location, number of spinal metastases, preoperative Frankel score, surgical approach, surgical type, level of decompression and level of instrumentation (p for interaction = 0.932, 0.765, 0.789, 0.554, 0.633, 0.898, 0.679, 0.352, 0.285, 0.846 and 0.428, respectively).
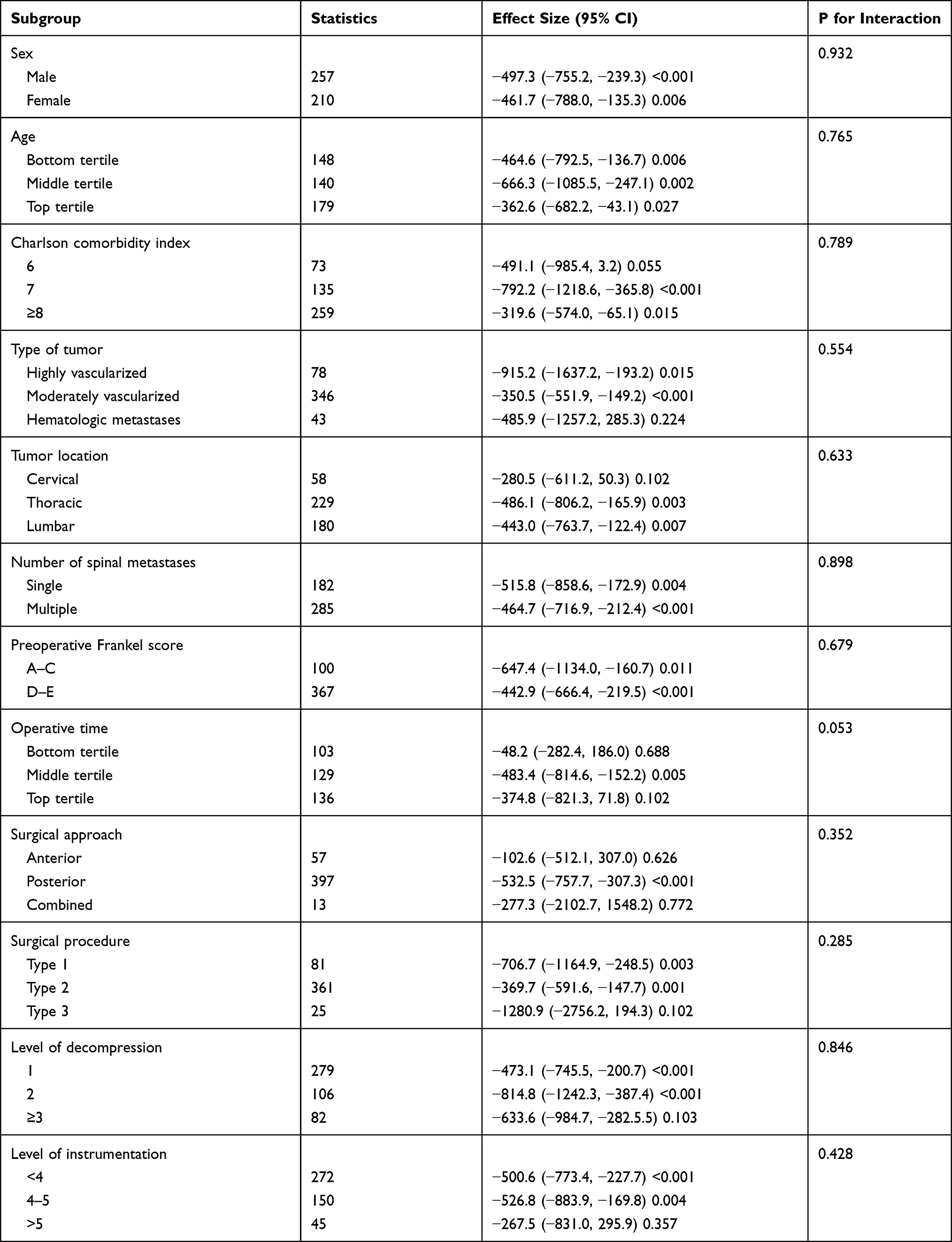 |
Table 4 Effect Size of Bisphosphonate on Blood Loss in Exploratory Subgroups |
We observed an interaction between operative time and bisphosphonate use, and the effects of bisphosphonate use on amount of blood loss were significantly different in different subgroups of operative time. The effect size in the bottom tertile group was significantly smaller than that in the other two groups (−48.2 versus −483.4 and −374.8).
Discussion
Patients with spinal metastases are often accompanied by unbearable pain, neurological deficits and spinal destabilization, which can seriously impair the quality of life and life expectancy of these cancer patients. Surgical treatment plays an important role in the multidisciplinary management of spinal metastases. However, due to the abundant blood supply of metastatic tumors, the huge amount of blood loss is one of the major difficulties faced by orthopedic oncologists.5 Excessive intraoperative bleeding will increase the risk of perioperative complications.19 We believe that reducing the amount of intraoperative bleeding can allow the operator to obtain a clearer surgical field to ensure the safe resection of the metastatic tumors. In addition, reducing the amount of bleeding can further speed up the operative process and shorten the operative time, which is essential for preventing postoperative infection and promoting postoperative recovery.
Bisphosphonates are often used in patients with spinal metastases to inhibit bone resorption, relieve unbearable pain and prevent skeletal-related events.20–22 The term skeletal-related events refer to the major complications of tumor bone disease, namely pathological fractures, need for radiotherapy, need for bone surgery and spinal cord compression. Bisphosphonates are potent inhibitors of osteoclast function. They have become a standard treatment for cancer hypercalcemia and an adjunct therapy to relieve metastatic bone pain, improve patient functioning and quality of life. However, its effect on reducing the amount of intraoperative blood loss has been rarely reported.12 Therefore, we designed and implemented a retrospective cohort study to validate this effect.
Previous literature had reported that the intraoperative blood loss of metastatic spinal tumor surgery was related to type of primary tumor, type of surgery, levels of instrumentation and decompression, operative time, tumor location, tumor volume, and preoperative embolism.6–8 A retrospective study conducted by Kumar et al reviewed 243 patients with metastatic spinal tumors who underwent surgery at the authors’ institution from 2005 to 2014 to analyze the intraoperative blood loss, the need for blood transfusion and their influencing factors.6 After adjusting of levels of instrumentation and decompression, comorbidity index, gender, age, tranexamic acid and preoperative embolism, the results of multivariate linear regression indicated that the important predictors of blood loss during surgery were primary tumor type, type of surgery and operative time. Important factors affecting blood transfusion included the primary tumor type, type of surgery, preoperative hemoglobin level, and operative time. However, this study did not include the use and frequency of bisphosphonates.
A cohort study carried out by Wu et al preliminarily verified the effectiveness of bisphosphonates in reducing intraoperative blood loss.12 They noted that use of zoledronic acid before surgery could effectively reduce the amount of intraoperative bleeding, whether for solid tumors or multiple myeloma. However, their conclusions are limited. First of all, the sample size is small (176 cases); more importantly, this study only conducted simple univariate analyses instead of multivariate regression analyses, so the adjustment of important confounding factors was not sufficient to obtain the independent effect of bisphosphonate use.
Our research has several advantages. Firstly, in order to obtain a pure study population, we excluded patients who underwent preoperative embolization or minimally invasive surgery. Compared with the general population, these excluded patients had less intraoperative bleeding. By comparing the baseline characteristics of patients with bisphosphonate use and patients without bisphosphonate use, we found that several items showed differences: operative time and tumor location. However, we used multivariate adjustment strategies to exclude the effects of these confounding factors. Secondly, in order to explore the dose–response relationship, we conducted a trend test on the timing and duration of bisphosphonate use. Finally, in order to explore potential effect modifiers and interactions, we performed subgroup analyses. The exploratory subgroup analysis is of great significance to scientific research.23 Unfortunately, the above papers did not perform subgroup analyses and interaction tests, which will hinder our explorations of the true relationship between bisphosphonate use and intraoperative blood loss.
In the current study, the fully adjusted model showed that intraoperative blood loss was 246.4mL less in patients with bisphosphonate use than in patients without bisphosphonate use. For the timing of use, the p value for trend test was 0.231, which indicated that the timing of use had no significant effect on reducing the amount of bleeding. For the duration of use, all three models validated a common conclusion: the longer the duration of use was, the better the effect of reducing intraoperative bleeding would be. Exploratory subgroup analysis showed that the effect of bisphosphonates in reducing blood loss was weaker in population with shorter operative time.
The explanations of the above conclusions may start with the mechanism of action of bisphosphonates. Previous literature have shown that bisphosphonates can inhibit the activity of osteoclasts, slow down the transformation of monocytes into osteoclasts, induce apoptosis of osteoclasts, and block the attachment of osteoclasts to host bone.20,24,25 Therefore, we reasonably speculate that the effect of reducing intraoperative blood loss may be due to the mechanism that bisphosphonates can reduce bone resorption and inhibit osteolysis and angiogenesis. This hemostatic property needs to be supported by further basic and clinical evidences. In addition, bisphosphonates have been shown to accumulate in bones and retain there for years,24 which can explain why the duration of use can affect the effect of reducing blood loss rather than timing. One possible explanation for the interaction of bisphosphonates and operative time is that the bleeding volume of operation with shorter operative time is relatively less, which may mask the effects of bisphosphonates.
Our research has some limitations. Firstly, this study is an observational study, so recall and selection bias are unavoidable. Secondly, the population of this study did not include patients who underwent preoperative embolization and minimally invasive surgery, which may prevent conclusions from being generalized to other populations. Thirdly, due to the limitation of the original data, we cannot observe the relationship between tranexamic acid and intraoperative blood loss, although some literature showed a correlation between them. Fourthly, the intraoperative blood loss in this study was obtained from the anesthetist’s medical records and records of intraoperative fluid management, there may be a deviation between the analysis using the data on the anesthesia record sheet and the real data.
Conclusion
We found that the use of bisphosphonates before surgery could reduce the amount of intraoperative blood loss during metastatic spinal tumor surgery, especially for surgery with longer operative time. The longer the duration of bisphosphonate use was, the more pronounced the effect of reducing intraoperative blood loss would be. There was no significant correlation between the timing of bisphosphonate use and the effect of reducing intraoperative blood loss. We therefore recommend that a period of preoperative bisphosphonate use is necessary and beneficial for patients with spinal metastases who need surgical treatments.
Ethical Approval and Consent of Participants
The study was conducted in accordance with the Declaration of Helsinki. The study received ethics approval from research ethics committee of Tianjin Hospital (2019-089). All participants provided voluntary written informed consent at study enrollment.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Luksanapruksa P, Buchowski JM, Zebala LP, et al. Perioperative complications of spinal metastases surgery. Clin Spine Surg. 2017;30(1):4–13. doi:10.1097/BSD.0000000000000484
2. Atkinson RA, Jones A, Ousey K, Stephenson J. Management and cost of surgical site infection in patients undergoing surgery for spinal metastasis. J Hosp Infect. 2017;95(2):148–153. doi:10.1016/j.jhin.2016.11.016
3. Quraishi NA, Rajabian A, Spencer A, et al. Reoperation rates in the surgical treatment of spinal metastases. Spine J. 2015;15(3 Suppl):S37–S43. doi:10.1016/j.spinee.2015.01.005
4. Patchell RA, Tibbs PA, Regine WF, et al. Direct decompressive surgical resection in the treatment of spinal cord compression caused by metastatic cancer: a randomised trial. Lancet. 2005;366(9486):643–648. doi:10.1016/S0140-6736(05)66954-1
5. Chen Y, Tai BC, Nayak D, et al. Blood loss in spinal tumour surgery and surgery for metastatic spinal disease: a meta-analysis. Bone Joint J. 2013;95-b(5):683–688. doi:10.1302/0301-620X.95B5.31270
6. Kumar N, Zaw AS, Khine HE, et al. Blood loss and transfusion requirements in metastatic spinal tumor surgery: evaluation of influencing factors. Ann Surg Oncol. 2016;23(6):2079–2086. doi:10.1245/s10434-016-5092-8
7. Reitz M, Mende KC, Cramer C, et al. Surgical treatment of spinal metastases from renal cell carcinoma-effects of preoperative embolization on intraoperative blood loss. Neurosurg Rev. 2018;41(3):861–867. doi:10.1007/s10143-017-0935-8
8. Schmidt R, Rupp-Heim G, Dammann F, et al. Surgical therapy of vertebral metastases. Are there predictive parameters for intraoperative excessive blood loss despite preoperative embolization? Tumori. 2011;97(1):66–73. doi:10.1177/030089161109700113
9. Morgan GJ, Child JA, Gregory WM, et al. Effects of zoledronic acid versus clodronic acid on skeletal morbidity in patients with newly diagnosed multiple myeloma (MRC Myeloma IX): secondary outcomes from a randomised controlled trial. Lancet Oncol. 2011;12(8):743–752. doi:10.1016/S1470-2045(11)70157-7
10. Lacerna L, Hohneker J. Zoledronic acid for the treatment of bone metastases in patients with breast cancer and other solid tumors. Semin Oncol. 2003;30(5 Suppl 16):150–160. doi:10.1053/j.seminoncol.2003.08.017
11. Dhillon S, Lyseng-Williamson KA. Zoledronic acid: a review of its use in the management of bone metastases of malignancy. Drugs. 2008;68(4):507–534. doi:10.2165/00003495-200868040-00010
12. Wu J, Zheng W, Tan Y, et al. Zoledronic acid may reduce intraoperative bleeding in spinal tumors: a prospective cohort study. Biomed Res Int. 2015;2015:936307.
13. Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47(11):1245–1251. doi:10.1016/0895-4356(94)90129-5
14. van Middendorp JJ, Goss B, Urquhart S, et al. Diagnosis and prognosis of traumatic spinal cord injury. Global Spine J. 2011;1(1):1–8. doi:10.1055/s-0031-1296049
15. Yang XG, Feng JT, Wang F, et al. Development and validation of a prognostic nomogram for the overall survival of patients living with spinal metastases. J Neurooncol. 2019;145(1):167–176. doi:10.1007/s11060-019-03284-y
16. von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–1457. doi:10.1016/S0140-6736(07)61602-X
17. Kernan WN, Viscoli CM, Brass LM, et al. Phenylpropanolamine and the risk of hemorrhagic stroke. N Engl J Med. 2000;343(25):1826–1832. doi:10.1056/NEJM200012213432501
18. Chen C, Dai JL. Triglyceride to high-density lipoprotein cholesterol (HDL-C) ratio and arterial stiffness in Japanese population: a secondary analysis based on a cross-sectional study. Lipids Health Dis. 2018;17(1):130. doi:10.1186/s12944-018-0776-7
19. Hu SS. Blood loss in adult spinal surgery. Eur Spine J. 2004;13(Suppl 1):S3–S5. doi:10.1007/s00586-004-0753-x
20. Tamburrelli FC, Proietti L, Scaramuzzo L, et al. Bisphosphonate therapy in multiple myeloma in preventing vertebral collapses: preliminary report. Eur Spine J. 2012;21(Suppl S1):S141–S145. doi:10.1007/s00586-012-2231-1
21. Berenson JR, Hillner BE, Kyle RA, et al. American society of clinical oncology clinical practice guidelines: the role of bisphosphonates in multiple myeloma. J Clin Oncol. 2002;20(17):3719–3736. doi:10.1200/JCO.2002.06.037
22. Berenson JR, Rosen LS, Howell A, et al. Zoledronic acid reduces skeletal-related events in patients with osteolytic metastases. Cancer. 2001;91(7):1191–1200. doi:10.1002/1097-0142(20010401)91:7<1191::AID-CNCR1119>3.0.CO;2-0
23. Vandenbroucke JP, von Elm E, Altman DG, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. Int J Surg. 2014;12(12):1500–1524. doi:10.1016/j.ijsu.2014.07.014
24. Erviti J, Alonso A, Oliva B, et al. Oral bisphosphonates are associated with increased risk of subtrochanteric and diaphyseal fractures in elderly women: a nested case-control study. BMJ Open. 2013;3(1):e002091. doi:10.1136/bmjopen-2012-002091
25. Rodan GA, Reszka AA. Bisphosphonate mechanism of action. Curr Mol Med. 2002;2(6):571–577. doi:10.2174/1566524023362104
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.