Back to Journals » Open Access Emergency Medicine » Volume 13
Bird’s-Eye View of COVID-19 Knowledge, Attitude and Practice Among Emergency Physicians in the Kingdom of Bahrain: A Cross-Sectional Study
Authors Alghanem S ![]() , Alqassim G, Abuzeyad F, Isa R, Falamarzi H
, Alqassim G, Abuzeyad F, Isa R, Falamarzi H
Received 10 June 2021
Accepted for publication 21 August 2021
Published 14 September 2021 Volume 2021:13 Pages 415—423
DOI https://doi.org/10.2147/OAEM.S323268
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hans-Christoph Pape
Salah Alghanem,1 Ghada Alqassim,2 Feras Abuzeyad,3 Ruqaya Isa,4 Horeya Falamarzi5
1Emergency Medicine, Bahrain Defence Force Hospital, West Riffa, Bahrain; 2Pediatric Emergency Medicine, Bahrain Defence Force Hospital, West Riffa, Bahrain; 3Emergency Medicine, King Hamad University Hospital, Muharraq, Bahrain; 4Emergency Medicine, Salmaniya Medical Complex, Manama, Bahrain; 5Emergency Department, Bahrain Defence Force Hospital, West Riffa, Bahrain
Correspondence: Salah Alghanem
Emergency Medicine, Bahrain Defence Force Hospital, P.O. Box: 28197, West Riffa, Bahrain
Email [email protected]
Background: Coronavirus 2019 (COVID-19) has exemplified the crucial role played by emergency physicians on the frontlines, by triaging, quarantining and treating myriad patients in time. Despite this, there exists a dearth of literature comprehensively assessing the knowledge and awareness of these health-care workers on the disease in the Kingdom of Bahrain. This study was designed to evaluate the knowledge, attitude, and practice (KAP) of emergency physicians in the Kingdom of Bahrain towards COVID-19.
Methods: This cross-sectional descriptive study included 142 emergency physicians from three major hospitals in Bahrain. A self-designed questionnaire divided into 4 parts, which consists of demographics, knowledge, attitude and practices towards COVID-19, was completed by the emergency physicians working in these hospitals. Analysis of variance (ANOVA), t-test, chi-square test, and multiple linear regression were employed to evaluate KAP scores.
Results: The mean COVID-19 knowledge and practice score was 26.29 for a maximum score of 32 suggesting an overall 82.15% correct rate on the knowledge and practice test. Multiple linear regression analysis highlighted age (p=0.038), genders (p=0.033), marital status (p=0.021), organization (p=0.032), having children (p=0.008), and continuing professional development (CPD) activity (p=0.0001) as significant predictors for knowledge and practice scores. The attitude towards the final success in controlling COVID-19 significantly differed across marital status (p=0.021), organization of participants (p=0.020) and position of participants (p=0.012), respectively.
Conclusion: Adequate knowledge, positive attitude and sufficient safe practice towards COVID-19 were observed in majority of the participants. These findings can foster development of nuanced and salient health management strategies that augment KAP so that proper control and elimination of the disease can be achieved, while prioritizing patient health and satisfaction.
Keywords: coronavirus infections, COVID-19, disease outbreaks
Introduction
Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) or novel coronavirus is the latest subset of RNA viruses that has crescendoed into a pandemic crisis. Moreover, it has simultaneously brought to fore a plethora of chinks in health-care systems as well as the indomitable spirit of physicians worldwide. This emerging respiratory infection was first discovered in December 2019, in Wuhan city, Hubei, China, and was declared as a global pandemic by the World Health Organization (WHO) on 11th March 2020.1,2 Coronaviruses constitute a large and ambiguous family of viruses that elicit a broad spectrum of symptoms and infections such as common cold, to more serious diseases, such as Middle East Respiratory Syndrome (MERS-CoV) and SARS-CoV.3 COVID-19 is characterized by rapid transmission of the virus, and occurs through close contact with an infected person.6–9 Disease progression revolves around respiratory illness (like flu) with main clinical symptoms such as fever, dry cough and dyspnea.4,5 This new outbreak has begotten undue hysteria partly due to misinformation and falsified news. The data surrounding the biology, epidemiology, and clinical characteristics, however, are evolving, thus making this a moving target.
Asymptomatic people can be contagious as the virus is mainly transmitted via respiratory droplets and has been detected in the respiratory secretions of such patients.10 Recent epidemiological and experimental evidences implicate airborne transmission of Covid-19 virus via aerosols as a potential route for spreading the disease depending upon the viral load.11–13 Reverse transcription polymerase chain reaction (RT-PCR) from a nasopharyngeal swab is the standard method of diagnosis. At present, there is no specific antiviral treatment or vaccine for COVID-19. Management includes supportive care, treatment of symptoms, isolation, and experimental measures.
The epidemics of COVID-19 has been recorded in over 216 countries, territories, and areas with more than 12 million confirmed cases and 5,68,573 deaths reported globally.14 Following the WHO declaration, countries around the globe including Kingdom of Bahrain have been relying on various strategies to combat and contain this pandemic. Following the confirmation of its first case of COVID-19 on 21 Feb 2020, the Bahrain government has been watchful in monitoring the situation and adopting specific measures that were in line with the WHO guidelines in dealing with the outbreak. The cause of the infection is novel, and the extent of the disease is unknown.
The battle against COVID-19 is an ongoing one, across the world. As emergency services are lifelines of healthcare in times of a pandemic disaster, the responsibility of emergency staff has increased tremendously. A burgeoning patient pool and failure of health-care system to retort to the increasing need of the patients during these testing times has led to an upsurge of negative emotions among emergency physicians. Physicians themselves are required to constantly update their knowledge on COVID-19 to assuage patient concerns. However, this knowledge must be supplemented with well-planned communication and management strategies to ensure the best outcome possible for each patient. Some hospitals have reportedly adopted an array of capacity-building avenues including TV, videos, podcasts, online seminars and social media for all categories of health-care personnel.15 Although several studies have been conducted in Asian countries indicating high levels of COVID-19 knowledge among the general population, there is very scarce literature available examining the knowledge and awareness in regard to COVID-19 among emergency physicians in different regions of the world, especially Kingdom of Bahrain. Therefore, this study was designed to investigate the KAP of emergency physicians towards COVID-19 in the Kingdom of Bahrain so as to improve awareness and attitudes among emergency physicians in recommending any remedial measures and additional interventions.
Methods
Study Design
This cross-sectional descriptive study was conducted in the months of May and June 2020 at three selected hospitals in the Kingdom of Bahrain among 142 emergency physicians after obtaining a written informed consent. The study was done after obtaining approval from the National COVID-19 Committee and from the Research & Research Ethical Committee at the BDF Hospital. The minimum sample size representing the population which should be reached was calculated to be 140 with a prevalence of 90%. The power of 80% with a confidence interval of 95% and precision of 5% with an error set at 95% was considered.
Patient and Public Involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Data Collection
The respondents were recruited on ease of accessibility based on the convenience sampling approach. A comprehensive questionnaire was carefully developed based on verified literature with suitable modifications and additions. Following that, it was scrutinized in terms of its integrity, simplicity and overall content, by three consultants hailing from the Emergency Medicine specialization. A pilot study on a small sample (n= 5) of emergency physicians was undertaken to assess the intelligibility and reliability of the questionnaire. Subsequently, the questionnaire as a research instrument for this study was further validated by an expert in the field of infectious diseases who was also a member of the Bahrain National COVID-19 committee. After thorough deliberation, the expert’s suggestions were incorporated and this self-administrable questionnaire was distributed to the participants by email for data collection. The cover page of the questionnaire included a short introduction regarding the objectives, procedures, the voluntary nature of participation, declarations of confidentiality and anonymity. The structured questionnaire was categorized into four parts. The first part consisted of respondent’s demographic information. The second part classified the respondents’ knowledge on COVID-19 transmission source, etiology, incubation period, symptoms, risk group, and consequences by the use of dichotomous questions with Yes or No as options. The third part evaluated the health-care worker’s attitude towards COVID-19 in which their response was assessed through 5-point Likert scale of agreement wherein, the responders specify their level of agreement to a statement typically in five points: (1) strongly disagree; (2) disagree; (3) neither agree nor disagree; (4) agree and (5) strongly agree.16 The last part depicted the practice statement of respondents regarding COVID-19 using a series of 11 Yes/No questions.
Statistical Analysis
Data were analyzed using SPSS software. Percentage mean and standard deviation (SD) were used to present data to evaluate the demographic variables. KAP scores of participants according to demographic characteristics were analyzed using t-test, Chi-square test and analysis of variance (ANOVA). Multivariable linear regression analysis was conducted to identify factors associated with knowledge. P-value of <0.05 was considered as significant.
Results
The distribution of participants based on their demographic characteristics is depicted in Table 1. Majority of the subjects were in the age range of 35–44 years (38.7%). A male predominance was noted (66.2%). With respect to the experience, most of them had >5 years of experience in Emergency medicine and 59.9% of them participated in continuing professional development (CPD) activity about COVID-19. Organization circulars/Guidelines were found to be the main source of knowledge on COVID-19 (90.8%) (Supplementary Figure 1).
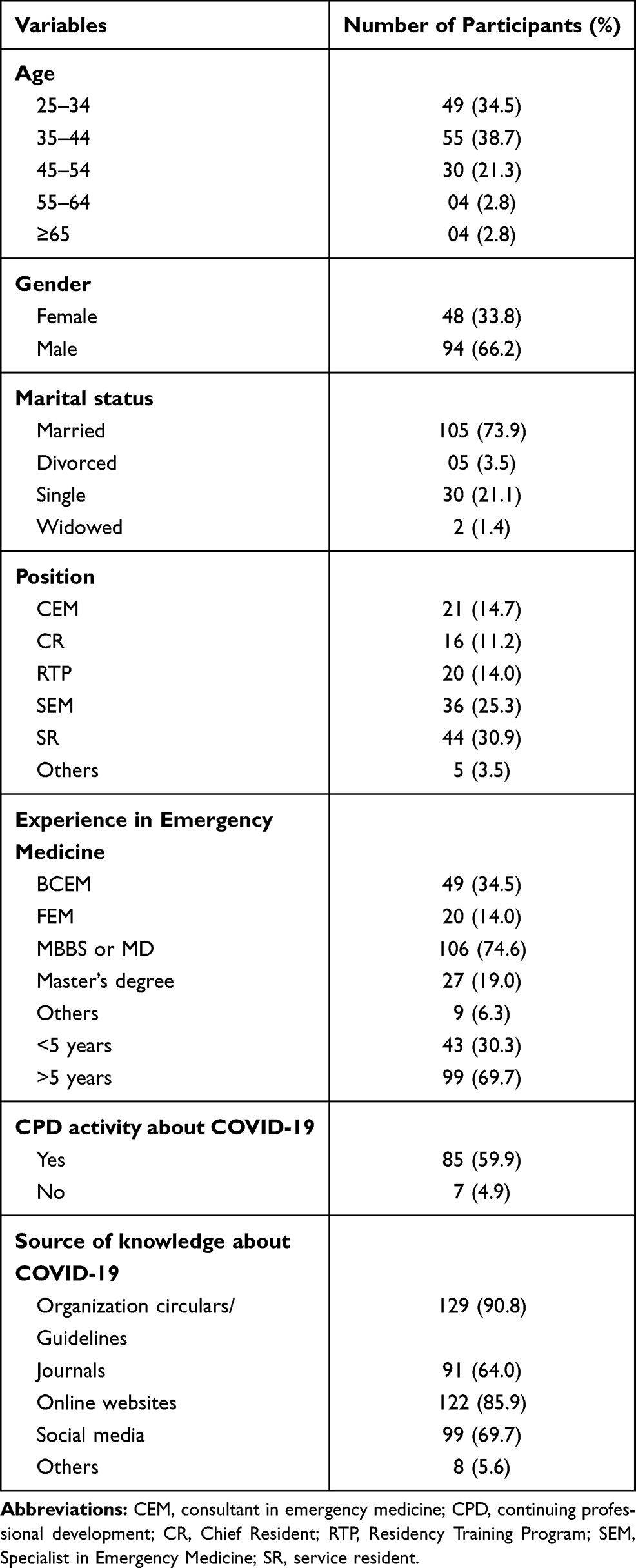 |
Table 1 Demographic Characteristics of Participants |
Based on the statements noted, more than 90% of the participants had correct knowledge about the main symptoms (fever and cough) of COVID-19 and transmission routes of the virus. In addition to this, majority of participants had good knowledge about patients who were at high risk such as elderly patients (96.4%), followed by patients on steroids (63.3%), pregnant females (43.6%), and children (23.2%). Furthermore, 93.6% of participants realized that people who had travel history should be immediately isolated for 14 days even if the test result was negative. Very limited number of participants (9.8%) felt that COVID-19 has been commonly reported in children and 91.5% of the participants felt that the patients were contagious even if they were asymptomatic. Most of the participants (70.4%) were of an opinion that COVID-19 was of a zoonotic origin. About 90.8% felt that the incubation period is between 1 and 14 days. Also, more than half of the participants (65.4%) were of the opinion that leukopenia and elevated CPK are associated with poor outcomes among cases of COVID-19.
With respect to attitude statements about COVID-19, majority of the participants (73%) agreed that this disease could be successfully controlled. In addition, majority of participants (72%) agreed to provide care for COVID-19 patients. Furthermore, most of the participants were inclined towards working in COVID-19 treatment/isolation center. In terms of practice statements about COVID-19, more than 90% of the participants were aware of the local guidelines, use of sanitizer and use of personal protective equipment (PPE). In addition, most of the participants were also aware of the standard precautions to be applied while dealing with COVID-19 patients and also were aware of the order of put and take off PPEs after use.
Various demographic characteristics were considered, with respect to the distribution of participants in terms of knowledge, attitude, and practice statements about COVID-19. Participants in the age group of 35–44 had higher scores as compared to other age groups with regard to practice statements (p=0.021).
Regarding the marital status, married participants had higher knowledge scores (p=0.016), attitude scores (p=0.0087) and practice scores (p=0.013) as compared to divorced, single and widowed. With respect to organization, participants from King Hamad University Hospital (KHUH) had highly significant knowledge score (p=0.026) and attitude scores (p=0.007) as compared to other organizations. In terms of position, consultant in emergency medicine and others which included registrar and senior resident had high practice scores (p=0.045) compared to other positions. Based on emergency medicine experience, participants with >5 years of experience had significantly higher practice scores (p=0.014). Emergency physicians who attended CPD activity had significantly higher knowledge scores (p < 0.001) and practice scores (p=0.000024) compared to those who did not attend any CPD activity (Table 2).
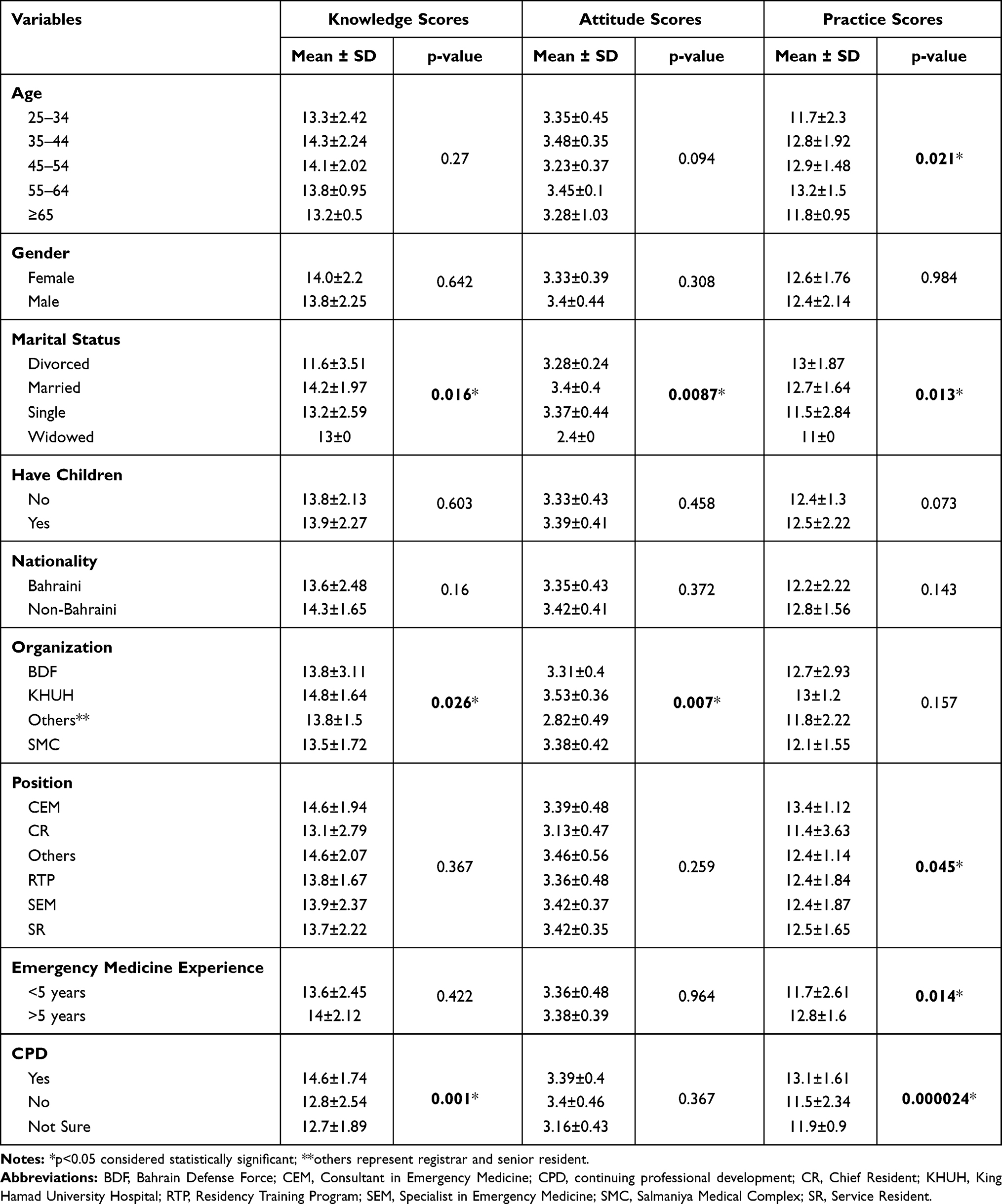 |
Table 2 Distribution of Participants in Terms of Knowledge, Attitude, and Practice Statements About Covid-19 |
The mean COVID-19 knowledge and practice score was 26.29 for a maximum score of 32 suggesting an overall 82.15% correct rate on the knowledge and practice test. Knowledge and practice scores significantly differed across age, genders, marital status, and education levels, etc. Multiple linear regression analysis showed that age group of 35–44 (p=0.038); male gender (p=0.033); marital status of married (p=0.021); participants having children (p=0.008); working in KHUH organization (p=0.032); and those who attended CPD activity about COVID-19 (p=0.0001) were significantly associated with higher knowledge and practice score. Overall, these variables were observed to be significant predictors for knowledge and practice scores (Table 3).
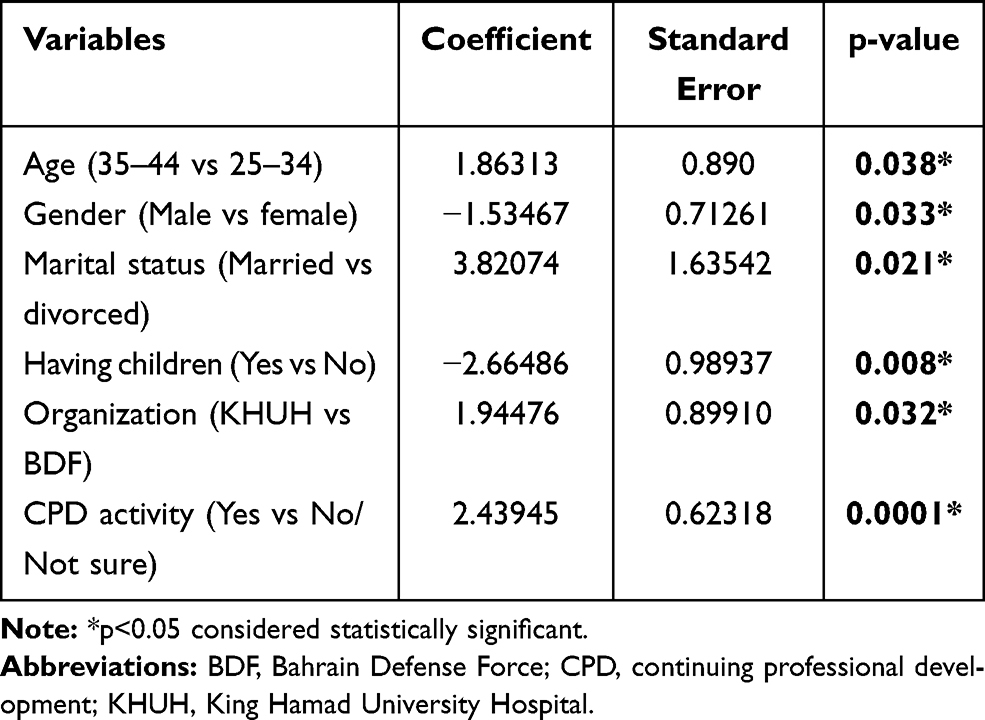 |
Table 3 Results of Multiple Logistic Regression Analysis on Factors Significantly Associated with Higher Knowledge Score of Covid-19 by Demographic Variables |
The attitude towards the final success in controlling COVID-19 significantly differed across marital status (p=0.021), organization of participants (p=0.020) and position of participants (p=0.012). Participants who reported “Disagree” and “Neither agree nor disagree” had significantly lower attitude scores than those reporting “Agree” and “strongly agree” (Table 4).
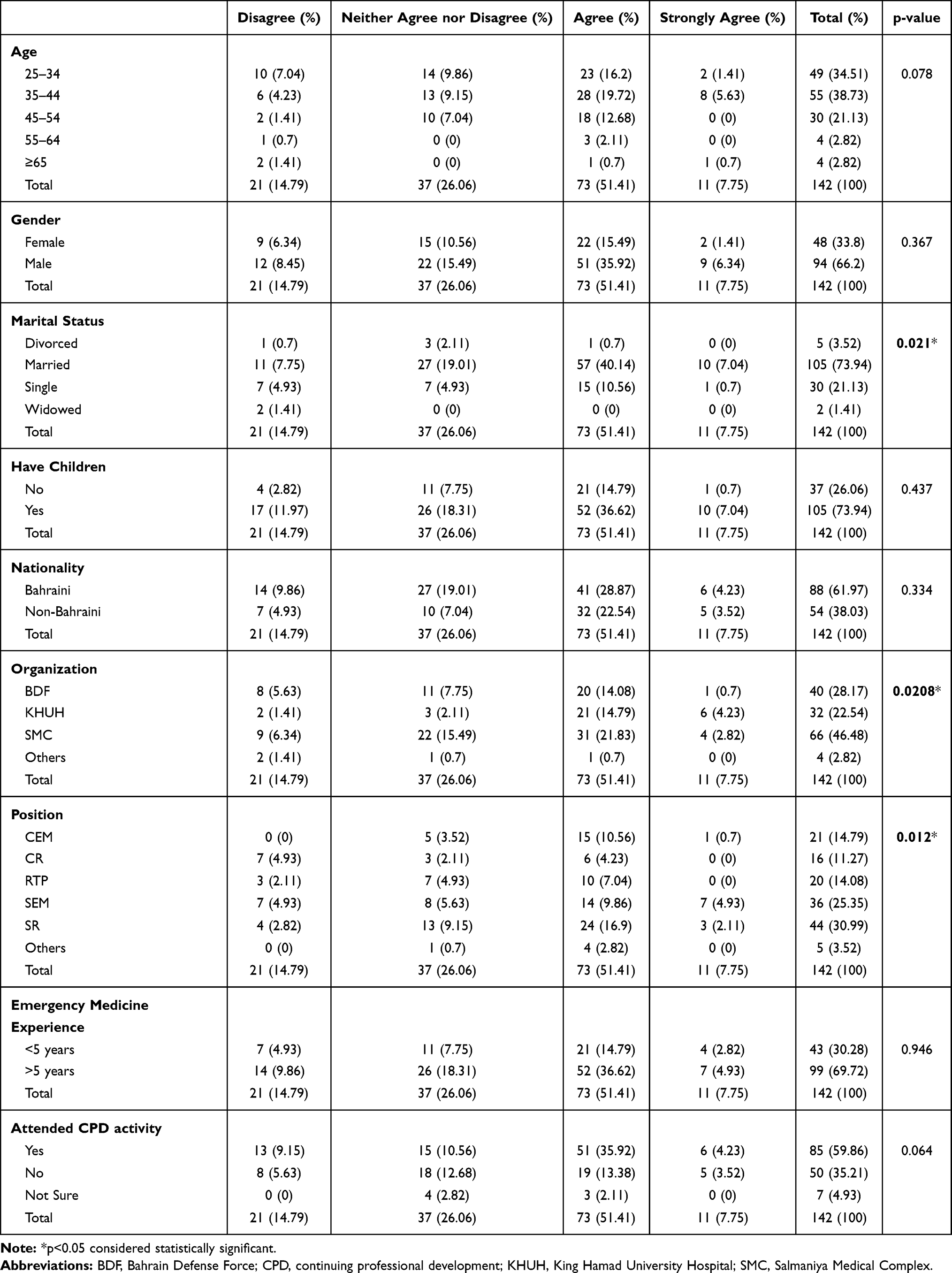 |
Table 4 Attitude Towards Covid-19 by Demographic Variables |
Discussion
COVID-19 pandemic, an infectious disease poses a significant threat to public health has brought the entire world to a standstill. Researchers all over the world are working extensively on the therapies and vaccines against the virus. KAP of the public is crucial towards the containment of this disease and in implementing directives such as social distancing, isolation, maintaining personal and community hygiene to fight against COVID-19. Accordingly, this study was designed to gauge the KAP of Bahraini emergency physicians through a questionnaire survey.
In the present study, depending on the knowledge scores of participants, an overall correct rate of 82.5% demonstrated that most of the participants were knowledgeable about this pandemic. Our results were slightly similar to the previous study regarding the COVID-19 KAP scores in China which also showed an overall correct rate of 90% knowledge among Chinese residents.17 Another study conducted by Al-Hanawi et al among public achieved a mean of 81.6% in the knowledge questionnaire which was in harmony with the current study.18 This may be due to participant characteristics, as 99% of participants in this study had experience of >5 years in emergency medicine.
Significant predictors of participant’s knowledge were age, marital status, organization of the physicians, position of physicians, emergency medicine experience, and CPD activity. Maheshwari et al, in their study, concluded that no significant difference was observed in relation to all demographic variables.19 The significance of these predictors in this study could be attributed to the fact that emergency physicians with experience of >5 years and those who were aged in the range of 35–44 years were more knowledgeable about emerging infectious diseases. Also, married participants depicted significantly higher KAP scores which could be because married people have more bonding towards their family and being an emergency physician, they cared about the well-being of their families as well, apart from the patients. The significance of organization, position of physicians and CPD activity towards KAP could be because of their vast knowledge and experience in the field of medicine.
Concerning attitudes, participants depicted an optimistic attitude towards controlling COVID-19 in the present study. Marital status, organization and position of the participants were observed to be significant predictors in this study. This finding was almost similar to the study conducted in Chinese residents, where participants were convinced that COVID-19 is curable, and their country will combat the disease successfully.16 Another population-based survey in Iran also provided similar results with 68% of participants believing that COVID-19 is a curable disease.20 A study conducted by Azlan et al also reported 83.1% of participants with positive attitudes towards successful control of COVID-19.21 Significant predictors of participant attitude towards COVID-19 can be attributed to the experience and high knowledge about COVID-19 which translates into safe practices during the outbreak of this pandemic.
The results of the present study can help in the development of public health policies targeting specific groups with low KAP and increase their KAP through appropriate, well planned, and tailored strategies. Consequently, health promotion activities are vital in improving KAP towards COVID-19 and therefore, further extensive interventional studies are needed to arrive at more conclusive results.
The study had some limitations such as the sample sizes being restricted to emergency physicians and hence the results cannot be applied in general to physicians. Another limitation of the study could be the misinterpretation of information and chances of errors due to the self-answered questionnaire by the participants. Therefore, more studies are warranted in future among all frontline health-care workers to investigate KAP towardsCOVID-19 rather than considering only a section of health-care professionals for better understanding of the arising pandemic.
Conclusion
The present findings suggest that emergency physicians demonstrated good knowledge, positive attitude and reasonable practice skills to combat COVID-19. Furthermore, based on the significant positive association between knowledge, attitude, and practice scores in our study, health education programs, particularly targeting lower knowledge individuals regarding COVID-19, is essential for encouraging positive attitude and safe practices. Hopefully, by increasing knowledge among the public health policymakers, and the general population, optimistic control and elimination of the disease can be anticipated.
Abbreviations
ANOVA, analysis of variance; BDF, Bahrain Defense Force; CEM, consultant in emergency medicine; CR, Chief Resident; CPD, continuing professional development; COVID-19, Coronavirus 2019; KAP, Knowledge, Attitudes, and Practices; KHUH, King Hamad University Hospital; MBBS, Bachelor of Medicine and Bachelor of Surgery; MERS-CoV, Middle East Respiratory Syndrome; RTP, Residency Training Program; RT-PCR, Reverse transcription polymerase chain reaction; SARS-CoV-2, Severe Acute Respiratory Syndrome Coronavirus 2; SD, standard deviation; SEM, Specialist in Emergency Medicine; SMC, Salmaniya Medical Complex; SR, service resident; WHO, World Health Organisation.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Research & Research Ethical Committee at the Bahrain Defence Force Hospital (BDF/R&REC/2020-434). Informed written consent was obtained from all the physicians. All collected data was anonymized. The data was stored electronically, with only the principal investigator having access to view the stored data.
Acknowledgments
Special thanks to Dr. Manaf Alqahtani – Associate Professor of Medicine - RCSI, Consultant Infectious Diseases & Clinical Microbiologist, Head of Microbiology Lab and Infection Control Unit. BDF Hospital, Member of the National COVID-19 Committee - Kingdom of Bahrain.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests.
References
1. Wu F, Zhao S, Yu B, et al. A new coronavirus associated with human respiratory disease in China. Nature. 2020;579(7798):265–269. doi:10.1038/s41586-020-2008-3
2. World Health Organization. WHO announces COVID-19 outbreak a pandemic. Available from: http://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/news/news/2020/3/who-announces-covid-19-outbreak-a-pandemic.
3. Zhou P, Yang X-L, Wang X-G, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. 2020;579(7798):270–273. doi:10.1038/s41586-020-2012-7
4. Chan JF-W, Yuan S, Kok K-H, et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster. Lancet. 2020;395(10223):514–523. doi:10.1016/S0140-6736(20)30154-9
5. Riou J, Althaus CL. Pattern of early human-to-human transmission of Wuhan 2019 novel coronavirus (2019-nCoV), December 2019 to January 2020. Eurosurveill. 2020;25(4):2000058. doi:10.2807/1560-7917.ES.2020.25.4.2000058
6. Shereen MA, Khan S, Kazmi A, Bashir N, Siddique R. COVID-19 infection: origin, transmission, and characteristics of human coronaviruses. J Adv Res. 2020;24:91–98. doi:10.1016/j.jare.2020.03.005
7. Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus–infected pneumonia. N Engl J Med. 2020;382(13):1199–1207. doi:10.1056/NEJMoa2001316
8. Parry J. China coronavirus: cases surge as official admits human to human transmission. BMJ. 2020;368:m236. doi:10.1136/bmj.m236
9. Phan LT, Nguyen TV, Luong QC, et al. Importation and human-to-human transmission of a novel coronavirus in Vietnam. N Engl J Med. 2020;382(9):872–874. doi:10.1056/NEJMc2001272
10. Lum LHW, Tambyah PA. Outbreak of COVID-19 – an urgent need for good science to silence our fears? Singapore Med J. 2020;61(2):55–57. doi:10.11622/smedj.2020018
11. World Health Organization. Coronavirus disease (COVID-2019) situation reports. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports/.
12. van Doremalen N, Morris DH, Holbrook MG, et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N Engl J Med. 2020;382(16):1564–1567. doi:10.1056/NEJMc2004973
13. Liu Y, Ning Z, Chen Y, et al. Aerodynamic analysis of SARS-CoV-2 in two Wuhan hospitals. Nature. 2020;582(7798):557–560. doi:10.1038/s41586-020-2271-3
14. World Health Organization. Coronavirus disease (COVID-2019) situation reports. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200713-covid-19-sitrep-175.pdf?sfvrsn=d6acef25_2.
15. Ma X, Li S, Yu S, et al. Emergency management of the prevention and control of novel coronavirus pneumonia in specialized branches of hospital. Acad Emerg Med. 2020;27(4):312–316. doi:10.1111/acem.13958
16. Slovic P. Perception of risk. Science. 1987;236(4799):280–285. doi:10.1126/science.3563507
17. Zhong B-L, Luo W, Li HM, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Boil Sci. 2020;16(10):1745–1752. doi:10.7150/ijbs.45221
18. Al-Hanawi MK, Angawi K, Alshareef N, et al. Knowledge, attitude and practice toward Covid-19 among the public in the Kingdom of Saudi Arabia: a cross-sectional study. Front Public Health. 2020;8:1–10. doi:10.3389/fpubh.2020.00217
19. Maheshwari S, Gupta PK, Sinha R, Rawat P. Knowledge, attitude, and practice towards coronavirus disease 2019 (COVID-19) among medical students: a cross-sectional study. J Acute Dis. 2020;9(3):100–104. doi:10.4103/2221-6189.283886
20. Erfani A, Shahriarirad R, Ranjbar K, Mirahmadizadeh A, Moghadami M. Knowledge, attitude and practice toward the Novel Coronavirus (COVID-19) outbreak: a population-based survey in Iran. Bull World Health Organ; March 30, 2020. Available from: https://www.who.int/bulletin/online_first/COVID-19/en/.
21. Azlan AA, Hamzah MR, Sern TJ, Ayub SH, Mohamad E. Public knowledge, attitudes and practices towards COVID-19: a cross-sectional study in Malaysia. PLoS One. 2020;15(5):e0233668. doi:10.1371/journal.pone.0233668
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.