Back to Journals » Infection and Drug Resistance » Volume 19
Biosample Donation Intentions of Patients with Infectious Disease Based on the Theory of Planned Behavior: A Qualitative Study
Authors Wang W, Pan M, Liu Y, Wang J, Zhou J, Zhao Y, Xie P, Dong H, Yi C, Sun H
Received 30 September 2025
Accepted for publication 11 January 2026
Published 20 March 2026 Volume 2026:19 571376
DOI https://doi.org/10.2147/IDR.S571376
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Oliver Planz
Wenhui Wang,1,* Mingyue Pan,2,* Yan Liu,3 Jin Wang,3 Jin Zhou,1 Yunli Zhao,1 Peiyi Xie,4 Hui Dong,1 Changhua Yi,1 Hui Sun5
1Clinical Research Center, The Second Hospital of Nanjing, Affiliated to Nanjing University of Chinese Medicine, Nanjing, Jiangsu, 210003, People’s Republic of China; 2Department of Hepatopathy, The Second Hospital of Nanjing, Affiliated to Nanjing University of Chinese Medicine, Nanjing, Jiangsu, 210003, People’s Republic of China; 3Department of Tuberculosis, The Second Hospital of Nanjing, Affiliated to Nanjing University of Chinese Medicine, Nanjing, Jiangsu, 210003, People’s Republic of China; 4Phase I Clinical Research Center, The Second Hospital of Nanjing, Affiliated to Nanjing University of Chinese Medicine, Nanjing, Jiangsu, 210003, People’s Republic of China; 5Department of Nursing, The Second Hospital of Nanjing, Affiliated to Nanjing University of Chinese Medicine, Nanjing, Jiangsu, 210003, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hui Sun, Department of Nursing, The Second Hospital of Nanjing, Affiliated to Nanjing University of Chinese Medicine, No. 1-1, Zhongfu Road, Gulou District, Nanjing, Jiangsu, 210003, People’s Republic of China, Tel +86 13376084696, Email [email protected] Changhua Yi, Clinical Research Center, The Second Hospital of Nanjing, Affiliated to Nanjing University of Chinese Medicine, No. 1-1, Zhongfu Road, Gulou District, Nanjing, Jiangsu, 210003, People’s Republic of China, Tel +8615818178091, Email [email protected]
Objective: To explore the biosample donation intentions and its influencing factors of infectious disease patients based on the Theory of Planned Behavior so as to provide references for formulating publicity strategy to improve patients’ awareness of donating biosamples and assist in the construction of infectious disease biobank.
Methods: By applying the phenomenological research method of qualitative research and using purposive sampling, 15 patients with infectious diseases who were hospitalized in a infectious disease hospital in Jiangsu Province from February to April 2025 were selected for semi-structured interviews. The interview data were collated and analyzed using Nvivo12.0 software and Colaizzi analysis methods.
Results: A total of 3 themes and 8 sub-themes were extracted. The themes including: patients with infectious diseases had different attitudes towards biosample donation intentions (positive attitude for donating behaviour were meaningful, negative attitude for no benefit to themselves, and neutral attitude for the unknown risks of donating behaviour); driven by multifaceted subjective norms (family support, medical staff intervention, and social concepts); the perceptual behavioral control was limited (multiple concerns such as privacy protection, research institutions, informed parties, types of donated samples, feedback on research results, costs and compensation, etc).
Conclusion: The biosample donation intention of infectious disease patients is influenced by multiple factors. Appropriate and targeted publicity strategies should be formulated, such as differentiated health education for patients with positive/negative/neutral attitudes, and leveraging the guiding role of family members and healthcare providers to enhance patients’ recognition of biosample donation behaviour, give more play to the potential driving role of family, medical staff and social support, explore reasonable and effective informed consent model therefore to assist in the scientific research of infectious diseases and the construction of infectious disease biobank.
Keywords: theory of planned behavior, infectious disease, directed tissue donation, behavioral intention, qualitative research
Introduction
Throughout history, infectious diseases have posed a persistent and severe threat to human health and social development. Before the COVID-19 pandemic, infectious diseases accounted for approximately 30% of global deaths annually1 and nearly half of all deaths in developing countries.2 During the pandemic, the incidence and mortality of certain infections that had been partially controlled, such as HIV and tuberculosis, rebounded.3,4 Meanwhile, newly emerging infectious diseases continue to be identified each year.5 With their wide dissemination, rapid transmission, and profound societal impact, infectious diseases remain a central, complex, and pressing challenge in global public health.
The establishment of infectious disease biobanks as core infrastructure supporting the investigation of infection patterns, disease mechanisms, therapeutic development, and preventive strategies has become an important global public health initiative.5 However, biosample recruitment represents a critical bottleneck in the development of such biobanks. A cross-sectional survey conducted by Ding et al6 reported that the consent rate for biosample donation among patients with infectious diseases (26.7%) was significantly lower than that of patients with non-infectious diseases (70.4%). This striking discrepancy suggests that decision-making among patients with infectious diseases may be influenced by unique factors. Yet, the study did not examine in depth the distinct concerns of these patients, particularly those stemming from disease transmissibility and stigma. Similarly, a survey by Gao et al7 revealed that public awareness of biobanks in China is generally low, with only a minority of respondents familiar with donation procedures and significance. However, that study did not specifically target patients with infectious diseases, leaving their cognitive characteristics and decision-making processes unexplored.
The Theory of Planned Behavior (TPB),8–10 originating from social psychology, provides a framework for explaining and predicting individual behaviors. According to TPB, behavioral intention is the decisive determinant of action and is shaped by three factors: attitude toward the behavior, subjective norms, and perceived behavioral control. A stronger positive attitude, supportive subjective norms, and greater perceived behavioral control are associated with stronger behavioral intentions and, consequently, a higher likelihood of action. Methodologically and theoretically, TPB has been widely applied as a classic model for explaining individual behavioral intentions, including in studies of biosample donation among patients with non-infectious diseases such as cancer and psychiatric disorders. For example, Sun et al11 employed TPB to investigate donation willingness among psychiatric patients, identifying privacy protection and financial compensation as key determinants. Domaradzki et al12 emphasized the importance of trust in healthcare professionals in shaping donation attitudes among patients with cancer. Nevertheless, several critical gaps remain in the existing literature: (1) Population limitations: Prior research has predominantly focused on patients with non-infectious diseases, with insufficient attention to the unique factors influencing patients with infectious diseases, such as concerns about biosample infectivity and the heightened risk of discrimination following privacy breaches. (2) Methodological limitations: Most studies have relied on quantitative approaches (eg, surveys), with little qualitative research to capture patients’ lived experiences, deeper concerns, and nuanced decision-making processes (eg, the specific ways family support influences donation willingness). (3) Theoretical limitations: Applications of TPB in the context of infectious disease biosample donation have largely remained at the macro-level dimensions of “attitude-subjective norms-perceived behavioral control”. Sub-dimensions tailored to infectious disease contexts (eg, acceptance of different biosample types or preferences regarding the source of information disclosure) have not been elaborated. This lack of refinement constrains the development of targeted intervention strategies.
This research introduces three major innovations: (1) Perspective: For the first time, TPB was applied as the guiding framework to focus specifically on patients with infectious diseases, a population largely overlooked in prior studies. By employing a qualitative lens, this study addresses the lack of attention to the distinctive concerns of this group. (2) Methodology: A phenomenological qualitative design was adopted, integrating the software NVivo 12.0 with Colaizzi’s method of analysis. This approach enabled in-depth exploration of patients’ authentic understandings of biobanks, their attitudes toward donation (positive, negative, or neutral, along with underlying reasons), and their decision-making logic (eg, the influence pathways of family and healthcare professionals). In doing so, it complements the limitations of prior quantitative research. (3) Content: The three TPB dimensions were further refined into context-specific subthemes relevant to infectious disease settings. For example, “social perceptions and stigma” under subjective norms, and “acceptance of different biosample types” under perceived behavioral control. These refinements provide more granular empirical evidence to support the development of tailored informed consent models and educational strategies for patients with infectious diseases.
Guided by TPB, a semi-structured interview framework was designed to investigate the authentic perceptions and determinants of biosample donation intentions among patients with infectious diseases, thereby enhancing patient awareness of biobank participation and providing a reference for the construction of infectious disease biobanks.
Subjects and Methods
Study Subjects
A purposive sampling strategy was employed, guided by the principle of maximum variation, to recruit patients hospitalized between February and April 2025 at a tertiary infectious disease specialty hospital in Jiangsu Province. Semi-structured qualitative interviews were conducted with patients representing diverse transmission routes, educational backgrounds, ages, sexes, and disease durations. Inclusion criteria were as follows: (1) diagnosis consistent with China’s statutory standards for infectious diseases; (2) age ≥18 years; (3) good communication skills and active cooperation; (4) voluntary participation with informed consent. Exclusion criteria were as follows: (1) severe complications of the heart, lungs, kidneys, or other major organs, or impaired consciousness; (2) severe psychiatric disorders. The study protocol was approved by the hospital’s ethics committee (Approval No. 2025-LS-ky-015). All participants volunteered and signed written informed consent. All participants provided written informed consent, which explicitly included consent for the publication of anonymized responses and direct quotations from interview transcripts. Sample size was determined by the principle of information saturation, ie, recruitment ceased once no new themes emerged. A total of 15 patients were interviewed, including 8 men, with a mean age of 41.2 ± 13.65 years. Diagnoses included chronic hepatitis B (n = 6), HIV/AIDS (n = 4), pulmonary tuberculosis (n = 3), syphilis (n = 1), and hepatitis C (n = 1). Participants were anonymized and labeled P1–P15. Additional demographic details are shown in Table 1.
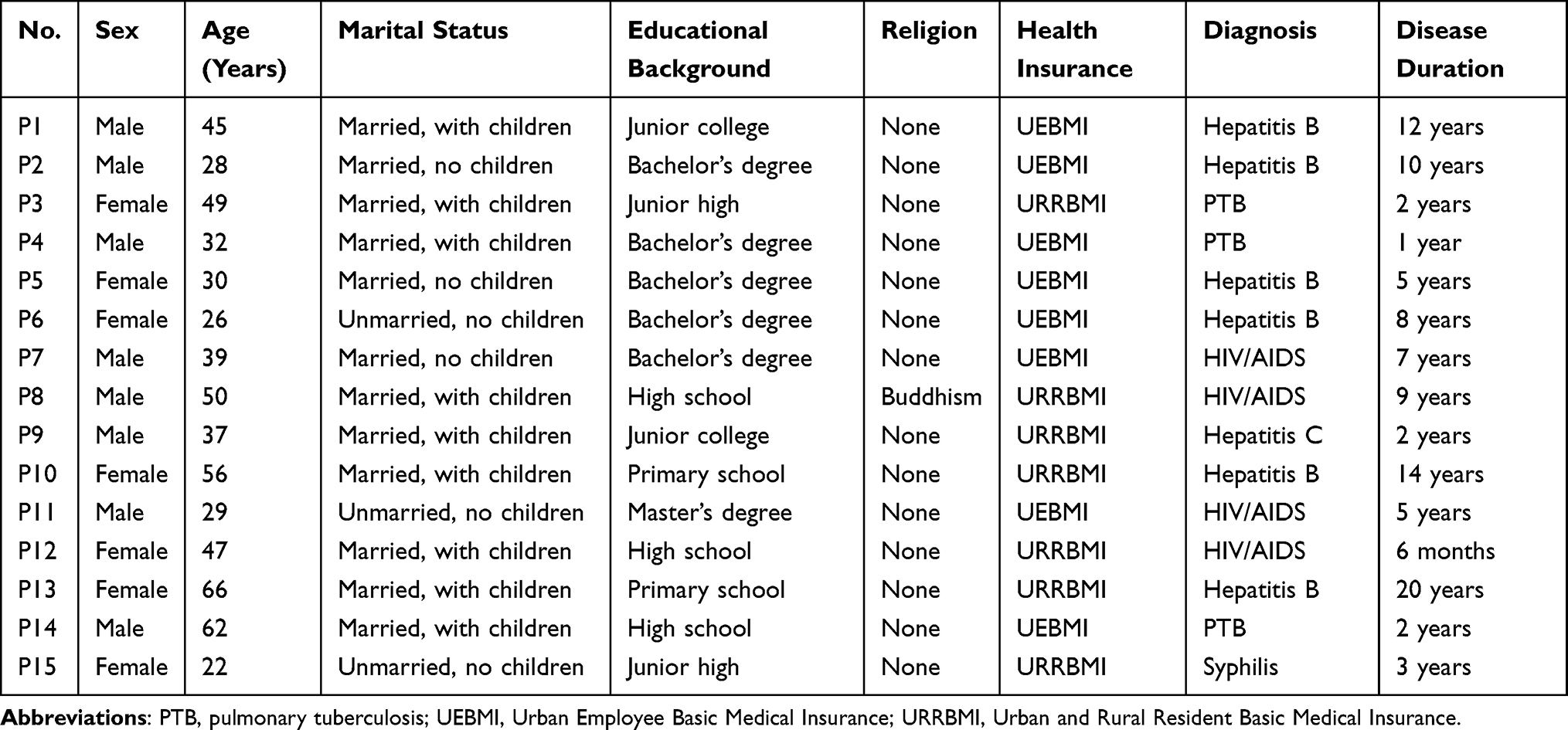 |
Table 1 Demographic and Clinical Characteristics of Participants (n = 15) |
The distribution of disease types in the sample was consistent with the overall composition of inpatients at the study site during the same period (February–April 2025). Hospital statistics indicated that hepatitis B accounted for 38.2% of inpatients with infectious diseases (reflecting the higher hospitalization frequency of patients requiring regular liver function monitoring and antiviral regimen adjustments). HIV/AIDS and tuberculosis accounted for 25.7% and 19.1%, respectively, while syphilis and hepatitis C each accounted for 8.5%, as these conditions are most often managed on an outpatient basis. To ensure representativeness, purposive sampling prioritized inclusion of patients with different transmission routes, including bloodborne (hepatitis B, HIV, hepatitis C), respiratory (tuberculosis), and sexually transmitted (syphilis), so as to minimize bias arising from perspectives specific to a single mode of transmission. This study adopted a purposive sampling strategy to cover major infectious disease types with different transmission routes (bloodborne, respiratory, sexually transmitted) to ensure thematic representativeness. As a qualitative exploratory study, the sample size was determined by information saturation (no new themes emerged after 15 interviews), which is consistent with the methodological norms of phenomenological research. However, the small sample size and limited representation of low-hospitalization diseases (eg, syphilis, hepatitis C) are acknowledged as limitations, which will be addressed in future studies.
Methods
Development of the Interview Guide
Based on the study objectives and a review of relevant literature,13–15 and with reference to prior applications of TPB,16–19 a preliminary interview guide was drafted following consultation with infectious disease specialists and nursing experts. Two patients meeting the inclusion criteria were recruited for pilot interviews, and the guide was subsequently refined and finalized. Before each interview, participants were provided with a brief explanation of biosample donation. The final interview questions were as follows: (1) Attitude: What is your view on donating biosamples? What significance do you think this behavior holds? (2) Subjective norm: Whose opinions (eg, family members, friends, fellow patients, healthcare professionals) would you consider when deciding whether to donate? How do they influence your decision? (3) Perceived behavioral control: How much do you know about biobanks, and from what sources did you obtain this information? Have you ever considered donating (or previously donated) your own biosamples? Which types of samples would you be willing to donate? What factors would facilitate or hinder your willingness to donate? In your view, who is the most appropriate person to ask whether you are willing to donate biosamples? The biosamples involved in this study include two categories: (1) Residual clinical samples generated during routine diagnosis and treatment (eg, blood, body fluids, and tissues that have completed clinical testing); (2) Additional non-invasive/minimally invasive samples (eg, extra blood draw) voluntarily provided by patients for research purposes. Invasive samples such as bone marrow, cerebrospinal fluid, or whole organs were not included in the study.
Data Collection
Before the interview, participants were fully informed of the following key information: (1) Genetic data may be extracted from biosamples for research purposes, and all genetic information will be anonymized and linked only to study codes (not personal identifiers); (2) Specific privacy protection measures: All data (including transcripts, sample information, and genetic data) will be stored in encrypted servers with limited access (only the research team can access after authorization), and all identifiers will be removed during data analysis and publication; (3) Safety of sample collection: Residual clinical samples involve no additional physical burden on patients; if additional samples (eg, extra blood draw) are required, the procedure is minimally invasive with no obvious complications (eg, bleeding, infection) based on clinical standards, and patients can refuse additional sampling at any time without affecting their clinical treatment. Participants signed written informed consent after confirming their understanding. Semi-structured interviews were conducted by two researchers trained in qualitative interviewing techniques. Interviews took place in a private, quiet room within the inpatient ward. At the beginning of each session, one researcher explained the study objectives and conducted a face-to-face interview following the guide, adapting the sequence and phrasing of questions as needed. Probing, paraphrasing, and clarification were used to ensure accuracy and depth of responses, and all sessions were audio-recorded in full. The second researcher documented participants’ non-verbal behaviors, including tone, facial expressions, and body language. Each interview lasted approximately 20–30 minutes.
Data Analysis
NVivo 12.0 is a qualitative data analysis software widely used for coding, theme extraction, and data management in qualitative research, which helps systematically organize interview transcripts and avoid subjective bias in coding. Colaizzi’s method is a classic phenomenological analysis framework that includes seven core steps: (1) Transcribing interview recordings into text; (2) Extracting meaningful statements related to the research topic; (3) Coding the meaningful statements; (4) Grouping codes into sub-themes based on logical connections; (5) Integrating sub-themes into core themes; (6) Describing the themes in detail with participant quotes; (7) Verifying the consistency between themes and original data. This study combined NVivo 12.0’s systematic data management function with Colaizzi’s rigorous analytical steps to ensure the reliability and validity of the results. Interview recordings were transcribed into text within 24 hours, and the transcripts were verified independently by the two interviewers. In cases of uncertainty, participants were re-contacted for clarification. Data were analyzed using NVivo 12.0 in combination with Colaizzi’s method. Recurrent statements were extracted and coded, and the research team organized the codes into categories based on the three TPB constructs (attitude toward the behavior, subjective norms, and perceived behavioral control), thereby forming a thematic pool. Coding discrepancies and disagreements in theme generation were resolved through team discussion until consensus was reached.
Quality Control
(1) Both interviewers had more than five years of professional experience at the infectious disease specialty hospital, held postgraduate degrees, and had received formal training in qualitative research prior to the study. (2) The interview guide was developed through a rigorous process of literature review, theoretical reference, expert consultation, and pilot testing with patients, ensuring its scientific validity and feasibility. (3) Interviews were conducted in a quiet, private setting. Researchers employed a variety of interviewing techniques to encourage free expression, while a second researcher documented participants’ non-verbal cues, thereby maximizing data richness. (4) Transcripts were verified independently by both interviewers. Any ambiguous content was clarified with the corresponding participant in a timely manner to ensure accuracy. Coding and theme identification underwent repeated scrutiny and discussion within the research team to guarantee reliability and rigor.
Results
A total of 15 interviews were conducted, with no repeat sessions. The cumulative interview time was 365 minutes, yielding 39,886 words of transcription. From the analysis, 59 codes were generated, which were refined into three major themes and eight subthemes.
Theme 1: Divergent Attitudes of Patients with Infectious Diseases Toward Biosample Donation
Positive Attitudes: Donation Perceived as Meaningful
Ten participants considered donation to be valuable, believing it could advance research on their own diseases, contribute to scientific progress, and benefit future patients.
P1 (hepatitis B, nodding):I have had this disease for many years. Donating my samples for research might one day help develop a cure. That makes it very meaningful.
P8 (HIV, giving a thumbs-up):This is a very meaningful topic. Many diseases, like mine, still cannot be cured. If donating samples helps scientists, maybe I won’t live to see the results, but future patients might. It’s a good deed, accumulating virtue by helping others.
P15 (syphilis):I think donating samples is valuable. The medicines and treatments I’m using now probably came from research on samples donated by earlier patients. If needed, I’m willing to donate too.
Negative Attitudes: Donation Perceived as Personally Unbeneficial
Two participants expressed reluctance, believing that biosample donation would bring them little personal benefit, especially given the long and uncertain path of scientific research.
P7 (HIV, shaking head):This disease has been known for years. Scientists worldwide are studying it, yet there’s still no cure. Even if I donate, who knows if it will ever lead to results—and if it does, that could take ages. I’m not very willing to donate.
P13 (hepatitis B, waving hand):I’m old now and have to be hospitalized every year, with lots of blood drawn each time. I don’t have extra blood to give, and it wouldn’t benefit me anyway. Better leave that to the younger patients.
Neutral Attitudes: Concerns About Unknown Risks
Three participants expressed neutral attitudes, emphasizing potential risks of biosample donation and the need to weigh benefits against harms.
P5 (hepatitis B):Everything has two sides. On the positive side, donating samples for disease research is the right thing to do. But from a patient’s perspective, we are already in poor health. Giving more blood might harm our bodies.
P3 (tuberculosis):I would consider who is using my sample. You doctors and nurses are trustworthy, so if it’s for your research, I’d cooperate. But if some company I don’t know gets it, who knows what they would do with it? I wouldn’t trust that.
Theme 2: Subjective Norms Shaping Patients’ Donation Intentions
In this study, “subjective norms” refer to patients’ perceptions of external opinions and social expectations, particularly from family and society, that influence their willingness to donate biosamples.
Influence of Family Support
Half of the participants reported that they would consult family members before deciding whether to donate.
P10 (hepatitis B):I didn’t go to school for long. My daughter always accompanies me to the hospital. For decisions like this, I would definitely ask her first.
P12 (HIV):Although it’s not a major matter, I’d still ask my family. If they don’t want me to donate, I probably won’t.
In contrast, some participants felt capable of making the decision independently, without family input.
P1 (hepatitis B):I don’t think it’s necessary to ask my family. It’s not like surgery that requires their signature. I can make this decision on my own.
P15 (syphilis):My parents are farmers and don’t understand these things. Besides, I haven’t told them about my illness. I usually make decisions myself.
Influence of Healthcare Professionals on Donation Intention
Thirteen participants indicated that the involvement of healthcare professionals could affect their willingness to donate.
P3 (tuberculosis):As I mentioned earlier, I am unsure who would use my samples and for what purpose, so I would not donate them casually. If the doctors or nurses here wanted to use my samples, I would cooperate. But if it were others, I would need to think carefully.
P12 (HIV):Many hospitals refuse to treat patients like us. Only this specialized hospital admits us. If the doctors or nurses here asked whether I would donate samples, I would definitely agree, because I’ll need to keep coming here for treatment.
Influence of Social Perceptions on Donation Intention
Previous studies have reported that patients with infectious diseases often experience stigma and illness-related shame.20,21 In this study, five participants expressed concerns that donating samples might expose them to discrimination or raise fears of disease transmission.
P2 (hepatitis B, frowning):I am a carrier, and those relatives and friends who know about my condition tend to distance themselves. I also try to avoid eating with them. Our samples must carry some infectivity, right? Who would want to use infectious samples like ours?
P4 (tuberculosis, sighing):Only healthy people are allowed to donate blood. Anyone with an illness is excluded. We have infectious diseases. We are already looked down upon. Who would want our blood? What if it infects others?
Theme 3: Limited Perceived Behavioral Control Regarding Biosample Donation Among Patients with Infectious Disease
Limited Knowledge of Biobank-Related Information
Compared with Western countries, biobank development in China started relatively late, and public awareness remains low.7 In this study, most participants reported that they had never heard of biobanks and had not actively sought relevant information. Only two participants had learned about biobanks from healthcare providers, but their knowledge was superficial.
P4 (tuberculosis):I had never heard of a biobank. Last year, I participated in a study at this hospital, which required a blood draw. The doctor explained the study purpose, but I didn’t ask for more details.
P10 (hepatitis B):I don’t know what the biobank is. A staff member once asked to use my samples, but the explanation was too technical for me to understand.
P14 (tuberculosis, shaking head):I have never seen any publicity or reports about this. I don’t really use the Internet, so I’m not familiar with it.
Multiple Concerns Regarding Biosample Donation
Privacy protection: Given the sensitive nature of infectious diseases, 12 participants expressed concerns that biosample donation might lead to disclosure of their personal health information, which could negatively affect their social life, employment, or family relations.
P4 (tuberculosis, pursing lips):If the information leaks out, I might be shunned. These days, the Internet can dig up everything. Even my family could be discriminated against.
P8 (HIV):I think it is essential to ensure the donor’s privacy, especially for people like us. Otherwise, it could cause major disruption or even harm to our lives.
Three participants, however, indicated that they were not particularly concerned about privacy issues.
P3 (tuberculosis):I’m not too worried about privacy. I’m just a farmer, and not many people know me.
Type of research institution: Nine participants indicated a preference for donating samples to non-profit institutions such as hospitals, universities, or research institutes, rather than commercial enterprises. The remaining participants stated that they were less concerned about the nature of the receiving institution.
P11 (HIV):I think biosample donation should be for disease research. It should not involve too much commercial interest or be used for direct profit.
P15 (syphilis):As long as the samples are used properly and formally, I don’t really mind who uses them.
Informed consent providers: All participants agreed that informed consent should be obtained before biosample donation. However, opinions differed regarding who should deliver the information. Twelve participants preferred that healthcare professionals seek their consent, with eight specifically expressing a preference for their attending physicians.
P5 (hepatitis B):Compared with others, I trust my attending doctor and department head more. It would be more appropriate if they asked me.
P8 (HIV):It doesn’t necessarily have to be my attending doctor. Other doctors or nurses would be fine, as long as they are from this hospital.
The remaining three participants felt that the person obtaining consent should be highly familiar with the study itself.
P11 (HIV):I want to know exactly what my samples will be used for. The person explaining should know the research well and be able to answer my questions thoroughly.
Type of biosample donation: All participants expressed willingness to donate residual clinical samples (including blood, body fluids, and tissues) generated during routine diagnostic or therapeutic procedures.
P2 (hepatitis B):These samples have already been tested. If you take them for research, that’s totally fine. Otherwise, they would just be discarded.
P7 (HIV):It doesn’t really affect me. If they are useful, I agree to donate the leftover samples.
Among participants with a generally positive attitude toward donation, five were willing to provide additional samples specifically for research purposes.
P1 (hepatitis B):“This is a meaningful thing. I don’t mind giving an extra tube of blood”.
In contrast, three participants declined extra sampling.
P10 (hepatitis B):“I’m anemic. I don’t want to give too much blood”.
Two participants noted that their decision would depend on the invasiveness of the sampling procedure.
P14 (tuberculosis):It depends on what kind of sample is needed. If it’s something simple, like an extra blood draw, I can consider it. But if it involves risk, like bone marrow or organ donation, I wouldn’t want to.
Feedback on research results: Most participants stated that they would like to receive feedback on research findings, although the absence of feedback would not affect their willingness to donate. Only two participants explicitly required feedback as a condition for donation.
P3 (tuberculosis):If my samples are used, I think I should be informed of the results. That way, I can know what they were used for and whether the research findings relate to my condition.
Costs and compensation: All 15 participants indicated that additional financial expenses would affect their decision to donate samples. Twelve explicitly stated that any extra costs would directly discourage them from donating. P3 (tuberculosis): “If I need to pay extra for this, I definitely wouldn’t want to donate”. The remaining three participants noted that their decision would depend on the amount of money involved.
P15 (syphilis):If the extra cost is small, like tens or a hundred yuan, I can afford it. But if it’s more than that, I may not donate.
Regarding compensation, 11 participants reported that appropriate incentives would positively motivate them to donate samples.
P10 (hepatitis B):This is already a meaningful thing. If there is some compensation, I would be even more willing to donate.
The other four participants stated that compensation would not influence their decision.
P8 (HIV):I’m not doing this for compensation. I would donate samples whether or not compensation is offered.
P13 (hepatitis B):My health is poor. I wouldn’t donate more blood just for a small amount of compensation. My body can’t take it.
Discussion
Biosamples from patients with infectious diseases play a pivotal role in both basic and clinical research. Understanding patients’ willingness to donate is therefore crucial for the establishment and sustainable development of infectious disease biobanks, as well as the advancement of infectious disease research. Findings from this study reveal three major insights: (1) patients’ attitudes toward biosample donation vary, with the majority expressing a positive outlook and recognizing its scientific and social value; (2) donation decisions are shaped by external influences, particularly family members, healthcare providers, and broader social perceptions; and (3) willingness to donate is constrained by limited awareness of biobanks and influenced by multiple factors, including concerns about privacy protection, type of research institution, the identity of the consent provider, sample type, feedback on research results, and issues of cost and compensation.
Positive Attitudes as Motivational Factors in Forming Behavioral Intention
As an exploratory qualitative study, this research focuses on uncovering the nuanced and context-specific factors influencing biosample donation intentions among infectious disease patients (a population understudied in prior literature) rather than testing generalizable conclusions. The novel findings (eg, the duality of family support, stigma-bound social norms) provide theoretical hypotheses and practical insights for future large-scale quantitative studies, which will further validate the generalizability of these themes. According to the TPB, attitudes are a key determinant of behavioral enactment; the more positive the attitude, the stronger the individual’s recognition and intention to perform the behavior.22 Unlike the findings of Ding et al,6 most participants in the present study acknowledged the significance of donating biosamples and expressed willingness to do so. A plausible explanation is that, over the decade since the earlier survey, continuous progress in scientific research has led to the development of improved treatments and therapeutic regimens. Patients with infectious diseases have directly benefited from these advances in terms of disease control and symptom relief, thereby reinforcing their recognition of research value and their willingness to contribute samples for scientific purposes. International studies, such as that by Pawlikowski et al,23 have reported that negative attitudes in the general population often stem from the perception of “no direct personal benefit”. However, such studies did not address the unique concerns of infectious disease patients, who additionally worry about the potential “infectivity” of their samples (eg, fear of transmission risk).
The novelty of this study lies in two aspects: (1) Categorization of attitudes: For the first time, patient attitudes toward biosample donation were classified as positive (66.7%, 10/15), negative (13.3%, 2/15), and neutral (20.0%, 3/15), with identification of their core drivers. Positive attitudes stemmed from their recognition of scientific value (eg, P1 mentioning “drug development for hepatitis B cure”; P8 emphasizing “helping future patients”), negative attitudes were linked to the absence of short-term personal benefit (eg, P7 perceiving “the long timeline of research outcomes”), while neutral attitudes focused on uncertainty about risks (eg, P5 worrying about “the health burden of extra blood collection”). (2) Association with chronic disease experience: We found that positive attitudes were closely associated with patients’ long-term experience of chronic disease. For instance, all six patients with hepatitis B (disease duration 5–20 years) expressed positive attitudes, likely because prolonged suffering increased their expectations for scientific breakthroughs. This contrasts with the findings of Sun et al,11 who observed no significant association between disease duration and attitudes among patients with mental illness. Such results highlight the unique mechanisms shaping attitudes in patients with infectious diseases.
Building on the principle of non-maleficence in the Measures of Ethical Review of Life Sciences and Medical Research Involving Humans,24 the stratification of attitudes observed in this study provides direct guidance for targeted health education. For patients with negative attitudes, communication should emphasize the indirect short-term benefits of biosample donation (eg, contributing to personalized treatment optimization). For patients with neutral attitudes, it is essential to highlight the safety of sample collection (eg, restricting donation to residual clinical specimens). Such tailored strategies enable precision beyond the conventional, generalized approach of merely “advocating for the scientific value” of donation. Moreover, because the act of donating biosamples does not entail a high degree of difficulty, patients’ trust in the research institution or investigators plays a pivotal role. The greater the trust, the stronger the recognition of the value of donation, which in turn fosters positive perceptions and attitudes.25 Conversely, insufficient trust may trigger doubts about the motives and reliability of the research, thereby undermining willingness to donate. These findings suggest that, prior to promoting the scientific value of biosample donation, efforts should focus on transparently presenting the legitimacy of the sponsoring institution and the reliability of sample storage and utilization. Reinforcing trust in these domains may enhance patients’ sense of security and strengthen their positive attitudes toward biosample donation.
Family and Social Support as Key Drivers of Subjective Norms
The influence of subjective norms on biosample donation has been confirmed by multiple studies; however, existing evidence has not fully addressed the specific circumstances of patients with infectious diseases. Internationally, Tesema et al8 found that family support accounted for 40% of the variance in kidney donation intentions, and Bondy et al26 reported that social attitudes explained 35% of the variance in vaccine acceptance. Yet, neither study incorporated the unique link between disease stigma and decision-making in those with infectious diseases. Domestically, Liu et al20 demonstrated that family support enhances psychological resilience among patients with HIV, but did not extend this finding to the context of biosample donation; meanwhile, studies involving patients with cancer merely noted that “healthcare professionals’ recommendations are effective”, without differentiating between specific healthcare roles.14 Consistent with these findings yet extending beyond them, our results show that among patients with infectious diseases, their willingness to donate biosamples is influenced by the perspectives of family members, healthcare providers, and the broader society. When these groups endorse and support donation, patients’ intentions to donate are significantly strengthened.
This study identified three unique insights: (1) The “duality” of family support. Half of the patients (eg, P10) reported reliance on family members for decision-making due to limited disease knowledge, whereas two patients with syphilis/HIV (eg, P15) deliberately avoided family consultation because of disease concealment. This novel “reliance-avoidance” dichotomy fills a gap in the literature on family support mechanisms among patients with infectious diseases, highlighting the need for differentiated health education strategies under conditions of “family disclosure” versus “family concealment”. (2) The “supervising role effect” of healthcare providers. Eight out of fifteen participants explicitly preferred their supervising clinicians to conduct the informed consent process (eg, P5 expressed trust in the attending physician), rather than generic “healthcare staff”. This finding contrasts sharply with previous evidence in patients with cancer, who showed no preference regarding provider roles.23 The key driver appears to be the long-term treatment dependency of patients with infectious diseases, which fosters heightened trust in their supervising clinicians. (3) The “stigma-bound” constraint of social norms. Five participants (eg, P2 worried that “hepatitis B samples would be rejected”) linked biosample donation directly with disease-related discrimination. In contrast, preceding public-focused studies only emphasized concerns about “uncertainty of sample use”.11,27 In China, although the Law of the People’s Republic of China on Prevention and Treatment of Infectious Diseases explicitly prohibits discrimination against patients with infectious diseases, and medical insurance policies (eg, basic medical insurance for urban and rural residents) do not exclude or increase premiums for patients with HIV, HBV, HCV, or leprosy, implicit discrimination (eg, social avoidance, employment restrictions) still exists due to public misunderstanding of disease transmission. For non-Chinese immigrants in China, there is no policy linking infectious disease diagnosis to deportation; their medical rights are protected by relevant national regulations. However, the fear of stigma and discrimination remains a key barrier for patients to donate biosamples, highlighting the need for multi-dimensional social support (eg, public science popularization, anti-discrimination campaigns) alongside biobank promotion. This indicates that social support interventions for patients with infectious diseases must simultaneously reinforce both the scientific value of biosample donation and the de-stigmatization of infectious diseases—neither component alone is sufficient. Collectively, these findings underscore the indispensable role of frontline healthcare professionals, whose ethical standards and scientific literacy are critical for advancing biomedical research. Accordingly, healthcare institutions should strengthen the cultivation of professional ethics, enhance doctor-patient communication skills, encourage attentiveness to specialized research progress, and improve healthcare providers’ understanding of the scientific value of biobanking, thereby fostering a stronger research-oriented mindset.
The interviews also revealed that patients’ subjective norms regarding biosample donation are constrained by social-level factors. Many patients with infectious diseases expressed concerns that biosample donation might lead to privacy breaches, which, in the context of an increasingly digital society, could negatively affect both themselves and their families. Others worried about the potential infectivity of their samples, fearing possible harm to the public and thus denying the scientific value of their own contribution. In recent years, the Chinese government has issued a series of policies to provide legal protection for medical care and employment of individuals with infectious diseases, while multiple levels of government and organizations have actively promoted public science education. As a result, public awareness and knowledge of infectious diseases have gradually improved. However, stigma and perceived discrimination remain prevalent, and the sense of shame associated with infectious diseases continues to be high among patients.20,21 Addressing the psychological health needs of this population remains a long-term, pressing challenge. These findings underscore the importance of strengthening social-level support. In line with national policy directions, greater efforts should be made to promote public education on infectious diseases and biobanking, while explicitly affirming the scientific value of infectious disease samples.
Enhancing Awareness and Ensuring Informed Consent as Key Measures to Strengthen Perceived Behavioral Control
According to TPB, perceived behavioral control reflects an individual’s ability to execute a given behavior. It is constrained by past experiences and situational conditions; the lower the anticipated resistance and difficulties in performing the behavior, the stronger the perceived behavioral control, and the higher the behavioral intention.8,16 In this study, we found that patients with infectious diseases generally demonstrated limited awareness of biobanking. Their willingness to donate samples was influenced by multiple factors, including privacy protection, type of research institution, the identity of the consent provider, sample type, feedback on research results, and issues of cost and compensation. These findings are consistent with prior reports.11,23,26
In medical research, biosamples are often collected in parallel with associated information (eg, personal demographics, medical records, diagnostic test results, and follow-up data) in order to maximize their scientific value. Privacy protection is therefore of paramount importance and is explicitly mandated by relevant legal and ethical frameworks.24 As mentioned earlier, patients with infectious diseases experience heightened internalized stigma and perceived public discrimination,21 which amplify their concerns about confidentiality. Fear of privacy breaches affecting themselves or their families emerged as a key barrier to biosample donation. Importantly, when the research institution and the personnel seeking consent (eg, medical facilities and treating healthcare professionals) were perceived as trustworthy, patients generally expressed confidence in the strength of privacy safeguards and were more willing to recognize the reliability of biosample donation.11
Compared with the potential scientific value of research outcomes, patients with infectious diseases were more concerned about the type of biosamples requested. All interviewees agreed to donate residual specimens (eg, blood, body fluids, tissues) generated during routine clinical procedures, as these impose no additional burden on the donor. However, when additional sampling was required or when the procedure carried certain risks, most patients reported hesitation or refusal to participate. Participants also expressed interest in receiving feedback related to studies utilizing their specimens. Nevertheless, given that scientific research often requires long-term accumulation of evidence, most patients indicated that the absence of feedback would not affect their willingness to donate.
Financial factors further shaped patients’ intentions. All participants emphasized that any additional personal expense would serve as a deterrent to donation, whereas modest compensation was generally regarded as a positive incentive. These views are consistent with findings in psychiatric patient populations24 and align with the stipulations of the Measures of Ethical Review of Life Sciences and Medical Research Involving Humans,24 which mandate that participants should not incur costs for research participation, and that expenses incurred must be appropriately compensated.
These findings highlight that the process of obtaining informed consent for biosample donation among patients with infectious diseases should comprehensively address the aforementioned concerns. Effective and sufficient informed consent requires that, under the premise of participants (or their guardians) having autonomous decision-making capacity, the information provided must be both understandable and complete.28 Such requirements should be reflected not only in the written consent form but also throughout the consent process. Specifically, researchers should employ clear, non-technical language to explain the sponsoring institution, study objectives, research content, types of specimens to be collected, privacy and confidentiality measures, participants’ rights, cost and compensation policies, and relevant contact information. Moreover, investigators should actively assess participants’ comprehension and clarify any doubts in a timely manner. These practices are essential to fostering trust between researchers and participants, thereby minimizing their concerns.
This study has two major limitations regarding disease distribution and patient sources. First, patients with hepatitis B accounted for a relatively high proportion (40%), whereas patients with syphilis and hepatitis C were underrepresented, which might be explained by their lower hospitalization rates. Although the core themes (eg, privacy concerns) were consistent across disease categories, disease-specific perceptions among patients with lower hospitalization rates may have been overlooked. Second, only inpatients were included, who typically have closer contact with healthcare providers, whereas outpatients (constituting 62.3% of the patient population) were not covered. Outpatients may prioritize concerns such as time cost and privacy to a greater extent, which limits the generalizability of the findings. Future research should expand sample sizes for low-hospitalization diseases through multicenter collaboration and adopt stratified sampling across inpatient and outpatient settings to compare differences in attitudes and perceived behavioral control toward biosample donation. In addition, the development of tailored educational strategies and the strengthening of public communication on biosample donation are warranted to enhance positive attitudes, leverage the supportive roles of families, healthcare providers, and society, and explore more appropriate informed consent models to facilitate infectious disease research and the establishment of biobanks. This study has two major limitations: First, the sample size is small (15 cases) and single-center, which may limit the generalizability of the results to other regions or healthcare settings; second, only hospitalized patients were included, while outpatients and home-care patients (who account for a large proportion of infectious disease patients) were not covered, and their donation intentions and influencing factors may differ. These limitations will be addressed in future multi-center studies with expanded sample sizes and inclusion of diverse patient groups.
Conclusion
Most patients with infectious diseases expressed positive attitudes toward biosample donation. Future research should expand to multi-center studies with larger sample sizes, include outpatients and home-care patients for stratified analysis, and further explore tailored informed consent models and publicity strategies to better support the construction of infectious disease biobanks.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethical Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by The Second Hospital of Nanjing (2025-LS-ky-015).
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Funding
This work was supported by Project of Nanjing Health Science and Technology Development Special Fund of Nanjing Municipal Health Commission (GAX23297) and Research Project on Hospital Management Innovation of Jiangsu Hospital Association (JSYGY-3-2023-584).
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. World health statistics 2022. 2022. Available from: https://www.who.int/data/gho/publications/world-health-statistics.
2. Li F. Construction and study of an epidemic model with asymptomatic infection in a complex network Qingdao University; 2022.
3. World Health Organization. Global Tuberculosis Report 2024. Geneva: World Health Organization; 2024:1–13.
4. UNAIDS. 2024 global AIDS report — the urgency of now: AIDS at a crossroads. Available from: https://www.unaids.org/es/node/58700.
5. Xiao Y, Li Y, Li Y, et al. Estimating the long-term epidemiological trends and seasonality of hemorrhagic fever with renal syndrome in China. Infect Drug Resist. 2021;14:3849–3862. doi:10.2147/IDR.S325787
6. Ding WB, Ma Y, Wang Y, et al. Cross-sectional survey of attitudes of patients towards biosample donation. J Shanghai Jiaotong Univ. 2014;34(10):1497–1502.
7. Gao Z, Huang Y, Yao F, et al. Public awareness and attitudes toward biobank and sample donation: a regional Chinese survey. Front Public Health. 2022;10:1025775. doi:10.3389/fpubh.2022.1025775
8. Tesema B, Bogale K, Wasihun Y, et al. Intention to donate kidney and associated factors among students in bahir dar university: application of theory of planned behavior. Int J Gene Med. 2023;16:5363–5376. doi:10.2147/IJGM.S441636
9. Salajegheh Z, Bagherian B, Rabori RM, et al. The effect of a training program based on the theory of planned behavior on the self-care of patients with cerebrovascular accident: a randomized controlled trial. Iranian J Nurs Midwifery Res. 2024;29(2):194–201. doi:10.4103/ijnmr.ijnmr_100_23
10. Chen Q, Ma J, Wu R, et al. Factors influencing hepatitis B vaccination intention and behavior among college students in Tibet: insights from the expanded theory of planned behavior. Hum Vaccines Immunother. 2025;21(1):2452026. doi:10.1080/21645515.2025.2452026
11. Sun LL, Suo L, Si JJ, et al. Donation willingness to biobank and influence factors in patients with mental diseases. Med Philos. 2020;41(16):24–27.
12. Domaradzki J, Czekajewska J, Walkowiak D. Trust and support for cancer research biobanks: insights from cancer patients in Poland. Med Sci Monit. 2024;30:e944263. doi:10.12659/MSM.944263
13. Griffin CP, Carlson MA, Walker MM, et al. “I’m standing next to him, I’m supporting him” - supporting a loved one with brain cancer to donate their brain: a qualitative study. Neuro-Oncol Pract. 2024;11(6):813–820. doi:10.1093/nop/npae049
14. Domaradzki J, Walkowiak D. When biobanks meet religion: Association between religiosity and attitudes of polish medical students toward biobanking of human biological material for research purposes. J Relig Health. 2024;63(2):1178–1213. doi:10.1007/s10943-023-01932-2
15. Pronicki L, Czech M, Gujski M, et al. Awareness, attitudes and willingness to donate biological samples to a biobank: a survey of a representative sample of polish citizens. Healthcare. 2023;11(20):2714. doi:10.3390/healthcare11202714
16. Latifi M, Rakhshanderou S, Najafizadeh K, et al. A theory-driven organ donation campaign: a field intervention among university students in Iran. Clin Transplant Res. 2024;38(2):90–97. doi:10.4285/ctr.24.0022
17. Sighaldeh SS, Moridi M, Kazemnejad A, et al. Effectiveness of a theory-based educational intervention on enhancing milk donation behavior: a cluster randomized controlled trial. Int Breastfeed J. 2025;20(1):17. doi:10.1186/s13006-025-00711-x
18. Liu CC, Lin HC, Wang JY. Promote middle-aged and older adults’ blood donation intention with concepts of social marketing and theory of planned behavior: a cross-sectional survey. Sage Open. 2025;15(1):21582440251318157. doi:10.1177/21582440251318157
19. Ye XY, Xu YL, Wang YL, et al. Noise management-associated behavioural intentions of ICU nurses based on the theory of planned behaviour: a qualitative study. Modern Clin Nurs. 2024;23(11):39–45.
20. Liu XJ, Luo L, Ye ZL, et al. Research progress on psychological resilience of human immunodeficiency virus/acquired immunodeficiency syndrome patients. Chin J Hum Sex. 2025;34(04):131–135.
21. Chen H, Jia WJ, Wang LH, et al. Modification effect of social support level on the perception of discrimination against HIV and adherence to antiviral therapy among middle-aged and elderly people living with HIV. Mod Preventive Med. 2024;51(14):2513–2516+2580.
22. Zhong MH, Su LH, Xie FL, et al. Factors in self-management disorder of arteriosclerotic obliterans of lower extremity in aged patient: a qualitative study based on planned behaviour theory. Modern Clin Nurs. 2025;24(01):24–29.
23. Pawlikowski J, Wiechetek M, Majchrowska A. Associations between the willingness to donate samples to biobanks and selected psychological variables. Int J Environ Res Public Health. 2022;19(5):2552. doi:10.3390/ijerph19052552
24. National Health Commission, Ministry of Education, Ministry of Science and Technology, National Administration of Traditional Chinese Medicine. Measures of ethical review of life sciences and medical research involving humans. 2023. Available from: http://www.nhc.gov.cn/qjjys/c100016/202302/6b6e447b3edc4338856c9a652a85f44b.shtml.
25. Nicholls SG, Camilleri E, Chesser T, et al. Patient and healthcare professional reflections on consenting for extra bone marrow samples to a biobank for research - a qualitative study. Current Oncol. 2025;32(3):179. doi:10.3390/curroncol32030179
26. Bondy S, Mcclymont E, Avgay G, et al. Acceptance and attitudes towards COVID-19 vaccination during pregnancy in Canada. Hum Vaccines Immunother. 2025;21(1):2458353. doi:10.1080/21645515.2025.2458353
27. Hamilton LJ, Middlestadt S. Beliefs about donating human milk to a milk bank: a theory-based salient belief elicitation. J Hum Lactation. 2024;40(4):582–592. doi:10.1177/08903344241274348
28. Domaradzki J, Czekajewska J, Walkowiak D. Perception of Polish patients with cancer of the ethical and legal issues related to biobank research. Oncologist. 2024;29(7):e887–e898. doi:10.1093/oncolo/oyae078
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
The Decision-Making Experience of Self-Management Behaviors in Home Peritoneal Dialysis for Patients with Diabetic Nephropathy: A Qualitative Study Using the Theory of Planned Behavior
Song Z, Xiao Y, Su Y, Qin G, Yang J
Patient Preference and Adherence 2025, 19:2283-2294
Published Date: 31 July 2025