Back to Journals » Drug Design, Development and Therapy » Volume 14
Bioequivalence Study of Amitriptyline Hydrochloride Tablets in Healthy Chinese Volunteers Under Fasting and Fed Conditions
Authors Zhai Y ![]() , Wu L, Zheng Y, Wu M, Huang Y, Huang Q
, Wu L, Zheng Y, Wu M, Huang Y, Huang Q ![]() , Shentu J, Zhao Q, Liu J
, Shentu J, Zhao Q, Liu J ![]()
Received 21 April 2020
Accepted for publication 17 July 2020
Published 4 August 2020 Volume 2020:14 Pages 3131—3142
DOI https://doi.org/10.2147/DDDT.S258173
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Manfred Ogris
You Zhai,1,2 Lihua Wu,1,2 Yunliang Zheng,1,2 Minglan Wu,1,2 Yujie Huang,1,2 Qian Huang,1,2 Jianzhong Shentu,1– 3 Qingwei Zhao,1,2 Jian Liu1,2
1Research Center for Clinical Pharmacy, State Key Laboratory for Diagnosis and Treatment of Infectious Disease, The First Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou, People’s Republic of China; 2Zhejiang Provincial Key Laboratory for Drug Evaluation and Clinical Research, The First Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou, People’s Republic of China; 3College of Medicine, Zhejiang University, Hangzhou, People’s Republic of China
Correspondence: Jian Liu
Research Center for Clinical Pharmacy, State Key Laboratory for Diagnosis and Treatment of Infectious Disease, Zhejiang Provincial Key Laboratory for Drug Evaluation and Clinical Research, The First Affiliated Hospital, College of Medicine, Zhejiang University, 79 Qingchun Road, Hangzhou 310003, People’s Republic of China
Tel +86 571 87236537
Fax +86 571 87214223
Email [email protected]
Purpose: This study compares the pharmacokinetic and safety profiles between a new generic and a branded reference formulation of amitriptyline hydrochloride tablets, and assesses the bioequivalence of the two products in healthy Chinese volunteers to obtain sufficient evidence for the marketing approval of the generic drug.
Materials and Methods: A randomized, open-label, two-period crossover study (clinicaltrials.gov, NCT03646526) was conducted under both fasting and fed conditions in healthy Chinese volunteers (24 subjects/condition). Eligible subjects randomly received a single 25 mg dose of either the test or the reference formulation, followed by a 3-week washout period. Blood samples were collected until 144 h following administration. The pharmacokinetic parameters were acquired based on the concentration-time profiles, including the areas under the plasma concentration-time curve (AUC0-t, AUC0-∞), the peak plasma concentration (Cmax), the time to achieve Cmax (Tmax), and the elimination half-life (t1/2). The geometric mean ratios (GMRs) and the corresponding 90% confidence intervals (CIs) of amitriptyline were acquired for bioequivalence analysis, and values of these parameters for nortriptyline were used for comparison of therapeutic outcomes. Safety assessments included laboratory tests, physical examination, vital signs, and incidence of adverse events (AEs).
Results: The values of t1/2 and Tmax for amitriptyline were not significantly different between the test and reference products under both fasting and fed conditions (P > 0.05). The GMRs of Cmax, AUC0–t, and AUC0-∞ between the two products, and corresponding 90% CIs, were all within the range of 80% to 125% under both fasting and fed conditions. The test and reference products were well tolerated and did not elicit serious adverse events.
Conclusion: This study demonstrated that the generic and reference products were well tolerated by the subjects and bioequivalent, according to the rate and extent of the drug absorption.
Keywords: bioequivalence, pharmacokinetics, amitriptyline hydrochloride, nortriptyline
Introduction
Depression is a major mental health disorders, which affected more than 300 million people in 2015. The World Health Organization (WHO) estimates that depression is the leading cause of disability and results in high morbidity, high suicide rates, and low clinical treatment rates worldwide.1 Various antidepressants, which are now available, are effective in treating depression, including tricyclic antidepressants (TCAs), monoamine oxidase inhibitors, selective serotonin reuptake inhibitors, serotonin-noradrenaline reuptake inhibitors, selective noradrenaline reuptake inhibitors, and noradrenergic and specific serotonergic antidepressants.2,3 Antidepressants were the 3rd most frequently prescribed drugs to individuals in the United States between 2005 and 2008.4,5 In addition, TCA amitriptyline has been regarded as one of the reference compounds for depression treatment.6
Amitriptyline, the most commonly used TCA, has a strong sedative effect and is primarily used to treat anxiety or agitated depression. Furthermore, it is slightly more effective than other TCAs or newer compounds.7,8 Amitriptyline was initially used in 1961 where it replaced imipramine soon after.9 Amitriptyline was the 3rd most frequently used antidepressant in Germany in 2008, corresponding to 94 million daily doses.10 According to a large primary care-based prescription database in the UK, approximately 13 in every 1000 individuals were prescribed amitriptyline for depression treatment in 2010.11 To date, it is one of the most commonly used antidepressants included in the WHO’s list of essential drugs.12 Currently there are more than 20 types of antidepressants mentioned in the Chinese national essential drug list. However, only amitriptyline and doxepin are primarily prescribed by primary care physicians.13
During amitriptyline metabolism, its side chain oxidizes producing a secondary amine nortriptyline, an N-oxide amitriptylinoxide (AT-NO), and a primary amine.14,15 Also, the demethylation of amitriptyline to the secondary amine nortriptyline does not result in its inactivation. Therefore, nortriptyline, which also has antidepressant and antinociceptive activities, subsequently became available.14 It is believed that the activities of amitriptyline and its active metabolite, nortriptyline, are primarily but not entirely due to their binding to the noradrenaline and serotonin transporters at central sites.16 In addition to major depression, amitriptyline was also reported to treat chronic neuropathic pain (pain due to nerve damage),17,18 fibromyalgia,19 migraine, and anxiety disorders.20,21
Although amitriptyline hydrochloride has been widely used in China for several years, only a limited number of reports have studied its efficacy and tolerability during treatment of depressive disorders or other diseases. Thus, the pharmacokinetic data of this drug are limited. Recently, a generic amitriptyline hydrochloride product has been developed by Hunan Dongting Pharmaceutical Co., Ltd., (Hunan, China). Consistent with National Medical Products Administration guidelines, we compared the bioavailability of the new amitriptyline hydrochloride tablets with the reference product, manufactured by Sandoz Inc. and listed in the FDA orange book in 2016. This study was performed in healthy Chinese subjects, under fasting and fed conditions, to support the marketing approval of the newly developed generic formulation in China.
Materials and Methods
Study Drugs
The amitriptyline hydrochloride test product was obtained from Dongting Pharmaceutical Co., Ltd, Hunan, China (batch number XB170502, expiry date 2019/04). Meanwhile, the reference product was purchased from Sandoz Inc., US (batch number HB3649, expiry date 2020/04).
Subjects
Healthy male and female Chinese adults, aged 18 to 45 years, with body mass indexes (BMIs) ranging from 19 to 26 kg/m2, and weights higher than 45 and 55 kg for females and males, respectively, were recruited. All participating subjects signed informed consent forms (ICFs) after receiving information and confirmed understanding of the study’s nature, objectives, procedures, possible risks, and requirement for study completion. All subjects were subjected to a comprehensive medical examination to evaluate their health conditions, including routine physical examination, detailed medical history, routine clinical laboratory test (including analyses of the blood, coagulation function, urine, and immunological system, and drug, alcohol, and nicotine tests), 12-lead electrocardiography (12-lead ECG), and chest X-ray. Only healthy subjects, who agreed to use contraceptive methods from 14 days prior to dosing to 6 months following the end of study, and fit the age, BMI, and weight criteria, and signed the ICFs, fulfilled the inclusion criteria and thus were randomized.
None of the subjects experienced any clinically significant abnormality during this study. Subjects with any history of allergy, sensitivity to any ingredient in the amitriptyline hydrochloride tablets, abuse of drug or alcohol, excessive smoking, or hepatic renal impairment were excluded. Subjects who used any drugs within 2 weeks before the first administration of amitriptyline hydrochloride, female subjects who were pregnant or lactating during the study, and subjects who suffered from any condition which could possibly affect the absorption of the drug were also excluded.
Study Design and Treatment
This study (ClinicalTrials.gov, NCT03646526) was performed at the Phase I Clinical Research Center of the First Affiliated Hospital, College of Medicine, Zhejiang University, China, in accordance with the Declaration of Helsinki, the Good Clinical Practice Guidelines of the International Conference on Harmonization, and other related guidelines. This study included two independent clinical trials (fasting and fed studies); each one was conducted using a randomized, open-label, single-dose, two-product, two-period crossover design. The research proposal was reviewed by the ethics committee of the First Affiliated Hospital, College of Medicine, Zhejiang University on February 8, 2018, and approved on March 20, 2018 (approval No. 2018-EC-38). The start and completion dates of the fasting and fed studies were August and September 2018, respectively.
All the subjects who were hospitalized on the day before the trial were randomly assigned to either group TR or group RT. Group TR received the test product in the first treatment period and the reference product in the second treatment period, while Group RT had the opposite administration sequence. These two treatment periods were separated by a 3-week washout phase. The randomization scheme was generated by the SAS software (version 9.4) in a 1:1 randomized block design. For subjects under fasting conditions, a single-dose test or reference product was orally taken with 240 mL warm water after fasting for at least 10 h, while subjects under fed conditions had standard high-fat breakfast of about 800–1000 kcal (approximately 150, 250, and 500~600 kcal of protein, carbohydrates, and fat, respectively) starting 30 min before each drug administration and followed the same scheme. A thorough oral examination was performed after each drug administration to confirm oral film dissolution. The subjects were ambulatory, prohibited from vigorous activity, and closely supervised by qualified staff during the entire period of confinement. Water intake within 1 h before and after dosing was prohibited. Standard lunches and dinners were provided at the same time for both groups of the study, at 4 and 10 h after dosing.
Blood Sampling and Analytical Determinations
A series of blood samples were collected before and after each treatment period. Blood samples (4 mL) for pharmacokinetic analyses were collected into coded, K2-EDTA anticoagulation tubes at pre-dose (baseline) and at 0.5, 1, 2, 3, 4, 5, 6, 7, 8, 10, 12, 24, 36, 48, 72, 96, 120, and 144 h post drug administration, and then centrifuged at 2000 × g and 4 °C for 10 min to separate the plasma. Plasma samples were temporarily stored at −20 °C within 2 h of collection and transferred to an ultra-low temperature freezer (−70 ± 10 °C) within 48 h for storage until analysis. In addition, all the collecting, processing, and storage procedures were performed under scarce light due to the photosensitive nature of the analytes. Plasma concentrations of amitriptyline and its metabolite nortriptyline were measured by the LC–MS/MS method, previously validated by CMIC (Suzhou) Pharmaceutical Technology Co., Ltd (Suzhou, China).
After performing a protein precipitation procedure, the quantitative determination of the target compounds was carried out in the positive ion mode and multiple reaction monitoring. Analytes were chromatographed by Shimadzu LC-30AD and analyzed by AB SCIEX tandem mass spectrometry Triple Quad 5500. Data were acquired with the analyst software, version 1.6.3. The linearity range of the detection method for amitriptyline and nortriptyline were 0.2–50 ng/mL and 0.1~25 ng/mL, respectively. The lower limits of quantitation of amitriptyline and nortriptyline were 0.2 ng/mL and 0.1 ng/mL, respectively. Additionally, Cmax and AUC0-t of amitriptyline were 18.7% and 14.9%, respectively. Based on previous pre-test results from 12 subjects, Cmax and AUC0-t of amitriptyline were 23.48% and 18.95%, respectively. Thus, the coefficient of variation in this study was considered as 24%. Assuming a one-sided test with α = 0.05, accuracy of 0.8 (β = 0.2), CV intra-subject = 24%, a mean ratio of the test and reference product of 1.00, and 90% CI of 80.00%~125.00% for the bioequivalence, 21 samples were required for testing, according to the PASS software (version 11.0.7). After considering the dropout rate, 24 subjects were enrolled for each study.
Safety Assessment
Safety assessments included laboratory tests, physical examinations, 12-lead ECG, vital sign measurement, and incidence of AEs. The laboratory tests included analyses of blood, coagulation function, urine, and immunological examination. Meanwhile, vital signs, such as blood pressure, pulse, temperature, and respiratory rate, were monitored before administration, as well as at 1, 4, 6, 8, 24, 48, 72, 96, 120, 144 h after each drug administration to evaluate the safety of these two products. Any AEs occurring throughout the trial was recorded by research doctors and spontaneously reported by volunteers.
Pharmacokinetic and Statistical Analysis
Amitriptyline pharmacokinetic parameters were calculated using the statistical software package SAS Enterprise Guide (V9.4) (SAS Institute Inc., Cary, North Carolina) and verified by performing the non-compartmental analysis with the Phoenix WinNonlin software, version 7.0 (Certara, L.P., St. Louis, MO). Plasma concentration-time curves were generated under both fasting and fed conditions where Cmax and Tmax were obtained. Meanwhile, AUC0−∞was calculated using the linear trapezoidal rule. AUC0–∞ was calculated as the sum of AUC0−t and the extrapolated area from the last quantifiable concentration (Ct) divided by the elimination rate constant (λz). T1/2 was calculated as ln2/λz. The percentage of the extrapolated area (AUC_%Extrap_obs) was obtained with the following formula: [(AUC0−∞-AUC0−t)/AUC0−∞] * 100%. The relative bioavailability (F) of the test product was calculated as: F=AUC0-t(test)/AUC0-t (reference) * 100%.
Statistical analyses were performed with the statistical software package SAS Enterprise Guide (V9.4) (SAS Institute Inc., Cary, North Carolina) using the non-compartmental pharmacokinetic analysis. Cmax, AUC0-t, and AUC0-∞ were considered the main variables. The bioequivalence was determined by the factorial analysis of variance (ANOVA) for crossover design and calculating the 90% CIs of the ratio test/reference, according to the Chinese regulatory guideline. Therefore, ANOVA (PROC MIXED) evaluated the effects of the products, dosing sequence, trial period, and subjects nested within sequence by measuring the natural logarithm (ln)-transformed pharmacokinetic parameters (Cmax, AUC0-t, and AUC0-∞). Parametric 90% CIs of GMR between the two products (test–reference) were then calculated. Wilcoxon Signed Rank Test was used for Tmax and t1/2 assessments. If the 90% CIs of the Cmax, AUC0-t and AUC0-∞ GMRs fell within 80% to 125%, the two products were considered bioequivalent.
Results
Participants
As shown in Figure 1, from Aug 7, 2018, to Sept 13, 2018, a total of 193 healthy Chinese adult potential subjects were screened. From among them, 48 were selected for the fasting and fed studies (n = 24 per group). Tables 1 and 2 summarize the demographic characteristics of all subjects.
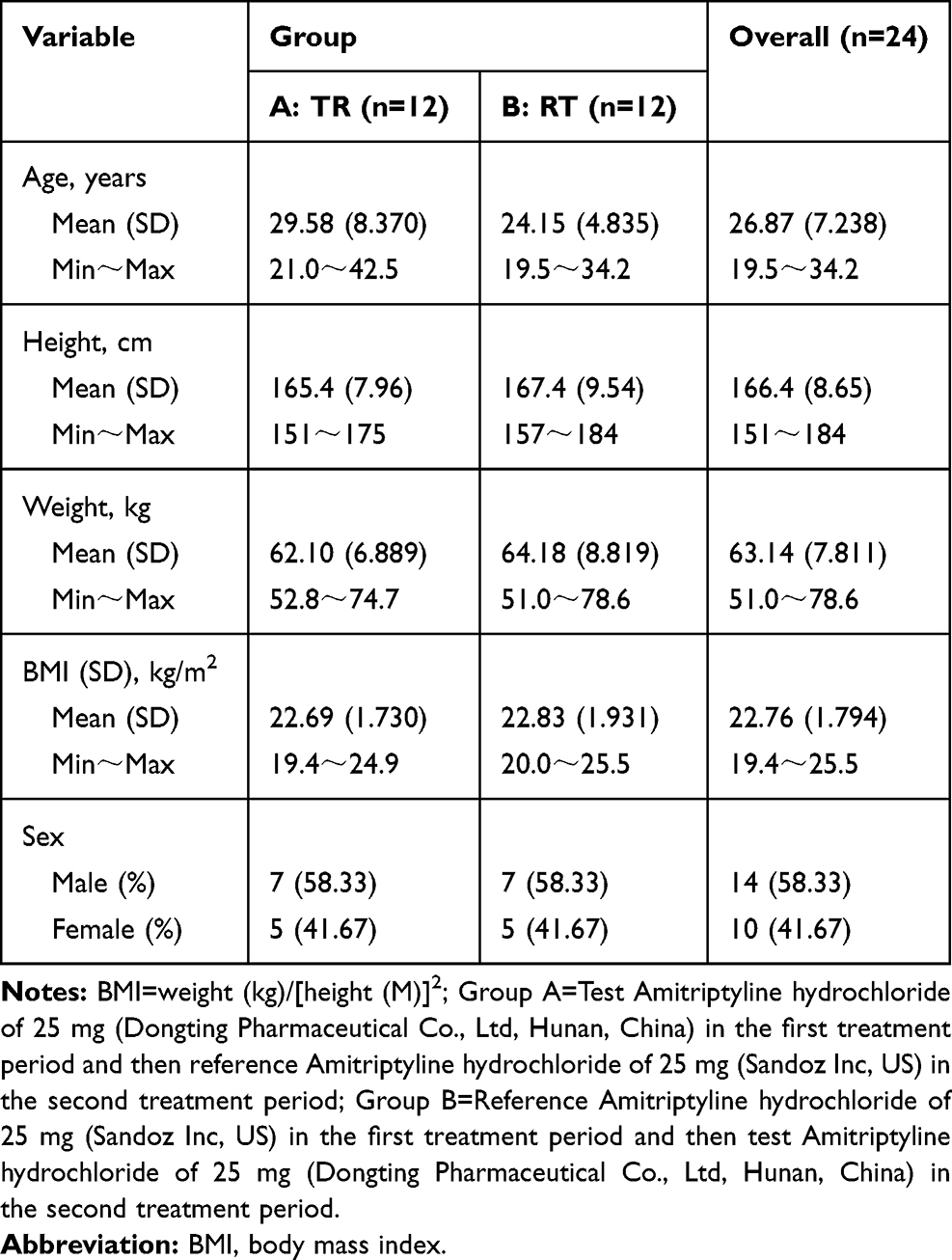 |
Table 1 Demographic Characteristics of Healthy Volunteers of the Fasted Study (n=24) |
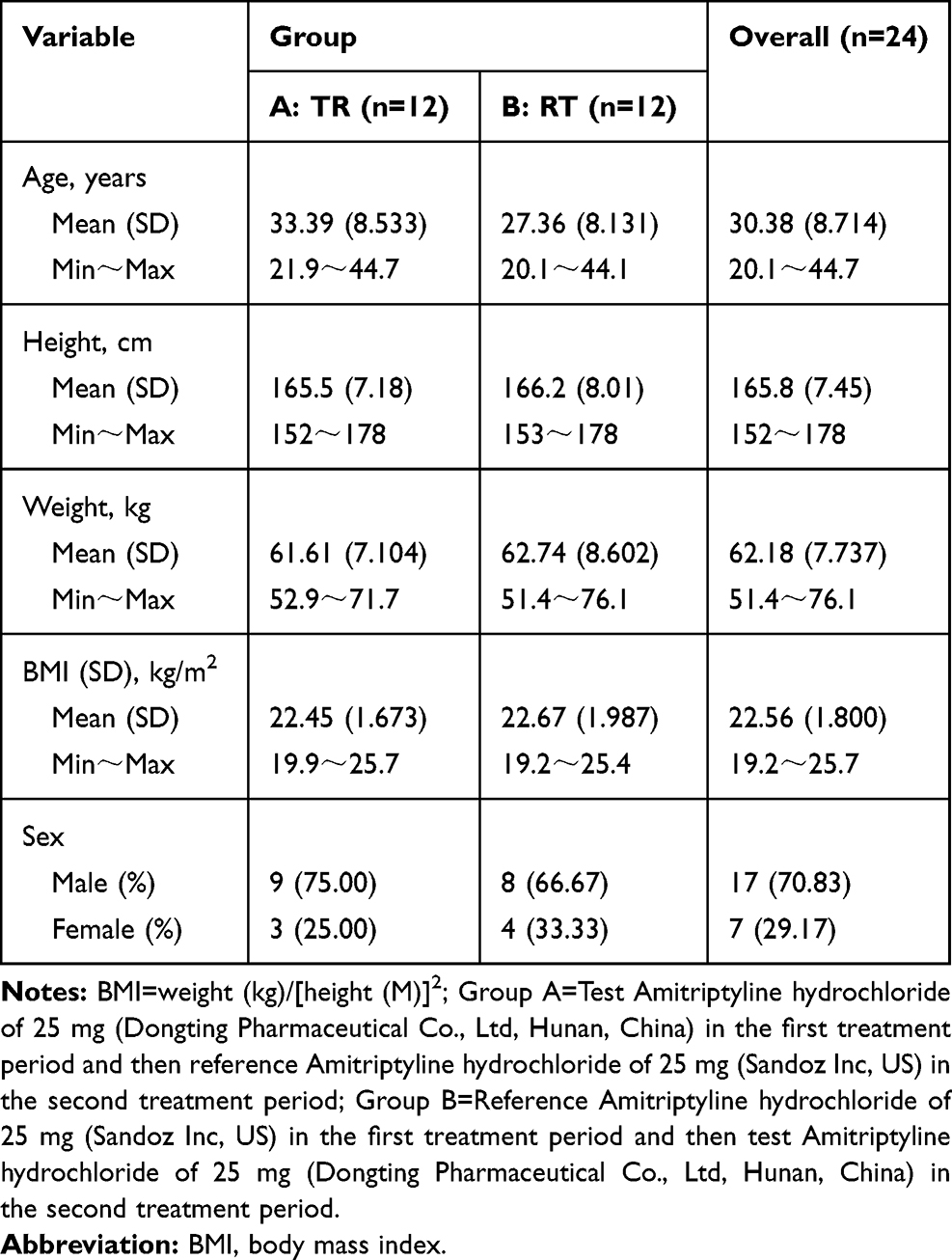 |
Table 2 Demographic Characteristics of Healthy Volunteers of the Fed Study (n=24) |
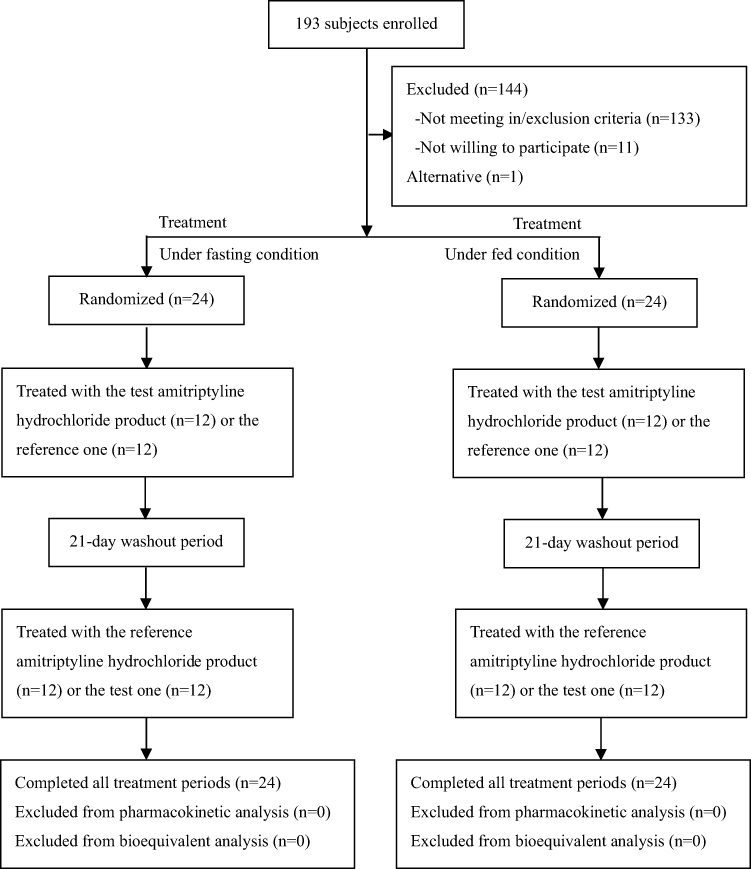 |
Figure 1 Study design and disposition of subjects. |
Pharmacokinetic Properties
All 48 randomized subjects completed the studies and were included in the pharmacokinetic analyses for the reference or the test product. Under fasting conditions, nortriptyline AUC_%Extrap_obs values of 5 subjects were greater than 20% in both periods. On the other hand, under fed conditions, nortriptyline AUC_%Extrap_obs values of 2 and 1 subjects surpassed 20% in the 2nd period and in both periods, respectively. These subjects were not included the calculation of the pharmacokinetic analysis of AUC0-∞, AUC_%Extrap_obs, λz, and t1/2 for the nortriptyline. The mean plasma concentration-time profiles of amitriptyline and nortriptyline following a single oral administration of the test and the reference products under fasting and fed conditions are shown in Figures 2 and 3, respectively. Major pharmacokinetic parameters of amitriptyline and nortriptyline under fasting and fed conditions are summarized in Tables 3 and 4, respectively. The t1/2 of amitriptyline was about 32 to 38 h and that of nortriptyline was approximately 39 h.
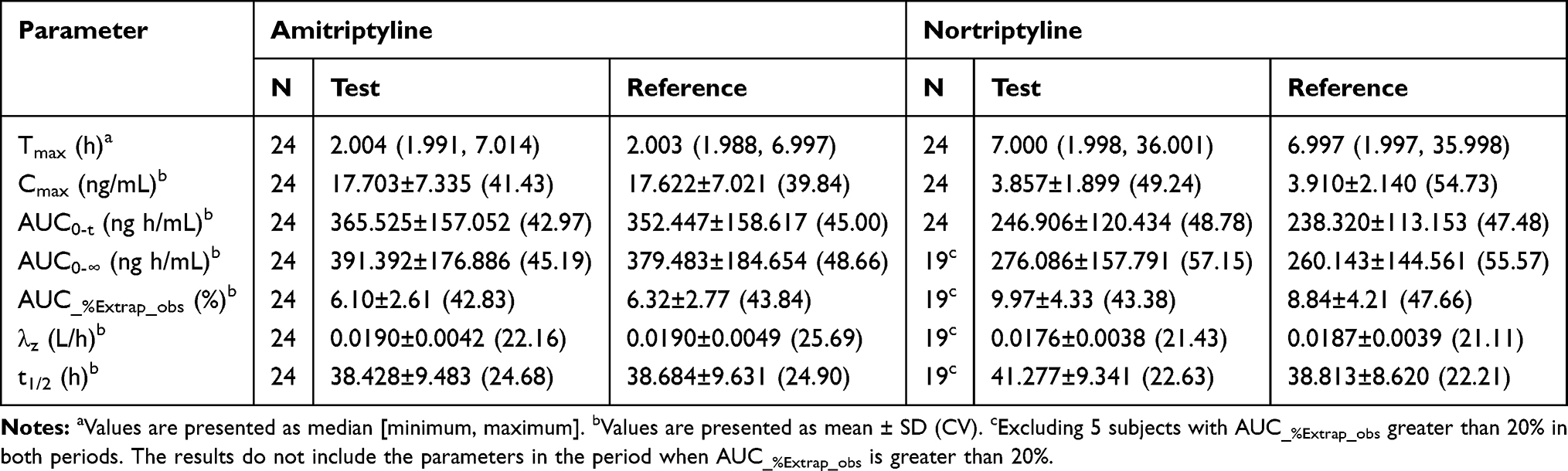 |
Table 3 Pharmacokinetic Parameters of Amitriptyline and Nortriptyline After Single Oral Administration of Test and Reference Amitriptyline Hydrochloride Tablet Under Fasting Condition |
 |
Table 4 Pharmacokinetic Parameters of Amitriptyline and Nortriptyline After Single Oral Administration of Test and Reference Amitriptyline Hydrochloride Tablet Under Fed Condition |
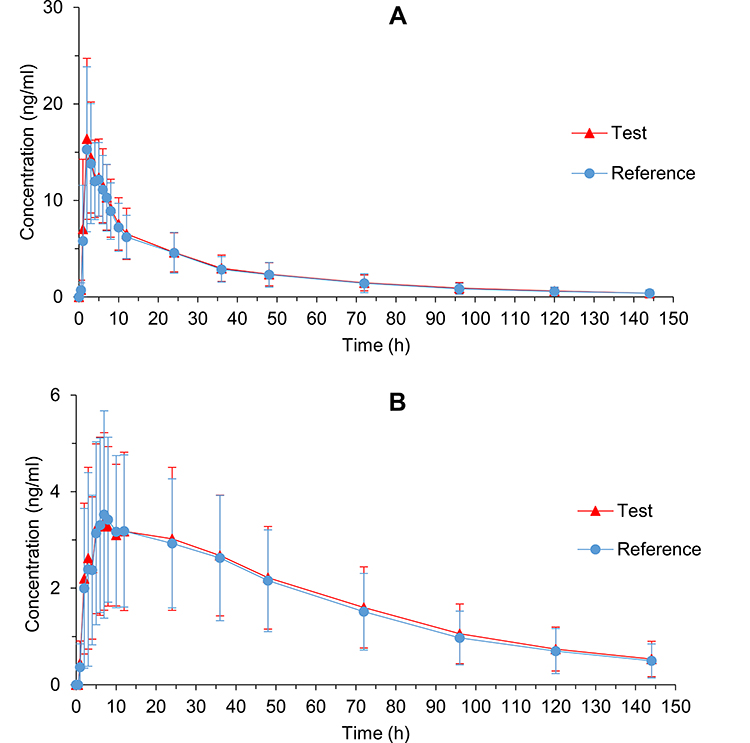 |
Figure 2 Mean plasma concentration-time profiles of amitriptyline (A) and nortriptyline (B) after single oral administration of reference and test amitriptyline hydrochloride tablet in 24 healthy Chinese volunteers under fasting condition. Data represent the mean value for the 24 volunteers, and error bars represent the SD. |
 |
Figure 3 Mean plasma concentration-time profiles of amitriptyline (A) and nortriptyline (B) after single oral administration of reference and test amitriptyline hydrochloride tablet in 24 healthy Chinese volunteers under fed condition. Data represent the mean value for the 24 volunteers, and error bars represent the SD. |
For bioequivalence evaluation, all the randomized 48 subjects were considered. Subjects whose nortriptyline AUC_%Extrap_obs values exceeded 20% were not considered in the evaluation of the equivalence. The 90% CIs for the GMR of pharmacokinetic parameters (Cmax, AUC0–t, and AUC0-∞) for both amitriptyline and nortriptyline between the test and reference products were all within 80% to 125% under both fasting and fed conditions (Tables 5 and 6). Therefore, the test and reference products were considered bioequivalent.
 |
Table 5 Geometric Mean Ratios (GMR) and the Corresponding 90% CIs for the Primary Pharmacokinetic Parameters of Amitriptyline and Nortriptyline Under Fasting Condition |
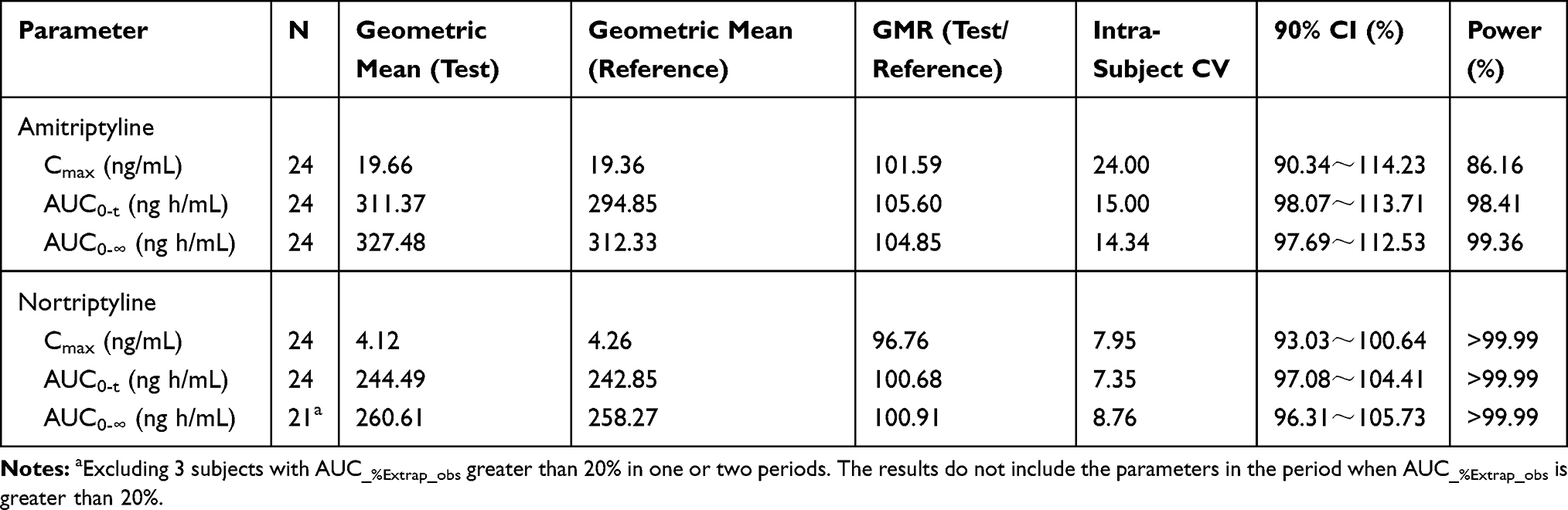 |
Table 6 Geometric Mean Ratios (GMR) and the Corresponding 90% CIs for the Primary Pharmacokinetic Parameters of Amitriptyline and Nortriptyline Under Fed Condition |
Safety Assessment
During the study, all subjects received at least one dose of the study drug and were included in the safety analysis. During the fasting study, 83 AEs were recorded in all 24 subjects taking the test and reference products. The incidence of AEs of the test product was 100% (24/24), while that of the reference drug was 91.67% (22/24). All AEs were mild and reported as grade 1, except for one case of serum triglyceride increase after drug administration, which was reported as grade 2. In the fed study, 86 AEs were recorded in 24 subjects taking the test and reference products. The incidence of AEs of the test product was 95.83% (23/24); meanwhile, that of the reference was 100% (24/24). All AEs were mild and reported as grade 1, except for grade 3 sinus bradycardia in one case and grade 2 hypotension in another case. Drowsiness was the most frequently reported AE, and one of the most commonly described with the use of amitriptyline hydrochloride.22 All AEs were spontaneously resolved without any specific treatment under fasting and fed conditions. The test and reference products were well tolerated and did not elicit serious adverse events (SAEs). In addition, no subject withdrew from the study due to AE (Table 7).
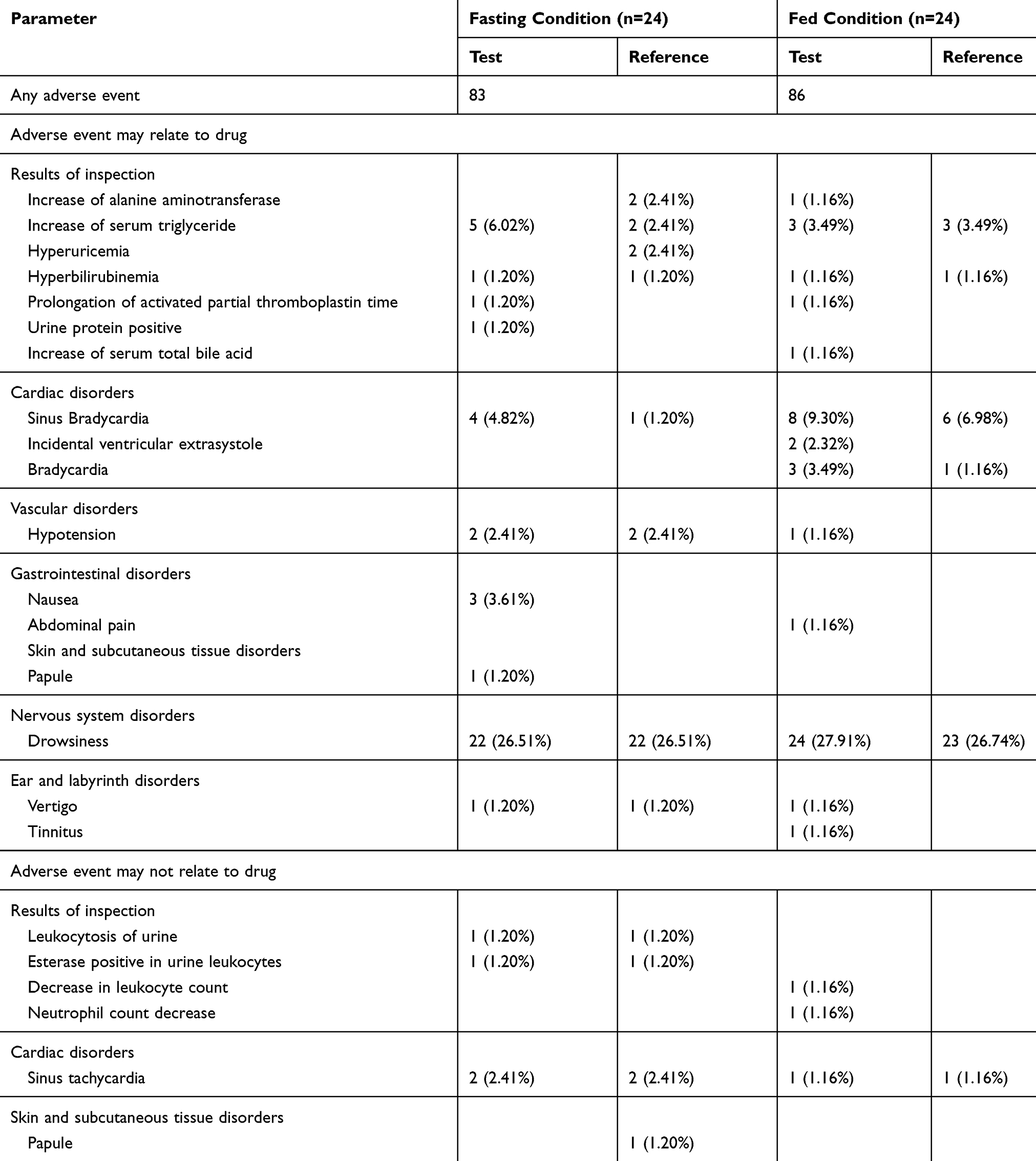 |
Table 7 Total Number of Adverse Events and Percentage of Healthy Subjects Experiencing Adverse Events in the Fasting or Fed Study. Values are Given as No. (%) |
Discussion
This study compared the pharmacokinetic characteristics of the test and reference products in healthy Chinese subjects under fasting and fed conditions. Both products were well tolerated, and no SAEs were reported. Bioequivalence was established considering the Cmax, AUC0-t, and AUC0-∞ of amitriptyline in both fasting and fed conditions. Statistical analysis of t1/2 and Tmax for amitriptyline between the test and reference products under both fasting and fed conditions showed no significant difference when using the non-parametric method (P > 0.05). However, the t1/2 of nortriptyline was significant different between the test and reference products under fasting condition (Table 8). In the fasting study, 5 subjects whose AUC_%Extrap_obs for nortriptyline exceeded 20% in both periods were excluded from the analysis, which may have contributed to the significance of t1/2. Amitriptyline undergoes demethylation forming the major metabolite nortriptyline.14 Both amitriptyline and nortriptyline are active pharmaceutical ingredients and treat depression.23 According to FDA’s Draft Guidance on Amitriptyline Hydrochloride,24 the bioequivalence of the test and reference products is primarily determined by pharmacokinetic parameters (Cmax, AUC0-t, and AUC0-∞) of amitriptyline. The results of nortriptyline confirmed the bioequivalence between the generic and reference drugs.
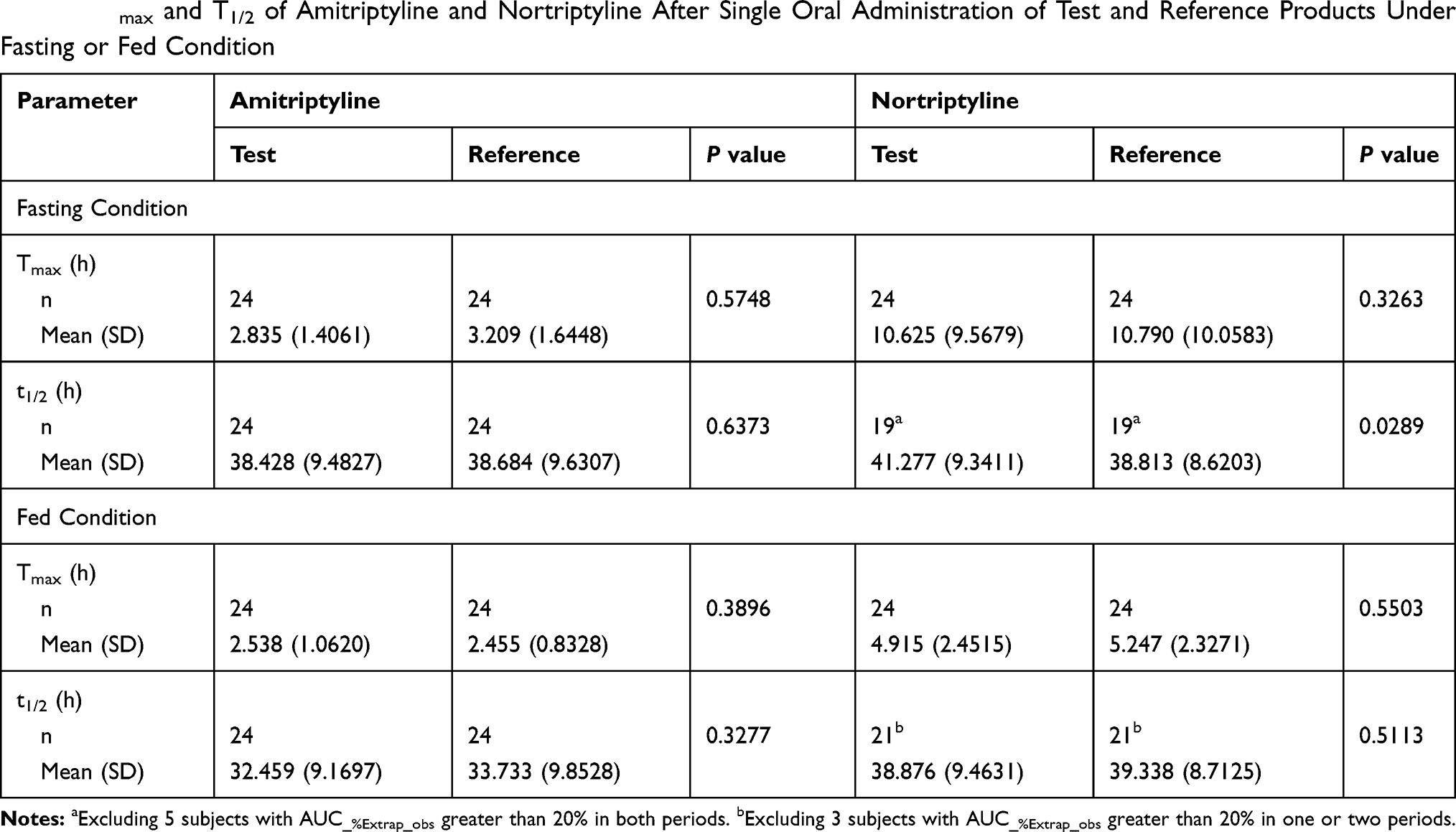 |
Table 8 Tmax and T1/2 of Amitriptyline and Nortriptyline After Single Oral Administration of Test and Reference Products Under Fasting or Fed Condition |
Under fasting and fed conditions, nortriptyline AUC_%Extrap_obs values were > 20% for 5 subjects in both periods and 3 patients in one or two periods, respectively, possibly due to insufficient blood collection time. Thus, a longer blood collection time may be necessary. In addition, subjects were not affected by the carryover effect since the amitriptyline and nortriptyline concentrations in the 2nd period were less than 5% Cmax, which proved enough washout time.
The pharmacokinetic parameters of amitriptyline in this study were compared with those previously reported.25 The observed Cmax for amitriptyline under fasting conditions was similar to previous reported, which validated our results. However, amitriptyline t1/2 in this study was much longer than what is previously reported (24 h). Compared to previous reports, AUC0-∞ increased by approximately 30% (296.87 ± 124.99 ng h/mL in the literature), while Tmax decreased by approximately 40% (the median value of 3.25 h in the literature).
The pharmacokinetic difference between the parameters of this study and previous studies maybe influenced by different drugs’ manufacturers.25 The amitriptyline hydrochloride used in literature is produced by Merck & Co, Inc., while the reference product in here was made by Sandoz Inc., US. Ethnicity difference could also be a reason, since previous studies were conducted using Korean subjects, while Chinese subjects were used in this study. In addition, the analytical determination methods may also play a role. Higher precision of the analytical instrument allows for detection of residual concentrations of chemicals, thus concentration-time curves closer to the actual pharmacokinetic characteristics can be obtained.
Furthermore, pharmacokinetic data under fasting and fed conditions were compared. Tables 3 and 4 indicate that food had an impact on the pharmacokinetic processes of amitriptyline and nortriptyline, regardless of using the test or reference product. With the addition of standard high-fat breakfast before administration, Cmax of amitriptyline increased by approximately 20%. Lipophilic amitriptyline could have been absorbed with fat into the lacteals and therefore avoided the liver first-pass effect. In this case, the resulting higher plasma amitriptyline levels might have increased the amitriptyline Cmax.26 Conversely, amitriptyline Tmax did not significantly change. Food inhibits the rate of gastric emptying, which increased the proportion of drugs dissolved prior to entering the small intestine thus delaying the rate of drug absorption.27 The dissolution of lipophilic amitriptyline in bile salt micelles may promote drug absorption. Both the rate of gastric emptying and the lipophilicity of the drug may cause the invariance of Tmax. The amitriptyline t1/2, AUC0−t, and AUC0−∞ decreased; meanwhile, the nortriptyline Tmax was reduced by approximately 28%, and nortriptyline Cmax and AUC0−t and AUC0−∞ were increased by approximately 15%, 10%, and 10%, respectively. One possible explanation is that amitriptyline is preferably absorbed in the gastrointestinal tract and is metabolized in the liver.28 Food can increase the hepatic-splanchnic blood flow, which may improve the metabolism of amitriptyline to nortriptyline.29 This may account for the decreased t1/2, AUC0−t, and AUC0−∞ values of amitriptyline and the increased bioavailability of nortriptyline in the fed study, which confirms that food affected the pharmacokinetics of amitriptyline.
Conclusion
This study was conducted under both fasting and fed conditions, in healthy Chinese volunteers. Both the test and reference products complied with the regulatory criteria for supposing bioequivalence based on Cmax, AUC0–t, and AUC0-∞. Both products were well tolerated and no serious or unexpected AEs were observed.
Data Sharing Statement
Individual deidentified participant data is not going to be shared. And all available data has been showed in the article. No other study-related document will be made available.
Disclosure
Hunan Dongting Pharmaceutical Co., Ltd. (Hunan, China) funded our study, which was the manufacturer of amitriptyline hydrochloride tablets. The funder had not any influence on data collection and analysis, manuscript preparation, and decision to publish. All authors report no conflicts of interest in this work.
References
1. World Health Organization. Depression and other common mental disorders: global health estimates. License: CC BY-NC-SA 3.0 IGO; 2017. Available from: http://www.who.int/iris/handle/10665/254610.
2. Carvalho AF, Sharma MS, Brunoni AR, et al. The safety, tolerability and risks associated with the use of newer generation antidepressant drugs: a critical review of the literature. Psychother Psychosom. 2016;85(5):270–288. doi:10.1159/000447034
3. Hillhouse TM, Porter JH. A brief history of the development of antidepressant drugs: from monoamines to glutamate. Exp Clin Psychopharmacol. 2015;23(1):1–21. doi:10.1037/a0038550
4. Pratt LA, Brody DJ, Gu Q. Antidepressant use in persons aged 12 and over: United States, 2005–2008. NCHS Data Brief. 2011;76:1–8.
5. National Center for Health Statistics. Health, United States, 2010: With Special Feature on Death and Dying. Table 95. Hyattsville, MD; 2011.
6. Vezmar S, Miljkovic B, Vucicevic K, et al. Amitriptyline for depression. Cochrane Database Syst Rev. 2007.
7. Barbui C, Hotopf M. Amitriptyline v. the rest: still the leading antidepressant after 40 years of randomised controlled trials. Br J Psychiatry. 2001;178(2):129–144. doi:10.1192/bjp.178.2.129
8. Cheng Q, Huang J, Xu L, et al. Analysis of time-course, dose-effect, and influencing factors of antidepressants in the treatment of acute adult patients with major depression. Int J Neuropsychopharmacol. 2020;23(2):76–87. doi:10.1093/ijnp/pyz062
9. Thour A, Marwaha R. Amitriptyline. 2020 Apr 20. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan–. PMID: 30725910.
10. Lohse MJ, Müller-Oerlinghausen B. Psychopharmaka. In: Schwabe U, Pfaffrath D, editors. Arzneiverordnungsreport 2009. Heidelberg: Springer; 2009:820–864.
11. Personal communication. GPRD. Available from: http://www.gprd.com/2011.
12. WHO Expert Committee. The selection and use of essential medicines. World Health Organ Tech Rep Ser. 2014;985:
13. Chinese national essential drug catalogue (basic medical and health institutions). China; 2018. Available from: http://www.nhc.gov.cn/wjw/jbywml/201810/600865149f4740eb8ebe729c426fb5d7.shtml.
14. Breyer-Pfaff U. The metabolic fate of amitriptyline, nortriptyline and amitriptylinoxide in man. Drug Metab Rev. 2004;36(3–4):723–746.
15. Krüger R, Hölzl G, Kuss HJ, et al. Comparison of the metabolism of the three antidepressants amitriptyline, imipramine, and chlorimipramine in vitro in rat liver microsomes. Psychopharmacology (Berl). 1986;88(4):505–513. doi:10.1007/BF00178516
16. UpToDate. Tricyclic and tetracyclic drugs: pharmacology, administration, and side effects; 2016 [cited August 2, 2016]. Available from: https://www.uptodate.com/contents/tricyclic-and-tetracyclic-drugs-pharmacology-administration-andsideeffects?source=machineLearning&search=tricyclic+antidepressants&selectedTitle=1~150§ionRank=2&anchor=H31-references.
17. Moore RA, Derry S, Aldington D, et al. Amitriptyline for neuropathic pain in adults. Cochrane Database Syst Rev. 2015;2015(7):CD008242.
18. Hiroki T, Suto T, Saito S, et al. Repeated administration of amitriptyline in neuropathic pain: modulation of the noradrenergic descending inhibitory system. Anesth Analg. 2017;125(4):1281–1288. doi:10.1213/ANE.0000000000002352
19. Rico-Villademoros F, Slim M, Calandre EP. Amitriptyline for the treatment of fibromyalgia: a comprehensive review. Expert Rev Neurother. 2015;15(10):1123–1150. doi:10.1586/14737175.2015.1091726
20. Rampello L, Alvano A, Chiechio S, et al. Evaluation of the prophylactic efficacy of amitriptyline and citalopram, alone or in combination, in patients with comorbidity of depression, migraine, and tension-type headache. Neuropsychobiology. 2004;50(4):322–328. doi:10.1159/000080960
21. Burch R. Antidepressants for preventive treatment of migraine. Curr Treat Options Neurol. 2019;21(4):18. doi:10.1007/s11940-019-0557-2
22. AMITRIPTYLINE HYDROCHLORIDE-amitriptyline hydrochloride tablet, film coated. Durham, NC: Inc, A.H.; 2016. Available from: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=1e6d2c80-fbc8-444e-bdd3-6a91fe1b95bd.
23. Hicks JK, Swen JJ, Thorn CF, et al. Clinical pharmacogenetics implementation consortium guideline for CYP2D6 and CYP2C19 genotypes and dosing of tricyclic antidepressants. Clin Pharmacol Ther. 2013;93(5):402–408. doi:10.1038/clpt.2013.2
24. Draft Guidance on Amitriptyline Hydrochloride. US Food and Drug Administration. USA. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/psg/Amitriptyline_HCl_tab_85966_85969_85968_85971_85967_85970_RC3-10.pdf.
25. Nam Y, Lim CH, Lee HS, et al. Single-dose, randomized, open-label, 2-way crossover study of the pharmacokinetics of amitriptyline hydrochloride 10- and 25-mg tablet in healthy male Korean volunteers. Clin Ther. 2015;37(2):302–310. doi:10.1016/j.clinthera.2014.09.010
26. Burch JE, Hullin RP. Amitriptyline pharmacokinetics. A crossover study with single doses of amitriptyline and nortriptyline. Psychopharmacology (Berl). 1981;74(1):35–42. doi:10.1007/BF00431754
27. Charman WN, Porter CJ, Mithani S, et al. Physiochemical and physiological mechanisms for the effects of food on drug absorption: the role of lipids and pH. J Pharm Sci. 1997;86(3):269–282. doi:10.1021/js960085v
28. Bae SK, Yang KH, Aryal DK, et al. Pharmacokinetics of amitriptyline and one of its metabolites, nortriptyline, in rats: little contribution of considerable hepatic first-pass effect to low bioavailability of amitriptyline due to great intestinal first-pass effect. J Pharm Sci. 2009;98(4):1587–1601. doi:10.1002/jps.21511
29. McLean AJ, McNamara PJ, duSouich P, et al. Food, splanchnic blood flow, and bioavailability of drugs subject to first-pass metabolism. Clin Pharmacol Ther. 1978;24(1):5–10. doi:10.1002/cpt19782415
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.