Back to Journals » Drug Design, Development and Therapy » Volume 13
Bioequivalence Study Of A Fixed-Dose Combination Tablet Containing Melitracen 10 mg And Flupentixol 0.5 mg In Healthy Chinese Volunteers Under Fasted And Fed Conditions
Authors Wu L ![]() , Xu C, Wu G, Zhou H, Lv D, Zhai Y, Huang Y, Tang W, Li F, Shentu J
, Xu C, Wu G, Zhou H, Lv D, Zhai Y, Huang Y, Tang W, Li F, Shentu J
Received 11 March 2019
Accepted for publication 29 August 2019
Published 19 September 2019 Volume 2019:13 Pages 3331—3342
DOI https://doi.org/10.2147/DDDT.S207561
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Cristiana Tanase
Lihua Wu,1,2,* Chang Xu,1,2,* Guolan Wu,1,2 Huili Zhou,1,2 Duo Lv,1,2 You Zhai,1,2 Yujie Huang,1,2 Wenling Tang,3 Fangqiong Li,4 Jianzhong Shentu1–3
1Research Center for Clinical Pharmacy, State Key Laboratory for Diagnosis and Treatment of Infectious Disease, The First Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou, People’s Republic of China; 2Zhejiang Provincial Key Laboratory for Drug Evaluation and Clinical Research, The First Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou, People’s Republic of China; 3College of Medicine, Zhejiang University, Hangzhou, People’s Republic of China; 4Clinical Research Department, Haisco Pharmaceutical Group, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jianzhong Shentu
Research Center for Clinical Pharmacy, State Key Laboratory for Diagnosis and Treatment of Infectious Disease, The First Affiliated Hospital, College of Medicine, Zhejiang University, 79 Qingchun Road, Hangzhou 310003, People’s Republic of China
Tel +86 571 87236560
Fax +86 571 87214223
Email [email protected]
Purpose: A fixed-dose combination (FDC) tablet of melitracen/flupentixol has been widely used for depression. The purpose of this study was to assess the safety profile and the relative bioavailability of two FDC products containing 10 mg melitracen and 0.5 mg flupentixol from two different manufacturers, in order to acquire adequate pharmacokinetic evidence for registration approval of the test formulation.
Methods: The study was designed as a single-dose, randomized, open-label, 2-period crossover study under fasted or fed conditions in healthy Chinese subjects. Twenty-four subjects (16 men and 8 women) were selected for fasted study, and another 24 cases (16 men and 8 women) were in fed study. Each subject was randomized at the beginning to receive either a single dose of the reference FDC or the test FDC tablet during the first period. Following two-week washout period, all subjects received the alternate formulation during the second period. Blood samples were collected up to 144 hrs after administration. Pharmacokinetic parameters, including Cmax, Tmax, AUC0-t, AUC0-∞, t½, CL/F, and Vd/F were acquired based on the time versus concentration profiles. Then, the geometric mean ratios (GMR) and corresponding 90% CIs were calculated for the determination of bioequivalence analysis. Safety assessment included changes in vital signs and laboratory tests, physical examination findings, and incidence or reports of adverse events (AEs).
Results: The present study has clearly indicated the test and the reference FDC products are bioequivalent in terms of rate and extent of drug absorption. GMR of Cmax, AUC0–t, and AUC0-∞ for both flupentixol and melitracen between the two formulation FDC products, and corresponding 90% CIs, were all within the range of 80% to 125% under fasted or fed conditions. Both the test and the reference FDC products indicated good tolerance in all volunteers. Chinese Clinical Trials Registry identifier: CTR20171256.
Keywords: bioequivalence, melitracen, flupentixol, pharmacokinetics, fixed-dose combination tablet
Introduction
Depression is becoming increasingly common worldwide, with more than 300 million people affected. It is ranked by WHO as a leading cause of global disability. At its worst, depression can lead to suicide deaths whose number is close to 800,000 per year.1 Decades of efforts have been taken to give birth to series of antidepressants like tricyclic antidepressants (TCAs), monoamine oxidase inhibitors, selective serotonin reuptake inhibitors (SSRIs), serotonin-noradrenaline reuptake inhibitors (SNRIs), etc.2,3 An estimate indicates that antidepressants were the third most frequently prescribed drugs taken by individuals between 2005 and 2008 in the USA.4 Furthermore, it is reported that Deanxit, the fixed-dose combination (FDC) tablet of melitracen/flupentixol, is the most frequent antidepressant prescription in China in terms of mean defined daily doses.5
The FDC tablet of melitracen/flupentixol is a fixed combination of 10 mg melitracen (a kind of tricyclic antidepressant) and 0.5 mg flupentixol (a classical antipsychotic component). It has been proven not only a rapid onset with anxiolytic, antidepressant, and activating properties in low doses but also less side effects by the reason of lower dosage of both chemicals.6 It may be clinically a reasonable alternative to SSRI treatment, especially in depression with psychotic features. It is also worth noting that except for anti-depression, Deanxit is also available as a concomitant medication in the treatment of other clinical conditions in China. For instance, it is effective with mosapride in the treatment of gastrointestinal disorders,7 with clonazepam in the treatment of tinnitus,8 and with trimebutin maleate in the treatment of irritable bowel syndrome.9
Although the FDC tablet of melitracen/flupentixol has been widely prescribed for more than 2 decades, only a few studies have been conducted providing the evidence for efficacy and tolerability of this combination in depressive syndromes or other disease conditions. So far, data concerning pharmacokinetic characteristics are very limited. The aim of the present study was to assess the relative bioavailability of two FDC products (test and reference) containing melitracen 10 mg and flupentixol 0.5 mg under fasting or fed conditions in healthy Chinese adult volunteers. The study was conducted to meet China Food and Drug Administration requirements for marketing of the new generic formulation. (Chinese Clinical Trials Registry identifier: CTR20171256).
Materials And Methods
Study Drugs
The test formulation is Lepan® tablet from Hasico Pharmaceutical Group, Sichuan, China (batch number 170201, expiry date 2020/02/27). The reference formulation is Deanxit® tablet, a commercially available original FDC preparation from Lundbeck A/S, Copenhagen, Denmark (batch number 2508833, expiry date 2019/02).
Subjects
Suitable Chinese male and female adults aged from 18 to 45 years, with a body mass index ranging from 19 to 26 kg/m2, were recruited as healthy volunteers. They provided written informed consents to participate in the study after being well informed about the study objectives, procedures, and possible risks. Then, all the subjects underwent a comprehensive medical examination to assess their health status, including routine physical examination, medical history, laboratory investigation (hematology, blood biochemistry, coagulation function, urinalysis, drug screening, hepatitis/HIV testing), 12-lead electrocardiography, and chest X-ray. Subjects with a history of allergy or sensitivity to any ingredient in the FDC tablet, of hepatic or renal impairment, or of drug or alcohol abuse were excluded. Subjects who had used medications of any kind within 4 weeks or food supplement within 2 weeks before first dosing, and female subjects who were pregnant, breastfeeding, or likely to become pregnant were also excluded.
Study Design And Treatment
This study was carried out at the Phase I Clinical Research Center of the First Affiliated Hospital, College of Medicine, Zhejiang University, China, in accordance with the Declaration of Helsinki,10 the International Conference on Harmonization’s Guideline for Good Clinical Practice.11 It composed of two separate parts: one was under fasted conditions and the other was under fed conditions. Each part was conducted according to a randomized, open-label, single-dose, 2-treatment, and 2-period crossover design. The protocol was reviewed and approved by the ethics committee of the First Affiliated Hospital, College of Medicine, Zhejiang University (approval No. 2017-EC-62).
Specifically, subjects were randomly assigned to Group A or Group B at the beginning of the study. Group A received the test FDC products in the first treatment period and the reference in the second, and the administration sequence was vice versa in Group B. The two dosing periods were separated by a 2-week washout phase. For subjects under fasted conditions, a single dose of the test or the reference FDC tablet was administrated orally with 240 mL warm water following an overnight fast of at least 10 hrs, while for those subjects under fed conditions, they followed a similar dosing scheme except for an additional standard high-fat breakfast [30.3% carbohydrate, 17% protein, and 52.7% fat] started 30 mins prior to administration. A thorough mouth check was performed after each dosing. The volunteers were ambulatory, prohibited from strenuous activity, and closely monitored by qualified staff throughout the entire confinement period of blood sampling. Water intake was withheld for at least 2 hrs after dosing. Standardized lunch and dinner were provided at 4 and 10 hrs after administration, respectively.
Blood Sampling And Analytical Determinations
During each treatment period, a series of blood samples were collected prior to and following administration. Blood samples (4 mL) were drawn into coded, K2-EDTA anticoagulation tubes predose (baseline) and at 0.5, 1, 2, 3, 4, 5, 6, 7, 8, 10, 12, 24, 48, 72, 96, 120, and 144 hrs postdose, and then centrifuged at 1710×g at 4°C for 10 mins. Plasma samples were separated and stored at –20°C within 2 hrs and transferred to −70±10°C freezer in 48 hrs for storage until taking to analyzation. Since these two main compounds are sensitive to light and can be degraded by light,12 all blood samples were light-proof during collecting, processing to storage. Plasma concentrations of both flupentixol and melitracen were measured by LC–MS/MS methods which were validated previously by WuXi AppTec, Shanghai. The method involved a repeated solid-phase extraction and the quantitation of the target compounds was determined in a positive ion mode and multiple reaction monitoring (MRM). The analytes were chromatographed by Shimadzu LC-30 and analyzed by tandem mass spectrometry API 5500. Data acquisition was performed with Analyst software, version 1.6.3 (Applied Biosystems). The linearity range of the method was 0.0100–10.0 ng/mL for flupentixol and 0.100–100 ng/mL for melitracen. The variation coefficient of the low, medium, high, and geometric mean control samples was 3.2–17.5% for flupentixol and 5.1–7.8% for melitracen.
Safety Assessment
Safety assessment included changes in vital signs and laboratory tests, physical examination findings, and incidence or reports of adverse events (AEs). Vital signs, such as temperature, blood pressure, pulse, and respiratory rate, were measured before dosing and at 2 and 4 hrs after each dose. Whereas, the laboratory tests, such as hematology, biochemistry, urinalysis, along with physical examination and 12-lead ECG, were performed at baseline and at the end of the study. Any AEs occurring during the study would be collected by physicians from direct observation, spontaneous reports by volunteers, medical conditions and nonspecific inquiry during the whole trial (both in hospital and at discharge).
Pharmacokinetic And Statistical Analysis
Pharmacokinetic parameters of flupentixol and melitracen were calculated by using a non-compartmental method with Phoenix WinNonlin software, version 6.3(Certara, L.P., St. Louis, MO). Individual plasma concentration–time curves were constructed. Cmax and Tmax were obtained directly from the observed data. AUC0–t was calculated using the linear trapezoidal rule. AUC0–∞ was calculated as the sum of AUC0–t and the extrapolated area determined by dividing the last quantifiable concentration (Ct) by the slope of the terminal log-linear phase (Ke). The apparent total clearance of the drug from plasma after oral administration (Cl/F) was calculated as dose/AUC0–∞. The apparent volume of distribution (Vd/F) was based on the terminal elimination phase (Cl/F/Ke). The elimination half-life (t1/2) was calculated from the slope of the terminal log-linear phase as 0.693/Ke. The relative bioavailability (F) of the tested formulation was calculated as follows: F=AUC0-t(test)/AUC0-t(reference)*100%.
Statistical analysis was performed with the statistical software package SAS Enterprise Guide (V7.1) (SAS Institute Inc, Cary, North Carolina) using the General Linear Model (GLM) procedure. AUC0-∞, AUC0-t, and Cmax were considered primary variables. Determination of bioequivalence, recommended by the Chinese regulatory guideline, was evaluated by the factorial analysis of variance (ANOVA) for crossover design and calculating of 90% confidence intervals (CIs) of the ratio test/reference. Thus, ANOVA was used to assess the effect of formulation, sequence, period, and subjects nested in sequence on natural logarithm(ln)-transformed PK parameters (AUC0-∞, AUC0-t, and Cmax). Parametric 90% confidence intervals (CIs) for the ratio in the geometric mean ratios (GMR) between the two formulations (test–reference) were determined using the Schuirmann method. The two products were considered bioequivalent if the difference between two compared parameters was found statistically insignificant (P>0.05) and 90% CIs for the GMR of AUC0-∞, AUC0-t and Cmax fell within the range of 80% to 125%.
Results
Participants
As shown in Figure 1, from November 22, 2017, to February 27, 2018, a total of 109 healthy Chinese adult volunteers were screened; ultimately, 48 participants were enrolled. Twenty-four subjects (16 men and 8 women) were selected for fasted study, and another 24 cases (16 men and 8 women) were in fed study. Tables 1 and 2 summarize the demographic characteristics of the subjects.
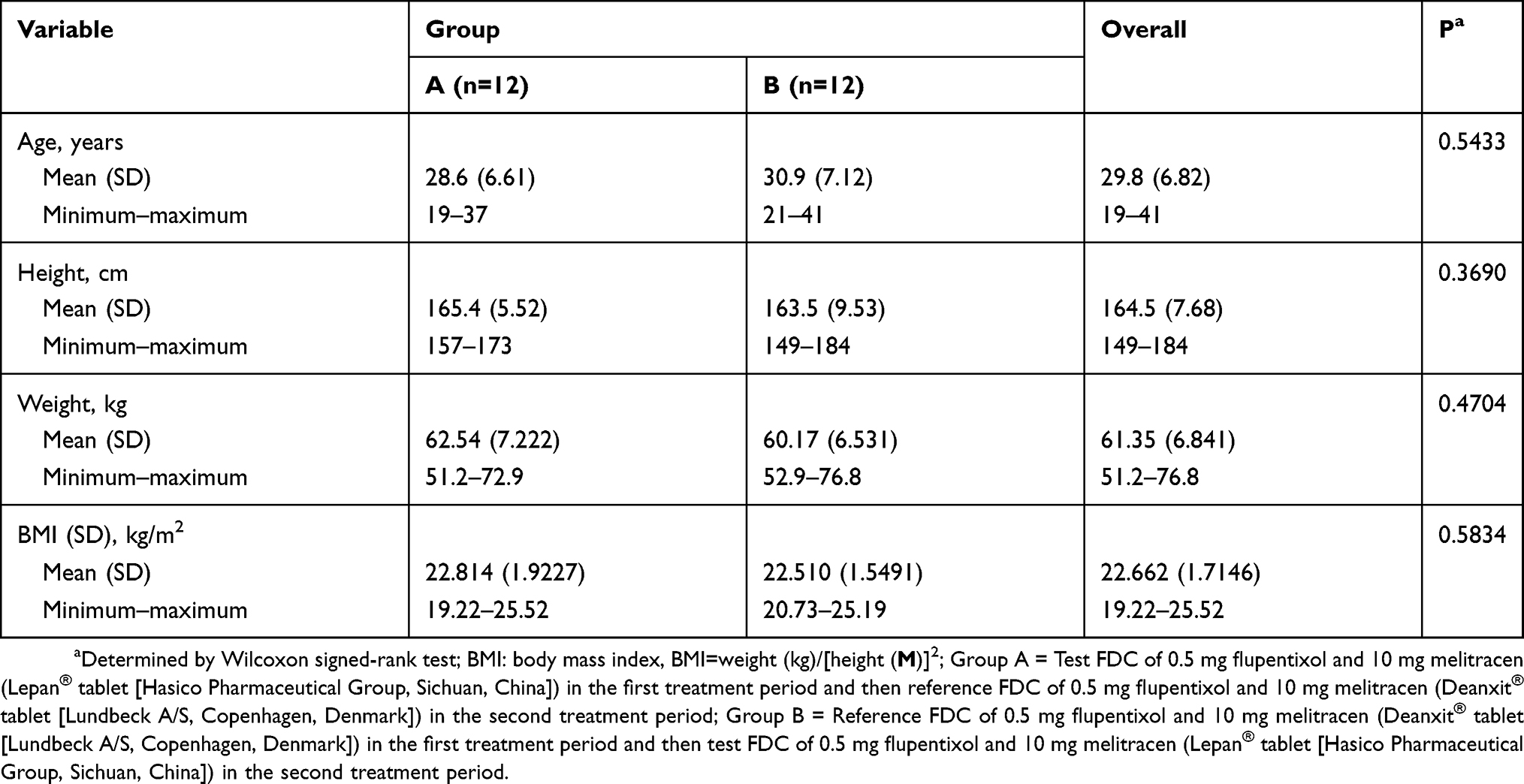 |
Table 1 Demographic Characteristics Of Volunteers Of The Fasted Study (n=24) |
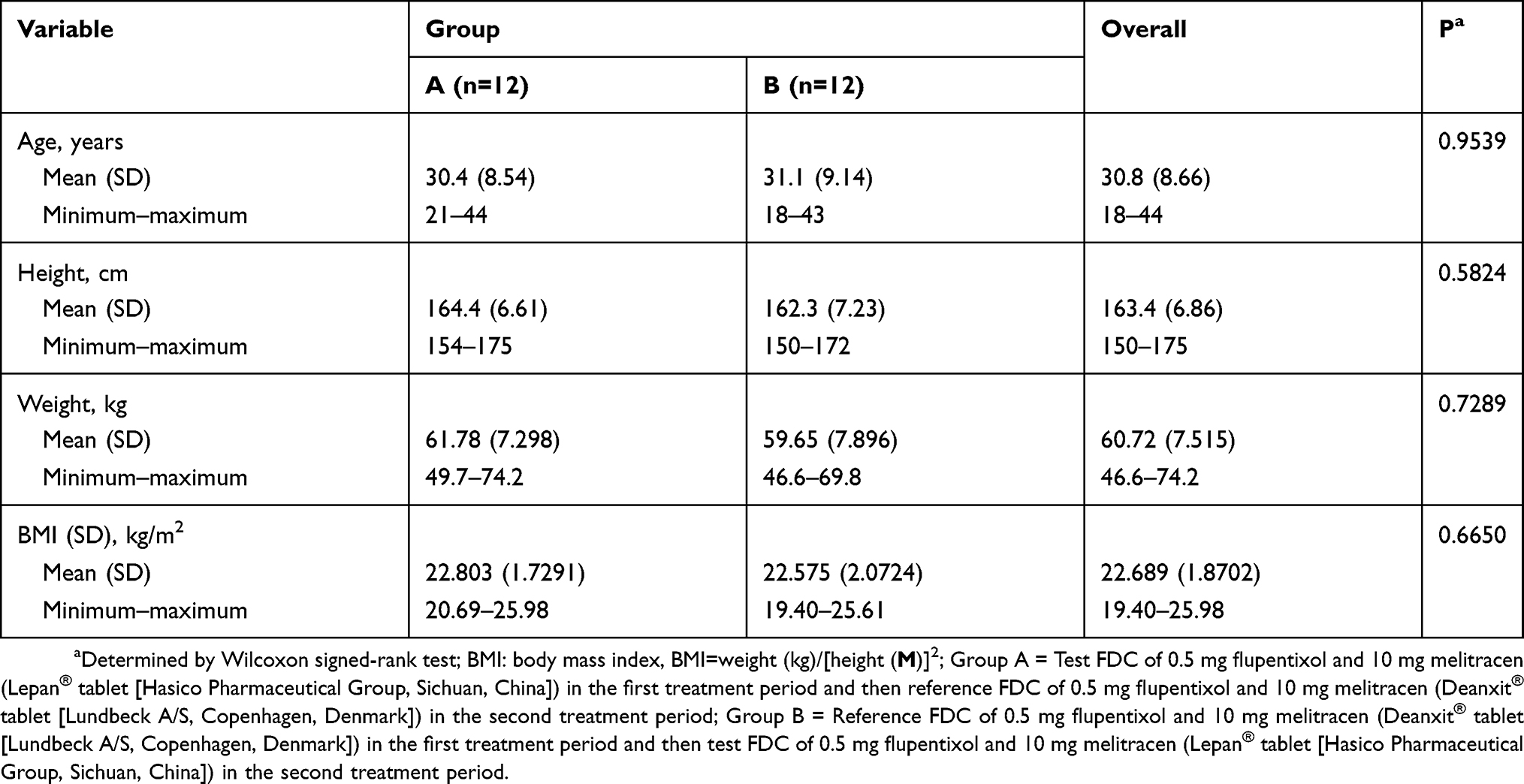 |
Table 2 Demographic Characteristics Of Volunteers In The Fed Study (n=24) |
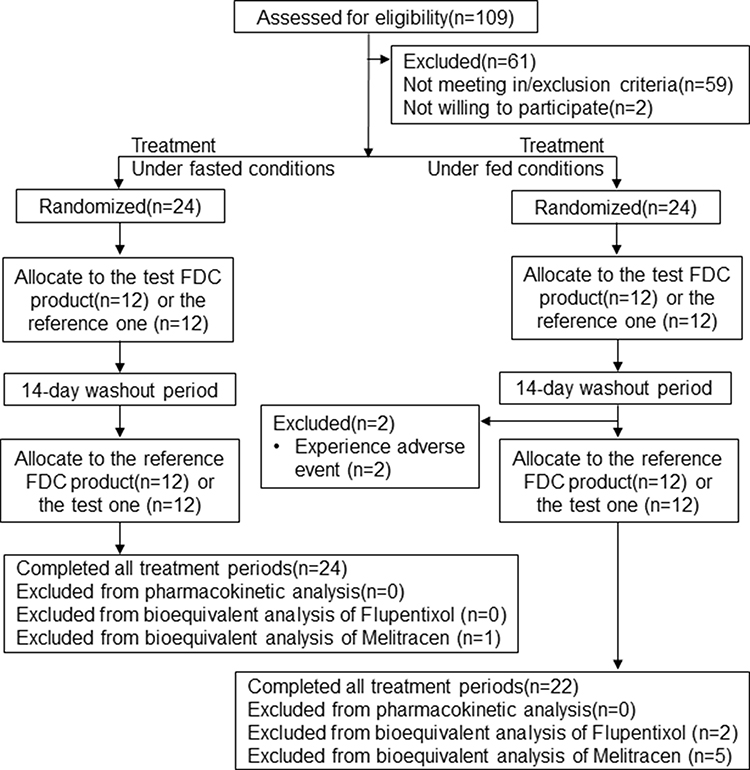 |
Figure 1 Study design and disposition of subjects. |
Pharmacokinetic Properties
All 24 randomized subjects completed both periods in the fasted study and were included in the pharmacokinetic analyses. In the fed study, 2 cases in Group A were withdrawn due to sustained hypertension and abnormal ECG manifestation before the second treatment period dosing. Consequently, only 22 subjects were included in the pharmacokinetic analysis for the reference FDC tablet, while 24 subjects for the test. The mean plasma concentration–time profiles of flupentixol and melitracen obtained after single oral administration of the test and reference FDC products under fasted and fed conditions are shown in Figures 2 and 3. Major pharmacokinetic parameters of flupentixol and melitracen under fasted or fed conditions are summarized in Tables 3 and 4. The elimination half-life (t½) of flupentixol is about 53 hrs and that of melitracen is about 60–73 hrs.
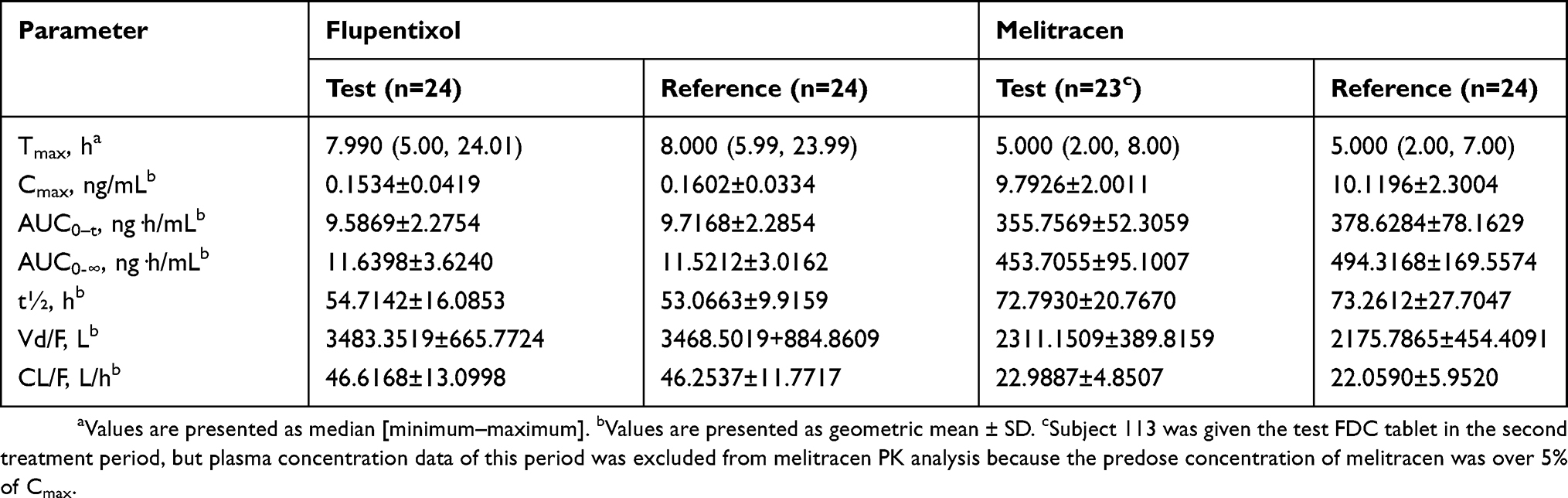 |
Table 3 Pharmacokinetic Parameters Of Flupentixol And Melitracen After Single Oral Administration Of Test And Reference FDC Tablet Under Fasted Conditions |
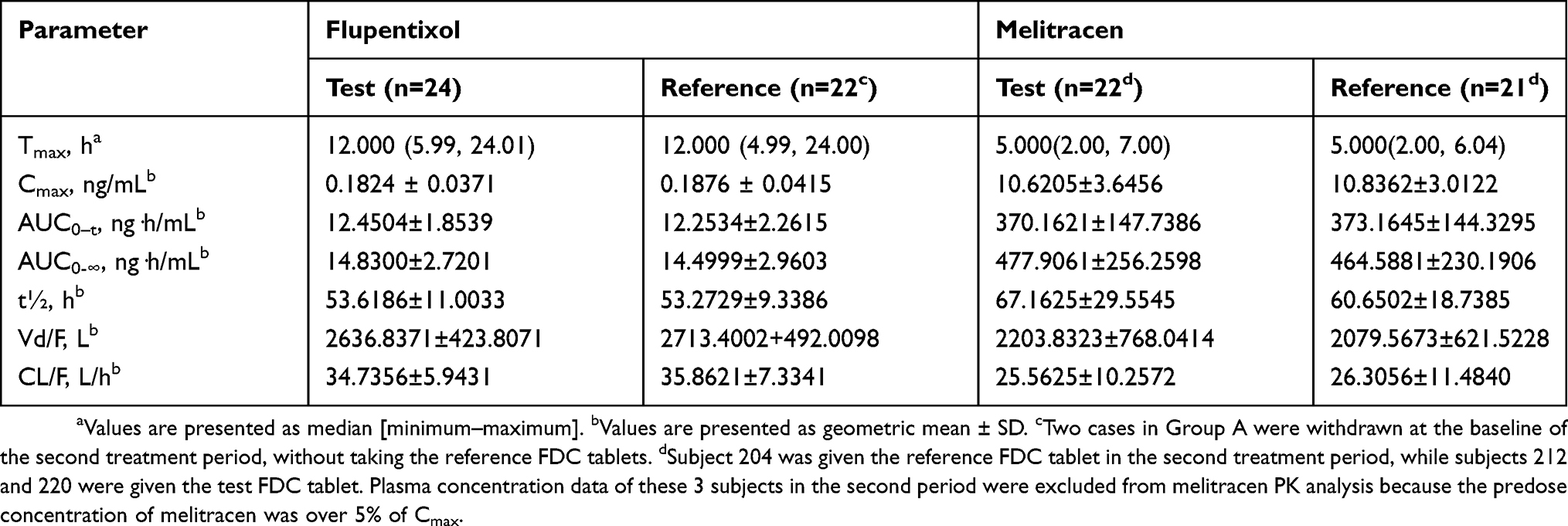 |
Table 4 Pharmacokinetic Parameters Of Flupentixol And Melitracen After Single Oral Administration Of Test And Reference FDC Tablet Under Fed Conditions |
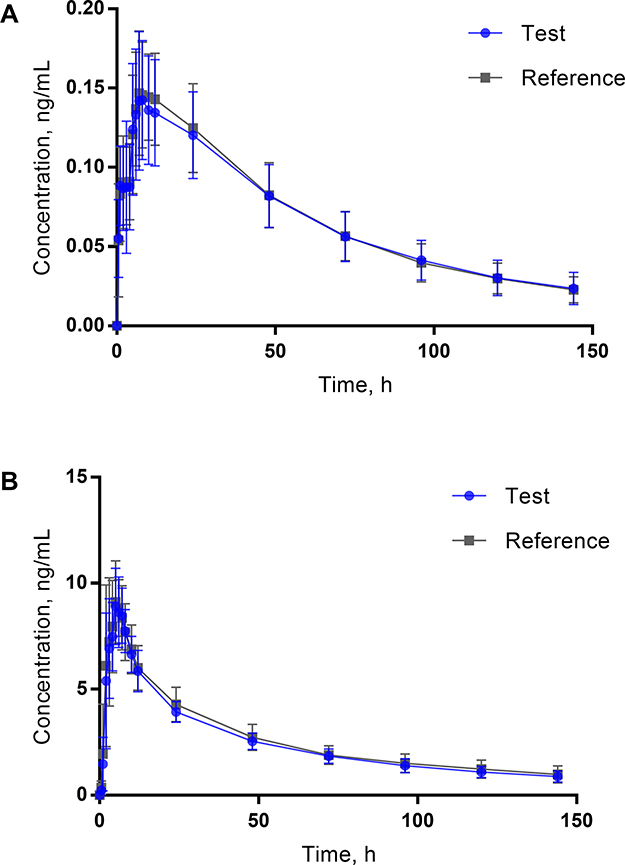 |
Figure 2 Mean plasma concentration-time profiles of flupentixol (A) after single oral administration of reference (n=24) and test (n=24) FDC tablet and of melitracen (B) after single oral administration of reference (n=24) and test (n=23) FDC tablet under fasted conditions. Data represent the mean value, and error bars represent the SD. |
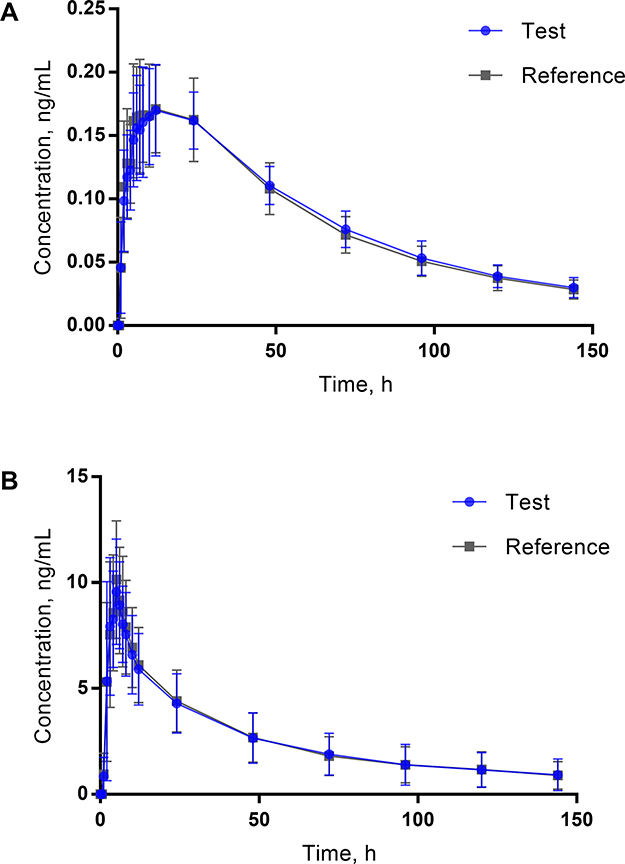 |
Figure 3 Mean plasma concentration–time profiles of flupentixol (A) after single oral administration of reference (n=22) and test (n=24) FDC tablet and of melitracen (B) after single oral administration of reference (n=21) and test (n=22) FDC tablet under fed conditions. Data represent the mean value, and error bars represent the SD. |
As for bioequivalence evaluation, cases (1 case in the fasted study and 3 cases in the fed study) with the predose concentration of melitracen in the second treatment period being over 5% of Cmax were excluded. The predose melitracen concentration in the second treatment period was either below the lower limit of quantitation (BLQ) or under 5% of Cmax in other cases. Therefore, in the fasted study, 24 individuals’ data were used for flupentixol, and only 23 were used for melitracen. In the fed study, 2 subjects were excluded because of their absence in second treatment period. Thus, 22 subjects who finished the whole study were used in the bioequivalence analysis of flupentixol in the fed study, while only 19 subjects were used in that of melitracen. Concerning pharmacokinetic parameters (Cmax, AUC0–t, and AUC0-∞) for both flupentixol and melitracen between the test and reference FDC products, GMR, and 90% CIs were all within the range of 80% to 125% under fasted or fed conditions (Tables 5 and 6). Therefore, the two FDC products of melitracen/flupentixol were bioequivalent.
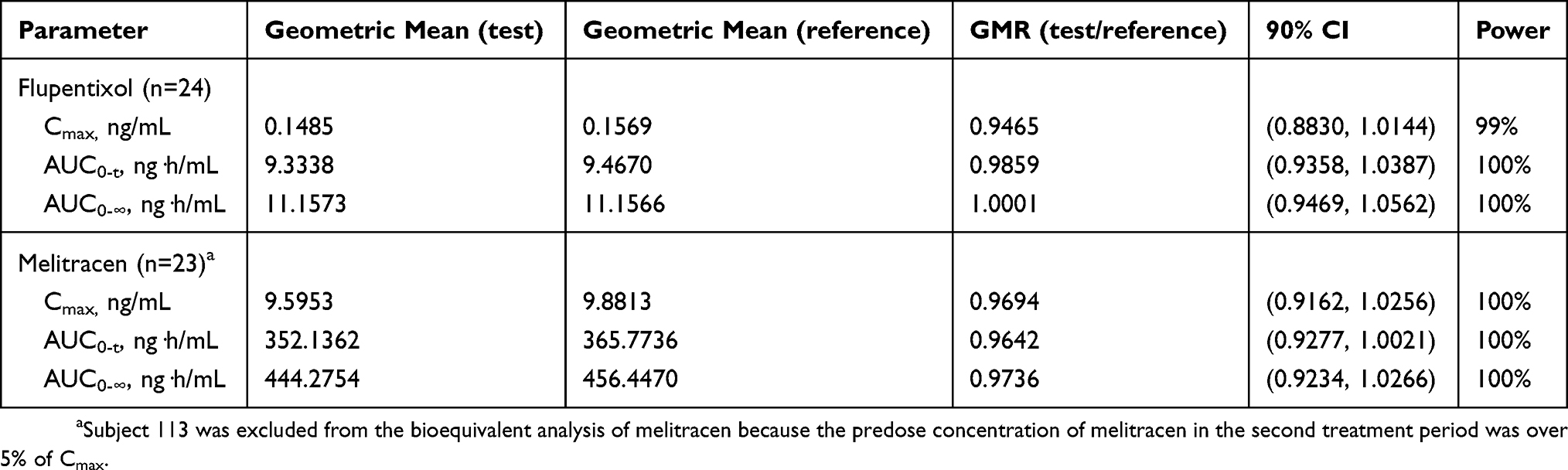 |
Table 5 Geometric Mean Ratios (GMR) And The Corresponding 90% CIs For The Primary Pharmacokinetic Parameters Of Flupentixol And Melitracen Under Fasted Conditions |
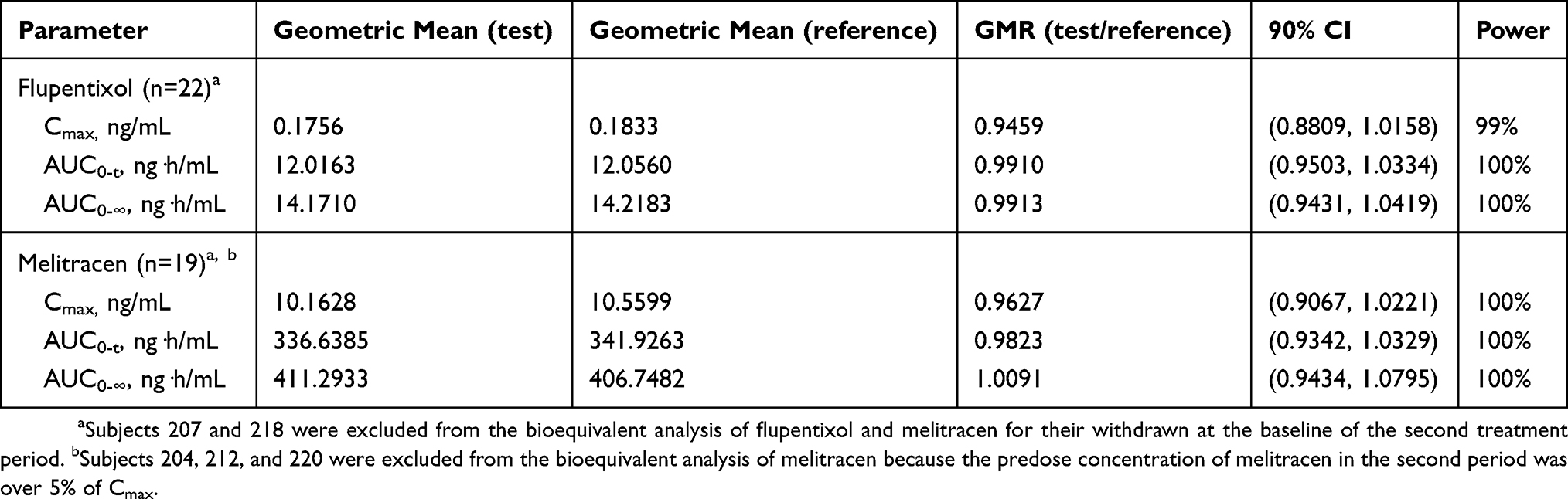 |
Table 6 Geometric Mean Ratios (GMR) And The Corresponding 90% CIs For The Primary Pharmacokinetic Parameters Of Flupentixol And Melitracen Under Fed Conditions |
Safety Assessment
A total of 22 AEs was recorded in 13 subjects during the fasted study; 14 of these AEs (63.6%) were identified through laboratory investigations. The vast majority of AEs (20/22, 90.9%) were transient and considered mild. One case of urinary tract infection as grade 2 and one case of hyperkalemia as grade 3 were observed, which were spontaneously recovered without intervention. In the fed study, a total of 21 AEs was recorded in 11 subjects. All AEs were mild except that one case of urinary tract infection, which was reported as grade 2, and spontaneously recovered. Two subjects were withdrawn before the second treatment period dosing because of sustained hypertension and abnormal ECG manifestation, respectively. The incidence of AEs is summarized in Table 7. No serious AEs were reported.
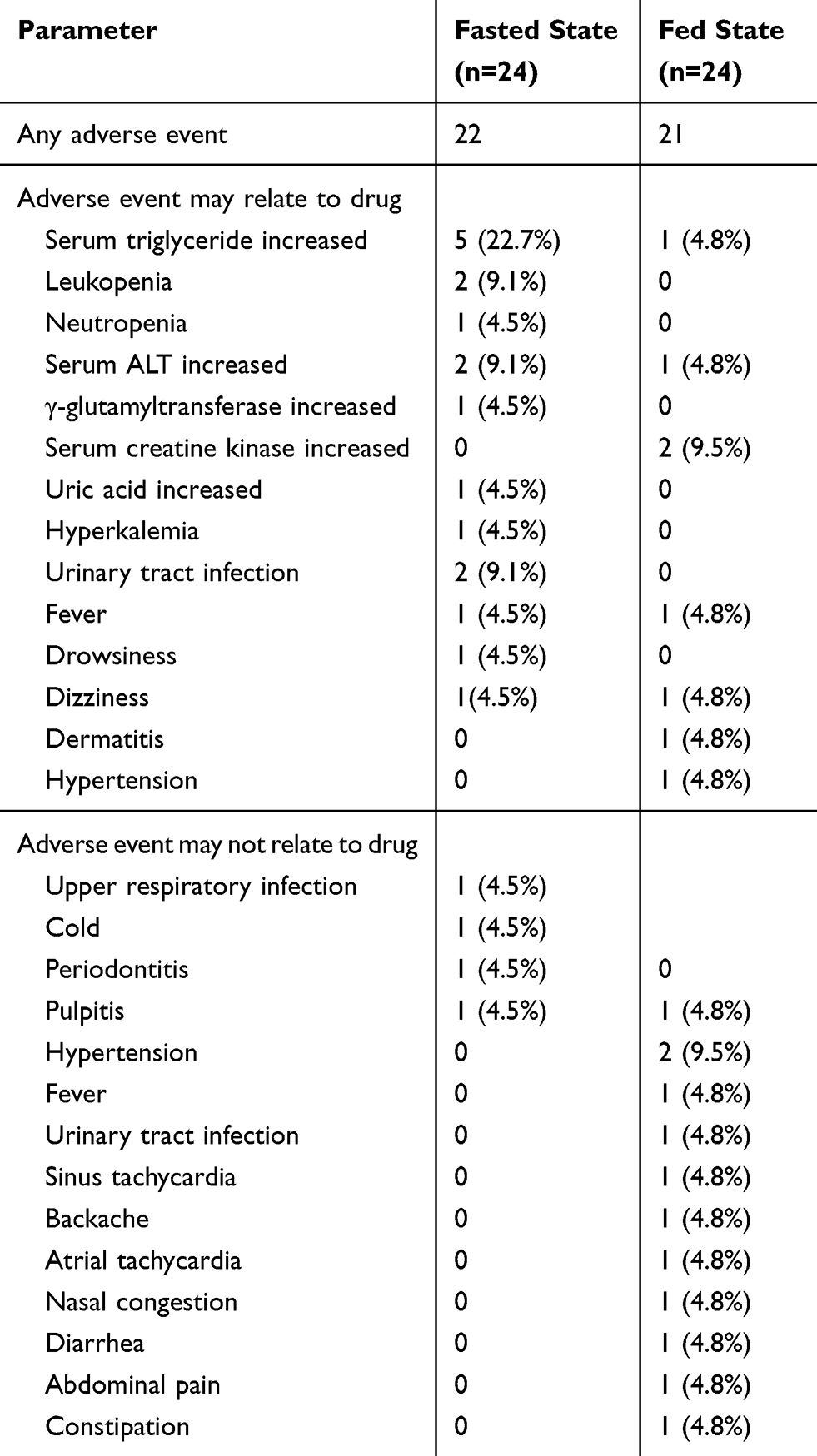 |
Table 7 Total Number Of Adverse Events And Percentage Of Healthy Subjects Experiencing Adverse Events In The Fasted Or Fed Study. Values Are Given As No. (%) |
Discussion
This study compared the pharmacokinetic characteristics of the test FDC formulation and the reference FDC product containing 10 mg melitracen and 0.5 mg flupentixol under fasted or fed conditions. Both formulations were well tolerated, with no serious AEs reported during the study. Bioequivalence was established with respect to Cmax, AUC0-t, and AUC0-∞ values of melitracen and flupentixol, regardless of fasted or fed conditions. Additionally, statistical analysis of t½ and Tmax by non-parametric method also indicated that there was no significant difference between the test and the reference FDC products under fasted or fed conditions (Table 8).
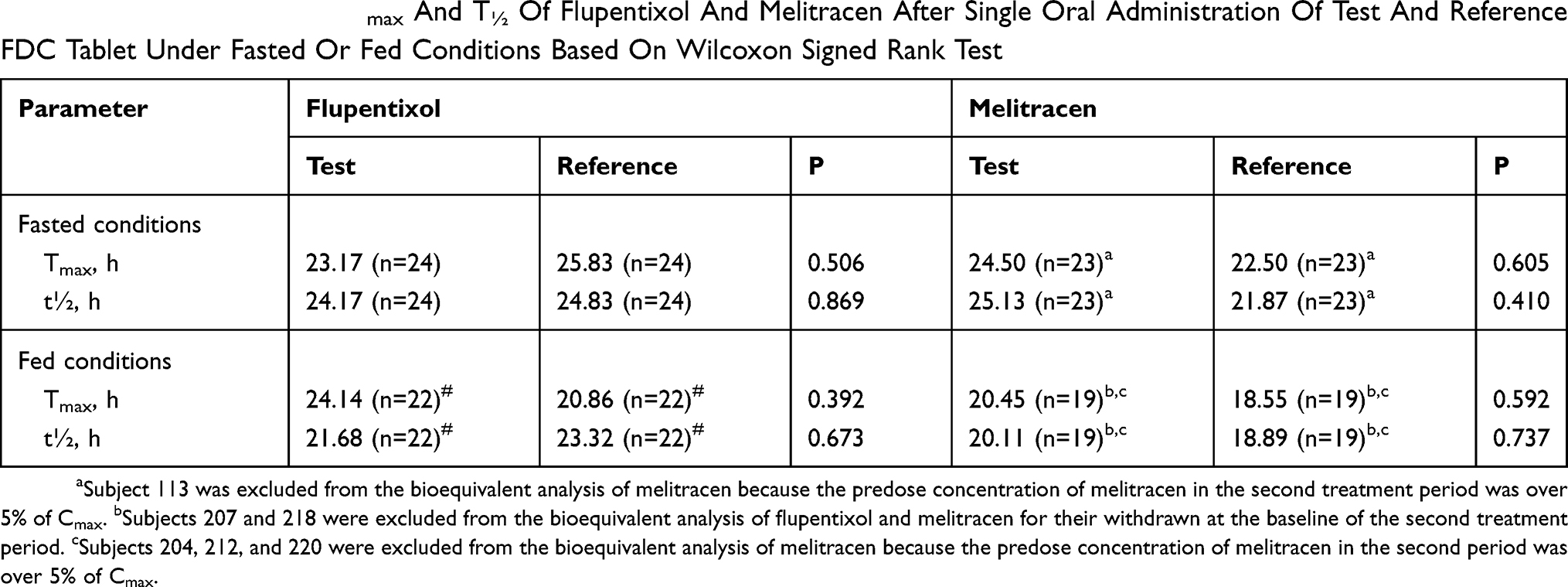 |
Table 8 The Mean Rank Of Tmax And T½ Of Flupentixol And Melitracen After Single Oral Administration Of Test And Reference FDC Tablet Under Fasted Or Fed Conditions Based On Wilcoxon Signed Rank Test |
From the results in the fasted study, Cmax of flupentixol and melitracen were reached after approximately 9 hrs and 5 hrs after oral administration, respectively. The observed Cmax and Tmax for flupentixol and melitracen were similar to those reported in the literature, which enhanced the validity of the present results. However, t½ of flupentixol and melitracen from our study were much longer than the previously published data, where the biological half-life of flupentixol was about 35 hrs and that of melitracen was about 19 hrs.
The t½ difference between our study and previous literature may be due to the analytical determination methods. With the development of the precision of analytical instruments, the residual concentration of chemicals has been caught and detected, which help us to obtain a better c-t curve that is much closer to the actual pharmacokinetic characteristic. Four subjects in our study were affected by carryover effect since the predose melitracen concentration of their second period was over 5% Cmax. Thus, a longer washout time seems to be necessary for melitracen to avoid the carryout effect.
Further, pharmacokinetic data between fasted and fed conditions were compared. As we can see from Tables 3 and 4, food exerted an obvious influence on the pharmacokinetic processes of flupentixol, regardless of the test or reference FDC formulation. With the addition of standard high-fat breakfast before dosing, Tmax of flupentixol increased by 50%, Cmax increased by about 17%, AUC0-t and AUC0-∞ increased by about 30%, while Vd/F and CL/F decreased by about 25%. This change indicated that food not only slowed down the rate but also enhanced the extent of the absorption of flupentixol. As to the case of melitracen, there is no critical change occurred in pharmacokinetic parameters despite the increase of their intersubject CV values. This study turned out to be the first to provide information about food effect on the pharmacokinetics of the FDC of flupentixol and melitracen.
The exposure of flupentixol and melitracen between male and female subjects was also compared and summarized in Tables 9 and 10. As to the test FDC formulation, statistically significant difference in Cmax, AUC0-t, and AUC0-∞ of flupentixol in fed condition existed between female and male subjects. For the reference FDC formulation, Cmax, AUC0-t, and AUC0-∞ of flupentixol in female subjects were higher than that in male subjects but did not reach statistical significance. Further study in a larger group of healthy Chinese individuals would be needed to determine the differences in flupentixol AUC and Cmax between male and female subjects, especially in fed condition. In this study, we did not find obvious differences in melitracen AUC and Cmax between male and female subjects. However, female subjects exhibited a much longer melitracen t½ than male subjects and there turned out to be a statistically significant difference in melitracen t½ of the test FDC formulation (p=0.017). Thus, more attention should be paid to gender when dosing.
 |
Table 9 Pharmacokinetic Parameters Of Flupentixol And Melitracen After Single Oral Administration Of Test and Reference FDC Tablet In Male and Female Subjects Under Fasted Conditions |
 |
Table 10 Pharmacokinetic Parameters Of Flupentixol And Melitracen After Single Oral Administration Of Test And Reference FDC Tablet In Male And Female Subjects Under Fed Conditions |
The combination of the two compounds was designed to enhance the pharmacological effects as well as to lower the AE incidents. In this study, all AEs were mild and with low incidence. No serious AEs were reported. Indeed, the test and the reference FDC products indicated good tolerance in all volunteers.
Conclusions
In this single-dose study conducted under fasting conditions as well as fed conditions in healthy Chinese volunteers, the test and reference FDC products met the regulatory criteria for assuming bioequivalence based on AUC0–t and Cmax. Both formulations were well tolerated.
Data Sharing Statement
Individual deidentified participant data are not going to be shared. And all available data have been shown in the article. No other study-related document will be made available.
Acknowledgments
This work was supported by Haisco Pharmaceutical Group. The authors would like to thank Wei Xu, Weiping Chen, Zhuojun Zhou and Liya Zheng from First Affiliated Hospital, College of Medicine, Zhejiang University, for their clinical assistance. Other coworkers, namely Jian Liu, Xingjiang Hu, Yunliang Zheng, Meihua Lin, Minglan Wu, Qiao Zhang, Juan Xu, Yuanfang Wang also paid a contribution during the whole study. Wuxi AppTec. took responsibility for bioanalytical parts of the study as well as the pharmacokinetics analysis, the statistical analysis, and data interpretation.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work. Lihua Wu and Chang Xu are co-first authors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Depression and other common mental disorders: global health estimates. 2017. License: CC BY-NC-SA 3.0 IGO. Available from: http://www.who.int/iris/handle/10665/254610.
2. Carvalho AF, Sharma MS, Brunoni AR, Vieta E, Fava GA. The safety, tolerability and risks associated with the use of newer generation antidepressant drugs: a critical review of the literature. Psychother Psychosom. 2016;85(5):270–288. doi:10.1159/000447034
3. Hillhouse TM, Porter JH. A brief history of the development of antidepressant drugs: from monoamines to glutamate. Exp Clin Psychopharmacol. 2015;23(1):1–21. doi:10.1037/a0038550
4. Pratt LA, Brody DJ, Gu Q. Antidepressant use in persons aged 12 and over: United States, 2005-2008. NCHS Data Brief. 2011;76(76):1–8.
5. Zhang Y, Becker T, Kosters M. Preliminary study of patterns of medication use for depression treatment in China. Asia Pac Psychiatr. 2013;5(4):231–236. doi:10.1111/appy.12022
6. Xu P, Li H, Zhu Y, et al. Validated liquid–liquid extraction and LC–ESI–MS method for the determination of melitracen in human plasma. Chromatographia. 2008;67(11):935–939. doi:10.1365/s10337-008-0619-1
7. Zhifeng Y. Clinical research on gastrointestinal disorders treated by mosapride combination with flupentixol and melitracen tablets. China Mod Med. 2010;17(18):30–31.
8. Meeus O, De Ridder D, De Heyning PV, et al. Administration of the combination clonazepam-Deanxit as treatment for tinnitus. Otol Neurotol. 2011;32(4):701–709. doi:10.1097/MAO.0b013e31820e737c
9. Xixian C. Observation the effect of trimebutin maleate combined with flupentixol melitracen treatment for irritable bowel syndrome. Guide China Med. 2011;9(3):5–7.
10. World Medical Association. Declaration of helsinki. Available from: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/.
11. The International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH). Guideline for good clinical practice. Available from: https://www.ich.org/products/guidelines/efficacy/efficacy-single/article/integrated-addendum-good-clinical-practice.html.
12. Sultana R. Determination of photolytic degradation of Frenxit (Flupentixol- Melitracen). East West University. 2008.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.