")
Back to Journals » Patient Preference and Adherence » Volume 17
Bioequivalence of Different Formulations of Zonisamide Oral Suspensions: A Short Review
Authors Stević I , Petrović N, Janković SM
Received 9 August 2023
Accepted for publication 2 November 2023
Published 7 November 2023 Volume 2023:17 Pages 2841—2845
DOI https://doi.org/10.2147/PPA.S383038
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Ivana Stević,1 Nemanja Petrović,2 Slobodan M Janković2
1Faculty of Pharmacy, University of Belgrade, Belgrade, Serbia; 2Faculty of Medical Sciences, University of Kragujevac, Kragujevac, Serbia
Correspondence: Slobodan M Janković, Faculty of Medical Science, University of Kragujevac, Svetozara Markovića street, 69, Kragujevac, 34000, Serbia, Email [email protected]
Abstract: To satisfy the needs of pediatric and other patients with focal onset seizures who cannot swallow solid dosage forms of zonisamide, an oral liquid form of this drug is necessary in clinical practice. Although there are two oral suspensions of zonisamide with marketing authorization (MA), there are issues of availability and high cost which limit their use and inspire extemporaneous compounding. Extemporaneously compounded oral suspensions of zonisamide are prepared according to different formulas and vary in stability; therefore it is essential to test this characteristic. Bioequivalence of extemporaneously compounded oral suspensions has never been tested, and the efficacy and safety of zonisamide oral suspensions have generally not been demonstrated in clinical trials. As a narrow therapeutic window drug, zonisamide requires precision in dosing, which could be achieved only with dosage forms with established bioavailability, efficacy, and safety. In order to avoid underdosing and toxicity with zonisamide oral suspensions and utilize their full therapeutic potential, it is necessary to perform bioequivalence studies with each variation of extemporaneously compounded oral suspension and also clinical trials with both commercial and extemporaneous oral suspensions of zonisamide.
Keywords: zonisamide, oral suspension, stability, bioequivalence
Introduction
Zonisamide is an oral anticonvulsant with benzisoxazole nucleus and sulfonamide radical approved as mono- or adjunctive therapy of focal onset seizures with or without secondary generalization in adult or pediatric patients.1 The precise mechanism of action of zonisamide is still unknown. It probably has more than one mechanism of action, such as blockage of voltage-gated sodium and T-type calcium channels, binding for gamma-aminobutyric acid (GABA)-benzodiazepine receptor complex leading to an increase in extracellular GABA, etc. A multitude of mechanisms of action may explain the efficacy of zonisamide in different types of seizures: generalized tonic-clonic seizures, simple and complex focal onset seizures, seizures within the framework of Lennox–Gastaut syndrome, myoclonic epilepsies, and infantile spasms.2,3 Elimination of zonisamide follows linear kinetics; since it is metabolized by two cytochrome isoforms in the liver, it rarely interacts with other anticonvulsants and other drugs in general.4 Protein binding of zonisamide is moderate (40–50%), and the apparent volume of distribution ranges from 1.1 to 1.7 L/kg in adults; parent drug and pharmacologically inactive metabolites are excreted slowly through kidneys, so half-life is almost 60h long, enabling once-daily administration and postponing the establishment of steady-state plasma to 13th −14th day after the therapy initiation.5,6 If zonisamide is used as monotherapy, starting dose is 100 mg once a day, with a recommended dose of 300 mg once a day, and in pediatric patients, dosage recommendation is to start with 1–2 mg/kg/day and to escalate up to 8–12 mg/kg/day until seizure freedom is achieved. If taken with other antiepileptics, starting dose is 50 mg daily divided into two doses, with recommended maintenance dose between 300 mg and 500 mg.7 When zonisamide is tested in clinical trials on patients with epilepsy, main outcomes that are followed are seizure freedom, decrease in frequency of seizures, and time-to-event outcomes (eg, time to 12-month remission from seizures).8
Zonisamide Formulations
The only pharmaceutical form of zonisamide with a valid MA in the European Union is a hard capsule (25 mg, 50 mg, 100 mg).9 However, in addition to hard capsules, the Food and Drug Administration (FDA)10 and Medicines and Healthcare Products Regulatory Agency (MHRA)11 have granted MA to oral suspension of zonisamide (20 mg/mL). The unavailability of a liquid oral formulation of zonisamide in many countries and the high prices of oral suspension (about 10 times higher than the price of hard capsules packages with an equivalent amount of active substance) compelled physicians in many areas of the world to prescribe extemporaneous oral suspension of zonisamide manufactured in local pharmacies.12
Why is Oral Suspension Necessary?
Children below 5–6 years of age are unable to swallow solid drug forms safely, and even older children sometimes have difficulty in swallowing gelatin capsules, which may affect treatment adherence; since the dose of zonisamide for children is calculated based on body weight, it is sometimes very difficult to prescribe exact necessary dose to a child using capsules of zonisamide with just a few fixed doses per capsule.13 These issues create a need for a liquid oral form of zonisamide for use in children. Some elderly patients may have difficulty swallowing capsules due to cognitive problems or diseases of the esophagus, and some patients have to be fed through a nasogastric tube which is also the only route for administering drugs enterally; it is evident that only liquid formulation of zonisamide could be administered to such patients, which creates an additional need for oral suspension of this drug on the market.5,12 With liquid pharmaceutical form instead of capsules, in all previously mentioned patients, adherence may be better and potential dosage errors avoided.14
Variability of Bioequivalence of Different Zonisamide Oral Suspensions
Drugs containing zonisamide as an active substance are widely used to treat focal onset seizures in children.15 If children are old enough to swallow capsules, this dosage form is widely available; however, for younger children and all other patients who cannot swallow solid dosage forms of drugs, the only solution is an oral suspension of zonisamide as a medication with MA, if available, or as extemporaneous oral suspension made in a local pharmacy. Extemporaneously compounded oral suspension of zonisamide is an official preparation only according to United States Pharmacopoeia (USP),16 while in other countries, it could be prepared in a number of ways. Table 1 provides a short overview of zonisamide oral suspensions with MA and published extemporaneous oral suspensions tested for stability.17–20
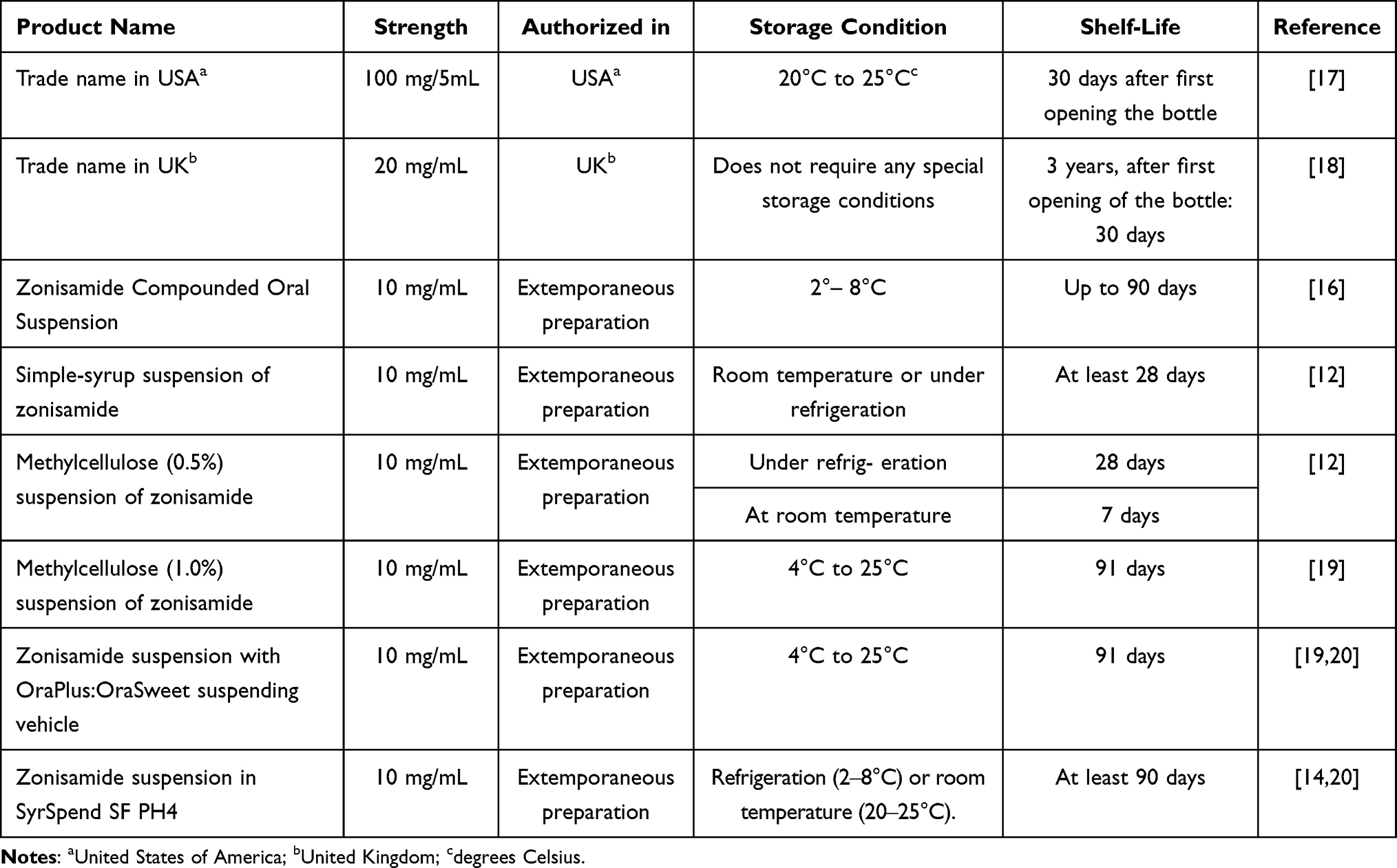 |
Table 1 Overview of Available Zonisamide Oral Suspensions |
Each of the oral suspensions of zonisamide listed in Table 1 has a somewhat different mixture of suspending agents (viscosity modifiers, density agents, wetting agents, and flocculating/deflocculating agents) used to provide stability of the suspension and prevent sedimentation of the suspended particles of zonisamide; flavors and other adjunctive agents also vary. Microcrystalline cellulose, xanthan gum, sodium carboxymethyl cellulose, and carrageenan are the main suspending agents used, however, in varying ratios and concentrations. Although there are published studies that tested the stability of these oral suspensions of zonisamide, so prescribers do know how long the patients may use them, the key question for clinical practice is whether these preparations have bioequivalence of zonisamide in hard capsules, which was originally tested in clinical trials and first received MA back in the year 2000.1 Since zonisamide is only moderately soluble, its oral suspensions could not be classified as Class 1 of the Biopharmaceutics Classification System (BCS) (drugs with high aqueous solubility and high intestinal permeability), and therefore bioequivalence studies could not be waived when applying for MA.21 The two oral suspensions which already received MA were tested for bioequivalence with zonisamide in hard capsules as reference product, and it was found that criteria for bioequivalence were met.22 However, bioequivalence limits are relatively wide (80–125% of the original product’s pharmacokinetic parameters), so significant differences in plasma concentrations and effects among products officially recognized as bioequivalent may exist.23 On the other hand, no efficacy/safety clinical trials were conducted with these two zonisamide products. With extemporaneous oral suspensions of zonisamide, the situation is even greyer: neither bioequivalence nor efficacy/safety clinical trials have been conducted to date; furthermore, extensive search of the ClinicalTrials.gov database during preparation of this article showed that no current or future clinical trials/bioequivalence studies with extemporaneous oral suspensions of zonisamide are registered. Although theoretically, one may expect that extemporaneous oral suspensions of zonisamide have bioequivalence of oral suspensions that have MA or hard capsules, experience with extemporaneous oral suspensions of other drugs has shown that bio inequivalence is a reality; however, this does not mean automatically that bio inequivalent preparation is not effective and safe.24 While slightly bio inequivalent oral suspensions of drugs with wider therapeutic window may still function well in clinical practice, narrow therapeutic window drugs like anticonvulsants, including zonisamide, require the use of strictly bioequivalent preparations (especially when switching from preparation to preparation) or the patient may experience loss of efficacy or emergence of toxicity.25 It is even recommended that bioequivalence studies should be accompanied with or followed by clinical trials if therapeutical equivalence of parallel pharmaceutical preparations (including oral suspensions) containing narrow therapeutic window drugs is to be confirmed.25
An additional source of variability of the actual dose that a patient is ingesting when using any oral suspension of zonisamide is shaking before taking a dose. When a group of pharmacy students was instructed to shake and then sample an extemporaneously compounded oral suspension of zonisamide to determine its beyond-use date, it turned out that the potency of their weekly samples (ie, dosing accuracy) varied 64%-111% of the label, with a relative standard deviation of 17–76%.26 Although more precise instructions about shaking and sampling later resulted in increased dosing accuracy (91%-118%, relative standard deviation of 5%-29%), variability is still there and may influence the actual ingested dose, plasma concentrations, and treatment outcome. It is crucial and critical for treatment success, to educate patients and their carers how to properly shake zonisamide suspension before use.
In conclusion, although zonisamide is an antiepileptic drug with proven safety and efficacy when used in the form of hard capsules, the clinical utility of zonisamide oral suspensions remains to be demonstrated in the future, especially when the suspensions are prepared extemporaneously according to different formulas. Oral suspension formulation may even improve patient adherence or reduce dosage errors resulting in better treatment outcomes in theory, but this needs to be confirmed in head-to-head clinical studies (either experimental or observational) between different pharmaceutical forms of zonisamide.
Funding
This work was partially supported by the Ministry of Education, Science and Technological Development under Grant No 175007 and contract No 451-03-47/2023-01/200111.
Disclosure
The authors have no competing interests to disclose in regard to content of this article.
References
1. Kadian R, Kumar A. Zonisamide. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023.
2. Wilfong AA, Willmore LJ. Zonisamide - a review of experience and use in partial seizures. Neuropsychiatr Dis Treat. 2006;2(3):269–280. doi:10.2147/nedt.2006.2.3.269
3. Leppik IE. Zonisamide: chemistry, mechanism of action, and pharmacokinetics. Seizure. 2004;13:S5–9. doi:10.1016/j.seizure.2004.04.016
4. Janković SM. Evaluation of zonisamide for the treatment of focal epilepsy: a review of pharmacokinetics, clinical efficacy and adverse effects. Expert Opin Drug Metab Toxicol. 2020;16(3):169–177. doi:10.1080/17425255.2020.1736035
5. van Maanen R, Bentley D. Bioequivalence of zonisamide orally dispersible tablet and immediate-release capsule formulations: results from two open-label, randomized-sequence, single-dose, two-period, two-treatment crossover studies in healthy male volunteers. Clin Ther. 2009;31(6):1244–1255. doi:10.1016/j.clinthera.2009.06.012
6. Sills GJ, Brodie MJ. Pharmacokinetics and drug interactions with zonisamide. Epilepsia. 2007;48(3):435–441. doi:10.1111/j.1528-1167.2007.00983.x
7. Zonisamide Key 100mg Hard Capsules, Public Assessment Report, Public Assessment Report, Key Pharmaceuticals Ltd; 2023. Available from: https://mhraproducts4853.blob.core.windows.net/docs/d27643bbbfa18a0ceee3353c7dfda8b68bae1a2d.
8. Marson AG, Burnside G, Appleton R, et al. Lamotrigine versus levetiracetam or zonisamide for focal epilepsy and valproate versus levetiracetam for generalised and unclassified epilepsy: two SANAD II non-inferiority RCTs. Health Technol Assess Winch Engl. 2021;25(75):1–134. doi:10.3310/hta25750
9. EMA. European Medicines Agency. Zonegran; 2018. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/zonegran.
10. Orange Book: approved drug products with therapeutic equivalence evaluations; 2023. Available from: https://www.accessdata.fda.gov/scripts/cder/ob/results_product.cfm?Appl_Type=N&Appl_No=214273#41417.
11. MHRA Products | Search results; 2023. Available from: https://products.mhra.gov.uk/search/?search=zonisamide+oral+suspension&page=1.
12. Abobo CV, Wei B, Liang D. Stability of zonisamide in extemporaneously compounded oral suspensions. Am J Health Syst Pharm. 2009;66(12):1105–1109. doi:10.2146/ajhp080250
13. Patel VP, Desai TR, Chavda BG, Katira RM. Extemporaneous dosage form for oral liquids. Pharmacophore. 2011;2(2):86–103.
14. Ferreira AO, Polonini HC, Silva SL, Patrício FB, Brandão MAF, Raposo NRB. Feasibility of amlodipine besylate, chloroquine phosphate, dapsone, phenytoin, pyridoxine hydrochloride, sulfadiazine, sulfasalazine, tetracycline hydrochloride, trimethoprim and zonisamide in SyrSpend(®) SF PH4 oral suspensions. J Pharm Biomed Anal. 2016;118:105–112. doi:10.1016/j.jpba.2015.10.032
15. Coppola G, Grosso S, Verrotti A, et al. Zonisamide in children and young adults with refractory epilepsy: an open label, multicenter Italian study. Epilepsy Res. 2009;83(2–3):112–116. doi:10.1016/j.eplepsyres.2008.10.012
16. Zonisamide Compounded Oral Suspension. In the United States Pharmacopeia Convention Committee of Revision (Ed.), United States Pharmacopeia - National Formulary; 2020. Available from: https://doi.usp.org/USPNF/USPNF_M8852_01_01.html.
17. Zonisadetm. FDA full prescribing information, revised 07/22. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/214273s000lbl.pdf.
18. Desizon 20 mg/mL oral suspension - Summary of Product Characteristics (SmPC) - (EMC); 2023. Available from: https://www.medicines.org.uk/emc/product/11954/smpc.
19. Nahata MC. Long-term stability of zonisamide, amitriptyline, and glycopyrrolate in extemporaneously prepared liquid-dosage forms at two temperatures. Int J Pharm Compd. 2016;20(2):164–166.
20. Loyd VA. Zonisamide 10 mg/mL in Ora-Sweet: Ora-Plus (1:1) or SyrSpend SF PH4. US Pharm. 2020;45(1):48–CV3.
21. Odi R, Franco V, Perucca E, Bialer M. Bioequivalence and switchability of generic antiseizure medications (ASMs): a re-appraisal based on analysis of generic ASM products approved in Europe. Epilepsia. 2021;62(2):285–302. doi:10.1111/epi.16802
22. Steven Dinsmore. Clinical review of zonisamide oral suspension bioequivalence studies (Application number: 214273Orig1s000). Center for Drug Evaluation and Research. The review completed 25.5.2021. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2023/214273Orig1s000MedR.pdf.
23. Micheal F, Sayana M, Prasad R, Motilal BM. Has the time come to employ population and individual bioequivalence for the evaluation of generics? Curr Drug Metab. 2020;21(2):112–125. doi:10.2174/1389200221666200401105119
24. Patel P, Nathan PC, Walker SE, Zupanec S, Volpe J, Dupuis LL. Relative bioavailability of an extemporaneously prepared aprepitant oral suspension in healthy adults. J Oncol Pharm Pract. 2019;25(8):1907–1915. doi:10.1177/1078155219828806
25. Habet S. Narrow therapeutic index drugs: clinical pharmacology perspective. J Pharm Pharmacol. 2021;73(10):1285–1291. doi:10.1093/jpp/rgab102
26. Darst EC, Shrewsbury RP. The positive impact of an extended intervention on dosing accuracy of student compounded suspensions. Am J Pharm Educ. 2019;83(5):6781. doi:10.5688/ajpe6781
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.