Back to Journals » Clinical Ophthalmology » Volume 20
Binocular Reading Speed Comparison: Patients After Bilateral Trifocal IOL Implantation versus Those without Cataract —A Prospective, Dual-Center Study
Authors Lin Y, Liang X, Tan Y, Chen Y, Li L, Xu Y, Zhao C, Qu H
Received 14 February 2026
Accepted for publication 3 June 2026
Published 8 June 2026 Volume 2026:20 603633
DOI https://doi.org/10.2147/OPTH.S603633
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Bharat Gurnani
Yingjie Lin,1– 3 Xianjun Liang,1,2 Yongchang Tan,1 Yun Chen,1 Li Li,1 Yanxue Xu,1,3 Chunyang Zhao,1 Haokun Qu2
1Department of Ophthalmology, Aier Eye Hospital, Jinan University, Guangzhou, Guangdong, People’s Republic of China; 2Department of Ophthalmology, Foshan Zhuoyue Aier Eye Hospital, Foshan, Guangdong, People’s Republic of China; 3Department of Ophthalmology, Foshan Aier Eye Hospital, Foshan, Guangdong, People’s Republic of China
Correspondence: Li Li, Department of Ophthalmology, Aier Eye Hospital, Jinan University, Guangzhou, Guangdong, People’s Republic of China, Tel +86-13827748321, Email [email protected]
Purpose: To explore the effect of binocular PanOptix intraocular lens (IOL) implantation on binocular reading speed in adult patients.
Methods: This prospective observational study was performed at Foshan Aier Eye Hospital and Guangzhou Aier Eye Hospital between October 2022 and June 2023. Patients with clinically significant cataract scheduled for AcrySof IQ PanOptix implantation (PanOptix group) and age-matched and educational level-matched patients without clinically significant cataract were enrolled as control group. Of note, the control group was tested without near addition for the reading speed assessment. The primary outcome was the binocular reading speed (characters per minute) at 40 cm with distance vision correction, measured using the Chinese version of the International Reading Speed Texts (IReST).
Results: Forty-two patients were included in each group. There were no significant differences in age, sex, and education level between the two groups (all P> 0.05). The preoperative visual acuity was 0.84± 0.41 logMAR in the PanOptix group. The PanOptix group displayed significantly better binocular reading speed at 3 months postoperatively than the control group (219.81± 35.94 vs 174.91± 42.21 characters/min, P< 0.001). In addition, postoperative uncorrected visual acuity (near, intermediate, and distant) and corrected visual acuity (near and intermediate) were all better in the PanOptix group compared with the control group (all P< 0.05). In the PanOptix group, compared with before surgery, sphere and cylinder, corrected distant vision, and uncorrected distance visual acuity were all improved after surgery in both eyes.
Conclusion: Binocular PanOptix IOL implantation was associated with significantly faster binocular reading speed compared with age-matched presbyopic individuals without near correction.
Keywords: cataract, presbyopia, multifocal intraocular lenses, reading speed
Introduction
Cataract is a partial or total opacification of the crystalline lens.1,2 It affects ~95 million people globally, with prevalence increasing with age: 3.9% in 55–64-year-olds and 92.6% in those over 80. Its main complication is progressive and irreversible vision loss, which may lead to blindness and visual aberrations without cataract surgery.1,2 Presbyopia, another age-related vision change, involves declining lens accommodative capacity causing near vision impairment, affecting ~1.8 billion people worldwide.
Both cataract and presbyopia affect vision and reading capacity since cataract affect vision irrespective of distance, and presbyopia affects near visual acuity.2–5 Near and intermediate visual acuities are crucial to reading.6 Assessing the reading speed is important for the assessment of reading disorders related to low vision, neurological diseases, or dyslexia.7,8 Standardized texts are now available in various languages to allow the assessment of the reading speed and capacity and comparison among populations.9 Reading Chinese requires a higher visual acuity than reading English,10 which is taken into account by the standardized texts.9
No pharmacological treatments are known to slow down progression or eliminate existing cataract, and the only symptomatic management method is the removal of the opacified lens and its replacement with an artificial intraocular lens (IOL).1 An artificial IOL is implanted following cataract removal to correct refractive errors and typically remains functional for life.1,11 The designs of IOLs differ in the number of focal points and range of focus, which can also correct for presbyopia and astigmatism.1,11 Monofocal designs typically require the continued use of eyeglasses or contact lenses for near or distance vision.1,2 Recent bifocal (distance and near focal points) and trifocal (distance, intermediate, and near focal points) IOLs, toric IOLs, and new materials led to improvements in visual acuity and a reduction in the need for eyeglasses but there is an increase in the risk of optical adverse events, such as halos and glare.1,11–14 The AcrySof IQ PanOptix Model TFNT00 (Alcon Laboratories, Fort Worth, TX) is an ultraviolet (UV) and blue light filtering, non-apodized, foldable, presbyopia-correcting IOL first launched in Europe in 2015 that uses the ENhanced LIGHT ENergy (ENLIGHTEN) optical technology,15,16 with a lower occurrence of halos and glare than with other multifocal IOLs.17,18
Still, there are few studies on using the AcrySof IQ PanOptix in patients with cataract and presbyopia, especially regarding reading speed. Therefore, this study aimed to compare binocular reading speed after bilateral PanOptix IOL implantation with that of age-matched presbyopic individuals without near correction, and to evaluate the functional near vision benefit of achieving spectacle independence through trifocal IOL implantation.
Subjects and Methods
Study Design and Patients
This prospective observational study was performed at Foshan Aier Eye Hospital and Guangzhou Aier Eye Hospital between October 2022 and June 2023. The patients with cataract and presbyopia scheduled to undergo phacoemulsification and AcrySof IQ PanOptix implantation were enrolled as the experimental group (ie, the PanOptix group). Age-matched and educational level-matched patients with presbyopia were selected from the patients and accompanying family members who visited the ophthalmology department of the hospitals as the control group.
The study was performed in accordance with the tenets of the Declaration of Helsinki and the Good Clinical Practice. The study was reviewed and approved by the Ethics Committee of Foshan Aier Eye Hospital and the Ethics Committee of Guangzhou Aier Eye Hospital. All participants signed the informed consent form.
The inclusion criteria for the PanOptix group were patients 1) aged 55–70 years, 2) with a diagnosis of presbyopia, ie, requiring presbyopic glasses, presbyopic add, or in some cases, the need to remove corrected distance visual acuity glasses to have near visual acuity, 3) a diagnosis of binocular age-related cataract in whom the surgical goal was to achieve emmetropia with a zero-target diopter after the implantation of binocular PanOptix IOLs, 4) preoperative best-corrected distance visual acuity (CDVA) of 0.2 to 0.5 logMAR, 5) educational level of junior high school or above, and 6) corneal astigmatism <1.0 D (IOLMaster 500). 7) Mesopic pupil size < 5.5 mm.
The exclusion criteria for the PanOptix group were patients 1) with irregular corneal astigmatism, 2) with a history of ophthalmic surgery, 3) with any disease or intraoperative complications that could affect the binocular reading speed like moderate to severe dry eye, corneal scars, amblyopia, glaucoma, pseudoexfoliation syndrome, uveitis, degeneration of the macula, or other conditions that may affect near visual acuity, 4) with reading or attention disorders, or 5) unable to complete the reading of all ten pieces of text.
After completing the data collection of the PanOptix group, the control group was created by matching the PanOptix group in terms of age and education level. Presbyopes without cataract or with mild cataract whose CDVA was 0.1 logMAR or better were enrolled in the control group. The inclusion criteria for the control group were patients 1) aged 55–70 years, 2) with a diagnosis of presbyopia, ie, requiring presbyopic glasses, presbyopic add, or in some cases, the need to remove corrected distance visual acuity glasses to have near visual acuity, 3) patients without cataract or with mild cataract, 4) with preoperative CDVA of 0.1 logMAR or better, and 5) with an education level of junior high school or above. The exclusion criteria were the same as for the PanOptix group.
Treatment
All patients in the PanOptix group underwent phacoemulsification and AcrySof IQ PanOptix trifocal intraocular lens implantation.19,20 The cataract was removed by phacoemulsification, and the patients received the AcrySof IQ PanOptix presbyopia-correcting IOL (model TFNT00). All procedures were performed using temporal clear corneal incisions, as well as curvilinear capsulorhexis. All other procedures were performed based on the surgeon’s experience to ensure the best patient and visual outcomes. The surgeons aimed at emmetropia (ie, 0.00±0.05 D) in the two eyes. As recommended by the manufacturer, the IOL power was calculated using the SRK/T formula and A=119.1.21
Outcomes
The primary outcome of the study was the binocular reading speed (characters per minute) at 40 cm with distance vision correction, which was measured by the Chinese version of the International Reading Speed Texts (IReST). The control group did not use a near addition for the binocular reading speed test. This design was chosen to reflect real-world conditions in which presbyopic individuals often do not wear reading glasses, and to evaluate the functional benefit of achieving spectacle independence through IOL implantation relative to uncorrected presbyopia. The IReST consists of sets of 10 texts of approximately 130 words, each available in 17 languages and with similar reading difficulty for repeated measurements in international studies.9,22 The follow-up of the PanOptix group was 3 months after surgery. The PanOptix group was assessed 3 months postoperatively, while the control group was assessed immediately after signing the informed consent form.
Each participant had to read aloud five of the ten randomly selected Chinese IReST texts, in random order, at a distance of 40 cm after correction to achieve optimal distance vision. The reading time for each text was recorded in seconds using a stopwatch, without pause, to correct errors, and the errors were corrected afterward. Incorrect or omitted words were counted and excluded when calculating the binocular reading speed. The binocular reading speed (characters per minute) at a distance of 40 cm was calculated as the “total number of characters read correctly (under distance vision correction)” / “reading time (in seconds)” × 60 seconds.
Secondary outcomes of the study included binocular corrected and uncorrected visual acuity at different distances (5 m, 60 cm, and 40 cm), subjective optometric findings (spherical lens, cylindrical lens, and axial direction), dysfunctional lens index (DLI) results (such as spherical aberration (SA), high-order aberration (HOA), point spread function (PSF), and modulation transfer function (MTF), and defocus curve results (from +1.0 D to −4.0 D). The PanOptix group was measured at 3 months postoperatively while the control group was evaluated right after signing the informed consent form.
In addition, patients’ age, sex, education, and preoperative visual acuity were collected.
Sample Size Calculation
The sample size was calculated based on the results of a pilot study that provided mean reading speeds of 242.95±31.60 characters per minute for the experimental group (n=5) and 207.77±72.88 for the control group (n=4). Using a two-sample t-test allowing unequal variances with a two-sided significance level of 0.05 and 80% power, a total of 84 subjects (42 per group) were required for the analysis. Accounting for an estimated 20% dropout rate in the PanOptix group, the required number of patients in the PanOptix group was 53 subjects and 42 subjects in the control group, resulting in a total sample size of 95.
Statistical Analysis
Statistical analysis was performed using STATA 14.0 (StataCorp LP, College Station, TX, USA) and SPSS 22.0 (IBM, Armonk, NY, USA). Continuous variables were described as mean ± standard deviation (SD). The Shapiro–Wilk test was used to assess normality. For comparisons between the PanOptix and control groups, the independent-samples t-test was used for normally distributed variables, and the Mann–Whitney U-test was used for non-normally distributed variables. Pre- and postoperative comparisons within the PanOptix group were performed using the paired t-test or Wilcoxon signed-rank test, as appropriate. Categorical variables were described as n (%) and analyzed using the chi-squared test. For multiple comparisons of visual acuity outcomes at different distances, Bonferroni correction was applied to adjust the significance threshold.
Results
Characteristics of the Patients
Fifty-three patients with cataract and presbyopia scheduled to undergo phacoemulsification and AcrySof IQ PanOptix trifocal intraocular lens implantation were enrolled. Among them, two patients were lost to follow-up, and nine finally did not undergo binocular surgery at the planned time. Therefore, 42 patients were included in the PanOptix group. The control group also included 42 patients (30 with mild cataracts and 12 without cataracts). There were no significant differences in age, sex, and education between the two groups (all P>0.05). The preoperative visual acuity was 0.84±0.41 logMAR in the PanOptix group (Table 1). All enrolled patients had mesopic pupils < 5.5 mm as large pupils may affect postoperative visual acuity, reading speed, visual quality, and the occurrence of visual disturbances.
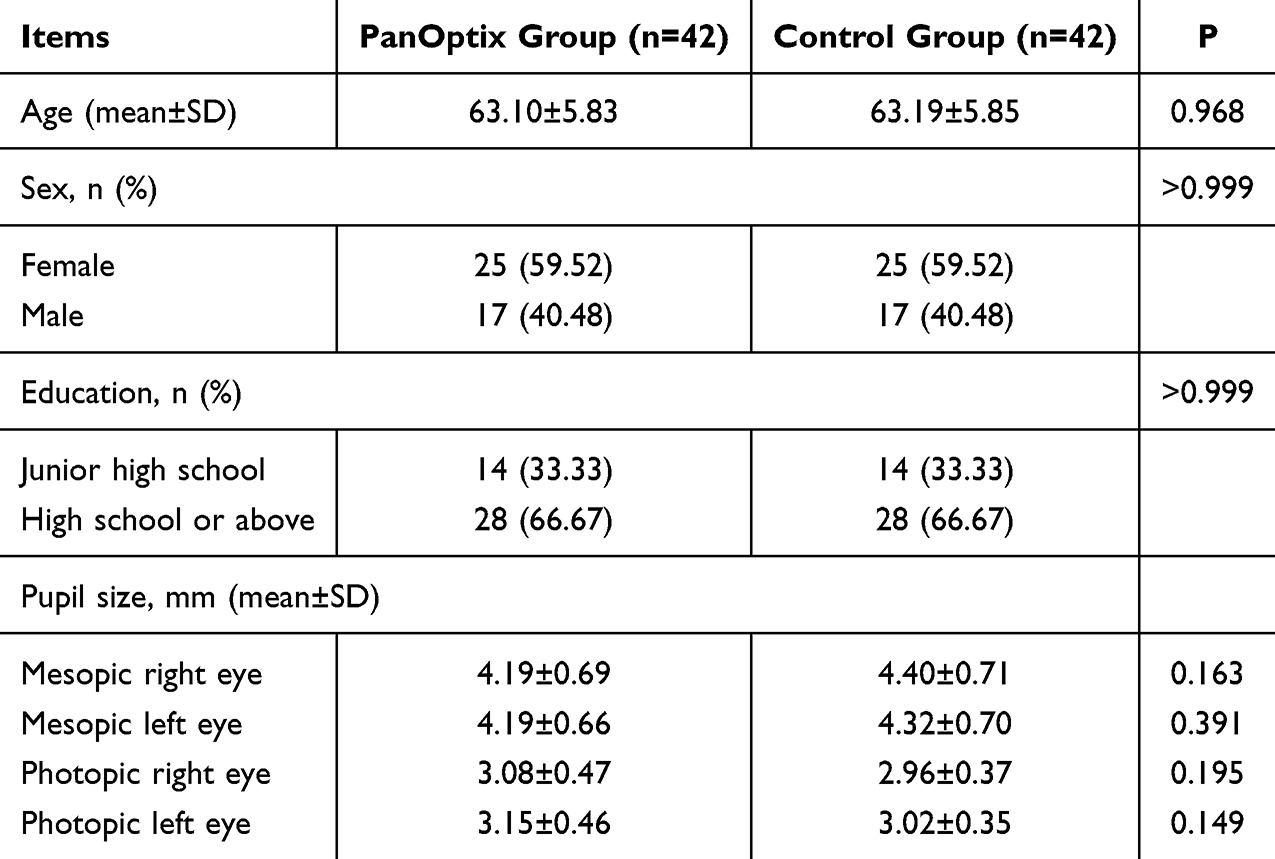 |
Table 1 Characteristics of the Patients |
Binocular Reading Speed
All participants underwent a binocular reading speed. The PanOptix group was assessed 3 months postoperatively, while the control group was assessed immediately after signing the informed consent form. The PanOptix group displayed significantly better binocular reading speed than the control group (219.81±35.94 vs 174.91±42.21 characters/min, P<0.001) (Table 2). The effect size (Cohen’s d) for the between-group difference in binocular reading speed was 1.14, indicating a large effect.
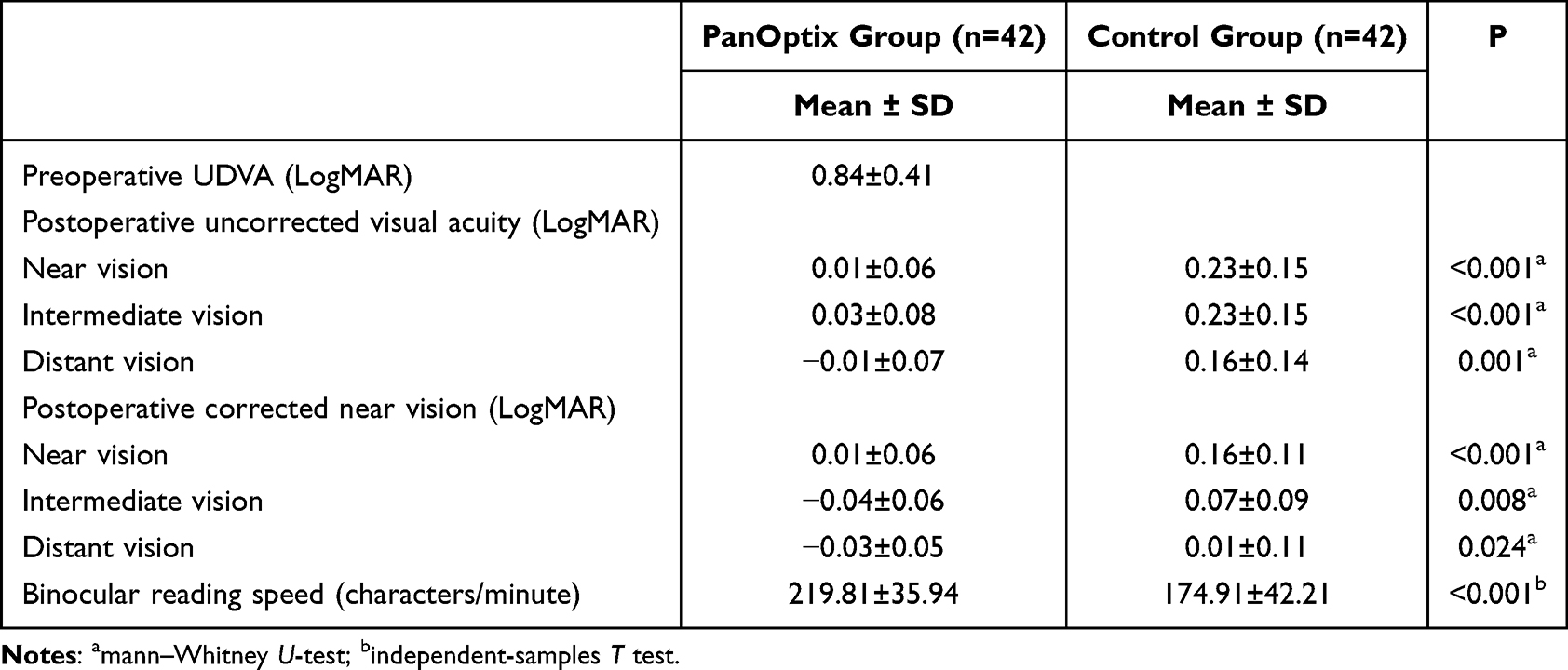 |
Table 2 Outcomes |
Visual Acuity
In the PanOptix group, as expected, visual acuity improved from 0.84±0.41 to 0.01±0.06 logMAR (uncorrected) (P<0.001). Postoperative uncorrected near (0.01±0.06 vs 0.23±0.15 logMAR, P<0.001), intermediate (0.03±0.08 vs 0.23±0.15 logMAR, P<0.001), and distant (−0.01±0.07 vs 0.16±0.14 logMAR, P<0.001) visual acuity evaluations were all better in the PanOptix group vs the control group. (near, intermediate, and distant). In addition, corrected near (0.01±0.06 vs 0.16±0.11 logMAR, P<0.001) and intermediate (−0.04±0.06 vs 0.07±0.09 logMAR, P<0.001) visual acuity evaluations were better in the PanOptix group, but the distant visual acuity evaluation (−0.03±0.05 vs 0.01±0.11 logMAR, P=0.024) showed a value nearer 0 for the control group (Table 2).
Manifest Refraction and Defocus Curve
In the PanOptix group, statistically significant improvements were observed in all refractive parameters postoperatively compared with baseline values (Table 3). Specifically, the mean refractive sphere shifted from −2.48 ± 4.13 D to −0.01 ± 0.72 D in the right eye and from −2.47 ± 4.49 D to 0.00 ± 0.54 D in the left eye (P < 0.001 for both). Cylinder values also improved significantly, decreasing from −0.52 ± 0.95 D to −0.19 ± 0.36 D in the right eye (P = 0.008) and from −0.48 ± 0.76 D to −0.27 ± 0.32 D in the left eye (P < 0.001). Consequently, the spherical equivalent showed marked improvement, moving from −2.76 ± 4.61 D to −0.10 ± 0.90 D in the right eye and from −3.95 ± 4.87 D to −0.14 ± 0.70 D in the left eye (P < 0.001 for both).
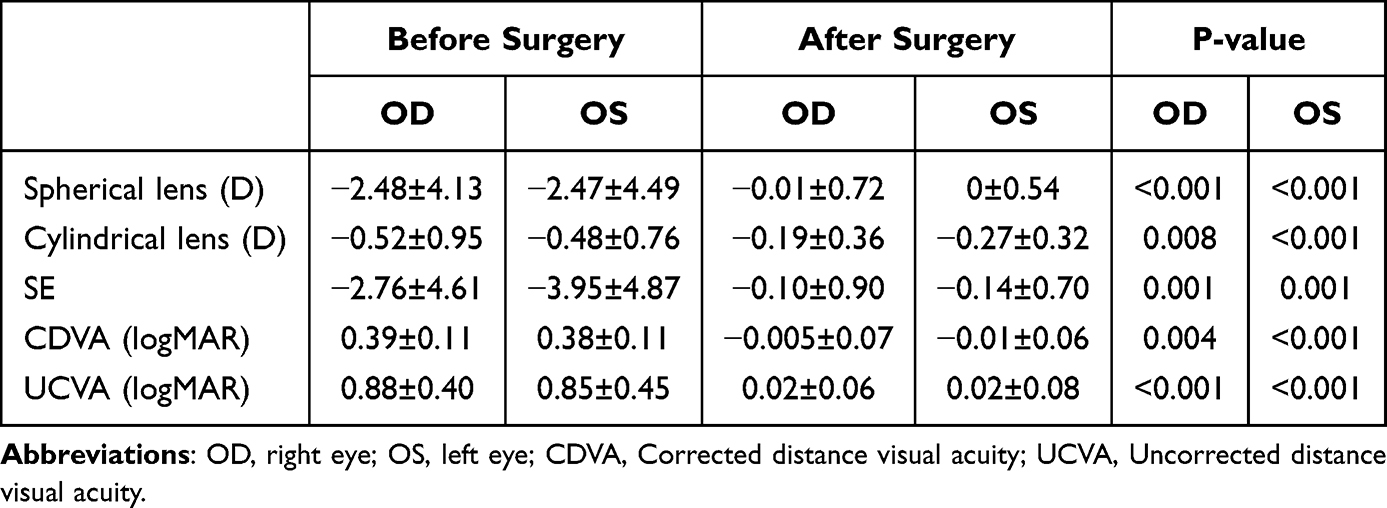 |
Table 3 Optometry and Objective Visual Quality Before and After Surgery in the PanOptix Group |
Following surgery, high visual acuity was achieved in both distance correction and uncorrected distance vision. Postoperative corrected distance visual acuity (CDVA) reached −0.005 ± 0.07 logMAR for the right eye and −0.01 ± 0.06 logMAR for the left eye. Uncorrected distance visual acuity (UDVA) was recorded at 0.02 ± 0.06 logMAR for the right eye and 0.02 ± 0.08 logMAR for the left eye.
The defocus curve for the PanOptix group is presented in Figure 1, demonstrating a continuous functional range of vision from distance to near. Visual acuity remained near 0 logMAR at 0 D defocus and maintained a functional level of approximately 0.3 logMAR even at the maximum induced defocus of −4 D.
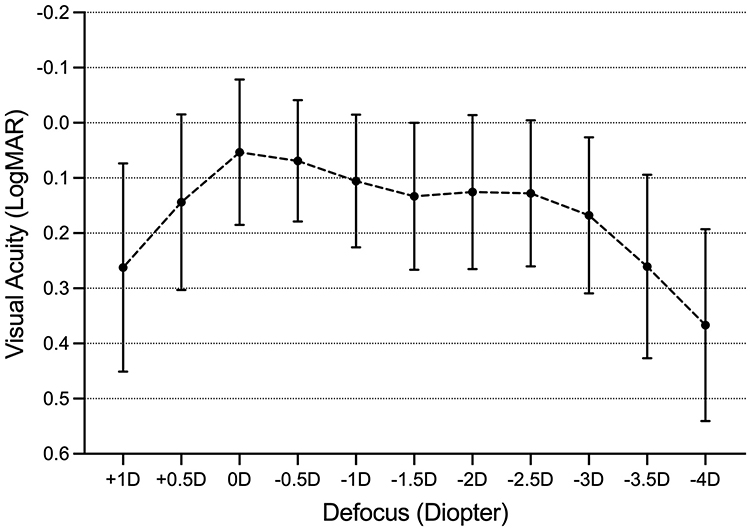 |
Figure 1 Defocus curve in the PanOptix group. |
Discussion
This prospective observational study examined the effect of bilateral PanOptix IOL implantation on binocular reading speed in patients with cataracts and presbyopia. The results showed that implantation of the PanOptix IOL in both eyes significantly improved visual acuity at all distances and accelerated binocular reading speed in patients with presbyopia compared to those without cataracts. Most trifocal IOLs use diffraction or diffraction-refraction hybrid technology to distribute incident light to three main focal points: far, intermediate, and near. Through this distribution of light energy, trifocal IOLs are designed to create an extended, functional range of visual acuity, allowing patients to eliminate the need to rely on glasses in most everyday scenarios.22,23 This conclusion is consistent with our research findings, demonstrating that both distant, intermediate, and near visual acuity significantly improved after surgery.
Conventional visual acuity tests measure the ability to identify the smallest characters under static, high-contrast conditions; however, daily reading is a dynamic and continuous task. Therefore, a patient with good near visual acuity may not necessarily experience comfortable and sustained reading performance. Research has indicated that good near visual acuity does not fully equate to good functional near vision.23 Reading speed quantifies the efficiency with which patients acquire information under conditions approximating real-life scenarios, and it comprehensively reflects visual acuity, contrast sensitivity, saccadic function, and the fluency of cognitive processing.24 Therefore, when evaluating multifocal IOLs designed to provide full-range vision, reading speed emerges as a critical performance indicator for assessing whether these lenses genuinely enhance patients’ quality of life.25 Chinese characters are logographic, and their structure is more complex than that of alphabetic scripts, implying that they manifest as high spatial frequency information visually, requiring the visual system to possess higher contrast sensitivity for recognition.10,26 Some studies comparing the readability of Chinese and English newspaper characters have found that reading Chinese characters requires greater visual acuity reserve compared to reading English letters.10 Our study provides critical data on the performance of trifocal IOLs in a non-Latin linguistic context. Utilizing the standardized Chinese version of the IReST, we offer novel insights into how trifocal optics handle the high-frequency spatial details required for Chinese reading.
The conventional wisdom is that implantation of a trifocal IOL will lead to an increase in reading speed, but recent studies have found that in terms of short-term results (within 1 to 3 months after surgery), patients may not experience a significant increase in reading speed, or even a slight decrease in some patients.27,28 This is inconsistent with the findings of our study. Possible reasons include the varying degrees of visual adaptation occurring during the early postoperative period. Trifocal IOLs broadens the functional vision range, it simultaneously reduces the amount of light energy reaching each focal point, thereby decreasing image contrast. Under special conditions such as mesopic visual environments, this reduction in contrast sensitivity directly impairs reading efficiency. Furthermore, common early postoperative visual disturbances such as halos and glare can distract attention, further compromising reading performance.27,28 By 6 months postoperatively, patients gradually learned to shift their fixation focus across different distances and to ignore optical artifacts, thereby optimizing functional visual performance. Consequently, long-term follow-up data exceeding 6 months indicate that the reading speed of most patients recovered to preoperative levels, and in some cases even improved.29 A study found that patients’ uncorrected reading speeds increased over time.30 This suggests that even if satisfactory reading speeds are achieved early after surgery, reading function may continue to improve further as neural adaptation progresses. In our study, patients achieved excellent reading speed as early as 3 months postoperatively, suggesting that the TFNT IOL may have a faster even better neural adaptation process. While the 3-month follow-up period is adequate for assessing visual acuity stabilization after cataract surgery, neural adaptation to multifocal optics is a dynamic process that may continue beyond this time frame. Some studies have observed ongoing improvements in reading speed between 3 and 6 months postoperatively, suggesting that the reading performance reported here may represent an intermediate rather than final outcome. Longer-term follow-up studies would be valuable to characterize the full trajectory of functional visual recovery.
Panoptix TFNT is a trifocal intraocular lens based on the principle of quadrifocal optics. Through its unique design, it redirects and superimposes light energy from the first intermediate focus at 120 cm onto the far focus, thereby enhancing distance vision and achieving approximately 88% optical energy utilization.31,32 High light utilization efficiency directly translates into superior visual quality, particularly under medium to low illumination conditions, enabling patients to perceive brighter and clearer images, which forms the foundation of the reading capability. Many first-generation trifocal IOLs have their intermediate focus set around 80 cm,33 whereas the Panoptix TFNT intermediate focus is set at 60 cm—a distance widely regarded as the “working distance” corresponding to arm’s length.17,34 Furthermore, the Panoptix TFNT near focus falls within the range of 40 to 42 cm, a distance recognized internationally as the preferred viewing distance.35 In contrast, some EDOF IOLs can extend the depth of focus, but the visual acuity at 40cm is often not sufficient to support easy reading of small fonts.17
It is noteworthy that in this study, we compared implantation of a presbyopia-correcting IOL with presbyopic eyes not using near addition lenses. Although it may argue that this optical comparison is not perfectly equivalent, the design aims to reflect real-world conditions where spectacle independence is achieved. The significantly slower reading speed in the control group (174.91 wpm) highlights the functional impairment caused by uncorrected presbyopia. In contrast, the PanOptix group achieved reading speeds comparable to those of young adults with normal, unaccommodating vision. It confirms that the PanOptix IOL not only effectively alleviates visual decline due to cataracts but also provides near vision superior to that of uncorrected presbyopia, successfully fulfilling patients’ desire for complete spectacle independence. These findings indicate that the PanOptix IOL is not merely an option for cataract treatment but also a viable solution for presbyopia correction, significantly enhancing patients’ uncorrected visual quality of life, even in refractive lens exchange procedures.
In conclusion, bilateral PanOptix IOL implantation was associated with faster binocular reading speed compared with age-matched presbyopic individuals tested without near correction. These findings suggest that the PanOptix IOL may offer functional near vision benefits in presbyopic patients undergoing cataract surgery. However, the absence of best-corrected near visual acuity in the control group and the lack of preoperative reading speed data limit the interpretation. The results should be understood as a comparison with uncorrected presbyopia rather than as evidence of superiority over optimally corrected presbyopia or healthy accommodation. Further studies with near-corrected control groups and preoperative reading speed assessments are warranted.
The innovation of this study is that this study abandoned the paradigm of comparing trifocal IOLs with other IOLs, and evaluated not only the efficacy of the PanOptix in treating cataracts, but also intuitively assessed its advantages as a means of correcting presbyopia relative to naturally aging eyes. Data specific to the Chinese reading environment were also examined. Anyway, there are some limitations of this study. First, this study had a relatively small sample size limits the generalizability of the findings. Secondly, the control group was not tested for best-corrected near visual acuity. Therefore, our conclusions apply only to the advantage of PanOptix in uncorrected presbyopia and not to the advantage compared with healthy accommodation systems or corrected presbyopia. Future studies should include a control group wearing reading add-on lenses to separate the optical quality of the IOL from the magnification advantage. Thirdly, reading speed was not assessed preoperatively in the PanOptix group. This is a notable limitation, as it precludes the ability to distinguish whether the observed postoperative reading speed improvement is attributable to cataract removal, the optical design of the trifocal IOL, or presbyopia correction alone. Future studies should include preoperative reading speed measurements to quantify the net benefit attributable to each component of the intervention. Fourthly, the 3-month follow-up period, while sufficient for visual acuity stabilization, may not capture the full extent of neural adaptation to multifocal optics, and reading performance may continue to improve beyond this time point.
Conclusion
Binocular PanOptix IOL implantation was associated with significantly faster binocular reading speed compared with age-matched presbyopic individuals without near correction.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Miller KM, Oetting TA, Tweeten JP, et al. Cataract in the adult eye preferred practice pattern®. Ophthalmology. 2022;129(1):P1–9. doi:10.1016/j.ophtha.2021.10.006
2. Liu YC, Wilkins M, Kim T, Malyugin B, Mehta JS. Cataracts. Lancet. 2017;390(10094):600–612. doi:10.1016/S0140-6736(17)30544-5
3. Holden BA. Global vision impairment due to uncorrected presbyopia. Arch Ophthalmol. 2008;126(12):1731. doi:10.1001/archopht.126.12.1731
4. Fricke TR, Tahhan N, Resnikoff S, et al. Global prevalence of presbyopia and vision impairment from uncorrected presbyopia. Ophthalmology. 2018;125(10):1492–1499. doi:10.1016/j.ophtha.2018.04.013
5. Reindel W, Zhang L, Chinn J, Rah M. Evaluation of binocular function among pre- and early-presbyopes with asthenopia. OPTO. 2018;10:1–8. doi:10.2147/OPTO.S151294
6. Jones YJ, Jones JJ. Near and intermediate visual acuity test. J Cataract Refract Surg. 2008;34(2):337–338. doi:10.1016/j.jcrs.2007.10.013
7. Conforti S, Marinelli CV, Zoccolotti P, Martelli M. The metrics of reading speed: understanding developmental dyslexia. Sci Rep. 2024;14(1):4109. doi:10.1038/s41598-024-52330-x
8. Lamoureux D, Yeo S, Bhambhwani V. Reading speed using the international reading speed texts in a normal canadian cohort. Cureus. 2023. doi:10.7759/cureus.38196
9. Trauzettel-Klosinski S, Dietz K. Standardized assessment of reading performance: the new international reading speed texts IReST. Invest Ophthalmol Vis Sci. 2012;53(9):5452. doi:10.1167/iovs.11-8284
10. Zhang J, Liu J, Jasti S, Suryakumar R, Bullimore MA. Visual demand and acuity reserve of Chinese versus english newspapers. Optom Vis Sci. 2020;97(10):865–870. doi:10.1097/OPX.0000000000001585
11. Lapp T, Wacker K, Heinz C, Maier P, Eberwein P, Reinhard T. Cataract surgery—indications, techniques, and intraocular lens selection. Deutsches Ärzteblatt International. 2023;30:377. doi:10.3238/arztebl.m2023.0028
12. Karam M, Alkhowaiter N, Alkhabbaz A, et al. Extended depth of focus versus trifocal for intraocular lens implantation: an updated systematic review and meta-analysis. Am J Ophthalmol. 2023;251:52–70. doi:10.1016/j.ajo.2023.01.024
13. Zamora-de La Cruz D, Zúñiga-Posselt K, Bartlett J, Gutierrez M, Abariga SA. Trifocal intraocular lenses versus bifocal intraocular lenses after cataract extraction among participants with presbyopia. Cochrane Database Syst Rev. 2020;2020(6). doi:10.1002/14651858.CD012648.pub2
14. Calladine D, Evans JR, Shah S, Leyland M. Multifocal versus monofocal intraocular lenses after cataract extraction. Cochrane Collab. 2012;CD003169. doi:10.1002/14651858.CD003169.pub3
15. Kohnen T. First implantation of a diffractive quadrafocal (trifocal) intraocular lens. J Cataract Refract Surg. 2015;41(10):2330–2332. doi:10.1016/j.jcrs.2015.11.012
16. Kohnen T, Herzog M, Hemkeppler E, et al. Visual performance of a quadrifocal (Trifocal) intraocular lens following removal of the crystalline lens. Am J Ophthalmol. 2017;184:52–62. doi:10.1016/j.ajo.2017.09.016
17. Sudhir RR, Dey A, Bhattacharrya S, Bahulayan A. AcrySof IQ PanOptix intraocular lens versus extended depth of focus intraocular lens and trifocal intraocular lens: a clinical overview. Asia-Pac J Ophthalmol. 2019;8(4):335–349. doi:10.1097/APO.0000000000000253
18. Galvis V, Escaf LC, Escaf LJ, et al. Visual and satisfaction results with implantation of the trifocal Panoptix® intraocular lens in cataract surgery. J Optometry. 2022;15(3):219–227. doi:10.1016/j.optom.2021.05.002
19. Kohnen T, Marchini G, Alfonso JF, et al. Innovative trifocal (quadrifocal) presbyopia-correcting IOLs: 1-year outcomes from an international multicenter study. J Cataract Refract Surg. 2020;46(8):1142–1148. doi:10.1097/j.jcrs.0000000000000232
20. Akman A, Asena L, Ozturk C, Güngör SG. Evaluation of quality of life after implantation of a new trifocal intraocular lens. J Cataract Refract Surg. 2019;45(2):130–134. doi:10.1016/j.jcrs.2018.12.003
21. Retzlaff JA, Sanders DR, Kraff MC. Development of the SRK/T intraocular lens implant power calculation formula. J Cataract Refract Surg. 1990;16(3):333–340. doi:10.1016/S0886-3350(13)80705-5
22. Ramulu PY, Swenor BK, Jefferys JL, Rubin GS. Description and validation of a test to evaluate sustained silent reading. Invest Ophthalmol Vis Sci. 2013;54(1):673–680. doi:10.1167/iovs.12-10617
23. Percival SP, Setty SS. Comparative analysis of three prospective trials of multifocal implants. Eye. 1991;5(Pt 6):712–716. doi:10.1038/eye.1991.131
24. Kretz FTA, Breyer D, Diakonis VF, et al. Clinical outcomes after binocular implantation of a new trifocal diffractive intraocular lens. J Ophthalmol. 2015;2015:962891. doi:10.1155/2015/962891
25. Ganesh S, Brar S, Rp N, Rathod D. Clinical outcomes, contrast sensitivity, reading performance and patient satisfaction following bilateral implantation of AT LARA 829MP EDoF IOLs. Clin Ophthalmol. 2021;15:4247–4257. doi:10.2147/OPTH.S331860
26. Hsiao CY, Chang CC, Liu CJ, Liu KH. Effects of the number of strokes, components and usage frequency on the legibility of Chinese characters for optical head-mounted display. Behaviour Inf Technol. 2024;43(4):749–763. doi:10.1080/0144929X.2023.2184181
27. Naujokaitis T, Auffarth GU, Baur ID, et al. Assessment of the efficacy of restoring reading performance after refractive lens exchange with a trifocal intraocular lens. J Refract Surg. 2025;41(8):e786–e796. doi:10.3928/1081597X-20250611-02
28. Kim JH, Won YK, Young CT, Hyung KJ, Lim DH. Comparison of near-distance reading speed based on the intraocular lens type using a Korean reading speed measurement application. Ann Optom Contact Lens. 2024;23(3):107–113. doi:10.52725/aocl.2024.23.3.107
29. Wendelstein JA, Vallotton K, Ziörjen A, et al. Reading speed and visual acuity in photopic and mesopic conditions after bilateral implantation of diffractive multifocal intraocular lenses. Am J Ophthalmol. 2026;281:516–525. doi:10.1016/j.ajo.2025.09.030
30. Ganesh S, Brar S, Pawar A. Long-term visual outcomes and patient satisfaction following bilateral implantation of trifocal intraocular lenses. Clin Ophthalmol. 2017;11:1453–1459. doi:10.2147/OPTH.S125921
31. Cano-Ortiz A, Sánchez-Ventosa Á, Villalba-González M, et al. Clinical and patient reported outcomes of an optimized trifocal intraocular lens. J Clin Med. 2024;13(14):4133. doi:10.3390/jcm13144133
32. Pedrotti E, Carones F, Talli P, et al. Comparative analysis of objective and subjective outcomes of two different intraocular lenses: trifocal and extended range of vision. BMJ Open Ophthalmol. 2020;5(1):e000497. doi:10.1136/bmjophth-2020-000497
33. Llovet-Rausell A, Ortega-Usobiaga J, Albarrán-Diego C, Beltrán-Sanz J, Bilbao-Calabuig R, Llovet-Osuna F. Visual outcomes and patient satisfaction after bilateral refractive lens exchange with a trifocal intraocular lens in 5226 patients with presbyopia. J Refract Surg. 2024;40(7):e468–e479. doi:10.3928/1081597X-20240517-01
34. Torky MA, Nokrashy AE, Metwally H, Abdelhameed AG. Visual performance following implantation of presbyopia correcting intraocular lenses. Eye. 2025;39(1):79–87. doi:10.1038/s41433-022-02188-y
35. Wu HC. Electronic paper display preferred viewing distance and character size for different age groups. Ergonomics. 2011;54(9):806–814. doi:10.1080/00140139.2011.600775
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Visual Outcomes with Enhanced Monofocal and Non-Diffractive Extended Depth-of-Field Intraocular Lenses
Poliński J, Walasik-Szemplińska D, Sempińska-Szewczyk J, Skrzypecki J
Clinical Ophthalmology 2026, 20:595557
Published Date: 9 May 2026
Two-Year Follow-Up of the MINI WELL Non-Diffractive Extended Depth-of-Focus Intraocular Lens: A Retrospective Observational Study
Sborgia A, Curatolo MC, Barattini DF, Niro A, Barattini L, Sborgia G
Clinical Ophthalmology 2026, 20:602800
Published Date: 24 June 2026