")
Back to Journals » Patient Preference and Adherence » Volume 17
Bimekizumab in the Treatment of Plaque Psoriasis: Focus on Patient Selection and Perspectives
Authors Camiña-Conforto G, Mateu-Arrom L, López-Ferrer A, Puig L
Received 3 April 2023
Accepted for publication 24 June 2023
Published 30 June 2023 Volume 2023:17 Pages 1541—1549
DOI https://doi.org/10.2147/PPA.S350760
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Gemma Camiña-Conforto, Laura Mateu-Arrom, Anna López-Ferrer, Lluís Puig
Department of Dermatology, Hospital de la Santa Creu i Sant Pau, Barcelona, Spain
Correspondence: Gemma Camiña-Conforto, Department of Dermatology, Hospital de la Santa Creu i Sant Pau, Mas Casanovas 90, Bloque A, 5a planta (secretaria Dermatología), Barcelona, 08041, Spain, Tel +34 93 553 7007, Fax +34 93 553 7008, Email [email protected]
Abstract: Psoriasis is a chronic systemic inflammatory disease that significatively impairs patients’ quality of life. Biological treatments are highly effective and safe and have led to breakthroughs in the management of patients with moderate-to-severe psoriasis. However, therapeutic response can be unsatisfactory or lost with time, leading to discontinuation of treatment. Bimekizumab is a humanized monoclonal antibody that specifically inhibits both interleukin (IL)-17A and IL-17F. The efficacy and safety of bimekizumab in moderate-to-severe plaque psoriasis has been demonstrated in Phase 2 and Phase 3 clinical trials. Bimekizumab may offer some advantages over other biological treatments, making it especially indicated for certain patients. This narrative review aims to summarize the latest published evidence on the use of bimekizumab for the treatment of moderate-severe plaque psoriasis, focusing on patient selection and therapeutic perspectives. Bimekizumab has been shown to be more efficacious than adalimumab, secukinumab and ustekinumab in clinical trials, with high estimated probabilities of achieving complete (approximately 60%) or almost complete clearance (approximately 85%) of psoriasis at weeks 10– 16, and a good safety profile. Response to bimekizumab is usually fast and maintained in the long term for both biologic-naive patients and those resistant to previous biologic treatments. The usual maintenance dose of 320 mg every 8 weeks makes bimekizumab especially convenient for non-compliant patients. Moreover, the efficacy and safety of bimekizumab have also been demonstrated in psoriasis affecting challenging-to-treat areas, psoriatic arthritis and hidradenitis suppurativa. In conclusion, dual inhibition of IL-17A and IL-17F with bimekizumab is a good therapeutic option for moderate-to-severe psoriasis.
Keywords: psoriasis, bimekizumab, patient selection, interleukin-17, patient compliance, biological therapy
Introduction
Psoriasis is a chronic systemic inflammatory disease,1 with a prevalence of up to 3% of the population worldwide.2 It affects mainly the skin, with variable phenotypes; plaque psoriasis is the most frequent variant, accounting for 80–90% of all cases.3,4 Psoriasis does not only impair patients’ quality of life, but it is also well known to be associated with several comorbidities and with other immune mediated inflammatory diseases such as psoriatic arthritis (affecting up to 30% of patients), inflammatory bowel disease, uveitis, hidradenitis suppurativa and other medical conditions such as cardiometabolic syndrome and depression.1,5,6
The immunopathogenesis of psoriasis involves the innate and adaptive immune system and leads to activation, proliferation, and changes in the differentiation of keratinocytes.3 The etiology of psoriasis is multifactorial, and the interaction between several exogenous and endogenous factors determines its remarkably variable clinical expression and degrees of severity.2
Biological treatments are highly effective and safe and have led to breakthroughs in the management of patients with moderate-to-severe psoriasis.4
Bimekizumab is a humanized monoclonal antibody with dual specificity, inhibiting both IL-17A and IL-17F, and has been approved for treatment of patients with moderate-to-severe plaque psoriasis in several countries (European Union, United Kingdom, Australia, Canada, and Japan).4 The recommended dose for adult patients is 320 mg at weeks 0, 4, 8, 12, 16 and every eight weeks thereafter.7 Several randomized clinical trials have demonstrated the efficacy and safety of bimekizumab for the treatment of psoriatic arthritis, and others are currently ongoing in ankylosing spondylitis, non-radiographic axial spondyloarthritis, and hidradenitis suppurativa.2 On June 7th, 2023, bimekizumab (Bimzelx®) has been granted marketing authorization for treatment of active psoriatic arthritis, non-radiographic axial spondyloarthritis, and ankylosing spondylitis by the European Commission.
This narrative review summarizes the latest published evidence on the use of bimekizumab for the treatment of moderate-severe plaque psoriasis, focusing on patient selection and therapeutic perspectives.
Materials and Methods
We conducted an electronic search of English-language medical literature using PubMed, spanning from the inception to March 31, 2023. The search employed Medical Subject Headings (MESH) terms and relevant medical terminology, focusing on the utilization of bimekizumab for psoriasis treatment, as well as patient preferences and adherence. The search criteria included the combinations of “bimekizumab” AND “psoriasis”, as well as “psoriasis” AND “biologic” AND/OR “treatment”, along with “adherence” AND/OR “preference”. We considered clinical and epidemiological studies, reviews, systematic reviews, meta-analysis, and clinical trials specifically related to the use of bimekizumab for psoriasis treatment or investigating patient preferences and adherence to biological treatment for psoriasis, in English or Spanish.
To date, since bimekizumab has been recently approved, there is limited experience in the clinical setting and no real-world data about adherence to treatment had been published by the time this review was made. Inclusion criteria were as follows: (1) clinical trials focusing on the safety and/or efficacy of bimekizumab; (3) studies focusing on the use of bimekizumab for psoriasis; (3) studies focusing on the preference and adherence of biological treatment in psoriasis.
We found a total of 414 articles. Studies about patients with psoriatic arthritis alone, duplicates or studies related to specific treatments were excluded. The selection of publications was performed by two researchers (G.C and L.M) and discrepancies were resolved by consensus.
From the 414 articles identified, 44 were duplicates and therefore excluded. Another 298 were excluded as they did not offer any pertinent information aligned with our research objectives. Following a comprehensive review of the full-text articles and application of the predefined inclusion/exclusion criteria, 34 publications out of the remaining 72 were eligible for inclusion in the review (Figure 1).
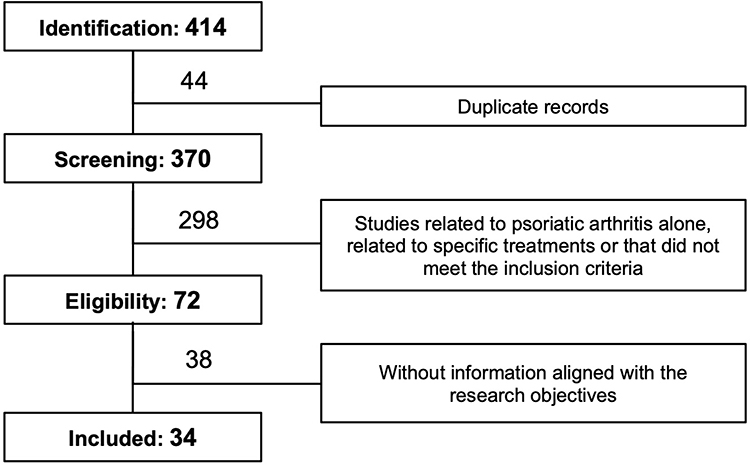 |
Figure 1 PRISMA diagram of the systematic review process. |
Psoriasis Pathogenesis and Targeted Therapies
Psoriasis is an immune mediated disease involving alterations in innate and adaptive immunity, with inflammation and keratinocyte alterations driven by the IL-23/IL-17 axis.3,8 IL-17A, the main effector cytokine of Th17 cells, contributes to protection of epithelial surfaces against extracellular bacteria and fungi, and is also involved in the development and maintenance of autoimmune and chronic inflammatory diseases.9,10 Adaptive immunity elements (T lymphocytes), cells of the innate immune system and resident skin cells can secrete IL-17, taking part in the development of chronic inflammation.11
Although IL-17A is the most biologically active pathogenic cytokine in psoriasis, there are five more IL-17 isoforms (IL-17B to F) involved in the inflammatory psoriatic response, expanding the potential targets for treatment options.12 Bimekizumab is a divalent humanized antibody with two antigen-binding sites recognizing shared epitopes of IL-17A and IL-17F monomers and preventing binding of the IL-17A and IL-17F homodimers and the IL-17A/F heterodimer to their receptors.12
According to some surveys, approximately one in three patients with plaque psoriasis in Spain have moderate-to-severe disease (Psoriasis Area and Severity Index [PASI]>10), and biologic agents account for approximately 20% of systemic treatments prescribed.13,14 So far, IL-17 and IL-23 inhibitors are the most effective biologics but approximately 50% of patients require discontinuation of their biological treatment before the fifth year of treatment due to lack (primary failure) or loss (secondary failure) of efficacy; complete or almost complete skin clearance (PASI100 or PASI90 response in clinical trials, absolute PASI <2 in clinical practice), the current goal of therapy, can be attained by just about 50% of patients, and it can take from 3 to 8 months after the start of treatment to achieve this goal.15–17 Bimekizumab provides an opportunity to improve on this performance with a good safety profile.4
Bimekizumab for the Treatment of Plaque Psoriasis: Efficacy and Safety
The efficacy of bimekizumab in moderate-to-severe plaque psoriasis has been demonstrated in phase 2 (Papp 2018 BE ABLE1, Blauvelt 2020 BE ABLE 2, Oliver 2021 PS0016, Gordon 2022 PS0018),18–21 and phase 3 clinical trials (Gordon 2021 BE READY, Reich 2021 NEJM BE RADIANT, Warren 2021 BE SURE, Reich 2021 Lancet BE VIVID).22–25 Some of the data regarding these clinical trials are shown in Table 1.
 |
Table 1 Table That Summarizes the Main Described Clinical Trials About the Use of Bimekizumab for Plaque Psoriasis |
When compared against placebo in a multicentric, randomized clinical trial (BE READY) including 435 adult patients with plaque psoriasis, bimekizumab treatment was associated with PASI90 and a PASI100 response rates of 91% and 68%, respectively, at week 16, whereas only 1 patient (1%) in the placebo group achieved PASI90 and PASI100 responses.2,22
Head-to-head phase 3/3b trials have compared the efficacy and safety of bimekizumab with secukinumab (BE RADIANT),23 adalimumab (BE SURE),24 and ustekinumab (BE VIVID).25 At week 16, the PASI 90 response rates achieved with bimekizumab (over 85%) were higher than those achieved with adalimumab (47%),24 secukinumab (74%),23 and ustekinumab (50%).25 According to Kokolaris et al. PASI 90 responses were maintained or improved at week 48 after switching from other biological treatments such as adalimumab (with a 96% of maintenance), ustekinumab (100%), or secukinumab (95%).26 The proportion of patients with PASI 90 who achieved PASI 100 with bimekizumab 48 weeks after switching from adalimumab was 83% (vs 59% only with adalimumab), 82% after switching from ustekinumab (vs 68%) and 80% after secukinumab (vs 65%).26
Bimekizumab treatment is associated with a rapid response: one out of two patients achieve PASI90 response in 4 weeks, a significantly higher proportion compared to ustekinumab;25 this finding might indicate the superiority of dual IL-17A and IL-17F blockade over IL-12/23 blockade.12
According to a recent systematic review and meta-analysis of the short-term efficacy of biologic treatments in psoriasis clinical trials, bimekizumab was the most effective biological treatment at weeks 10–16.4 The response rate estimations were 92.3% for PASI 75, 84.0% for PASI 90, and 57.8% for PASI 100, the latter two being significantly higher than those of all the other biologic treatments. The number needed to treat (NNT) estimates for bimekizumab versus placebo were 1.16, 1.22 and 1.74 for PASI 75, PASI 90 and PASI 100, respectively.4 Regarding PASI 100, the NNT estimates of bimekizumab versus adalimumab, ustekinumab, and secukinumab were 2.71, 2.65, and 7.85, respectively.4
Regarding long-term efficacy, most patients with moderate-to-severe psoriasis receiving bimekizumab maintain their clinical response from week 16 to year 3, according to the results of the BE BRIGHT open-label extension trial.27 Strober et al showed that 93% of patients who achieved PASI 90, 81% of patients with PASI 100, and 94% of those with an absolute PASI ≤2 at week 16 maintained the response throughout three years, using modified non-responder imputation (mNRI) of missing data.27
Neutralizing anti-drug antibodies have been found at week 56 in up to 34% of patients receiving the standard treatment regimen of bimekizumab (320 mg every 4 weeks until week 16 and 320 mg every 8 weeks afterwards), but they did not impair the clinical response or the safety profile.7
Sustained skin clearance beyond pharmacokinetic expectations after treatment withdrawal, considered a hallmark of some IL-23 inhibitors, has also been observed for bimekizumab, with a median time to loss of PASI75 and PASI90 response after the last dose of bimekizumab of 32 and 28 weeks, respectively.12,22 The higher rates of complete lesion clearance provided by dual inhibition of IL-17A and IL-17F with bimekizumab, as compared with IL-23 inhibitors, might be explained by the production of IL-17 isoforms by innate lymphoid cells that do not necessarily depend on IL-23 receptor activation.28,29 Furthermore, inhibition of the IL-17F homodimer, which is present in psoriasis lesions at concentrations 30 times higher than IL-17A, might explain the superiority of bimekizumab compared to IL-17A inhibitors.4,23
Bimekizumab is well tolerated and has an acceptable safety profile. A pooled analysis of the safety results of 8 randomized clinical trials (4 phase 2 clinical trials and 4 phase 3 randomized clinical trials) included 1789 patients with moderate-to-severe plaque psoriasis who received at least one dose of bimekizumab.30 The most frequent treatment-emergent adverse events (AEs) were nasopharyngitis (19.1 per 100 person-years), oral candidiasis (12.6 per 100 person-years), and upper respiratory tract infection (8.9 per 100 person-years).30 Serious AEs occurred at a rate of 5.9 per 100 person-years, and AEs leading to discontinuation occurred mainly during the first year of treatment, with an overall incidence rate of 3.8 per 100 person-years.30
Higher rates of oral candidiasis were observed with bimekizumab than with other currently approved IL-17 inhibitors, hinting at a protective role of IL-17F against mucosal Candida infections,12 but the vast majority of oral candidiasis in patients with moderate-to-severe psoriasis treated with bimekizumab in clinical trials were mild to moderate, and did not require treatment discontinuation.30 Serious infections (requiring systemic treatment) were reported in 1.5% of patients, and grade 3/4 neutropenia in 1%, but they were not associated with the use of bimekizumab.7
Thus, treatment with bimekizumab should not be initiated in patients with any clinically important active infection; its use should be cautious in patients with chronic or recurrent infections and it should be discontinued if a patient develops any infection that is severe or is not responding to antimicrobial therapy, until its resolution.7 Bimekizumab treatment should not be initiated in patients with active tuberculosis (TB), and anti-TB therapy should be considered prior to the start of bimekizumab in patients with latent TB or inadequately treated active TB in the past.7
The incidence of inflammatory bowel disease, suicidal ideation or behaviour and major adverse cardiac events was low (≲0.5 per 100 person-years), and no drug safety alerts appeared.30
Bimekizumab in Special Situations
Given the multiple treatment options currently available for psoriasis, treatment should be individualized considering the specific needs for each patient. According to guidelines, the decision-making process should be determined by the disease severity and impact on quality of life, the presence of comorbidities, previous administration and response to previous treatments, taking also into consideration patient’s preferences.31–34
Psoriasis is associated with increased risk of comorbidities, including psoriatic arthritis, hidradenitis suppurativa, and inflammatory bowel disease.1,6,35
To date, there are a total of 38 clinical trials registered in “www.clinicaltrials.gov” focusing on the utilization of bimekizumab; some of them are still ongoing and have not yet produced results. These trials encompass a wide range of conditions, including plaque psoriasis, hidradenitis suppurativa (HS0005), axial spondyloarthritis, ankylosing spondylitis and nonradiographic axial spondyloarthritis (As0014), and psoriatic arthritis (Pa0012).36
The potential therapeutic role of bimekizumab in PsA has already been investigated.37,38 In a phase 3 multicentre double blinded randomized placebo-controlled clinical trial in biologic-naïve patients with active adult-onset psoriatic arthritis, 431 received bimekizumab, 140 received adalimumab (reference treatment), and 281 received placebo.38 At week 16, significantly more patients receiving bimekizumab (44%) reached a 50% or greater improvement in American College of Rheumatology criteria (ACR50) response, compared with the placebo group (10%).38 A similar benefit has been shown in patients with a history of inadequate response or intolerance to treatment with one or two TNFα inhibitors for either psoriatic arthritis or psoriasis.37
Dual inhibition of IL-17A and IL17-F could also be a treatment option for patients with hidradenitis suppurativa: in a double-blind, placebo-controlled randomized clinical trial, the Hidradenitis Suppurativa Clinical Response (HiSCR) rate at week 12 was 57.3% for bimekizumab versus 26.1% for placebo (95% credible interval for difference, 11.0%–50.4%; posterior probability of superiority = 0.998).39
The incidence of inflammatory bowel disease observed with bimekizumab is low, but cases have been reported.29 Thus, in patients with a personal history of inflammatory bowel disease, the use of bimekizumab is not recommended, and it should be interrupted in case of exacerbations or the appearance of symptoms suggestive of inflammatory bowel disease.7
It is known that psoriasis affecting challenging-to-treat areas –such as nails, scalp or palms and soles– is associated with a higher impact in patients’ quality of life and poorer functional outcomes.40 Bimekizumab has demonstrated to be effective for these high-impact areas, with complete clearance sustained by a high number of patients treated for two years, regardless of the dosing regimen (320 mg every four or eight weeks).41 Eighty-nine percent of patients achieved Scalp Investigator’s Global Assessment (IGA) of 0 after one year, and 86.7% after two years under maintenance treatment with 320 mg every 4 weeks.7,41 Regarding nail disease, 54% of patients with a baseline modified Nail Psoriasis Severity Index (mNAPSI) >10 achieved complete clearance (mNAPSI 0) at week 52, and 67.6% after 2 years with the maintenance dose every 4 weeks.41 Also, 81.4% of patients had a palmoplantar-IGA of 0 after the first year of treatment and 83.7% maintained this response at 2 years.41
Although current biologic therapies approved for psoriasis are highly effective, primary and secondary therapeutic failure are still relatively frequent.12 Outcomes may improve after switching (or combining) biological therapies that have primarily or secondarily failed, at the expense of increased costs.15,42,43 In some patients, drug switching can be unsuccessful.12
Dual inhibition of IL-17A and IL-17F may be an option for patients with disease refractory to IL-17 signalling pathway blockade.12 Studies assessing the response of patients not achieving PASI 90 response with adalimumab, ustekinumab, and secukinumab showed a fast and long-term maintained response after switching to bimekizumab without any wash-out period.26 Furthermore, the proportions of patients achieving responses in terms of PASI 100, IGA 0/1, body surface area (BSA) ≤1%, Dermatology Life Quality Index (DLQI) of 0/1, and improvement in scales assessing itch or skin pain were similar in patients who had received prior systemic treatment but were biologic-naïve and those previously treated with biologic agents.44–46
Patients’ Preferences and Adherence to Bimekizumab
Success in treatment of psoriasis depends to a large extent on patients’ adherence to treatment, and it is estimated that up to 40% of patients with psoriasis do not use medication as prescribed.47 Since bimekizumab has been recently approved and there is limited experience in the clinical setting, no real-world data about adherence to treatment have been published yet. Adherence is often influenced by patients’ preferences and satisfaction with the treatment.48,49 Treatment satisfaction with biological therapies is remarkably higher than with other modalities such as topical treatment, phototherapy, or non-biologic systemic treatments, partly due to their efficacy and convenience.50–52 In their systematic review, Belinchon et al observed that a higher efficacy –measured by reduction in Psoriasis Area and Severity Index (PASI)– was related to an increase in treatment satisfaction.47
Incremental PASI improvements allow higher rates of achievement of DLQI 0/1, meaning absent health-related quality of life impairment.53,54 A DLQI score of 0 is reported by 91% of patients with complete skin clearance –measured by static Physician’s Global Assessment (sPGA) of 0–, compared to just 48% of patients with almost complete clearance of psoriasis (sPGA of 1).53 The perception of disease severity is also improved in patients with complete clearance, with 65.5% and 32.6% reporting their disease to be “not at all severe”, respectively.53
These data highlight the importance of complete skin clearance for patients with plaque psoriasis and suggest that residual skin disease may still negatively impact health-related quality of life of patients under treatment.53,55
However, patients’ adherence to psoriasis treatment is not only determined by clinical benefit. Florek et al conducted a systematic review on treatment preferences and treatment satisfaction in psoriasis patients and concluded that treatment preferences were heterogeneous and changed over time.50 Some factors such as treatment location, route of administration or risk of adverse events were also related to patients’ preferences.50 Convenient frequency of administration of some biological agents could play an important role to explain treatment satisfaction associated with the treatment modality.50,52,54
Bimekizumab is administered every 4 weeks until week 16 and then every 8 weeks in most patients; thus, it requires fewer injections and provides some advantages compared to other IL-17 inhibitors.12 However, in some patients, an intensified maintenance dosing regimen with injections every 4 weeks can increase treatment response, especially in patients over 120kg, as described in the Summary of Product Characteristics.7,24 Development of a 2 mL autoinjector containing 320 mg of bimekizumab (ClinicalTrials.gov Identifier: NCT05292131) would reduce the number of injections and might further improve patients’ satisfaction with treatment administration.
Disease severity and expectations based on probability of response also influence patients’ treatment preferences.50 According to Alcusky et al, patients with moderate psoriasis rated dosing as the most important treatment attribute, followed by probability of improvement, while patients with severe psoriasis preferred treatments with high probability of improvement, followed by quality-of-life improvement, and considered safety as relatively less important.48
Patient Selection and Perspectives
Bimekizumab may provide some advantages over other biological treatments, especially in some patient populations. The longer administration interval compared to other IL-17 inhibitors makes bimekizumab well suited for patients with a history of non-compliance or those facing challenges in accessing treatment. Bimekizumab is an ideal option for patients seeking a rapid and complete response, especially those experiencing a significant impairment of their quality of life. Additionally, individuals with involvement of locations with high impact on quality of life (nails, scalp, palmoplantar) or those who have previously experienced failure of other biological treatments for psoriasis would benefit from bimekizumab, which has shown high rates of sustained complete or near-complete clearance in these subgroups of patients. Furthermore, bimekizumab is particularly indicated for patients with comorbid psoriatic arthritis, non-radiographic axial spondyloarthritis, and ankylosing spondylitis, where high levels of response have been demonstrated to start early and continue improving with time.
Conclusion
There is extensive evidence in support of bimekizumab as one of the treatments of choice for moderate-to-severe plaque psoriasis. It provides high expectations of fast response and is the most likely agent to achieve PASI 90 and PASI 100 responses at 10–16 weeks. Its good safety profile, acceptable tolerability, convenient posology, long-term efficacy (with most patients maintaining the response for up to at least 3 years), make bimekizumab a suitable therapeutic option for patients with a chronic disease such as moderate-to-severe psoriasis. In psoriasis, a chronic inflammatory disease with high impact on health-related quality of life, one of the keys to therapeutic success is patients’ adherence to treatment, which is directly related to their preferences and satisfaction. Real-world experience can be expected to eventually confirm the high rates of treatment persistence and maintenance of response observed in open-label extensions of bimekizumab clinical trials.
Disclosure
G. Camiña-Conforto has received honoraria as a speaker for Sun Pharma and UCB. L. Mateu-Arrom does not have any potential conflicts of interest involving the work under consideration for publication. A. López-Ferrer has received honoraria as a speaker, in consultancies and in participation as an investigator in clinical trials for AbbVie, Almirall, Amgen, Janssen, Novartis, Eli Lilly, Leo Pharma and UCB. L. Puig has perceived consultancy/speaker’s honoraria from and/or participated in clinical trials sponsored by AbbVie, Almirall, Amgen, Biogen, BIOCAD, Boehringer Ingelheim, Bristol Myers Squibb, Janssen, Leo-Pharma, Lilly, Novartis, Pfizer, Samsung-Bioepis, Sandoz, Sanofi, and UCB.
References
1. Yamazaki F. Psoriasis: comorbidities. J Dermatol. 2021;48(6):732–740. doi:10.1111/1346-8138.15840
2. Ruggiero A, Potestio L, Camela Snr E, Fabbrocini G, Megna M. Bimekizumab for the treatment of psoriasis: a review of the current knowledge. Psoriasis. 2022;12:127–137.
3. Vidal S, Puig L, Carrascosa-Carrillo JM, González-Cantero Á, Ruiz-Carrascosa JC, Velasco-Pastor AM. From Messengers to Receptors in Psoriasis: the Role of IL-17RA in Disease and Treatment. Int J Mol Sci. 2021;22(13):6740.
4. Armstrong A, Fahrbach K, Leonardi C, et al. Efficacy of bimekizumab and other biologics in moderate to severe plaque psoriasis: a systematic literature review and a network meta-analysis. Dermatol Ther (Heidelb). 2022;12(8):1777–1792.
5. Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker JNWN. Psoriasis. Lancet. 2021;397(10281):1301–1315.
6. Ben Abdallah H, Johansen C, Iversen L. Key signaling pathways in psoriasis: recent insights from antipsoriatic therapeutics. Psoriasis. 2021;11:83–97.
7. Bimekizumab - European medicines agency EMA; 2023. Available from: https://www.ema.europa.eu/en/documents/product-information/bimzelx-epar-product-information_en.pdf.
8. Aggarwal S, Ghilardi N, Xie MH, de Sauvage FJ, Gurney AL. Interleukin-23 Promotes a Distinct CD4 T Cell Activation State Characterized by the Production of Interleukin-17. J Biol Chem. 2003;278(3):1910–1914.
9. Langrish CL, Chen Y, Blumenschein WM, et al. IL-23 drives a pathogenic T cell population that induces autoimmune inflammation. J Exp Med. 2005;201(2):233–240.
10. Louten J, Boniface K, de Waal Malefyt R. Development and function of TH17 cells in health and disease. J Allergy Clin Immunol. 2009;123(5):1004–1011. doi:10.1016/j.jaci.2009.04.003
11. Schön MP, Erpenbeck L. The Interleukin-23/Interleukin-17 Axis Links Adaptive and Innate Immunity in Psoriasis. Front Immunol. 2018;9:1323.
12. Iznardo H, Puig L. Dual inhibition of IL-17A and IL-17F in psoriatic disease. Ther Adv Chronic Dis. 2021;12:204062232110378.
13. Carrascosa J, Pujol R, Dauden E, et al. A prospective evaluation of the cost of psoriasis in Spain (EPIDERMA project: phase II). J Eur Acad Dermatol Venereol. 2006;20(7):840–845.
14. Accion Psoriasis. Encuesta NEXT sobre necesidades actuales y expectativas de futuro en psoriasis en Espana. Informe de resultados 2019. Available from: https://www.accionpsoriasis.org/recursos/publicaciones/otraspublicaciones.html.
15. Zozaya N, Abdalla F, Alfonso Zamora S, et al. Assessing the value contribution of bimekizumab for the treatment of moderate-to-severe psoriasis using a multidisciplinary reflective multi-criteria decision analysis. Expert Rev Pharmacoecon Outcomes Res. 2022;22(6):941–953.
16. Armstrong AW, Soliman AM, Betts KA, et al. Comparative efficacy and relative ranking of biologics and oral therapies for moderate-to-severe plaque psoriasis: a network meta-analysis. Dermatol Ther (Heidelb). 2021;11(3):885–905.
17. Lin P-T, Wang S-H, Chi C. Drug survival of biologics in treating psoriasis: a meta-analysis of real-world evidence. Sci Rep. 2018;8(1):16068.
18. Papp KA, Merola JF, Gottlieb AB, et al. Dual neutralization of both interleukin 17A and interleukin 17F with bimekizumab in patients with psoriasis: results from BE ABLE 1, a 12-week randomized, double-blinded, placebo-controlled phase 2b trial. J Am Acad Dermatol. 2018;79(2):277–286.
19. Blauvelt A, Papp KA, Merola JF, et al. Bimekizumab for patients with moderate to severe plaque psoriasis: 60-week results from BE ABLE 2, a randomized, double-blinded, placebo-controlled, phase 2b extension study. J Am Acad Dermatol. 2020;83(5):1367–1374.
20. Oliver R, Krueger JG, Glatt S, et al. Bimekizumab for the treatment of moderate-to-severe plaque psoriasis: efficacy, safety, pharmacokinetics, pharmacodynamics and transcriptomics from a phase IIa, randomized, double-blind multicentre study. Br J Dermatol. 2022;186(4):652–663.
21. ClinicalTrials.gov. A study to evaluate the long-term safety, tolerability and efficacy of bimekizumab in adult patients with chronic plaque psoriasis; 2017. https://clinicaltrials.gov/ct2/show/NCT03230292.
22. Gordon KB, Foley P, Krueger JG, et al. Bimekizumab efficacy and safety in moderate to severe plaque psoriasis (BE READY): a multicentre, double-blind, placebo-controlled, randomised withdrawal phase 3 trial. Lancet. 2021;397(10273):475–486.
23. Reich K, Warren RB, Lebwohl M, et al. Bimekizumab versus secukinumab in plaque psoriasis. N Engl J Med. 2021;385(2):142–152.
24. Warren RB, Blauvelt A, Bagel J, et al. Bimekizumab versus adalimumab in plaque psoriasis. N Eng J Med. 2021;385(2):130–141.
25. Reich K, Papp KA, Blauvelt A, et al. Bimekizumab versus ustekinumab for the treatment of moderate to severe plaque psoriasis (BE VIVID): efficacy and safety from a 52-week, multicentre, double-blind, active comparator and placebo controlled phase 3 trial. Lancet. 2021;397(10273):487–498.
26. Kokolakis G, Warren RB, Strober B, et al. Bimekizumab efficacy and safety in patients with moderate-to-severe plaque psoriasis who switched from Adalimumab, ustekinumab or secukinumab: results from phase III/IIIb trials. Br J Dermatol. 2023;188(3):330–340.
27. Strober B, Tada Y, Mrowietz U, et al. Bimekizumab maintenance of response through three years in patients with moderate to severe plaque psoriasis: results from the BE BRIGHT open-label extension trial. Br J Dermatol. 2023;ljad035.
28. Armstrong AW, Read C, Leonardi C, Kircik L. IL-23 Versus IL-17 in the pathogenesis of psoriasis: there is more to the story than IL-17A. J Drugs Dermatol. 2019;18(8):S202–8.
29. Jones SA, Sutton CE, Cua D, Mills KH. Therapeutic potential of targeting IL-17. Nat Immunol. 2012;13(11):1022–1025.
30. Gordon KB, Langley RG, Warren RB, et al. Bimekizumab safety in patients with moderate to severe plaque psoriasis. JAMA Dermatol. 2022;158(7):735.
31. Nast A, Smith C, Spuls PI, et al. EuroGuiDerm Guideline on the systemic treatment of Psoriasis vulgaris - Part 1: treatment and monitoring recommendations. J Eur Acad Dermatol Venereol. 2020;34(11):2461–2498.
32. Nast A, Smith C, Spuls PI, et al. EuroGuiDerm Guideline on the systemic treatment of Psoriasis vulgaris – part 2: specific clinical and comorbid situations. J Eur Acad Dermatol Venereol. 2021;35(2):281–317.
33. Carrascosa JM, Puig L, Romero IB, et al. Actualización práctica de las recomendaciones del Grupo de Psoriasis de la Academia Española de Dermatología y Venereología (GPS) para el tratamiento de la psoriasis con terapia biológica. Parte 2 «Manejo de poblaciones especiales, pacientes con comorbilidad y gestión del riesgo». Actas Dermosifiliogr. 2022;113(6):583–609.
34. Carrascosa JM, Puig L, Belinchón Romero I, et al. Actualización práctica de las recomendaciones del Grupo de Psoriasis de la Academia Española de Dermatología y Venereología (GPS) para el tratamiento de la psoriasis con terapia biológica. Parte 1. «Conceptos y manejo general de la psoriasis con terapia biológica». Actas Dermosifiliogr. 2022;113(3):261–277.
35. Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker JNWN. Psoriasis. Lancet. 2021;397(10281):1301–1315.
36. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/ct2/results?cond=&term=bimekizumab&cntry=&state=&city=&dist=.
37. Merola JF, Landewé R, McInnes IB, et al. Bimekizumab in patients with active psoriatic arthritis and previous inadequate response or intolerance to tumour necrosis factor-α inhibitors: a randomised, double-blind, placebo-controlled, phase 3 trial (BE COMPLETE). Lancet. 2023;401(10370):38–48.
38. McInnes IB, Asahina A, Coates LC, et al. Bimekizumab in patients with psoriatic arthritis, naive to biologic treatment: a randomised, double-blind, placebo-controlled, phase 3 trial (BE OPTIMAL). Lancet. 2023;401(10370):25–37.
39. Glatt S, Jemec GBE, Forman S, et al. Efficacy and Safety of Bimekizumab in Moderate to Severe Hidradenitis Suppurativa: a Phase 2, Double-blind, Placebo-Controlled Randomized Clinical Trial. JAMA Dermatol. 2021;157(11):1279–1288.
40. Callis Duffin K, Mason MA, Gordon K, et al. Characterization of Patients with Psoriasis in Challenging-to-Treat Body Areas in the Corrona Psoriasis Registry. Dermatology. 2021;237(1):46–55.
41. Merola JF, Gottlieb A, Morita A, et al. Bimekizumab (BKZ) Efficacy in High-impact Areas for Patients (pts) with Moderate to Severe Plaque Psoriasis: pooled Results through Two Years from the BE SURE and BE RADIANT Phase 3 Trials.
42. Tsai YC, Tsai TF. Switching biologics in psoriasis - practical guidance and evidence to support. Expert Rev Clin Pharmacol. 2020;13(5):493–503.
43. Usha M, Abrar Q, Raquel L. The economic burden of switching biologics in psoriasis: a real-world analysis in the US population. J Am Acad Dermatol. 2014;70:AB191.
44. Strober B, Krueger J, Magnolo N, et al. Bimekizumab versus Ustekinumab Efficacy Across Subgroups of Patients with Moderate to Severe Plaque Psoriasis: results from the Multicenter, Randomized, Double-Blinded Phase 3 BE VIVID Trial. SKIN J Cutaneous Med. 2021;5(1):s16.
45. Lebwohl M, Armstrong AW, Merola JF, et al. Bimekizumab efficacy through one year in patients with moderate to severe plaque psoriasis in subgroups defined by prior biologic treatment: pooled results from four phase 3/3b trials. SKIN J Cutaneous Med. 2022;6(6):s64.
46. Blauvelt A, Iversen L, McBride S, et al. Bimekizumab versus secukinumab efficacy across subgroups of patients with moderate to severe plaque psoriasis: results from the multicenter, randomized, double-blinded phase 3b BE RADIANT trial. SKIN J Cutaneous Med. 2021;5(6):s53.
47. Belinchon I, Rivera R, Blanch C, Comellas M, Lizan L. Adherence, satisfaction and preferences for treatment in patients with psoriasis in the European Union: a systematic review of the literature. Patient Prefer Adherence. 2016;10:2357–2367.
48. Alcusky M, Lee S, Lau G, et al. Dermatologist and Patient Preferences in Choosing Treatments for Moderate to Severe Psoriasis. Dermatol Ther (Heidelb). 2017;7(4):463–483.
49. van Cranenburgh OD, de Korte J, Sprangers MAG, de Rie MA, Smets EMA. Satisfaction with treatment among patients with psoriasis: a web-based survey study. Br J Dermatol. 2013;169(2):398–405.
50. Florek AG, Wang CJ, Armstrong AW. Treatment preferences and treatment satisfaction among psoriasis patients: a systematic review. Arch Dermatol Res. 2018;310(4):271–319.
51. Kromer C, Schaarschmidt ML, Schmieder A, Herr R, Goerdt S, Peitsch WK. Patient preferences for treatment of psoriasis with biologicals: a discrete choice experiment. PLoS One. 2015;10(6):e0129120.
52. Kromer C, Peitsch WK, Herr R, Schmieder A, Sonntag D, Schaarschmidt M. Treatment preferences for biologicals in psoriasis: experienced patients appreciate sustainability. JDDG. 2017;15(2):189–200.
53. Boswell ND, Cook MK, Balogh EA, Feldman SR. The impact of complete clearance and almost complete clearance of psoriasis on quality of life: a literature review. Arch Dermatol Res. 2022. doi:10.1007/s00403-022-02420-5
54. Zhang M, Brenneman SK, Carter CT, et al. Patient-reported treatment satisfaction and choice of dosing frequency with biologic treatment for moderate to severe plaque psoriasis. Patient Prefer Adherence. 2015;9:777–784.
55. Viswanathan HN, Chau D, Milmont CE, et al. Total skin clearance results in improvements in health-related quality of life and reduced symptom severity among patients with moderate to severe psoriasis. J Dermatolog Treat. 2015;26(3):235–239.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.