Back to Journals » Infection and Drug Resistance » Volume 19
Bilateral Knee Infectious Arthritis Caused by Proteus mirabilis Mimicking Reactive Arthritis in an Elderly Patient with Metastatic Cancer: A Case Report
Authors Li Y, Du D, Wen F, Li N, Jia Y
Received 15 December 2025
Accepted for publication 9 March 2026
Published 30 March 2026 Volume 2026:19 589227
DOI https://doi.org/10.2147/IDR.S589227
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sandip Patil
Yang Li,1 Dongjie Du,2 Fenghua Wen,1 Na Li,1 Yitao Jia1
1The Third Department of Oncology, Hebei General Hospital, Shijiazhuang, Hebei, 050051, People’s Republic of China; 2Vascular Surgery Catheterization Room, Hebei General Hospital, Shijiazhuang, Hebei, 050011, People’s Republic of China
Correspondence: Yitao Jia, The Third Department of Oncology, Hebei General Hospital, Shijiazhuang, Hebei, 050051, People’s Republic of China, Email [email protected]
Background: Infectious arthritis is an uncommon but serious condition in older adults and may be easily misdiagnosed due to atypical clinical presentations. Proteus mirabilis is a rare causative pathogen of infectious arthritis, and its manifestations can resemble reactive arthritis, particularly in elderly patients with malignancy or immunocompromised status.
Case Presentation: A 74-year-old woman with advanced endometrial cancer was admitted with fever and urinary tract infection caused by Proteus mirabilis, complicated by septic shock. After initial improvement with intravenous antibiotic therapy, she developed recurrent fever accompanied by bilateral knee swelling and pain. Reactive arthritis was initially suspected, and empiric glucocorticoid therapy resulted in transient symptomatic relief. However, magnetic resonance imaging of both knees demonstrated bone destruction consistent with infectious arthritis. Repeated joint irrigation combined with prolonged antibiotic therapy led to clinical improvement, resolution of fever, and recovery of knee function. Follow-up blood cultures were negative, and the patient remained clinically stable.
Conclusion: This case highlights the diagnostic challenges of differentiating infectious arthritis from reactive arthritis in elderly patients with cancer. In older adults with Proteus mirabilis bacteremia who develop acute joint symptoms, infectious arthritis should be carefully considered, even when initial response to glucocorticoids is observed. Early imaging evaluation and repeated microbiological assessment are essential to avoid delayed diagnosis and improve outcomes in the aging population.
Keywords: Proteus mirabilis, infectious arthritis, reactive arthritis, urinary tract infection
Background
Infectious arthritis is rare, and it is the infection of joints caused by bacteria or viruses that invade the joint cavity, which often affects children or elderly individuals with low resistance.1 The most common pathogens are Staphylococcus aureus and Neisseria gonorrhoeae, but various mycobacteria, spirochetes, fungi and viruses can also infect the articular cavity. The main manifestations of infectious arthritis are joint swelling, increased local skin temperature, pain, accumulation of a large number of serous, fibrinous or purulent exudate in the joint cavity, joint capsule expansion, pressure fluctuation and so on, often accompanied by an increase in body temperature. Articular cartilage destruction, subchondral bone erosion, periarticular hyperosteogeny, bone destruction and synovial thickening can develop into fibrous or bony joint healing, joint rigidity or dead joint over time.
However, the clinical manifestation of reactive arthritis (ReA) is very similar to infectious arthritis, which often occurs secondary to acute non-pyogenic arthritis following infection of the urinary, reproductive, or intestinal tracts.1 Reiter’s syndrome, also known as this disease, is an autoimmune disorder that differs significantly from infectious arthritis in that it is characterized by sterile synovitis.2 The ReA patients are usually young adults, with a mean age of nearly 30–40 years.3,4 It primarily manifests as involvement of one or more joints with varying degrees of severity. Mild cases may only experience joint pain while severe cases present with obvious polyarthritis even leading to restricted movement. Typical manifestations include progressively worsening asymmetric monoarthritis or oligoarthritis affecting lower limb joints such as knee, ankle and hip.
Infectious arthritis especially that caused by Proteus mirabilis is rare. Infectious arthritis secondary to urinary tract infection is also easily confused with ReA. We report an elderly cancer patient who developed bloodstream infection caused by Proteus mirabilis and septic shock after urinary tract infection, followed by high fever and bilateral knee joint swelling and pain. Finally, after several consultations and repeated evaluations, infectious arthritis was diagnosed. The purpose of this case report is to clarify the diagnosis, treatment, and differential diagnosis of high fever and bilateral knee pain in an elderly cancer patient after bloodstream infection, and to provide a reference for clinicians. We obtained written informed consent from the patient and her family to publish clinical details and images.
Case Presentation
A 74-year-old woman with endometrial serous carcinoma and multiple bone metastases was admitted for routine anti-tumor therapy. On admission, vital signs were stable: blood pressure 137/82 mmHg, heart rate 80 bpm, respiratory rate 19 breaths/min, and oxygen saturation 99%. However, she developed chills, sweating, and high fever (peak 38.9°C) on the first night. Blood cultures were obtained, and the following day, she developed hypotension (68/45 mmHg) and tachycardia (125 bpm). Blood cultures revealed Gram-negative bacilli, later identified as Proteus mirabilis, with markedly elevated inflammatory markers.
The patient presented with septic shock and bacteremia, prompting immediate administration of vasopressors and fluid resuscitation. Additionally, meropenem, a susceptible antibiotic against Proteus mirabilis, was promptly initiated for targeted antimicrobial therapy. When the vital signs of the patient were stable, we conducted the CT scan, which revealed the migration of previous left kidney stone into the left ureter, resulting in obstruction by a stone (Figure 1). The etiology of bloodstream infection and septic shock caused by Proteus mirabilis was evident. Therefore, the urological surgeon performed a left ureteral stent implantation for the patient.
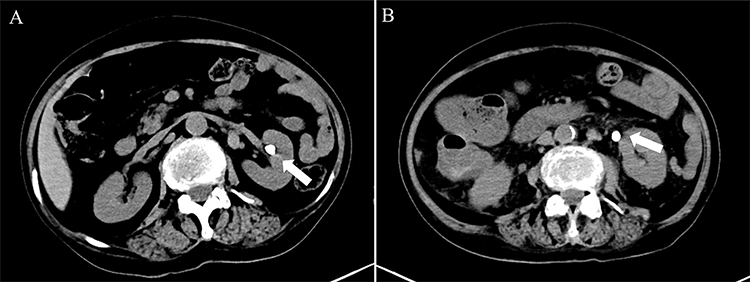 |
Figure 1 Typical CT images of the abdomen during the patient’s two most recent hospitalization. (A) A stone approximately 9 mm in diameter was present in the left renal pelvis on September 20, 2023. (B) A stone about 9 mm in diameter was found at the beginning of the left ureter on November 1, 2023. (The position of the kidney stone is indicated by the white arrow). |
After 8 days of meropenem, the patient experienced a recurrence of fever with a body temperature of 39.0°C, accompanied by an elevation in inflammatory markers. Urine routine analysis revealed a significant presence of white blood cells and bacteria, while both blood culture and urine culture yielded negative results (Figure 2). Following consultation with the pharmacy department, the antibiotic regimen was adjusted to ceftazidime in combination with vancomycin. Despite receiving 12 days of antibiotic therapy since admission, the patient developed another episode of fever along with increased inflammatory markers (Figure 2). During this febrile period, the patient reported pain, local swelling, and elevated skin temperature in bilateral knee joint. Infectious arthritis was considered as a possible diagnosis based on the clinical presentation and history of bloodstream infection of the patient. Intra-articular saline irrigation and local application of meropenem were administered under orthopedic expert guidance. Synovial fluid extracted from bilateral knee joint appeared Greenish-yellow and turbid. Gram stain smears as well as bacterial and fungal cultures were performed but showed no evidence of infection. Moreover, urine routine analysis returned to normal levels. Despite these interventions, the patient’s fever persisted along with sustained elevation in inflammatory markers and continued knee joint pain during episodes.
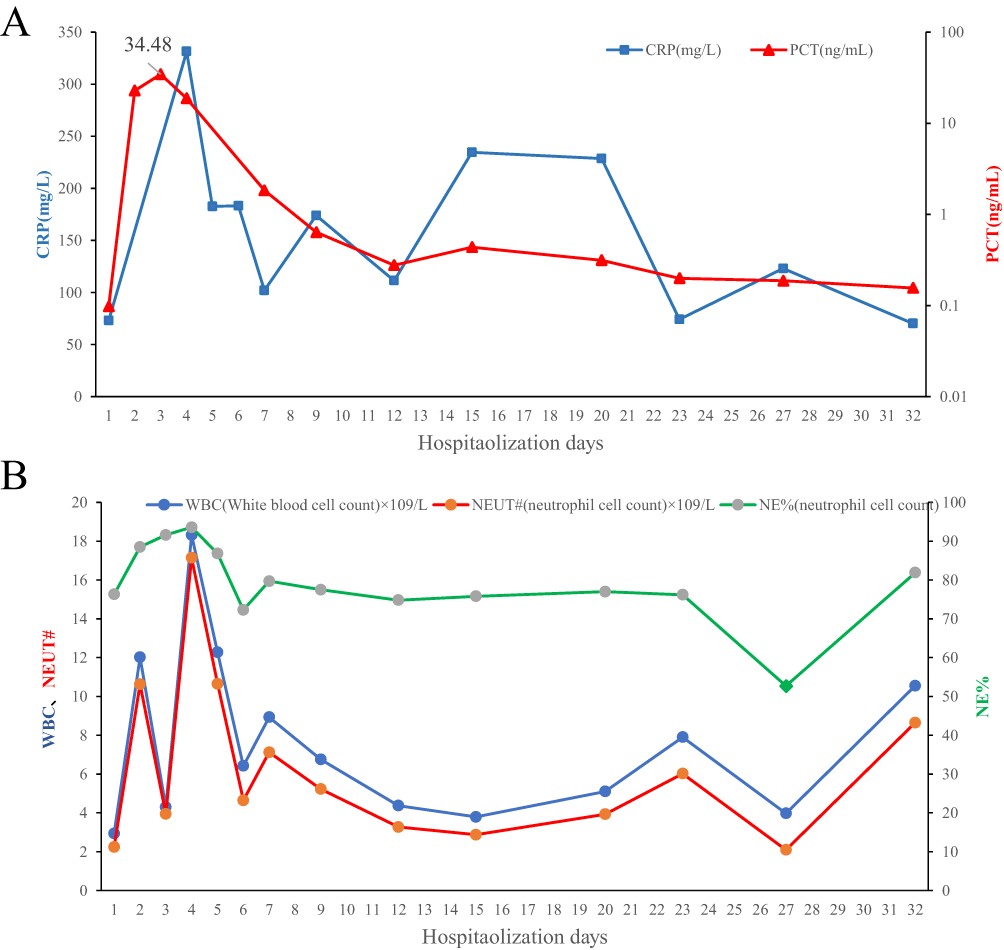 |
Figure 2 The changes in inflammatory markers of patients since admission. (A) CRP and PCT. (B) Leukocyte, neutrophils and the percent of neutrophils. |
We observed inadequate blood concentration of vancomycin, thus the dosage was escalated to 0.5g, q8h. The knee joint continued to be irrigated with saline and locally treated with meropenem. However, the response was not significant. Subsequently, we sought input from multidisciplinary experts in orthopedics, anesthesiology, pharmacy, pain management and rheumatology who opined that other osteoarthritis-related conditions, particularly ReA, cannot be ruled out. Therefore, it is recommended to continue systemic administration of antibiotics. Additionally, a low-dose intravenous dexamethasone (3mg) was administered for its anti-inflammatory effects while bilateral knee joint cavities were continuously irrigated with saline and locally treated with ozone and betamethasone (7mg). Following successful control of bilateral knee joint pain in the patient’s case, an MRI scan can be conducted. As a result of the aforementioned treatment regimen, significant relief in bilateral knee joint pain was achieved along with normalization of body temperature and reduction in inflammatory markers. Furthermore, the patient’s overall condition including mental state and appetite also exhibited improvement.
After glucocorticoid treatment, the patient did not experience fever recurrence and observed improvement in local knee joint pain, swelling, and heat. The possibility of ReA was considered, but rheumatoid arthritis and infectious arthritis needed to be ruled out. Nevertheless, most rheumatoid immune-related hematological indicators such as rheumatoid factor, erythrocyte sedimentation rate, antinuclear antibodies, immunoglobulin, antistreptolysin O were predominantly negative. Unexpectedly, MRI results revealed bilateral knee joint bone destruction with accompanying soft tissue swelling (Figure 3). With guidance from imaging experts and evidence of bloodstream infection taken into account, the final diagnosis was determined as infectious arthritis. Consequently, glucocorticoids were discontinued while antibiotic therapy continued. Subsequently, there was significant relief in local swelling and heat of the bilateral knee joint along with a return to normal body temperature (Figure 4). After a one-month follow-up period without any episodes of high fever or noticeable local pain in the bilateral knee joint (pain score: 1–2), no signs of local swelling in either knee or positive floating patella test were observed. Additionally, the range of motion for the left knee was measured at 0–160° while that for the right knee ranged from 0–150.
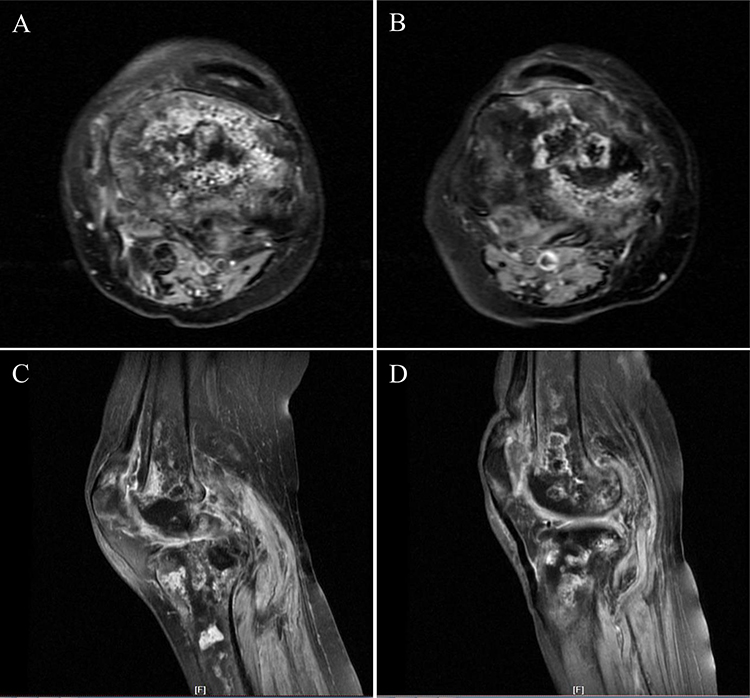 |
Figure 3 Typical MRI images of both knees showed multiple bone destruction, accompanied by surrounding soft tissue swelling. (A) Transverse section images of the left knee. (B) Transverse section images of the left knee. (C) Sagittal section images of the left knee. (D) Sagittal section images of the right knee. |
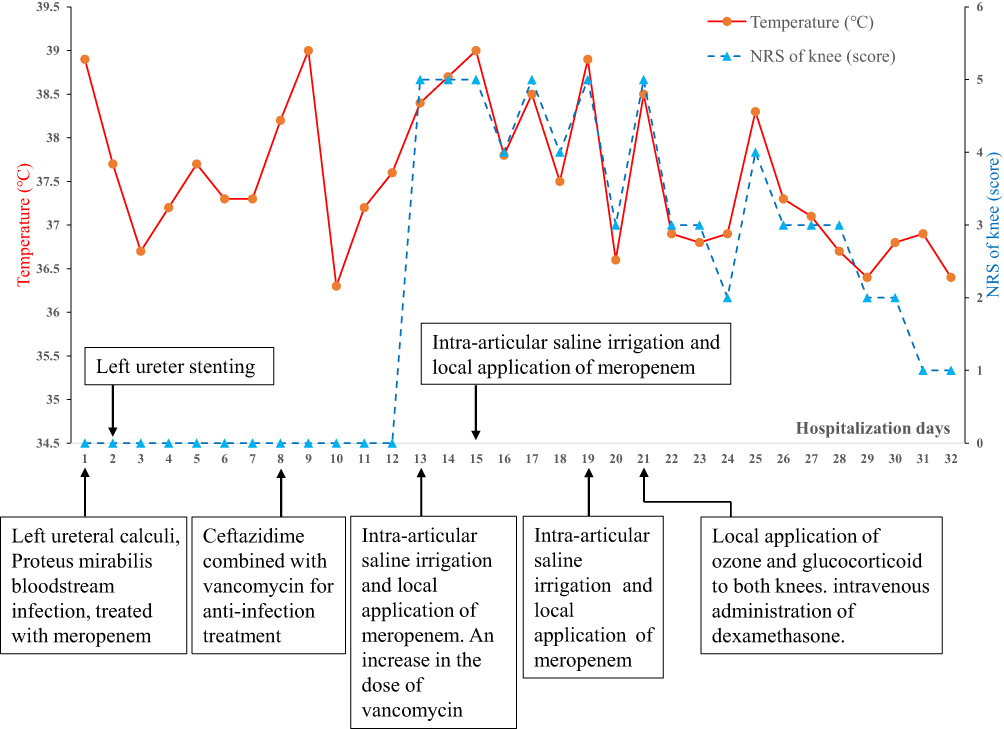 |
Figure 4 Body temperature, NRS of both knees, important symptoms, and treatment timeline during hospitalization. |
Discussion and Conclusion
Clinically, infectious arthritis may not always present typical manifestations, leading to potential misdiagnosis and missed diagnoses. Infectious arthritis is typically characterized by acute joint inflammation and destruction caused by bacterial or fungal infections, with the detection of pathogenic bacteria in joint effusion or tissue still considered the gold standard for diagnosis. However, the positive rate of bacterial culture in articular effusion or synovial fluid ranges from 51% to 80%, while smear tests yield a positive rate of approximately 29% to 71%. The combined detection rate of both methods can be increased.5,6 Clinical manifestations include localized pain, redness and swelling, joint dysfunction, as well as systemic symptoms such as fever and fatigue. Early diagnosis, immobilization of the affected joints, and administration of appropriate antibiotics are crucial for effective treatment.
Infectious arthritis caused by Proteus mirabilis in both knees is a rare occurrence.7 The patient initially presented with septic shock following bloodstream infection due to left ureteral calculi. After the resolution of fever and normalization of vital signs, including blood pressure, heart rate, oxygen saturation, and respiratory rate, the patient experienced recurrent fever accompanied by pain and discomfort in both knees along with local redness, swelling, heat and pain. At this point, infectious arthritis was suspected. Intravenous antibiotics ceftazidime and vancomycin were administered to the patient while adjusting antibiotic concentration as needed. Bilateral knee joint cavity aspiration for effusion extraction was performed along with bacterial and fungal culture as well as smear examination, however all yielded negative results. Local saline irrigation and application of antibiotic meropenem were also implemented in both knees but proved unsatisfactory.
In cases where conservative treatment fails to produce satisfactory outcomes, arthroscopic surgery may be considered for exploration or debridement of the infected site. However, due to the patient being an elderly female with a frail constitution and a history of advanced malignant tumors, she was unable to tolerate arthroscopic surgery despite receiving local application of sensitive antibiotics through intravenous and bilateral knee joint. As a result, intermittent fever and knee joint pain persisted. After conducting a comprehensive evaluation, we speculated whether there might be alternative diagnostic possibilities for the patient.
ReA is an immune-mediated seronegative form of arthritis that typically manifests 1–4 weeks following infections in other body regions, often associated with genitourinary or gastrointestinal tract infections without microbial invasion into the joint cavity.8–10 It presents with conjunctivitis, arthritis, and urethritis but can also display diverse additional manifestations.11 Diagnosis primarily depends on clinical evaluation, and around 10% of patients might have previously experienced asymptomatic related infections while only one-third exhibit the aforementioned typical triad symptoms.1
Furthermore, ReA can solely manifest as symptoms related to joint inflammation which are challenging to differentiate from clinical manifestations associated with infectious arthritis such as fever, swelling and pain. Severe cases may also experience restricted joint mobility. Evidence for prior infection can be detected through blood culture, urine culture or stool culture in nearly 60% clinically diagnosed ReA patients. Previous studies had indicated that HLA-B27 sensitivity is not highly reliable as a diagnostic marker for acute ReA. Furthermore, ReA can present solely as symptoms related to joint inflammation, which pose challenges in distinguishing them from clinical manifestations associated with infectious arthritis such as fever, swelling, and pain. Severe cases may also exhibit restricted joint mobility. Evidence of prior infection can be detected through blood culture, urine culture, or stool culture in approximately 60% of clinically diagnosed ReA patients.12 Previous studies have indicated that HLA-B27 sensitivity is not highly reliable as a diagnostic marker for acute ReA.1
Bacterial and fungal cultures as well as smear staining of the joint effusion yielded negative results. No significant pain relief was observed with either systemic or intraarticular administration of antibiotics. Therefore, considering the patient’s history of urinary tract infection, ReA was considered while rheumatoid arthritis was ruled out. The treatment for ReA primarily involves systemic and topical application of glucocorticoids. Additionally, oral nonsteroidal anti-inflammatory drugs can help alleviate associated symptoms.2 In cases where there is a clear history of prodromal infection, short-term use of antibiotics may be considered. Following the administration of low-dose glucocorticoids to the knee joint and systemically, the patient’s temperature returned to normal and local swelling and pain in the knee joint were relieved. Surprisingly, MRI results revealed significant bone destruction in both knees, leading to a final diagnosis of infective arthritis.
Our analysis concluded that infective arthritis typically results in early bone destruction and is frequently accompanied by damage to surrounding tissues. Considering the patient’s history of malignancy, weakened immune system, and previous bloodstream infections, treatment should be prolonged. The initial administration of antibiotics did not yield satisfactory outcomes, possibly due to inadequate treatment. Glucocorticoids (GC) are crucial regulatory molecules with anti-inflammatory properties within the body. In this patient who experienced a bloodstream infection caused by urinary calculi from Proteus mirabilis followed by septic shock and fever, GC was administered in conjunction with antibiotics.13,14 The patient exhibited severe systemic inflammation and involvement of both knees. Combining antibiotic therapy with glucocorticoids may prove more effective; however, due to the presence of infective arthritis in the patient, antibiotic treatment should remain the primary approach supplemented by glucocorticoids.
It should be noted that this study has certain limitations in etiological diagnosis. The final diagnosis of this case was mainly derived from a comprehensive inference based on typical imaging findings, clinical symptoms and signs, and laboratory test results. The synovial fluid culture result was negative, and a clear etiological confirmation could not be achieved through synovial fluid detection. Ideally, further molecular biological tests should be carried out for joint effusion, among which metagenomic next-generation sequencing (mNGS) can effectively make up for the deficiencies of traditional culture methods. However, due to the extremely small amount of joint effusion in the patient, it was impossible to obtain sufficient samples for detection, so the above-mentioned molecular biological tests could not be completed, resulting in the failure to achieve 100% etiological confirmation of this case. This is the main limitation of this study.
This case suggests that in situations where clinical manifestations fail to differentiate between infectious arthritis and ReA, it is crucial to promptly conduct a thorough pathological examination for confirmation of the diagnosis. In cases where the pathological examination yields negative results, the diagnosis should be confirmed by considering both the bloodstream infection and imaging examination. For clinically suspected infectious arthritis with atypical manifestations and culture‑negative joint effusion, especially in elderly immunocompromised patients, mNGS and other molecular biological detections of articular effusion should be prioritized to achieve rapid and precise etiological diagnosis, so as to guide individualized and accurate anti‑infective treatment. Furthermore, it is essential to ensure comprehensive and meticulous collection of medical history, perform a thorough physical examination, and carry out relevant laboratory tests in order to remain vigilant for subtle changes in disease progression and minimize misdiagnosis.
Data Sharing Statement
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This case report is retrospectively. It only collects clinical data and images of patients, does not interfere with the patient’s treatment plan, and does not bring risks to the patient’s physiology. The need for ethics approval and consent was waived.
Consent for Publication
This report has obtained informed consent signed by the patient and her family.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was not supported by any fundings.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Hannu T. Reactive arthritis. Best Pract Res Clin Rheumatol. 2011;25(3):347–8. doi:10.1016/j.berh.2011.01.018
2. Stegert M. Reactive arthritis. Ther Umsch. 2023;80(1):34–38. doi:10.1024/0040-5930/a001404
3. Mattila L, Leirisalo-Repo M, Koskimies S, et al. Reactive arthritis following an outbreak of Salmonella infection in Finland. Br J Rheumatol. 1994;33(12):1136–1141. doi:10.1093/rheumatology/33.12.1136
4. Mattila L, Leirisalo-Repo M, Pelkonen P, et al. Reactive arthritis following an outbreak of Salmonella Bovismorbificans infection. J Infect. 1998;36(3):289–295. doi:10.1016/S0163-4453(98)94243-8
5. Hassan AS, Rao A, Manadan AM, et al. Peripheral bacterial septic arthritis: review of diagnosis and management. J Clin Rheumatol. 2017;23(8):435–442. doi:10.1097/RHU.0000000000000588
6. Ross JJ. Septic arthritis of native joints. Infect Dis Clin North Am. 2017;31(2):203–218. doi:10.1016/j.idc.2017.01.001
7. Sbiti M, Bouhamidi B, Louzi L. Proteus mirabilis septic arthritis. Pan Afr Med J. 2017;26:197. doi:10.11604/pamj.2017.26.197.12271
8. Ahmed S, Padhan P, Misra R, et al. Update on post-streptococcal reactive arthritis: narrative review of a forgotten disease. Curr Rheumatol Rep. 2021;23(3):19. doi:10.1007/s11926-021-00982-3
9. Inman RD, Whittum-Hudson JA, Schumacher HR, et al. Chlamydia and associated arthritis. Curr Opin Rheumatol. 2000;12(4):254–262. doi:10.1097/00002281-200007000-00004
10. Lv P, Liu P, Zhou X, et al. A case of reactive arthritis caused by a perianal abscess. SAGE Open Med Case Rep. 2023;11:2050313X231177764. doi:10.1177/2050313X231177764
11. Buchanan WW, Kean WF, Rainsford KD, et al. Reactive arthritis: the convoluted history of Reiter’s disease. Inflammopharmacology. 2023. doi:10.1007/s10787-023-01336-4
12. Fendler C, Laitko S, Sörensen H, et al. Frequency of triggering bacteria in patients with reactive arthritis and undifferentiated oligoarthritis and the relative importance of the tests used for diagnosis. Ann Rheum Dis. 2001;60(4):337–343. doi:10.1136/ard.60.4.337
13. Bannuru RR, Schmid CH, Kent DM, et al. Comparative effectiveness of pharmacologic interventions for knee osteoarthritis: a systematic review and network meta-analysis. Ann Intern Med. 2015;162(1):46–54. doi:10.7326/M14-1231
14. Yang M, Chen J, Wei W. Dimerization of glucocorticoid receptors and its role in inflammation and immune responses. Pharmacol Res. 2021;166:105334. doi:10.1016/j.phrs.2020.105334
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.