Back to Journals » Clinical Ophthalmology » Volume 18
Bilateral Femtosecond Laser-Assisted Clear Lens Extraction with Trifocal Intraocular Lens Implantation for Presbyopia Correction: A Short-Term Observational Study in Chinese Adults
Authors Li Q ![]() , Xie X, Yang J, Gao P, Li W
, Xie X, Yang J, Gao P, Li W
Received 4 December 2023
Accepted for publication 25 February 2024
Published 29 February 2024 Volume 2024:18 Pages 623—630
DOI https://doi.org/10.2147/OPTH.S453143
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Qingchen Li,1– 3,* Xiaolin Xie,1,2,* Jiasong Yang,1,2,4 Peng Gao,5 Wensheng Li1,2,4
1Shanghai Aier Eye Hospital, Aier Eye Hospital Group Co. Ltd, Shanghai, 201103, People’s Republic of China; 2Shanghai Aier Eye Institute, Aier Eye Hospital Group Co. Ltd, Shanghai, 201103, People’s Republic of China; 3Department of Ophthalmology, The Second Xiangya Hospital of Central South University, Changsha, Hunan Province, 410011, People’s Republic of China; 4Aier School of Ophthalmology, Central South University, Changsha, Hunan Province, 410015, People’s Republic of China; 5Department of Ophthalmology, Shanghai Tenth People’s Hospital of Tongji University, Tongji University School of Medicine, Shanghai, 200072, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wensheng Li, Shanghai Aier Eye Hospital, Aier Eye Hospital Group Co. Ltd, No. 83 Wuzhong Road, Xuhui District, Shanghai, 201103, People’s Republic of China, Email [email protected]
Purpose: To observe the outcome of bilateral femtosecond laser-assisted clear lens extraction with trifocal intraocular lens (IOL) implantation for presbyopia correction and evaluate its feasibility in early presbyopic adults.
Methods: Prospective case series of eyes with clear crystalline lenses that underwent femtosecond laser-assisted lens extraction and trifocal IOL (Acrysof IQ PanOptix, Model TFNT00, Alcon) implantation between 2021 and 2023 were followed up for at least 3 months after surgery. Outcome measures included monocular uncorrected visual acuity at near (UNVA, 40 cm), intermediate (UIVA, 60 cm), and distance (UDVA, 5 m), monocular manifest refraction, corrected distance visual acuity (CDVA), defocus curve assessment, and spectacle independence at both near and distance.
Results: A total of 60 eyes from 30 consecutive patients were included, and their mean age was 50.4± 6.5 years. After surgery, the mean UNVA (LogMAR) increased from 0.28± 0.16 to 0.08± 0.07, UIVA increased from 0.25± 0.12 to 0.09± 0.06, and UDVA increased from 0.27± 0.21 to 0.01± 0.08. The enhancements of UNVA, UIVA and UDVA were all significant (P < 0.05). The optometric results showed that the mean postoperative spherical equivalent (SE) was − 0.21± 0.24 D, and the mean postoperative CDVA (LogMAR) was − 0.00± 0.06. The preoperative spectacle independences at near and distance were 46.7% (14/30) and 56.7% (17/30), respectively, and both increased to 100% at 3 months after surgery.
Conclusion: Satisfactory visual outcomes and safe surgical procedures were observed in this study, which demonstrate that bilateral femtosecond laser-assisted clear lens extraction with PanOptix IOL implantation could be a feasible approach for presbyopia correction in working-age Chinese patients.
Keywords: presbyopia-correcting, clear lens extraction, refractive lens exchange, trifocal intraocular lens, refractive surgery
Introduction
As a global problem affecting over a billion people worldwide, presbyopia is characterized by loss in physiological accommodation and causes an inability to focus on nearby objects.1 Due to aging, near vision in adults older than age 40 progressively decreases. Epidemiologic studies have shown that approximately 1.8 billion people worldwide suffer from presbyopia, and nearly half of them are working-age individuals.2 Growing evidence suggests that near vision is important in terms of quality of life, as much as, if not more than, distance vision, and both distance and near visual impairments are likely to experience difficulties in daily living, restrictions in educational achievement, increased risks of falls and fractures, social isolation, cognitive deficits, and increased needs for health care services.3
Strategies for correcting presbyopia include optical devices, medication and surgery, and surgical treatments can be subdivided into three major categories that involve the sclera (scleral expansion), cornea (corneal inlays) and crystalline lens. The removal of the natural crystalline lens followed by implantation of an artificial multifocal intraocular lens (IOL) has been an option for presbyopia. Separating from conventional cataract surgery, where an opaque crystalline lens has to be removed for visual improvement, the term “clear lens exchange” was mainly used in patients with extreme myopia for refractive correction4 and in patients with angle-closure glaucoma in the past few decades.5 Although it was not a new concept, clear lens exchange has not become widely accepted as a definite therapy for presbyopia correction. In recent years, there have been some advances in the field of refractive cataract surgery, such as modern biometry, novel IOL design and manufacturing, new generation of IOL power formulas, and precise surgical techniques such as intraoperative navigation and femtosecond laser assistance, which have made it possible to correct presbyopia by means of clear lens exchange.
Per a literature review, we found that there are few studies about the outcomes of clear lens exchange for presbyopia correction in early presbyopic adults in the Chinese population. Contrary to that is the increasing clinical need for presbyopia correction, which could be seen in working-age patients accompanied by increased visual requirements. Recently, studies focusing on a trifocal/quadrifocal IOL called “PanOptix” provided inspiring postoperative visual outcomes and satisfaction in elderly patients with cataracts,6,7 which led us to believe that surgery combining femtosecond laser assistance and this trifocal/quadrifocal IOL implantation would offer more satisfying results in working-age presbyopic patients. Thus, we conducted the present study to make a short-term observation of the above therapeutic approach and evaluate its feasibility in early presbyopic adults with clear crystalline lenses. To our knowledge, this is the first case series describing the outcomes of bilateral femtosecond laser-assisted clear lens extraction with trifocal IOL implantation for presbyopia correction in China, where it is considered an “off-label” procedure.
Methods
Ethics
This prospective, observational study was conducted at Shanghai Aier Eye Hospital. All study procedures were performed in accordance with the tenets of the Declaration of Helsinki and its amendments. The ethics committee of Shanghai Aier Eye Hospital approved this study. Written informed consent was obtained from all participants for the usage and publication of their clinical data.
Patients and Eligibility
Presbyopia in the present study was generally defined as distance corrected near vision of 0.3 LogMAR (20/40) or worse, with healthy eyes and clinically insignificant media opacity with corrected distance visual acuity (CDVA) of 0.1 LogMAR (20/25) or better. Presbyopic patients who were willing to undergo extraction of a clear crystalline lens combined with implantation of a trifocal IOL between October 2021 and June 2023 in Shanghai Aier Eye Hospital were screened for possible inclusion. After a clinic consultation, some patients were preliminarily excluded according to the criteria described below:
Preoperative Biometry
After the primary screening, the enrolled patients received a complete preoperative ophthalmic examination, including subjective optometry with spherical equivalent (SE) and CDVA, A/B-scan ultrasound (Aviso S, 10 MHz probe, Paris, France), noncontact specular microscopy (EM-4000, Tomey Nishi-Ku, Nagoya, Japan), biometry with the IOLMaster (Model 700, Carl Zeiss Meditec Ltd, Jena, Germany), Scheimpflug device imaging (Pentacam HR, Oculus Optikgeräte GmbH, Wetzlar, Germany), scanning laser ultrawide-field fundus imaging (P200 Optomap Plus, Optos, Edinburgh, UK), a spectral-domain optical coherence tomography (OCT) scan for both the macula and optic nerve head (Spectralis, Heidelberg Engineering, Heidelberg, Germany), and a comprehensive evaluation of dry eye. In addition, higher order aberrations (HOAs), angle alpha and angle kappa were measured with a ray-tracing aberrometry, iTrace Visual Function Analyzer (Tracey™ Technologies, TX, USA). Data acquisition was performed according to the user guidelines of each device, and high-quality measurements were used. Patients were further excluded from the present study if their measurements met the following criteria:
Trifocal Intraocular Lens
The Acrysof IQ PanOptix (Model TFNT00, Alcon Laboratories, Inc, Fort Worth, TX, USA) is a single-piece IOL consisting of hydrophobic, ultraviolet and blue light–filtering acrylate/methacrylate copolymer material. The biconvex lens has a 6.0-mm optical zone composed of a central 4.5-mm diffractive area with 15 diffractive zones and an outer refractive rim on the aspheric anterior surface. The Acrysof IQ PanOptix TFNT00 divides incoming light based on a nonapodized quadrifocal technology and creates focal points at near (40 cm), intermediate (60 cm), and distant positions. Moreover, there is an extended intermediate focal point at 120 cm. The light from the 120 cm focal point is diffracted to the distance focal point, leading to optimized light use toward distance vision. In summary, the PanOptix TFNT00 is a quadrifocal IOL that acts like a trifocal IOL and provides high spectacle independence. (Courtesy of Alcon Laboratories)
Intraocular Lens Power Calculation
IOL power calculations were performed with the Barrett Universal II formula using the IOLMaster 700 system built-in Barrett Suite or via an online calculator (http://calc.apacrs.org/barrett_universal2105/). The lens factor value of PanOptix TFNT00 was +1.94 according to the manufacturers. For the Barrett Universal II formula, it is nonessential but recommended that the anterior chamber depth, the white-to-white corneal diameter, and the lens thickness are additionally input because they might contribute to more accurate results. Targeted postoperative refraction was planned for all eyes, and the IOL power with the minimum myopic prediction rather than hypermetropic was selected.
Surgical Procedures
All patients received surgery on both eyes on separate days. Surgery was performed under topical anesthesia induced with 0.5% proparacaine hydrochloride (Alcaine, Alcon Laboratories, Inc, Fort Worth, TX, USA) and sufficient pupillary dilation. Femtosecond laser-assisted procedures were performed using the Catalys Precision Laser System (Abbott Medical Optics Inc, Santa Ana, CA, USA). A disposable vacuum interface was positioned and fixed to the globe using a suction ring, and the laser aperture was engaged with the vacuum interface-globe complex, which was liquid-mediated without corneal contact. After the biometric information was measured and displayed on the control panel, capsulotomy (diameter 5.1 mm) and lens fragmentation (grid of 500 μm size with 2 segment cuts, energy profiles were set by the manufacturer) were performed. Then, the patients were transported to a conventional surgical platform. Corneal incisions (a 2.2-mm width clear corneal primary incision at 135 degrees and a side-port incision at 30 degrees) were performed manually, followed by traditional phacoemulsification, irrigation and aspiration of the cortex using the CONSTELLATION® Vision 106 System (Alcon Laboratories, Inc, Fort Worth, TX, USA) by the same surgeon (W.L.), and all the IOLs were placed in the capsular bag. All the procedures in this study were uneventful, and none of the patients had any significant intraoperative complications. Postoperatively, operative eyes received the same treatment regimen, consisting of a combination of an antibiotic, steroid, and nonsteroidal anti-inflammatory eye drop.
Main Outcome Measures
Postoperative follow-up was at least 3 months. Slit-lamp examination, intraocular pressure, monocular manifest refraction and visual acuity were the primary outcomes, and visual acuity included uncorrected visual acuity at near (UNVA, 40 cm), intermediate (UIVA, 60 cm), and distance (UDVA, 5 m). Visual acuity was measured using a Snellen chart under photopic conditions and converted to a logarithm of the minimum angle of resolution (LogMAR) scale for statistical analysis. Secondary outcomes were defocus curve assessment and spectacle independence at both near and distance. In addition, all the side effects or complications that occurred during the follow-up period were also recorded.
Statistical Analysis
Statistical analyses were performed using the software package SPSS Statistics 26.0 for Windows (SPSS Inc, Chicago, IL, USA). The Kolmogorov‒Smirnov test was used to assess data normality. Continuous variables of normality are expressed as the mean ± standard deviation (SD) or the median. Comparisons between preoperative and postoperative visual acuity were performed using paired t-tests. Statistical significance was set at P < 0.05.
Results
A total of 60 eyes from 30 consecutive patients were included. Their mean age was 50.4±6.5 years, and half of the patients were female. The demographic data and characteristics are presented in Table 1. As shown in Figure 1, UNVA (LogMAR) increased from 0.28±0.16 to 0.08±0.07, UIVA increased from 0.25±0.12 to 0.09±0.06, and UDVA increased from 0.27±0.21 to 0.01±0.08. The enhancements in UNVA, UIVA and UDVA were all statistically significant (all P < 0.05). The optometric results at 3 months after surgery revealed that the mean postoperative sphere was −0.03±0.24 D (ranging from −0.5 D to +0.25 D), the mean postoperative cylinder was −0.36±0.13 D (ranging from −0.75 D to −0.25 D), and the mean postoperative SE was −0.21±0.24 D (ranging from −0.75 D to +0.13 D). The mean postoperative CDVA (LogMAR) was −0.00±0.06 (ranging from −0.1 to 0.1). Monocular defocus curves were measured as shown in Figure 2. There were two visual peaks observed at distance and near-intermediate area (40 to 60 cm), and the mean VA LogMAR at distance and near-intermediate area were 0.01±0.08 and 0.09±0.06, respectively. The preoperative spectacle independence at near and distance was 46.7% (14/30) and 56.7% (17/30), respectively. The postoperative spectacle independence at both near and distance was increased to 100% at 3 months after surgery, which revealed a significant improvement.
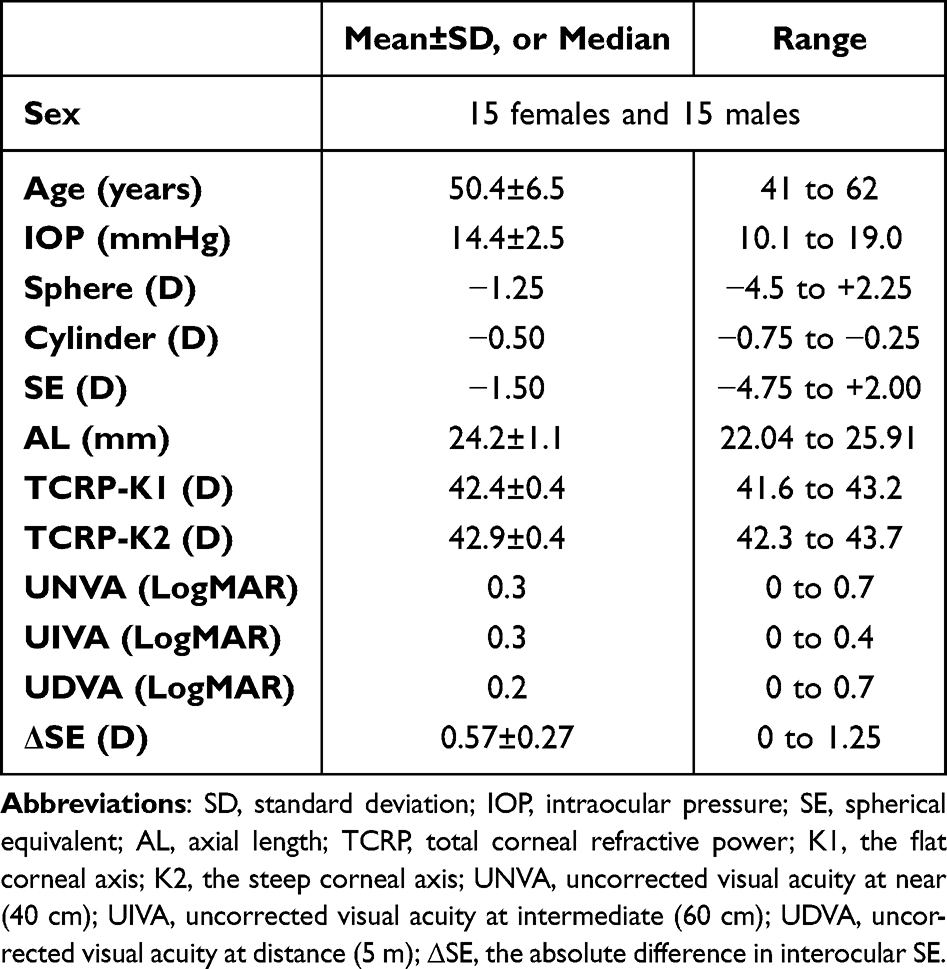 |
Table 1 The Demographic Data and Characteristics of Patients with Clear Lens Extraction |
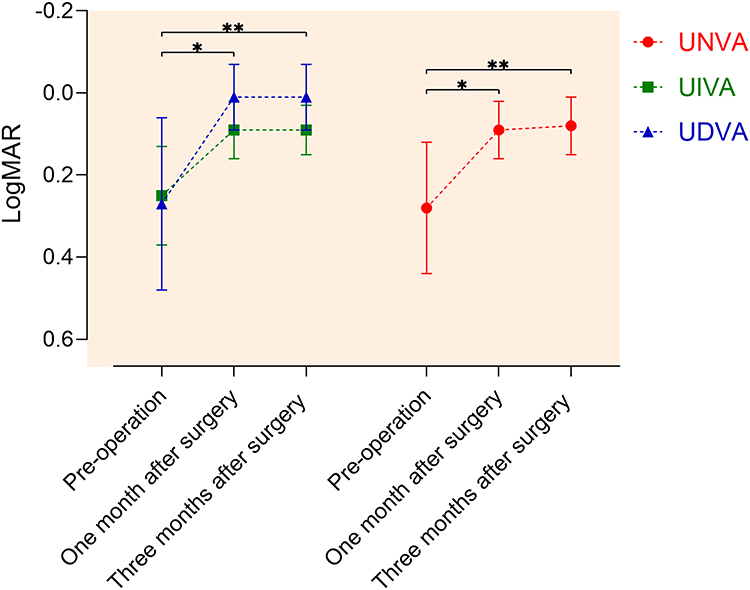 |
Figure 1 Uncorrected visual acuity at near (UNVA, 40 cm), intermediate (UIVA, 60 cm), and distance (UDVA, 5 m) over the 3-month follow-up period. Compared with the preoperative values, the UNVA, UIVA and UDVA improved significantly (*Preoperation vs 1 month after surgery, P < 0.05; **Preoperation vs 3 months after surgery, P < 0.05). |
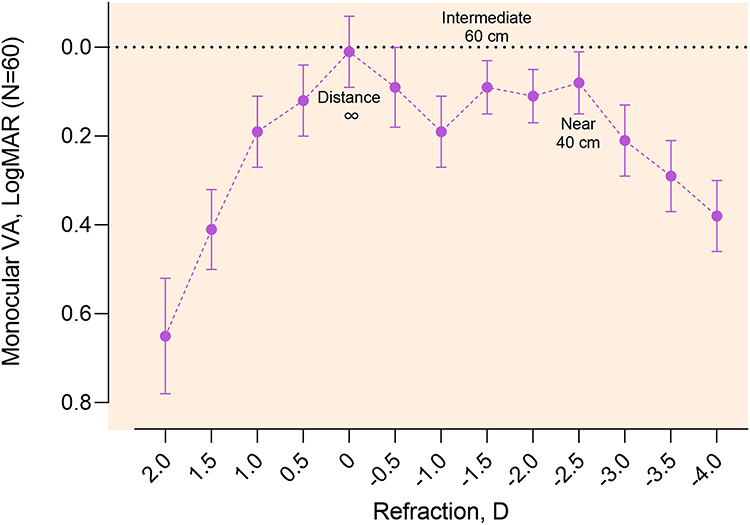 |
Figure 2 Monocular defocus curve at 3 months after PanOptix TFNT00 implantation (N = 60). |
Discussion
Since there is surgical risk and IOLs induce aberrant light perception disturbances, the motivation to achieve spectacle independence should outweigh the potential adverse effects. Only for those who were definitely not satisfied with their near vision could the subsequent surgery be meaningful. In recent years, benefiting from technological advances, there has been an increasing tendency of refractive lens exchange. In this prospective, observational study, all patients with clear crystalline lenses were included through a prudent screening; therefore, it was not surprising that excellent surgical outcomes were observed. We reported the first clinical results of bilateral femtosecond laser-assisted clear lens extraction with PanOptix IOL implantation for presbyopia correction in working-age Chinese presbyopic patients. As noted above, the mean postoperative UNVA, UIVA and UDVA (LogMAR) were 0.08±0.07, 0.09±0.06, and 0.01±0.08, respectively. The spectacle independence rate increased from 46.7% to 100% at near and from 56.7% to 100% at distance, with neither intraoperative nor postoperative complications occurring. Our results showed that we could get satisfactory outcome in Chinese population, as reported in Caucasians,8,9 and this successful case series could be regarded as evidence for clear lens extraction and provided us with a referable protocol for future presbyopia therapy.
The Acrysof IQ PanOptix TFNT00 is the first and only trifocal IOL to be approved by the US Food and Drug Administration.10 At a pupil diameter of 3.0 mm, approximately 40% of the light energy is directed to distance, with approximately 25% at near and 22% at intermediate. When the pupil dilates to 6.0 mm, the light energy at distance increases to 70% with 10% each at near and intermediate. The surgical strategy that combines femtosecond laser assistance with PanOptix IOL implantation might be the optimum choice for presbyopia correction via the lens approach at the current stage. The benefits of femtosecond laser-assisted cataract surgery include lower cumulative phacoemulsification time and endothelial cell loss, more centered capsulotomy, and less posterior capsular opacification (PCO) formation. The PanOptix IOL could offer better postoperative UNVA compared with the extended depth of focus IOL7 and decrease the risk of PCO formation.11 Therefore, considering that working-age presbyopic patients require high visual quality and frequent near vision, we chose the present surgical strategy and observed the outcome. Since the focuses at near, intermediate, and distance are probably different between various IOLs, to unify the conditions as much as possible, patients who underwent other trifocal IOL or extended depth of focus IOL (such as AT LISA tri 839MP or Symfony ZXR00) were excluded. In addition, we believe that binocular vision is a more physical solution and should be the first-line approach for presbyopia correction. According to Lan et al, among six treatment protocols for cataract surgery with presbyopia correction, the bilateral trifocal protocol showed the best performance, while the monovision protocol presented the worst performance in most perspectives of binocular visual quality.12 Thus, patients without bilateral PanOptix IOL implantation were also excluded from our observation.
Interestingly, the mean difference in absolute interocular SE was 0.57±0.27 D in the enrolled patients. In some epidemiologic studies, a healthy adult with an absolute difference in interocular SE of 0.5 D or less could be regarded as having isometropia.13–15 If we use an absolute difference in interocular SE of 0.5 D or greater as the diagnostic criterion, the prevalence of anisometropia would climb to approximately 20%.16 In other words, the proportion of isometropic people in the population is approximately 80%. The percentage of isometropic patients in the present study was only 60% (18/30). Although a difference in interocular SE of 0.5 D could be coordinated by physiologic adaptability, it might aggravate asthenopia symptoms and impel patients to presbyopia correction. In our study, the mean UNVA (LogMAR) in patients with an absolute difference in interocular SE greater than 0.5 D was 0.29±0.16 (12 patients, 24 eyes), and their preoperative spectacle independence was 50% at near. It would be interesting to evaluate the relationship between the level of mild anisometropia and the degree of presbyopic symptoms.
There were limitations of this observational study that should be interpreted. We obtained the present conclusion using some basic indicators, while a series of metric-based measurements would be indispensable for evaluating the visual prognosis comprehensively, including contrast sensitivity, objective scatter index, and modulation transfer function. Subjective scales and questionnaires are also necessary to quantify vision-related quality of life and patient satisfaction after refractive clear lens exchange for presbyopia correction. Although several studies have reported positive results in Caucasians,10,17 we believe that a similar study in a Chinese population would have particular clinical significance. The second limitation is that the relatively small sample size limited the stratification analysis. The visual demand of working-age people with different occupations, lifestyles and hobbies must vary, and this should be noted and compared in future research.
In conclusion, this observational study observed the outcome and safety of bilateral femtosecond laser-assisted clear lens extraction with PanOptix IOL implantation for presbyopia correction in working-age Chinese patients. Satisfactory visual outcomes and safe surgical procedures demonstrate that the present treatment could be a feasible approach for early presbyopic adults in China.
Funding
The study was funded by Scientific Research Project of Shanghai Municipal Health Commission (202040247), Scientific Research Project of Shanghai Xuhui District Municipal Health Commission (SHXH202237), Hunan Province scientific and technological talents lifting project “Xiaohe” special plan (2023TJ-X68), Research Project of Aier Eye Hospital Group (AR2201D3), and a research grant from Alcon (investigator initiated trial).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Wolffsohn JS, Davies LN. Presbyopia: effectiveness of correction strategies. Prog Retin Eye Res. 2019;68:124–143. doi:10.1016/j.preteyeres.2018.09.004
2. Fricke TR, Tahhan N, Resnikoff S, et al. Global prevalence of presbyopia and vision impairment from uncorrected presbyopia: systematic review, meta-analysis, and modelling. Ophthalmology. 2018;125(10):1492–1499. doi:10.1016/j.ophtha.2018.04.013
3. Han X, Ellwein LB, Abdou A, et al. Influence of distance and near visual impairment on self-reported near visual functioning in a Multinational Study. Ophthalmology. 2021;128(2):188–196. doi:10.1016/j.ophtha.2020.07.006
4. Fernandez-Vega L, Alfonso JF, Villacampa T. Clear lens extraction for the correction of high myopia. Ophthalmology. 2003;110(12):2349–2354. doi:10.1016/S0161-6420(03)00794-2
5. Azuara-Blanco A, Burr J, Ramsay C, et al. Effectiveness of early lens extraction for the treatment of primary angle-closure glaucoma (EAGLE): a randomised controlled trial. Lancet. 2016;388(10052):1389–1397. doi:10.1016/S0140-6736(16)30956-4
6. Galvis V, Escaf LC, Escaf LJ, et al. Visual and satisfaction results with implantation of the trifocal Panoptix® intraocular lens in cataract surgery. J Optom. 2022;15(3):219–227. doi:10.1016/j.optom.2021.05.002
7. Scheepers MA, Bunce CB, Michaelides M, Hall B. Clinical outcomes of a trifocal compared with an extended depth of focus IOL following bilateral cataract surgery. Can J Ophthalmol. 2023;58(5):393–400. doi:10.1016/j.jcjo.2022.05.005
8. Fernandez-Garcia JL, Llovet-Rausell A, Ortega-Usobiaga J, et al. Unilateral versus bilateral refractive lens exchange with a trifocal intraocular lens in emmetropic presbyopic patients. Am J Ophthalmol. 2021;223:53–59. doi:10.1016/j.ajo.2020.09.044
9. Fernandez-Garcia JL, Ortega-Usobiaga J, Mayordomo-Cerdá F, et al. Comparison of patients with emmetropia and presbyopia and different accommodation who undergo unilateral or bilateral implantation of a trifocal IOL. J Refract Surg. 2023;39(12):817–824. doi:10.3928/1081597X-20231018-01
10. Yim CK, Dave A, Strawn A, et al. Visual outcomes and patient satisfaction after bilateral refractive lens exchange with a trifocal intraocular lens in patients with presbyopia. Ophthalmol Ther. 2023;12(3):1757–1773. doi:10.1007/s40123-023-00708-x
11. Sahin V, Unal M, Ayaz Y. Outcomes after bilateral implantation of AcrySof IQ PanOptix trifocal intraocular lens: a prospective interventional study. Med Hypothesis Discov Innov Ophthalmol. 2023;12(1):36–45. doi:10.51329/mehdiophthal1468
12. Lan Q, Xu F, Sun T, et al. Comparison of binocular visual quality in six treatment protocols for bilateral cataract surgery with presbyopia correction: a prospective two-center single-blinded cohort study. Ann Med. 2023;55(2):2258894. doi:10.1080/07853890.2023.2258894
13. Li Y, Bao FJ. Interocular symmetry analysis of bilateral eyes. J Med Eng Technol. 2014;38(4):179–187. doi:10.3109/03091902.2014.899401
14. Vincent SJ, Collins MJ, Read SA, et al. The short-term accommodation response to aniso-accommodative stimuli in isometropia. Ophthalmic Physiol Opt. 2015;35(5):552–561. doi:10.1111/opo.12225
15. Yang M, Wang W, Xu Q, Tan S, Wei S. Interocular symmetry of the peripapillary choroidal thickness and retinal nerve fibre layer thickness in healthy adults with isometropia. BMC Ophthalmol. 2016;16(1):182. doi:10.1186/s12886-016-0361-7
16. Barrett BT, Bradley A, Candy TR. The relationship between anisometropia and amblyopia. Prog Retin Eye Res. 2013;36:120–158. doi:10.1016/j.preteyeres.2013.05.001
17. Viljanen A, Koskela K, Koskela H, Tuuminen R, Uusitalo H. One-year results of health-related and vision-related quality of life after clear lens extraction and multifocal intraocular lens implantation. Am J Ophthalmol. 2021;227:240–244. doi:10.1016/j.ajo.2021.03.023
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.