Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Bilateral Adult-Onset Orbital Xanthogranuloma: A Case Report
Authors Chen Y ![]() , Gao A, Tian X
, Gao A, Tian X ![]()
Received 29 August 2023
Accepted for publication 14 November 2023
Published 13 December 2023 Volume 2023:16 Pages 3575—3580
DOI https://doi.org/10.2147/CCID.S437616
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Yue Chen, Aili Gao, Xin Tian
Department of Dermatology, Guangzhou Institute of Dermatology, Guangzhou, People’s Republic of China
Correspondence: Xin Tian, Department of Dermatology, Guangzhou Institute of Dermatology, Guangzhou, Guangdong, People’s Republic of China, Tel/Fax +86-20-83593472, Email [email protected]
Abstract: Adult-onset xanthogranuloma (AOX) is one of the four rare syndromes collectively referred to as adult xanthogranulomatous disease (AXD). It primarily occurs in the orbit and ocular adnexa and displays distinctive histopathological features, characterized by the infiltration of non-Langerhans-derived foam-like histiocytes and Touton giant cells. The presence of diffuse yellow plaques on the eyelids serves as a highly indicative feature. In this report, we present a compelling case of bilateral periorbital AOX. Initially, the patient received a diagnosis of necrotizing xanthogranuloma (NBX) and underwent treatment with dapsone, which yielded a poor response. Subsequently, through repeated biopsy, immunoprotein electrophoresis, and high-throughput sequencing, the diagnosis was revised to AOX. Subsequently, the patient’s treatment was modified to include oral hormone therapy, and no further progression of the periorbital plaque was observed. Notably, the patient’s sister was diagnosed with xanthelasma palpebrarum (XP), suggesting a potential genetic association between AOX and XP. Unfortunately, the sister declined further histologic examination and genetic sequencing of her skin lesions, impeding the acquisition of additional evidence regarding the genetic link between these two disorders. Despite the divergent pathological features, pathogenesis, and clinical presentation of AOX and xanthelasma palbrarum, clinicians should remain cognizant of the plausible genetic correlation between these two conditions and pursue further investigations when feasible.
Keywords: adult-onset xanthogranuloma, adult xanthogranulomatous disease, histopathology, protein electrophoresis
Introduction
Adult orbital xanthogranulomatosis (AOXGD) represents a rare category of non-Langerhans cell histiocytosis, marked by xanthogranulomatous infiltration within periorbital and orbital tissues. AOXGDs are currently categorized in the literature as four distinct syndromes: adult-onset xanthogranuloma (AOX), adult-onset asthma with periocular xanthogranuloma (AAPOX), Erdheim-Chester disease (ECD), and necrotizing xanthogranuloma (NBX). AOXGDs is a relatively rare condition. Based on available case reports worldwide, this disease can affect individuals between the ages of 17 and 85, with no significant difference in incidence observed between genders. The most common subtype is NBX, followed by ECD and AAPOX, while AOX is relatively less common.1 While sharing similar histologic patterns, these disorders vary in terms of their systemic associations and overall prognosis. In this study, we present a case of bilateral periorbital AOX. Initially diagnosed with NBX, the patient was subsequently re-diagnosed with AOX following re-biopsy and protein electrophoresis.
Case Report
A 52-year-old female Chinese patient exhibited a yellowish-brown periorbital hyperplastic mass persisting for over a decade. A decade ago, irregular hyperplastic masses were identified on both sides of the nasal ala. The skin lesions exhibited limited improvement following self-administration of undisclosed medications and laser treatment. Subsequently, the mass slowly expanded and grew, accompanied by persistent burning sensations (Figure 1a and b). The patient, previously diagnosed with NBX at other medical institutions, underwent treatment involving local lesional triamcinolone injection and oral dapsone. However, due to the persistence of signs and symptoms, the patient was subsequently referred to our center. Xanthoma was histologically diagnosed in the periorbital tissue 5 years ago. There was no indication of hyperlipidemia in her medical history, and no family history of asthma or atopy was noted. Furthermore, there were no documented instances of infectious diseases such as tuberculosis or hepatitis. Additionally, there was no evidence of specific contact, trauma, blood transfusion, or significant psychiatric illness. Notably, her sister had xanthelasma palpebrarum (XP). Physical examination revealed a normal general condition, and no evident abnormalities were detected upon examining various systems. Antinuclear antibody (ANA) spectrum indicated positive anti-Jo-1 antibody (3+), with ANA (immunofluorescence assay) at 1:320 in a nucleolar pattern and 1:100 in a granular pattern. Fibrinogen level was 4.37 g/L (normal range: 2–4 g/L), while immunoglobulin A (IgA) was 3.58 g/L (normal range: 0.7–3.5 g/L), and complement C4 measured 0.526 g/L (normal range: 0.16–0.47 g/L). B cell count (CD3-CD19+) stood at 18.66% (normal range: 8–15%). Tuberculosis T cell testing yielded a positive result. Serum lipid levels, immunoglobulin E levels, and protein electrophoresis results were all within normal ranges. Subsequent biopsy of the right periorbital plaque displayed histological findings of mild epidermal hyperplasia, a granulomatous mass containing foam cells and histiocytes within the dermis, as well as concurrent collagen hyperplasia and perivascular lymphocytic infiltration primarily composed of inflammatory cells (Figure 1c and d). No Touton giant cells were identified. Immunohistochemical results indicated positive staining for CD68, while S100 and CD1a were negative (Figure 1e–g).
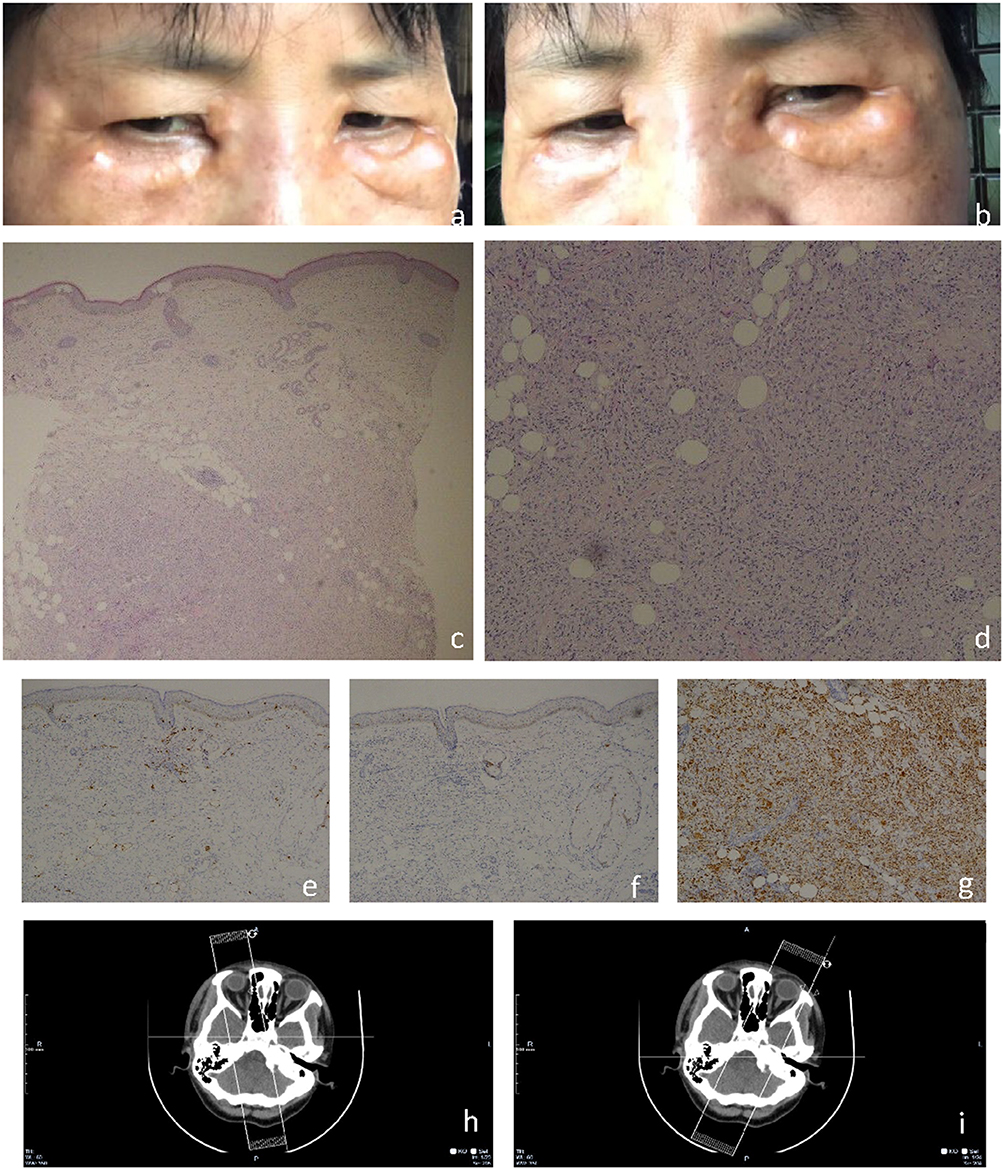 |
Figure 1 Clinical images and relevant examination results obtained during the patient’s initial visit to our hospital. (a and b) Skin examination unveiled infiltrative symmetrical Orange or brown patches with distinct borders on the inner canthi as well as upper and lower eyelids. The surface was smooth, devoid of scales, atrophy, erosion, or necrosis, and exhibited no tenderness. (c) The epidermis displayed mild hyperplasia, while the dermis exhibited a conglomerate of foam cells, histiocytes, and multinucleated giant cells. Additionally, a minor lymphocytic infiltration was observed around the dermal blood vessels and adnexal structures adjacent to the conglomerate (H and E×50). (d) Intense lymphoplasmacytic infiltration was observed (H&E, magnification ×200). (e) Negative result for S100 immunohistochemistry (magnification ×200). (f) Absence of CD1a immunohistochemical staining (magnification ×200). (g) Positive immunohistochemical staining for CD68 (magnification ×200). (h and i) The axial contrast-enhanced orbital CT scan revealed no abnormalities in either eye. Swelling of the subcutaneous soft tissue was noted in the bilateral maxillofacial region and eyelids, with a subtle prominence on the right side. |
Simultaneously, high-throughput sequencing was conducted on the patient’s left periorbital yellow plaque, revealing the absence of pathogenic infections. Over the past decade, neither ulceration nor ocular inflammation had occurred, and no evidence of monoclonal B-cell abnormalities was observed. Based on clinical and histopathological findings, the patient received a diagnosis of AOX. Additionally, prior to the AOX diagnosis, an extended study was conducted to exclude involvement of other sites. Bilateral periorbital B-ultrasonography unveiled nodular or fusiform subcutaneous tissue thickening in the lower, medial, and lateral aspects of the face, as well as the nasal root. Plain CT scans of the eyes indicated no abnormalities. Slight soft tissue swelling was evident on the right side beneath the skin of the bilateral collar and periocular area. Whole-body CT ruled out systemic involvement (Figure 1h and i). The patient declined undergoing local tumor resection; consequently, she was administered a 30 mg oral prednisone treatment. Presently, the patient remains under observation, with no evidence of further skin lesion enlargement.
Discussion
AOX and NBX are categorized within the spectrum of AOXGD. This condition represents a rare type II non-Langerhans histiocytosis, characterized by an unknown etiology and pathogenesis. Characterized by lipid-rich non-Langerhans histiocytosis and the presence of Touton giant cells.2 AOX primarily affects the skin and subcutaneous tissue of the eyes and face. It typically presents with xanthoma-like alterations in the eyelids, often accompanied by periorbital and facial edema. This condition is characterized by its localization and generally lacks involvement of other tissues and organs.3 Conversely, beyond affecting the orbit, NBX can infiltrate various tissues throughout the entire body, including the heart, respiratory tract, spleen, kidney, ovary, liver, skeletal muscle, and central nervous system.4 Typically, the lesions predominantly affect the bilateral eyelids, the anterior segment of the orbit, and the periorbital tissue. In the early stages, the lesions manifest as localized xanthomas. With disease progression, over 40% of patients develop skin ulcers, ranging in size from 0.3 cm² to a maximum of 25 cm².5 The predominant site for skin lesions is periorbital, which can affect either eyelid. Over 80% of patients experience skin lesions in other regions of the face, trunk, or limbs. Approximately 80% of patients experience complicating systemic immune system disorders, including monoclonal paraproteinemia (with a majority being IgG gamma globulin leukemia), hypocomplementemia, and cryoglobulinemia. Certain patients experience complicating malignant hematological conditions, including multiple myeloma, non-Hodgkin’s lymphoma, lymphoplasmacytic lymphoma, and others. On average, the time interval from identifying ocular lesions to the manifestation of hematological complications was 2.4 years.4,6,7
In this particular case, the patient initially received a diagnosis of NBX and exhibited an inadequate response to oral dapsone treatment. Following this, we conducted a repeat biopsy of the right eyelid, combining immunohistochemical and serum fixation electrophoresis techniques. The resultant pathology demonstrated a granulomatous mass comprised of foamy and histiocytic cells within the dermis. Additionally, collagenous hyperplasia and perivascular lymphocytic infiltration with predominantly inflammatory cells were observed. Notably, no Touton giant cells were detected. A few histiocytes and foam cells were noted around the superficial and middle dermal vessels (Figure 1c and d). Immunohistochemical findings demonstrated positive staining for CD68, while S100 and CD1a were negative. Abnormal results were detected in laboratory tests and whole-body CT scans, along with other examinations (Figure 1e–g). Consequently, a diagnosis of AOX was established.
Currently, the disease is believed to result from the reactive proliferation of free tissue macrophages; however, the exact proliferation mechanism remains uncertain.8 Prior case reports propose that AOX might arise as a secondary effect of trauma or autoimmune skin conditions like vitiligo and pemphigus vulgaris.9 These conditions could result from inadequate pathogen clearance due to immune deficiency, resulting in prolonged exposure to foreign antigens. This patient lacked any history of trauma, other skin disorders, or systemic conditions; thus, other underlying diseases should be considered. In this particular case, the patient’s sister presented XP (Figure 2), potentially implying a familial genetic connection to AOX. However, this linkage has not been previously reported. A significant direct correlation between XP and AOX in terms of their pathophysiology or clinical course is lacking. Although both conditions feature the buildup of lipid-filled cells, they stem from distinct root causes and exhibit varying clinical manifestations. Typically categorized as a form of histiocytosis, AOX entails the excessive proliferation of specific immune cells. In contrast, XP is closely linked to lipid metabolism disorders.10 As far as our knowledge extends, no published literature exists concerning AOX and XP. The genetic relationship between XP and AOX remains unclear due to the patient’s sister declining genetic sequencing and blood tests. Due to the infrequent occurrence of AOX, treatment options are primarily based on empirical approaches. Available treatment modalities encompass local or systemic glucocorticoid therapy, surgery, radiotherapy, immunosuppressive agents, interferon-α, and chemotherapy.11 Notably, systemic corticosteroids are often favored by experts. For instance, London et al12 recommended oral prednisone at a dosage of 1 mg per kilogram per day, with gradual reduction to a maintenance dose based on effectiveness, as an efficacious approach for such patients. In the context of AOX and NBX patients, intralesional glucocorticoid injections have been utilized, demonstrating substantial improvements in the eyelid and anterior orbital segment following local administration. A case report exists on the use of external beam radiotherapy for controlling local symptoms in the periocular region of patients with AOX.13 This treatment could be effective in specific circumstances. Additionally, rituximab has demonstrated efficacy for AOX patients with Systemic IgG4-Related Disease.14 AOX distinguishes itself from other subtypes mainly through its localized and self-limited nature. Radical treatment measures are typically unnecessary, and local lesions can be excised through surgery. Currently, there is limited literature available on the recurrence rate of AOX, highlighting the need for additional long-term, large-scale studies. In the present case, considering the patient’s refusal of surgical intervention, we opted for the administration of systemic hormones and implemented regular monitoring.
 |
Figure 2 Clinical picture of the patient’s sister. Soft, yellow plaques were observed at the medial canthus of both the upper and lower eyelids. |
Conclusion
In summary, AOX represents an uncommon variant of non-Langerhans cell histiocytosis. Therefore, it is imperative to conduct a comprehensive patient assessment, encompassing histopathological and immunohistochemical analyses, protein electrophoresis, and the exclusion of potential systemic disease linkages. Furthermore, diligent attention should be given to gathering information about the patient’s familial history of ocular substantive diseases and periocular skin disorders. If warranted, a thorough familial lineage analysis should be undertaken.
Data Sharing Statement
All data used in this work are publicly available.
Ethical Approval
The ethical committee of the hospital gave the agreement to report this case.
Consent Statement
A formal written consent was obtained for publication the case details and associated images from the patient and her sister.
Acknowledgments
We would like to express our gratitude to Dr. Guihua Jiang from the Department of Medical Imaging at Guangdong Second Provincial General Hospital for his valuable imaging support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Science and Technology Program of Guangzhou (Grant No. 2023A03J0468).
Disclosure
The authors declare no conflict of interest.
References
1. Sivak-Callcott JA, Rootman J, Rasmussen SL, et al. Adult xanthogranulomatous disease of the orbit and ocular adnexa: new immunohistochemical findings and clinical review. Br J Ophthalmol. 2006;90(5):602–608. doi:10.1136/bjo.2005.085894
2. Burris CK, Rodriguez ME, Raven ML, Burkat CN, Albert DM. Adult-onset asthma and periocular xanthogranulomas associated with systemic IgG4-related disease. Am J Ophthalmol Case Rep. 2016;1:34–37. doi:10.1016/j.ajoc.2016.03.006
3. Vick VL, Wilson MW, Fleming JC, Haik BG. Orbital and eyelid manifestations of xanthogranulomatous diseases. Orbit. 2006;25(3):221–225. doi:10.1080/01676830600666201
4. Nelson CA, Zhong CS, Hashemi DA, et al. A multicenter cross-sectional study and systematic review of necrobiotic xanthogranuloma with proposed diagnostic criteria. JAMA Dermatol. 2020;156(3):270–279. doi:10.1001/jamadermatol.2019.4221
5. Geoloaica LG, Pătraşcu V, Ciurea RN. Necrobiotic xanthogranuloma - case report and literature review. Curr Health Sci J. 2021;47(1):126–131. doi:10.12865/CHSJ.47.01.21
6. Szalat R, Arnulf B, Karlin L, et al. Pathogenesis and treatment of xanthomatosis associated with monoclonal gammopathy. Blood. 2011;118(14):3777–3784. doi:10.1182/blood-2011-05-356907
7. Mehregan DA, Winkelmann RK. Necrobiotic xanthogranuloma. Arch Dermatol. 1992;128(1):94–100. doi:10.1001/archderm.1992.01680110104016
8. Chen PK, Chen DY. An update on the pathogenic role of macrophages in adult-onset still’s disease and its implication in clinical manifestations and novel therapeutics. J Immunol Res. 2021;2021:8998358. doi:10.1155/2021/8998358
9. Salem I, Hodson EL, Davis MJ, et al. Multiple adult-onset xanthogranulomas associated with skin dysbiosis: a presenting sign of common variable immune deficiency, supported by next-generation sequencing. JAAD Case Rep. 2023;36:4–7. doi:10.1016/j.jdcr.2023.03.009
10. Nair PA, Singhal R. Xanthelasma palpebrarum - a brief review. Clin Cosmet Investig Dermatol. 2018;11:1–5. doi:10.2147/CCID.S130116
11. Guo J, Wang J. Adult orbital xanthogranulomatous disease: review of the literature. Arch Pathol Lab Med. 2009;133(12):1994–1997. doi:10.5858/133.12.1994
12. London J, Soussan M, Gille T, et al. Adult-onset asthma associated with periocular xanthogranuloma: new diagnostic and therapeutic approaches in a very rare systemic disease. Ophthalmic Plast Reconstr Surg. 2013;29(2):104–108. doi:10.1097/IOP.0b013e31827ae96a
13. Chicas SR, Pons LO, Celada ÁF, et al. A case report of recurrent adult-onset xanthogranuloma: is the radiotherapy a treatment option? Int Cancer Conf J. 2016;5(2):77–81. doi:10.1007/s13691-015-0232-8
14. Barke MR, Vempuluru VS, Lally SE, Shields CL. Truxima (rituximab-abbs) for periocular xanthogranuloma with adult-onset asthma and systemic IgG4-related disease. Ophthalmic Plast Reconstr Surg. 2023;39(5):e158–e160. doi:10.1097/IOP.0000000000002412
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.