Back to Journals » Integrated Pharmacy Research and Practice » Volume 4
Big data in pharmacy practice: current use, challenges, and the future
Authors Ma C, Smith H, Chu C, Juarez D ![]()
Received 18 April 2015
Accepted for publication 3 June 2015
Published 6 August 2015 Volume 2015:4 Pages 91—99
DOI https://doi.org/10.2147/IPRP.S55862
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Jonathan Ling
Carolyn Ma, Helen Wong Smith, Cherie Chu, Deborah T Juarez
Department of Pharmacy Practice, The Daniel K Inouye College of Pharmacy, University of Hawai'i at Hilo, Hilo, HI, USA
Abstract: Pharmacy informatics is defined as the use and integration of data, information, knowledge, technology, and automation in the medication-use process for the purpose of improving health outcomes. The term “big data” has been coined and is often defined in three V's: volume, velocity, and variety. This paper describes three major areas in which pharmacy utilizes big data, including: 1) informed decision making (clinical pathways and clinical practice guidelines); 2) improved care delivery in health care settings such as hospitals and community pharmacy practice settings; and 3) quality performance measurement for the Centers for Medicare and Medicaid and medication management activities such as tracking medication adherence and medication reconciliation.
Keywords: clinical pharmacy data base, pharmacy informatics, patient outcomes
Corrigendum for this paper has been published
Introduction
Medicine informatics is defined as the “field of information science concerned with the analysis, use and dissemination of medical data and information through the application of computers to various aspects of health care and medicine”.1
In 2007, the American Society of Health System Pharmacists (ASHP) released a position paper that describes the pharmacist’s role in informatics and defined this subspecialty area of pharmacy practice as the use and integration of data, information, knowledge, technology, and automation in the medication-use process for the purpose of improving health outcomes.2 The term “big data” has been coined and is defined as the emerging use of rapidly collected, complex data.3 Big data is a term often defined in three V’s: volume, velocity, and variety. Other dimensions may also include variability and complexity.4 A paper released by the Center for US Health System Reform describes the revolution of big data in health care and cites four major sources of big data that include:
- Pharmaceutical research and development from pharmaceutical companies and academia, clinical trials, and high-throughput screening libraries
- Claims and cost data from payers and providers that contain utilization of care and cost estimates
- Clinical data provided by the electronic medical record (EMR) that contain patient-specific data on treatment outcomes
- Patient behavior and sentiment data that come from consumers and stakeholders outside of health care (for instance, from retail exercise apparel and exercise monitoring equipment).4
The Center for US Health System Reform paper also defines five new value pathways through a patient-centered framework that balances health care cost and patient impact or outcomes, and describes how big data can affect these five pathways:5 1) right living; 2) right care; 3) right provider; 4) right value; and 5) right innovation.
Health information technology leverages big data to capture disparate streams of information and merges them into actionable information. Pharmacy is poised to leverage data to help with patient medication safety, improve outcomes, and lower costs.
What are the driving forces to share and utilize all these data? Most likely, fiscal concerns with rising health care expenses that now represent 17.6% of the gross domestic product is the most pressing driving force behind sharing data.4 Attempts to decrease costs have moved payers from fee-for-service compensation to risk-sharing arrangements where treatments need to deliver desired results or “value pathways” for payment. Physicians have been forced to move to more evidence-based medicine that involves the systematic review of clinical data and treatment decisions on algorithms and best practice guidelines. Technology now allows for easier collection and analysis of information. Researchers can mine data to evaluate the most effective treatments for particular conditions, identify patterns of drug side effects, and identify patterns of hospital readmissions. Payers are entering into risk-sharing agreements with pharmaceutical companies and are reimbursing for drugs that produce measureable improvements in patient health.
The current review paper will review the various ways that pharmacy has been utilizing big data. Table 1 lists three major areas, including informed decision making, improved care delivery in health care settings such as hospitals and community pharmacies, and quality performance measurement.
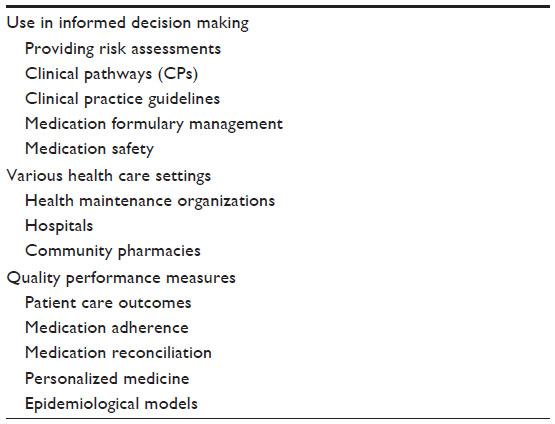 | Table 1 Synopsis of big data used in pharmacies |
Informed decision making
Critical pathways
Critical pathways (CPs) differ from evidence-based clinical practice guidelines in that CPs include elements meant to track compliance, patient outcomes, or continuous quality improvements. CPs focus on targeting the clinical management of patient groups instead of addressing decisions for patient care management.6 Originally, CPs were designed to control health care costs without sacrificing quality of care by targeting high-volume, high-cost, and/or high-risk diagnoses or procedures across health care systems. Pharmacists have long been involved in the development of CPs.7
One of the critical steps in developing a CP is to define the desired clinical outcomes. This is done by examining current practice habits via literature review and by benchmarking. Large variations in outcomes can occur in length of stay, average costs, departmental costs, and in timing of interventions and utilization of resources. For some CPs, the use of pharmacy resources and the drug itself are major components of a pathway. Pharmacists can utilize big data to build the most rational and cost-effective drug therapy into the standard of practice and to justify their recommendations with data and cost analyses.7
In a 2013 study, Bereznik et al used data mining to develop a CP aimed at streamlining community pharmacy asthma interventions. They were able to utilize pharmacy dispensing records to identify asthma patients with sub-optimal control and then compare the uptake and effectiveness of streamlined pharmacists’ interventions. The development of this CP helped to successfully integrate streamlined pharmacy asthma interventions into the “real-life” workflow of a community pharmacy. The use of dispensing records allowed for an objective measure of medication use, making the intervention relatively easy to implement without disrupting workflow.8
Evaluation of implemented CPs should also include analyses of variance. Variance in pharmacy data could also include differences in drug acquisition costs or even availability of drugs for a CP.7
In evaluating a CP, pharmacists need to utilize data involving allergies, drug dosing, safety and efficacy, therapeutic uses, monitoring parameters, patient demographics, and adverse effects. Pharmacists must also review current policies, procedures, and protocols to ensure that best practices are maintained for all drugs, including drugs used in ancillary settings such as in diagnostic or surgical procedures.7
Monitoring a CP requires pharmacists to provide pharmacotherapy consultation services. Other pathways aimed at patient satisfaction and process improvement may involve pharmacist-driven services such as antimicrobial stewardship, pain management, discharge drug counseling, medication reconciliation, and transitional care. Development of these types of services can generate cost savings and overall improvement in quality of care. Prospective drug use evaluations can be designed from outcome data derived from these types of services.8
Evans et al utilized computer-based systems in a study to improve detection of nosocomial infections. The study involved identifying patients who were not receiving appropriate antibiotics, those who were candidates for less expensive antibiotics, and those who were receiving prophylactic antibiotics for an excessive duration. Examined data from over 4,500 patients during a 2-month period and computerized alerts were generated to address the potential gaps in care and cost savings. This automated alert system efficiently detected 90% of nosocomial infections, compared with 76% detected by manual surveillance. The authors were also able to identify 37 patients who were not receiving appropriate antibiotics, 31 who could have received less expensive antibiotics, and 142 patients who received longer-than-needed duration of antibiotic prophylaxis.9
Clinical practice guidelines
Clinical practice guidelines differ from CPs in that the former are intended to define appropriate care for a specific indication. The Cochrane Library provides numerous systematic reviews based upon clinical trial data and suggestions for clinical practice guidelines.10
An example of changes made in guideline recommendations due to big data is evident in the recently updated 2012 Surviving Sepsis Guidelines, with respect to choice of a vasopressor. The previous 2008 guideline was unable to provide high-quality primary evidence to recommend the use of one vasopressor over another for the treatment of sepsis. Norepinephrine and dopamine were merely recommended due to observational data that hypothesized potential benefits of their use in patients with sepsis. With the newly updated 2012 guidelines, big data were extracted from five different randomized controlled trials comparing use of norepinephrine to dopamine (n=1,993 patients). Analysis of pooled data resulted in significant decreases in relative risk of short-term mortality (95% confidence interval [CI], 0.84–0.99), supraventricular arrhythmias (95% CI, 0.38–0.58), and ventricular arrhythmias (95% CI, 0.19–0.66) in favor of norepinephrine. Results from pooled analysis supported the designation of a higher quality recommendation in the guidelines to support the use of norepinephrine over the routine use of dopamine in the management of septic shock.11,12
Pharmacist clinicians utilize guideline recommendations to stratify risk–benefits of safety and efficacy for individual patients. With recent advances in the field of informatics, big data are becoming more commonly integrated into the development of clinical guidelines. As big data outputs increase in value and diversity, pharmacists will see increases in utilization over meta-analysis and randomized controlled trials.
In this era, standards mandate that medical specialty practices utilize best practice guidelines. Specialty cooperative groups in oncology have pooled research data in order to provide sufficient power and quantity of patients to develop best practice guidelines. Examples of such combined group data include the ECOG (Eastern Cooperative Oncology Group) and SWOG (Southwest Oncology Group). From pooled data, specialty organizations such as the National Cancer Comprehensive Network (NCCN) create guidelines for supportive care management for the plethora of chemotherapy side effects. Specific examples include control of chemotherapy-induced nausea and vomiting and control of cancer pain.13
Improved care delivery in various health care settings Health maintenance organizations and hospitals
Health maintenance organizations began in the 1920s and are organizations that provide care with contracted physicians and facilities in a group plan with prepaid insurance.14 Kaiser Foundation Health Plan in the state of California, USA, is regarded as an innovator of this type of health care model.15 Kaiser uses the Health Connect system to ensure timely and complete information exchange across all medical facilities and to incorporate details of patient care into their EMRs. Other hospitals, private or community, have also utilized the types of information systems to help improve areas that would affect admissions or readmissions such as with prescription refills.
Medication formulary management and medication safety
Hospitals have long had formulary management from their pharmacy and therapeutics committees to try to curtail costs and promote effective and safe drug utilization. Depending upon the size of the health system, big data can be utilized to decide on multi-institution medication formulary management. Data entered in multi-institution systems that deal with adverse drug events (ADEs), high alert medications, and other safety issues have spurred the creations of the National Patient Safety Goals from the US Joint Commission for Accreditation of Healthcare Organizations (JCAHO).16
Community pharmacy
With the help of technology in the grocery and retail industry, community pharmacies, especially chain retail stores, have a distinct advantage in the volume of actionable data. As one of the largest US national retail chains, CVS Pharmacy reports utilizing 2 years’ worth of data in an effort to investigate inappropriate prescribing for controlled substances.17 The goal of the program was to identify and take action against prescribers who exhibited extreme patterns of use of “high-risk drugs” by benchmarking them against others in the same geographic region in a specific specialty. Parameters included not just the volume of high-risk drug prescriptions but also the volume of these types of prescriptions in proportion to the prescribers other prescriptions. Thresholds were set for both volume (98th percentile) and for proportion (95th percentile). Additional parameters included those patients who paid cash for high-risk prescriptions and those patients who were 18–35 years of age. The last comparison for the prescriber included the number of non-controlled substances with controlled substances. Out of a database of 1 million prescribers, CVS contacted the 42 identified outliers and either interviewed in person or phoned these prescribers to understand their rationale for their high-prescribing pattern for controlled substances. Of these, 10 prescribers did not offer valid explanation or try to curb their prescribing, and CVS elected to not fill controlled substances prescriptions from these prescribers. Analyses of this type of community data can help curb unwanted prescribing patterns and can also support the pharmacist on the frontline.
Other uses of health information technology include use of data in the field of immunizations. Activities would include utilizing the infrastructure to deliver immunizations data for state, regional, or national registries. This information helps to coordinate patient care for documentation, reimbursement, and quality reporting.18
Community pharmacies are fast becoming centers for health screenings and maintenance. US retail chains such as Walgreens, Rite Aid, and CVS offer Health Care Clinics, Rediclinics, and One-minute clinics, respectively, as options for urgent care. Data related to treatment for influenza, birth control, and other diseases, and screenings for hepatitis, HIV, and other types of viruses may now be trackable through these types of ambulatory care clinics.19–21
Measuring quality of care and patient outcomes
Big data can be leveraged by the US federal government through the US Center for Medicare and Medicaid Services (CMS), as well as private payers, nonprofit organizations, research centers, and health care delivery systems to measure, benchmark, and improve the quality of care and patient outcomes. The Pharmacy Quality Alliance (PQA), started in 2006, is a US nonprofit membership organization that promotes appropriate medication use and helps its 165 organizations that include community pharmacies, health planners, government agencies, pharmaceutical manufacturers, and academic institutions to develop strategic plans for measuring and reporting performance information related to medications.22 By consensus, PQA develops consensus-based measures that are used internally or in public reporting programs. One such program is the CMS Star Rating System that involves Medicare Part C and D health plans to ensure quality patient care. For 2015, approximately 50% of the 13 quality metrics (5/13) are directly related to medication use. PQS has developed the Electronic Quality Improvement Platform for Plans and Pharmacies (EQuiPP) platform, a performance information management platform used by more than 55,000 pharmacies. Big data from this platform provide health plans and community pharmacies with unbiased, benchmarked performance information including medication adherence metrics. Pharmacists can track patients’ adherence to certain medications for diabetes, antihypertensive agents, and cholesterol management with statins.22
CMS rates Part D prescription drug plans using a one to five star rating. Quality performance metrics play an immense role (50%) in achieving higher Part D star ratings in stand-alone prescription programs and also for Medicare Part C (ie, Medicare Advantage programs). The quality measures include medication adherence of greater than 80%, statin use in persons with diabetes, use of high-risk medications in the elderly, drug–drug interactions, completion rates for comprehensive medication review, and percentage of children 5 years or younger who are using antipsychotic medications.22
Accountable care organizations are groups of physicians, hospitals, and providers who voluntarily work together to care for patients with the express goal of delivering high-quality care while wisely spending dollars. Thus, value-based payment occurs as opposed to payment based on patient volumes.23
PQA measures are also being used for community and specialty pharmacy accreditation that have been developed by the Center for Pharmacy Practice Accreditation (CPPA), a partnership formed between the American Pharmacists Association (APhA), the National Association of Boards of Pharmacy (NABP), and the American Society of Health-System Pharmacists (ASHP). CPPA helps to manage the process of utilizing consensus-based standards to pharmacy practice accreditation.22,24 Preferred pharmacy networks, health plans, and pharmacy benefit managers are implementing models that include bonus payments to top-performing pharmacies. A private US company, Pharmacy Quality Solutions that is owned by PQA, uses big data to track performance and awards bonuses based upon performance on four-star measures and the quantity of patients seen in each store. Pharmacy benefit managers will use quality ratings to form their preferred pharmacy networks. Pharmacies can view a dashboard on how they are performing over time.25
Medication adherence
Big data can also be used to promote medication adherence. Through its PBM, CVS tracks prescription filling patterns, especially for chronic conditions.26 By contacting customers through texts, emails, and phone calls, an automatic fill program helps to initiate refills. Alerts are added to customer accounts when a prescription is left unfilled; even if the customer comes into the pharmacy for a different medication, they still receive the alert.
An integrated delivery system in the northern California area in the USA used an online patient portal to try to improve medication adherence.27 Large datasets were used to generate the underlying data for the portal. The researchers categorized 8,705 patients with diabetes as using the online portal exclusively or occasionally to obtain medication refills. They found that non-adherence declined by 6% among exclusive users.27
Medication reconciliation
The American Recovery and Reinvestment Act (ARRA) of 2009 provided $20 billion USD in incentives to promote the “meaningful use” of technology such as the electronic health record and computerized provider order entry (CPOE) among health care practitioners. Although health care professionals’ uptake of these tools has been slow, data show a decrease in ADEs,22,23 enhanced patient safety, and improved vaccination rates resulting from electronic health records and CPOE.28 These tools make information that lay previously buried in paper charts much more accessible, thus allowing for the creation of big datasets that can be used by pharmacists and others to improve the quality of care.
Medication reconciliation is the process of comparing a patient’s medication orders in hospitals or other type of health care setting to all of the medications that the patient has been taking. This reconciliation is done to avoid medication errors such as omissions, duplications, dosing errors, or drug interactions. Confusion over medication regimens is a major cause of ADEs in the hospital and post-discharge.29–34 Recognizing this problem, the JCAHO mandated that by 2006, hospitals would develop of a process to “accurately and completely reconcile medications across the continuum of care”.35 Pharmacists and other health care professionals can leverage big data to reduce incomplete medication histories and to facilitate medication reconciliation.35
An integrated delivery network in the US city of Boston, Massachusetts, has leveraged its outpatient EMRs and inpatient CPOE systems to generate an accurate pre-admission medication list (PAML) to facilitate medication reconciliation.36 An application created to combine EMR and CPOE datasets “supports the writing of admission and discharge orders by physicians, performance of admission assessment by nurses, and reconciliation of inpatient orders by pharmacists”.36 Initial findings from a pilot study of the application show that the support provided for the combined inpatient and outpatient areas meets the informational needs of providers and may reduce adverse events due to medication discrepancies.
Another study that looked at medication reconciliation describes an approach called controlled terminology technology to automatically analyze medication information from a mixture of coded and narrative text sources (admission notes, clinic notes, medication orders, discharge orders/plans, etc). This new method was also used to summarize drugs by medication class and in chronological order. This new technology potentially provides a new way to summarize patient drug information to support automated medication reconciliation.37
Another study was conducted at two large academic medical centers in the US city of Boston, Massachusetts.38 The intervention included introduction of an information technology application designed to facilitate medication reconciliation that is integrated into the hospital CPOE. As part of the redesigned medication reconciliation workflow, pharmacists reviewed the PAML, planned actions on admission and admission orders, confirmed reconciliation, identified important discrepancies, and notified admitting physicians during admission. During the remainder of the hospitalization, pharmacists gathered additional sources of PAML information, helped resolve uncertainties or discrepancies in PAML, and notified the responsible physician. Results demonstrated that the computerized medication reconciliation tool, based on big data, along with process redesign, was associated with a decrease in unintentional medication discrepancies.33
The US Hawaii Health Information Exchange (HHIE) is a 501 (C) (3) nonprofit, state-wide organization established in 2006. By facilitating assessment and implementing targeted health initiatives, HHIE strives to enhance care coordination, to improve the health outcomes of Hawai‘i’s patients, and to reduce the cost of care for both patients and health care providers.39
A project called Pharm2Pharm, funded for $14.3 million USD by an innovation grant from CMS, uses information provided by HHIE to facilitate all written communication between hospitals and outpatient health care teams.40 HCS Med 360 is a software solution now also being used to support medication reconciliation. This technology allows a pharmacist to query over a dozen national databases (including Surescripts®) and to see the patient’s prescription fill history as well as gaps in the fill history. HCS Med 360 captures all prescription medications in Hawai‘i except for prescriptions filled at health maintenance organizations such as Kaiser Permanente, prescriptions filled at the US Department of Veteran Affairs clinics, and those prescriptions paid in cash. Pharmacists then complete a medication reconciliation process and produce a current medications list, including over-the-counter medications, herbals, and supplements. Thus, the patient’s prescription fill history and complete medication list are built and included in the patient’s HHIE Community Health Record, a tool that pharmacists can use to access patient lab values and other clinical information. This complete record of medications, labs, and other clinical information can then be utilized to support additional health care strategies specifically designed for each patient.39,40
Personalized medicine
For chemotherapy, in many cases, the regimen associated with a specific protocol does not exist commercially, so it must be produced specifically by the hospital’s central pharmacy.41 A group of hospitals in Switzerland is using big data to support computerized production protocols that can be adapted for a number of factors including patient-specific data to mass production variables. The system includes information on all lots, production and expiration dates, suppliers, end users, remaining stocks, and the position of the product in the production workflow, and ensures standards in the production chain. Before the chemotherapy is administrated, complete instructions specific to the formulation and patient are printed in the ward for nurses, including information about drugs, sides effects and their prevention (such as nausea), and precautions for drug administration itself.41
In a recent article, Panahiazar et al emphasize the need to be able to process vast volumes of structured and unstructured data about individual patients.42 For their project, they combined data on lab results, medications, and patient demographics from four large datasets (three electronic health records databases from different clinical systems and one heart failure clinical trial database) to produce a dataset with over 150 million patient records. This dataset is used to predict survival scores of heart failure patients.
Epidemiological models
Schwartz et al examined the feasibility of using big data to address the problem of antimicrobial resistance.43 According to the authors, the increasingly computerized process of health care delivery has made possible the automated acquisition of antimicrobial utilization data. Hospitals generally have computerized laboratory, pharmacy, admission-discharge-transfer, and patient demographic and financial data. A comparison of these computerized datasets to a gold standard based on manual chart review found discrepancies ranging from <1% to almost 18%. Thus, while it is feasible to use computerized datasets to track antimicrobial resistance, threats to validity must be examined and addressed.
Accurately monitoring influenza infection levels and predicting which regions have higher infection risk in future time periods can instruct targeted prevention and treatment efforts by pharmacists and other health care professionals. Developed by Google, Google Flu Trends (GFT) uses aggregated search query data to estimate influenza activity in the regions of the USA.44 Researchers combined GFT and US Centers for Disease Control and Prevention (CDC) data in a model that recalibrates to produce better estimates of actual cases of the flu using methods borrowed from social network analysis.45,46 With these types of applications, big data can be an effective tool for estimating disease burden and spread. These authors found that their improved model predicts infections 1 week into the future as well as GFT predicts the present, and that their model does particularly well 1) in regions that are most likely to facilitate influenza spread; and 2) during epidemics. Hence, with data generated by these applications, pharmacists in high-risk areas could upscale education and vaccination efforts. These efforts could extend beyond flu vaccination to other epidemics or even chronic disease management.
In British Columbia, Canada, a large database, PharmaNet, has been developed that contains records for all ambulatory care prescriptions in the province.47 Data include the date of dispensing, drug name and dose, duration of treatment, age, sex of the patient, and geographic location of the pharmacy. Reliability and validity testing show underreporting and misclassification of drug prescribing is minimal.48 One study used this database to track annual rates of antibiotic prescribing by examining all antibiotics for systemic use and for the six major classes of antibiotics including tetracyclines, penicillins, cephalosporins, sulphonamides and trimethoprim, macrolides, lincosamides and streptogramins, and quinolones.43 Results showed that while overall antibiotic use declined in children from 1996 to 2003, increased use of macrolides increased, which may have ramifications on macrolide-resistant streptococci, including Streptococcus pneumoniae and group A streptococci. Using big data in this manner can assist pharmacists in educating patients and other health professionals regarding issues in antibiotic use. This dataset and ones like it in other provinces have also been used to assess medication adherence.43
Challenges for big data
The three V’s of big data, volume, velocity and variety, all pose challenges in terms of technology, data validity, and privacy.
Technology
The sheer volume of data poses technological challenges not only for storage on the size scale of petabytes but for secure data transmission and continued development of tools to analyze the data. According to Drenik in a recent Forbes article, “Knowing not only what happened, but why it happened (diagnostic), what will happen (predictive) and how we can make it happen (prescriptive) is important for moving beyond big data to knowledge”.49 This advancement can only be accomplished if we are able to develop new analytic tools that incorporate logic and experience of users.
The issue of velocity is not just about the rate of accumulation of volume, but the timeliness in which analytics are performed in relation to real-time need. Physicians and health care workers need to make quick decisions. Analytics can be slow, posing a challenge to figure out how to take the volume and variety of data we have, and utilize the real-time need for data to improve both the quality of health care while also ensuring good value for the expenditures.50
Data validity
Data of all types are becoming increasingly available, and this availability leads to the second challenge of variety and the issue of data integrity – many sources and users. Consumers/patients may be entering data not just into their medical records, but data may also be entered from consumer health/fitness activity trackers such as FitBit®.51 It would be an enormous challenge to try to ensure the validity of each data element in an extremely large dataset; however, there should at least be documentation as to the source of data and possible validity issues.
Patient confidentiality
Big data also raises issues regarding how to keep the information safe. Of great concern is patient confidentiality. One issue with big data is that big data often require patient-identifiable information to link different data sources. Hence, strict protocols must outline processes to remove personal identifiers prior to data release. Even with the protections provided through the Health Insurance Portability and Accountability Act (HIPAA), there is still the risk of re-identification, particularly if datasets are merged with other information. Risk may be reduced by aggregating small samples as required through the Safe Harbor and Limited Dataset provisions of the HIPAA and by carefully considering what data are available through other public use datasets prior to releasing health care data. Privacy can also be safeguarded through authorized and secure access of medical servers and by accountable data transmission.52
The goal is to minimize these risks to confidentiality while making patients aware of them. Even when the entities housing the data are following appropriate protocols to maintain confidentiality, we know that databases and websites can be hacked and that confidential information can be revealed, even when safeguards are in place. Given these risks, should patients be given the option to have their medical information excluded from big datasets?
Physician prescribing patterns
In the suit of William H Sorrell, Attorney General of Vermont, et al, Petitioners vs IMS Health Inc., et al, the issue at hand was whether detailed information about prescriptions written by doctors, with the doctor identified, can be bought and sold.53 This practice still remains legal in some states. Data mining companies extract information from retail pharmacies about patients, drugs, prescriptions, prescribers, etc. Further processing occurs with each physician’s prescribing history for each patient, and then this information is sold to pharmaceutical companies. Prescribing information on each doctor can then be linked to the Physician Masterfile of the American Medical Association (AMA). The Physician Masterfile, which is sold by the AMA, includes information on every physician’s education, licensure, certification, hospital privileges, and practice details. Drug company marketing departments, in turn, use the information to develop strategies to sell drugs to individual doctors. In the end, the retail pharmacies, the Pharmaceutical Research and Manufacturers of America (PhARMA), and the AMA continue to make money while costs are passed on to patients and physicians’ prescribing practices are manipulated by drug salespeople. In response to the lawsuit mentioned earlier in this section, some states have developed prescription confidentiality laws, but these laws have been criticized as going against the First Amendment right of a business to communicate about its products (“commercial speech”).52 In another twist to this issue, CMS has recently released detailed physician prescribing information for millions of Medicare Part D enrollees free to the public, rendering these state-level restrictions somewhat meaningless. However, the question of how much identifiable provider information should be made available remains a valid one.
Conclusion
Certainly, the era of big data is here to stay, and both commercial organizations and consumers are utilizing the information for a wide range of purposes ranging from designing clinical pathways and clinical practice guidelines to institutional settings and community pharmacies. In comparison, to retailers such as grocery chains, pharmacy is just beginning to touch upon the iceberg of information available and how the pharmaceutical side of health care may benefit from accessing data about patient care, costs, and reimbursements. A multitude of other areas warrant further exploration on how big data can be utilized by pharmacists. The possibilities are endless, but the challenges need to be addressed in a comprehensive fashion through protocols and policy initiatives.
Disclosure
The authors report no conflicts of interest in this work.
References
National Library of Medicine. Collection development manual: medical informatics. Available from: http://www.nlm.nih.gov/tsd/acquisitions/cdm/CDMBook.pdf. Accessed on June 5, 2015. | |
Proceedings of the Pharmacy Practice Model Summit: An invitational consensus conference conducted by ASHP and the ASHP Research and Education Foundation, November 7–9, 2010, Dallas, Texas. Available from http://www.ashp.org/DocLibrary/PPMI/PPMI-Summit-Proceedings.aspx | |
Erickson AK, editor, Pharmacy Today. Pharmacy: Harnessing the power of big data. American Pharmacists Association. http://www.pharmacist.com/pharmacy. Accessed March 20, 2015. | |
Groves P, Kayyali B, Knott D, Van Kuiken S. The “big data” revolution in healthcare: accelerating value and innovation. New York, NY: Center for US Health System Reform, Business Technology Office, McKinsey and Company; 2013. | |
Kirk JK, Michael KA, Markowsky SJ, Restino MR, Zarowitz BJ. Critical pathways: the time is here for pharmacist involvement. American College of Clinical Pharmacy. Pharmacotherapy. 1996;16(4):723–733. | |
Dobesh PP, Bosso J, Wortman S, et al. Critical pathways: the role of pharmacy today and tomorrow. Pharmacotherapy. 2006;26(9):1358–1368. | |
McCaffrey S, Nightingale CH. How to develop critical paths and prepare for other formulary management changes. Hosp Formul. 1994;29:628–635. | |
Bereznicki BJ, Peterson G, Jackson S, et al. Uptake and effectiveness of a community pharmacy intervention programme to improve asthma management. J Clin Pharm Ther. 2013;38(3):212–218. | |
Evans RS, Larsen RA, Burke JP, et al. Computer surveillance of hospital-acquired infections and antibiotic use. JAMA. 1986; 256(8):1007–1011. | |
The Cochrane Library, 2995-2015. Chichester: Wiley. http://www.cochranelibrary.com/. Accessed April 1, 2015. | |
Dellinger RP, Levy MM, Carlet JM, et al. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008. Crit Care Med. 2008;36(1):296–327. | |
Dellinger RP, Levy MM, Rhodes A, et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41(2):580–637. | |
Guidelines, National Comprehensive Cancer Network, 2014. Available from: http://www.nccn.org/professionals/physician_gls/f_guidelines.asp. Accessed April 11, 2015. | |
Health Maintenance Organizations. Dictionary of American History. Encyclopedia.com. http://www.encyclopedia.com/topic/health_maintenance_organization.aspx. Published 2003. Accessed July 6, 2015. | |
History of the Kaiser Permanente Medical Care Program. Kaiser Permanente Thrive Exposed. Available from: http://www.kaiserthrive.org/kaiser-permanente-history/. Accessed July 6, 2015. | |
The Joint Commission. National Patient Safety Goals. Available from: http://www.jointcommission.org/standards_information/npsgs.aspx. Accessed March 25, 2015. | |
Betses M, Brennan T. Abusive prescribing of controlled substances–a pharmacy view. N Engl J Med. 2013;369(11):989–991. | |
Hull J, Schueth AJ, Hein W. Health information technology: facilitating an evolution in health care. Specialty Pharmacy Times, February 18, 2014. Available from: www.specialtypharmacytimes.com/publications/specialty-pharmacy-times/2014/february-2014/Health-Information-Technology-Facilitating-an-Evolution-in-Health-Care. Accessed April 10, 2015. | |
Healthcare clinic. Walgreens. Available from: http://www.walgreens.com/topic/pharmacy/healthcare-clinic.jsp. Accessed July 6, 2015. | |
Rite Aid Corporation. Rite Aid Acquires RediClinic, One of the Nation’s Leading Operators of Retail Clinics. Available from: http://www.rediclinic.com/rite-aid-acquires-rediclinic-one-of-the-nations-leading-operators-of-retail-clinics/. Published April 2014. Accessed July 6, 2015. | |
MinuteClinic. Available from: http://www.cvs.com/minuteclinic/services. Accessed July 6, 2015. | |
Scarlatos M, Warholak T, Arya V, Stolpe S. Innovation in pharmacy quality. Pharmacy Today. 2015 March:49. | |
Accountable Care Organizations. Center for Medicare and Medicaid Services. Available from: https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/ACO/index.html. Accessed April 10, 2015. | |
Center for Pharmacy Practice Accreditation. Available from: http://pharmacypracticeaccredit.org/. Accessed April 1, 2015. | |
Clifford S. Using Data to Stage-Manage Paths to the Prescription Counter. NYT. JUNE 19, 2013. Available from: http://bits.blogs.nytimes.com/2013/06/19/using-data-to-stage-manage-paths-to-the-prescription-counter/?_r=2. Accessed February 24, 2015. | |
Sarkar U, Lyles CR, Parker MM, et al. Use of the refill function through an online patient portal is associated with improved adherence to statins in an integrated health system. Med Care. 2014;52(3):194–201. | |
Nebeker JR, Hoffman JM, Weir CR, Bennett CL, Hurdle JF. High rates of adverse drug events in a highly computerized hospital. Arch Intern Med. 2005;165(10):1111–1116. | |
Ammenwerth E, Schnell-Inderst P, Machan C, Siebert U. The effect of electronic prescribing on medication errors and adverse drug events: a systematic review. J Am Med Inform Assoc. 2008;15(5):585–600. | |
Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161–167. | |
LaPointe NM, Jollis JG. Medication errors in hospitalized cardiovascular patients. Arch Intern Med. 2003;163(12):1461–1466. | |
Rozich JD, Howard RJ, Justeson JM, Macken PD, Lindsay ME, Resar RK. Standardization as a mechanism to improve safety in health care. Jt Comm J Qual Saf. 2004;30(1):5–14. | |
Lau HS, Florax C, Porsius AJ, De Boer A. The completeness of medication histories in hospital medical records of patients admitted to general internal medicine wards. Br J Clin Pharmacol. 2000;49(6):597–603. | |
Tam VC, Knowles SR, Cornish PL, Fine N, Marchesano R, Etchells EE. Frequency, type and clinical importance of medication history errors at admission to hospital: a systematic review. CMAJ. 2005;173(5):510–515. | |
Coleman EA, Smith JD, Raha D, Min SJ. Posthospital medication discrepancies: prevalence and contributing factors. Arch Intern Med. 2005;165(16):1842–1847. | |
The Joint Commission. Sentinel Event Alert Issue 35: Using medication reconciliation to prevent errors, January 25, 2006. Available from: http://www.jointcommission.org/assets/1/18/SEA_35.pdf. | |
Poon EG, Blumenfeld B, Hamann C, et al. Design and implementation of an application and associated services to support interdisciplinary medication reconciliation efforts at an integrated healthcare delivery network. J Am Med Inform Assoc. 2006;13(6):581–592. | |
Cimino JJ, Bright TJ, Li J. Medication reconciliation using natural language processing and controlled terminologies. Stud Health Technol Inform. 2007;129(Pt 1):679–683. | |
Schnipper JL, Hamann C, Ndumele CD, et al. Effect of an electronic medication reconciliation application and process redesign on potential adverse drug events: a cluster-randomized trial. Arch Intern Med. 2009;169(8):771–780. | |
Hawai i Health Information Exchange. Available from: https://www.hawaiihie.org/. Accessed March 20, 2015. | |
Patient-Centered Primary Care Collaborative, Pharm2Pharm. April 2014. Available from: https://www.pcpcc.org/initiative/pharm2pharm-formal-hospital-pharmacist-community-pharmacist-collaboration. Accessed April 14, 2015. | |
Spahni S, Lovis C, Ackermann M, Mach N, Bonnabry P, Geissbuhler A. Securing chemotherapies: fabrication, prescription, administration and complete traceability. Stud Health Technol Inform. 2007;129(Pt 2):953–957. | |
Panahiazar M, Taslimitehrani V, Jadhav A, Pathak J. Empowering Personalized Medicine with Big Data and Semantic Web Technology: Promises, Challenges, and Use Cases. Proc IEEE Int Conf Big Data. 2014;2014:790–795. | |
Schwartz DN, Evans RS, Camins BC, et al. Deriving measures of intensive care unit antimicrobial use from computerized pharmacy data: methods, validation, and overcoming barriers. Infect Control Hosp Epidemiol. 2011;32(5):472–480. | |
Google FluTrends, available from: https://www.google.org/flutrends/us/#US. Accessed April 10, 2015. | |
Paul MJ, Dredze M, Broniatowski D. Twitter improves influenza forecasting. PLoS Curr. 2014 Oct 28;6. | |
Davidson MW, Haim DA, Radin JM. Using networks to combine “big data” and traditional surveillance to improve influenza predictions. Sci Rep. 2015;5:8154. | |
Marra F, Patrick DM, Chong M, Bowie WR. Antibiotic use among children in British Columbia, Canada. J Antimicrob Chemother. 2006;58(4):830–839. | |
Price C, Stallard N, Creton S, et al. A statistical evaluation of the effects of gender differences in assessment of acute inhalation toxicity. Hum Exp Toxicol. 2011;30(3):217–238. | |
Drenick G. Going beyond big data to knowledge webpage on the internet. Forbes [updated March 11, 2014]. Available from: http://www.forbes.com/sites/prospernow/2014/03/11/going-beyondbig-data-to-knowledge/. Accessed April 10, 2015 | |
Wilson S. Data protection: Big data held to privacy laws, too. Nature. March 26, 2015;519(7544):414. | |
Fitbit [homepage on the Internet]. Available from: www.Fitbit.com. Accessed April 10, 2015. | |
Curfman GD, Morrissey S, Drazen JM. Prescriptions, privacy, and the First Amendment. N Engl J Med. 2011;364(21):2053–2055. | |
Sorrell, Attorney General of Vermont v. IMS Health Inc. 630 F.3d 263 (2d Cir. 2010). | |
Padwal R, Kezouh A, Levine M, Etminan M. Long-term persistence with orlistat and sibutramine in a population-based cohort. Int J Obes (Lond). 2007;31(10):1567–1570. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.