Back to Journals » Clinical Ophthalmology » Volume 16
Bicanalicular Annular Stent Compared with Bicanalicular Nasal Intubation in Management of Traumatic Lower Canalicular Laceration
Authors Mansour HO, Ramadan Ezzeldin E ![]()
Received 11 November 2021
Accepted for publication 7 January 2022
Published 28 January 2022 Volume 2022:16 Pages 213—222
DOI https://doi.org/10.2147/OPTH.S347057
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Hosam Othman Mansour,1,2 Ezzeldin Ramadan Ezzeldin2
1Magrabi Eye Hospital, Tanta, Egypt; 2Ophthalmology Department, Al Azhar University, Damietta Branch, New Damietta, Egypt
Correspondence: Hosam Othman Mansour
Ophthalmology Department, Faculty of Medicine, Al Azhar University, New Damietta, Egypt
, Email [email protected]
Purpose: To report the functional and anatomical results of bicanalicular annular stent compared to bicanalicular nasal intubation in the management of traumatic lower canalicular laceration.
Patients and Methods: A retrospective comparative, non-randomized interventional study. The study included consecutive patients suffering from traumatic lower canalicular laceration attended to ophthalmology department causality at Al Azhar University hospital Damietta branch, between December 2018 and August 2020.
Results: The study recruited eighty-five eyes of eighty-five patients admitted for treatment of traumatic lower canalicular laceration. In thirty-three patients, canalicular integrity was restored by bicanalicular annular stent (group 1) and in twenty five patients by bicanalicular lacrimal intubation (group 2). The affected patients were predominantly males (78.8% in the first group and 80% in the second group). Etiology of trauma was due to occupational hazards; 48.5% in the first group and 36% in the second group. Anatomical success in the first group was 93.9%, and 92% in the second group. Canalicular patency was achieved in 90.9% in the first group and in 80% in the second group.
Conclusion: There was no statistically significant difference between bicanalicular annular stent and bicanalicular nasal intubation regarding both anatomical and functional success. Both techniques represent a successful alternative to monocanalicular stent.
Keywords: lacrimal stent, bicanalicular nasal intubation, canalicular laceration and epiphora
Introduction
Eyelid injury is a common ophthalmic emergency, requiring planned treatment to provide the best outcome and to reduce the risks of post-operative complications. The most common causes of eyelid injury, which can be dull or sharp; are traffic, sports injuries, accidents, dog bites, and injuries related to violence.1,2 The lower eyelids are more commonly involved than upper eyelids.3
Lacrimal canalicular lacerations are more common in males in comparison with females and more in children and young adults. Blunt trauma from fist fighting is the most frequent cause. Elderly patients may be susceptible to this type of injury as a result of facial trauma during falls.4 Lacrimal canaliculi are vital structures that play an important role in tear drainage from the eye and are considered a significant part of the active pump system. The risk of canalicular laceration is more in injuries to the medial eyelid and canthal region. Canalicular injury can result in cosmetic problems and epiphora.5
Based on the mechanisms of damage, Wulc et al divided canalicular lacerations into indirect trauma, such as blunt trauma and direct trauma as knife and dog bite injuries. It has been reported that the condition of patients with canalicular lacerations due to diffused or indirect injuries can be attributed to factors other than the presence of penetrating injuries.6 There is a risk of lacrimal drainage dysfunction with epiphora, if not appropriately managed with lacrimal canalicular anastomosis, combined with bicanalicular or monocanalicular stent intubation for primary canalicular laceration repairs.7
The monocanalicular stent in comparison with bicanalicular stent remains an issue of debate, but the most perceived adverse effects of bicanalicular stent are the risks of potential injury to intact canaliculus, canalicular or punctal splitting, superior loop dislocation, chronic nasal irritation and granuloma formation.8
The present study compares bicanalicular lacrimal annular stent to bicanalicular nasal intubation in patients with traumatic lower canalicular laceration as alternative options to monocanalicular stent.
Patients and Methods
A retrospective, non-randomized comparative interventional study was retrieved from medical records of 58 patients diagnosed with primary lower canalicular laceration that require surgical repair. The study was conducted at Ophthalmology department in Al Azhar University Hospital Damietta branch, from December 2018 to August 2020 by a single surgeon. All patients or their legal guardians signed a written informed consent to participate in the study and for publication of data before being enrolled in the study (after explaining the nature of the procedure and all study details).
In thirty three patients canalicular laceration was repaired aided by bicanalicular annular stent (group 1), and in twenty five patients by bicanalicular lacrimal intubation (group 2).
All patients included in this study were subjected to complete general and ophthalmic examinations.
Exclusion Criteria
Pre-injury epiphora.
Additional lacerations involving upper punctum, the lacrimal sac and/or nasolacrimal duct.
Associated rupture globe.
Previous lacrimal passage surgery.
Lack of adequate follow up.
Surgical Procedures
Surgical intervention was carried out using an operating room microscope, under general anesthesia.
Examination of the lacrimal system was done by irrigation of the lacrimal canaliculi with a 2.0 mL syringe of 0.9% saline solution. If the liquid flowed from the wound, a lacrimal probe was used to confirm the position of the distal lacerated end of the lacrimal canaliculus. The distance from the lacrimal punctum and the distal lacerated end was measured.
In Group (1);Figure 1
First, we prepare the stent by cutting an area of about 25mm of the silicone stent and placement of 6\0 prolene inside the stent of about three times the length of the stent. After routine sterilization, a punctum dilator was used to dilate the lacrimal punctum. Pigtail probe introduced into the lower punctum to get silicone tube from the wound. Withdrawal of the pigtail probe from the lower punctum, and this step will be repeated in the intact punctum. Tying the prolene 6\0 in 4 knots, and baring the knots inside the stent then rotated to be inside the lacrimal sac. The canalicular edges were then approximated using 6\0 vicryl sutures. Any coexistent lid laceration was repaired using 6\0 vicryl to ensure tissue integrity.
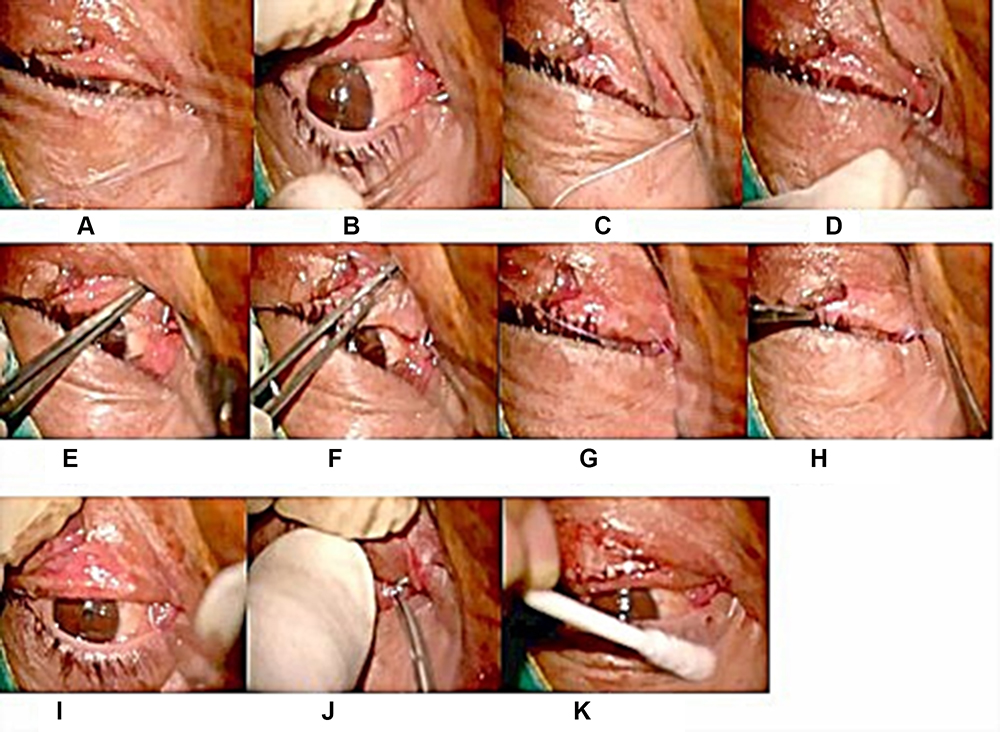 |
Figure 1 Bicanalicular annular stent: (A) preparing the stent. (B) Pigtail probe was introduced into the lower punctum to get silicone tube from the wound. (C and D) Withdrawal of the pigtail probe from lower punctum. (E and F) This step repeated in the intact punctum. (G and H) Tying the proline 6\0 in 4 knots (I) Baring knots inside the stent then rotated to be inside the lacrimal sac. (J and K) Then canalicular edges were approximated using 6\0 vicryl sutures and repair lid laceration. |
In Group (2);Figure 2
After routine sterilization, the proximal lacerated end was located using the surgical microscope. The most challenging point of the surgery is to identify the medial cut end of the lacerated canaliculus. In addition to direct inspection of the pinkish tubular canalicular mucosal tissue and traction surrounding soft tissue, we used saline injection through the opposite punctum while maintaining pressure over the lacrimal sac. After injection, the flow of saline from the medial cut area facilitated the identification of the cut end of the canaliculus. A punctum dilator was used to enlarge the lacrimal puncti, and the proximal lacerated end was located; then, one head of Crawford lacrimal tube was inserted into the lower canaliculus. The tube was then pulled from the inferior meatus of the nose. The previous two steps were repeated in the upper canaliculus by the same technique. Tie and trim ends in the nose just before skin closure. The proximal and distal lacerated ends were subsequently anastomosed with 6\0 absorbable suture and then canalicular edges were approximated using 6\0 vicryl sutures.
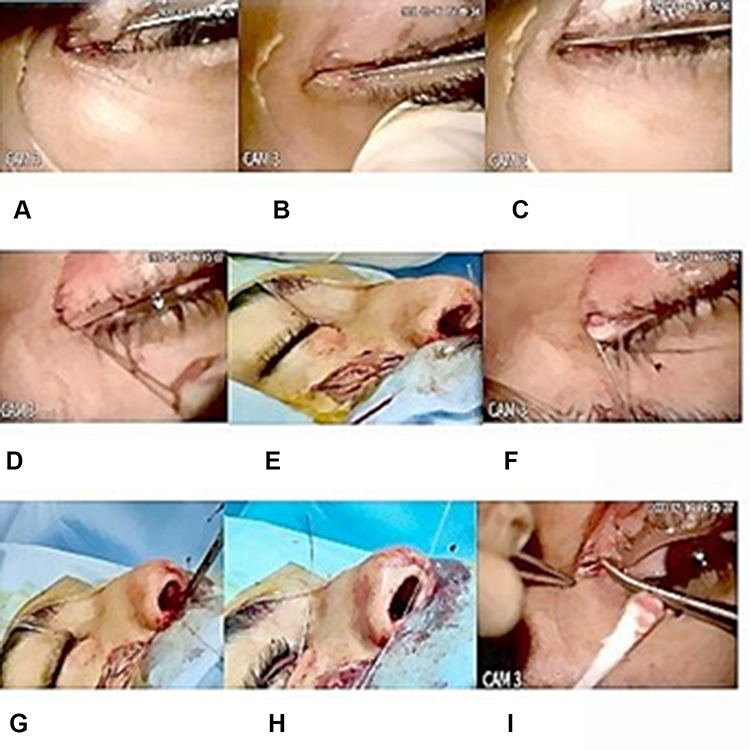 |
Figure 2 Bicanalicular nasal intubation: (A and B) A punctum dilator was used to enlarge the lacrimal puncti. (C) The proximal lacerated end was located. (D) One head was inserted into the lower canaliculus. (E) It was pulled from the inferior meatus of the nose. (F and G) The other end was placed into the upper canaliculus and pulled out from the nasal cavity by same technique. (H) Tie and trim ends of the tube in the nose. (I) The proximal and distal lacerated ends were subsequently anastomosed with 6\0 absorbable suture and Canalicular edges were approximated using 6\0 vicryl sutures. |
Post-Operative Management
Patients were warned against rubbing or removal of the tube themselves. Antibiotics were simultaneously administrated locally and intravenously to guard against infection. Post-operative follow-up visits were recorded at 1 week and 1, 3, and 6 months. The silicone tube was shifted and checked monthly. Tube removal performed 6 months after surgery, followed by lacrimal irrigation.
The surgery outcome was defined by lacrimal irrigation and the presence of symptomatic epiphora.
Statistical Analysis
Quantitative data were expressed in the form of mean, standard deviation (SD), and range. On the other side, qualitative data were expressed in the form of relative frequency and percent distribution. The P-value was considered significant if <0.05. Statistical analysis was performed using the commercially available statistical package for social sciences (SPSS) software package, for windows, version 24 (IBM®SPSS® Inc., Chicago, Illinois, USA).
Results
Demographic Data (Table 1)
The study included 58 patients (58 eyes). Thirty-three patients were treated by bicanalicular annular stent (group 1), and 25 were treated by bicanalicular nasal intubation (group 2). No significant differences were found between the 2 groups regarding sex distribution, patients’ age, laterality, time of surgical intervention or type of trauma. There was male sex predominance in both groups and most patients were young adults. The most common cause of trauma in both groups was occupational injuries.
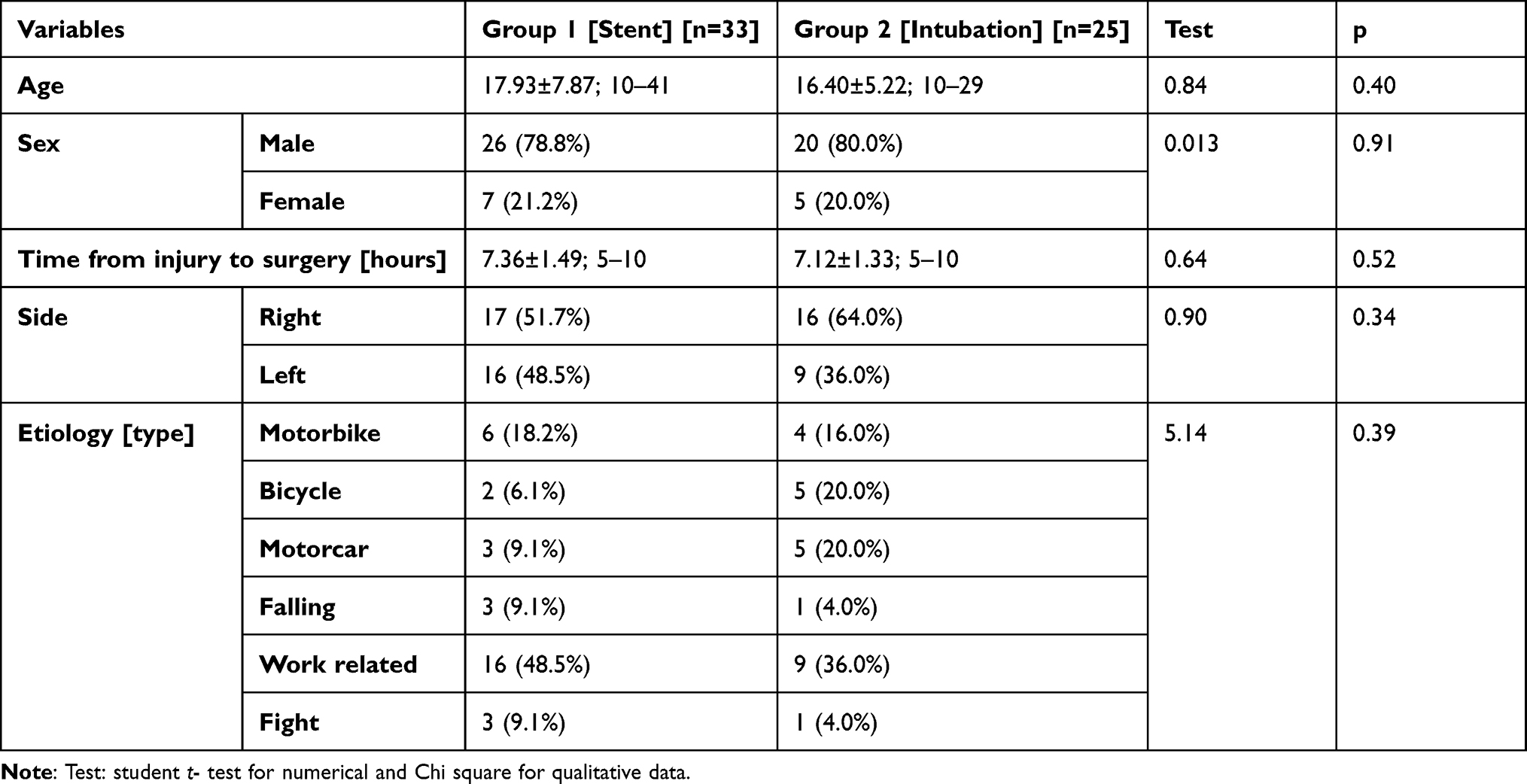 |
Table 1 Patients’ Characteristics |
Table 1 includes the Patients’ characteristics
Anatomical Results, Figures 3 and 4
There was no statistically significant difference between two groups as regard the postoperative anatomical success, canalicular block nor punctal slit. Group 1 achieved overall anatomical success in 93.9% of patients, while group 2 achieved 92% overall anatomical success.
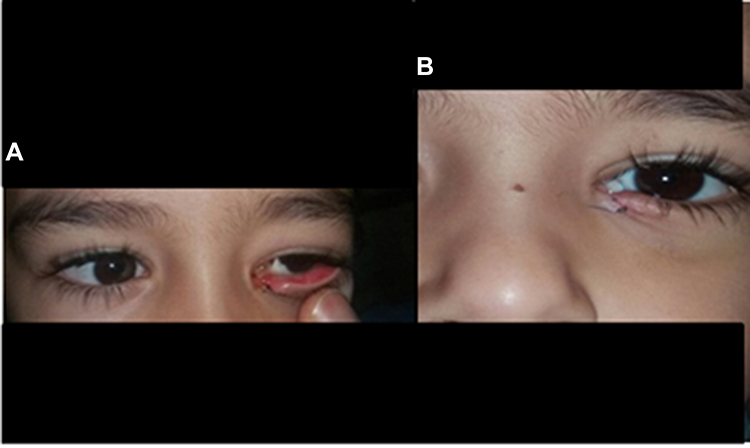 |
Figure 3 Bicanalicular annular stent; (A) preoperative. (B) postoperative. |
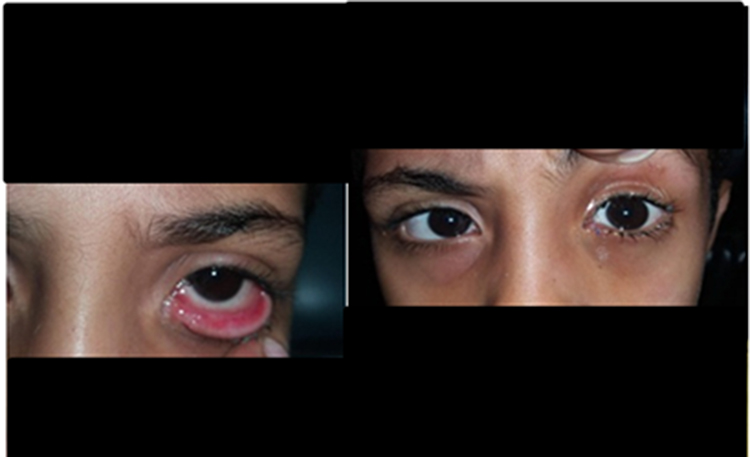 |
Figure 4 Bicanalicular nasal intubation; (A) preoperative. (B) postoperative. |
Functional Results (Figures 5 and 6)
Postoperative functional success was defined by patency of the lacrimal passage and absence of clinical epiphora. With regard to functional results, there were no statistically significant differences. The first group (treated by bicanalicular annular stent) achieved 90.9% success, while in the second group (treated by bicanalicular nasal intubation) the success rate was 80%.
 |
Figure 5 Premature extrusion of the tube after bicanalicular nasal intubation. |
 |
Figure 6 Punctal slit (cheese wiring) after bicanalicular nasal intubation. |
The risk of premature tube extrusion was higher in group 2; in the first three months premature tube extrusion was recorded in 16.0% in comparison with 6.1% in group 1, and between 3 and 6 months premature tube extrusion was recorded to be 8% in comparison with 3% in group 1 (Table 2).
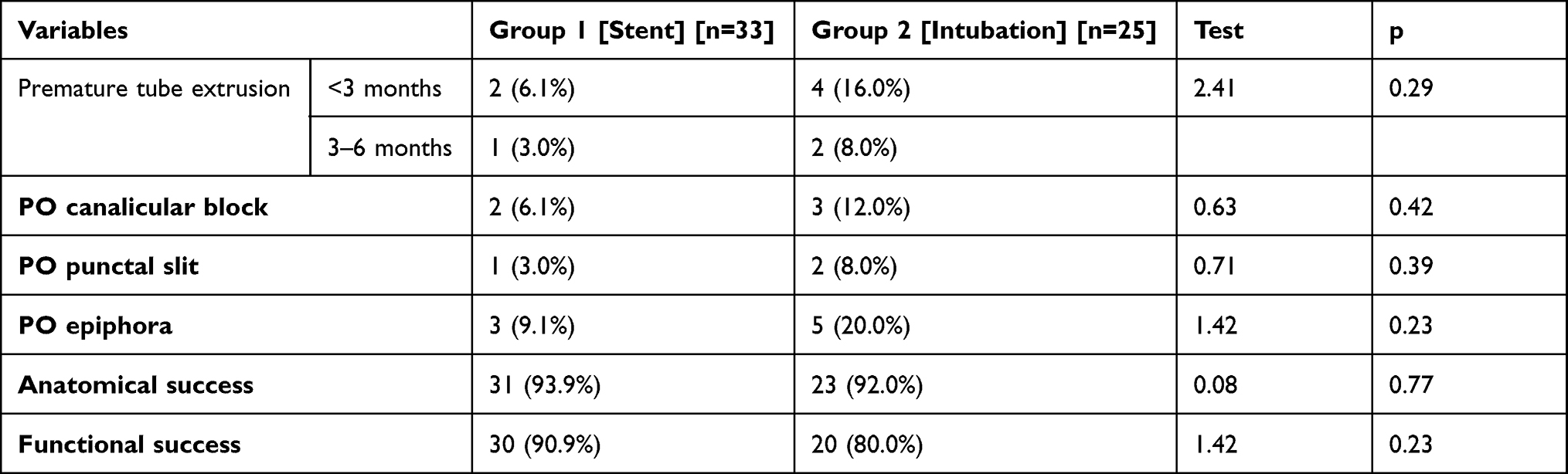 |
Table 2 Post-Operative Results |
Discussion
Eyelid injuries are once in a while associated with a lacrimal canalicular laceration on behalf of this the canaliculi present just beneath the thin layer of the eyelid skin without additional protection. The lower canaliculi are particularly more vulnerable to direct penetrating and diffuse avulsion, or indirect blunt injury.9
The reconstruction of the lacrimal canalicular lacerations requires repair with stent placement. Various surgical techniques for repair and different materials for the intubation of the damaged canaliculus (both monocanalicular and bicanalicular) have already been described in literature. Silicone is the most common material used to prevent canalicular obstruction. Silicone has gained popularity as the ideal stent as it is soft, inert, and pliable, thus avoiding trauma to the healing tissues. Silicone stability and inert nature allows it to remain in place for longer periods. For the canalicular stenting, one essentially must choose from either a monocanalicular stenting, an annular stent-assisted by pigtail probe, or bicanalicular intubation.10
Prevention of epiphora following trauma can be achieved with proper diagnosis, and an appropriate surgical approach. Some authors have stated that the lower canaliculus is more important, and therefore prefer not to use a probe in the repair of the upper canaliculus. On the contrary, other authors have reported that tear drainage has a significant role in the function of both canaliculi.11
The present study demonstrated no significant differences between the two groups regarding sex distribution, patient age, laterality, time of surgical intervention, and type of trauma. However, there was male sex predominance in both groups, and most of the patients were young adults. The most common cause of trauma was occupational hazards.
Several studies demonstrated that these injuries affect mostly young patients; indeed, the age of patients in the current study ranged from 10 months to 60 years.
In the current work, the affected patients were predominantly males 78.8% in the first group and 80% in the second group.
In agreement with our work, Adibelli and Cakmak showed that males are more prone to such injury; 51 out of 64 patients (79.7%) were males, with a mean age at presentation of 14.6 years (range: 1–69 years). The incidence of lower canalicular lacerations was 65.6%, and 29.7% of patients had isolated upper canalicular lacerations.12
Sendul et al demonstrated that the most common causes of injuries were assaults, motor vehicle accidents, falling, and trauma from a sharp object, in order of decreasing frequency.10
In our work, the most common cause of canalicular laceration was due to occupational hazards; 48.5% in the first group and 36% in the second group.
The bicanalicular versus monocanalicular stent remains a controversial issue. One of the most perceived disadvantages of bicanalicular stent is the risk of potential injury to uninvolved canaliculus in addition to other complications such as punctal cheese wiring, chronic nasal irritation, and granuloma formation. Nevertheless, one potential advantage of bicanalicular stent is the ability to maintain distal tension while the surrounding soft tissue is repaired, which is considered important for canalicular laceration repair and it would be beneficial for the connection between the distal and proximal canaliculus breakages8.
In agreement with the present study, Maheshwari and Maheshwari reported that the bicanalicular annular stent minimizes the chances of extrusion of the tube, retains the integrity of the delicate canalicular tissue, and maintains the natural anatomic alignment of the cut ends of the canaliculus.13
In the present study, there was a higher risk of premature tube extrusion in group 2 (although not statistically significant); in the first three months premature tube extrusion was 16.0% compared with 6.1% in group 1. Between 3 and 6 months the incidence was 8% in group 2 compared to 3% in group 1.
Murchison et al found no significant difference in the success rate of bicanalicular and monocanalicular repairs but did find that the training level of the surgeon significantly affected success for all types of repair.14
There is no consensus as regards the exact duration of canalicular stent to obtain long-term canalicular patency. Nevertheless, the majority of studies still tend to maintain the stent for a longer duration (3 to 12 months), and they postulated that it is important for the epithelization and healing process of the lumen of the lacrimal canaliculi.14,15
A study conducted by Zhang et al on 43 eyes underwent canalicular intubation. The success rate was estimated six months after the surgery.16
In the present study, we kept the tube in place for 6 months in the majority of eyes, earlier tube removal was done in cases of premature tube extrusion; before 3 months 6.1% in group 1, and 16% in group 2. Between 3 and 6 months 3.0% in group 1, and 8.0% in group 2.
In the current study, there was no statistically significant difference between the two groups regarding postoperative anatomical success, canalicular block or punctal slit. The functional success is known as lack of postoperative epiphora, while anatomic success defined as softly diagnostic probing to sac. Anatomical success in group 1 was 93.9%, while group 2 achieved 92% overall anatomical success. Postoperative functional success was 90.9% in group 1 treated by bicanalicular annular stent and it was 80% in group 2 treated by bicanalicular nasal intubation.
Most studies showed that primary canalicular laceration repair with canalicular stent intubation could retain a high success rate (from 58% to 100%) in avoiding posttraumatic epiphora.17
Lang et al reported the result of 34 eyes and showed that the 31 eyes (91.18%) achieved complete success (complete disappearance of epiphora after tube removal), and 3 eyes (8.82%) achieved partial success (some residual symptoms under irritating conditions, such as winter weather or wind), postoperative tearing was noticed in three eyes, among which, two eyes had a lower canalicular laceration and one eye had bicanalicular lacerations before surgery. They reported cheese wiring of the lower punctum in only one case (2.86%) 1 month after the surgery, and the tubes in this patient were removed prematurely. This patient had recurrent epiphora 1 month after removal of the tube.18
Guo et al conducted bicanalicular stent intubation on 142 patients, and concluded that 98.59% had anatomic success and 83.8% had functional success.7
Liu et al reported the results of canalicular laceration in 47 eyes, the study concluded that all cases were anatomically rehabilitated after surgery; 91.11% achieved complete success, and 8.89% achieved partial success (epiphora occurs under irritant conditions, such as wind or cold), 4 eyes showed postoperative tearing, with three eyes having inferior lacrimal duct laceration, and one eye with a superior canalicular laceration. Apart from two cases (4.26%) suffering inferior punctum splitting.19
Limitations of This Study
The study was limited by its retrospective nature.
Conclusion
There was no statistically significant difference between bicanalicular annular stent and bicanalicular nasal intubation regarding both anatomical and functional success. Both techniques represent a successful alternative to monocanalicular stent.
Compliance with Ethical Standards
The study was approved by the Ethical Committee of Al Azhar University. All parents or legal custodians of the children recruited in the study received through explanation of the nature of the surgical procedures entailed, the expected outcome and possible complications, and provided an informed consent. The study adhered strictly to the tents of the Declaration of Helsinki (2013 revision).
Acknowledgment
The present study was conducted in Al Azhar University Hospital, New Damietta, Egypt.
Funding
None of the authors has financial interests or other relationships including grants or research support relative to the content of the study.
Disclosure
The authors report no conflicts of interest.
References
1. Bowling B. Kanski’s Clinical Ophthalmology: A Systematic Approach.
2. Pauly M, Naik M, Abraham PS, Anantharaman G. Eyelid avulsion managed with composite auto graft in a 6-year-old child. Kerala J Ophthalmol. 2017;29(1):49–50. doi:10.4103/kjo.kjo_53_17
3. Subramanian N. Reconstructions of eyelid defects. Indian J Plast Surg. 2011;44(1):5–13. doi:10.4103/0970-0358.81437
4. Wladis EJ, Dewan MA. Periorbital trauma from pit bull terrier attacks. Orbit. 2012;31(3):200–202. doi:10.3109/01676830.2012.669008
5. Aytoğan H, Uğurlu ŞK. Evaluation of anatomical and functional outcomes in patients undergoing repair of traumatic canalicular laceration. Ulus Travma Acil Cerrahi Derg. 2017;23(1):66–71. doi:10.5505/tjtes.2016.65021
6. Wulc AE, Arterberry JF. The pathogenesis of canalicular laceration. Ophthalmology. 1991;98:1243–1249. doi:10.1016/S0161-6420(91)32148-1
7. Guo T, Qin X, Wang H, Lu Y. Etiology and prognosis of canalicular laceration repair using canalicular anastomosis combined with bicanalicular stent intubation. BMC Ophthalmol. 2020;20(1):246. doi:10.1186/s12886-020-01506-w
8. Bai F, Tao H, Zhang Y, Wang P. Old canalicular laceration repair: a retrospective study of the curative effects and prognostic factors. Int J Ophthalmol. 2017;10(6):902–907. doi:10.18240/ijo.2017.06.11
9. Kim T, Yeo C-H, Chung K-J, Lee JH, Kim,Y-H. Repair of lower canalicular laceration using the Mini-Monoka stent. J Craniofac Surg. 2018;29(4):949–952. doi:10.1097/SCS.0000000000004423
10. Sendul SY, Cagatay HH, Dirim B, et al. Reconstructions of traumatic lacrimal canalicular lacerations: a 5 years’ experience. Open Access J Sci Technol. 2015;3:1–6. doi:10.11131/2015/101121
11. Ho T, Lee V. National survey on the management of lacrimal canalicular injury in the United Kingdom. Clin Exp Ophthalmol. 2006;34(1):39–43. doi:10.1111/j.1442-9071.2006.01137.x
12. Adibelli FM, Cakmak SS. The repair of canalicular lacerations with an annular silicone tube and round-tipped pigtail probe. Asian J Ophthalmol. 2020;17:188–195. doi:10.35119/asjoo.v17i2.561
13. Maheshwari RD, Maheshwari M. Annular intubation with pigtail probe for canalicular lacerations. Indian J Ophthalmol. 2020;68(10):2166–2169. doi:10.4103/ijo.IJO_8_20
14. Murchison AP, Bilyk JR. Canalicular laceration repair. An analysis of variables affecting success. Ophthalmic Plast Reconstr Surg. 2014;30(5):410–414. doi:10.1097/IOP.0000000000000133
15. Liang T, Zhao G, Li Y, Yang S, Zhang L, Wu Y. Efficiency and therapeutic effect of modified pigtail probe in anastomosing lacerated lacrimal canaliculus. Chin J Traumatol. 2009;12(2):87–91.
16. Zhang M, Li B, Zhang N. The study of a new modified bicanalicular intubation for the repairment of traumatic canalicular laceration. J Ophthalmol. 2019;2019:8435185. doi:10.1155/2019/8435185
17. Tao H, Wang P, Han C, Zhang J, Bai F, He ZY. One-stitch anastomosis through the skin with bicanalicular intubation: a modified approach for repair of bicanalicular laceration. Int J Ophthalmol. 2013;6(5):656–658. doi:10.3980/j.issn.2222-3959.2013.05.19
18. Liang X, Lin Y, Wang Z, Lin L, Zeng S. A modified bicanalicular intubation procedure to repair canalicular lacerations using silicone tubes. Eye. 2012;26(12):1542–1547. doi:10.1038/eye.2012.212
19. Liu Z, Sha X, Liang X, Wang Z. Use of silicone tubes to repair canalicular lacerations via a novel method. Eye Sci. 2013;28(4):195–200.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.