Back to Journals » International Journal of Women's Health » Volume 17
Beyond the Cycle: Investigating the Relationship Between Menstrual Hygiene Factors, Family Economic Stability, and Depression Among Adolescent Girls in Uganda—A 24 Month Mixed-Effects Regression Analysis of the Suubi4Her Trial
Authors Namuwonge F ![]() , Namatovu P, Kizito S, Ssentumbwe V, Tutlam NT, Nabunya P, McKay MM, Ssewamala FM
, Namatovu P, Kizito S, Ssentumbwe V, Tutlam NT, Nabunya P, McKay MM, Ssewamala FM
Received 23 May 2025
Accepted for publication 24 October 2025
Published 31 October 2025 Volume 2025:17 Pages 4033—4046
DOI https://doi.org/10.2147/IJWH.S536692
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Flavia Namuwonge,1 Phionah Namatovu,1 Samuel Kizito,2 Vicent Ssentumbwe,2 Nhial T Tutlam,2 Proscovia Nabunya,2 Mary M McKay,3 Fred M Ssewamala2
1International Center for Child Health and Development, Masaka Field Office, Masaka, Uganda; 2Brown School, International Center for Child Health and Development, Washington University in St. Louis, St. Louis, MO, 63130, USA; 3Office of the Provost, Washington University in St. Louis, St. Louis, MO, 63130, USA
Correspondence: Flavia Namuwonge, International Center for Child Health and Development, Masaka Field Office, P.O. Box 1988, Masaka, Uganda, Email [email protected]
Purpose: Menstrual hygiene management (MHM) is essential for adolescent well-being, yet many girls lack adequate menstrual products. While MHM factors are linked to depression, little is known about these associations in Uganda. Because financial insecurity and family context can intensify or buffer menstrual challenges, we examined the relationships between menstrual knowledge, pain, affordability barriers, supply type, restrictions, and depression in the context of an intervention targeting economic and family support.
Methods: We analyzed data from a three-arm cluster randomized controlled trial (Suubi4Her) with a 24 month follow up (2018 to 2022). A total of 1260 adolescent girls aged 14 to 17 from 47 secondary schools in Uganda were randomized into three study arms: Control (n=16 schools, n=408); Economic Empowerment using Youth Development Accounts (YDA) (n=16 schools, n=471), matched savings accounts promoting financial literacy and economic stability; and YDA plus Family Strengthening Intervention using Multiple Family Group (MFG) meetings (n=15 schools, n=381), structured caregiver-adolescent sessions to improve family communication, support, and problem solving. Depression was assessed using the Beck Depression Inventory (BDI). Mixed effects regression models examined associations, adjusting for school and individual clustering.
Results: Age (β= -0.98, 95% CI: -1.32, -0.64, p < 0.001) was significantly associated with lower depression. Menstrual knowledge (β=0.83, 95% CI: 0.61, 1.06, p < 0.001), menstrual pain (β=0.73, 95% CI: 0.51, 0.95, p < 0.001), affordability barriers (β=3.55, 95% CI: 2.41, 4.30, p < 0.001), and menstrual restrictions (β=1.22, 95% CI: 0.16, 2.28, p= 0.024) were also associated with increased depression. Hygienic products weakened the psychological impact of menstrual pain (β=-0.40, 95% CI: -0.63, -0.16, p= 0.001). Intervention participants had lower depression (YDA: β= -1.88, 95% CI: -3.09, -0.68, p = 0.002; YDA+MFG: β= -1.89, 95% CI: -3.21, -0.56, p= 0.005). Taken together, these results suggest that menstrual hygiene challenges increase the risk of depression, while age, access to hygienic products, and participation in supportive interventions can mitigate these negative effects.
Conclusion: Findings point to a need for comprehensive MHM programs integrating family economic support, pain management, and mental health. Addressing affordability barriers and menstrual stigma enhances adolescent girls’ well-being.
Plain Language Summary: Many adolescent girls in Uganda face challenges managing their periods. Some cannot afford menstrual products like pads. Others experience physical discomfort, such as pain, and are often limited in what they can do during their period, including attending school or participating in daily activities.
This study looked at whether these menstrual hygiene challenges are linked to symptoms of depression. It included 1260 girls between the ages of 14 and 17 from 47 secondary schools in Uganda. The girls were part of a larger study testing two programs: one offered support through savings accounts and financial education, and the other added family group meetings to support better communication and care within families.
The researchers found that girls who had more menstrual pain, could not afford pads, or had restrictions on their activities during menstruation were more likely to report feeling depressed. Those who participated in the savings and family support programs also had better mental health compared to those who received only basic school support.
These results suggest that improving access to menstrual products and offering support through savings and family programs can help reduce depression in adolescent girls. Addressing menstrual health needs is important for supporting girls’ mental well-being.
Keywords: affordability constraints, adolescent mental health, adolescent girls, economic empowerment
Introduction
Adolescence is a critical period marked by significant physical, emotional, and social change.1 In Uganda, many girls lack resources needed to manage menstruation, often resulting in stigma, school absenteeism, and emotional distress.2,3 Menstrual hygiene management involves using clean materials, maintaining personal hygiene, ensuring privacy for changing, safely disposing of used products, and having essential knowledge to manage menstruation with dignity and confidence.4 These challenges mirror global patterns. More than three hundred million women menstruate daily, and about five hundred million lack products and adequate hygiene facilities.5,6 Similar barriers to facilities, privacy, and education hinder school participation in India, South Sudan, Kenya, and Bangladesh,7–9 while access to products and education improves school experiences, as shown in Ghana.10
Poor menstrual hygiene and related barriers are linked to psychological distress11 and depression.12 Stigma and anxiety around menstruation, combined with pain and inadequate facilities, can heighten feelings of helplessness and emotional burden. Evidence also suggests a bidirectional relationship between menstrual pain and depression,13–16 and heavy menstrual bleeding has been associated with higher depression.17 Period poverty, defined as inadequate access to products, safe facilities, and information,18 is consistently associated with worse mental health,19–21 with the COVID-19 pandemic further disrupting access to products and increasing economic strain.22 Use of unhygienic supplies and sanitation insecurity are linked to greater distress and depressive symptoms,23,24 and mobility restrictions during menstruation can contribute to isolation and low self-worth.25,26 Economic interventions, such as subsidies or the removal of taxes on menstrual products, can reduce these barriers and improve access. For example, tax strategies, such as reducing or eliminating the tax on menstrual products, have enhanced the accessibility and affordability of these essential items.27 Beyond fiscal measures, large-scale government-led interventions, such as the Menstrual Health Scheme in Northeast India, have shown that while pad distribution can expand access, it has limited effects unless paired with education, stigma reduction, and supportive facilities.28
The Biopsychosocial Model (BPS)29 provides a comprehensive framework for understanding how biological, psychological, and social factors interact to influence health outcomes. Biological factors encompass physiological processes such as hormonal fluctuations, menstrual pain, and the physical burden of menstruation, which can contribute to emotional distress.30 Social factors, such as access to menstrual hygiene products, affordability of supplies, cultural taboos, and menstrual-related activity limitations, further shape adolescent girls’ experiences with menstruation.31 We apply the BPS Model to examine how interrelated menstrual hygiene-related factors associate with depression among adolescent girls in Uganda. For instance, menstrual pain (a biological factor and an individual-level factor) may lead to psychological distress, particularly if an adolescent holds negative beliefs about menstruation or perceives it as a limitation. These psychological effects may be reinforced by social factors such as inadequate access to sanitary supplies or community-level taboos surrounding menstruation, leading to increased absenteeism from school and social withdrawal. Previous studies have demonstrated that period poverty, including the inability to afford hygienic menstrual products, is associated with higher levels of stress and depressive symptoms.19
Depression is the leading cause of disability worldwide.32 Globally, about one in seven adolescents aged 10 to 19 experience a mental health condition, with depression affecting an estimated 3.5% of those aged 15 to 19.33 The condition arises from a complex interplay of social, psychological, and biological factors,34 with prevalence higher among women (6%) compared to men (4%).35 In Uganda, depressive disorders affect 4.6% of the population,36,37 making it one of the top six African countries with the highest prevalence.36 Rates are higher among females (5.1%) than males (3.6%),38 and approximately 21% of adolescents report depressive symptoms,39 with girls more affected than boys.35 Social determinants such as poverty, gender-based violence, and limited access to education further exacerbate adolescent mental health challenges.40 Despite this high burden, Uganda faces a severe shortage of mental health services, with fewer than one psychiatrist per million people and very limited school-based counseling.41
Regional studies, including work in Gambia, have examined menstrual management challenges, supply access, and psychological impact,42 and research elsewhere has linked period poverty to higher depression among adolescents and young adults.19 However, these studies do not reflect the Ugandan context, where menstrual hygiene challenges may present unique risks to adolescent well-being. In Uganda, prior work has examined menstrual health and mental health, but often with broad tools such as the Strengths and Difficulties Questionnaire (SDQ), which do not capture clinically relevant conditions like depression.43 The present study addresses this gap using the BDI and testing associations between menstrual hygiene-related factors, including affordability barriers, menstrual restrictions, supply type, economic empowerment, and depression. This paper builds on our previously published study that examined the effects of the Suubi4Her intervention on psychosocial well-being (hopelessness, self-esteem, and self-concept) among adolescent girls in Uganda.44 While that study focused on general psychosocial outcomes, the current analysis extends the work by examining depression as a primary outcome and introducing menstrual hygiene-related factors as key predictors. Specifically, we ask: To what extent are menstrual hygiene-related factors, such as affordability barriers, menstrual restrictions, supply type, and menstrual pain, associated with depression among adolescent girls in Uganda, while accounting for economic empowerment and family strengthening interventions?
Methods
Study Setting
Suubi4Her is a National Institutes of Health (NIH)-funded three-arm cluster-randomized trial conducted in 47 secondary schools in the greater Masaka region of Southwestern Uganda. The schools were in five geopolitical districts: Masaka, Kyotera, Lwengo, Rakai, and Kalungu.
Recruitment and Study Population
All eligible participants were identified in collaboration with the school administration and Masaka Diocese. Informational flyers outlining the study and enrolment process were then distributed to these individuals. Interested adolescents and their caregivers subsequently had individual meetings with the local project coordinator to discuss eligibility criteria, the voluntary nature and objectives of the study, the expected participation level, potential risks and benefits, and safety and confidentiality considerations. To meet the eligibility criteria, participants needed to be (1) female, (2) between the ages of 14 and 17, and (3) in their first or second year of secondary school. Individuals residing in institutions or orphanages were deemed ineligible, as one of the interventions was family-based. In total, 1260 adolescent girls were enrolled between March 2018 and February 2019, as shown in the consort diagram (Figure 1). For details on recruitment and intervention, see the study protocol paper.45–48
 |
Figure 1 Suubi4Her Consort flow diagram. |
 |
Figure 2 Interaction plot showing predicted depression scores by menstrual pain and menstrual supply type, from mixed-effects regression. |
Randomization
All eligible girls were recruited and randomized into three study arms at the school level after school selection. Stratified random sampling allocated schools into four strata based on student population size (medium vs large) and geographical location (rural vs urban), ensuring balance across these variables. Restricted randomization (Hayes and Moulton)49 was applied within strata to maintain overall balance across conditions.
The control group (16 schools; 408 students) received usual care, including a school-based sexual and reproductive health curriculum and school supplies. Treatment 1 (16 schools; 471 students) received the control package plus a savings-led Family Economic Empowerment (EE) intervention, which included financial literacy training and Youth Development Accounts (YDA). Treatment 2 (15 schools; 381 students) received all components of the control and Treatment 1 groups, along with a Family Strengthening (FS) intervention delivered via Multiple Family Groups (MFG).
The YDA intervention provided adolescents with matched savings accounts co-signed by a caregiver, with funds designated for school fees or family-based income-generating activities. Participation required completion of financial literacy workshops on savings, asset building, and use of financial institutions. The YDA+MFG intervention combined the economic empowerment package with structured family group sessions focused on the “4Rs” (Rules, Responsibility, Relationships, Respectful communication) and “2Ss” (Stress and Social support). These 16-session meetings involved 12–20 families and extended family members, creating opportunities for shared learning, social support, and problem-solving.47 For details on sessions, refer to Supplemental Tables 1 and 2.
Data Collection Procedure
The survey instruments were translated into Luganda and back-translated into English to ensure accuracy, under the supervision of experts from Makerere University School of Languages. Translators were fluent in both English and Luganda and held relevant academic qualifications. Translations were reviewed by at least three individuals for consistency in meaning. Local research assistants, fluent in both languages, conducted structured interviews at baseline, 12, and 24 months. They received training in good clinical practice, data collection techniques, and human subjects’ protection, and completed the Collaborative Institutional Training Initiative (CITI) Human Subjects certification. Follow-up completion rates were high—96.7% at 12 months and 92.5% at 24 months.
Study Measures
Outcome Variable
Depressive symptoms were assessed using the 21-item Beck Depression Inventory, a validated measure of depressive symptomatology in adolescents.50 Participants were presented with a series of statements reflecting their emotional state over the past two weeks and asked to select the one that best described their experience. Example items include: “I do not feel sad”, “I feel sad”, “I am sad all the time and I cannot snap out of it”, and “I am so sad and unhappy that I cannot stand it”. Each item was coded on a four-point Likert scale ranging from 0 to 3, with 0 indicating the least severe symptom and 3 indicating the most severe symptom. No items required reverse coding. Total scores were computed by summing all 21 items, resulting in a theoretical range of 0 to 63, with higher scores indicating greater depressive symptomatology. In the current sample, the Cronbach’s alpha was 0.83, indicating good internal consistency.
Sociodemographic Characteristics
Participants’ sociodemographic characteristics included 1) age, 2) Orphanhood status categorized as double orphan, single orphan, and non-orphan; 3) Primary caregiver categorized as biological parent, grandparent, and other relative; 4) total number of individuals living in a household; 5) number of children living in a household; and 6) asset ownership assessed by a 21-item index in which participants were asked, “Does the family you live in own the following: house, rentals, car, coffee plantation, banana plantation, etc.?” - coded 1 if they owned the assets and 0 if they did not. The total number was summed up to get the total number of assets in a household. Notably, some participants had not started menstruating at baseline.
Menstrual Hygiene Related Factors
The study included several menstrual hygiene-related factors as predictor variables: 1) Menstrual hygiene knowledge: This was measured using a nine-item true/false scale. Sample statements include: “Women stop menstruating as they grow old”, “Pregnant women menstruate”, and “Pain during the menstruation period means that someone is sick”. Items were coded as “true” (1), “false” (0). Statements in the opposite direction were reverse-coded to ensure higher scores indicated higher menstrual knowledge. The theoretical range for this variable is 0–9 (Cronbach’s alpha 0.572). 2) Affordability barriers were assessed with three yes/no items examining whether participants had purchased disposable sanitary pads in the past six months, whether they had ever wanted to buy pads but were unable to, and whether lack of money prevented them from purchasing pads. Sample items included: “Have you bought disposable sanitary pads from a shop in the last six months?” and “I do not have enough money to buy disposable sanitary pads from a shop”. Responses were recorded as “Yes” (1) or “No” (0). For analysis, these items were combined into a binary variable: No Affordability Barriers (0) vs Faced Affordability Barriers (1). 3) Menstrual-related restrictions were assessed with eight yes/no items that examined whether menstruation limited girls’ participation in daily activities (eg, religious engagement, physical activities, housework, school attendance). Sample items included: “Does your menstruation period make you unable to go to church/mosque/place of worship?” “Does your menstruation period make you unable to do sports?” and “Does your menstruation period make you stay home?” Responses were recorded as “Yes” (1) or “No” (0). The eight-item scale demonstrated acceptable internal consistency (Cronbach’s alpha = 0.74). For analysis, the variable was categorized into two groups: No Menstrual Barriers (0) for those who did not report any restrictions and Faced Menstrual Barriers (1) for those who reported at least one restriction due to menstruation. 4) Menstrual pain was measured with a single item numeric rating scale, where participants rated the average pain experienced during menstruation from 0 (“no pain”) to 10 (“worst pain ever”). 5) Menstrual Supplies were categorized as hygienic vs non-hygienic based on the products participants reported usually using. Participants were asked what they usually use during menstruation, with response options including cloth/towel, tampons, purchased sanitary pads, menstrual cups, toilet paper, reusable pads, cotton, mattress, natural materials (for example, mud, cow dung, leaves), and other materials. Hygienic supplies were defined as tampons, purchased sanitary pads, menstrual cups, and reusable pads. Non-hygienic supplies included cloth/towels, toilet paper, cotton, mattresses, natural materials, and other unspecified items. For classification, participants were coded as using non-hygienic supplies (0) if they reported any non-hygienic item, even if combined with a hygienic item. Participants were coded as using hygienic supplies (1) only if they reported exclusively hygienic items.
Data Analysis Procedure
The data was analyzed in Stata version 18.0. We summarized the baseline characteristics using means and standard deviations for continuous variables and counts and percentages for categorical variables. Summary statistics for baseline characteristics were stratified per study arm. Prior to analysis, we performed preprocessing of the dataset to ensure its cleanliness. We had missing data on menstrual pain (3.6%), menstrual supply type (3.8%), barriers to menstruation (8.23%), total assets (3.6%), and depression (3.6%). Because the proportion of missing data was low, we applied listwise deletion. We utilized mixed-effects linear regression analysis to examine the association between menstrual hygiene management-related factors, economic empowerment, and depression among adolescent girls in Uganda. Because data were collected at multiple time points and participants were nested within schools, we specified a three-level model: repeated observations (level 1) nested within participants (level 2), who were in turn nested within schools (level 3). Fixed effects included age, menstrual knowledge, menstrual pain, affordability barriers, menstrual restrictions, menstrual supply type, the interaction between pain and supply type, and study arm. Random intercepts were specified at both the participant and school levels to account for repeated measures within participants and clustering within schools. Robust standard errors were clustered at the school level. During model construction, we opted for an unstructured covariance structure for the random effects, the most flexible covariance structure. We specified an unstructured covariance matrix for the random effects because it provides the most flexible approach, allowing each variance and covariance to be freely estimated without assuming a particular pattern. This was important in our study, given the hierarchical design (repeated observations nested within participants and participants within schools) and the potential for correlations across levels that may not follow simple structures such as compound symmetry or autoregressive forms. Using an unstructured matrix ensured that we did not impose restrictive assumptions that could bias the estimation of intervention and menstrual health effects, thereby allowing for a more accurate representation of the data’s correlation structure despite the added complexity. We examined the models to determine that the residuals were normally distributed, there was homoskedasticity (VIFs were below 5), and no multicollinearity was detected. The intra-class correlation coefficients were determined using the calculated variances at each level. We reported beta coefficients along with their Huber–White cluster-adjusted confidence intervals. Statistical significance was established at a p-value of 0.05.
Results
Baseline Sample Characteristics
Table 1 shows the participants’ baseline characteristics. The mean age was 15.4 years. Most participants were non-orphans (82.9%), and most reported biological parents as their primary caregivers (76.6%). Each household/family comprised an average of 7 individuals and an average of 3 children. At baseline, 89.1% reported having started menstruating. All baseline characteristics were comparable across the three study arms.
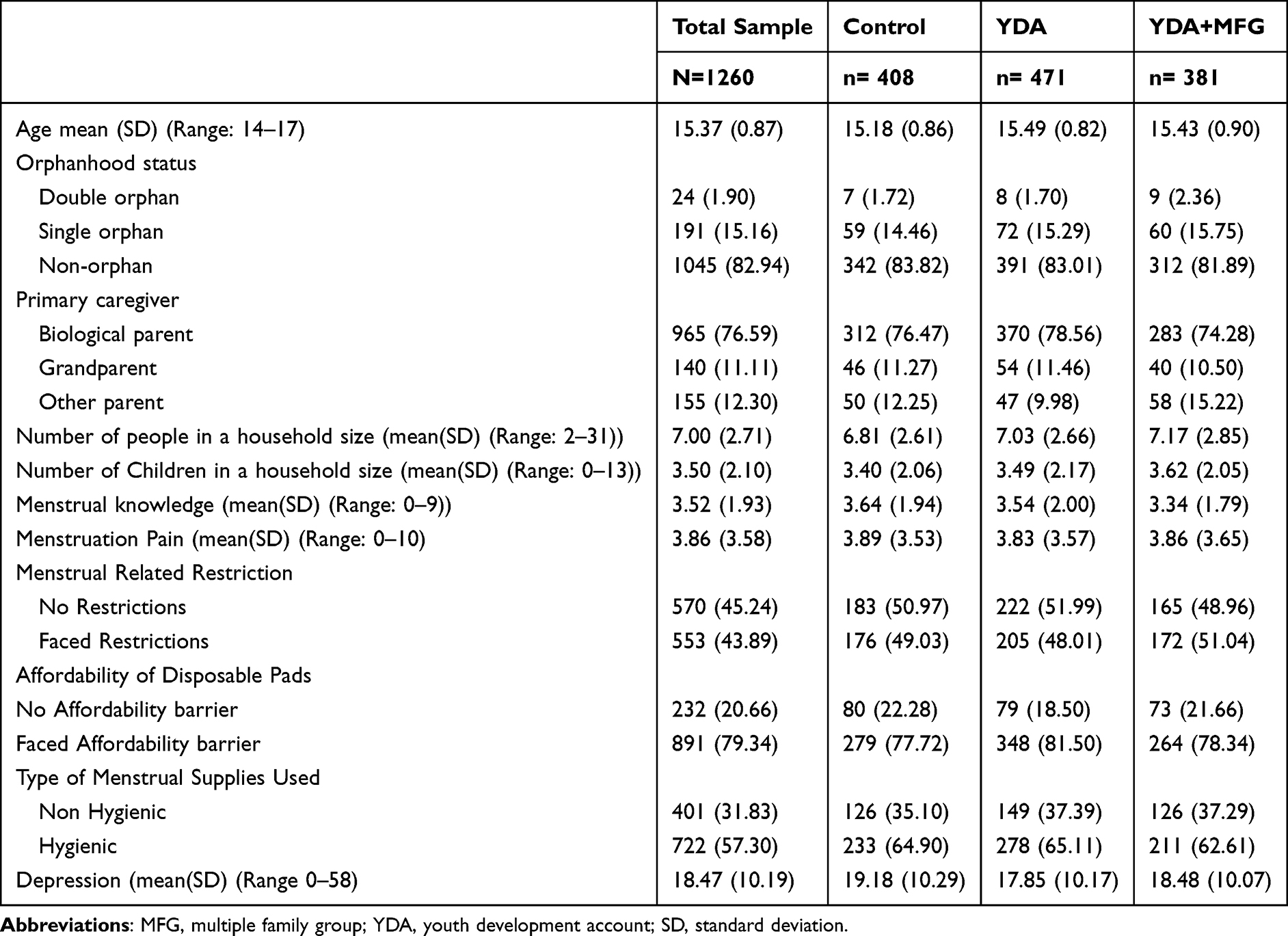 |
Table 1 Baseline Characteristics |
The Association Between Menstrual Hygiene Management Factors and Depression
Results from the mixed-effects model shown in Table 2 indicate that age was significantly associated with lower depression (β = -0.98, 95% CI: -1.32, -0.64, p < 0.001), with older adolescents reporting fewer depressive symptoms. Higher menstrual knowledge (β = 0.83, 95% CI: 0.61, 1.06, p < 0.001) and menstrual pain (β = 0.73, 95% CI: 0.51, 0.95, p < 0.001) were significantly associated with increased depression. Affordability barriers (β = 3.35, 95% CI: 2.41, 4.30, p < 0.001) and menstrual restrictions (β = 1.22, 95% CI: 0.16, 2.28, p = 0.024) were also associated with higher depression. As shown in Figure 2, the interaction between menstrual supply type and pain was significant (β = -0.40, 95% CI: -0.63, -0.16, p = 0.001). Compared to usual care, participants in the YDA (β = -1.88, 95% CI: -3.09, -0.68, p = 0.002) and YDA+MFG (β = -1.89, 95% CI: -3.21, -0.56, p = 0.005) intervention arms reported significantly lower depression scores. These findings are novel because they extend existing evidence on menstrual health by showing that economic and family-strengthening interventions can buffer the psychological effects of menstrual challenges. In particular, the demonstration of an interaction between menstrual pain and hygienic product use provides new evidence that product access can moderate the mental health impact of physical discomfort. The combination of menstrual health factors and intervention arms in one model highlights a unique contribution of this study.
 |
Table 2 Mixed-Effects Regression Model Examining the Association Between Menstrual Hygiene Related Factors and Depression |
Discussion
This study aimed to assess the association between menstrual hygiene-related factors, economic empowerment, and depression among adolescent girls. We examined how menstrual knowledge, affordability, structural barriers, menstrual pain, and supply type contribute to psychological distress. Additionally, we explored the moderating effect of menstrual supply type on the relationship between menstrual pain and depression. The findings highlight key socio-economic and menstrual health factors associated with depression in this population. Menstrual knowledge was significantly associated with depression, suggesting that increased awareness of menstruation may either reflect or contribute to psychological distress. This contrasts with previous research suggesting that better-informed and prepared girls experience positive impacts from menstrual knowledge.51–53 Menstrual knowledge can be beneficial because it reduces uncertainty, improves preparedness, and builds confidence.7,54,55 However, menstrual knowledge may also have adverse effects because it increases awareness of stigma, social restrictions, and the lack of hygienic supplies or adequate facilities in resource-limited contexts.56 In such cases, girls may recognize what they should do to manage menstruation but be unable to act on that knowledge, leading to frustration, anxiety, and psychological distress. Previous research using data from the Suubi4Her study found no significant effect of menstrual hygiene knowledge on self-esteem across intervention groups.48 Our findings expand on this by showing a significant link between menstrual knowledge and depressive symptoms, underscoring the need to pair education with practical resources and supportive environments to ensure that menstrual health knowledge enhances, rather than compromises adolescent girls’ psychological well-being. Evidence from a pilot intervention in Northwest Tanzania similarly demonstrated that education alone was insufficient, psychosocial improvements were observed only when knowledge was combined with access to menstrual products and supportive school environments, reinforcing the importance of multifaceted approaches.57
Affordability barriers were strongly associated with depression, supporting prior findings that financial constraints on menstrual supplies can exacerbate psychological distress by reinforcing social exclusion and limiting participation in daily activities.58 Similarly, other menstrual management barriers beyond affordability were also significantly linked to depression, emphasizing the role of inadequate sanitation, stigma, and lack of privacy in adolescent mental health.59
Menstrual pain was a strong predictor of depression, reinforcing the well-documented link between physical discomfort and mental health.60 However, an interaction was observed between menstrual pain and the type of menstrual supply used. While hygienic menstrual products were initially not significantly associated with higher depression levels, the interaction term indicates that the relationship between menstrual pain and depression is weaker for those using hygienic products. This interaction suggests that while hygienic products alone do not eliminate menstrual-related distress, they may offer some protective effects by improving comfort and reducing hygiene-related anxieties.59 They also improve girls’ ability to attend school and participate in daily activities during menstruation, reducing isolation and stress.61 Conversely, reliance on non-hygienic products may intensify physical discomfort and amplify worry about health risks such as reproductive urinary infections and mental health, thereby strengthening the link between menstrual pain and depression.62 Previous research has shown that access to improved menstrual products can enhance well-being by reducing physical and psychological discomfort and school absenteeism.63 When properly cleaned and dried, reusable menstrual products are considered hygienic and can offer a sustainable option for menstrual management. However, a study in Uganda found that the use of reusable menstrual pads was associated with mental health challenges, possibly due to the complexities of their management.43 This implies that adolescents using hygienic menstrual products may be more likely to perceive menstrual pain as a medical concern rather than a normalized experience. With improved menstrual management, they might become more aware of pain and report it more frequently, as other discomforts such as leakage or poor hygiene are minimized. As a result, this heightened awareness could contribute to increased reporting of both menstrual pain and depressive symptoms rather than indicating an actual increase in these symptoms.
The findings also indicate that participants in both treatment groups reported significantly lower depression levels than those in the control group. This suggests that economic empowerment and family-strengthening interventions may have mitigated psychological distress through economic support, education,47,64,65 or improved menstrual management resources. Even small reductions in depressive symptoms can translate into meaningful gains for adolescents in low-resource contexts, easing distress and improving participation in school and social life, however clinicians should seek evidence for detecting depression.66 Prior interventions integrating economic empowerment and menstrual health education have demonstrated similar mental health benefits,63 highlighting the importance of comprehensive approaches to adolescent well-being. Consistent with this, we observed that older adolescent girls reported lower levels of depression compared to their younger peers. One possible explanation is that older participants may have had more time to benefit from the intervention, potentially gaining greater confidence and support. However, this finding contrasts with other studies showing that depression tends to increase with age during adolescence.33,67 The difference may point to the protective role of intervention exposure and the value of early engagement in support programs. This improvement is particularly notable given that baseline data from this study showed high levels of depressive symptoms among participants.68 It is also possible that developmental variability plays a role, as younger adolescents may experience heightened sensitivity to stigma, peer pressure, or body changes, while older adolescents may have developed greater coping skills and autonomy.69 Alternatively, differences in social roles or expectations across age groups may contribute to variability in depressive symptoms.70
The findings underscore the need for comprehensive menstrual health programs beyond traditional hardware (for example, provision of menstrual products and infrastructure) and software (for example, education and awareness campaigns) approaches. Evidence from East Africa, including large-scale distribution of MHM kits in four countries, showed that dignity, confidence, and participation improved only when girls received not just pads but also supplementary items such as soap, buckets, private storage pouches, and clear information on use and disposal. These interventions highlight that hardware provision must be accompanied by enabling factors such as safe water, sanitation, and hygiene (WASH) facilities and stigma reduction to be effective.71
In the Ugandan context, economic interventions like the Suubi YDA could further reduce financial barriers by helping families consistently afford hygienic products. Equally important, family and community engagement through MFGs offers a pathway to involve not only girls and their caregivers but also boys and men, whose awareness and support have been shown in regional evidence to reduce stigma, shift cultural norms, and promote shared responsibility for menstrual health. Evidence shows that when parents are directly engaged in menstrual health education, girls report greater confidence, reduced shame, and stronger support from their families.72 Building on these lessons, schools can strengthen their role by embedding menstrual health within existing health and life-skills curricula while ensuring access to safe and private WASH facilities, and public health systems can extend support by integrating menstrual health into sexual and reproductive health services, including counseling and pain management. This suggests that pairing adolescent-focused interventions with parental and broader community engagement can amplify the psychosocial benefits of menstrual health programming. Moreover, regional lessons underscore the value of linking menstrual health initiatives with sexual and reproductive health (SRH) services, ensuring that girls receive accurate information, access to care for infections or pain, and broader support around puberty and reproductive well-being.58,71 Taken together, these lessons reinforce that menstrual health initiatives in schools and communities must move beyond product provision alone, linking education with resources, household financial capacity, supportive family and community environments, and integration with health services to sustainably improve adolescent girls’ well-being.
This study has several methodological strengths. The use of the Beck Depression Inventory provides a valid and reliable measure of depressive symptoms. High response and retention rates minimize selection bias and enhance the generalizability of findings, supporting the study’s robustness in low-resource settings. However, some limitations should be noted. However, some limitations should be noted. The study relied on self-reported data, including sensitive topics such as menstruation and depression, which may be subject to recall bias, social desirability, or underreporting. In addition, menstrual product use was assessed categorically (hygienic vs non-hygienic), without capturing variations or mixed use patterns. Adolescents may switch products due to cost, availability, or school context, which may influence associations with depression. The internal consistency of the menstrual knowledge scale was relatively low (Cronbach’s alpha = 0.57), which may indicate heterogeneity in the items. Given this, results should be interpreted cautiously, and future research should refine the measure to improve reliability. Longitudinal designs are also needed to assess causality and the durability of intervention effects over time.
Conclusion
This study provides critical insights into the relationship between menstrual hygiene management and adolescent depression. The findings highlight the need for holistic menstrual health interventions that address not only knowledge gaps but also economic and structural barriers that contribute to psychological distress. Specifically, affordability barriers were strongly linked to higher depressive symptoms, and the moderating role of hygienic products showed that access to appropriate supplies can buffer the psychological burden of menstrual pain. Moreover, participants in the intervention arms (YDA and YDA+MFG) reported lower depression levels than those in the control group, underscoring the value of combining economic empowerment and family-strengthening strategies. Given the high prevalence of depressive symptoms among adolescent girls in low-resource settings, integrating mental health support into menstrual health programs is essential. Such integration could include economic interventions (like YDAs to reduce affordability barriers), family and community-based engagement (via MFGs), and linkage with school or health system based counseling services. These approaches offer practical pathways for policy and program design. Future research should examine the sustained effects of such approaches particularly whether economic support remains effective over time, whether family and community engagement continues to reduce stigma, and whether pain management strategies improve long-term psychological outcomes.
Data Sharing Statement
The dataset used for analysis in the current study is available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Written informed assent was obtained from the adolescent participants, and written informed consent was obtained from their caregivers. The term “caregivers” refers to parents, or legal or primary guardians. For adolescents with living parents, consent was provided by a parent or their designated legal/primary guardian. For adolescents who lost both parents, consent was obtained from the appointed legal or primary caregiver. This was confirmed by both the adolescent and the school. To prevent any compulsion, the procedures for adolescents and adult caregivers were separate. Forms for consent and assent were translated into Luganda from English. Adolescent participants spoke English, although most were more comfortable speaking Luganda. In light of the participants’ English competence, the assent procedure was conducted in either English or Luganda. The research outlined in this manuscript was performed in accordance with the Declaration of Helsinki. All study procedures were approved by the Washington University in St. Louis Institutional Review Board (#201703102) and by in-country local IRBs in Uganda: Uganda Virus Research Institute-Research Ethics Committee (UVRI-REC – GC/127/17/07/619), and Uganda National Council for Science and Technology (UNCST – SS4406). The study is registered in the Clinical Trials database with the identifier NCT03307226.
Acknowledgments
We appreciate the field Research Team at the International Center for Child Health and Development, the participating families, and the children for their outstanding contribution to the research. We also thank our research and implementation partners, the Rakai Health Sciences Program, and Reach the Youth Uganda. Lastly, we thank the research teams at Washington University in St. Louis, Columbia University in New York, the University of California-San Francisco, and the participating schools for supporting the work.
Author Contributions
All authors made a significant contribution to the work reported, that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The National Institute of Mental Health (NIMH) funded the study under Award Number 1R01MH113486-01 (PI: Fred M. Ssewamala, PhD).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Gniewosz G, Gniewosz B. Psychological adjustment during multiple transitions between childhood and adolescence. J Early Adolescence. 2020;40(4):566–598. doi:10.1177/0272431619858422
2. Ssemata AS, Ndekezi D, Kansiime C, et al. Understanding the social and physical menstrual health environment of secondary schools in Uganda: a qualitative methods study. PLOS Global Public Health. 2023;3(11):e0002665. doi:10.1371/journal.pgph.0002665
3. Miiro G, Rutakumwa R, Nakiyingi-Miiro J, et al. Menstrual health and school absenteeism among adolescent girls in Uganda (MENISCUS): a feasibility study. BMC Women’s Health. 2018;18:1–13. doi:10.1186/s12905-017-0502-z
4. Jmp U; WHO. Consultation on Draft Long List of Goal, Target and Indicator Options for Future Global Monitoring of Water, Sanitation and Hygiene. 2012.
5. WorldBank. Menstrual Health and Hygiene. 2022. Available from: https://www.worldbank.org/en/topic/water/brief/menstrual-health-and-hygiene.
6. WHO. Global report reveals major gaps in menstrual health and hygiene in schools. 2024. Available from: https://www.who.int/news/item/28-05-2024-global-report-reveals-major-gaps-in-menstrual-health-and-hygiene-in-schools.
7. Van Eijk AM, Sivakami M, Thakkar MB, et al. Menstrual hygiene management among adolescent girls in India: a systematic review and meta-analysis. BMJ Open. 2016;6(3):e010290. doi:10.1136/bmjopen-2015-010290
8. Tamiru S, Mamo K, Acidria P, Mushi R, Ali CS, Ndebele L. Towards a sustainable solution for school menstrual hygiene management: cases of Ethiopia, Uganda, South-Sudan, Tanzania, and Zimbabwe. Waterlines. 2015;2015:92–102.
9. Mucherah W, Thomas K. Reducing barriers to primary school education for girls in rural Kenya: reusable pads’ intervention. Int J Adolescent Med Health. 2019;31(3):20170005.
10. Montgomery P, Ryus CR, Dolan CS, Dopson S, Scott LM. Sanitary pad interventions for girls’ education in Ghana: a pilot study. PLoS One. 2012;7(10):e48274. doi:10.1371/journal.pone.0048274
11. Strine TW, Chapman DP, Ahluwalia IB. Menstrual-related problems and psychological distress among women in the United States. J Women’s Health. 2005;14(4):316–323. doi:10.1089/jwh.2005.14.316
12. Handy AB, Greenfield SF, Yonkers KA, Payne LA. Psychiatric symptoms across the menstrual cycle in adult women: a comprehensive review. Harvard Rev Psychiatry. 2022;30(2):100–117. doi:10.1097/HRP.0000000000000329
13. Zhao S, Wu W, Kang R, Wang X. Significant increase in depression in women with primary dysmenorrhea: a systematic review and cumulative analysis. Front Psychiatry. 2021;12:686514. doi:10.3389/fpsyt.2021.686514
14. Padda J, Khalid K, Hitawala G, et al. Depression and its effect on the menstrual cycle. Cureus. 2021;13(7):1.
15. Jacquelyn NJ, Sinha A. Menstrual pain, depression, anxiety and stress among women. Int J Indian Psychol. 2023;11(2):1.
16. Xi’an J. Depression increases risk of menstrual pain. 2024.
17. Weyand AC, Fitzgerald KD, McGrath M, et al. Depression in female adolescents with heavy menstrual bleeding. J Pediatr. 2022;240:171–176. doi:10.1016/j.jpeds.2021.09.007
18. Sommer M, Mason DJ. Period poverty and promoting menstrual equity. Ame Med Assoc. 2021;2021:e213089–e213089.
19. Cardoso LF, Scolese AM, Hamidaddin A, Gupta J. Period poverty and mental health implications among college-aged women in the United States. BMC Women’s Health. 2021;21(1):1–7. doi:10.1186/s12905-020-01149-5
20. Marí-Klose M, Julià A, Escapa S, Gallo P. Period poverty and mental health in a representative sample of young women in Barcelona, Spain. BMC Women’s Health. 2023;23(1):201. doi:10.1186/s12905-023-02328-w
21. Muhaidat N, Karmi JA, Karam AM, Abushaikha F, Alshrouf MA. Period poverty, reuse needs, and depressive symptoms among refugee menstruators in Jordan’s camps: a cross-sectional study. BMC Women’s Health. 2024;24(1):384. doi:10.1186/s12905-024-03193-x
22. Rohatgi A, Dash S. Period poverty and mental health of menstruators during COVID-19 pandemic: lessons and implications for the future. Front Global Women’s Health. 2023;4:1128169. doi:10.3389/fgwh.2023.1128169
23. Caruso BA, Cooper HL, Haardörfer R, et al. The association between women’s sanitation experiences and mental health: a cross-sectional study in Rural, Odisha India. SSM-Population Health. 2018;5:257–266. doi:10.1016/j.ssmph.2018.06.005
24. Rapp A, Kilpatrick S. Changing the cycle: period poverty as a public health crisis. University of Michigan School of Public Health: Ann Arbor; 2020
25. Mohamed Y, Durrant K, Huggett C, et al. A qualitative exploration of menstruation-related restrictive practices in Fiji, Solomon Islands and Papua New Guinea. PLoS One. 2018;13(12):e0208224. doi:10.1371/journal.pone.0208224
26. Ians. How period taboo impacts girl child’s mental health. 2022. Available from: https://www.onmanorama.com/lifestyle/women/2022/12/16/period-taboo-impacts-girl-child-mental-health.html.
27. Rossouw L, Ross H. An economic assessment of menstrual hygiene ProductTax cuts. Gates Open Res. 2020;4(137):137.
28. Achuthan K, Khobragade S, Kolil VK. Beyond access to sanitary pads: a comprehensive analysis of menstrual health scheme impact among rural girls in Northeast India. Health Policy Plann. 2025;40(2):218–233. doi:10.1093/heapol/czae117
29. Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196(4286):129–136. doi:10.1126/science.847460
30. Silvestris E, De Pergola G, Rosania R, Loverro G. Obesity as disruptor of the female fertility. Reprod Biol Endocrinol. 2018;16:1–13. doi:10.1186/s12958-018-0336-z
31. Fahs B. There will be blood: women’s positive and negative experiences with menstruation. Women’s Reprod Health. 2020;7(1):1–16. doi:10.1080/23293691.2019.1690309
32. WHO. Adolescent and young adult health. 2024. Available from: https://www.who.int/news-room/fact-sheets/detail/adolescents-health-risks-and-solutions.
33. WHO. Mental health of adolescents. 2024. Available from: https://www.who.int/news-room/fact-sheets/detail/adolescent-mental-health.
34. UN. UN health agency reports depression now ‘leading cause of disability worldwide. 2017. Available from: https://news.un.org/en/story/2017/02/552062#:~:text=Depression%20is%20the%20leading%20cause,young%20people%20and%20the%20elderly.
35. WHO. Depressive disorder (depression). 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/depression#:~:text=An%20estimated%203.8%25%20of%20the,among%20women%20than%20among%20men.
36. Miller AP, Kintu M, Kiene SM. Challenges in measuring depression among Ugandan fisherfolk: a psychometric assessment of the Luganda version of the Center for Epidemiologic Studies Depression Scale (CES-D). BMC Psychiatry. 2020;20:1–13. doi:10.1186/s12888-020-2463-2
37. WHO. Depression and Other Common Mental Disorders: global Health Estimates. Available from: https://apps.who.int/iris/bitstream/handle/10665/254610/WHO-MSD-MER-2017.2-eng.pdf. (PDF, 1.63MB).
38. Kagaari J. Mental health in Uganda Many people in low- and middle-income countries face daily challenges, and their mental health has been additionally burdened by COVID-19. 2021. Available from: https://www.apa.org/international/global-insights/uganda-mental-health.
39. Nalugya-Sserunjogi J, Rukundo GZ, Ovuga E, Kiwuwa SM, Musisi S, Nakimuli-Mpungu E. Prevalence and factors associated with depression symptoms among school-going adolescents in Central Uganda. Child Adolescent Psychiatry Mental Health. 2016;10:1–8. doi:10.1186/s13034-016-0133-4
40. Kinyanda E, Kizza R, Abbo C, Ndyanabangi S, Levin J. Prevalence and risk factors of depression in childhood and adolescence as seen in 4 districts of north-eastern Uganda. BMC Int Health Human Rights. 2013;13:1–10. doi:10.1186/1472-698X-13-19
41. Kigozi F, Ssebunnya J, Kizza D, Cooper S, Ndyanabangi S. An overview of Uganda’s mental health care system: results from an assessment using the world health organization’s assessment instrument for mental health systems (WHO-AIMS). Int J Mental Health Systems. 2010;4(1):1–9. doi:10.1186/1752-4458-4-1
42. Nabwera HM, Shah V, Neville R, et al. Menstrual hygiene management practices and associated health outcomes among school-going adolescents in rural Gambia. PLoS One. 2021;16(2):e0247554. doi:10.1371/journal.pone.0247554
43. Ssesanga T, Thomas KA, Nelson KA, et al. Understanding menstrual factors associated with poor mental health among female secondary school students in Uganda: a cross-sectional analysis. Child Adolescent Psychiatry Mental Health. 2024;18(1):129. doi:10.1186/s13034-024-00829-6
44. Filiatreau LM, Tutlam N, Brathwaite R, et al. Effects of a combination economic empowerment and family strengthening intervention on psychosocial well-being among ugandan adolescent girls and young women: analysis of a cluster randomized controlled trial (Suubi4Her). J Adolesc Health. 2023;72(5):S33–S40. doi:10.1016/j.jadohealth.2022.11.250
45. Ssewamala FM, Bermudez LG, Neilands TB, et al. Suubi4Her: a study protocol to examine the impact and cost associated with a combination intervention to prevent HIV risk behavior and improve mental health functioning among adolescent girls in Uganda. BMC Public Health. 2018;18(1):1–11. doi:10.1186/s12889-018-5604-5
46. Brathwaite R, Namuwonge F, Magorokosho N, et al. Impact of economic and family intervention on adolescent girls’ education performance, school absenteeism, and behavior in school: the suubi4her study. J Adolesc Health. 2024;74(2):340–349. doi:10.1016/j.jadohealth.2023.08.043
47. Karimli L, Nabunya P, Ssewamala FM, Dvalishvili D. Combining asset accumulation and multifamily group intervention to improve mental health for adolescent girls: a cluster-randomized trial in Uganda. J Adolesc Health. 2024;74(1):78–88. doi:10.1016/j.jadohealth.2023.08.012
48. Namuwonge F, Kizito S, Ssentumbwe V, et al. Culture, self-esteem and menstrual hygiene management among adolescent girls in Uganda: the impact of economic and family strengthening. BMC Women’s Health. 2025;25(1):1–14. doi:10.1186/s12905-025-03778-0
49. Hayes RJ, Moulton LH. Cluster Randomised Trials. Chapman and Hall/CRC; 2017.
50. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. 1961;4(6):561–571. doi:10.1001/archpsyc.1961.01710120031004
51. Chandra-Mouli V, Patel SV. Mapping the knowledge and understanding of menarche, menstrual hygiene and menstrual health among adolescent girls in low-and middle-income countries. The Palgrave Handbook of Critical Menstruation Studies. 2020;609–636.
52. Long JL, Haver J, Mendoza P, Vargas Kotasek SM. The more you know, the less you stress: menstrual health literacy in schools reduces menstruation-related stress and increases self-efficacy for very young adolescent girls in Mexico. Front Global Women’s Health. 2022;3:859797. doi:10.3389/fgwh.2022.859797
53. Hennegan J. Interventions to improve menstrual health in low-and middle-income countries: do We know what works? In: The Palgrave Handbook of Critical Menstruation Studies. 2020:637–652.
54. Uzoechi CA, Parsa AD, Mahmud I, Alasqah I, Kabir R. Menstruation among in-school adolescent girls and its literacy and practices in Nigeria: a systematic review. Medicina. 2023;59(12):2073. doi:10.3390/medicina59122073
55. Munro AK, Keep M, Hunter EC, Hossain SZ. Confidence to manage menstruation among university students in Australia: evidence from a cross-sectional survey. Women’s Health. 2022;18:17455065211070666. doi:10.1177/17455065211070666
56. McHugh MC. Menstrual shame: exploring the role of ‘menstrual moaning’. In: The Palgrave Handbook of Critical Menstruation Studies. 2020:409–422.
57. Ayieko P, Torondel B, Renju J, et al. A multifaceted menstrual health intervention to improve psychosocial outcomes and menstrual practices among secondary schoolgirls in Northwest Tanzania: a pilot intervention study. BMC Women’s Health. 2025;25(1):190. doi:10.1186/s12905-025-03723-1
58. Phillips-Howard PA, Nyothach E, Ter Kuile FO, et al. Menstrual cups and sanitary pads to reduce school attrition, and sexually transmitted and reproductive tract infections: a cluster randomised controlled feasibility study in rural Western Kenya. BMJ Open. 2016;6(11):e013229. doi:10.1136/bmjopen-2016-013229
59. Hennegan J, Montgomery P. Do menstrual hygiene management interventions improve education and psychosocial outcomes for women and girls in low and middle income countries? A systematic review. PLoS One. 2016;11(2):e0146985. doi:10.1371/journal.pone.0146985
60. Li Y, Kang B, Zhao X, Cui X, Chen J, Wang L. Association between depression and dysmenorrhea among adolescent girls: multiple mediating effects of binge eating and sleep quality. BMC Women’s Health. 2023;23(1):140. doi:10.1186/s12905-023-02283-6
61. UK PI. Break the Barriers: girls’ Experiences of Menstruation in the UK. 2018. Available from: https://plan-uk.org/file/plan-uk-break-the-barriers-report-032018pdf/download?token=Fs-HYP3v.
62. Health–Americas TLR. Menstrual health: a neglected public health problem. Lancet Reg Health-Americas. 2022;15:100399. doi:10.1016/j.lana.2022.100399
63. Benshaul-Tolonen A, Zulaika G, Nyothach E, et al. Sanitary Products, Absenteeism and Psychosocial Well-Being: Evidence From a Three-Arm Cluster Randomized Controlled Feasibility Study in Western Kenya. Columbia, SIPA: Center for Development Economics and Policy; 2021.
64. Byansi W, Ssewamala FM, Neilands TB, et al. The short-term impact of a combination intervention on depressive symptoms among school-going adolescent girls in Southwestern Uganda: the Suubi4Her cluster randomized trial. J Adolesc Health. 2022;71(3):301–307. doi:10.1016/j.jadohealth.2022.04.008
65. Ssewamala FM, Han C-K, Neilands TB. Asset ownership and health and mental health functioning among AIDS-orphaned adolescents: findings from a randomized clinical trial in rural Uganda. Soc sci med. 2009;69(2):191–198. doi:10.1016/j.socscimed.2009.05.019
66. Wang Y-P, Gorenstein C. Assessment of depression in medical patients: a systematic review of the utility of the Beck Depression Inventory-II. Clinics. 2013;68:1274–1287. doi:10.6061/clinics/2013(09)15
67. Lewis G, Neary M, Polek E, Flouri E, Lewis G. The association between paternal and adolescent depressive symptoms: evidence from two population-based cohorts. Lancet Psychiatry. 2017;4(12):920–926. doi:10.1016/S2215-0366(17)30408-X
68. Nabunya P, Damulira C, Byansi W, et al. Prevalence and correlates of depressive symptoms among high school adolescent girls in southern Uganda. BMC Public Health. 2020;20:1–11. doi:10.1186/s12889-020-09937-2
69. Patton GC, Sawyer SM, Santelli JS, et al. Our future: a Lancet commission on adolescent health and wellbeing. Lancet. 2016;387(10036):2423–2478.
70. Cheung ESL, Mui AC. Gender variation and late-life depression: findings from a national survey in the USA. Ageing International. 2023;48(1):263–280. doi:10.1007/s12126-021-09471-5
71. Giles-Hansen C, Mugambi G, Machado A. Experiences from East Africa and lessons in addressing the menstrual hygiene needs of women and girls. Waterlines. 2019;38(3):1.
72. Sidle AA, Suedi A, Schwarz H, Swai M-Z, Kafanabo E, Oulo B. ‘She has become Brave:’the role of menstrual health education in building girls’ agency. Int J Adolesc Youth. 2025;30(1):2467116. doi:10.1080/02673843.2025.2467116
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.