Back to Journals » Patient Preference and Adherence » Volume 18
Beyond the Burden: A Qualitative Inquiry into the Experiences of Chinese Informal Caregivers for People Living with HIV or AIDS
Authors Zhang Y, Liu M, Han J, Tian X, Xin Y
Received 12 December 2023
Accepted for publication 11 March 2024
Published 15 March 2024 Volume 2024:18 Pages 677—685
DOI https://doi.org/10.2147/PPA.S454590
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Ying Zhang,1 Mingyuan Liu,2 Jing Han,3 Xin Tian,4 Youqing Xin5
1School of Public Health, Capital Medical University, Beijing, 100069, People’s Republic of China; 2Department of Vascular Surgery, Beijing Friendship Hospital, Capital Medical University, Beijing, 100050, People’s Republic of China; 3Department of Beijing Home of Red Ribbon, Beijing Ditan Hospital, Capital Medical University, Beijing, 100102, People’s Republic of China; 4Administrative office of hospital, Beijing Ditan Hospital, Capital Medical University, Beijing, 100102, People’s Republic of China; 5Administrative Office of Hospital, Beijing Friendship Hospital, Capital Medical University, Beijing, 100050, People’s Republic of China
Correspondence: Xin Tian, Administrative office of hospital, Beijing Ditan Hospital, Capital Medical University, No. 8 Jingshun Dong Street, Chaoyang District, Beijing, 100102, People’s Republic of China, Email [email protected] Youqing Xin, Administrative office of hospital, Beijing Friendship Hospital, Capital Medical University, No. 95 Yongan Road, Xicheng District, Beijing, 100050, People’s Republic of China, Email [email protected]
Purpose: Informal caregivers are defined as families or close friends of patients, which take considerable responsibilities for providing care to people living with HIV/AIDS (PLWHA). Although there have been a number of studies in caregiver of PLWHA, research studies that sought to quantify the effects of informal caregiving for the caregivers failed to successfully provide empirical understanding of the nature of caregiving experience. Therefore, this study adopted a qualitative approach to explore the experiences and feelings of caregivers of PLWHA during the long-term care process.
Methods: The qualitative study was conducted in August 2023 in Beijing, China. Data were collected through individual in-depth semi-structured interviews with informal caregivers of PLWHA. Theme analysis was used to identify themes from the interview transcripts.
Results: A total of 21 participants were recruited into our study, 16 were family members of PLWAHA, and 5 were homosexual lover or close friend of PLWHA. Three major themes and ten sub themes were identified by thematic analysis: (1) care burden experience (including 5 sub-themes: negative emotional experience, psychological burden, economic burden, physical health loss and limitation of social interaction); (2) benefit findings from care (including 3 sub-theme: positive emotional experience, perceived social support, health promotion); (3) Demands for caregiving capacity (including 2 sub-theme: inadequate caregiving capacity and inadequate psychological comfort capacity).
Conclusion: This qualitative study provides a comprehensive exploration of the experiences faced by informal caregivers of PLWHA in China, uncovering the complex spectrum of psychological, physical, social, and economic challenges inherent in their caregiving roles, while predominantly challenging, caregivers also reported personal growth, increased social support, and emotional fulfillment. The research results could help in developing effective interventions to reduce the caregiver burden and improve their mental health.
Keywords: people living with HIV/AIDS, caregiver, care experience, care burden, benefit findings, qualitative research
A Letter to the Editor has been published for this article.
Introduction
The acquired immune deficiency syndrome (AIDS) is a highly harmful infectious disease caused by the human immunodeficiency virus (HIV).1 It is also a great public health challenge worldwide. According to world health organization (WHO), there were an estimate 39.0 million people living with HIV at the end of 2022, and 630,000 people died from HIV-related causes in 2022.2 In China, there were 107,000 new reported cases of HIV/AIDS, with 30,000 reported deaths and 1.3 million reported living case by the end of 2022.3 With the widespread availability of anti-retro-viral therapy, the mortality and disability rates of AIDS have been effectively controlled, and rendering it a chronic, manageable disease like hypertension and diabetes.4 Thus, patients living with HIV/AIDS (PLWHA) may require long-term care from themselves, healthcare professionals, and informal caregivers.
Healthcare service provide only limited care and support to PLWHA, leaving a substantial amount of work to their informal caregivers.5 An informal caregiver is defined as individuals who are unpaid and provide non-professional care for patients, always be family members, friends, couple of patients.6 In China, informal caregivers, particularly family caregivers, take considerable responsibilities for providing care to PLWHA.7 They provide health-related, psychosocial and physical care for PLWHA, such as accompanying relatives to hospitals, administering medication, encouraging and spending time with PLWHA, cooking, bathing, and washing.8 They are the primary source of social support for PLWHA, and can improve medicine adherence of PLWHA.9 However, the long-term responsibility for providing care to PLWHA place significant burden on informal caregivers.
In addition, HIV/AIDS is always associated with evil and dirty behaviors in society, so discrimination and stigma are almost inevitable among PLWHA.10 However, social discrimination not only cause psychological distress to PLWHA, but also impose psychological pressure on their caregivers. It is reported that 47% of the caregivers for PLWHA perceived stigma, which impeded both patients and family members to participate in social activities.11 Besides, Khan’s study reported that 46% of PLWHA’s caregivers have depression symptoms, 27% have anxiety symptoms, most of them were stressed.12 The psychological distress is not only detrimental to the physical and mental health of caregivers but also to the quality of caring PLWHA.13
Therefore, it is necessary to investigate the real experience and feelings of informal caregivers of PLWHA. But in China most of the current researches on care experience of informal caregivers of PLWHA are quantitative in nature,7,14 which may appear insufficient for understanding informal caregivers’ lived experiences and perceptions. However, a qualitative approach would provide a more nuanced understanding of the caregivers’ perspectives.15 Hence, this study adopts a qualitative approach to understand caregivers’ caring experiences and feelings, aimed at understand and analyze the specific content of care experience beyond Chinese culture. We hope that the results will provide some insights for care experience of PLWHA’s informal caregivers, and provide theoretical basis for development of intervention measures.
Materials and Methods
Study Design and Ethical Considerations
This was qualitative research conducted in the infectious disease outpatient clinics and wards of a tertiary hospital in Beijing, China. All procedures of this study were in accordance with ethical standards of the institutional research committee and the Helsinki Declaration. Verbal informed consent was obtained from participants before interview.
Participants and Procedures
The data were collected from 2 August to 30 August 2023. We used a convenience sampling to recruit participants. The inclusion criteria for participants included: (1) aged 18 years old or older; (2) undertaking the main caregiving responsibility of the PLWHA; (3) be able to communicate in mandarin; (4) be willing to participate in this study. The exclusion criteria for participants included: (1) professional caregivers receiving salary; (2) with serious physical or mental illnesses, such as cancer and depression; (3) caregivers of new diagnosed PLWHA; (4) be unwilling to participate in interviews. The targeted number of participants of 20–25 was estimated to reach data saturation.16
Data Collection
The study activities were conducted in a separate room at the clinics of hospital. Demographic information collected included age, sex, educational background, relationship with PLWHA, HIV infectious condition, duration of care. The qualitative in-depth interviews were conducted by researchers. An interview guide was used to facilitate conversation around the participant’s experience on caring PLWHA. The interview guide was developed by the study team based on a thorough literature review and pilot testing. The interview lasted from 20 to 60 min. All of the interviews were audio recorded with the interviewees’ consent, then transcribed verbatim.
Data Analysis
Qualitative analyses of interviews were conducted by means of a thematic analysis approach. Transcriptions, coding, and analyses in this study were completed in Mandarin, and results in this study were translated to English for manuscript preparation. Thematic analysis identified themes within the transcription data through a set of standardized steps: (1) the researchers familiarized themselves with the data by reading transcript multiple times and listening to audiotapes; (2) using deductive and inductive methods, codes were generated according to things that appeared meaningful and identified any possible themes. These themes were reviewed, named, and identified as experience and feelings of caregiver of PLWHA. All analyses were conducted by researchers through NVivo qualitative data analysis software.
Results
Characteristics of Participants
A total of 21 caregivers of PLWHA participated in the study, including 14 (66.7%) females and 7 (33.3%) males. Caregivers’ age ranged from 24 to 69 years, with a mean age of 44.14 (SD 13.02) years. Most of them (16, 76.2%) were family members of PLWHA. and 13 (61.9%) of participants have high school and below educational background. Almost of them (19, 90.5%) were HIV-negative. The specific sociodemographic characteristics of the participants are shown in Table 1.
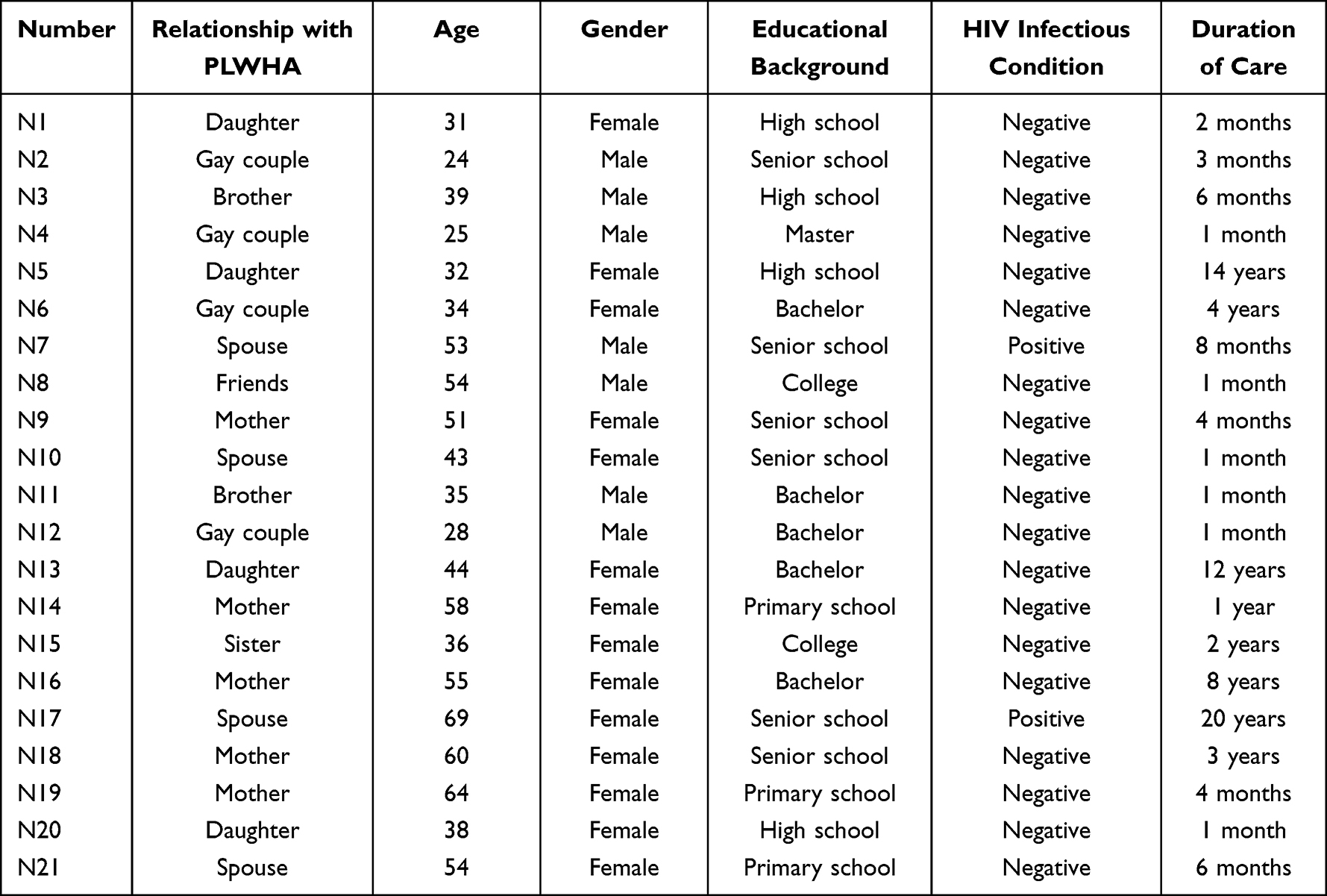 |
Table 1 Demographic Characteristics of Caregivers of PLWHA (N=21) |
The Framework of Thematic Analysis
Thematic analysis of the interviews revealed three major themes and ten sub-themes, including care burden experience, benefit findings from care, demands for caregiving capacity. The specific contents were presented in Table 2.
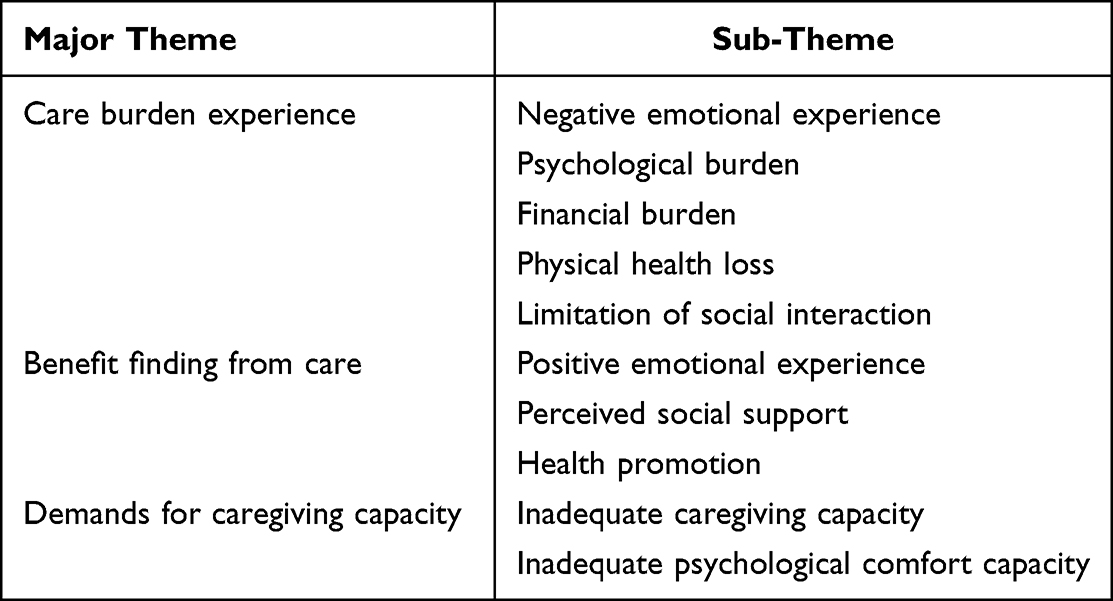 |
Table 2 Themes of Caregivers’ Interviews |
Care Burden Experience
Negative Emotional Experience
When participants were faced with HIV/AIDS diagnosis, they experience various emotions such as shock, disbelief, collapse, fear, and sadness and other feelings of psychological distress. And then during the long-term care, caregivers were prone to mental distress such as anxiety and depression.
(N1) “After staying two days at the China-Japan Friendship Hospital, he was diagnosed with HIV. I was so surprised and feel unbelievable.” (N8) “I didn’t dare to think about it, when I heard this news, I thought that his life would be over, so those two days were very devastating.”
Something different about HIV/AIDS is that participants mentioned feeling repressed and resentful sometimes due to the fear of social discrimination and internalized stigma.
(N13) “There is one confusion that this disease is still an infectious disease after all, and it may not be able to talk to others, so I feel that it has been quite depressing for so many years”.
In addition, most participants reported that their emotional experiences throughout the caregiving process were constantly fluctuating. These experiences not only mirrored the patient’s emotions but also shifted with the patient’s physical conditions. Furthermore, these emotional experiences tended to gradually stabilize as the illness progressed.
(N1) “If my dad’s in a good mood, then I’m in a much better mood.” (N15) “When I take his temperature and find it within the normal range, I experience a sense of relief. However, if the temperature is slightly elevated, I begin to feel apprehensive. (N10)”
Initially, I found it challenging, but I later realized that it bore resemblance to chronic conditions such as hypertension and diabetes, which necessitate prolonged treatment. Consequently, my mental stress significantly decreased.”
Psychological Burden
During the long-term care process, most participants mentioned that experiencing significant psychological stress, stemming from fear of infection, concerns about potential discrimination, worries about the progression of patient’s illness and future prospects, and anxiety about the patient’s psychological well-being. Additionally, they expressed concerns that public stigma associated with HIV/AIDS might impact their own future as well as other family members, leading to feelings of anxiety and worry.
(N2) “When I heard this news, my first thought was fear that I might get infected.” (N15)“I don’t want his classmates and friends to know about his illness.”(N6) “I’m worried that as he gets older, AIDS will cause an increase in other illnesses and his resistance will be lower than that of normal people.” (N14) “I’m almost 60 years old and my health is not good anymore. If I were to die one day, who would take care of him?”
Economic Burden
The majority of participants stated that they encounter significant financial pressure when caring for PLWHA. This pressure originates from two primary sources: the fear of unpredictable future medical expenses and the fear of losing financial resources.
(N2) “This chronic disease, even if cured this time, will always cost money in the future.” (N5) “My husband and me were both working and earning an income, but now that I’m here full time with my father, that financial income has definitely been cut in half”.
Physical Health Loss
Some of the participants mentioned that their health had deteriorated considerably since caring for PLWHA, mainly in terms of decreased sleep quality, weight loss, and lack of energy.
(N2) “I can’t sleep well at night, and then I feel tired all day. It’s like a never-ending cycle.” (N1) “When he was hospitalized, I had to take care of him 24 hours a day and my physical strength couldn’t quite keep up.”
Limitation of Social Interaction
Several participants mentioned that they may have overlooked other family members while caring for PLWHA, which could have a negative impact on their relationships with them. Additionally, PLWHA in the chronic disease stage often struggle to independently care for themselves, thus relying heavily on caregivers. This dependency can impede caregivers’ social interactions with friends. PLWHA require regular visits to medical facilities for medication and physical examinations. Some participants noted that these demands disrupt their usual work schedule.
(N5) “If I come here to care for my father, I will neglect my own family, I can only focus on one thing at a time.“ (N16) “ After finishing previous work, I used to relax with colleagues or classmates. But now, I have less energy. All of my time is spent on my children, and I no longer attend social gatherings. ” (N2) ”I work in another city, but if he gets sick, I will have to come here to care for him. It’s not easy for me to take time off work.”
Benefit Finding from Care
Positive Emotional Experience
In addition to negative emotional experiences, some participants expressed positive emotions such as intimacy, optimism and hope that they had not previously experiences.
(N16) “I also firmly believe that he will get better. Now, I have the same mindset even though the journey has been quite tough. Anyway, I haven’t given up.” (N13) “I’m really thankful that my dad has been sick for so many years because it gave me the opportunity to take care of him, and I feel really content with that.”
Perceived Social Support
Long-term care process was very painful for caregivers, but some participants pointed out that support from family, friends, medical staff and social worker can alleviate all psychological discomfort. In addition, some participants mentioned that the“Four Frees and One Care”policy, which was the Chinese government implemented in 2003, significantly alleviate the pressure on drug treatment.
(N16) “When he was first diagnosed, I felt very disheartened and sought advice at the Red Ribbon House. With the support and guidance of the volunteers, I began to feel calm and gradually accepted the fact that he was ill”. (N5) “Now, the government’s care policy for AIDS patients is really good. You can easily get medication and medical consultations in our city, and the service is also quite thoughtful”.
Health Promotion
Health promotion have 2 aspects, including health education promotion and health behavior promotion. Some participants indicated that this was the first time they had learned about AIDS. But because of the demands of caring PLWHA, they voluntarily acquired a little of knowledge related to AIDS. Furthermore, many participants reported awareness of protective measures when interacting with patients in their daily activities, and actively engaged in HIV screening.
(N10) “When he got this illness, I searched a lot of knowledge about AIDS through internet.” (N15) “If we touch his blood or even a cut on his skin, we always wear gloves.”
Demands for Caregiving Capacity
Inadequate Caregiving Capacity
Because of lack of understanding of transmission approaches and symptom management of AIDS, part of participants indicated that they always feel overwhelmed.
(N1) “Because I haven’t taken care of any other patients, I have no idea what to do.” (N12) “I need to know how to avoid getting infected in daily life because I have no idea how to do it right.”
Inadequate Psychological Comfort Capacity
PLWHA always suffered from common psychological issues like depression, hopelessness, anger and sleeplessness after AIDS diagnosis. However, caregivers were not prepared for this. Some participants indicated that they do not know how to communicate with PLWHA or how to deal with the adverse emotions.
(N11) “Then, I do not know how to persuade him or how to assist him.” (N16) “Sometimes I’m scared to talk to him because I’m worried he might have negative emotions, but I don’t know how to help him chill out.”
Discussion
This qualitative study explores the experiences and feelings of caregivers for PLWHA in China, aiming to enhance our understanding of their unique challenges and needs. To our knowledge, our study is the first to explore the caring experiences of caregivers for PLWHA in China with a qualitative approach. Three main themes were identified through the extraction and summarization of interview texts. Based on the analysis of these themes, we revealed that the caregiving experience, while predominantly challenging, also offers opportunities for positive transformation.
This study found that informal caregivers endure physical, psychological, social, and economic pressures during the caregiving process, constituting a multifaceted care burden, which was consisted with the previous researches.17,18 Our study found that the psychological burden was the most significant encounter among the four dimensions of care burden, and it was also the burden most frequently reported by the participants. This result may be attributed to the young age of the care recipients in this study. A previous study conducted by Monteiro et al have proved that informal caregiver’s psychological stress is higher when the care recipient is younger.19 Similar to informal caregivers of other disease, caregivers of PLWHA experience significant negative emotions at the beginning of the disease diagnosis. And as time was prolonged, they gradually learned to accept the consequences and adjust to life changes during the caring process.20 However, the different is that the caregiver of PLWHA always experienced significant internalized stigma throughout their whole caring process. They often become reluctant to communicate, increasing feelings of loneliness, which can lead to mental health issues such as anxiety and depression.21,22 In addition, our study found that caregivers with no comprehensive HIV and AIDS knowledge always experience higher psychological burden, which is also similar to other studies.17 Such as, some participants with low educational background mentioned that they always suffered from the fear of being infected during the caring process.
Previous study indicated that the more patients spent on their illness monthly, the worse quality of life of informal caregivers, in particular the population with low income and lack of medical security.23 This result was similar to our study. It is well-known that PLWHA require lifelong therapy with combinations of antiretroviral drugs, necessitating substantial economic resources. And caregivers had to pay medical expense and support the family while caring for PLWHA. Thus, it is unsurprising that most caregivers experience an economic burden. Interestingly, researchers found that participants rarely use the term “burden” when describing their caring experiences, besides economic burden. This phenomenon may be related to Chinese social and cultural background which is deeply rooted in Confucian values. Caring for patients is viewed as both a filial obligation and social responsibility.24
In contrast to other studies, few participants in ours mentioned physical burden, which might correlate with the caregivers’ age and health status in our sample. Some studies have revealed that the age of caregivers increase and the caring burden increase.25 And the older usually suffered from multiple disease and has poor health condition.26 However, most caregivers included in this study were mid-aged, with good self-related health condition. Nevertheless, some participants reported suffering from sleep disturbances. Due to lack sufficient sleep, they may have a greater feeling of tiredness and loss of energy during the caring process, which can clearly have an impact on quality of care.
Informal caregivers are required to dedicate a significant amount of time and energy to accompanying PLWHA, particularly during the AIDS period, to prevent accidents from occurring. According to a previous study, among the informal caregivers of hospitalized patients, 70.7% of them spend more than 8 hours daily accompanying the patients, resulting in a decrease in both leisure time and activity time.27 The caregivers of PLWHA in this study also mentioned that they became estranged from other family members and friends after the commencement of the caregiving process. However, the reduction of social connections leads to the social isolation, which lead to the physical and psychological exhaustion of caregivers.28
Besides negative care burden experiences, some participants reported benefit findings, including perceived social support, personal growth, emotional fulfillment and so on. Our study suggested that exploring the benefit findings may be helpful for alleviate the negative care burden experiences of caregivers, which is consistent with previous study.17 Such as, caregivers of our study often seek the meaning of care role through caregiving activities, such as responsibility, filial piety, and emotional connection, and they transform this role meaning into internal motivation and caregiving energy to achieve self-worth and gain a sense of satisfaction from caregiving experience. This result suggested that we should pay attention to caregivers’ evaluation of their caregiving role, and help them realize their importance to patients and families, seeking the possibility of maintaining or enhancing their caregiving motivation from the inner level. Meanwhile, perceived social support plays an important role in caring process, which means that we need to understand how to maximize the full effectiveness of social support. Due to the unique nature of AIDS, most patients and their caregivers are reluctant to disclose their HIV status to others.16 Medical institutions are one of the few places where PLWHA and their caregivers are willing to openly disclose their status.29 It is important to further integrate social support into medical services, expand traditional medical concepts and service areas.
Limitation
There are some limitations of this study. Firstly, this study only conducted in one hospital in Beijing, although this is a reference center that attends to participants from very diverse urban, rural and socioeconomic backgrounds. Secondly, because of the long duration of this interview, most of the interviewees were caregivers of hospitalized patients. The patients’ condition may be more severe. Lastly, only caregivers who agreed to participate in the study were interviewed, some potential participants with a history of particular disorders were excluded.
Conclusion
This study utilized a qualitative research approach to delve deeply into the genuine experiences and feelings of informal caregivers of PLWHA. It not only described the enormous psychological, physical, economic, and social stresses that caregivers bear, but also captured some of the positive experiences that caregivers derived from the caregiving process. However, the study also found that the caregivers’ need for disease-related care and psychological counseling knowledge cannot be satisfied. Therefore, this study suggests that while focusing on PLWHA, we should also pay attention their informal caregivers. And we advocate for a balanced understanding of the caregiver’s plight, advocating for policies that recognize and support their dual experience of burden and resilience.
Abbreviations
HIV, Human Immunodeficiency Virus; AIDS, Acquired Immune Deficiency Syndrome; PLWHA, People Living with HIV/AIDS; WHO, World Health Organization.
Data Sharing Statement
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
All participants were explained the purpose of this study and provided their verbal informed consent, and participants were only included in this research if consenting to publication of anonymized responses. The Ethics committee of Beijing Ditan Hospital, Capital Medical University approved this study (including verbal informed consent process).
Acknowledgments
We would like to thank all the caregivers who voluntarily participated in this study and research assistants who performed the data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dieleman JL, Haakenstad A, Micah A. Spending on health and HIV/AIDS: domestic health spending and development assistance in 188 countries, 1995-2015. Lancet. 2018;391(10132):1799–1829. doi:10.1016/S0140-6736(18)30698-6
2. World Health Organization. HIV/AIDS. Available from: https://www.who.int/en/news-room/fact-sheets/detail/hiv-aids.
3. Chines Center for Disease Control and Prevention. The data-center of China Public Health Science. Available from: https://www.phsciencedata.cn/Share/ky_sjml.jsp?id=c2ca694e-3995-4c7f-9078-3ed0aaf14556.
4. Simon V, Ho DD, Karim QA. HIV/AIDS epidemiology, pathogenesis, prevention, and treatment. Lancet. 2006;368(9534):489–504. doi:10.1016/S0140-6736(06)69157-5
5. Ntuli M, Madiba S. The Burden of Caring: an Exploratory Study of the Older Persons Caring for Adult Children with AIDS-Related Illnesses in Rural Communities in South Africa. Int J Environ Res Public Health. 2019;16(17):3162. doi:10.3390/ijerph16173162
6. Adelman RD, Tmanova LL, Delgado D, Dion S, Lachs MS. Caregiver Burden A Clinical Review. JAMA J Am Med Assoc. 2014;311(10):1052–1059. doi:10.1001/jama.2014.304
7. Hsieh J, Li L, Lin C, Luo S, Ji G. Spousal role and caregiver burden in HIV affected families in Anhui Province, China. AIDS Care. 2017;29(10):1270–1274. doi:10.1080/09540121.2017.1300631
8. Kyomuhendo C, Boateng A, Agyemang FA. Experiences of elderly women caring for people living with HIV and AIDS in Masindi District, Uganda. AIDS Care. 2021;33(8):993–996. doi:10.1080/09540121.2020.1832191
9. Aggarwal B, Liao M, Mosca L. Medication adherence is associated with having a caregiver among cardiac patients. Ann Behav Med. 2013;46(2):237–242. doi:10.1007/s12160-013-9492-8
10. Wu XH, Chen J, Huang HG, Liu ZP, Li XH, Wang HH. Perceived stigma, medical social support and quality of life among people living with HIV/AIDS in Hunan, China. Appl Nurs Res. 2015;28(2):169–174. doi:10.1016/j.apnr.2014.09.011
11. Singh D, Chaudoir SR, Escobar MC, Kalichman S. Stigma, burden, social support, and willingness to care among caregivers of PLWHA in home-based care in South Africa. AIDS Care. 2011;23(7):839–845. doi:10.1080/09540121.2010.542122
12. Khan R, Pai K, Kulkarni V, Ramapuram J. Depression, anxiety, stress and stigma in informal caregivers of People Living with HIV (PLHIV). AIDS Care. 2018;30(6):722–726. doi:10.1080/09540121.2017.1418831
13. Logie C, James L, Tharao W, Loutfy M. Associations Between HIV-Related Stigma, Racial Discrimination, Gender Discrimination, and Depression Among HIV-Positive African, Caribbean, and Black Women in Ontario, Canada. Aids Patient Care and Stds. 2013;27(2):114–122. doi:10.1089/apc.2012.0296
14. Song YQ, Wang H, Yin Y, et al. Caregiver Burden Among Informal Caregivers of Persons Living with HIV/AIDS in Liangshan Prefecture, China. Patient Preference Adherence. 2022;16:1027–1035. doi:10.2147/PPA.S357580
15. Mfoafo-M’Carthy M, Grischow J. Hierarchy and inequality in research: navigating the challenges of research in Ghana. Qual Res. 2022;22(5):729–742. doi:10.1177/14687941221098927
16. Aurpibul L, Tangmunkongvorakul A, Detsakunathiwatchara C, et al. Social effects of HIV disclosure, an ongoing challenge in young adults living with perinatal HIV: a qualitative study. Front Public Health. 2023;11.
17. Lin S, Wang C, Wang Q, et al. The experience of stroke survivors and caregivers during hospital-to-home transitional care: a qualitative longitudinal study. Int J Nurs Stud. 2022;130:104213. doi:10.1016/j.ijnurstu.2022.104213
18. Booker R, Bays S, Burnett L, Torchetti T. Supporting People and Their Caregivers Living with Advanced Cancer: from Individual Experience to a National Interdisciplinary Program. Semin Oncol Nurs. 2021;37(4):151169. doi:10.1016/j.soncn.2021.151169
19. Monteiro S, Fournier M, Favrod J, et al. Ability to Care for an Ill Loved One During the First COVID-19 Lockdown: mediators of Informal Caregivers’ Stress in Europe. Front Psychiatry. 2022;13:852712. doi:10.3389/fpsyt.2022.852712
20. LeSeure P, Chongkham-Ang S. The Experience of Caregivers Living with Cancer Patients: a Systematic Review and Meta-Synthesis. J Pers Med. 2015;5(4):406–439. doi:10.3390/jpm5040406
21. Montenegro MC, Abdul-Chani M, Valdez D, et al. Perceived Stigma and Barriers to Accessing Services: experience of Caregivers of Autistic Children Residing in Latin America. Res Dev Disabil. 2022;120:104123. doi:10.1016/j.ridd.2021.104123
22. Zhao Q, Huangfu C, Li J, Liu H, Tang N. Psychological Resilience as the Mediating Factor Between Stigma and Social Avoidance and Distress of Infertility Patients in China: a Structural Equation Modeling Analysis. Psychol Res Behav Manag. 2022;15:391–403. doi:10.2147/PRBM.S354803
23. Ogunnubi OP, Aina FO, Busari CO, et al. From ideation to attempt: a study of suicidality and its correlates amongst patients with schizophrenia in a resource-poor country. S Afr J Psychiatr. 2022;28:1547. doi:10.4102/sajpsychiatry.v28i0.1547
24. Hsiao CY, Tsai YF. Factors of caregiver burden and family functioning among Taiwanese family caregivers living with schizophrenia. J Clin Nursing. 2015;24(11–12):1546–1556. doi:10.1111/jocn.12745
25. Yu H, Wang X, He R, Liang R, Zhou L. Measuring the Caregiver Burden of Caring for Community-Residing People with Alzheimer’s Disease. PLoS One. 2015;10(7):567.
26. Wang Z, Luo Y, Yang S, et al. Death burden of high systolic blood pressure in Sichuan Southwest China 1990-2030. BMC Public Health. 2020;20(1):406. doi:10.1186/s12889-020-8377-6
27. Madruga M, Gozalo M, Prieto J, Adsuar JC, Gusi N. Psychological Symptomatology in Informal Caregivers of Persons with Dementia: influences on Health-Related Quality of Life. Int J Environ Res Public Health. 2020;17(3). doi:10.3390/ijerph17031078
28. Zhang HY, Chong MC, Tan MP, Chua YP, Zhang JH. The Association Between Depressive Symptoms and Sarcopenia Among Community-Dwelling Older Adults: a Cross-Sectional Study. J Multidiscip Healthc. 2022;15:837–846. doi:10.2147/JMDH.S355680
29. Chaudoir SR, Fisher JD, Simoni JM. Understanding HIV disclosure: a review and application of the Disclosure Processes Model. Soc Sci Med. 2011;72(10):1618–1629. doi:10.1016/j.socscimed.2011.03.028
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025