Back to Journals » Psychology Research and Behavior Management » Volume 19
Beyond Stigma–Integrating Neurobiology, Genetics, and Awareness Integration Theory in Addiction Recovery
Authors Blum K ![]() , Gold MS
, Gold MS ![]() , Jafari N, Lewandrowski KU
, Jafari N, Lewandrowski KU ![]() , Sharafshah A
, Sharafshah A ![]() , Mohankumar K, Lorio MP
, Mohankumar K, Lorio MP ![]() , Bowirrat A
, Bowirrat A ![]() , Pinhasov A
, Pinhasov A ![]() , Thanos KZ, Elman I
, Thanos KZ, Elman I ![]() , Baron D, Dennen CA, Fuehrlein B, Lewandrowski AP, Modestino EJ, Thanos PK, Zeine F
, Baron D, Dennen CA, Fuehrlein B, Lewandrowski AP, Modestino EJ, Thanos PK, Zeine F ![]()
Received 22 August 2025
Accepted for publication 30 January 2026
Published 10 February 2026 Volume 2026:19 561157
DOI https://doi.org/10.2147/PRBM.S561157
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gabriela Topa
Kenneth Blum,1– 6 Mark S Gold,7 Nicole Jafari,8,9 Kai-Uwe Lewandrowski,3,5 Alireza Sharafshah,10 Kavya Mohankumar,6 Morgan P Lorio,11 Abdalla Bowirrat,2 Albert Pinhasov,2 Kyriaki Z Thanos,12 Igor Elman,2,13 David Baron,1,14 Catherine A Dennen,15 Brian Fuehrlein,16 Alexander PL Lewandrowski,17 Edward J Modestino,18 Panayotis K Thanos,2,12 Foojan Zeine19,20
1Center for Exercise and Sport Mental Health, Western University Health Sciences, Pomona, CA, USA; 2Department of Molecular Biology, Adelson School of Medicine, Ariel University, Ariel, Israel; 3Center for Advanced Spine Care of Southern Arizona, Tucson, AZ, USA; 4Institute of Psychology, ELTE Eötvös Loránd University, Budapest, Hungary; 5Graduate Program, Department of General and Specialized Surgery, Gaffrée E Guinle Universitary Hospital, Federal University of the State of Rio de Janeiro (UNIRIO), Rio de Janeiro, Brazil; 6Division of Clinical Neurology, The Kenneth Blum Institute of Neurogenetics and Behavior, LLC, Austin, Tx., USA; 7Department of Psychiatry, Washington University School of Medicine, St. Louis, MO, USA; 8Department of Applied Clinical Psychology, The Chicago School of Professional Psychology, Los Angeles, CA., USA; 9Division of Personalized Medicine, Cross-Cultural Research and Educational Institute, San Clemente, CA., USA; 10Cellular and Molecular Research Center, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran; 11Advanced Orthopedics, Altamonte Springs, FL., USA; 12Behavioral Neuropharmacology and Neuroimaging Laboratory on Addictions (BNNLA), Research Institute on Addictions, Department of Pharmacology and Toxicology, Jacobs School of Medicine and Biomedical Sciences, University at Buffalo, Buffalo, NY., USA; 13Department of psychiatry, Harvard University, School of Medicine, Cambridge, MA., USA; 14Department of Psychiatry & Behavioral Sciences, Stanford University School of Medicine, Palo Alto, CA., USA; 15Department of Family Medicine, Jefferson Health Northeast, Philadelphia, PA., USA; 16Department of Psychiatry, Yale University, New Haven, CT., USA; 17Department of Biological Sciences, Dornsife College of Letters, Arts & Sciences, University of Southern California, Los Angeles, CA., USA; 18Brain & Behavior Laboratory, Department of Psychology, Curry College, Milton, MA., USA; 19Department of Health Science, California State University, Long Beach, CA., USA; 20International Awareness Integration Institute, San Clemente, CA, USA
Correspondence: Foojan Zeine, Email [email protected]
Abstract: Addiction continues to be heavily stigmatized due to lingering misconceptions that frame substance use as a moral failing rather than a treatable neurobiological disorder. This stigma, when internalized, intensifies shame and obstructs recovery. Awareness Integration Theory, a multidisciplinary therapeutic model, addresses these internalized beliefs by identifying and integrating fragmented aspects of the self across thoughts, emotions, behaviors, and promotes self-awareness, emotional regulation, and cognitive restructuring, critical components in reducing shame and fostering resilience. This paper explores the interplay between self-perception, shame, resilience, and biological predisposition in addiction recovery. Research shows that shame-prone individuals are more likely to relapse, while guilt-prone individuals demonstrate greater capacity for change. Resilience, cultivated through self-forgiveness, social support, and neuroplastic interventions, mitigates the impact of shame. Genetic variants and epigenetic modifications influence reward deficiency syndrome, increasing vulnerability to addiction. The Genetic Addiction Risk Severity test can identify at-risk individuals, enabling precision-targeted interventions. Awareness Integration Therapy’s integrative framework complements genomic and neurobiological insights by fostering self-acceptance, enhancing insight into unconscious belief systems, and motivating purposeful action. Neuroimaging studies support the role of resilience-based practices, including those embedded in Alcoholics Anonymous, in promoting dopamine homeostasis and neural recovery. In conclusion, stigma reduction must advance alongside personalized medicine. Integrating Awareness Integration Therapy with genetic screening, trauma-informed care, and psychoeducation offers a comprehensive, compassionate approach. Reframing addiction as a brain-based, treatable condition empowers clients and families, facilitating sustainable recovery grounded in science and self-awareness.
Keywords: awareness integration theory, AIT, GARS, genetic addiction risk severity, stigma, shame, addiction, substance abuse
Introduction
Individuals struggling with drug or alcohol addiction often face significant societal stigma, which can hinder their path to recovery. There is often a lack of understanding about the thought processes behind their choices and behaviors. Alcoholics Anonymous (AA) emphasizes the importance of separating the individual from the illness.1 Stigma largely stems from outdated views that associate addiction, often linked to reward deficiency,2 with moral weakness, rather than recognizing it as a chronic, relapsing, yet treatable brain disorder. These societal misconceptions are frequently internalized by those with substance use disorders, fostering feelings of shame, social withdrawal, and hesitance to seek treatment.
Combating this stigma is essential to recovery, as highlighted by the American Society of Addiction Medicine (ASAM), the Addiction Policy Forum (APF),3 and Volkow et al.4 ASAM’s ethical guidelines for addiction medicine underscore the importance of respecting patient autonomy, delivering compassionate, nonjudgmental care, and employing multifaceted strategies to reduce stigma. Similarly, Miller and Sheppard5 argue that broader medical recognition of addiction as a treatable condition will improve understanding and reduce stigma surrounding diagnosis and treatment. Against this backdrop, Awareness Integration Theory offers a structured, compassionate framework that helps individuals reduce shame, understand the beliefs and emotional patterns driving substance use, and build the self-awareness, regulation skills, and aligned action needed for sustained recovery.
Persistence and Recovery
Recovery from addiction is a process that demands persistent effort, day after day. Relapse should not be viewed as failure but rather as a signal to reassess and recommit to the path of recovery. Just as elite athletes like Tom Brady and Michael Jordan were not defined by flawless records, but by how they responded to setbacks, so too are those in recovery defined by their resilience, not perfection.6
A dominant view in the literature suggests guilt and shame have opposing behavioral impacts: guilt-prone individuals are more inclined to take corrective action and make amends, while those prone to shame may remain stuck in harmful behaviors, avoid accountability, or react with defensiveness. Snoek et al6 propose a rethinking of this framework, suggesting that outcomes depend on the nature of self-blame, whether it is punitive or constructive (“scaffolding”). This, in turn, shapes whether an individual views themselves as capable of change or as permanently flawed, influencing whether guilt and shame become recovery barriers or tools for growth.
Resilience
Psychiatrists Dennis Charney and the late Steven Southwick were pioneers in resilience research. Drawing on over two decades of clinical studies and interviews, they identified key traits of resilient individuals: optimism, fear regulation, meaning-making, social connection, faith, cognitive and emotional flexibility, perseverance, and attention to physical health and self-care.7 Their work helped shift psychiatric focus from trauma-related deficits to strengths such as neuroplasticity and post-traumatic growth (PTG).
While interpersonal trauma, particularly domestic and sexual violence, is associated with long-term psychological harm, recent studies have highlighted potential positive psychological changes among survivors. In one study, Edwards et al8 used regression analysis to show that post-traumatic growth (PTG) was linked to lower depression levels and a stronger sense of community.
Meaning-making is often central to trauma survival, helping individuals preserve a coherent sense of self. Strong interpersonal relationships serve as powerful protective factors, and spiritual or existential beliefs can provide grounding during adversity. The scientific community increasingly recognizes that physical exercise supports resilience by protecting brain health.9 Chronic stress elevates oxidative stress, contributing to neural damage. Exercise, however, has been shown to mitigate such effects by reducing markers of cell death (eg, Bax) and inflammation (eg, Cox-2), as well as limiting microglial activation in brain areas like the cortex and hippocampus. These findings suggest that exercise enhances the brain’s resilience to stress-induced damage.
Our laboratory has similarly observed that exercise fosters both mental and physical wellbeing, offering protection against a range of conditions, including cardiovascular, neurological, and psychiatric illnesses. In a study by Hanna et al,10 PET imaging revealed that exercised, cocaine-exposed rats showed altered brain metabolism compared to sedentary, cocaine-exposed rats. Notable differences were seen in regions linked to sensory processing, emotional regulation, addiction, and motor control. These results support the hypothesis that aerobic exercise can rewire brain responses to drugs and stress, potentially aiding in addiction recovery.
Resilience is deeply woven into the ethos and practice of Alcoholics Anonymous, even predating formal scientific inquiry into the concept. The Big Book, the Twelve Steps, and the Twelve Traditions emphasize resilience in spiritual, emotional, and communal dimensions, especially in the context of overcoming shame, stigma, and relapse. In AA, self-worth is rebuilt not through perfection, but through daily acts of connection, contribution, and self-reflection.1 Members are encouraged to maintain hope while accepting reality, embracing personal growth, humility, and healing within a supportive community.
“Recovery is not about staying up all the time. It is about learning how to get up-every time”. - AA speaker.
Compassion and empathy toward individuals with addiction are linked to improved treatment engagement and outcomes, compared to perspectives that frame addiction as a moral failure. Experts strongly advocate for conceptualizing addiction within a chronic disease framework, with an emphasis on early risk detection not through pathologizing youth, but by equipping them with the tools to thrive. This paradigm shift from “What’s wrong with you?” to “How can we help you grow stronger?” holds promise as one of the most impactful strategies for long-term addiction prevention. Importantly, addiction is not a fixed, immutable identity; rather, it is a condition from which recovery is possible, including among healthcare professionals such as addicted physicians.11,12
Resilience and forgiveness offer a forward-looking and empowering framework for both prevention and early intervention. Reducing stigma remains central to effective treatment and long-term recovery. The focus should be on stigmatizing the substance, and not the person. In this regard, resilience and recovery have emerged as key areas of interest in the field of alcohol and drug dependence (ADD). Functional magnetic resonance imaging (fMRI) and positron emission tomography (PET) studies have demonstrated that resilience is associated with lower task-elicited neural activation in the basal ganglia and enhanced prefrontal cortex (PFC) activity, particularly in the context of relapse prevention during early abstinence from substance use. These neural adaptations appear to be influenced by several moderating factors, including genotype-dependent neuronal regeneration, gender-specific neural recovery, psychiatric comorbidities, concurrent use of tobacco or marijuana, and adolescent alcohol abuse.13
Neurogenetic & Epigenetic Correlates to Resilience and Stigma in Recovery
Addiction is a multifaceted behavioral disorder shaped by both genetic and environmental influences. Traits such as novelty-seeking, impulsivity, and heightened cue reactivity have been identified as behavioral risk factors for substance use.14–19 These traits are partially rooted in neurobiological variation, particularly dysfunctional dopaminergic signaling in the striatum and impaired prefrontal cortical regulation of subcortical emotional and motivational responses.20
A major advance in mapping genes implicated in addiction and reward deficiency syndromes has been led by Blum et al. Their pharmacogenomic research using the Genetic Addiction Risk Score (GARS) employed a multi-layered in silico approach encompassing: (1) Protein–Protein Interactions (PPIs), (2) Gene Regulatory Networks (GRNs), (3) Disease–Drug–Chemical interactions (DDCs), and (4) Gene Coexpression Networks (GCNs). This comprehensive analysis supports the concept of “pre-addiction”, endorsed by institutions such as the National Institute on Drug Abuse (NIDA) and the National Institute on Alcohol Abuse and Alcoholism (NIAAA), as a form of dopamine dysregulation within the broader framework of Reward Deficiency Syndrome (RDS). Findings from this work, centered around the Brain Reward Cascade (BRC), suggest that RDS may represent a primary phenotype, with various behavioral disorders acting as endophenotypes influenced by specific genetic variants. An enrichment analysis of 59 key genes revealed significant associations with dopaminergic pathways in the BRC, offering strong support for using GARS as a predictive tool. This test may assist in early identification of addiction vulnerability, guide personalized pharmacotherapy (including for pain management), and improve prescription drug safety.21
Notably, foundational research from the 1970s and 1980s, prior to completion of the Human Genome Project, established dopamine’s pivotal role in substance-related pharmacodynamics, including alcohol and cocaine dependence.22,23 Addiction can be conceptualized as a behavioral choice influenced by competing contingencies, especially sensitivity to immediate (NOW) versus delayed (LATER) rewards.24 Volkow and Baler25 proposed a model in which dopamine modulates both phasic signaling (associated with NOW-oriented reward circuits) and tonic signaling (associated with LATER-oriented control circuits). Dopamine’s regulation of the orbitofrontal cortex enables shifts in salience attribution, while its modulation of the insula influences reward-driven decisions based on interoceptive states. Dysregulation of these circuits has been implicated in multiple conditions with genetic underpinnings, including addiction and obesity.
The interplay of neurotransmitters and genes regulating dopamine release defines the Brain Reward Cascade [see Figure 1]. Genetic and epigenetic variations within this system may influence susceptibility to addiction and alter pain tolerance. The Reward Deficiency Syndrome (RDS) Consortium has proposed novel strategies for addressing the opioid crisis, particularly iatrogenic addiction, by targeting dopaminergic tone in pain processing pathways.26 Variability in the mesolimbic system, due to genetic polymorphisms, may predispose individuals to heightened pain sensitivity or enhanced tolerance.27 These genetic insights point to new therapeutic targets for pain management and addiction prevention and recovery.26,28–32 Pharmacogenomic testing of candidate genes such as CB1, mu-opioid receptors, and proenkephalin may offer personalized treatment strategies and improved clinical outcomes. Identifying individuals at high genetic risk for RDS-related behaviors, particularly in vulnerable populations, could be an essential tool for optimizing public health resources and intervention strategies.
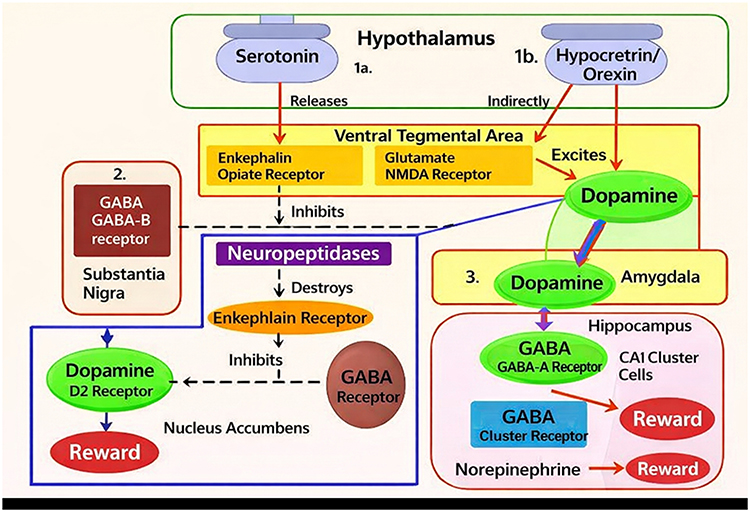 |
Figure 1 Illustrates a schematic of the Brain Reward Cascade. |
The ongoing addiction crisis has devastated countless lives, with millions of fatalities worldwide. While it is now widely accepted that addictive behavioral patterns stem from a complex interplay of neurobiological and spiritual dimensions, short-term solutions such as substitution therapies, particularly for opioid use disorder, focus on harm reduction rather than long-term recovery or true prevention. While valuable in mitigating immediate risks, these strategies do not constitute a harm-free or curative model.
We propose a novel and comprehensive approach that includes genetic risk assessment, the promotion of dopamine homeostasis, and a Brain Health Check during youth as part of a preventive framework.33 Central to this model is the “Reward Dysregulation Syndrome Solution System”, a six-hit paradigm designed to identify individuals at risk and address the root cause of addiction, dopaminergic dysregulation. While we acknowledge and commend the wealth of research in neurogenetics and neuropharmacology, we argue that future addiction science must expand to include early identification strategies. These may involve validated tools such as the RDSQ29 questionnaire, GARS genetic risk testing, Brain Health Checks, and diagnostic frameworks that identify early-stage or preclinical substance use disorders (SUD).34–36
The “preaddiction” concept, gaining traction with support from institutions like the National Institute on Drug Abuse and National Institute on Alcohol Abuse and Alcoholism, offers a powerful opportunity to develop interventions before addiction fully manifests. By identifying neurochemical imbalances and inherited vulnerabilities early on, clinicians can implement timely and targeted therapies.37
In a recent study, Legaki et al38 highlighted the genetic and environmental complexity of alcohol use disorder. Using the Qiagen AllPrep RNA/DNA Mini Kit, researchers analyzed patient samples before and after treatment, identifying 35 dysregulated genes in individuals with AUD. Notably, EPHB2, EGR, and AKT1 expression decreased, while responders demonstrated distinct baseline gene expression profiles. Post-treatment, expression of 57 genes normalized, with NCAM1, GRM2, and BDNF showing significant recovery. EGR4, INHBA, and NCAM1 emerged as promising predictive biomarkers for treatment response.
Our own laboratory has presented findings from a case series applying the Genetic Addiction Risk Score (GARS), demonstrating a high prevalence of risk alleles for reward deficiency among members of a single nuclear family affected by RDS behaviors. This family, comprising a mother, father, son, and daughter, exhibited a spectrum of behavioral health challenges, including memory issues, amotivation, substance misuse, depression, and anxiety. After receiving their GARS results, family members reported reduced feelings of guilt and increased optimism for recovery. Prior studies from our group have shown that possession of four or more reward gene polymorphisms (eg, DRD1-DRD4, DAT1, MOR, GABABR3, COMT, MAOAA, and 5HTTLPR) is predictive of higher Addiction Severity Index (ASI) scores for drug misuse, while seven or more alleles predict severe alcoholism.39 These findings underscore the value of genetic feedback in destigmatizing addiction and empowering families with actionable insight.
Further evidence supports a biological substrate to recovery potential. Alcohol-dependent individuals often exhibit reduced hippocampal volume and impaired neurocognition relative to healthy controls. While findings have varied, premorbid factors likely influence these deficits. In a 2014 study, individuals homozygous for the BDNF Val allele showed increased hippocampal volume after seven months of abstinence, with significantly larger hippocampi compared to Met carriers.40
Serotonin (5-hydroxytryptamine or 5-HT) is another critical neurotransmitter implicated in SUD acquisition, persistence, and recovery. Recent studies have uncovered numerous 5-HT genetic polymorphisms linked to SUDs. Variants in genes such as SLC6A4, HTR1B, HTR2A, HTR2C, and the HTR3 gene family (HTR3A-HTR3E) contribute to patient variability. The short allele of the 5-HT transporter-linked polymorphic region (5-HTTLPR) within SLC6A4 has shown modest but significant associations with alcohol dependence in two meta-analyses.41
Glutamatergic systems also play a significant role. N-methyl-D-aspartate (NMDA) receptors are key regulators of synaptic plasticity and behavior. Ethanol (EtOH) inhibits these receptors even at low concentrations. In mice, the F639A mutation in the transmembrane domain (TMD) 3 of the NR1 NMDA subunit decreases EtOH sensitivity and, in certain models, reduces EtOH-related behavioral responses while increasing voluntary EtOH consumption. Parallel mutations in Drosophila, affecting the same receptor regions, further support the role of NMDA receptor sensitivity in alcohol use behaviors.42
Addiction impacts not only individuals but also entire communities and health systems. While preventing initial substance use remains the most effective approach, preventing relapse is equally vital for sustained recovery. Emerging research identifies a set of genes with stable expression changes post-drug exposure and abstinence. These molecular shifts correspond with behavioral alterations and structural brain changes, positioning them as promising therapeutic targets. Continued investigation of these candidate genes, and interventions to manipulate them, will support the development of effective treatments to reduce relapse rates and improve long-term outcomes.43 See Table 1
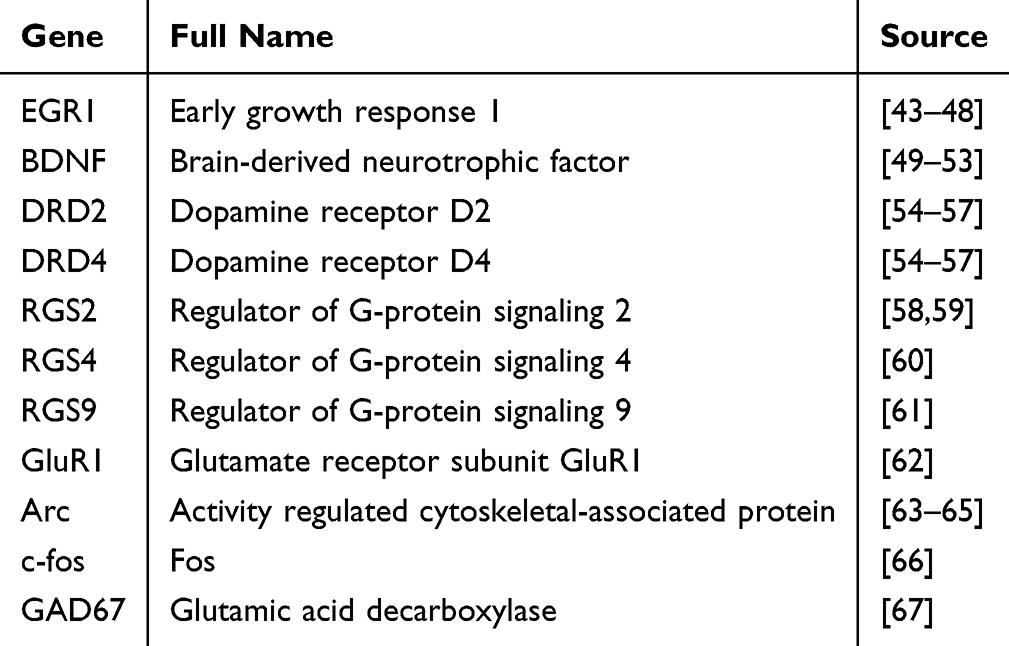 |
Table 1 Several Genes Have Been Identified to Be Changed in Models of Relapse. Kai or ALEX Make Nice |
Synaptic proteins involved in neuronal regulation are evolutionarily conserved targets of ethanol. Krishnan et al68 demonstrated that shibire and Syntaxin 1A are required for the acquisition of rapid functional tolerance to ethanol. The shibire gene product, Dynamin, is specifically required for the early cellular response to ethanol exposure, which initiates the adaptive processes responsible for rapid tolerance.
The expanding field of neuro-nutrigenomics represents a promising frontier in human health and addiction medicine. A major advancement in this area is the development of the Genetic Addiction Risk Score, which demonstrates predictive validity for the severity of both substance and non-substance addictive behaviors. While personalized neuro-nutrient interventions based on genotype are not yet commercially available, growing evidence suggests future applicability for tailoring addiction treatment.69
Polymorphisms in genes such as COMT and DRD2 have been associated with alcohol craving intensity during abstinence. Notably, traits such as self-directedness and self-acceptance appear more strongly linked to DRD2 polymorphisms than temperamental factors, underscoring the relevance of personality-genotype interactions in addiction vulnerability.70
The GABAA receptor family, particularly receptors containing ρ1, ρ2, or ρ3 subunits, has been primarily studied in retinal tissue but is also expressed in multiple brain regions. Receptors containing the ρ1 subunit are inhibited by low ethanol concentrations. In animal models, genetic deletion of ρ1 alters ethanol consumption, sensitivity, and motor effects, indicating that ρ1 plays a central role in the in vivo behavioral effects of ethanol.71
According to the American Society of Addiction Medicine (ASAM), individuals with SUDs suffer from impaired reward circuitry, often due to hypodopaminergic function caused by genetic or environmental factors. The “Brain Reward Cascade” (BRC) is a well-characterized neurochemical pathway leading to dopamine release. Disruptions in this cascade reduce dopamine availability, contributing to craving and addiction. Neuro-nutrient therapies, grounded in nutrigenomic principles, have been developed over the past four decades to restore dopaminergic balance and show promising clinical results when appropriately applied.72
Adolescence is a key period of vulnerability for addiction, during which environmental exposures can epigenetically activate or suppress inherited risk factors. Early-life adversity, such as low birth weight, maternal depression, or family instability, can epigenetically regulate genes involved in behavioral inhibition, stress response, and cognitive control, contributing to the emergence of reward deficiency syndromes (RDS).73,74
Brain-derived neurotrophic factor (BDNF) plays a pivotal role in the maturation of dopaminergic, serotonergic, noradrenergic, glutamatergic, and cholinergic systems. Plasma levels of BDNF are associated with both cognitive function and aggressive impulsivity, making it a critical biomarker in addiction vulnerability and recovery.75
Since the identification of the DRD2 Taq A1 allele’s association with severe alcoholism in 1990,15 the gene has been implicated across a spectrum of neuropsychiatric conditions. DRD2 variants exhibit pleiotropic effects on cognition, stress response, social behaviors, and reward learning. Epigenetic mechanisms, such as DNA methylation and histone modifications, can suppress DRD2 expression, compounding genetic vulnerability. These findings support the use of interventions aimed at restoring dopamine homeostasis, either by correcting epigenetic insults or enhancing receptor expression.76
Anhedonia, the inability to experience pleasure from normally rewarding activities, is a common symptom in addiction, depression, PTSD, and schizophrenia. It is thought to arise from dysfunction in the mesolimbic dopamine system and may persist long after substance clearance. Gold et al74 conceptualize anhedonia as an epiphenomenon of hypodopaminergic traits shaped by both genetics and environment. These disrupted reward mechanisms may interact with anti-reward systems, exacerbating addiction-related symptoms. D2/D3 receptor-targeted interventions offer potential for restoring pleasure responses and preventing relapse.77
Loneliness, a growing public health concern, contributes significantly to both psychological and physical morbidity. Blum et al78 identified multiple factors influencing loneliness: (1) genetic predisposition; (2) mental health-related genetic overlap; (3) epigenetic consequences of adverse childhood experiences; and (4) hypodopaminergic reward deficiency states caused by early-life stress. Recognizing the neurobiological underpinnings of loneliness could inform new treatment pathways.79–82
Anti-Stigma Modeling
Recent studies highlight the promise of anti-stigma interventions that integrate genetic education. In one study, women who underwent genetic testing for SUD showed favorable attitudes toward precision prevention in adolescents. Perceived benefits included increased youth engagement, family protection, and behavior change, though concerns about stigma and privacy persisted.83 Other studies caution that while the brain-disease model can reduce blame, it may also decrease hope for recovery and increase perceptions of dangerousness.82,84–89
Public attitudes toward individuals with addiction remain markedly negative, often more so than attitudes toward those with other mental health conditions.90–93 Importantly, gender-specific stigma also plays a role; women more frequently cite stigma as a barrier to engaging in SUD group therapy, highlighting the need for gender-tailored treatment strategies.94
Awareness Integration Therapy
This paper proposes Awareness Integration Therapy (AIT) as an effective and versatile psychotherapeutic approach for prevention, treatment, and relapse prevention in various psychological conditions, including those underlying addiction. AIT is an evidence-based, multidimensional framework designed to enhance self-awareness, resolve past traumas, dismantle psychological barriers, and foster clarity and positive mindsets. Developed through the integration of diverse therapeutic modalities—including Cognitive Behavioral Therapy (CBT), Existential Therapy, Person-Centered Therapy, Emotion-Focused Therapy (EFT), Mind-Body Therapy (MBT), Eye Movement Desensitization and Reprocessing (EMDR), Hypnosis, and Mindfulness, AIT offers a flexible and holistic method to address the full spectrum of the human experience, encompassing both intrapsychic processes and interpersonal dynamics, and fostering healthier, more authentic connections with others in one’s life. This synthesis maximizes therapeutic outcomes, enabling lasting and transformative change.95
Clinical research demonstrates AIT’s substantial effectiveness. Zeine (2016) reported that AIT achieved a 76% reduction in depression, 60% reduction in anxiety, 43% improvement in self-esteem, and 20% increase in self-efficacy.96 A six-hour therapeutic workshop study (Zeine et al, 2017) further showed reductions in depression (27.5%) and anxiety (37%), along with increases in self-esteem (15%) and self-efficacy (13%).97 AIT’s self-help module has also proven beneficial for college students, leading to decreased stress and marked reductions in anxiety (21.72%) and depression (68%).98 Case studies reinforce these findings. Madani and Zeine (2023) observed a 50% decrease in anxiety and 60% increase in self-esteem after AIT intervention,99 while Zarbakhsh and Zeine (2023) documented significant improvements in PTSD (66%), anxiety (75%), and depression (66%) in a transgender male college student.100 Additionally, data from the “Foojan” app (Zeine, 2023) revealed improvements in self-perception (75%), body image and health (71%), intimate relationships (71%), and various family relationships (73%), career satisfaction (70%), financial wellbeing (70%), and addiction recovery (73%).101
Awareness Integration Therapy works by reconciling fragmented aspects of the self arising from psychological trauma and fostering awareness from past experiences through to the present. The approach guides individuals to examine how their perceptions shape interactions, choices, and behaviors, engaging both conscious and subconscious processes. Through structured self-exploration, clients learn to Identify and integrate fragmented self-aspects for harmonious functioning, differentiate constructive from nonconstructive thoughts and schemas, and recognize and revise deep-seated beliefs, replacing harmful patterns with beneficial principles. This process extends to multiple life domains relationships, family dynamics, career, finances, and spirituality resulting in broad personal and interpersonal transformation.95
For individuals struggling with substance abuse, AIT provides tools to move beyond the emotional void that addiction attempts to fill. While the initial motivation for change may stem from avoiding the pain of consequences or seeking more meaningful experiences, sustainable recovery requires addressing unresolved emotional distress. AIT helps clients confront and process inner pain, dismantle maladaptive coping mechanisms, and develop resilience.95
Within the framework of Awareness Integration Theory (AIT), self-identity is understood as a central mechanism in addiction recovery, as addictive behaviors are often rooted in fragmented self-concepts, unresolved core beliefs, and a diminished sense of agency. AIT facilitates recovery by guiding individuals through structured self-awareness and identity exploration, allowing them to examine how past experiences, emotional patterns, and internalized beliefs have shaped a substance-centered or maladaptive identity. Through its integrative process—addressing cognitive, emotional, behavioral, and somatic dimensions AIT supports the reconstruction of a coherent, values-based sense of self that replaces addiction-driven narratives with self-efficacy, accountability, and purpose. As individuals develop a clearer and more integrated self-identity, substances are no longer relied upon to regulate emotions, manage stress, or define self-worth, thereby strengthening intrinsic motivation for change and supporting sustained recovery.102
Living with a person in addiction can cause family frustration, exhaustion, and conflict. AIT’s therapeutic stance offering unconditional acceptance alongside accountability helps individuals remain engaged in recovery even after relapse. Family therapy within the AIT model allows members to address enabling behaviors, set healthy boundaries, and understand their influence on the addicted individual. This shared responsibility fosters a supportive environment conducive to long-term recovery.95
AIT’s Six-Phase Intervention Model
Phase 1 – Cultivating Foundational Awareness
The first phase centers on developing a deep awareness of the participant’s cognitive, emotional, and behavioral patterns in relation to their external environment. Through guided questioning, clients uncover their perceptions, attitudes, and implicit biases toward others. This exploration brings to light the underlying belief systems and the behaviors that shape their worldview and influence the quality of their interpersonal interactions.101
Phase 2 – Exploring Subjective Projections
In this phase, participants identify and examine the internalized narratives they carry about how others perceive them. They explore the meaning they assign to these perceptions, assess the accuracy of their assumptions, and evaluate the emotional and behavioral impact these projections have on their lives. This stage is particularly valuable for individuals struggling with heightened anxiety, social phobia, facing stigma, or patterns of shame and self-consciousness.101
Phase 3 – Deepening Self-Understanding and Self-Compassion
Phase three turns the focus inward, encouraging participants to reflect on their core beliefs and emotional truths about themselves. Clients examine self-perception, emotional patterns, and tendencies toward self-judgment. Through this process, they learn to cultivate self-compassion, reframe distorted self-views, and strengthen the foundation for overall mental and emotional well-being.101
Phase 4 – Integrating Cognitive, Emotional, and Somatic Awareness
This phase involves a structured process for connecting thoughts, emotions, and bodily sensations—particularly as they relate to negative core beliefs rooted in trauma. Participants identify how maladaptive thoughts and emotional reactivity disrupt rational decision-making and are guided in developing skills for emotional regulation. By releasing and integrating previously fragmented aspects of the self, caused by trauma or childhood adverse conditions, clients re-evaluate old belief systems, opening the way to greater authenticity and a more connected engagement with the external world.101
Phase 5 – Envisioning and Embodying a New Self
Looking toward the future, clients engage in visualization practices to define and commit to a healthier self-concept. This includes fostering a constructive mindset, embracing personal agency, and developing intentional patterns of perception and behavior toward self and others. Clients learn and apply new skills that support an addiction-free, balanced, and purpose-driven life.101
Phase 6 – Relapse Prevention and Sustained Alignment
The final phase focuses on maintaining long-term change by creating a value system that aligns intentions, emotions, and behaviors. Clients design and visualize their desired future self, often using creative tools such as collages or vision boards to reinforce motivation and direction. These visual anchors serve as ongoing touchstones, reinforcing clients’ goals and aspirations while keeping them grounded in both recovery and purposeful living. Alongside these internal motivators, clients design sustainable support structures engaging in meaningful programs, nurturing relationships with friends and family, and building accountability networks that strengthen resilience, reinforce healthy habits, and safeguard long-term sobriety.101
This six-phase process is applied holistically across all areas of life affected by addiction—whether related to substances, behaviors, or relational dynamics—ensuring both comprehensive healing and sustainable transformation.
Futuristic
Between 2000 and 2021, global prevalence of alcohol use disorder, alcohol-associated liver disease, and alcohol-attributable liver cancer rose significantly, with especially sharp increases in women between 2019–2021.95 Yet current OUD treatments focus on harm reduction through opioid replacement, without restoring neurochemical balance. A forward-looking model, termed “Precision Behavioral Management” (PBM), aims to address this gap.103
Novel Policy
PBM integrates five key components designed to personalize addiction treatment and address underlying neurobiological imbalances. (1) GARS Testing involves the use of a 10-gene panel to predict addiction severity using the Addiction Severity Index (ASI), thereby enabling early identification of genetic predisposition to substance use disorders. Genetic testing should be used only with appropriate informed consent, privacy protections, and clinical oversight. (2) The RDS Questionnaire is a validated tool that helps phenotype reward deficiency syndromes by assessing behavioral and cognitive traits linked to dopaminergic dysfunction. (3) Comprehensive Analysis of Reported Drugs (CARD™) offers real-time monitoring of treatment compliance and abstinence from illicit substances, serving as a critical accountability and safety mechanism during recovery. (4) Pro-Dopamine Regulation (KB220Z) utilizes targeted nutrient-based therapies, administered intravenously or orally, to restore dopamine homeostasis, reduce craving, and prevent relapse. (5) DNA-Directed Gene Expression Profiling allows clinicians to track mRNA expression patterns and guide therapeutic decisions, optimizing treatment outcomes through precision targeting of the brain’s reward circuitry. (6) Awareness Integration Therapy stands out as a comprehensive, integrative, and empirically supported method for addressing psychological distress and addiction. By uniting multiple evidence-based modalities into a cohesive framework, AIT promotes profound self-awareness, emotional regulation, and interpersonal growth, making it a promising approach for both individual healing and systemic change.
This paradigm can be applied across populations, including underserved communities such as African Americans disproportionately affected by RDS. We are also developing a diagnostic classification system for RDS, which could provide a much-needed tertiary care model.
Conclusion
Understanding the genetic and epigenetic foundations of addiction may aid in reframing it as a neurobiologically based, treatable disorder rather than a moral failing. This reconceptualization could help dismantle stigma at its core and replace shame with science-informed empathy. Genetic markers such as DRD2, COMT, and SLC6A4, as well as epigenetic alterations shaped by trauma and environmental stress, contribute to reward deficiency syndrome and influence addiction vulnerability. Tools such as the Genetic Addiction Risk Severity test enable personalized, dopamine-centered interventions that address the underlying neurobiology. At the same time, psychotherapy through Awareness Integration Therapy fosters resilience by cultivating self-forgiveness, strengthening social connections, and promoting neuroplastic change, offering a holistic pathway to healing and serving as a critical safeguard against relapse. Recovery frameworks like Alcoholics Anonymous already incorporate these resilience principles, aligning with current neuroscience. Societal narratives must continue to evolve along with precision medicine and anti-stigma education. Reducing shame and strengthening self-awareness through compassionate, individualized care can improve recovery pathways for individuals and, when implemented at scale, support more effective and humane public health approaches to addiction.
Summary
Addiction is still widely misunderstood and stigmatized, and many people are treated as if substance use reflects a personal or moral failure rather than a brain-based, treatable condition. This stigma often becomes internalized as shame, which can increase isolation, reduce help-seeking, and make recovery harder. The study was done to clarify how shame, self-perception, resilience, and biological vulnerability interact in addiction recovery, and to describe a more compassionate, personalized path forward.
The researchers reviewed and integrated findings from prior clinical and biological research. They highlight consistent evidence that shame-proneness is linked to higher relapse risk, while constructive guilt can support accountability and change. They also summarize research showing that resilience supported by self-forgiveness, social connection, meaning making, and health behaviors buffers stress and supports sustained recovery.
The paper also brings in “precision” approaches that use biology to tailor care. It explains how genetic variants and stress-related biological changes can increase vulnerability (often discussed as reward deficiency), and it describes the Genetic Addiction Risk Severity test as one tool to identify elevated risk and match supports more intentionally. The authors propose combining this kind of biological insight with structured psychotherapy that builds self-awareness, emotional regulation, healthier beliefs, and aligned action, so care addresses both the body and the lived psychological experience of recovery.
What these results mean is practical: reducing shame and stigma is not “extra”, it is treatment. When care pairs evidence-based psychotherapy with personalized, biology-informed supports, people and families gain a clearer, more hopeful pathway to sustainable recovery.
Disclosure
Dr Kenneth Blum reports royalties from Synaplife, during the conduct of the study; In addition, Dr Kenneth Blum has a patent in USA with royalities paid to Synap life and a patent in Europe issued to GARS. Dr. Foojan Zeine is the originator of the Awareness Integration Theory with a patent issued. The authors report no other conflicts of interest in this work.
References
1. Blum K, Thompson B, Demotrovics Z, et al. The molecular neurobiology of twelve steps program & fellowship: connecting the dots for recovery. J Reward Def Syndrome. 2015;1(1):46–14. PMID: 26306329; PMCID: PMC4545669. doi:10.17756/jrds.2015-008
2. Blum K, Sheridan PJ, Wood RC, et al. The D2 dopamine receptor gene as a determinant of reward deficiency syndrome. J R Soc Med. 1996;89(7):396–400. PMID: 8774539; PMCID: PMC1295855. doi:10.1177/014107689608900711
3. Feder A, Fred-Torres S, Southwick SM, Charney DS. The biology of human resilience: opportunities for enhancing resilience across the life span. Biol Psych. 2019;86(6):443–453. Epub 2019 Jul 24. PMID: 31466561. doi:10.1016/j.biopsych.2019.07.012
4. Volkow ND. Stigma and the Toll of Addiction. N Engl J Med. 2020;382(14):1289–1290. PMID: 32242351. doi:10.1056/NEJMp1917360
5. Miller NS, Sheppard LM. The role of the physician in addiction prevention and treatment. Psychiatr Clin North Am. 1999;22(2):489–505. PMID: 10385946. doi:10.1016/s0193-953x(05)70089-7
6. Snoek A, McGeer V, Brandenburg D, Kennett J. Managing shame and guilt in addiction: a pathway to recovery. Addict Behav. 2021;120:106954. Epub 2021 Apr 17. PMID: 33957551. doi:10.1016/j.addbeh.2021.106954
7. Ozbay F, Fitterling H, Charney D, Southwick S. Social support and resilience to stress across the life span: a neurobiologic framework. Curr Psych Rep. 2008;10(4):304–310. PMID: 18627668. doi:10.1007/s11920-008-0049-7
8. Edwards KM, Siller L, Ullman SE, Lee KDM, Murphy SB. Post-traumatic growth in women with histories of addiction and victimization residing in a sober living home. J Interpers Violence. 2022;37(13–14):NP11180–NP11197. Epub 2021 Feb 4. PMID: 33541201. doi:10.1177/0886260521991283
9. Gerecke KM, Kolobova A, Allen S, Fawer JL. Exercise protects against chronic restraint stress-induced oxidative stress in the cortex and hippocampus. Brain Res. 2013;1509:66–78. Epub 2013 Mar 13. PMID: 23499928. doi:10.1016/j.brainres.2013.02.027
10. Hanna C, Yao R, Sajjad M, Gold M, Blum K, Thanos PK. Exercise modifies the brain metabolic response to chronic cocaine exposure inhibiting the stria terminalis. Brain Sci. 2023;13(12):1705. PMID: 38137153; PMCID: PMC10742065. doi:10.3390/brainsci13121705
11. DuPont RL, McLellan AT, White WL, Merlo LJ, Gold MS. Setting the standard for recovery: Physicians’ health programs. J Subst Abuse Treat. 2009;36(2):159–171. PMID: 19161896. doi:10.1016/j.jsat.2008.01.004
12. DuPont RL, Compton WM, McLellan AT. Five-year recovery: a new standard for assessing effectiveness of substance use disorder treatment. J Subst Abuse Treat. 2015;58:1–5. Epub 2015 Aug 1. PMID: 26277423. doi:10.1016/j.jsat.2015.06.024
13. Charlet K, Rosenthal A, Lohoff FW, Heinz A, Beck A. Imaging resilience and recovery in alcohol dependence. Addiction. 2018;113(10):1933–1950. PMID: 29744956; PMCID: PMC6128779. doi:10.1111/add.14259
14. Noble EP, Blum K. Alcoholism and the D2 dopamine receptor gene. JAMA. 1993;270(13):1547–1548. PMID: 8371464. doi:10.1001/jama.270.13.1547
15. Blum K, Noble EP, Sheridan PJ, et al. Allelic association of human dopamine D2 receptor gene in alcoholism. JAMA. 1990;263(15):2055–2060. PMID: 1969501.
16. Noble EP, Blum K, Ritchie T, Montgomery A, Sheridan PJ. Allelic association of the D2 dopamine receptor gene with receptor-binding characteristics in alcoholism. Arch Gen Psychiatry. 1991;48(7):648–654. PMID: 2069496. doi:10.1001/archpsyc.1991.01810310066012
17. Blum K, Noble EP, Sheridan PJ, et al. Association of the A1 allele of the D2 dopamine receptor gene with severe alcoholism. Alcohol. 1991;8(5):409–416. PMID: 1839129. doi:10.1016/0741-8329(91)90693-q
18. Noble EP, Blum K, Khalsa ME, et al. Allelic association of the D2 dopamine receptor gene with cocaine dependence. Drug Alcohol Depend. 1993;33(3):271–285. Erratum in: Drug Alcohol Depend 1993 Dec;34(1):83-4. PMID: 8261891. doi:10.1016/0376-8716(93)90113-5
19. Blum K, Noble EP, Sheridan PJ, et al. Genetic predisposition in alcoholism: association of the D2 dopamine receptor TaqI B1 RFLP with severe alcoholics. Alcohol. 1993;10(1):59–67. PMID: 8095394. doi:10.1016/0741-8329(93)90054-r
20. Yan Z, Rein B. Mechanisms of synaptic transmission dysregulation in the prefrontal cortex: pathophysiological implications. Mol Psychiatry. 2022;27(1):445–465. PMID: 33875802; PMCID: PMC8523584. doi:10.1038/s41380-021-01092-3
21. BLum K, Baron D, McLaughlin T, et al. Summary document research on RDS anti-addiction modeling: annotated bibliography. J Addict Psychiatry. 2024;8(1):1–33. PMID: 38765881; PMCID: PMC11100022.
22. Blum K, Eubanks JD, Wallace JE, Schwertner HA. Suppression of ethanol withdrawal by dopamine. Experientia. 1976;32(4):493–495. PMID: 944645. doi:10.1007/BF01920816
23. Dackis CA, Gold MS. New concepts in cocaine addiction: the dopamine depletion hypothesis. Neurosci Biobehav Rev. 1985;9(3):469–477. PMID: 2999657. doi:10.1016/0149-7634(85)90022-3
24. Lamb RJ, Maguire DR, Ginsburg BC, Pinkston JW, France CP. Determinants of choice, and vulnerability and recovery in addiction. Behav Processes. 2016;127:35–42. PMID: 27083500; PMCID: PMC4968700. doi:10.1016/j.beproc.2016.04.001
25. Volkow ND, Baler RD. Now vs Later brain circuits: implications for obesity and addiction. Trends Neurosci. 2015;38(6):345–352. PMID: 25959611. doi:10.1016/j.tins.2015.04.002
26. Blum K, Chen ALC, Thanos PK, et al. Genetic addiction risk score (GARS) ™, a predictor of vulnerability to opioid dependence. Front Biosci. 2018;10(1):175–196. PMID: 28930612. doi:10.2741/e816
27. Chen AL, Chen TJ, Waite RL, et al. Hypothesizing that brain reward circuitry genes are genetic antecedents of pain sensitivity and critical diagnostic and pharmacogenomic treatment targets for chronic pain conditions. Med Hypotheses. 2009;72(1):14–22. PMID: 18951726; PMCID: PMC4098664. doi:10.1016/j.mehy.2008.07.059
28. Loçasso FA, Filho HA, Alvarenga RMP, et al. Assessing the impact of IL-6 and serotonin on pain and symptomatology in fibromyalgia: an exploratory clinical study. J Pers Med. 2024;14(8):886. PMID: 39202077; PMCID: PMC11355107. doi:10.3390/jpm14080886
29. Lewandrowski KU, Sharafshah A, Elfar J, Schmidt SL, Blum K, Wetzel FT. A pharmacogenomics-based in silico investigation of opioid prescribing in post-operative spine pain management and personalized therapy. Cell Mol Neurobiol. 2024;44(1):47. PMID: 38801645; PMCID: PMC11129978. doi:10.1007/s10571-024-01466-5
30. Gold MS, Blum K, Bowirrat A, et al. A historical perspective on clonidine as an alpha-2A receptor agonist in the treatment of addictive behaviors: focus on opioid dependence. INNOSC Theranostics Pharmacol Sci. 2024;7(3):1918. PMID: 39119149; PMCID: PMC11308626. doi:10.36922/itps.1918
31. Lorio MP, Lewandrowski KU, Blum K. Top three healthcare trends in orthopaedics affecting musculoskeletal care in the elderly. Curr Aging Sci. 2024. PMID: 39113299. doi:10.2174/0118746098309054240721180720.
32. Zeine F, Jafari N, Baron D, et al. Solving the global opioid crisis: incorporating genetic addiction risk assessment with personalized dopaminergic homeostatic therapy and awareness integration therapy. J Addict Psychiatry. 2024;8(1):50–95. PMID: 39635461; PMCID: PMC11615735.
33. Blum K, Bowirrat A, Gomez LL, et al. Why haven’t we solved the addiction crisis? J Neurol Sci. 2022;442:120404. PMID: 36084363. doi:10.1016/j.jns.2022.120404
34. Blum K, Han D, Gupta A, et al. Statistical validation of risk alleles in genetic addiction risk severity (GARS) test: Early identification of risk for alcohol use disorder (AUD) in 74,566 case-control subjects. J Pers Med. 2022;12(9):1385. PMID: 36143170; PMCID: PMC9505592. doi:10.3390/jpm12091385
35. Kótyuk E, Urbán R, Hende B, et al. Development and validation of the reward deficiency syndrome questionnaire (RDSQ-29). J Psychopharmacol. 2022;36(3):409–422. PMID: 35102768. doi:10.1177/02698811211069102
36. Kotyuk E, Demetrovics Z, Urbán R, et al. Psychometric properties of the Reward Deficiency Syndrome Questionnaire among a non-clinical sample and its relationship with the characteristics of potentially addictive behaviors. Addict Behav Rep. 2025;21:100598. PMID: 40248688; PMCID: PMC12005299. doi:10.1016/j.abrep.2025.100598
37. Blum K, Han D, Bowirrat A, et al. Genetic addiction risk and psychological profiling analyses for “preaddiction’ severity index”. J Pers Med. 2022;12(11):1772. PMID: 36579510; PMCID: PMC9696872. doi:10.3390/jpm12111772
38. Legaki E, Dovrolis N, Moscholiou N, et al. Altered expression of neuroplasticity-related genes in alcohol addiction and treatment. Int J Mol Sci. 2024;25(21):11349. PMID: 39518903; PMCID: PMC11546795. doi:10.3390/ijms252111349
39. Dennen CA, Blum K, Bowirrat A, et al. Genetic addiction risk severity assessment identifies polymorphic reward genes as antecedents to reward deficiency syndrome (RDS) hypodopaminergia’s effect on addictive and non-addictive behaviors in a nuclear family. J Pers Med. 2022;12(11):1864. PMID: 36579592; PMCID: PMC9694640. doi:10.3390/jpm12111864
40. Hoefer ME, Pennington DL, Durazzo TC, et al. Genetic and behavioral determinants of hippocampal volume recovery during abstinence from alcohol. Alcohol. 2014;48(7):631–638. PMID: 25262572; PMCID: PMC4266697. doi:10.1016/j.alcohol.2014.08.007
41. Herman AI, Balogh KN. Polymorphisms of the serotonin transporter and receptor genes: susceptibility to substance abuse. Subst Abuse Rehabil. 2012;3(1):49–57. PMID: 22933845; PMCID: PMC3427938. doi:10.2147/SAR.S25864
42. Troutwine B, Park A, Velez-Hernandez ME, Lew L, Mihic SJ, Atkinson NS. F654A and K558Q mutations in NMDA receptor 1 affect ethanol-induced behaviors in drosophila. Alcohol Clin Exp Res. 2019;43(12):2480–2493. PMID: 31593608; PMCID: PMC9210938. doi:10.1111/acer.14215
43. Kuntz-Melcavage KL, Freeman WM, Vrana KE. CNS genes implicated in relapse. Subst Abuse. 2008;2:1–12. PMID: 25922574; PMCID: PMC4395042. doi:10.4137/sart.s1042
44. Schmidt ED, Voorn P, Binnekade R, Schoffelmeer AN, de Vries TJ. Differential involvement of the prelimbic cortex and striatum in conditioned heroin and sucrose seeking following long-term extinction. Eur J Neurosci. 2005;22:2347–2356. doi:10.1111/j.1460-9568.2005.04435.x
45. Hellemans KG, Everitt BJ, Lee JL. Disrupting reconsolidation of conditioned withdrawal memories in the basolateral amygdala reduces suppression of heroin seeking in rats. J Neurosci. 2006;26:12694–12699. doi:10.1523/JNEUROSCI.3101-06.2006
46. Covington HE III, Kikusui T, Goodhue J, Nikulina EM, Hammer RP Jr, Miczek KA. Brief social defeat stress: long lasting effects on cocaine taking during a binge and zif268 mRNA expression in the amygdala and prefrontal cortex. Neuropsychopharmacology. 2005;30(2):310–21
47. Freeman WM, Patel KM, Brucklacher RM, et al. Persistent alterations in mesolimbic gene expression with abstinence from cocaine self-administration. Neuropsychopharmacology. 2008;33:1807–1817. doi:10.1038/sj.npp.1301577
48. Lee JL, Di CP, Thomas KL, Everitt BJ. Disrupting reconsolidation of drug memories reduces cocaine-seeking behavior. Neuron. 2005;47:795–801. doi:10.1016/j.neuron.2005.08.007
49. Graham DL, Edwards S, Bachtell RK, DiLeone RJ, Rios M, Self DW. Dynamic BDNF activity in nucleus accumbens with cocaine use increases self-administration and relapse. Nat Neurosci. 2007;10:1029–1037. doi:10.1038/nn1929
50. Pu L, Liu QS, Poo MM. BDNF-dependent synaptic sensitization in midbrain dopamine neurons after cocaine withdrawal. Nat Neurosci. 2006;9:605–607. doi:10.1038/nn1687
51. Liu QR, Zhu XG, Gong JP, Shaham Y, Uhl GR. Rodent BDNF genes, novel promoters, novel splice variants, and regulation by cocaine. Brain Res. 2008;1067:1–12. doi:10.1016/j.brainres.2005.10.004
52. Filip M, Faron-Gorecka A, Kusmider M, Golda A, Frankowska M, Dziedzicka-Wasylewska M. Alterations in BDNF and trkB mRNAs following acute or sensitizing cocaine treatments and withdrawal. Brain Res. 2006;1071:218–225. doi:10.1016/j.brainres.2005.11.099
53. Itoh K, Hashimoto K, Shimizu E, et al. Association study between brain-derived neurotrophic factor gene polymorphisms and methamphetamine abusers in Japan. Am J Med Genet B Neuropsychiat Genet. 2005;132B:70–73. doi:10.1002/ajmg.b.30097
54. Li Y, Shao C, Zhang D, et al. The effect of dopamine D2, D5 receptor and transporter (SLC6A3) polymorphisms on the cue-elicited heroin craving in Chinese. Am J Med Genet B Neuropsychiatr Genet. 2006;141B:269–273. doi:10.1002/ajmg.b.30264
55. Shao C, Li Y, Jiang K, et al. Dopamine D4 receptor polymorphism modulates cue-elicited heroin craving in Chinese. Psychopharmacology. 2006;186:185–190. doi:10.1007/s00213-006-0375-6
56. David SP, Munafo MR, Murphy MF, Proctor M, Walton RT, Johnstone EC. Genetic variation in the dopamine D4 receptor (DRD4) gene and smoking cessation: follow-up of a randomised clinical trial of transdermal nicotine patch. Pharmacogenomics J. 2008;8:122–128. doi:10.1038/sj.tpj.6500447
57. David SP, Strong DR, Munafo MR, et al. Bupropion efficacy for smoking cessation is influenced by the DRD2 Taq1A polymorphism: analysis of pooled data from two clinical trials. Nicotine Tob Res. 2007;9:1251–1257. doi:10.1080/14622200701705027
58. Gold SJ, Han MH, Herman AE, et al. Regulation of RGS proteins by chronic morphine in rat locus coeruleus. Eur J Neurosci. 2003;17:971–980. doi:10.1046/j.1460-9568.2003.02529.x
59. Stanwood GD, Parlaman JP, Levitt P. Genetic or pharmacological inactivation of the dopamine D1 receptor differentially alters the expression of regulator of G-protein signalling (Rgs) transcripts. Eur J Neurosci. 2006;24:806–818. doi:10.1111/j.1460-9568.2006.04970.x
60. Schwendt M, Hearing MC, See RE, McGinty JF. Chronic cocaine reduces RGS4 mRNA in rat prefrontal cortex and dorsal striatum. Neuroreport. 2007;18:1261–1265. doi:10.1097/WNR.0b013e328240507a
61. Zachariou V, Georgescu D, Sanchez N, et al. Essential role for RGS9 in opiate action. Proc Natl Acad Sci USA. 2003;100:13656–13661. doi:10.1073/pnas.2232594100
62. Backtell RA, Choi KH, Simmons DL, et al. Role of GluR1 expression in nucleus accumbens neurons in cocaine sensitization and cocaine-seeking behavior. Eur J Neurosci. 2008;27:2229–2240. doi:10.1111/j.1460-9568.2008.06199.x
63. Klebaur JE, Ostrander MM, Norton CS, Watson SJ, Akil H, Robinson TE. The ability of amphetamine to evoke arc (Arg 3.1) mRNA expression in the caudate, nucleus accumbens and neocortex is modulated by environmental context. Brain Res. 2002;930:30–36. doi:10.1016/s0006-8993(01)03400-x
64. Zavala AR, Osredkar T, Joyce JN, Neisewander JL. Upregulation of Arc mRNA expression in the prefrontal cortex following cue-induced reinstatement of extinguished cocaine-seeking behavior. Synapse. 2008;62:421–431. doi:10.1002/syn.20502
65. Hearing MC, Miller SW, See RE, McGinty JF. Relapse to cocaine seeking increases activity-regulated gene expression differentially in the prefrontal cortex of abstinent rats. Psychopharmacology. 2008;198:77–91. doi:10.1007/s00213-008-1090-2
66. Ostrander MM, Badiani A, Day HE, et al. Environmental context and drug history modulate amphetamine-induced c-fos mRNA expression in the basal ganglia, central extended amygdala, and associated limbic forebrain. Neuroscience. 2003;120:551–571. doi:10.1016/s0306-4522(03)00247-1
67. Carta AR, Moreno CC, Cadoni C, Tronci E, Di CG. Long-term increase in GAD67 mRNA expression in the central amygdala of rats sensitized by drugs and stress. Eur J Neurosci. 2008;27:1220–1230. doi:10.1111/j.1460-9568.2008.06095.x
68. Krishnan HR, Al-Hasan YM, Pohl JB, Ghezzi A, Atkinson NS. A role for dynamin in triggering ethanol tolerance. Alcohol Clin Exp Res. 2012;36(1):24–34. PMID: 21797886; PMCID: PMC3208067. doi:10.1111/j.1530-0277.2011.01587.x
69. Blum K, Downs BMW, Dushaj K, et al. The benefits of customized DNA directed nutrition to balance the brain reward circuitry and reduce addictive behaviors. Precis Med. 2016;1(1):18–33. PMID: 28066828; PMCID: Pmc5210211.
70. Czarnecki D, Ziółkowski M, Chodkiewicz J, et al. Initial study on COMT and DRD2 gene polymorphisms as well as the influence of temperament and character trait on the severity of alcohol craving in alcohol-dependent patients. J Clin Med. 2021;10(24):5892. PMID: 34945190; PMCID: PMC8704345. doi:10.3390/jcm10245892
71. Blednov YA, Benavidez JM, Black M, et al. GABAA receptors containing ρ1 subunits contribute to in vivo effects of ethanol in mice. PLoS One. 2014;9(1):e85525. PMID: 24454882; PMCID: PMC3894180. doi:10.1371/journal.pone.0085525
72. Blum K, Oscar-Berman M, Stuller E, et al. Neurogenetics and nutrigenomics of neuro-nutrient therapy for reward deficiency syndrome (RDS): clinical ramifications as a function of molecular neurobiological mechanisms. J Addict Res Ther. 2012;3(5):139. PMID: 23926462; PMCID: PMC3733258. doi:10.4172/2155-6105.1000139
73. Archer T, Oscar-Berman M, Blum K, Gold M. Neurogenetics and epigenetics in impulsive behavior: impact on reward circuitry. J Genet Syndr Gene Ther. 2012;3(3):1000115. PMID: 23264884; PMCID: PMC3526005. doi:10.4172/2157-7412.1000115
74. Gold MS, Blum K, Febo M, et al. Molecular role of dopamine in anhedonia linked to reward deficiency syndrome (RDS) and anti- reward systems. Front Biosci. 2018;10(2):309–325. PMID: 29293435. doi:10.2741/s518
75. Ornell F, Scherer JN, Schuch JB, et al. Serum BDNF levels increase during early drug withdrawal in alcohol and crack cocaine addiction. Alcohol. 2023;111:1–7. Epub 2023 Apr 8. PMID: 37037287. doi:10.1016/j.alcohol.2023.04.001
76. Blum K, Bowirrat A, Baron D, et al. Identification of stress-induced epigenetic methylation onto dopamine D2 gene and neurological and behavioral consequences. Gene Protein Dis. 2024;3(1):10–36922. PMID: 38766604; PMCID: PMC11100097. doi:10.36922/gpd.1966
77. Hou G, Hao M, Duan J, Han MH. The formation and function of the VTA dopamine system. Int J Mol Sci. 2024;25(7):3875. PMID: 38612683; PMCID: PMC11011984. doi:10.3390/ijms25073875
78. Bowirrat A, Elman I, Dennen CA, et al. Neurogenetics and Epigenetics of Loneliness. Psychol Res Behav Manag. 2023;16:4839–4857. PMID: 38050640; PMCID: PMC10693768. doi:10.2147/PRBM.S423802
79. van Roekel E, Goossens L, Scholte RH, Engels RC, Verhagen M. The dopamine D2 receptor gene perceived parental support, and adolescent loneliness: longitudinal evidence for gene-environment interactions. J Child Psychol Psychiatr. 2011;52(10):1044–1051. PMID: 21675993. doi:10.1111/j.1469-7610.2011.02424.x
80. Blum K, Steinberg B, Gondre-Lewis MC, et al. A review of DNA risk alleles to determine epigenetic repair of mRNA expression to prove therapeutic effectiveness in reward deficiency syndrome (RDS): embracing “Precision Behavioral Management”. Psychol Res Behav Manag. 2021;14:2115–2134. PMID: 34949945; PMCID: PMC8691196. doi:10.2147/PRBM.S292958
81. Witt SH, Frank J, Frischknecht U, et al. Acute alcohol withdrawal and recovery in men lead to profound changes in DNA methylation profiles: a longitudinal clinical study. Addiction. 2020;115(11):2034–2044. PMID: 32080920. doi:10.1111/add.15020
82. Li Y, Re GF, Zhao Y, et al. Messenger RNA expression profiles and bioinformatics analysis of mouse hippocampi during exercise alleviates methamphetamine dependence via mRNA profile change in hippocampi. Ann Transl Med. 2022;10(18):957. PMID: 36267776; PMCID: PMC9577721. doi:10.21037/atm-22-450
83. Weitzman ER, Blakemore LM, Pierce SE, Kossowsky J, Levy S. Returning genetic information about risk for alcohol use disorder to adolescents: findings of a preliminary qualitative study of precision prevention. AJPM Focus. 2023;3(1):100153. PMID: 38089426; PMCID: PMC10711383. doi:10.1016/j.focus.2023.100153
84. Keller A, Bosk EA, Mendez A, et al. Exploring perceptions of genetic risk and the transmission of substance use disorders. Addict Sci Clin Pract. 2024;19(1):57. PMID: 39095898; PMCID: PMC11295387. doi:10.1186/s13722-024-00470-w
85. Hendy K. Media framings of the role of genomics in “addiction” in the United States from 2015 to 2019: individualized risk, biomedical expertise, and the limits of destigmatization. Public Underst Sci. 2024;33(2):158–173. PMID: 37658669. doi:10.1177/09636625231190743
86. Lebowitz MS, Appelbaum PS. Beneficial and detrimental effects of genetic explanations for addiction. Int J Soc Psychiatry. 2017;63(8):717–723. PMID: 29058960; PMCID: PMC5693609. doi:10.1177/0020764017737573
87. Kelly JF, Greene MC, Abry A. A US national randomized study to guide how best to reduce stigma when describing drug-related impairment in practice and policy. Addiction. 2021;116(7):1757–1767. doi:10.1111/add.15333
88. Rundle SM, Cunningham JA, Hendershot CS. Implications of addiction diagnosis and addiction beliefs for public stigma: a cross-national experimental study. Drug Alcohol Rev. 2021;40(5):842–846. doi:10.1111/dar.13244
89. Pennington CR, Monk RL, Heim D, et al. The labels and models used to describe problematic substance use impact discrete elements of stigma: a registered report. Psychol Addict Behav. 2023;37(6):723–733. doi:10.1037/adb0000919
90. Rey CN, Kurti AN, Badger GJ, Cohen AH, Heil SH. Stigma, discrimination, treatment effectiveness, and policy support: comparing behavior analysts’ views on drug addiction and mental illness. Behav Anal Pract. 2019;12(4):758–766. PMID: 31976287; PMCID: PMC6834810. doi:10.1007/s40617-019-00345-6
91. Szutorisz H, Hurd YL. Overcoming addiction stigma: epigenetic contributions to substance use disorders and opportunities for intervention. Neuron. 2022;110(10):1611–1614. PMID: 35413242. doi:10.1016/j.neuron.2022.03.018
92. Wiss DA, Avena N, Gold M. Food addiction and psychosocial adversity: biological embedding, contextual factors, and public health implications. Nutrients. 2020;12(11):3521. PMID: 33207612; PMCID: PMC7698089. doi:10.3390/nu12113521
93. Buchman D, Reiner PB. Stigma and addiction: being and becoming. Am J Bioeth. 2009;9(9):18–19. PMID: 19998183; PMCID: PMC2791913. doi:10.1080/15265160903090066
94. Sugarman DE, Meyer LE, Reilly ME, Greenfield SF. Women’s and men’s experiences in group therapy for substance use disorders: a qualitative analysis. Am J Addict. 2022;31(1):9–21. PMID: 34730866; PMCID: PMC8799487. doi:10.1111/ajad.13242
95. Zeine F, Jafari N, Manoukian E, Blum K. Addictive behavior and evolutionary adaptation: mitigated through genetic addiction risk severity early identification and Awareness Integration Theory. Med Res Arch. 2024;12(8). doi:10.18103/mra.v12i8.5702
96. Zeine F. Awareness Integration: a new therapeutic model. Int J Emerg Ment Health Hum Resilience. 2016;16:60–65.
97. Zeine F, Jafari N, Haghighatjoo F. Awareness Integration: an alternative therapeutic methodology to reducing depression and anxiety while improving low self-esteem and self- efficacy in separated or divorced individuals. Ment Health Fam Med. 2017;13(2):451–458.
98. Zeine F, Jafari N, Forouzesh M. Awareness integration: a non-invasive recovery methodology in reducing college student anxiety, depression, and stress. TOJET. 2017; Special Issue for IETC (2017):105-114. Presented at Harvard University. Available from: www.tojet.net/special/2017_11_1.pdf.
99. Madani H, Zeine F. Awareness integration therapy for generalized anxiety disorder. Int J Psychol Res. 2023;5(4):1–7.
100. Zarbakhsh L, Zeine F. Awareness integration theory case report: therapeutic intervention for anxiety and depression in a transsexual male college student. Int J Sci Res. 2023;12(3):73–77.
101. Zeine F, Changizi S. Enhancing mental health support: integrating artificial intelligence–powered mobile apps and chatbots for psychoeducation and skill-building. Med Res Arch. 2025;13(5). doi:10.18103/mra.v13i5.6513
102. Zeine F, Jafari N, Manoukian E, et al. A multidisciplinary exploration of self-identity development: applying awareness integration theory in psychopathology and genetic research. Med Res Arch. 2025;13(3). doi:10.18103/mra.v13i3.6294
103. Danpanichkul P, Díaz LA, Suparan K, et al. Global epidemiology of alcohol-related liver disease, liver cancer, and alcohol use disorder, 2000-2021. Clin Mol Hepatol. 2025;31(2):525–547. Epub 2025 Jan 9. PMID: 39788109; PMCID: PMC12016609. doi:10.3350/cmh.2024.0835
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Updated Perspectives on the Neurobiology of Substance Use Disorders Using Neuroimaging
Murnane KS, Edinoff AN, Cornett EM, Kaye AD
Substance Abuse and Rehabilitation 2023, 14:99-111
Published Date: 10 August 2023
Chronic Methylphenidate Effects on Brain Gene Expression: An Exploratory Review
Klein SR, Blum K, Gold MS, Thanos PK
Psychology Research and Behavior Management 2024, 17:577-592
Published Date: 15 February 2024