Back to Journals » International Journal of General Medicine » Volume 19
Beyond Inflammation: A Comprehensive Outlook on the Integrated Traditional Chinese and Western Medicine Treatment of Pelvic Inflammatory Disease
Received 22 September 2025
Accepted for publication 15 January 2026
Published 17 February 2026 Volume 2026:19 569421
DOI https://doi.org/10.2147/IJGM.S569421
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Woon-Man Kung
Siqin Yang,1 Qian Zeng2
1Clinic Medical School, Chengdu University of Traditional Chinese Medicine, Chengdu, 610075, People’s Republic of China; 2Gynecology, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, 610075, People’s Republic of China
Correspondence: Qian Zeng, Gynecology, Hospital of Chengdu University of Traditional Chinese Medicine, No. 39, Shierqiao Road, Jinniu District, Chengdu, Sichuan, 610075, People’s Republic of China, Email [email protected]
Abstract: Pelvic inflammatory disease (PID) is an inflammatory process of the upper genital tract that is mainly caused by sexually transmitted infections (STI). It can cause tubal factor infertility, ectopic pregnancy, or chronic pelvic pain. In recent years, its incidence has increased annually owing to various factors, such as sexually transmitted diseases and intrauterine surgery. Although empirical treatment, such as antibiotics or surgery, can alleviate the symptoms of pelvic inflammatory disease, the obstetric outcome is not ideal and the recurrence rate is high, which places a heavy physical and mental burden on women. Traditional Chinese medicine (TCM) is a complementary therapy to Western medicine that has a complete theoretical and practical system and has attracted international attention because of its excellent curative effect. An increasing number of people are accepting and trying to use traditional Chinese medicine to treat gynecological diseases, including infertility, polycystic ovary syndrome, and PID; however, its efficacy and mechanism are still controversial. Therefore, this article summarizes the related research on traditional Chinese medicine and Western medicine in the treatment of PID for clinical reference.
Keywords: pelvic inflammatory disease, epidemiology, pathological mechanism, TCM treatment, Western medicine treatment
Introduction
Pelvic inflammatory disease (PID) is a general term for inflammatory diseases of the female upper genital tract caused by microbial pathogens, including those of the uterus, fallopian tubes, ovaries, and pelvic peritoneum, with clinical manifestations of fever, lower abdominal pain, abdominal distension, vaginal secretion, and abnormal bleeding.1 In traditional Chinese medicine, pelvic inflammatory disease is usually attributed to “leukorrhagia” and “women’s abdominal pain”, mainly due to damp-heat, blood stasis, qi stagnation and so on.2 At present, the treatment of PID mainly includes drug, physical, and surgical treatment, but the complex etiology and pathological mechanism of PID, non-specific clinical signs, and lack of rapid diagnosis make it difficult for a single treatment method to deal with.3 Combination therapy has become an important research direction to solve this problem; in particular, the combination therapy of antibiotics and other drugs (such as traditional Chinese medicine and physical therapy) has attracted wide attention.4 This combination therapy not only covers a variety of pathogens and inhibits the inflammatory response but also improves clinical efficacy and reduces drug resistance through synergistic effects.5 This article reviews the research progress of PID combined therapy in recent years and explores the synergistic mechanism and clinical application potential of integrated traditional Chinese and western medicine treatment to provide a reference for optimizing the treatment strategy of PID.
Methods
Literature Search Strategy
A systematic literature search was performed in electronic databases, including PubMed, Web of Science, the Cochrane Library, China National Knowledge Infrastructure (CNKI), and Wanfang Data. The search covered publications from January 2000 to December 2024. Search terms included combinations of keywords and Medical Subject Headings (MeSH) terms related to “pelvic inflammatory disease,” “traditional Chinese medicine,” “Chinese herbal medicine,” “acupuncture,” “integrated medicine,” “pathogenesis,” “treatment,” and “clinical trial.” The reference lists of retrieved articles were also manually screened for additional relevant studies.
Study Selection and Eligibility Criteria
Studies were considered eligible if they: (1) investigated PID in human subjects or relevant animal models; (2) involved interventions of Western medicine (eg, antibiotics, surgery), TCM therapies (eg, herbal formulas, patent medicines, acupuncture), or their combination; (3) reported on epidemiology, pathogenesis, treatment efficacy, or mechanistic insights; and (4) were published in English or Chinese. No restrictions were placed on study design at the initial stage to capture a broad spectrum of evidence, including randomized controlled trials (RCTs), observational studies, basic science research, and systematic reviews. Comments, editorials, and non-peer-reviewed articles were excluded.
Study Screening and Data Extraction
Two authors (S.Y. and Q.Z.) independently screened the titles and abstracts of identified records against the eligibility criteria. Full texts of potentially relevant articles were then retrieved and assessed independently. Any disagreements during screening were resolved through discussion or consultation with a third researcher. Data from included studies were extracted using a standardized form, capturing information on authors, publication year, study design, sample characteristics, interventions, comparisons, main outcomes, and key findings.
Data Synthesis and Quality Assessment
Given the anticipated heterogeneity in study designs, interventions, and outcome measures across the included literature—encompassing both clinical studies and basic research—a quantitative meta-analysis (statistical pooling) was deemed inappropriate (therefore, statistical analysis was not applicable). Consequently, a narrative synthesis approach was adopted. Extracted data were organized thematically according to the main review sections: epidemiology, pathogenesis, Western medicine treatment, and TCM treatment (subdivided into oral formulas, patent medicines, and external therapies). Findings were summarized, compared, and synthesized to identify patterns, consistencies, and gaps in the current evidence base.
Epidemiology of Pelvic Inflammatory Disease
The current data on the global epidemiology of PID are limited. The 2013–2016 American Health and Nutrition Examination Survey and 2015–2017 American Family Growth Survey reported that the self-reported history of PID in women aged 18–44 years was 4.1% (95% CI, 3.2% – 5.1%) and 3.6% (95% CI, 2.9% – 4.5%), respectively.5,6 In another study, a national dataset for the UK from 2009 to 2019 observed a 39% decline in the diagnosis of PID over the decade, especially PID caused by Chlamydia and gonococcus.7 We believe that extensive chlamydial screening and prompt treatment may be the main reasons for the large decline in chlamydial PID. In a meta-analysis of studies published from 1990 to 2019, it was found that the ASR (age-standardized rates) of the global prevalence of PID in women of childbearing age in 2019 was 53.19 per 100000. Compared with 1990 (estimated annual percentage changes: − 0.50),8 the infection rate of women aged 16–24 dropped to about 35%, and the infection rate of women aged 25–44 dropped to about 11%.9,10 However, some studies have shown that these epidemiological studies were from high-income populations. For most populations in low-income and middle-income countries, epidemiological data on pelvic inflammatory disease and its sequelae are still missing,8 and the epidemiological situation may vary with subtle changes in pathogens and the socio-economic development of the country. Despite the overall downward trend in the incidence of PID, the direct medical costs associated with PID and its sequelae are estimated to be more than $2.4 billion in the United States,11–13 while the average cost of a simple PID episode in the United Kingdom is £ 163.14 Pelvic inflammatory disease remains a disease with a huge global burden and an urgent need for prevention.
Morbidity Mechanism of Pelvic Inflammatory Disease
Ascending Infection of Pathogen
The types of pathogens are divided into two categories: (1) STI pathogens, including Chlamydia trachomatis, Neisseria gonorrhoeae, Mycoplasma genitalium, and Trichomonas vaginalis. The former two are the main exogenous pathogenic microorganisms causing acute PID.15 (2) opportunistic pathogens, and more than half of PID cases are non-gonococcal and non-chlamydial. There are mainly anaerobic bacteria from the vaginal flora (eg, Prevotella, Peptostreptococcus), gram-negative bacilli, and bacterial vaginosis-associated microorganisms (Lactobacillus, Gardnerella vaginalis, Mycoplasma hominis, anaerobic gram-negative bacilli, and, to a lesser extent, Ureaplasma urealyticum).16 A longitudinal study found that BV-associated bacteria in the vagina were also associated with a doubled risk of developing PID.17 These endogenous bacteria usually multiply after an imbalance in vaginal microecology and are prone to mixed infections.
The pathogen ascends, the host defense barrier breaks down, and the pathogen colonizes the lower genital tract. Under normal circumstances, the cervical mucus plug, the acidic environment of the vagina, and local immune defense can prevent its further spread.18 Sexually transmitted pathogens such as Neisseria gonorrhoeae and Chlamydia trachomatis have strong adhesion and invasion abilities, which can induce cell damage and apoptosis by binding to epithelial cell receptors through adhesion molecules, thus breaking through the epithelial barrier.15 Cervical barrier function is weakened after menstruation, IUD placement, delivery, or induced abortion. Pathogens break through the cervical mucus barrier and ascend to the endometrium, causing endometritis, and then continue to spread to the fallopian tube, causing salpingitis, which is the most common pathological manifestation of PID.4 Further inflammation can spread to the ovaries (forming tubo-ovarian abscesses), pelvic peritoneum (pelvic peritonitis), and even the liver capsule (Fitz-Hugh-Curtis syndrome).
Immune Inflammatory Response
Successful colonization and ascension of pathogens are closely related to the functional status of the host immune system. The first is activation of harmful immunity. Pathogens and their products (such as lipopolysaccharides and lipooligosaccharides), as pathogen-associated molecular patterns (PAMPs), are recognized by pattern recognition receptors (such as Toll-like receptors (TLRs)) on the surface of host immune cells (such as macrophages and epithelial cells)19 and activate key signaling pathways such as NF-κB. Triggers the release of large amounts of pro-inflammatory cytokines (eg, TNF-α, IL-1β, IL-6) and chemokines (eg, IL-8). This leads to the infiltration of inflammatory cells such as neutrophils and macrophages. Second, some pathogens can also suppress protective immunity, especially Chlamydia trachomatis, showing a unique biphasic developmental cycle that can evade host immune clearance and lead to persistent infection.20 Opa proteins on N. gonorrhoeae interact with CEACAM1, inactivate CD4 + T cells, and inhibit the intracellular neutrophil killing mechanism by interacting with CEACAM3 on neutrophils.21 Chronic antigen stimulation and metabolic reprogramming further lead to T-cell failure. Inhibition of mitochondrial oxidative phosphorylation in T cells upregulates genes associated with immune exhaustion and cell death, resulting in the inability of T cells to effectively eliminate pathogens and lose their ability to form memory.22–24
Tissue Damage and Sequelae Formation
If acute inflammation is not effectively controlled over time, it can progress to irreversible tissue damage. When pathogens enter the uterus and fallopian tubes, epithelial and immune cells release inflammatory mediators, resulting in mucosal edema, increased vascular permeability, and leukocyte infiltration.25,26 While neutrophils and macrophages try to remove pathogens, they also cause tissue congestion, edema, exudation, and suppuration, and the clinical signs include acute lower abdominal pain, fever, and abnormal secretion.27 With recurrence and persistence of inflammation, inflammatory exudation occurs in local tissues, and the uterus, fallopian tubes, ovaries, intestines, and greater omentum adhere to each other, forming extensive pelvic adhesions. Pus accumulates in the fallopian tube cavity to form pyosalpinx or adheres and fuses with the ovary to form tubo-ovarian abscesses (TOA), which ultimately affects fertility.28 Delayed-type hypersensitivity and cellular immune response triggered by Chlamydia trachomatis are important mechanisms for severe injury of the tubal mucosa, loss of cilia function, and tubal fibrosis occlusion.29 This immune-mediated injury persists after the resolution of acute infection and is critical for the sequelae of PID. (See Figure 1).
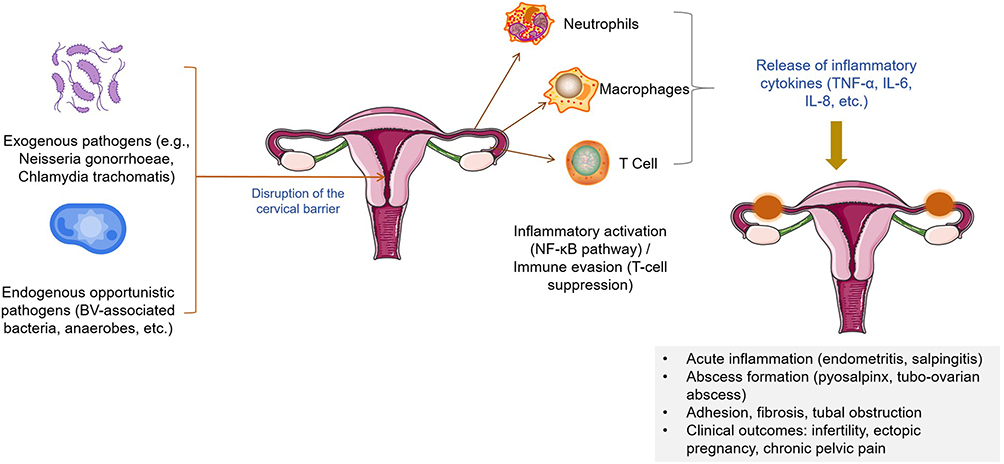 |
Figure 1 Pathogenesis of pelvic inflammatory disease (PID). Exogenous pathogens (eg, Neisseria gonorrhoeae, Chlamydia trachomatis) and endogenous opportunistic bacteria (eg, BV-associated bacteria, anaerobes) ascend through a disrupted cervical barrier. Pathogen recognition via Toll-like receptors activates NF-κB signaling, inducing infiltration of immune cells and release of pro-inflammatory cytokines (TNF-α, IL-6, IL-8). Some pathogens evade immunity through T-cell suppression, leading to persistent infection. Uncontrolled inflammation results in endometritis, salpingitis, abscess formation, pelvic adhesions, and fibrosis, ultimately causing infertility, ectopic pregnancy, and chronic pelvic pain. |
Western Medicine Treatment
Antibiotic Treatment
Antibiotics are the cornerstone of PID treatment. As PID is mostly a mixed infection, an empirical combination of drugs is recommended in clinical practice. The guiding principle for the selection of antimicrobial therapy for PID is that the protocol should cover N. gonorrhoeae and C. trachomatis, regardless of the results of diagnostic tests for these pathogens.30 The current CDC guidelines state that a combination of oral and parenteral regimens should be used in the outpatient setting for mild-to-moderate infections. Severe PID should be treated with a complete parenteral regimen for at least 24–72 hours on a hospital basis. There was no difference in the incidence of short-term clinical and microbiological improvement or subsequent infertility, recurrent PID, chronic pelvic pain (CCP), or ectopic pregnancy between women hospitalized for PID and women treated as outpatients.11 The US CDC (2021) guidelines recommend ceftriaxone plus doxycycline ± metronidazole as first-line therapy (Table 1).31 The addition of metronidazole to treatment is usually at the discretion of the attending physician, but a randomized controlled trial demonstrated that the conventional antibiotic plus metronidazole regimen was superior to the antibiotic plus placebo in reducing pain and improving pathogen clearance.32 Another trial of parenteral combination oral azithromycin, either as monotherapy or in combination with doxycycline and metronidazole, showed clinical survival rates of 97–98% at 2 weeks post-treatment and a microbial survival rates of 90–94% at 6 weeks post-treatment. However, there was no statistically significant difference in clinical or microbiological survival rates when this regimen was compared with third-generation cephalosporin-based or parenteral amoxicillin-based regimens.33 Despite the use of multiple antibiotic regimens and routes of administration (intravenous, intramuscular, or oral), the optimal combination of drugs remains unknown. Ginecologia, which included 6894 women to assess the optimal treatment for PID, could not prove that one treatment was superior to other treatments or safer and more effective in curing mild to moderate or severe PID, but found that it was more effective than tetracycline (doxycycline), based on a single study with a low risk of bias. Macrolides (azithromycin) may increase the survival rate of mild-to-moderate PID.34 In addition, fluoroquinolones can be used in allergic patients, but the risk of drug resistance should be noted. Attention should be paid to the simultaneous treatment of sexual partners; even if the sexual partners are asymptomatic, empirical treatment should be carried out with effective regimens for gonorrhea and chlamydia.
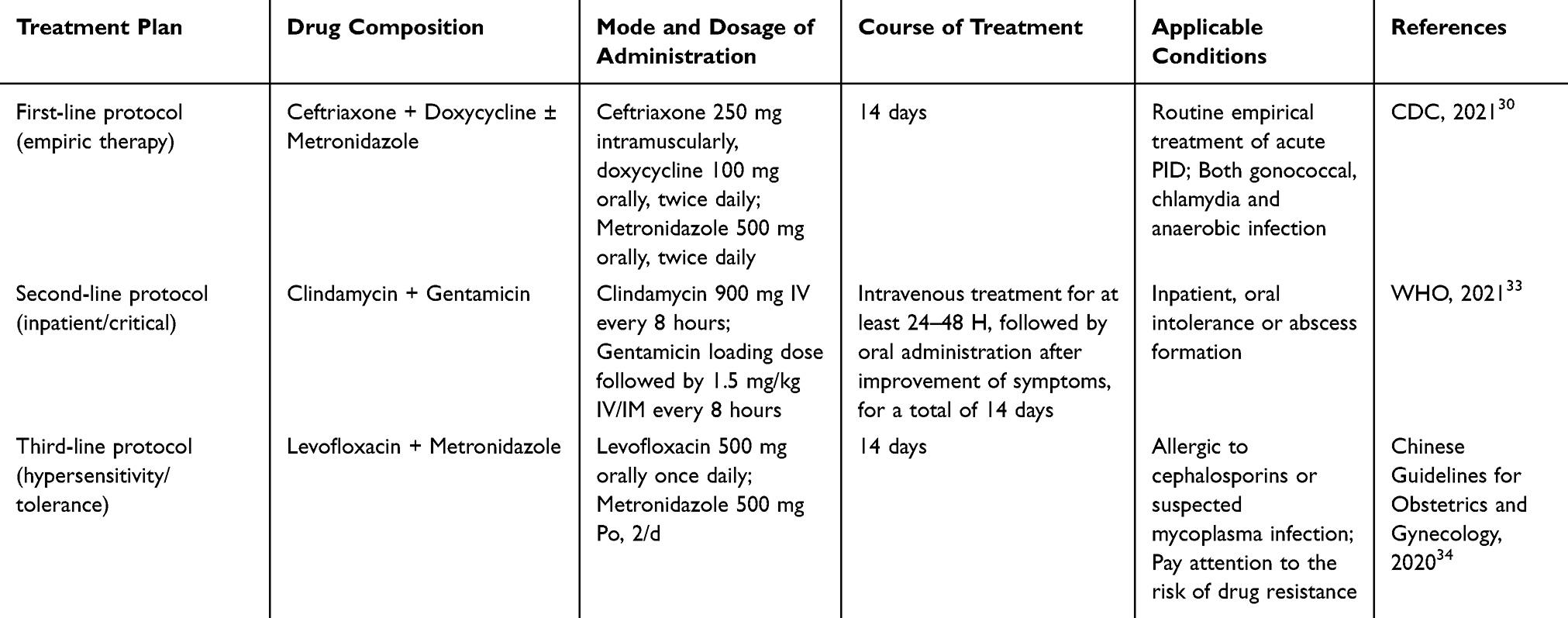 |
Table 1 Antibiotic Treatment for PID |
Physical and Adjuvant Therapy
The long-term use of antibiotics is facing problems of increasing drug-resistant strains and high recurrence rates. In recent years, researchers have tried to use physical therapy, anti-inflammatory drugs, immunomodulators, and probiotics in the treatment of PID to alleviate inflammatory injury and restore the balance of the reproductive tract microecology. Physical therapy mainly includes ozone, ultrasound, and infrared radiation, which can improve local blood circulation and promote inflammatory absorption. The effect of ozone therapy on the inflammatory process in PID has been evaluated, showing that inflammation can be gradually reduced by reducing the concentration of proinflammatory interleukin 6 and improving the sonographic features of PID.35 Laser biostimulation of neurogenically sensitized acupoints significantly improves pain perception, intensity, and quality of life in women with CPP.36 Nonsteroidal anti-inflammatory drugs (NSAIDs) are commonly used to relieve pain and inflammation. Short-term and combined use of antibiotics can safely and effectively improve the symptoms of patients, but it is necessary to be alert to their adverse reactions to the digestive tract and kidneys.37 Psychological intervention and rehabilitation training can be considered to improve the quality of life of patients with recurrent attacks or combined with CCP.38,39 In addition, some studies have reported that intrauterine perfusion and pelvic irrigation can assist in controlling infection, but their efficacy and safety remain controversial.40
Surgical Treatment
Surgical treatment should be considered when medical treatment is ineffective or when serious complications such as TOA rupture, extensive pelvic adhesions, or persistent chronic pain occur.28 Minimally invasive laparoscopic exploration is not only helpful in making a definite diagnosis but also feasible for adhesion release, abscess drainage, or lesion resection. A cohort study showed that the complication rate of laparoscopy was lower than that of open surgery in a matched cohort of patients undergoing acute PID surger.41 In young women with clear fertility requirements, the fallopian tube and ovarian tissue should be preserved as far as possible during the operation to reduce damage to reproductive function. (See Figure 2).
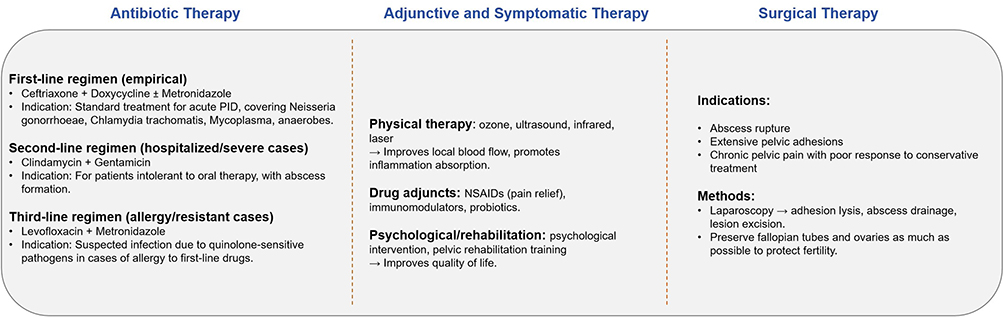 |
Figure 2 Western medicine treatment strategies for PID. Antibiotics remain the cornerstone of therapy, including first-line empirical regimens (ceftriaxone + doxycycline ± metronidazole), second-line regimens for hospitalized/severe cases (clindamycin + gentamicin), and third-line regimens for allergy/resistant cases (levofloxacin + metronidazole). Adjunctive therapies include physical modalities (ozone, ultrasound, infrared, laser), NSAIDs, immunomodulators, probiotics, as well as psychological interventions and pelvic rehabilitation. Surgical treatment is indicated for abscess rupture, extensive adhesions, or refractory chronic pelvic pain, typically performed laparoscopically with adhesion lysis, abscess drainage, and lesion excision while preserving fertility when possible. |
Traditional Chinese Medicine Treatment
Treatment of Pelvic Inflammatory Disease with Oral Chinese Medicine Compound Formula (CMCF)
CMCF has multiple effects, such as anti-inflammatory effects, immune regulation, and tissue repair, due to the compatibility of multiple drugs. An increasing number of randomized controlled trials have shown that oral CMCF combined with conventional therapy for PID can greatly improve clinical efficiency and reduce adverse reactions and recurrence rate.42 Traditional Chinese medicine treatment of pelvic inflammatory disease in the acute stage is mostly from the perspective of “damp-heat stasis” and “excessive toxic heat”, while in the sequelae stage, it is mostly from the syndrome differentiation of “qi stagnation and blood stasis”, “cold-dampness stagnation”, and “qi deficiency and blood stasis”. Li et al43 found that Longdan Xiegan Decoction combined with antibiotics was superior to metronidazole alone in improving symptoms such as distending pain in the lower abdomen, lumbosacral distending pain, excessive leucorrhea, yellow odor, and fatigue in patients with PID of heat and blood stasis PID. Jia used the modified Danggui Shaoyao Powder for pelvic inflammatory disease of damp heat and blood stasis type, and the results showed that Danggui Shaoyao Powder could also improve local symptoms, such as lower abdominal pain and lumbosacral discomfort, and improve the quality of life of patients.44 Xu et al found that the combination of Qingre Huashi Tongluo Decoction, ceftriaxone, and doxycycline had a synergistic effect in the treatment of acute PID of the damp-heat accumulation type, and the time for abdominal pain to disappear and body temperature to return to normal was significantly shortened, and the inflammation-related indicators were significantly reduced.45 Zhang used a Qingjie Mixture for PID with excessive toxic heat. After the course of treatment, the cure rate in the treatment group was higher than that in the control group. The Qingjie Mixture not only reduces pelvic effusion but also promotes the absorption of pelvic inflammatory masses.46 Caulis Lonicerae, Folium Isatidis, and Flos Chrysanthemi Indici have heat-clearing and detoxifying effects, and pharmacological studies have shown that they have different degrees of bacteriostatic and anti-inflammatory effects.47–49 Salpingitis, the main ingredients of Herba Violae and Herba Taraxaci, can improve salpingitis.50 Yan observed the treatment of sequelae of pelvic inflammatory disease of qi stagnation and blood stasis type by Liqi Zhuyu Decoction compared with Sanjie Zhentong Capsule, and found that the levels of serum pain mediators and hydrosalpinx in both groups decreased after treatment, and the effect of Liqi Zhuyu Decoction was better, but the improvement of pelvic effusion in both groups was similar.51 For the treatment of PID due to qi deficiency and blood stasis, Li used Yiqi Huoxue Prescription, and the results showed that symptoms such as limitation of uterine activity or tenderness, bilateral adnexal masses, tenderness, thickening, and tenderness of uterosacral ligaments were significantly improved, and irregular menstruation, fatigue, anorexia, low fever, and pain during sexual intercourse were also improved.52 (Table 2) Liu used the Lizhong Decoction, and the results showed that the cure rates of the treatment and control groups were 25.0% and 15.63%, respectively, and the total efficacy rates were 90.63% and 75.0%, respectively.53 The Wenjing Decoction is often used to treat cold-dampness stagnation-type PID. Gong found that the time of pelvic mass regression, the duration of pelvic pain, and the time of normal menstruation in patients taking Wenjing Decoction combined with fleroxacin were significantly shorter than those in patients taking fleroxacin alone.54 (See Figure 3 for details of the above prescriptions). Animal experiments have also provided evidence for the oral administration of compound Chinese medicines. Bu found that the administration of Danzhi Decoction accelerated pelvic blood flow and reduced the expression of VEGF, Ang-2, and OPN in the upper genital tract, which could effectively reduce CCP in pelvic inflammatory mice and improve the hemodynamics of the pelvic blood stasis microenvironment.55 The Shipi Shugan Decoction significantly reduces the infiltration of inflammatory cells in the upper genital tract, inhibits mitochondrial dysfunction and oxidative stress, and inhibits inflammatory damage in the uterus and fallopian tubes.56 Systematic reviews and meta-analyses of oral Chinese medicine in the treatment of PID have been published. Although these studies have different risks of bias, the conclusion still provides strong evidence for the use of compound Chinese medicine in the treatment of pelvic inflammatory diseases.
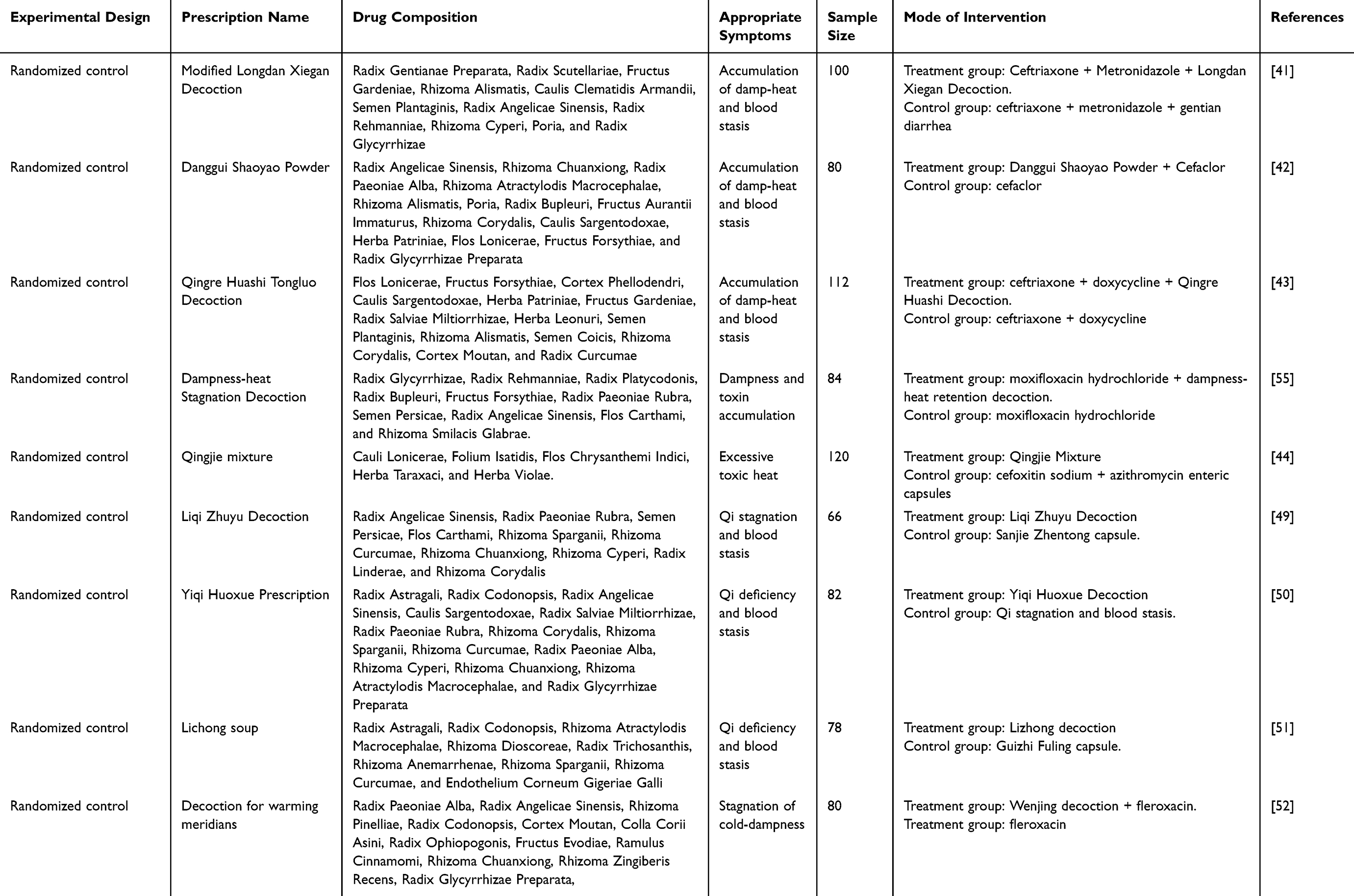 |
Table 2 Treatment of PID of Each Syndrome Type by Oral Administration of Compound Chinese Medicine |
 |
Figure 3 Traditional Chinese medicine (TCM) treatment strategies for PID. Herbal compound decoctions are tailored to syndrome differentiation: in the acute phase, heat-clearing and detoxifying formulas (eg, Longdan Xiegan Decoction, Qingre Jiedu) aim to resolve dampness and discharge; in the chronic/sequelae phase, formulas for Qi regulation and blood activation, Qi tonification and blood activation, or warming the meridians are applied. Chinese patent medicines such as Jinying capsules, Kangfuyan capsules, and Fuke Qianjin tablets provide anti-inflammatory and antifibrotic effects and reduce recurrence. External therapies include herbal retention enemas, acupuncture, moxibustion, and acupoint patches. TCM exerts multi-target actions by reducing inflammation, modulating immunity, improving microcirculation, and preventing fibrosis. |
Treatment of PID with Chinese Patent Medicine
A double-blind, multicenter, randomized, placebo-controlled clinical trial of 155 patients diagnosed with PID identified the symptoms of damp-heat accumulation. After 28 days of treatment, Jinying capsule was found to reduce the dosage of antibiotics needed for PID treatment and improve the symptoms of PID patients. However, there was no statistically significant difference in physical and chemical indicators, such as white blood cell count, erythrocyte sedimentation rate, C-reactive protein, leucorrhea smear, and pelvic ultrasound.57 Feng et al conducted a randomized controlled trial and found that Fuyanshu capsules combined with levofloxacin and metronidazole could reduce the recurrence rate of pelvic inflammation and relieve pelvic pain and inflammatory status of patients by regulating the expression of IL-10 and IL-1β in peripheral serum.58 Wang compared the treatment of PID with ceftriaxone sodium + metronidazole alone and Kangfuyan capsules based on antibiotics. The results showed that the serum inflammatory factor levels of the two groups were significantly lower than before treatment (P < 0.05), and the improvement rate of the combined treatment group was significantly better than that of the control group (P < 0.05). Kangfuyan capsules combined with antibiotics can effectively relieve the symptoms and signs of patients, improve treatment efficiency, and prevent adverse reactions.59 Fuke Qianjin Capsule can improve the pathological damage of the uterus in rats with pelvic inflammatory disease, reduce the area of uterine fibrosis, inhibit the level of inflammatory factors and chemokines, regulate the immune system of the body, and may reduce the mortality of mixed infection.60 Xiong et al found that Fuke Qianjin Capsule could also inhibit inflammation and cell apoptosis and relieve endometritis through the TLR4/NF-κB/NLRP3 pathway.61
External Treatment of Traditional Chinese Medicine
External treatment with traditional Chinese medicine, such as enema of traditional Chinese medicine, acupoint application, acupuncture, and moxibustion, also shows the advantages of improving pain and regulating immunity in the clinic. Retention enemas with traditional Chinese medicine conform to the physiological and anatomical characteristics of the female pelvic cavity. Rectal administration can allow the drug to enter the internal iliac vein through the inferior rectal vein and/or anal vein and finally enter the systemic circulation, which can reduce the stimulation to the digestive system and avoid first-pass elimination to improve the bioavailability of the drug.62 Studies have confirmed that compared with 55 patients with conventional anti-inflammatory treatment, the effective rate of traditional Chinese medicine retention enema combined with anti-inflammatory treatment is significantly higher, and the decrease in serum TNF, IL-2, and IL-10 levels is statistically significant.63 However, only a very small number of patients had severe diarrhea and abdominal distension. Yi et al divided 240 CPP patients into a conventional antibiotic treatment group and an antibiotic combined acupuncture treatment group and found that the effective rate of the synergistic treatment group was 93.46%, while the effective rate of the control group was 79.70%. Combined acupuncture treatment not only effectively alleviated symptoms but also reduced the recurrence rate of symptoms and improved the overall quality of life of patients.64 Sixty women with PID were treated with retention enemas and moxibustion therapy. After 6 weeks, the low, medium and high shear rate parameters of whole blood in the PID group decreased from 12.32 ± 0.31, 6.66 ± 0.13 and 5.15 ± 0.52 to the normal levels of 9.19 ± 0.13, 5.42 ± 0.56 and 4.34 ± 0.43 (p < 0.05). The symptom score decreased from 13.73 ± 3.7 to 3.8 ± 1.4 (p < 0.05).65
Discussion
At present, the clinical treatment of PID mainly focuses on antibiotics, but the increase in drug resistance, high recurrence rate, and sequelae burden make it difficult for a single therapy to meet clinical needs. In recent years, the treatment of integrated traditional Chinese and Western medicine has gradually attracted attention. Western medicine has the advantages of rapid onset, clear pathogen, and effective control of acute infection. Traditional Chinese medicine treatment emphasizes overall regulation, focusing on improving the internal environment and immune balance of the body, especially in alleviating chronic inflammation, reducing recurrence, and improving quality of life and reproductive prognosis.42 These combinations have synergistic anti-inflammatory, antibacterial, immune regulation, and tissue repair effects, which may bring a new breakthrough in the treatment of PID. At the level of clinical research, randomized controlled trials and systematic reviews have shown that oral compound Chinese medicine, modified classical prescriptions, Chinese patent medicines, and external treatment can improve the symptoms of patients, reduce inflammatory indicators and recurrence rates to a certain extent, and have fewer adverse reactions.57,64,65 However, it should be noted that most of these studies had a limited sample size, some had insufficient design quality, and there was a certain risk of bias. Therefore, current evidence is insufficient to form a unified evidence-based conclusion. From the perspective of mechanistic research, traditional Chinese medicine and its compounds have certain effects in inhibiting the release of inflammatory factors, regulating the balance of Th17/Treg, improving local blood microcirculation, and alleviating tissue fibrosis,66 which are complementary to the direct antibacterial mechanism of Western medicine. However, most of these mechanisms remain in animal experiments or small-sample studies, lacking in-depth verification at the molecular level. For example, the key pathological basis of PID sequelae is chronic inflammation and fibrosis, and the role of traditional Chinese medicine in anti-fibrosis and the maintenance of immune homeostasis deserves further exploration. Future research directions should include multi-center, large-sample, randomized controlled studies to verify the efficacy and safety of integrated traditional Chinese and Western medicine treatment in different types of PID (acute, chronic, sequelae), strengthen the docking of basic research and clinical practice, promote the modernization of classical prescriptions and Chinese patent medicines, and enhance their standardization, standardization, and internationalization levels. (See Figure 4).
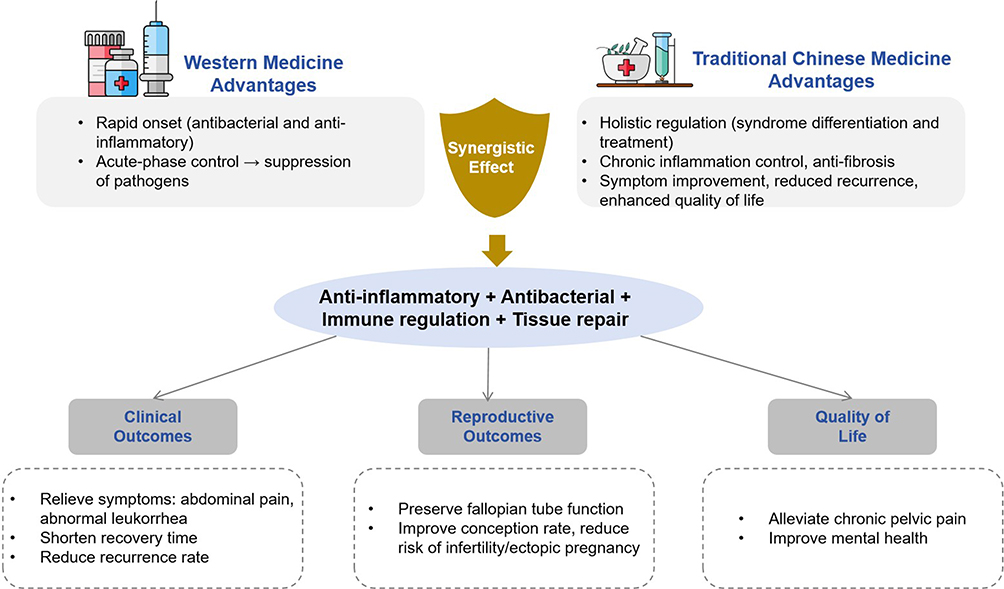 |
Figure 4 Integration of TCM and Western medicine in PID management and future perspectives. Western medicine provides rapid onset and acute-phase pathogen control, while TCM emphasizes holistic regulation, chronic inflammation control, antifibrosis, and quality-of-life improvement. Their synergistic effects—anti-inflammatory, antibacterial, immunoregulatory, and tissue repair—lead to clinical benefits such as symptom relief, shorter recovery, reduced recurrence, preservation of tubal function, improved fertility, and better quality of life. Future directions include large-scale randomized controlled trials, application of modern technologies (network pharmacology, omics, AI), standardization of herbal formulations, international collaboration, and precision medicine. |
Conclusion
The morbidity mechanism of PID is extremely complex and involves microbial infection, multiple immune responses, fibrosis process, abnormal signaling pathways, and other multi-factor interactions, which promote the disease from acute to chronic and form a chronic state that is difficult to cure. It is difficult for a single treatment model to comprehensively address the complex etiology and course of the disease. With the advantages of multi-target and synergistic effects, integrated traditional Chinese and western medicine treatments have shown broad prospects in improving clinical signs and symptoms, reducing recurrence rates, and protecting reproductive function. Evidence-based research and mechanism exploration should be further strengthened in the future to provide more scientific and systematic strategies for clinical prevention and treatment of PID.
Disclosure
The authors declare that they have no affiliations with or involvement in any organization or entity with any financial interest in the subject matter or materials discussed in this manuscript.
References
1. Pelvic inflammatory disease and infertility. Australian Journal of General Practice. Available from: https://www1.racgp.org.au/ajgp/2023/april/pelvic-inflammatory-disease-and-infertility.
2. Zou W, Gong L, Zhou F, et al. Anti-inflammatory effect of traditional Chinese medicine preparation Penyanling on pelvic inflammatory disease. J Ethnopharmacol. 2021;266:113405. doi:10.1016/j.jep.2020.113405
3. Hillier SL, Bernstein KT, Aral S. A review of the challenges and complexities in the diagnosis, etiology, epidemiology, and pathogenesis of pelvic inflammatory disease. J Infect Dis. 2021;224(Suppl 2):S23–13
4. Gradison M. Pelvic inflammatory disease. Am Fam Physician. 2012;85(8):791–796.
5. Kreisel KM, Llata E, Haderxhanaj L, et al. The burden of and trends in pelvic inflammatory disease in the united states, 2006-2016. J Infect Dis. 2021;224(12 Suppl 2):S103–S112
6. Kreisel K, Torrone E, Bernstein K, Hong J, Gorwitz R. Prevalence of pelvic inflammatory disease in sexually experienced women of reproductive age - United States, 2013-2014. MMWR Morb Mortal Wkly Rep. 2017;66(3):80–83
7. Davis GS, Horner PJ, Price MJ, et al. What do diagnoses of pelvic inflammatory disease in specialist sexual health services in england tell us about chlamydia control? J Infect Dis. 2021;224(12 Suppl 2):S113–S120
8. He D, Wang T, Ren W. Global burden of pelvic inflammatory disease and ectopic pregnancy from 1990 to 2019. BMC Public Health. 2023;23(1):1894
9. Brunham RC, Gottlieb SL, Paavonen J. Pelvic inflammatory disease. N Engl J Med. 2015;372(21):2039–2048
10. Price MJ, Ades AE, Welton NJ, et al. Proportion of pelvic inflammatory disease cases caused by chlamydia trachomatis consistent picture from different methods. J Infect Dis. 2016;214(4):617–624
11. Ness RB, Soper DE, Holley RL, et al. Effectiveness of inpatient and outpatient treatment strategies for women with pelvic inflammatory disease: results from the Pelvic Inflammatory Disease Evaluation and Clinical Health (PEACH) Randomized Trial. Am J Obstet Gynecol. 2002;186(5):929–937
12. Ness RB, Trautmann G, Richter HE, et al. Effectiveness of treatment strategies of some women with pelvic inflammatory disease: a randomized trial. Obstet Gynecol. 2005;106(3):573–580
13. Mahafzah AM, Al-Ramahi MQ, Asa’d AM, et al. Prevalence of sexually transmitted infections among sexually active Jordanian females. Sex Transm Dis. 2008;35(6):607–610
14. Trent M, Ellen JM, Frick KD. Estimating the direct costs of pelvic inflammatory disease in adolescents: a within-system analysis. Sex Transm Dis. 2011;38(4):326–328
15. Darville T. Pelvic inflammatory disease due to neisseria gonorrhoeae and chlamydia trachomatis: immune evasion mechanisms and pathogenic disease pathways. J Infect Dis. 2021;224(Suppl 2):S39–S46
16. Mitchell CM, Anyalechi GE, Cohen CR, et al. Etiology and diagnosis of pelvic inflammatory disease: looking beyond gonorrhea and chlamydia. J Infect Dis. 2021;224(Suppl 2):S29–S35
17. Ness RB, Kip KE, Hillier SL, et al. A cluster analysis of bacterial vaginosis-associated microflora and pelvic inflammatory disease. Am J Epidemiol. 2005;162(6):585–590
18. Soper DE, Brockwell NJ, Dalton HP, et al. Observations concerning the microbial etiology of acute salpingitis. Am J Obstet Gynecol. 1994;170(4):1008–1014. doi:10.1016/s0002-9378(94)70094-x
19. Taylor-Robinson D, Jensen JS, Svenstrup H, et al. Difficulties experienced in defining the microbial cause of pelvic inflammatory disease. Int J STD AIDS. 2012;23(1):18–24
20. Abdelrahman YM, Belland RJ. The chlamydial developmental cycle. FEMS Microbiol Rev. 2005;29(5):949–959
21. Russell MW. Immune responses to neisseria gonorrhoeae: challenges and opportunities with respect to pelvic inflammatory disease. J Infect Dis. 2021;224(12 Suppl 2):S96–S102
22. Zhu W, Ventevogel MS, Knilans KJ, et al. Neisseria gonorrhoeae suppresses dendritic cell-induced, antigen-dependent CD4 T cell proliferation. PLoS One. 2012;7(7):e41260. doi:10.1371/journal.pone.0041260
23. Liu Y, Liu W, Russell MW. Suppression of host adaptive immune responses by Neisseria gonorrhoeae: role of interleukin 10 and type 1 regulatory T cells. Mucosal Immunol. 2014;7(1):165–176. doi:10.1038/mi.2013.36
24. Zheng X, O’Connell CM, Zhong W, et al. Discovery of blood transcriptional endotypes in women with pelvic inflammatory disease. J Immunol. 2018;200(8):2941–2956
25. Mitchell C, Prabhu M. Pelvic inflammatory disease: current concepts in pathogenesis, diagnosis and treatment. Infect Dis Clin North Am. 2013;27(4). doi:10.1016/j.idc.2013.08.004
26. Xu SX, Gray-Owen SD. Gonococcal pelvic inflammatory disease: placing mechanistic insights into the context of clinical and epidemiological observations. J Infect Dis. 2021;224(Suppl 2):S56–S63
27. Stevens JS, Gray MC, Morisseau C, et al. Endocervical and neutrophil lipoxygenases coordinate neutrophil transepithelial migration to neisseria gonorrhoeae. J Infect Dis. 2018;218(10):1663–1674
28. Chappell CA, Wiesenfeld HC. Pathogenesis, diagnosis, and management of severe pelvic inflammatory disease and tuboovarian abscess. Clin Obstet Gynecol. 2012;55(4):893–903
29. Van Voorhis WC, Barrett LK, Sweeney YT, et al. Repeated Chlamydia trachomatis infection of Macaca nemestrina fallopian tubes produces a Th1-like cytokine response associated with fibrosis and scarring. Infect Immun. 1997;65(6):2175–2182. doi:10.1128/iai.65.6.2175-2182.1997
30. Workowski KA, Berman S. Centers for Disease Control and Prevention (CDC). Sexually transmitted diseases treatment guidelines, 2010. MMWR Recomm Rep. 2010;59(RR–12):1–110.
31. Workowski KA, Bachmann LH, Chan PA, et al. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR. Recomm Rep. 2021;70(4):1–187. doi:10.15585/mmwr.rr7004a1
32. Wiesenfeld HC, Meyn LA, Darville T, et al. A randomized controlled trial of ceftriaxone and doxycycline, with or without metronidazole, for the treatment of acute pelvic inflammatory disease. Clin Infect Dis. 2020;72(7):1181–1189
33. Bevan CD, Ridgway GL, Rothermel CD. Efficacy and safety of azithromycin as monotherapy or combined with metronidazole compared with two standard multidrug regimens for the treatment of acute pelvic inflammatory disease. J Int Med Res. 2003;31(1):45–54
34. Savaris RF, Fuhrich DG, Duarte RV, et al. Antibiotic therapy for pelvic inflammatory disease: an abridged version of a Cochrane systematic review and meta-analysis of randomised controlled trials. Sex Transm Infect. 2019;95(1):21–27
35. Wei A, Feng H, Jia XM, et al. Ozone therapy ameliorates inflammation and endometrial injury in rats with pelvic inflammatory disease. Biomed Pharmacother. 2018;107:1418–1425
36. Hasanin ME, Aly SM, Taha MM, et al. The effect of laser biostimulation at sensitized acupoints on chronic pelvic pain and quality of life in women with pelvic inflammatory disease: a randomized controlled trial. Medicina. 2025;61(2):354
37. Csirzó Á, Kovács DP, Szabó A, et al. Comparative analysis of medical interventions to alleviate endometriosis-related pain: a systematic review and network meta-analysis. J Clin Med. 2024;13(22):6932. doi:10.3390/jcm13226932
38. Lin X, Pan XB, Guo BZ, et al. The effect of psychological intervention combined with standard pharmacological therapy in patients with chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS): a randomized controlled trial. Medicine. 2025;104(35):e44110
39. Chen J, Luo J. Rehabilitation therapies in pelvic floor dysfunction for women. J Community Health Nurs. 2025:1–10
40. Gondwe T, Ness R, Totten PA, et al. Novel bacterial vaginosis-associated organisms mediate the relationship between vaginal douching and pelvic inflammatory disease. Sex Transm Infect. 2020;96(6):439–444
41. Carlson S, Batra S, Billow M, et al. Perioperative complications of laparoscopic versus open surgery for pelvic inflammatory disease. J Minim Invasive Gynecol. 2021;28(5):1060–1065. doi:10.1016/j.jmig.2020.08.488
42. Wang D, Jiang Y, Feng J, et al. Evidence for the use of complementary and alternative medicine for pelvic inflammatory disease: a literature review. Evid Based Complement Alternat Med. 2022;2022:1364297
43. Li Y, Zhang X, Zhang W, et al. The therapeutic effect of modified Longdan Xiegan Tang on pelvic inflammatory disease of damp-heat stasis type and its impact on inflammatory response and immune function. J Mod Chin West Med. 2025;34(12):1668–1672.
44. Jia SM. Clinical effect of modified Danggui Shaoyao San in the treatment of chronic pelvic inflammatory disease of damp-heat and blood stasis type. Inner Mongolia J Tradit Chin Med. 2024;43(11):36–38. doi:10.16040/j.cnki.cn15-1101.2024.11.019
45. Xu XY, Shen FF. Clinical observation on self-formulated Qingre Huashi Tongluo Tang combined with western medicine for 56 cases of acute pelvic inflammatory disease with damp-heat accumulation syndrome. Chin J Tradit Chin Med Sci Technol. 2025;32(3):514–516.
46. Zhang Y, Tang S, Zhang L, et al. Clinical study on treatment of pelvic inflammatory disease with Qingjie mixture. Chin J Emerg Med. 2018;27(11):1943–1945.
47. Yang WS, Kim D, Yi YS, et al. AKT-targeted anti-inflammatory activity of the methanol extract of Chrysanthemum indicum var. albescens. J Ethnopharmacol. 2017;201:82–90. doi:10.1016/j.jep.2017.03.001
48. Recio MC, Cerdá-Nicolás M, Potterat O, et al. Anti-Inflammatory and antiallergic activity in vivo of lipophilic isatis tinctoria extracts and tryptanthrin. Planta Med. 2006;72(6):539–546
49. Lee JH, Ko WS, Kim YH, et al. Anti-inflammatory effect of the aqueous extract from Lonicera japonica flower is related to inhibition of NF-kappaB activation through reducing I-kappaBalpha degradation in rat liver. Int J Mol Med. 2001;7(1):79–83.
50. Wang Y, Tan Y, He Z, et al. Chicoric acid ameliorates rat salpingitis by inhibiting the Nrf2/Notch1 signaling pathway. Eur. J. Pharmacol. 2025;1003:177980
51. Yan H. Clinical Observation of Liqi Zhuyu Tang in Treating Postsequelae of Pelvic Inflammatory Disease with Qi Stagnation and Blood Stasis Type and Its Effects on Serum Pain Mediators and Anxiety Status [Dissertation]. Nanjing University of Chinese Medicine; 2025; doi:10.27253/d.cnki.gnjzu.2025.000252
52. Li ZF, Li JJ, Li RH, et al. Yiqi Huoxue Recipe for the treatment of sequela of pelvic inflammatory disease of qi deficiency and blood stasis type. J. Tradit Chin Med. 2025;40(8):1795–1800. doi:10.16368/j.issn.1674-8999.2025.08.287
53. Liu HT. Clinical efficacy of modified Lichong Decoction in treating sequelae of pelvic inflammatory disease (qi deficiency and blood stasis type). Inner. Mongolia J Tradit Chin Med Med. 2022;41(9):14–16. doi:10.16040/j.cnki.cn15-1101.2022.09.050
54. Song JC, Luo HM. Clinical research on the treatment of chronic pelvic inflammatory disease with cold-damp stagnation syndrome using Wenjing Decoction combined with fleroxacin tablets. New J Tradit Chin Med. 2023;55(2):14–17. doi:10.13457/j.cnki.jncm.2023.02.004
55. Bu X, Liu Y, Lu Q, Jin Z. Effects of “danzhi decoction” on chronic pelvic pain, hemodynamics, and proinflammatory factors in the murine model of sequelae of pelvic inflammatory disease. Evid Based Complement Alternat Med. 2015;2015:547251. doi:10.1155/2015/547251
56. Wang Y, Huang Y, Shi L, et al. Shipi shugan decoction protected against sequela of pelvic inflammatory disease via inhibiting sirt1/nlrp3 signaling pathway in pelvic inflammatory disease rats. Evid Based Complement Alternat Med. 2022;2022:6382205
57. Yang Y, Lu Y, Zhou D, et al. Effectiveness of Jinying capsule on pelvic inflammatory disease in patients with symptom pattern of damp and heat accumulation: a double-blinded, multicenter, randomized, placebo-controlled clinical trial. J Tradit Chin Med. 2020;40(3):432–439
58. Feng XL, Jiang S, Chen J, Liu X, Zhang Y, Chen L. Effect of Fuyanshu Capsules combined with antibiotics on inflammatory factors in patients with pelvic inflammatory disease. Zhongguo Zhong Yao Za Zhi. 2019;44(12):2637–2643
59. Wang L, Chen Y, Ouyang YL, Wang FW, Zhang RJ, Chen X. Curative effect of kangfuyan capsule combined with antibiotic treatment on pelvic inflammatory disease. Pak J Pharm Sci. 2021;34(6 Spec):2479–2485.
60. Xu C, Yi M, Xiao Z. New idea of Fuke Qianjin capsule in treating sequelae of pelvic inflammatory disease: anti-inflammatory in the early stage and reparative in the later stage. J Ethnopharmacol. 2025;338:119066
61. Xiong S, Xu C, Yang C, et al. FuKe QianJin capsule alleviates endometritis via inhibiting inflammation and pyroptosis through modulating TLR4/NF-κB/NLRP3 pathway. J Ethnopharmacol. 2025;337:118962. doi:10.1016/j.jep.2024.118962
62. Kong S, Zhang YH, Liu CF, et al. The complementary and alternative medicine for endometriosis: a review of utilization and mechanism. Evid Based Complement Alternat Med. 2014;2014:146383
63. Li LJ, Fu JF. The effect of retention enema of traditional Chinese medicine on chronic pelvic inflammatory disease and inflammatory factors. World Chin Med. 2017;12:772–775,779.
64. Yin J, Feng M, Xu H. Cai’s gynecology chronic pelvic formula with acupuncture alleviates chronic pelvic pain and reduces recurrence in patients with pelvic inflammatory disease sequelae. Am J Transl Res. 2025;17(7):5241–5256
65. Liu YH, Wang X, Liang Z, et al. Acupuncture combined with western medication on chronic pelvic pain after pelvic inflammatory disease: a multi-center randomized controlled trial. Zhongguo Zhen Jiu. 2021;41(1):31–35. doi:10.13703/j.0255-2930.20191218-k0002
66. Zhang LJ, Zhu JY, Sun MY, et al. Anti-inflammatory effect of Man-Pen-Fang, a Chinese herbal compound, on chronic pelvic inflammation in rats. J Ethnopharmacol. 2017;208:57–65
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.