Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Beyond Cardiometabolic: Health Disorders Risk in Metabolically Healthy Obese Children – A Systematic Review and Meta-Analysis of 19,119 Children
Authors Kurniawan RC, Suhamdy F ![]() , Akhlaq MM, Ariyanto EF
, Akhlaq MM, Ariyanto EF ![]()
Received 2 September 2025
Accepted for publication 31 October 2025
Published 12 November 2025 Volume 2025:18 Pages 4127—4140
DOI https://doi.org/10.2147/DMSO.S560672
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jae Woong Sull
Richard Christophorus Kurniawan,1,* Frederick Suhamdy,1,* Muhammad Makarimal Akhlaq,1 Eko Fuji Ariyanto2,3
1Faculty of Medicine, Universitas Padjadjaran, Sumedang, West Java, 45363, Indonesia; 2Department of Biomedical Sciences, Faculty of Medicine, Universitas Padjadjaran, Sumedang, West Java, 45363, Indonesia; 3Study Center for Medical Genetics, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, 40161, Indonesia
*These authors contributed equally to this work
Correspondence: Richard Christophorus Kurniawan, Faculty of Medicine, Universitas Padjadjaran, Sumedang, West Java, 45363, Indonesia, Email [email protected]
Background and Objectives: Childhood obesity is associated with both short-term and long-term health complications, yet a new obesity phenotype called metabolically healthy obesity (MHO) has emerged. While MHO is often perceived as a “benign” form of obesity, research specifically examining health disorders risks in children with MHO remains limited. This systematic review and meta-analysis aimed to evaluate health disorders in children with MHO.
Methods: Following PRISMA 2020 guidelines, we systematically searched five databases (PubMed, Scopus, Google Scholar, EBSCO, and ScienceDirect) for observational studies examining MHO children aged 0– 18 years. The studies were analyzed using R and R Studio software, with study quality assessed using the Newcastle Ottawa Scale.
Results: Ten studies with a total of 19,119 children were included in this review. Children with MHO demonstrated significantly higher overall health disorders risk compared to MHNW children (pooled OR 2.88, 95% CI [1.64; 5.06]). This trend aligns with the subgroups analysis of left ventricle hypertrophy, hypertension, and kidney damage. However, some of the subgroup analyses showed insignificant results. Additionally, MHO children showed lower risks of experiencing health disorders compared to MUO children (pooled OR 0.56, 95% CI [0.23; 1.34]). The underlying mechanism of the increased health risk is excess adipokines causing systemic inflammation and leading to increased various health risks.
Conclusion: Despite metabolically “healthy” status, children with MHO remain at increased risk for health disorders compared to normal-weight peers. This systematic review and meta-analysis is the first one discussing the health disorders in children with MHO. More studies are required in the future to reinforce these findings in order to produce much more comprehensive insights.
Keywords: children, disorders, metabolically healthy obesity, obesity
Introduction
Childhood obesity has significantly increased in various countries over the past few decades and has become a concerning public health issue. It is estimated that 197 million children aged 0–18 years old are living with obesity in 2022, significantly increased from 11 million in 1975.1 This trend is further backed up by a recent review, showing one in five children is classified as overweight and obese globally.2 Unfortunately, this trend cannot be taken lightly. Beyond its high prevalence, childhood obesity also increases the risk of numerous health disorders, such as diabetes mellitus, dyslipidemia, hypertension, non-alcoholic fatty liver disease, obstructive sleep apnea, and polycystic ovary syndrome. Additionally, children with obesity often face negative stigma and reduced quality of life.3 Therefore, obesity prevention and management through lifestyle and dietary modifications must be implemented as early as possible.
Childhood obesity is associated with both short-term and long-term health problems that may extend into adulthood. However, a new obesity phenotype known as Metabolically Healthy Obesity (MHO) has recently been gaining attention. MHO in children is characterized by age- and sex-specific body mass index (BMI) categories and the absence of metabolic disorders.4,5 Due to its healthy metabolic markers, MHO is often perceived as a benign form of obesity and does not increase health disorders.
Interestingly, some studies state that individuals with MHO still have a higher risk of health issues despite their normal metabolic status.6–15 However, most of the existing literature, including systematic reviews and meta-analyses, has primarily focused on the health risks associated with MHO in adult populations. This causes the health risks of MHO in children to remain underexplored, making it crucial to elaborate on this topic further. Research findings in this younger demographic have also been inconsistent and conflicting, leading to confusion and improper management.
The research question of this systematic-review and meta-analysis is how is the health risk in children with MHO compared to those with MUO (Metabolically Unhealthy Obese) and MHNW (Metabolically Healthy Normal Weight)? To address this issue, this systematic review and meta-analysis were conducted to assess the health risks in children with MHO, comparing them to those with MUO (Metabolically Unhealthy Obese) and MHNW (Metabolically Healthy Normal Weight).
Materials and Methods
This systematic review and meta-analysis were conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. The protocol of our review was registered in the PROSPERO: CRD420251084858.
Data Sources and Literature Search
Our review used five different large electronic databases for obtaining a potential study, including PubMed, Scopus, Google Scholar, EBSCO, and ScienceDirect. The search strategy included the keywords “child” and “metabolically healthy obesity” along with their synonyms. These terms were searched in the title, abstract, and Medical Subject Headings (MeSH) fields using appropriate Boolean operators such as “AND” and “OR” adapted to each database’s specifications for a comprehensive literature search. Detailed search strategies for each database can be found in Table 1.
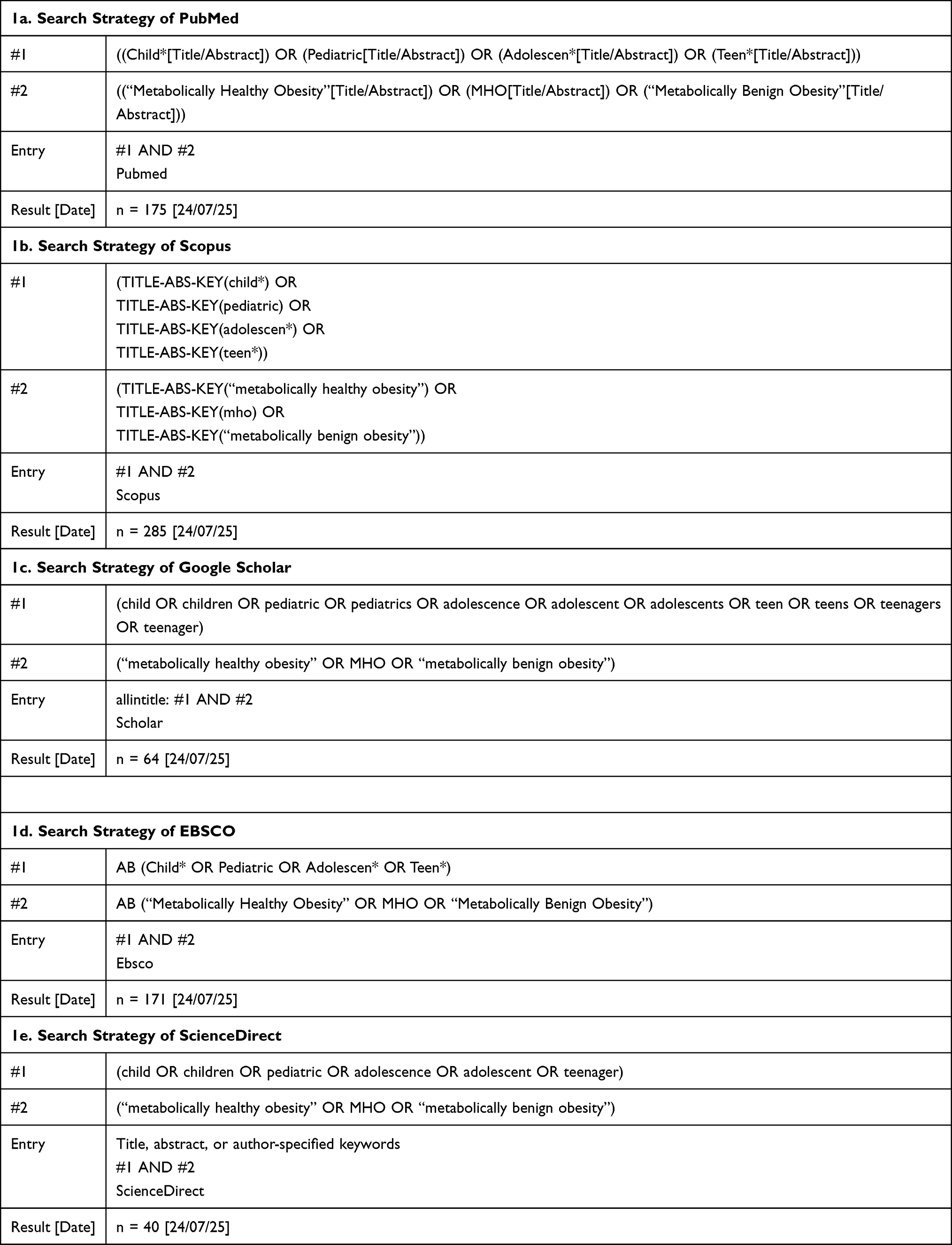 |
Table 1 Search Strategy of Pubmed, Scopus, Google Scholar, EBSCO, and ScienceDirect |
Three reviewers independently conducted a comprehensive literature search across five electronic databases: PubMed, Scopus, Google Scholar, EBSCO, and ScienceDirect.
Study Selection
Each of the collected studies’ title and abstracts were screened by three reviewers independently. Then, the full text of the studies that met the inclusion and exclusion criteria was retrieved. After that, the full texts were assessed against inclusion and exclusion criteria. The PECO framework was defined as follows:
- Population: children aged 0–18 years;
- Exposure: MHO;
- Comparison: MUO and/or MHNW;
- Outcome: risk of health disorders.
Studies meeting the following criteria were included: (1) full-text availability; (2) observational study (cohort, case control, and cross-sectional); (3) articles published in English; (4) evaluation of the association between MHO and the development of health disorders in children; and (5) reporting of effect estimate and its confidence interval (CI). Exclusion criteria were: (1) in vitro studies; (2) in vivo studies; (3) case reports, reviews, editorials, and commentaries; (4) studies that did not compare MHO with MHNW and/or MUO; (5) articles irrelevant to the research topic; and (6) studies whom full text cannot be retrieved.
Data Extraction and Risk of Bias Assessment
The following data were systematically and independently extracted by three reviewers from each eligible study: (1) first author surname; (2) DOI; (3) publication year; (4) country; (5) study design; (6) MHO definition; (7) age of study population; (8) sample size and proportion for MHO, MUO, and MHNW; (9) investigated health disorders risk. The risk of bias and study quality were independently assessed using the Newcastle-Ottawa Scale (NOS). The results of the NOS are then converted into Agency for Healthcare Research and Quality (AHRQ) standards based on the following criteria: (1) good quality studies are those who obtain 3 or 4 stars in selection domain AND 1 or 2 stars in comparability domain AND 2 or 3 stars in outcome/exposure domain; (2) fair quality studies are those who obtain 2 stars in selection domain AND 1 or 2 stars in comparability domain AND 2 or 3 stars in outcome/exposure domain; (3) poor quality studies are those who obtain 0 or 1 star in selection domain OR 0 stars in comparability domain OR 0 or 1 stars in outcome/exposure domain.
Statistical Analysis
Statistical analyses were performed in R using the meta, metafor, and tidyverse packages following the Cochrane Handbook’s recommendations. This review used odds ratios (OR) with corresponding 95% confidence intervals (CI) as the primary measure of association between MHO and health disorders risks. A random-effects model and the inverse variance method were applied for data synthesis. To address and control heterogeneity, subgroup analyses were performed for specific health disorder outcomes. Potential sources of heterogeneity, such as differences in MHO definition, study design, and population characteristics, were explored in detail in the results. Statistical test with p < 0.05 considered statistically significant; substantial heterogeneity was defined as I2 > 50% and p < 0.1, and subgroup analyses were performed for each specific health disorder risk.
Results
Study Selection Result
Eligibility screening was conducted in a stepwise manner as illustrated in the PRISMA flow diagram (see Figure 1). A total of 735 articles were identified from various databases (see Table 1 for details). After removing 424 duplicates, 311 articles were screened based on their titles and abstracts. At this stage, 273 articles were excluded due to irrelevance, inappropriate study designs, or failure to meet the PECO criteria, leaving 38 articles for full-text assessment. Also, 2 articles were unavailable in full text. Of the 36 articles reviewed in full text, 12 were excluded due to wrong outcome, 10 due to wrong population, 1 due to wrong comparator, 1 due to wrong publication type, 1 due to irrelevant topic, and 1 due to no English full-text was available. Consequently, 10 articles were included in the review (see Figure 1 for details).
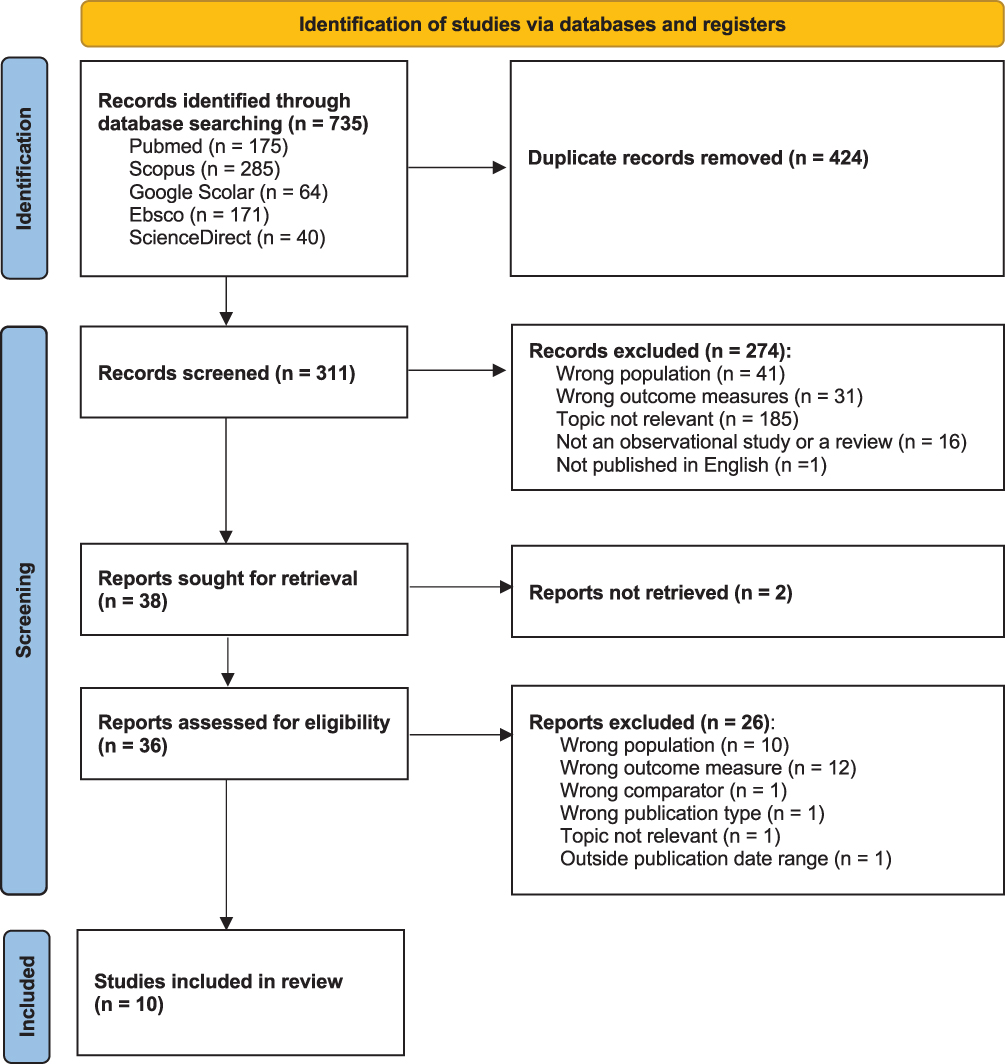 |
Figure 1 PRISMA Flow Diagram PRISMA figure adapted from Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Creative Commons. |
Characteristic of the Included Study
Our review included studies published at any time, comprising a total sample of 19,119 children aged under 18 years. Among these studies, two used MUO as the comparator group and ten used MHNW as the comparator group. Several health disorders risk were assessed: two studies on diabetes mellitus (DM), two on carotid intima media thickness (CIMT), four on LVH (left ventricular hypertrophy), one on hypertension, one on kidney damage, and one on poor cardiorespiratory fitness (PCRF) (see Table 2). The results of the risk of bias and quality assessments indicated generally good quality across most studies, except for the article by Genovesi et al, which was judged as having poor quality (see Table 3).
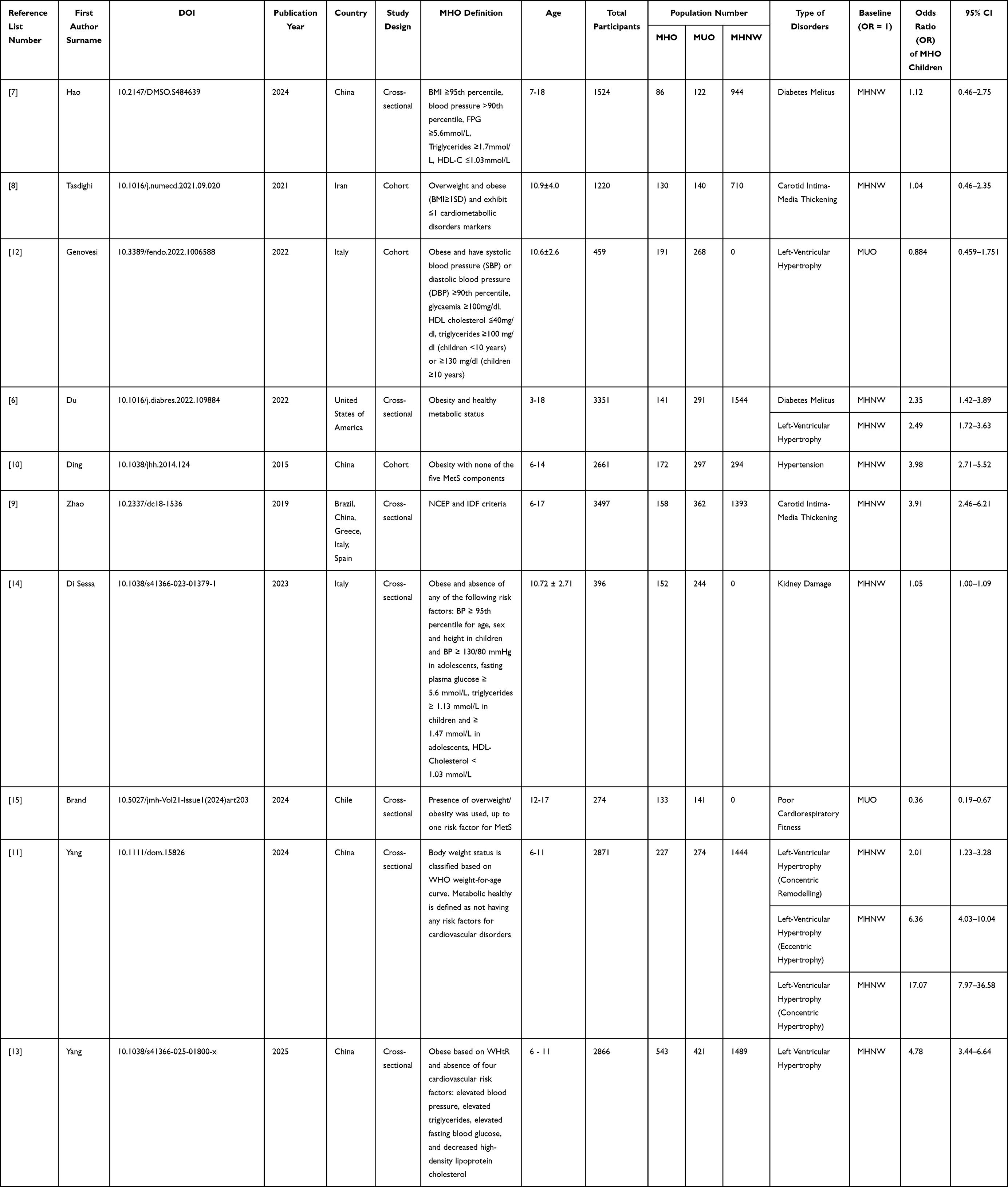 |
Table 2 Characteristics of Each Study |
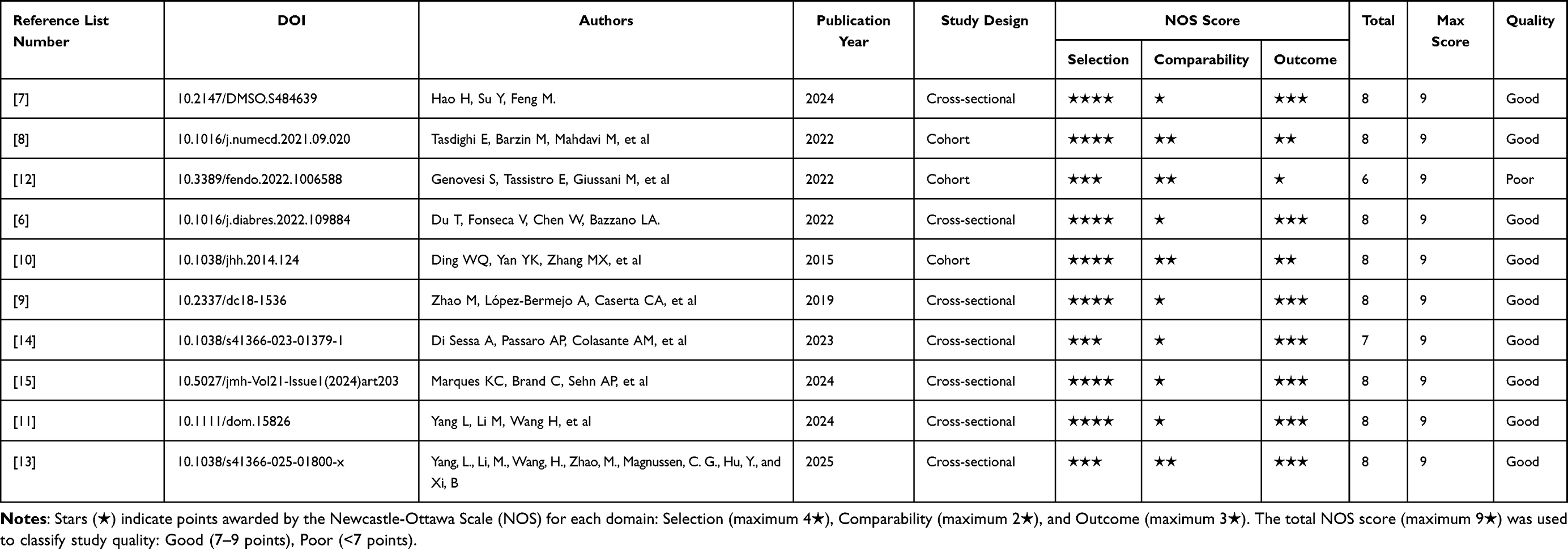 |
Table 3 Risk of Bias and Study Quality Assessment |
Association Between MHO and Health Disorders Risk
Ten studies were included in this review to analyze the risk of health disorders in MHO compared to MHNW and/or MUO.6–15 Participants were classified into MHO, MUO, and MHNW groups based on standardized clinical criteria reported in each study. Because each study applied different modified thresholds and definitions for metabolic health, these variations may contribute to heterogeneity in the pooled estimates.
Despite minimal or absent metabolic abnormalities, children with MHO still show a significantly higher overall risk of developing health disorders than those with MHNW (OR=2.88, 95% CI: 1.64–5.06), with substantial heterogeneity (I2 = 96.6%, p < 0.0001) (Figure 2).6–15 In contrast, findings from the studies demonstrated that MHO carries a lower overall health disorders risk compared to MUO (OR = 0.56, 95% CI: 0.23–1.34), and accompanied by significant heterogeneity (I2 = 72.5%, p = 0.0564) (Figure 3).6–15
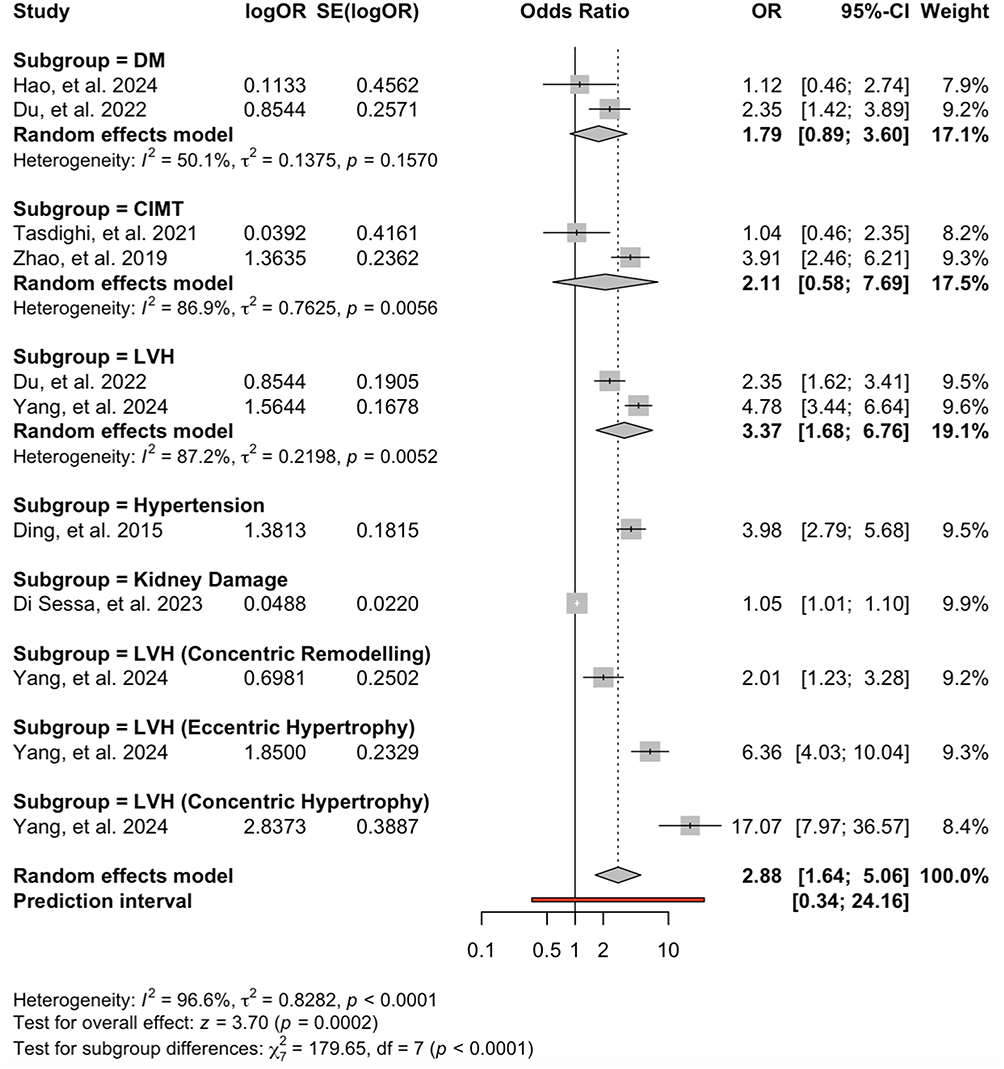 |
Figure 2 Risk of Cardiometabolic Disorders in MHO vs MHNW Children. Forest plot showing pooled odds ratios (ORs) with 95% confidence intervals (CIs) for various cardiometabolic outcomes in metabolically healthy obese (MHO) compared with metabolically healthy normal weight (MHNW) children. Each subgroup represents a specific outcome analyzed using a random-effects model. Bolded lines denote the pooled summary estimates for each subgroup and the overall meta-analytic summary effect, emphasizing the combined results derived from multiple studies rather than individual estimates. The bold line at the bottom represents the prediction interval, indicating the expected range of effects for future studies based on between-study heterogeneity. |
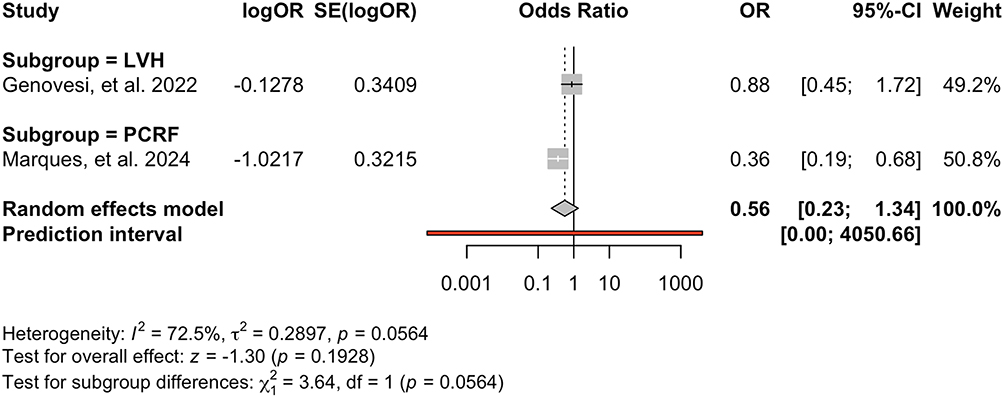 |
Figure 3 Risk of Cardiometabolic Disorders in MHO vs MUO Children. Forest plot showing odds ratios (ORs) with 95% confidence intervals (CIs) for various cardiometabolic outcomes in metabolically healthy obese (MHO) compared with metabolically unhealthy obese (MUO) children. Each subgroup represents a specific outcome analyzed using a random-effects model. Bolded lines denote the pooled summary estimates for each subgroup and the overall meta-analytic summary effect, emphasizing the combined results derived from multiple studies rather than individual estimates. The bold line at the bottom represents the prediction interval, indicating the expected range of effects for future studies based on between-study heterogeneity. |
For further evaluation, subgroup analyses were also performed based on each type of health disorders outcome. Children with MHO showed a higher risk of DM compared to those with MHNW (OR 1.79, 95% CI [0.89–3.60]) (see Figure 2).6,7
In studies assessing CIMT, statistical analysis indicated that children with MHO had a higher risk of CIMT thickening compared to those with MHNW (OR 2.11, 95% CI [0.58–7.79]) (see Figure 2).8,9
The study focusing on hypertension in children with obesity demonstrated that those with MHO had a higher risk of developing hypertension compared to MHNW children (OR 3.98, 95% CI [2.79–5.68]) (see Figure 2).10
Studies evaluating the risk of left ventricular hypertrophy (LVH) were also statistically analyzed. Results showed that children with MHO were at higher risk of developing LVH compared to those with MHNW (OR 3.37, 95% CI [1.68–6.76]) (see Figure 2).6,11–13 Additionally, a study breaks down the risk of different types of LVH in children with MHO compared to children with MHNW. According to the said study, the risk of MHO children having concentric remodelling, eccentric hypertrophy, and concentric hypertrophy are OR 2.01 (95% CI [1.23–3.28]), OR 6.36 (95% CI [4.03–10.04]), and OR 17.07 (95% CI [7.97–36.57]) respectively.13 Conversely, the risk of LVH in children with MHO was lower than in those with MUO (OR 0.88, 95% CI [0.45–1.72]) (see Figure 3).12
Analysis of the study on kidney damage indicated that children with MHO had a higher risk of kidney damage compared to those with MHO (OR 1.05, 95% CI [1.01–1.10]) (see Figure 2).14
Lastly, statistical analysis of the study assessing poor cardiorespiratory fitness (PCRF) showed that children with MHO had a reduced risk of PCRF compared to those with MUO (OR 0.36, 95% CI [0.19–0.68]) (see Figure 3).15
Discussion
In general, children with MHO have a higher risk of developing health disorders compared to those with MHNW. On the other hand, children with MHO exhibit a lower risk than those with MUO, which is largely due to more favorable fat distribution and adipokine profiles in the MHO group.6–15
A similar pattern among MHO, MUO, and MHNW was also observed across more specific disorders. The main differences lie in the statistical significance of outcomes for each disease. Disorders such as DM, CIMT thickening, and LVH (MHO vs MUO) showed non-significant statistical results.6–9,12 In contrast, LVH (general and specific types in MHO vs MHNW), hypertension, kidney damage, and PCRF demonstrated statistically significant associations.6,10,11,13–15
The risk of diabetes mellitus in children with MHO is influenced by the degree of fat accumulation, particularly visceral fat.6,7,16 Studies have shown that visceral adipose tissue can produce pro-inflammatory cytokines such as TNF-α and IL-6, which, when present in excess, can lead to systemic inflammation that disrupts insulin signaling in muscle, liver, and adipose tissue.6,7,16 This systemic inflammation is further exacerbated by adipokine imbalance—characterized by increased leptin levels and decreased adiponectin—resulting in worsened insulin resistance and impaired glucose metabolism.6,7,16 In contrast, children with MHNW typically have a lower and more evenly distributed fat mass, along with a more balanced adipokine profile, which helps prevent systemic inflammation.16
The CIMT thickening risk in MHO children is increased compared to MHNW children due to adipokine imbalance and accumulation of visceral fat. Excess leptin level causes endothelial cell activation, resulting in the expression of cell-adhesive molecules such as VCAM-1 and ICAM-1.8–10,17–27 The endothelial activation causes inflammation to its cells and reduces nitrate oxide, in which is crucial in vasodilation.8–10,17–27 Additionally, as mentioned earlier, the accumulation of visceral fat produce pro-inflammatory cytokines such as TNF-α and IL-6, which, when present in excess, cause shear stress to the vascular endothelial.8–10,17–27 To overcome the stress, the body activates the compensatory mechanisms, which include the hypertrophy of the arteries’ intima-media.8–10,17–27 On the other hand, children with MHNW have a better adipokine profile and fat distribution than MHO children, making them less risked having CIMT thickening.8–10,17–24,26,27
Hypertension in MHO children is more common than in MHNW children. Children with MHO have a higher visceral fat than children with MHNW. The higher visceral fat increases the intra-abdominal pressure, resulting in the activation of renal baroreceptors. The baroreceptor activation then causes sodium reabsorption and fluid retention to compensate for the intra-abdominal pressure increase.10,18,19,21–24,26,27 In addition to that, higher visceral fat also causes MHO children to be more susceptible to endothelial dysfunction and vascular resistance due to the endothelial inflammation. This condition favors the occurrence of hypertension in MHO children.10,18,19,21–24,26,27 Additionally, high adiposity level also activates renin-angiotensin-aldosterone system (RAAS), aggravating vasoconstriction and hypertension even further.10,18,19,21–24,26,27 Furthermore, adipokine imbalance also contributes to raising hypertension risk in MHO children.10,18,19,21–24,26,27 Higher leptin level in MHO children also activates the sympathetic nervous system and increases endothelin-1 production, resulting in vasoconstriction and higher blood pressure.10,18,19,21–24,26,27
Compared to MHNW, MHO children have a higher risk of developing LVH, yet lower than MUO children. Children with MHO have a higher visceral fat than children with MHNW. The higher visceral fat increases the intra-abdominal pressure, resulting in the activation of renal baroreceptors. The baroreceptor activation then causes sodium reabsorption and fluid retention to compensate for the intra-abdominal pressure increase. This cascade then causes hypertension, which results in prolonged increase in hemodynamic burden and eventually LVH.6,11–13,18,19,21–24,26,27 Additionally, high leptin level also causes plasma volume expansion through the activation of the RAAS. This expansion also triggers hypertension and LVH due to an increase in hemodynamic burden.6,11–13,18,19,21–24,26,27 In addition to that, imbalance adiponectin profile also causes endothelial dysfunction and increased vascular resistance. It then aggravates the heart burden and eventually causes LVH.6,11–13,18,19,21–24,26,27 Additionally, it has been shown that an increase in leptin-adiponectin ratio has also contributed to LVH incidence in MHO children via complex and various pathways.6,11–13,18,19,21–24,26,27 In contrast, MHO children have a lower risk of LVH compared to MUO children. As mentioned previously, this phenomenon may be caused by a worse adiponectin profile in MUO children compared to MHO children.6,11–13,18,19,21–24,26,27 The worse adiponectin profile further aggravates the hemodynamic burden, causing children with MUO to have higher risk of developing LVH.6,11–13,18,19,21–24,26,27 In addition to that, the atherogenic dyslipidemia in MUO children causes ceramide myocardial accumulation, which is cardiotoxic. Its accumulation impairs myocardial functioning, thus increasing the risk of having LVH further.6,11–13,18,19,21–24,26,27
Compared to children with MHO, children with MUO are more susceptible to kidney damage. Greater insulin resistance in MUO children causes a chronic hyperinsulinemic state, triggering the activation of PI3K/Akt/mTOR pathways in kidney tubular cells. The activation induces the hypertrophy of mesangial cells, a rise in glomerulus extracellular matrix synthesis, and activation of Na+/H+ symporter. These cause an increase in the reabsorption of sodium and intraglomerular pressure, making the kidney more susceptible to damage.14,27–31 Additionally, lipotoxicity, consequent to dyslipidemia, also causes kidney damage. The lipotoxicity increases the accumulation of ceramide in podocyte cells. The accumulation impairs the function of mitochondria and increases oxidative stress, resulting in kidney damage. Although MHO children also experience lipotoxicity, kidney damage is not as significant due to their greater antioxidant activities, such as superoxide dismutase.14,27–31
Overall, the theories from various studies show that the risk of health disorders in children with MHO, MUO, and MHNW is affected by lipid distribution and metabolic profile. When one’s lipid distribution and metabolic profile becomes unbalanced (eg leptin imbalance, excess visceral fat), a chronic systemic inflammation process is triggered. This inflammation slowly damages the organs leading to an increase in various health risks. Not only that, each adverse effect resulting from MHO may also interact with one another. For instance, an unbalanced metabolic and lipid profile increases the risk of having hypertension which in turn also increases the risk of CIMT, and LVH. Another example is kidney damage which is triggered by DM (insulin resistance state) which is also triggered by dyslipidemia in the first place.
This systematic review and meta-analysis may be the first that discusses the risk of health disorders in children with MHO. However, this review also has several limitations. First, substantial heterogeneity in some subgroups (I2 > 50%) may affect the stability of pooled estimates. Second, the small number of included studies limits analytical sensitivity and makes the estimated effects tend to be unstable Third, variations in the clinical definitions of MHO, MUO, and MHNW across studies likely contribute to heterogeneity in effect estimates. Nevertheless, with this review, the view of MHO as being “benign”, especially in children, can be refuted. In clinical settings, this review may become a guide for pediatric practice by underscoring the need for routine screening of cardiometabolic and non-cardiometabolic risk factors even in obese children without overt metabolic syndrome; it supports early, individualized intervention strategies—including lifestyle modification, nutritional counseling, and regular monitoring—to prevent the progression of subclinical disorders; and it informs pediatric guidelines by highlighting that “healthy obesity” may still confer elevated risks for organ dysfunction and long-term morbidity, thereby guiding clinicians to adopt a more proactive approach in managing all obese pediatric patients. In future research, updating this review to include a greater number of studies and employing standardized phenotype criteria is recommended.
Conclusion
This review shows that children with MHO are at greater risk of health disorders compared to children with MHNW, yet smaller risk than children with MUO. Nevertheless, this result should be interpreted cautiously, considering the high value of heterogeneity and the risk of bias.
Data Sharing Statement
The authors confirm that the data supporting the findings of this study are available within the article.
Acknowledgments
The authors gratefully acknowledge Universitas Padjadjaran for supporting the publication fee of this manuscript.
Author Contributions
According to CRediT contributorship taxonomy, Richard Christophorus Kurniawan performed the role of conceptualization, data curation, formal analysis, investigation, project administration, software, supervision, visualization, writing—original draft, and writing—review & editing. Frederick Suhamdy performed the role of conceptualization, data curation, formal analysis, investigation, project administration, software, visualization, writing—original draft, and writing—review and editing. Muhammad Makarimal Akhlaq performed the role conceptualization, formal analysis, methodology, resources, validation, and writing—original draft. Eko Fuji Ariyanto performed the role of funding acquisition, supervision, validation, and writing—original draft. All authors have given final approval of the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
The authors disclosed receipt for this article publication grant from Universitas Padjadjaran.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. World Health Organization: WHO. Obesity and overweight. 2025. Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
2. Zhang X, Liu J, Ni Y, et al. Global prevalence of overweight and obesity in children and adolescents. J Am Medical Association Pediatrics. 2024;178(8):800. doi:10.1001/jamapediatrics.2024.1576
3. Valerio G, Di Bonito P, Calcaterra V, et al. Cardiometabolic risk in children and adolescents with obesity: a position paper of the Italian society for pediatric endocrinology and diabetology. Italian J Pediatrics. 2024;50(1). doi:10.1186/s13052-024-01767-x
4. Güngör NK. Overweight and obesity in children and adolescents. J Clinical Res Pediatric Endocrinol. 2014;129–143. doi:10.4274/jcrpe.1471
5. Damanhoury S, Newton AS, Rashid M, Hartling L, Byrne JLS, Ball GDC. Defining metabolically healthy obesity in children: a scoping review. Obesity Rev. 2018;19(11):1476–1491. doi:10.1111/obr.12721
6. Du T, Fonseca V, Chen W, Bazzano LA. Changes in body size phenotypes from childhood to adulthood and the associated cardiometabolic outcomes. Diabetes Res Clin Pract. 2022;187:109884. doi:10.1016/j.diabres.2022.109884
7. Hao H, Su Y, Feng M. Association between metabolic and obesity phenotypes and diabetes risk in children and adolescents. Diabetes Metabolic Syndrome Obesity. 2024;17:4479–4487. doi:10.2147/dmso.s484639
8. Tasdighi E, Barzin M, Mahdavi M, et al. Association of childhood obesity phenotypes with early adulthood Carotid Intima-Media Thickness (CIMT): tehran lipid and glucose study. Nutr Metab Cardiovasc Dis. 2021;32(1):249–257. doi:10.1016/j.numecd.2021.09.020
9. Zhao M, López-Bermejo A, Caserta CA, et al. Metabolically healthy obesity and high carotid intima-media thickness in children and adolescents: international childhood vascular structure evaluation consortium. Diabetes Care. 2018;42(1):119–125. doi:10.2337/dc18-1536
10. Ding WQ, Yan YK, Zhang MX, et al. Hypertension outcomes in metabolically unhealthy normal-weight and metabolically healthy obese children and adolescents. J Human Hypertens. 2015;29(9):548–554. doi:10.1038/jhh.2014.124
11. Yang L, Li M, Wang H, et al. Metabolically healthy obesity and left ventricular geometric remodelling in Chinese children. Diabetes, Obesity and Metabolism. 2024;26(10):4629–4638. doi:10.1111/dom.15826
12. Genovesi S, Tassistro E, Giussani M, et al. Association of obesity phenotypes with left ventricular mass index and left ventricular hypertrophy in children and adolescents. Front Endocrinol. 2022:13. doi:10.3389/fendo.2022.1006588
13. Yang L, Li M, Wang H, et al. Metabolically healthy abdominal obesity is associated with higher odds of left ventricular geometric remodeling in children: evidence from two school-based studies in China. Int J Obesity. 2025. doi:10.1038/s41366-025-01800-x
14. Di Sessa A, Passaro AP, Colasante AM, et al. Kidney damage predictors in children with metabolically healthy and metabolically unhealthy obesity phenotype. Int J Obesity. 2023;47(12):1247–1255. doi:10.1038/s41366-023-01379-1
15. Brand C, Marques KC, Sehn AP, et al. Metabolically healthy versus unhealthy obesity in adolescents: is there a difference in cardiorespiratory fitness, physical activity, and active commuting? J Movement Health. 2023;21(1). doi:10.5027/jmh-vol21-issue1(2024)art203
16. Chandrasekaran P, Weiskirchen R. The role of obesity in type 2 diabetes mellitus—an overview. Int J Mol Sci. 2024;25(3):1882. doi:10.3390/ijms25031882
17. Vukovic R, Santos TJD, Ybarra M, Atar M. Children with metabolically healthy obesity: a review. Front Endocrinol. 2019;10. doi:10.3389/fendo.2019.00865
18. Ding W, Cheng H, Chen F, et al. Adipokines are associated with hypertension in metabolically healthy obese (MHO) children and adolescents: a prospective population-based cohort study. J Epidemiol. 2017;28(1):19–26. doi:10.2188/jea.je20160141
19. Petek TH, Varda NM. Childhood cardiovascular health, obesity, and some related disorders: insights into chronic inflammation and oxidative stress. Int J Mol Sci. 2024;25(17):9706. doi:10.3390/ijms25179706
20. Farello G, Antenucci A, Stagi S, Mazzocchetti C, Ciocca F, Verrotti A. Metabolically healthy and metabolically unhealthy obese children both have increased carotid intima-media thickness: a case control study. BioMed Cardiovascular Disord. 2018;18(1). doi:10.1186/s12872-018-0874-5
21. Costa KCM, Del Ciampo LA, Silva PS, Lima JC, De Paula Martins W, Nogueira-De-Almeida CA. Marcadores Ultrassonográficos De Risco Cardiovascular Em Crianças Obesas. Rev Paulista Pediatria. 2018;36(2):171–175. doi:10.1590/1984-0462/;2018;36;2;00016
22. Sorof JM, Poffenbarger T, Franco K, Bernard L, Portman RJ. Isolated systolic hypertension, obesity, and hyperkinetic hemodynamic states in children. J Pediatr. 2002;140(6):660–666. doi:10.1067/mpd.2002.125228
23. Sorokman TV, Popeliuk NO. Obesity in children: criteria for predicting the development of hypertension. Int J Endocrinol. 2020;16(2):138–144. doi:10.22141/2224-0721.16.2.2020.201299
24. Khutsishvili N, Geldiyeva S, Nikishova T, et al. Disorders of the neurohumoral, psychological, and electroneurophysiological profile in patients with arterial hypertension and exogenous constitutional obesity. J Hypertension. 2025;43(Suppl 1):e189. doi:10.1097/01.hjh.0001117128.88673.13
25. Wang P, Liu M, Zhuang X, et al. Association of metabolically healthy obesity in young adulthood with myocardial structure and function. Int J Obesity. 2023;47(5):399–405. doi:10.1038/s41366-023-01288-3
26. Litwin M, Michałkiewicz J, Gackowska L. Primary hypertension in children and adolescents is an immuno-metabolic disease with hemodynamic consequences. Curr Hypertens Rep. 2013;15(4):331–339. doi:10.1007/s11906-013-0360-5
27. Dziedzic-Jankowska K, Kołodziej M, Skrzypczyk P. Association of subclinical inflammation markers with primary hypertension in children—a systematic review with meta-analysis. J Clin Med. 2025;14(7):2319. doi:10.3390/jcm14072319
28. Iqbal J, Wu H, Nawaz MA, et al. Risk of incident chronic kidney disease in metabolically healthy obesity and metabolically unhealthy normal weight: a systematic review and meta‐analysis. Obesity Rev. 2023;25(2). doi:10.1111/obr.13656
29. Lee JW. Obesity and chronic kidney disease: what should pediatric nephrologists know? Clin Experimental Pediatrics. 2021;64(10):521–522. doi:10.3345/cep.2021.00556
30. Kotsis V, Martinez F, Trakatelli C, Redon J. Impact of obesity in kidney diseases. Nutrients. 2021;13(12):4482. doi:10.3390/nu13124482
31. Chernyshov VA, Nesen AA. Obesity as a risk factor for chronic kidney disease: a contemporary view on the problem. Ukrainian Therapeutical J. 2023;(3):62–70. doi:10.30978/utj2023-3-62
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.