Back to Journals » Patient Preference and Adherence » Volume 19
Between Surveillance and Support: A Qualitative Study of Tuberculosis Patients’ Expectations and Concerns About AI-Assisted Remote Health Services in China
Authors Wang X, Xu L, Zhang H, Fu Q
Received 13 June 2025
Accepted for publication 19 August 2025
Published 21 November 2025 Volume 2025:19 Pages 3717—3729
DOI https://doi.org/10.2147/PPA.S546926
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Xiaojun Wang,1,* Luo Xu,2,* Han Zhang,2 Qian Fu2
1Wuhan Pulmonary Hospital, Medical Department, Jianghan University, Wuhan, Hubei, People’s Republic of China; 2School of Medicine and Health Management, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qian Fu, Email [email protected]
Objective: This study explores how tuberculosis (TB) patients in China perceive AI-assisted remote health services, focusing on the psychological and sociocultural dynamics involved in balancing perceived support and perceived surveillance.
Methods: A qualitative descriptive approach was adopted. 25 TB patients were recruited from urban and rural health facilities in Hubei Province, including both those currently in treatment and those who had recently completed it. In-depth, semi-structured interviews were conducted to examine patients’ treatment experiences, digital literacy, and attitudes toward AI-assisted care. The AI system described to participants was a hypothetical prototype based on emerging technologies rather than an implemented service. Thematic analysis was guided by the Health Belief Model and Affordance Theory to identify key patterns and interpret their meanings.
Results: Five key themes emerged. Patients reported treatment fatigue and fluctuating motivation, reflecting complex psychological demands. Trust in AI systems was conditional, shaped by concerns about usability, digital unfamiliarity, and system reliability. Participants experienced a tension between viewing AI tools as supportive and feeling uncomfortable with constant monitoring, especially given the stigmatized and regulated nature of TB. A strong desire to preserve autonomy and dignity shaped patients’ preferences for systems that minimize disruption and allow self-regulation. Acceptability was influenced by interface simplicity, preferred modalities such as voice-based prompts, and the assurance that AI would supplement rather than replace human care. These findings were synthesized into a conceptual framework, illustrating how treatment burden, psychological interpretations of AI, and perceived empowerment converge into a process of contextualized acceptance.
Conclusion: This study offers new insight into digital health engagement among an underserved population. It shows that TB patients do not passively receive AI interventions but interpret and evaluate them in light of their experiences and expectations. Designing acceptable AI-assisted systems requires sensitivity to patients’ social contexts, emotional needs, and desire for agency in care.
Keywords: tuberculosis, artificial intelligence, health management, expectation, concern, qualitative study
Introduction
Tuberculosis (TB) poses ongoing public health, social, and economic challenges in many low- and middle-income countries, including China, where the disease remains highly prevalent and difficult to manage.1,2 Although biomedical treatments and policy-driven control strategies have advanced, effective TB management continues to depend heavily on patients’ sustained adherence to lengthy and often demanding treatment regimens.3,4 In response, China implemented the Directly Observed Treatment, Short-course (DOTS) strategy as a core mechanism for promoting adherence.5 While DOTS has played a critical role in national TB control, it relies on a labor-intensive and logistically complex supervision model that may reinforce stigma, particularly among patients with limited health literacy or those from socioeconomically disadvantaged backgrounds.6 These limitations, especially the burden of face-to-face supervision and its associated psychosocial costs, have prompted growing interest in digital health technologies as more flexible and patient-centered alternatives.7,8 However, digital health adoption remains uneven across China, with urban-rural disparities in health literacy, infrastructure availability, and trust in technology posing additional challenges for equitable access and use.9
As a response to these challenges, advances in digital health have opened new possibilities for reconfiguring traditional disease management models.10 AI-assisted remote health systems, which integrate machine learning, mobile platforms, and real-time data analytics, have emerged as promising tools for enhancing treatment monitoring and supporting patient self-management.11 To date, however, these technologies have been applied primarily in the context of non-communicable diseases such as diabetes and cardiovascular conditions, where they are supported by well-established digital infrastructures and are often perceived as convenient and empowering.12,13 In contrast, the use of AI in TB care remains limited. Only a small number of AI-based remote management tools have been piloted in TB-specific settings (eg, electronic medication monitors and mobile applications for symptom tracking), and little is known about how patients perceive or respond to such systems.14 Despite this limited application, artificial intelligence has been increasingly promoted in policy agendas as part of broader efforts to modernize public health services. In China, national digital health strategies have begun encouraging the development and pilot use of intelligent tools such as AI-enabled follow-up platforms and electronic medication monitors to support infectious disease control. These initiatives reflect growing institutional interest, yet their implementation in TB care remains preliminary and largely unevaluated from the patient perspective.
Within this context, AI-assisted remote health systems in TB care raise a distinct set of challenges, particularly the tension between perceived support and perceived surveillance.15 While these systems may offer tangible benefits such as timely medication reminders, reduced travel, and decreased reliance on face-to-face supervision, they may also generate discomfort related to continuous monitoring, data collection, and concerns over privacy.16,17 For TB patients, who are already subject to heightened public health oversight due to the communicable nature of the disease, the integration of AI may reinforce perceptions of external control rather than foster a sense of supportive care.18 This dynamic is especially pronounced in settings where stigma, mandatory reporting, and institutional regulation shape the everyday experience of treatment.19 Unlike patients with non-communicable diseases, individuals undergoing TB treatment are often positioned not only as recipients of care but also as subjects of public health surveillance and control.2,20
Existing studies on AI-driven health interventions have primarily focused on system design, usability, and clinical outcomes, with limited attention to how patients, particularly those navigating both illness and institutional oversight, interpret the sociotechnical dimensions of these systems.21–23 In the case of TB, where AI infrastructures are not yet widely implemented, patient perspectives remain largely anticipatory. Accordingly, the AI-assisted service discussed in this study was introduced as a hypothetical prototype informed by existing digital tools, allowing participants to reflect on potential benefits, risks, and ethical considerations. Understanding how such technologies are imagined and evaluated is essential for guiding their development in ways that are context-sensitive, ethically sound, and aligned with patient needs. To address this gap, the present study investigates how Chinese TB patients perceive the potential use of AI-assisted remote health management systems, with particular attention to the psychological and sociocultural tensions between support and surveillance. Drawing on an integrated theoretical framework that combines the Health Belief Model (HBM) and Affordance Theory,24,25 the study first explores how patients’ beliefs about disease severity, treatment benefits, and self-efficacy influence their openness to AI-based interventions, as described in HBM. It then examines how these systems are socially interpreted as affording particular possibilities such as discretion, autonomy, or convenience, or as introducing constraints such as intrusion, exposure, or diminished control.
By grounding AI health technologies in the lived experiences of a stigmatized and often marginalized patient population, this qualitative study provides a more nuanced understanding of how digital systems are not only designed but also interpreted, negotiated, and at times resisted by users. In doing so, it extends current digital health scholarship beyond functional and instrumental perspectives by emphasizing the interaction between technical affordances and the socio-institutional realities of infectious disease management. The study offers both theoretical and practical insights for the future development of AI-assisted TB care systems that are responsive to patients’ psychological needs, structural conditions, and expectations for dignity and support.
Materials and Methods
Study Design
This study adopted a qualitative descriptive design, which is well-suited to exploring individual perspectives and experiences within under-researched or complex healthcare contexts.26 This approach was chosen to gain an in-depth understanding of how tuberculosis patients perceive the potential use of AI-assisted remote health management systems in their treatment. As AI-based technologies are still in the exploratory phase in the context of TB care in China, the qualitative approach allowed the researchers to gather detailed, context-specific accounts of patients’ expectations, concerns and interpretations. In-depth, semi-structured interviews were conducted to capture patients’ subjective experiences and views, offering insight into the perceived tension between support and surveillance in AI-enabled health interventions.
Participants and Setting
This study targeted individuals with a confirmed diagnosis of pulmonary TB, including both patients currently undergoing treatment and those who had completed treatment within the past six months. Inclusion criteria were: (1) age 18 years or older; (2) a diagnosis of pulmonary TB recorded in official health facility registries; (3) the ability to provide informed consent and participate in an in-depth interview; and (4) adequate cognitive and language capacity to communicate personal experiences and opinions. Patients with severe psychiatric disorders, cognitive impairments, or other medical conditions that could interfere with the interview process were excluded.
Participants were recruited from designated TB clinics and public health institutions in Wuhan and nearby areas in Hubei Province, China. Recruitment was conducted with the support of local TB prevention and control agencies. Eligible patients were identified through outpatient clinics, follow-up registries, and community-based TB care programs. To capture a range of perspectives, purposive sampling was used to ensure variation in gender, age, treatment stage, and residential setting. Based on the study objectives and methodological guidance for qualitative research, the minimum estimated sample size was set at 20 participants to ensure thematic saturation.27
All interviews were conducted in private, quiet settings within the healthcare facilities or local community health centers. Each participant was provided with a brief, non-technical explanation of the AI-assisted remote health management system under discussion.
Data Collection
Data were collected through semi-structured, in-depth interviews conducted between April and May 2025 in designated TB clinics and affiliated community health centers in Wuhan and surrounding areas of Hubei Province, China. Interviews were conducted in Mandarin by members of the research team with experience in qualitative health research. All interviewers received standardized training in qualitative interviewing and ethical research with stigmatized or vulnerable populations. Before each interview, participants were presented with a plain-language description of a hypothetical AI-assisted remote health management system for TB care.
To facilitate understanding, the system was presented as a conceptual prototype inspired by existing AI-enabled telehealth tools used in chronic disease management in China. In addition to a verbal explanation, participants were shown printed visual materials illustrating how the system would function, including possible interaction formats such as text, voice, and video. The explanation covered core features such as automated reminders, symptom tracking, feedback generation, and risk alerts, as well as basic operational requirements like internet access and smartphone use. It was clarified that the AI component would rely on patient-input data and predefined rules to identify risk patterns and generate tailored feedback. The description aimed to help participants meaningfully engage with the concept, as no such system is currently in routine use.
The interview explored four major themes: patients’ treatment experiences and adherence behaviors, health-related beliefs and motivations, attitudes toward AI-assisted services, and perceptions of support versus surveillance. The interview guide was informed by two theoretical frameworks: the HBM and Affordance Theory. HBM guided questions related to illness perceptions, perceived treatment benefits and barriers, and self-efficacy. Affordance Theory informed inquiry into how participants interpreted the AI system’s potential to enable or constrain autonomy, discretion, convenience, and control. The complete version of the interview guide, along with the selected questions and their partial theoretical alignment, can be found in Appendix 1 (Table S1).
Interviews lasted approximately 25 to 45 minutes and were audio-recorded with informed consent. All recordings were transcribed verbatim in Chinese and subsequently translated into English by trained bilingual researchers familiar with qualitative health research. To ensure consistency and fidelity, translations were reviewed by a second bilingual team member, and discrepancies were resolved through discussion.
Data Analysis
The data were analyzed using thematic analysis, adopting a combined inductive and deductive strategy. Transcripts were first read in full for familiarization. Open coding was then conducted line by line to capture recurring concepts across the data. Similar codes were clustered into subthemes, which were further refined into overarching themes through iterative comparison. NVivo11 was used to support data management and coding. While the analysis remained grounded in participants’ narratives, selected constructs from the HBM and Affordance Theory were used as sensitizing concepts to guide interpretation. Where relevant, emergent subthemes were mapped to these theoretical categories. Themes that could not be accommodated within the frameworks were retained inductively to reflect new insights beyond the initial conceptual model.
To enhance reliability, two researchers independently coded a sample of transcripts and resolved discrepancies through discussion. The coding framework was then applied to the full dataset. Regular team meetings were held to review theme development and ensure consistency in interpretation. Analysis continued until no new major themes emerged.
Ethics Statement
All participants were adults and provided written informed consent prior to participation. The study was approved by the Ethics Committee of Wuhan Pulmonary Hospital (Ethics Number: 20241218) and conducted in accordance with the principles of the Declaration of Helsinki. Participants were informed of their right to withdraw at any time without consequences, and all personal information was anonymized to ensure confidentiality. Interviewers were trained in trauma-informed and nonjudgmental communication techniques to build rapport and reduce participant discomfort.
Results
Characteristics of Participants
This study included 25 patients with TB, comprising 13 men and 12 women aged between 20 and 72 years (mean age: 44.6). Fourteen participants were currently undergoing treatment, while 11 had recently completed it. The sample consisted of 15 urban and 10 rural residents, with diverse educational backgrounds: 8 had completed junior high school, 9 had completed high school, and 8 held a college degree or higher. Eleven participants were employed, while the remaining 14 were retired, unemployed, or engaged in domestic responsibilities. Regarding digital literacy, 10 participants reported being very comfortable using smartphones, 9 somewhat comfortable, and 6 not very comfortable Prior exposure to AI technologies also varied: 6 participants reported frequent use, 6 occasional used, 5 seldom used, and 7 had never used such tools. Participant characteristics are summarized in Table 1.
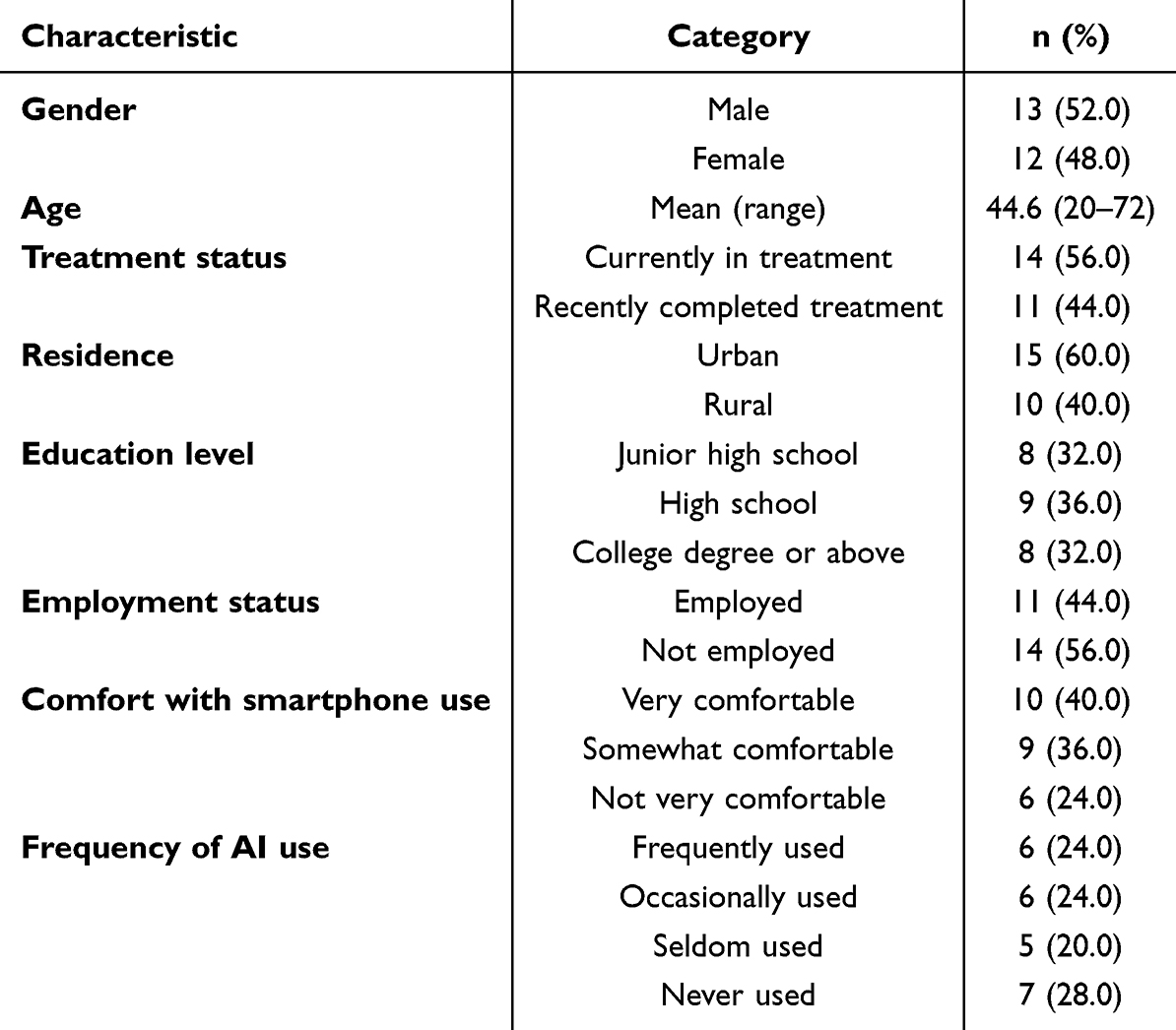 |
Table 1 Participant Characteristics (N = 25) |
Thematic Analysis
This section presents the thematic analysis of patients’ perspectives on AI-assisted remote health services for TB management. Through a structured thematic analysis process, five overarching themes were identified, each comprising several interrelated subthemes that reflect patients’ lived experiences, concerns, and expectations. The themes cover treatment adherence, perceptions of AI, the dual interpretation of technology as either surveillance or support, efforts to preserve autonomy, and contextual conditions that shape acceptability. An overview of these themes and their corresponding subthemes is presented in Table 2.
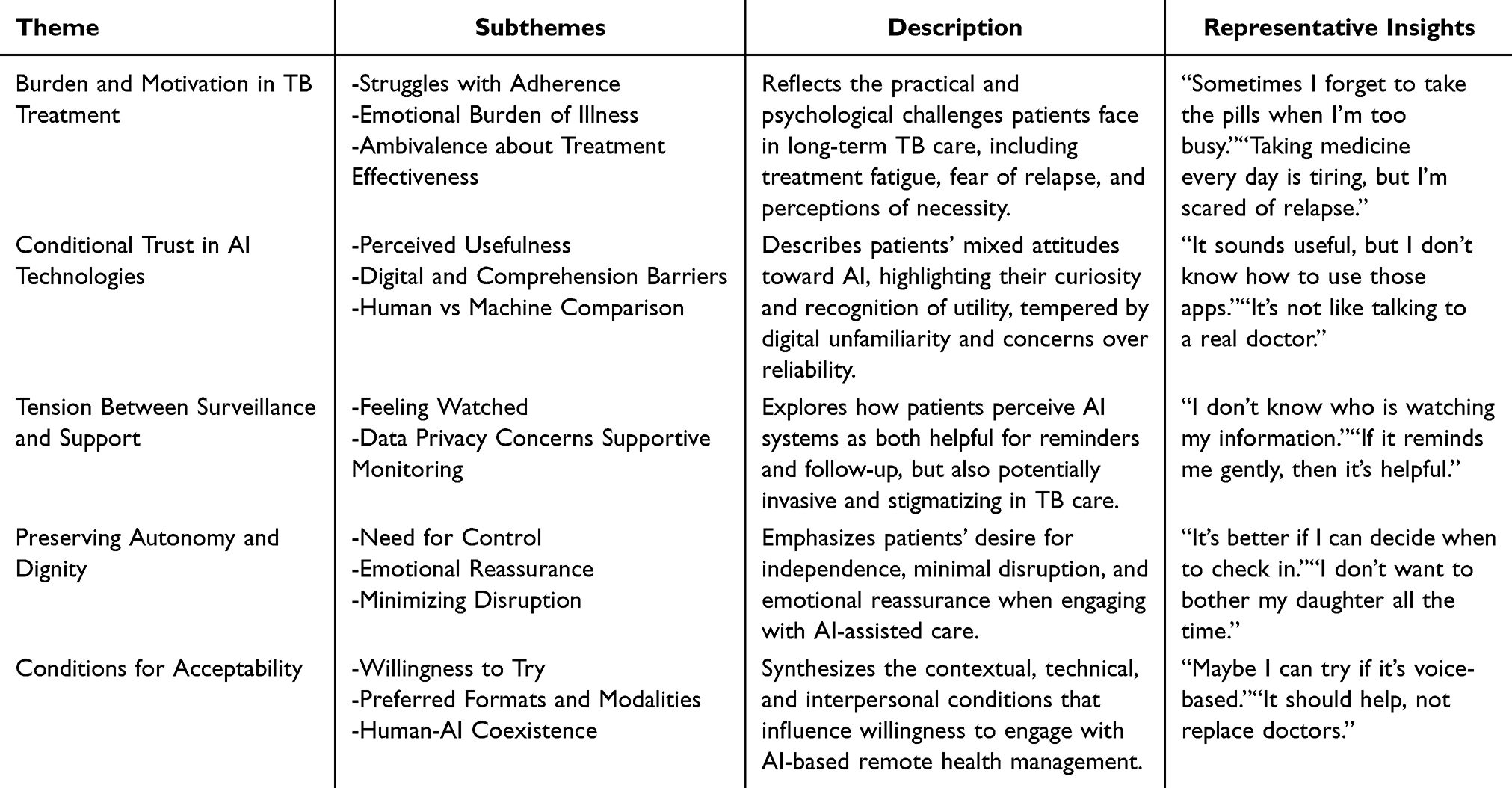 |
Table 2 Theme Framework |
Theme 1: Burden and Motivation in TB Treatment
This theme captures the lived realities of tuberculosis patients as they navigate the physical and emotional challenges of long-term treatment. Participants described both practical and psychological obstacles in maintaining adherence to the treatment regimen, revealing a complex interplay between motivation, fatigue, and belief in the treatment’s efficacy.
Subtheme 1.1: Struggles with Adherence
Many participants admitted difficulties in consistently taking their medications, often due to forgetfulness or disruptions in daily routine. Some relied on family members or external reminders to stay on track. The challenge of sustaining adherence over an extended period emerged as a common concern.
Sometimes I just forget to take it. If someone reminds me, like my husband, I remember. But if no one says anything, I might miss it. (P03, female, 62)
It’s hard to keep up every day for so long. I get tired of it. (P19, male, 60)
Subtheme 1.2: Emotional Burden of Illness
Beyond the logistical demands of treatment, participants expressed a deep emotional toll related to TB, often describing fear, anxiety, and social stigma. The prolonged treatment timeline and uncertainty about full recovery contributed to stress and psychological fatigue.
I’ve been taking medicine for months, but I still worry I’ll get sick again. It’s always on my mind. (P14, male, 19)
Sometimes I feel people are still afraid of me, even after I’ve gotten better. (P22, male, 42)
Subtheme 1.3: Ambivalence About Treatment Effectiveness
While most participants acknowledged the importance of medication, several conveyed doubts about whether the treatment was truly working or worth the effort. This ambivalence often stemmed from slow progress or lingering symptoms, leading to diminished confidence and motivation.
It’s not like I feel much different. I take all these pills, but I still feel tired and cough sometimes. (P08, male, 51)
The doctor says I need to keep taking it, but I’m not sure if it’s helping that much. (P05, female, 70)
Theme 2: Conditional Trust in AI Technologies
This theme captures the ambivalence of participants towards AI-assisted remote health services. While many participants expressed interest in the potential benefits of such technologies, their enthusiasm was often tempered by limited digital literacy and skepticism about the reliability and adequacy of AI compared to human care. Trust in AI was found to be conditional, depending on the system’s usability and its ability to replicate essential human qualities.
Subtheme 2.1: Perceived Usefulness
Several participants acknowledged the practical value of AI in managing their health, particularly in supporting medication adherence and reducing the need for clinic visits. Automated reminders, remote monitoring, and access to health information were seen as potentially helpful features that could ease the burden of treatment.
If it reminds me to take medicine, that’s good. Sometimes I forget, especially when I’m busy. (P10, female, 39)
It can help me check how I’m doing without always going to the hospital. That would be more convenient. (P21, male, 61)
Subtheme 2.2: Digital and Comprehension Barriers
Despite recognizing potential benefits, many participants reported difficulty using digital tools, particularly complex apps or text-heavy interfaces. Barriers related to age, literacy, and lack of prior exposure to technology limited their willingness or ability to engage with AI-based systems.
I can use my phone to make calls, but apps are too difficult. I don’t understand them. (P06, male, 41)
Sometimes I can’t read the words clearly... if it’s voice, maybe I can try. But it has to be simple. (P18, female, 74)
Subtheme 2.3: Human vs Machine Comparison
Participants often contrasted AI with human healthcare providers, expressing a preference for personal interaction, empathy and reassurance. Although they viewed AI as potentially helpful for routine tasks, many were reluctant to rely on it for complex care decisions, highlighting the enduring importance of human relationships in healthcare.
Machines are smart, but they don’t know how you feel. A doctor can talk to you and understand. (P11, female, 37)
I’d rather go to the hospital and talk to someone, especially when I’m not feeling well. (P23, male, 33)
Theme 3: Tension Between Surveillance and Support
This theme explores the dual perception of AI-assisted systems: as enablers of supportive care, and as sources of discomfort due to monitoring and privacy concerns. While some participants welcomed helpful tools such as medication reminders and remote follow-up, others were uneasy about constant surveillance, particularly in the context of TB, a disease which is often stigmatized. These tensions reveal the fine line between perceived care and perceived control.
Subtheme 3.1: Feeling Watched
Several participants described a sense of being monitored when interacting with AI systems. Even well-intentioned features could trigger discomfort if they were perceived as overly intrusive or lacking transparency. For TB patients, whose diagnosis may already subject them to societal scrutiny, this feeling was amplified.
Sometimes I feel like someone is watching me through the system. I don’t know who it is, and it makes me uneasy. (P09, male, 25)
If I don’t take the medicine and it records it, will someone know? Will it affect my treatment? (P02, female, 25)
Subtheme 3.2: Data Privacy Concerns
Concerns about data security and the lack of clarity on how personal health information is used or shared were common. Participants were particularly worried about unintended consequences, such as stigma or institutional penalties, arising from their digital health data being accessed by others.
I don’t know who is watching my information. I hope it doesn’t go to the wrong people. (P13, male, 43)
I’m not sure if the data goes to the doctor or somewhere else. That makes me nervous. (P01, male, 35)
Subtheme 3.3: Supportive Monitoring
Despite these concerns, many participants recognized the potential of AI systems to improve follow-up and provide timely, non-intrusive support, provided they felt in control. Monitoring was more readily accepted when it was framed as gentle and empowering rather than punitive.
If it reminds me gently, then it’s helpful. I can still decide what to do. (P22, male, 42)
It saves time and helps me stay on track with medicine. But I want to be the one choosing. (P10, female, 39)
Theme 4: Preserving Autonomy and Dignity
This theme highlights patients’ strong preference for maintaining control over their health management and interactions with AI-assisted systems. Participants expressed a need for emotional reassurance, minimal disruption to daily life, and the ability to engage with technology on their own terms. For many, the appeal of AI systems depended not only on functionality but also on whether they preserved a sense of independence and dignity throughout the care experience.
Subtheme 4.1: Need for Control
Several participants emphasized the importance of being able to choose when and how to interact with AI-based tools. They favored systems that supported self-regulation rather than enforced strict routines, viewing autonomy as a core component of respectful care.
It’s better if I can decide when to check in. I don’t like being told exactly what to do. (P25, female, 26)
Reminders are fine, but I still want the choice to delay or skip if I’m busy. (P02, female, 44)
Subtheme 4.2: Emotional Reassurance
AI tools that could provide timely feedback or gentle encouragement were generally welcomed, especially when they helped patients feel secure without adding pressure. Emotional support, even when automated, was considered meaningful as long as it respected users’ emotional states.
Sometimes I just want a simple reminder. It feels like someone cares. (P17, female, 40)
Knowing it’s there gives me peace of mind, even if I don’t use it every day. (P08, male, 51)
Subtheme 4.3: Minimizing Disruption
Participants appreciated AI features that reduced the need for frequent clinic visits or external assistance. This was particularly valued by those who did not want to burden family members or health workers for routine matters, underscoring a desire to manage illness discreetly and efficiently.
I don’t want to bother my daughter all the time. If the app can help me check, that’s good. (P19, male, 60)
If I don’t need to go to the hospital each time, it saves everyone trouble. (P21, male, 61)
Theme 5: Conditions for Acceptability
This theme summarizes the contextual, technical and relational factors that influence TB patients’ willingness to accept AI-assisted remote health management. While many participants expressed a willingness to try new tools, this was conditional on aspects such as interface design, preferred communication methods, and assurances that AI would complement, rather than replace, human care. These findings highlight the importance of addressing patients’ preferences, limitations, and trust concerns for successful implementation.
Subtheme 5.1: Willingness to Try
Participants commonly expressed a cautious openness toward AI-assisted services. This willingness was often framed as conditional, shaped by their comfort level with technology and the perceived ease of use.
Maybe I can try if it’s voice-based. Reading is harder for me. (P20, male, 53)
I’ve never used this kind of thing, but if someone teaches me slowly, I can learn. (P15, male, 50)
Subtheme 5.2: Preferred Formats and Modalities
Patients voiced clear preferences for voice-based interfaces over text-heavy applications, especially those with limited literacy or digital skills. Simplicity, local language support, and minimal interaction steps were commonly cited as critical to usability.
If it talks to me like a person, that’s better. I don’t always understand the words. (P05, female, 70)
I can press a button or listen, but too many steps and I’ll forget. (P12, male, 39)
Subtheme 5.3: Human-AI Coexistence
A recurring sentiment was that AI tools should serve as supplementary support rather than replacements for human providers. Participants emphasized the irreplaceable value of personal interaction, trust, and empathy in care relationships.
It should help, not replace doctors. I still need to see a real person sometimes. (P07, male, 20)
AI is fine for reminders or small things, but for big decisions, I want to talk to my doctor. (P24, female, 46)
Conceptual Synthesis
Building on the thematic analysis, we synthesized the empirical themes into higher-order conceptual categories to clarify how TB patients perceive and evaluate AI-assisted remote health services. This synthesis connects participants’ lived experiences with theoretical constructs from the Health Belief Model (HBM) and Affordance Theory, enabling a deeper interpretive understanding of patient behavior beyond descriptive accounts.
At the foundation of this conceptual structure is treatment burden and self-regulation, which captures the long-term physical and psychological challenges faced by TB patients. Participants described inconsistent medication adherence, fatigue resulting from extended treatment durations, and uncertainty regarding the effectiveness of therapy. These accounts reflect key components of the Health Belief Model, including perceived severity, perceived benefits, and self-efficacy, while also highlighting the ways in which patients regulate their behavior to maintain adherence over time.
Building on this foundation, the analysis identifies three interrelated psychological constructs that shape how patients interpret and evaluate AI-based interventions. The first, conditional technological trust, reflects patients’ simultaneous recognition of AI’s potential utility and hesitation stemming from limited digital literacy, unfamiliarity with system features, and doubts about reliability. This construct aligns with the HBM’s perceived barriers and the affordance perspective on system usability and accessibility.
The second construct, surveillance–support paradox, captures the tension between perceiving AI as a helpful tool and as a mechanism of control. While participants acknowledged the value of reminders and remote monitoring, many expressed unease about constant surveillance, data privacy, and the potential for judgment or punitive consequences. These concerns are heightened in the TB context, where public health oversight is already present. This construct reflects both perceived threat in the HBM and the dual affordances of technology as simultaneously enabling and constraining.
The third construct, patient autonomy and technological empowerment, centers on the desire to maintain control over health-related decisions while receiving assistance. Participants responded more positively to AI when it supported independence, respected routines, and complemented rather than replaced human care. This construct corresponds to the HBM’s emphasis on self-efficacy and cues to action, as well as the affordance theory’s notion of action possibilities grounded in user agency.
These three constructs converge into the overarching concept of contextualized acceptance, which posits that patient willingness to adopt AI-assisted services is shaped by a dynamic evaluation of technological, social, and emotional factors. Acceptance is not a uniform response but a negotiated outcome, influenced by trust, perceived support, autonomy, and contextual relevance. Figure 1 presents this conceptual framework, illustrating how the treatment burden informs psychological engagement with AI, which in turn affects acceptance. The model offers an integrated understanding of patient responses to AI-assisted care and provides a foundation for the development of ethically sensitive, user-centered interventions.
 |
Figure 1 Conceptual framework. |
Discussion
This study examined how TB patients in China perceive the potential use of AI-assisted remote health services, with particular attention to the psychological and sociocultural dynamics between perceived support and surveillance. The thematic analysis identified five key domains. Patients described the burden of long-term treatment and the emotional toll it entails, illustrating a complex motivational landscape affecting adherence. Attitudes toward AI systems were characterized by conditional trust, reflecting a balance of curiosity and caution shaped by digital literacy and concerns about system reliability. AI technologies were simultaneously viewed as supportive and intrusive, revealing tension between their monitoring functions and patients’ desire for dignity and privacy. Autonomy emerged as a central concern, with participants favoring systems that minimized disruption and respected personal agency. Ultimately, the acceptability of AI-assisted services depended on usability, clarity, and whether they were perceived as complementary to, rather than substitutes for, human care.28
This study offers one of the first empirical investigations into AI-assisted digital health technologies within the specific context of TB management. Although prior research has explored AI-based interventions in non-communicable diseases such as diabetes or hypertension, few studies have addressed their relevance or reception in the management of communicable and highly regulated conditions like TB.29 This omission is particularly important, as TB patients often receive care under conditions of institutional surveillance, social stigma, and psychological vulnerability.30 By focusing on this underrepresented population, the study contributes new insights to the literature on digital health engagement, where the dominant emphasis has been on settings with higher technological readiness and patient autonomy.
This research contributes to the theoretical understanding of digital health engagement by integrating the HBM and Affordance Theory to interpret how patients evaluate emerging technologies. While the HBM has traditionally addressed individual beliefs about illness and behavior, our findings demonstrate that such beliefs are inseparable from patients’ perceptions of technological design, accessibility, and symbolic meaning in digitally mediated care.31 The construct of conditional technological trust extends the HBM’s notion of perceived barriers by illustrating how digital unfamiliarity, usability concerns, and emotional ambivalence jointly influence receptivity. Likewise, the support-surveillance paradox complicates the narrative of AI as an inherently empowering tool, emphasizing that monitoring functions may reinforce perceived threats and social vulnerability, particularly in stigmatized infectious disease contexts.20 From the perspective of Affordance Theory, this study offers insight into how the same technical features can be understood as either enabling or constraining, depending on users’ social context, expectations, and degree of trust.32 Participants evaluated AI affordances not solely in functional terms, but through a lens shaped by their treatment burden, social roles, and experiences of institutional oversight. The concept of contextualized acceptance underscores that patient engagement with AI technologies involves an ongoing evaluative process in which emotional, relational, and structural dimensions are continuously weighed.33
These insights have several practical implications. In terms of design, AI systems should be developed with features that support low-literacy users, including voice-based interfaces, simplified navigation, and culturally appropriate language. Ensuring transparency in data management and offering users meaningful choices about how and when their information is shared can help reduce anxiety and foster trust.34 In terms of service delivery, community health workers and primary care providers play a vital role in mediating between patients and technology.35 Their ability to provide guidance, emotional reassurance, and hands-on assistance can help bridge the gap between system functionality and patient needs.36 Training health personnel to serve as digital facilitators is particularly important in settings where relational care remains a primary source of patient trust.37
From a policy perspective, the findings highlight the importance of integrating equity and ethics into digital health strategies. AI-supported interventions should be evaluated not only for clinical efficacy and efficiency, but also for their acceptability, accessibility, and social impact.38 Consistent with emerging global frameworks, recent ethical and regulatory guidance has emphasized the principles of transparency, accountability, equity, and human oversight in the development and deployment of AI technologies in health care.39,40 These considerations are especially pertinent in the context of tuberculosis, where stigma, surveillance, and structural asymmetries may exacerbate patient vulnerability. Our results underscore that patient acceptance of AI-assisted services depends not only on technical utility, but also on whether such systems are perceived as respectful, non-intrusive, and ethically aligned. To support responsible innovation, policymakers should promote inclusive innovation frameworks that prioritize infrastructure development, affordability, and participatory system design, particularly for vulnerable or digitally underserved populations.41
Several limitations should be noted. The sample was drawn from a single province, which may limit transferability to other regions or health systems. In addition, interviews were conducted in Mandarin and translated into English, which may have introduced interpretive loss. Moreover, as AI tools for TB care remain largely conceptual in China, participant responses reflect anticipatory perceptions rather than direct experience. Future research could expand upon these findings in several directions. Comparative studies could examine how disease type, stigma, and treatment trajectories influence technology interpretation. Longitudinal and experimental designs could assess whether patients’ initial attitudes evolve with real-world use. Finally, integrating participatory design, usability testing, and behavioral tracking could yield actionable insights into how AI interventions are adapted in practice and experienced across diverse patient populations.
Conclusion
While patients acknowledged the potential benefits of AI-assisted remote health services in supporting treatment adherence and reducing burden, they also expressed concerns about surveillance, loss of autonomy, and usability. These findings emphasize that AI in TB care functions not only as a supportive tool but also as a source of psychological tension. Designing acceptable and effective systems requires attention to patients’ lived experiences, digital capabilities, and sociocultural contexts. Incorporating patient perspectives into system development is essential to ensure that AI technologies are human-centered, ethically responsive, and sensitive to both individual and social dimensions of care.
Acknowledgments
This study was supported by the National Natural Science Foundation of China (Grant Number 72404105 and 72104083), and the Knowledge Innovation Specialized Basic Research Project of Wuhan Science and Technology Bureau (Grant Number 2023020201010213).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Ndjeka N, Jassat W. Cash incentives as a bold new strategy for tuberculosis control. Lancet Infect Dis. 2025. doi:10.1016/S1473-3099(25)00030-1
2. Bloom BR. A half-century of research on tuberculosis: successes and challenges. J Exp Med. 2023;220:e20230859. doi:10.1084/jem.20230859
3. Naidoo K, Perumal R, Cox H, et al. The epidemiology, transmission, diagnosis, and management of drug-resistant tuberculosis—lessons from the South African experience. Lancet Infect Dis. 2024;24:e559–75. doi:10.1016/S1473-3099(24)00144-0
4. Zumla A, Abubakar I, Raviglione M, et al. Drug-resistant tuberculosis—current dilemmas, unanswered questions, challenges, and priority needs. J Infect Dis. 2012;205:S228–40. doi:10.1093/infdis/jir858
5. Chen X, Zhou J, Yuan Q, et al. Challenge of ending TB in China: tuberculosis control in primary healthcare sectors under integrated TB control model–a systematic review and meta-analysis. BMC Public Health. 2024;24:163. doi:10.1186/s12889-023-16292-5
6. Netto TAL, Diniz BD, Odutola P, et al. Video-observed therapy (VOT) vs directly observed therapy (DOT) for tuberculosis treatment: a systematic review on adherence, cost of treatment observation, time spent observing treatment and patient satisfaction. PLoS Negl Trop Dis. 2024;18:e0012565. doi:10.1371/journal.pntd.0012565
7. Guo X, Yang Y, Takiff HE, et al. A comprehensive app that improves tuberculosis treatment management through video-observed therapy: usability study. JMIR mHealth and uHealth. 2020:
8. Guo P, Qiao W, Sun Y, et al. Telemedicine technologies and tuberculosis management: a randomized controlled trial. Telemed E-Health. 2020;26:1150–1156. doi:10.1089/tmj.2019.0190
9. Zhao Y, Li J. Opportunities and challenges of integrating artificial intelligence in China’s elderly care services. Sci Rep. 2024;14:9254. doi:10.1038/s41598-024-60067-w
10. Ngwatu BK, Nsengiyumva NP, Oxlade O, et al. The impact of digital health technologies on tuberculosis treatment: a systematic review. Eur Respir J. 2018:51. doi:10.1183/13993003.01596-2017
11. Pong C, Tseng RMWW, Tham YC, et al. current implementation of digital health in chronic disease management: scoping review. J Med Internet Res. 2024;26:e53576. doi:10.2196/53576
12. Pelly M, Fatehi F, Liew D, Verdejo-Garcia A. Artificial intelligence for secondary prevention of myocardial infarction: a qualitative study of patient and health professional perspectives. Int J Med Inform. 2023;173:105041. doi:10.1016/j.ijmedinf.2023.105041
13. Potapenko I, Thiesson B, Kristensen M, et al. Automated artificial intelligence-based system for clinical follow-up of patients with age-related macular degeneration. Acta Ophthalmologica. 2022;100:927–936. doi:10.1111/aos.15133
14. Streba CT, Şerbănescu M-S, Miulescu A, et al. TB-monitor: advancing tuberculosis management through innovative technologies. Appl Med Informat. 2025;47:S29–S29.
15. Bavli I, Ho A, Mahal R, et al. Ethical concerns around privacy and data security in AI health monitoring for Parkinson’s disease: insights from patients, family members, and healthcare professionals. AI & Soc. 2025;40:155–165. doi:10.1007/s00146-023-01843-6
16. Fazakarley C-A, Breen M, Thompson B, et al. Beliefs, experiences and concerns of using artificial intelligence in healthcare: a qualitative synthesis. Digital Health. 2024. doi:10.1177/20552076241230075
17. Witkowski K, Okhai R, Neely SR. Public perceptions of artificial intelligence in healthcare: ethical concerns and opportunities for patient-centered care. BMC Med Ethics. 2024;25:74. doi:10.1186/s12910-024-01066-4
18. Kim AJ, Yang J, Jang Y, et al. Acceptance of an informational antituberculosis chatbot among korean adults: mixed methods research. JMIR mHealth and uHealth. 2021;9:e26424. doi:10.2196/26424
19. Yuan Y, Jin J, Bi X, et al. Gender-specific association between perceived stigma toward tuberculosis and acceptance of preventive treatment among college students with latent tuberculosis infection: cross-sectional analysis. JMIR Public Health Surveill. 2023;9:e43972. doi:10.2196/43972
20. Datiko DG, Jerene D, Suarez P. Stigma matters in ending tuberculosis: nationwide survey of stigma in Ethiopia. BMC Public Health. 2020;20:190. doi:10.1186/s12889-019-7915-6
21. Hendrix N, Veenstra DL, Cheng M, et al. Assessing the economic value of clinical artificial intelligence: challenges and opportunities. Value Health. 2022;25:331–339. doi:10.1016/j.jval.2021.08.015
22. Wang B, Asan O, Zhang Y. Shaping the future of chronic disease management: insights into patient needs for AI-based homecare systems. Int J Med Inform. 2024;181:105301. doi:10.1016/j.ijmedinf.2023.105301
23. Kuziemsky CE, Chrimes D, Minshall S, et al. AI quality standards in health care: rapid umbrella review. J Med Internet Res. 2024;26:e54705. doi:10.2196/54705
24. Rosenstock IM. Health Belief Model. In: Kazdin AE, editor. Encyclopedia of psychology. Vol. 4. Oxford University Press; 2000:78–80.
25. Sadler E (Bess), Given LM. Affordance theory: a framework for graduate students’ information behavior. J Doc. 2007;63:115–141. doi:10.1108/00220410710723911
26. Sandelowski M. Whatever happened to qualitative description? Res Nurs Health. 2000;23:334–340. doi:10.1002/1098-240x(200008)23:4<334::aid-nur9>3.0.co;2-g
27. Hennink MM, Kaiser BN, Marconi VC. Code saturation versus meaning saturation: how many interviews are enough? Qual Health Res. 2017;27:591–608. doi:10.1177/1049732316665344
28. Kuo RYL, Freethy A, Smith J, et al. Stakeholder perspectives towards diagnostic artificial intelligence: a co-produced qualitative evidence synthesis. eClinicalMedicine. 2024;71. doi:10.1016/j.eclinm.2024.102555
29. Arefin S. Chronic disease management through an AI-powered application. J Serv Sci Manage. 2024;17:305–320. doi:10.4236/jssm.2024.174015
30. Iribarren SJ, Rodriguez Y, Lin L, et al. Converting and expanding a mobile support intervention: focus group and field-testing findings from individuals in active tuberculosis treatment. Int J Med Inform. 2020;136:104057. doi:10.1016/j.ijmedinf.2019.104057
31. Sazali MF, Rahim SSSA, Mohammad AH, et al. Improving tuberculosis medication adherence: the potential of integrating digital technology and health belief model. Tuberc Respir Dis. 2023;86:82–93. doi:10.4046/trd.2022.0148
32. Li C-Y, Fang Y-H, Chiang Y-H. Can AI chatbots help retain customers? An integrative perspective using affordance theory and service-domain logic. Technol Forecast Soc Change. 2023;197:122921. doi:10.1016/j.techfore.2023.122921
33. Dalton-Brown S. The ethics of medical AI and the physician-patient relationship. Cam Q Healthc Ethics. 2020;29:115–121. doi:10.1017/S0963180119000847
34. Shaik T, Tao X, Higgins N, et al. Remote patient monitoring using artificial intelligence: current state, applications, and challenges. WIREs Data Mining Knowl Discover. 2023;13:e1485. doi:10.1002/widm.1485
35. Allen MR, Webb S, Mandvi A, et al. Navigating the doctor-patient-AI relationship - a mixed-methods study of physician attitudes toward artificial intelligence in primary care. BMC Prim Care. 2024;25:42. doi:10.1186/s12875-024-02282-y
36. Garies S, Liang S, Weyman K, et al. Artificial intelligence in primary care practice: qualitative study to understand perspectives on using AI to derive patient social data. Can Family Physician. 2024;70:e102–9. doi:10.46747/cfp.700708e102
37. Ciecierski-Holmes T, Singh R, Axt M, et al. Artificial intelligence for strengthening healthcare systems in low- and middle-income countries: a systematic scoping review. Npj Digit Med. 2022;5:1–13. doi:10.1038/s41746-022-00700-y
38. van de Sande D, Chung EFF, Oosterhoff J, et al. To warrant clinical adoption AI models require a multi-faceted implementation evaluation. Npj Digit Med. 2024;7:1–5. doi:10.1038/s41746-024-01064-1
39. Organization WH. Regulatory Considerations on Artificial Intelligence for Health. World Health Organization; 2023.
40. Organization WH. Ethics and governance of artificial intelligence for health: large multi-modal models. WHO guidance. World Health Organiz. 2024.
41. Bates DW, Levine D, Syrowatka A, et al. The potential of artificial intelligence to improve patient safety: a scoping review. Npj Digit Med. 2021;4:1–8. doi:10.1038/s41746-021-00423-6
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
LSTM-Based Prediction Model for Tuberculosis Among HIV-Infected Patients Using Structured Electronic Medical Records: A Retrospective Machine Learning Study
Chen J, Liu L, Huang J, Jiang Y, Yin C, Zhang L, Li Z, Lu H
Journal of Multidisciplinary Healthcare 2024, 17:3557-3573
Published Date: 23 July 2024