Back to Journals » Journal of Pain Research » Volume 15
Best Practices for Minimally Invasive Lumbar Spinal Stenosis Treatment 2.0 (MIST): Consensus Guidance from the American Society of Pain and Neuroscience (ASPN)
Authors Deer TR ![]() , Grider JS, Pope JE, Lamer TJ
, Grider JS, Pope JE, Lamer TJ ![]() , Wahezi SE, Hagedorn JM
, Wahezi SE, Hagedorn JM ![]() , Falowski S
, Falowski S ![]() , Tolba R, Shah JM, Strand N
, Tolba R, Shah JM, Strand N ![]() , Escobar A, Malinowski M, Bux A, Jassal N, Hah J
, Escobar A, Malinowski M, Bux A, Jassal N, Hah J ![]() , Weisbein J
, Weisbein J ![]() , Tomycz ND, Jameson J, Petersen EA
, Tomycz ND, Jameson J, Petersen EA ![]() , Sayed D
, Sayed D ![]()
Received 23 December 2021
Accepted for publication 6 April 2022
Published 5 May 2022 Volume 2022:15 Pages 1325—1354
DOI https://doi.org/10.2147/JPR.S355285
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Krishnan Chakravarthy
Timothy R Deer,1 Jay S Grider,2 Jason E Pope,3 Tim J Lamer,4 Sayed E Wahezi,5 Jonathan M Hagedorn,6 Steven Falowski,7 Reda Tolba,8 Jay M Shah,9 Natalie Strand,10 Alex Escobar,11 Mark Malinowski,12 Anjum Bux,13 Navdeep Jassal,14 Jennifer Hah,15 Jacqueline Weisbein,16 Nestor D Tomycz,17 Jessica Jameson,18 Erika A Petersen,19 Dawood Sayed20
1Centers for Pain Relief, Charleston, WV, USA; 2UK HealthCare Pain Services, Department of Anesthesiology, University of Kentucky College of Medicine, Lexington, KY, USA; 3Evolve Restorative Center, Santa Rosa, CA, USA; 4Division of Pain Medicine, Department of Anesthesiology, Mayo Clinic, Rochester, MN, USA; 5Montefiore Medical Center, SUNY-Buffalo, Buffalo, NY, USA; 6Department of Anesthesiology and Perioperative Medicine, Division of Pain Medicine, Mayo Clinic, Rochester, MN, USA; 7Director Functional Neurosurgery, Neurosurgical Associates of Lancaster, Lancaster, PA, USA; 8Pain Management Department, Anesthesiology Institute, Cleveland Clinic, Abu Dhabi, UAE; 9SamWell Institute for Pain Management, Colonia, NJ, USA; 10Department of Anesthesiology, Division of Pain Medicine, Mayo Clinic, Phoenix, AZ, USA; 11Department of Anesthesiology and Pain Medicine, University of Toledo Medical Center, Toledo, OH, USA; 12OhioHealth, Neurological Physicians, Columbus, OH, USA; 13Bux Pain Management, Lexington, KY, USA; 14Excel Pain and Spine, Lakeland, FL, USA; 15Department of Anesthesiology, Perioperative, and Pain Medicine, Stanford University, Palo Alto, CA, USA; 16Napa Valley Orthopaedic Medical Group, Inc., Napa, CA, USA; 17Department of Neurological Surgery, Allegheny General Hospital, Allegheny Health Network, Pittsburgh, PA, USA; 18Axis Spine Center, Coeur d’Alene, ID, USA; 19Department of Neurosurgery, University of Arkansas for Medical Sciences, Little Rock, AR, USA; 20Pain Medicine, Multidisciplinary Pain Fellowship, The University of Kansas Health System, Kansas City, KS, USA
Correspondence: Timothy R Deer, The Spine and Nerve Centers of the Virginias, 400 Court Street, Suite 100, Charleston, WV, 25301, USA, Tel +1 304 347-6141, Email [email protected]
Introduction: Lumbar spinal stenosis (LSS) is a common spinal disease of aging with a growing patient population, paralleling population growth. Minimally invasive treatments are evolving, and the use of these techniques needs guidance to provide the optimal patient safety and efficacy outcomes.
Methods: The American Society of Pain and Neuroscience (ASPN) identified an educational need for guidance on the prudent use of the innovative minimally invasive surgical therapies for the treatment of symptomatic LSS. The executive board nominated experts spanning anesthesiology, physiatry, orthopedic surgery, and neurosurgery based on expertise, publications, research, diversity and field of practice. Evidence was reviewed, graded using the United States Preventive Services Task Force (USPSTF) criteria for evidence and recommendation strength and grade, and expert opinion was added to make consensus points for best practice.
Results: The world literature in English was searched using Medline, EMBASE, Cochrane CENTRAL, BioMed Central, Web of Science, Google Scholar, PubMed, Current Contents Connect, Scopus, and meeting abstracts to identify and compile the evidence (per section) for LSS-related pain. Search words were selected based upon the section represented. Identified peer-reviewed literature was critiqued using USPSTF criteria and consensus points are presented.
Discussion: The algorithm for patient selection in the management of symptomatic spinal stenosis is evolving. Careful consideration of patient selection and anatomic architecture variance is critical for improved outcomes and patient safety.
Conclusion: ASPN created a guidance for best practice for minimally invasive surgical treatment of symptomatic spinal stenosis.
Keywords: percutaneous image-guided lumbar decompression, interspinous spacers, intrathecal drug delivery, open decompression, neurostimulation, epidural steroid injections
Introduction
In 1954, the Dutch neurosurgeon Henk Verbiest provided the first clinical definition of lumbar spinal stenosis (LSS).1 Since that time, LSS has been well studied, and is recognized as a progressive clinical entity involving neurogenic claudication (NC), expected stenotic imaging findings, and chronic nonradicular pain and weakness.2 A recently published systematic review concluded that the pooled prevalence estimates of symptoms of LSS were 11% in the general population and ranged from 25% to 39% in clinical settings.3 Surgical treatments were performed in 135.5 to 137.5 patients per 100,000 Medicare beneficiaries between 2002 and 2007, with estimated hospital costs of $1.65 billion.4 When considering lost or reduced productivity from surgery, costs greater than $100 billion per year have been estimated.5
In 2019, the first version of the minimally invasive spinal treatment (MIST) guidelines was published.6 A consensus group of physician leaders encompassing multiple disciplines, including anesthesiology, physiatry, neurosurgery, and orthopedic surgery, was formed and evaluated the literature regarding diagnosis and minimally invasive treatment of LSS. The authors provided 11 wide-ranging consensus points and concluded that minimally invasive spine treatments should be used algorithmically in a multimodal fashion.
Given the rapidly evolving LSS treatment landscape, a second expert consensus group was formed to update and expand the 2019 MIST guidelines. The objectives of these second MIST guidelines were to review the published literature since the first MIST guidelines, modify existing consensus points based on the latest research, describe a treatment algorithm, and provide new consensus points where new evidence exists. Similar to the 2019 guidelines, the Institute of Medicine (IOM) framework was used to appropriately organize the expert group, evidence, and consensus creation.7 Consensus points were based on the literature where evidence allowed and expert agreement when the literature was incomplete.
Literature Review and Evidence Grading
The MIST expert panel performed systematic literature searches that served as the evidence basis for the recommendations and consensus points. Subgroups were created to focus on specific topics and interventional treatments, including epidural steroid injections (ESI), percutaneous image-guided lumbar decompression (PILD), interspinous spacers, interspinous fusion, neurostimulation, intrathecal drug delivery systems (IDDS), and open decompression. Similar to other consensus guidelines, the current manuscript was prepared using the United States Preventive Services Task Force (USPSTF) criteria for evidence level and degree of recommendation, along with the strength of consensus.8 USPSTF descriptors appear with the consensus points in this publication. In treatment areas with early or incomplete literature, expert consensus was sought to fill gaps in knowledge.
The MIST expert panel was chosen by the executive board of the American Society of Pain and Neuroscience (ASPN) after receiving nominations from members. Selection was based on expertise, publications, speaking engagements, medical specialty, and work in the field. The panel members were also chosen to assure a diversity of practice location, specialty, race, gender, and age. Individual invitations were sent to each of the nominated panel members. Following invitation acceptance, specific assignments were made with multiple panelists assigned to the same topic. In doing so, consensus could be rendered within the subgroup before presenting it to the entire expert panel. Conflict of interest was managed to assure that members recused themselves from any section where a perceived or real conflict of interest existed and some members of the panel with no conflicts of interest edited the paper to remove any potential bias.
Literature Search, Evidence Ranking and Consensus Development
The world literature in English was searched using Medline, EMBASE, Cochrane CENTRAL, BioMed Central, Web of Science, Google Scholar, PubMed, Current Contents Connect, Scopus, and meeting abstracts to identify and compile the evidence (per section as described in the manuscript) for the treatment of LSS-related pain. Search words were selected based upon the section represented. Identified peer-reviewed literature was critiqued using the USPSTF criteria for quality of evidence,8 with modifications for neuromodulation studies (Table 1). After USPSTF letter grading was assigned, the working subgroup then assigned the “level of certainty regarding benefit” as described in Table 2.
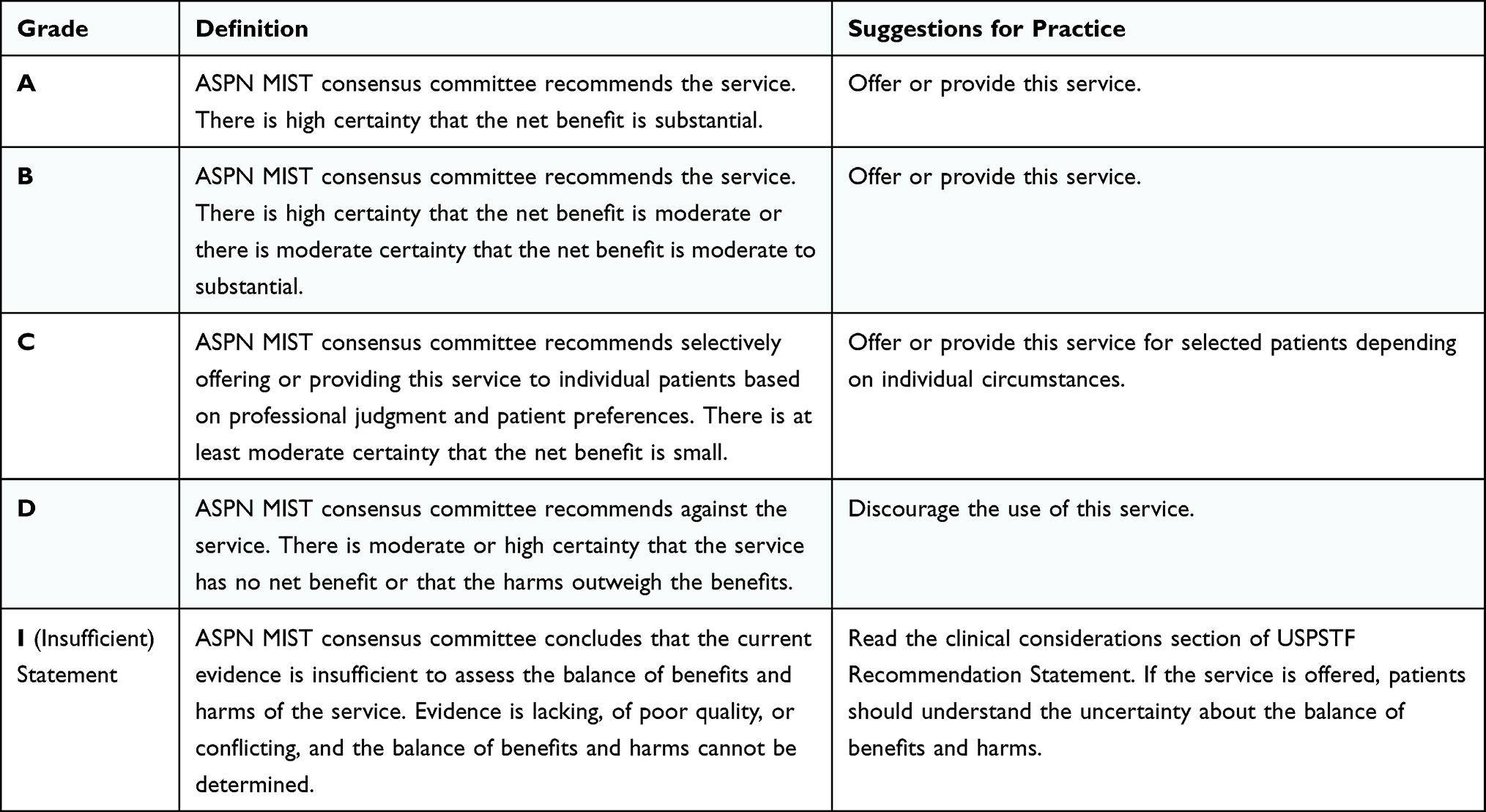 |
Table 1 Quality of Evidence Ranking Using United States Preventative Services Task Force Criteria Modified for Therapy |
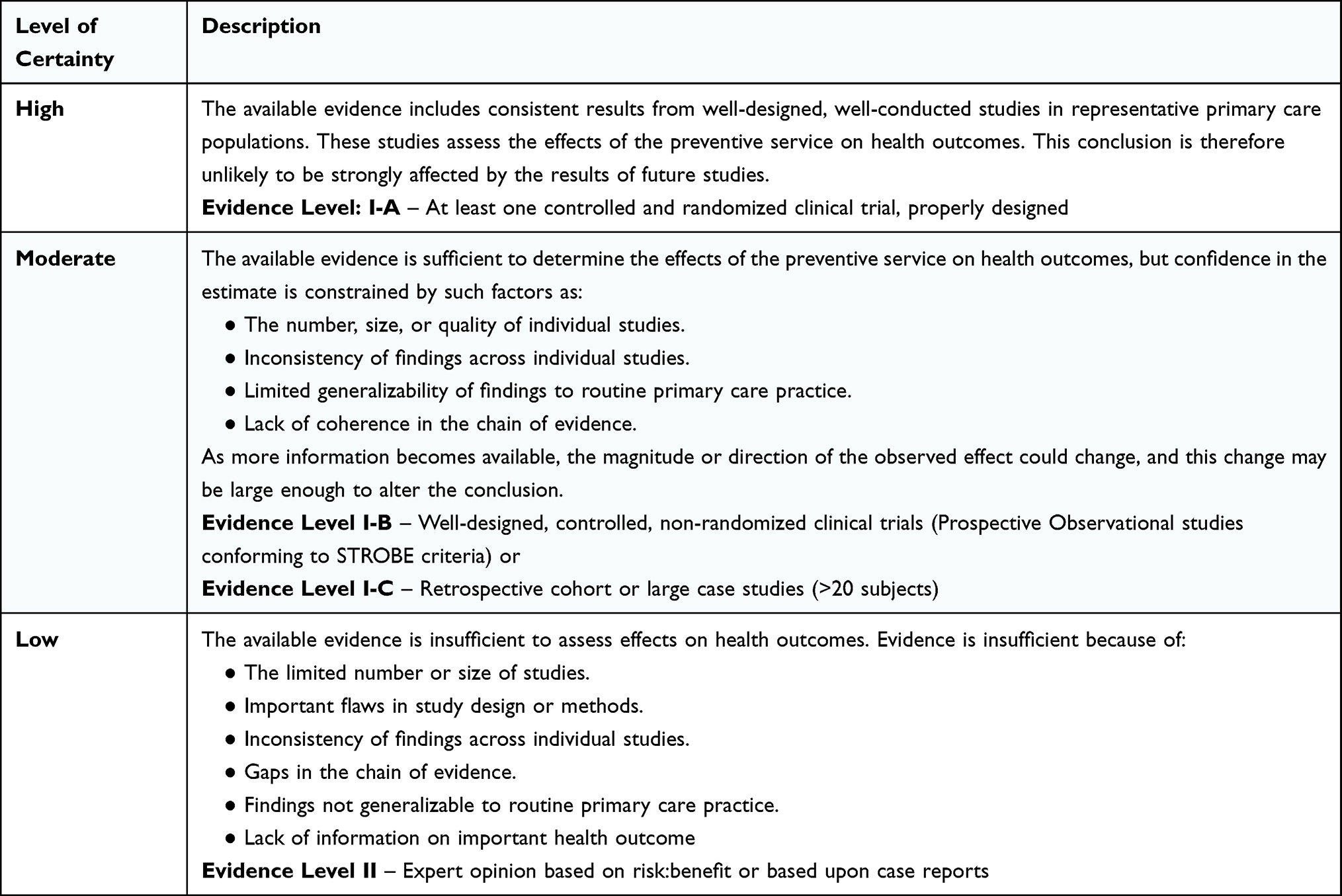 |
Table 2 Levels of Certainty Regarding Net Benefit |
For each major section or topic, ASPN formulated consensus points. These consensus points should not be confused with recommendations based on consensus alone, which were rendered as clinical guidance due to the lack of evidence-based literature (such as randomized controlled trials [RCTs], prospective observational studies, and retrospective cohort/case series). The guidance represented in this manuscript is a directive for best practice and does not necessarily define the standard of care because of individual patient variation.
Lumbar Spinal Stenosis
Introduction
Lumbar spinal stenosis refers to a reduction in anatomical size of the spinal canal, nerve root canals, or neuroforamen that can lead to buttock or leg pain with or without back pain. This definition aims to combine the anatomic anomaly and clinical manifestations of LSS, which contribute to the variability in the diagnosis and management across medical specialties. Although no broadly quantitative criteria for LSS exist, the earliest findings of Dutch neurosurgeon Dr. Verbiest in 1954 are still generally accepted today as relative and absolute stenosis with a lumbar canal diameter of <12 mm and <10 mm (midsagittal diameter), respectively.1 The reduction in spinal canal volume leading to compression of neurovascular elements is further classified as primary (congenital) vs secondary (acquired). The prevalence of acquired or degenerative LSS has been estimated to be approximately 11% in the general population,3 and as high as 47% in those over the age of 60 years.9 Lumbar spinal stenosis remains the most common reason for spine surgery in patients over the age of 65. However, the long-term morbidity and financial burden of open surgical decompression in an aging population provides opportunity for improved treatment approaches. Despite no universal gold standard for the diagnosis of LSS, medical disciplines have relied on expert physician opinion that correlates imaging studies with a detailed history and physical examination. This correlation is necessary as not all patients with narrowing of the central canal present with NC, the most common symptom of LSS. Patients with LSS present with a variable pattern of back, buttock, thigh, or lower leg pain associated with standing or walking. Pain may be confined to the lower extremities or span multiple dermatomes. Patients with LSS may present with paresthesias, numbness, or weakness. A history of leg or buttock pain while walking, lumbar flexion to relieve symptoms, relief when using a shopping cart or bicycle, motor or sensory disturbances while walking, intact and symmetric foot pulses, lower extremity weakness, and low back pain point to a high likelihood of LSS.
Stenosis Characterization
The most common type of LSS is secondary due to degenerative pathology and can involve the central canal, lateral recess, neuroforamen or a combination of these locations. Depending on the anatomical structures involved, clinical manifestations and treatment options will vary. The spinal cord and nerve roots are protected within the central canal and are enclosed circumferentially by osseous, ligamentous, and intervertebral disc structures that all are subject to degeneration and hypertrophy, leading to encroachment of the canal that causes compression of neurovascular tissue. This compression can lead to mechanical and/or chemical irritation.
Central
Central canal stenosis results from a reduction in diameter and volume of the thecal sac either anteroposteriorly (AP) or transversely at a particular intervertebral level. The ventral portion of the canal is comprised of the intervertebral disc, posterior longitudinal ligament and vertebral body, while the dorsal area is made of the posterior vertebral arch (pedicle, lamina, facet joint) and ligamentum flavum (LF). A spinal midsagittal AP diameter of the dural sac that is <10 mm is considered spinal stenosis.10 Central canal stenosis can also be quantified through compression of the thecal sac (as a percentage of the normal midsagittal diameter), and cross-sectional area of the dural sac. A number of qualitative radiological parameters are associated with central canal stenosis, and expert consensus highlights the relationship between fluid and the cauda equina, and compromise of the central zone as reliable parameters for the diagnosis of LSS on imaging.10 The most common clinical phenomenon with central canal stenosis is neurogenic intermittent claudication or pseudoclaudication. This complex clinical syndrome manifests as postural-induced back, buttock, or leg pain, typically bilateral, that is exacerbated by prolonged walking or standing and relieved with sitting posture or forward flexion of the lumbar spine (ie, “shopping cart” sign).
Lateral Recess
The lateral recess (aka the subarticular zone) is the outermost region of the spinal canal that is bordered laterally by the pedicle, posteriorly by the superior articular facet and LF, and anteriorly by the vertebral body, endplate and disc margin. This region is considered stenotic when AP measurement is <4 mm.11 Nerve root compression in the lateral recess is also another important qualitative parameter in the radiological assessment for lateral recess stenosis.10 Due to the close proximity within the canal, stenosis in this region can lead to symptoms of radiculopathy due to nerve root compression with or without NC and can have a bilateral or unilateral presentation.
Foraminal
The neuroforamen is formed by the interpedicular osseous opening in which each spinal nerve root exits the dural sac passing through the lateral recess. The anterior anatomic boundaries of the intervertebral foramen include the adjacent superior-inferior vertebral pedicles, posteroinferior margin of the superior vertebral body, the intervertebral disc, and the posterosuperior margin of the inferior vertebral body, and the posterior anatomic boundaries include the LF and the superior and inferior articular facets.11 This region has three anatomical zones: internal, intraforaminal and extraforaminal. Degenerative changes such as hypertrophy and bone spurs from facet joints and bulging or herniated discs often contribute to foraminal stenosis.12 The neuroforamen are considered stenotic based on reduced perineural fat and/or reduced foraminal dimensions on MRI. A height less than 15 mm and a posterior disc height of 4 mm or less are associated with significant nerve root compression.12 Lumbar foraminal stenosis has a reported prevalence of 8% to 11%.4 Symptoms of pure foraminal stenosis typically are due to neural compression or neural irritation from an inflammatory cascade with a dermatomal distribution. Although no clinical finding is specific enough to suggest foraminal stenosis, patients often present with radicular leg pain and limited lumbar range of motion, particularly with extension. Low back pain, particularly in the buttock region, is often associated with foraminal stenosis.
Multistructural
Multistructural narrowing involving the central, lateral recess, and neuroforamen is the most frequently encountered LSS in those >60 years old. The narrowing typically has a trefoil or cloverleaf appearance on axial cross-sections, in which all three regions of the spinal canal are narrowed. Symptoms are a combination of the above with nonspecific physical examination findings.
Work-Up
Patient-Specific History
Symptomatic LSS often manifests with NC, with people in their sixth or seventh decade of life most affected.13 The typical manifestation of NC is progressive pain radiating to one or both lower extremities in the posterior aspect of the thighs and legs. The pain is typically reproduced by walking, prolonged standing and lumbar spine extension, and typically improves or resolves with sitting and lying down. Walking in a flexed position, such as pushing a shopping cart, can also relieve the pain. Patients often complain of a sense of heaviness and numbness of the lower extremities. As the condition progresses, patients may suffer from neurological deficits and autonomic dysfunction that may require surgical intervention. The symptoms are typically worse when the patient walks downhill due to increased lumbar lordosis; on the other hand, they may be less severe when the patient walks uphill or rides a bicycle due to spine flexion. We can often observe patients stooping forward while walking, to increase the diameter of the spinal canal.14 Particularly in older people, the clinical picture may be blurred by accompanying comorbidities, such as peripheral vascular disease, which can present clinically as vascular claudication (VC). To differentiate between the NC and VC, VC typically does not get better with forward flexion or walking uphill. Other comorbidities such as osteoporosis may also be present, which may be an important consideration if open surgical procedures are being considered.
Patients with LSS can also have superimposed radicular pain or mechanical back pain, leading to a mixed clinical picture. Lumbar radicular pain can be present unilaterally in cases of lateral recess stenosis or foraminal stenosis causing nerve root compression. Patients with LSS may also complain of nociceptive axial back pain due to lumbar facet arthropathy. The Zurich Claudication Questionnaire (ZCQ), Swiss Spinal Stenosis Questionnaire (SSSQ), and the Walking Tolerance Test (WTT) are validated instruments for assessment of spinal stenosis NC.15–20
Focused Physical Examination Findings
Building on the description of physical examination for symptomatic spinal stenosis patients outlined in the MIST 1.0, the physical examination findings in patients with LSS can be normal or nonspecific. In 1977, Dyck and Doyle reported the utility of Van Geldern’s bicycle test in the differentiation of VC vs NC.21 In patients who had symptoms due to LSS, their symptoms improved while leaning forward to ride a bicycle. Katz et al discussed that patients with LSS often demonstrated wide-based gait, abnormal Romberg testing, lower extremity pain following 30 seconds of lumbar extension (Kemp’s test), and other neuromuscular abnormalities.17 Unfortunately, Fritz et al concluded that these physical examination findings had a positive and negative likelihood ratio close to 1, indicating that these variables did not help rule LSS in or out.22
On examination, patients often ambulate with a flexed posture as this creates a stretch on the LF, decreasing its diameter and protecting it from buckling and creating increased pressure in the narrowed canal.23 Patients often develop a “simian stance” with their hips and knees also slightly flexed.24 Iversen and Katz also found that pain and balance were the primary limiting factors with regard to ambulation in patients with LSS.25 Patients may also exhibit limited mobility in extension of the lumbar spine.26 The neurological examination may be normal or vague, but changes may be noted after patients perform symptomatic exercises.27 Some patients may present with more radicular symptoms related to lateral recess or foraminal stenosis, and may be younger26 or present with pain at night or rest, aggravated by the Valsalva maneuver.28
Electromyogram (EMG) and nerve conduction velocity (NCV) often are normal or may demonstrate multisegmental abnormalities in the bilateral lower extremities that do not correlate to symptoms evidenced by positive findings in asymptomatic control subjects.29 While EMG and NCV may be useful adjunctive diagnostic tools in distinguishing peripheral neuropathy from LSS, these tests may not be specific enough to aid in diagnosis.30–32
Radiographic Findings
The previous edition of the MIST guidelines extensively reviewed the radiographic analysis that is required to evaluate a patient with symptoms of LSS.6 The radiographic analysis section has been cited by studies since publication, demonstrating the need for a single repository of clinical information on this topic.33 In the time interval since publication of the previous edition of the MIST guidelines, there have been studies that build upon the foundational descriptive approach used in the radiographic analysis section of that manuscript. Hartman et al, in their technical review, used the necessary interplay between the dynamic flexion/extension film and the combined axial views on CT and MRI to determine optimal evaluation of soft tissue and ligamentous structures vs bony overgrowth in both central and lateral canal stenosis. Their technical report suggests that measurements in the sagittal view alone underestimate lateral stenosis.33 The authors suggest that measurement in all planes of the axial and sagittal view with both CT and MRI may lead to better preprocedural planning, whether for direct or indirect decompression. In agreement with this approach, a recent study suggested that sagittal radiographic analysis showed a poor correlation with postoperative outcomes.34
There is growing evidence suggesting that conventional MRI evaluation may overestimate the lateral recess dimensions in patients with LSS. A small study recently demonstrated that in LSS subjects mean foraminal area decreased by 13% when moving from supine to upright imaging and was further impacted by hyperlordotic positioning (21% reduction in area from supine to hyperlordosis), suggesting that the positioning of maximal symptoms (hyperlordosis) is poorly evaluated by traditional imaging positioning.35 The superiority of MRI to CT as stand-alone modalities has also been suggested.36,37 The concomitant application of standing flexion-extension films in combination with supine MRI evaluation as a predictor of instability is further demonstrated in the study by Lee et al.38
As the tools of artificial intelligence (AI) and machine learning continue to rapidly evolve, imaging analysis and disease detection with imaging hold great promise in the comprehensive evaluation of patients with LSS. A recent study suggested that a deep learning model detected central canal and lateral recess stenosis at a rate comparable to subspecialist radiology evaluation.39 This technique did have slightly lower detection agreement for foraminal stenosis. This study and others like it suggest that we are nearing an inflection point that may revolutionize the clinical imaging evaluation process. It may be possible to consider the axial/sagittal planes simultaneously across several modalities to determine the true presence of clinically meaningful stenosis.10
Consensus Point 1: The diagnosis of LSS with neurogenic claudication should be made based on a combination of imaging and history. Grade A; Level of certainty high; Level of evidence I-A
Consensus Point 2: MRI and/or CT evaluation in the axial and sagittal planes should be evaluated to enhance detection of lateral recess and central canal stenosis. Grade A; Level of certainty moderate; Level of evidence 1-A
Consensus Point 3: Upright hyperlordotic positioning may have a higher detection yield vs conventional supine MRI imaging and could be considered in select symptomatic individuals. Grade C; Level of certainty low; Level of evidence II
Consensus Point 4: Standing flexion-extension films, with care to evaluate the index level of stenosis detected on advanced imaging, are recommended for dynamic instability evaluation. Grade B; Level of certainty moderate; Level of evidence 1-C
Differential Diagnosis
Peripheral Neuropathies
One of the most challenging aspects of determining the appropriate treatment for patients with pain is accurately diagnosing the patient’s pain etiology. In the setting of lumbar stenosis, a patient with pain in the distal “stocking” distribution or with a mononeuropathy presentation can present a conundrum for even seasoned physicians. Thus, physicians must have a thorough understanding of the similarities and differences of peripheral neuropathies and NC and/or lumbar radiculopathies.
Peripheral neuropathy is exceedingly common, with about 8% of adults over age 55 being affected.40,41 Clinical history alone is not enough to screen for peripheral neuropathy, and pain physicians should consider physical examination techniques such as monofilament testing, vibration testing with a tuning fork, light tough for sensory disturbances (both pinprick and soft), and evaluation of deep tendon reflexes.42 A length-dependent presentation of peripheral neuropathy is the most common;43 this is the so-called “stocking and glove” distribution.
One of the most important differentiating factors with peripheral neuropathy vs intermittent NC in the setting of lumbar stenosis is how the pain manifests. Peripheral neuropathy is often painful at rest and can cause problems for patients at night when they are trying to sleep. As described, with intermittent NC, the symptoms are typically markedly reduced when seated, improved with bending forward, and worsened with ambulation.44
Another clue in the patient’s history that helps to differentiate NC symptoms from neuropathy is the involvement of the proximal limbs–a change from the length-dependent nature of peripheral neuropathies. In addition, diagnostic testing like EMG and nerve conduction studies (NCS) can help differentiate very similar clinical pictures, such as S1 radiculopathy compared to peripheral neuropathy.45
Neurogenic Claudication
Claudication refers to intermittent pain in the lower extremities that is exacerbated by activity and relieved with rest. Neurogenic claudication must be differentiated from other mimickers, most significantly VC. NC is a pain syndrome whose etiology is LSS, which is a reduction in the cross-sectional area of the lumbar spinal canal. The symptoms of NC are thought to arise from a combination of mechanical compression and circulatory dysfunction within the cauda equina nerve roots. In addition to pain, patients with NC may complain of leg heaviness, numbness, tingling, and weakness. The pain from NC is classically worsened by lumbar extension and alleviated with lumbar flexion.45 The improvement in pain and facilitating of ambulation with forward flexion is sometimes called the positive shopping cart sign. The diagnosis of NC is made from the history and involves pain in the low back, buttocks, thighs, and/or legs that develops with prolonged standing and walking and is relieved when the patient sits down. The symptoms of NC are generally bilateral.
CT and MRI images of LSS have been shown to sometimes correlate poorly with lower extremity symptoms, and therefore, the history and examination remain important.46 A study of the reliability of differentiating NC from VC based on symptomatology has shown that the most sensitive symptom (sensitivity 0.97) to rule out NC was the absence of “triggering of pain with standing alone.”47 This same study found that there was a strong likelihood of NC if patients showed a constellation of positive “shopping cart sign,” symptoms above the knees, symptoms triggered with standing alone and symptoms relieved with sitting. Patients with symptoms in the calf relieved with standing alone had a strong likelihood of VC.
There is no gold standard diagnostic tool for NC and patients with radiographically severe LSS may be asymptomatic.3 In some settings, the diagnosis of NC is supported by a positive response to intralaminar lumbar epidural injection with steroid and local anesthetic or with local anesthetic alone. The published evidence has shown that such epidural injections provide both short- and long-term relief for patients with NC and can improve gait function.48 Thus, it is the opinion of the authors that a response to such injections can be helpful in making a diagnosis of NC.
Vascular Claudication
Vascular claudication is a disease of supply vs demand as it relates to oxygen consumption during muscular activity;49 VC is a resistance imbalance as blood is delivered to the extremities during activity that creates an oxygen delivery deficit. Patients who suffer from VC describe symptoms that worsen after walking a distance and resolve when at rest and sitting. Identification of risk factors associated with peripheral atherosclerotic disease include, but are not limited to, tobacco use history, diabetes mellitus, hyperlipidemia, hypertension and strong family history.49 A distinguishing feature of VC is that truncal position, such as forward flexion, has no impact on pain relief in the lower extremities, whereas posture and truncal position (forward flexion) does alleviate the symptoms of NC. Relief from exercise-induced symptoms of VC appears to be within 1 to 2 minutes as opposed to relief from NC that may take more than 10 minutes. A diagnostic quandary exists for those patients with mild-to-moderate spinal stenosis and a history of claudication complaints. Clinicians should maintain a high index of clinical suspicion for peripheral arterial disease (PAD) in the presence of MRI evidence of mild-to-moderate lumbar disc disease and associated mild-to-moderate stenosis through the proper use of validated screening tools.50 Furthermore, some patients may temporarily relieve the lower extremity pain from PAD by hanging the affected extremity off the side of a bed.
Early detection of risk factors and formal diagnosis of PAD or deep venous thrombosis (DVT) is paramount to early interventions and recovery. Life-threatening outcomes may exist when lumbar decompression operations are pursued in lieu of ruling out vascular conditions.51 Whether DVT prophylaxis or early limb ischemia are misdiagnosed, elevated morbidity and mortality risk is present either through pursuant chronic limb-threatening ischemia (CLTI) or life-threatening pulmonary embolism. Bedside diagnostic testing early is of paramount importance, and this includes the use of skin perfusion pressure, toe pressures, transcutaneous oxygen pressures, and more advanced measures such as ankle-brachial index and exercise arteriograms. While there is no gold standard for the treatment of PAD, less invasive options such as cilostazol, lifestyle changes and exercise headline early conservative measures, with surgical revascularization or amputation as more aggressive measures.51
Lumbar Radiculopathies
Radiculopathy is related to inflammation or compression of a nerve root with treatment focused on reducing edema and/or inflammation.52,53 Lumbosacral radiculopathy has a constellation of symptoms secondary to mechanical and/or inflammatory involvement of at least one of the lumbosacral nerve roots.54 These symptoms include radiating pain, numbness, tingling, weakness and possible gait abnormalities of the lower extremities in a particular dermatome or myotome, depending on the nerve root(s) affected.55
The incidence of radicular symptoms in patients presenting with low back pain ranges from 12% to 40%.54 Any process that causes irritation or compression of the spinal nerves can cause radicular symptoms, with the most common etiology being degenerative changes of the spine, followed by trauma and benign or malignant tumors. Evaluation of a patient with radiculopathy starts with a history and physical examination with incorporation of the straight leg test or Lasègue test. A positive test with reproduction of the patient’s symptoms during passive movement between 30 and 60 degrees is suggestive of L4 to S1 nerve root involvement. A reverse straight leg test or Ely test will stretch the femoral nerve, with a positive result indicating involvement of the L2 to L4 nerve roots. In cases of radiculopathy symptoms that fail to resolve within 1 to 2 months, MRI is considered the gold standard in evaluation. For patients unable to undergo an MRI, CT scan is an acceptable alternative. In those patients where it is difficult to clinically distinguish lumbosacral radiculopathy from peripheral neuropathy or plexopathy, EMG and NC studies can be utilized to localize a lesion with relatively high diagnostic specificity.56
Treatment varies depending on the etiology and severity of symptoms, but usually begins with conservative management of symptoms. Oral medications including nonsteroidal anti-inflammatory drugs (NSAIDS), acetaminophen, and neuropathic agents, such as gabapentin and pregabalin, are often used first to treat radicular symptoms, and in severe cases opiates may be used sparingly. Nonpharmacologic interventions, including physical therapy, acupuncture, chiropractic manipulation and traction are often utilized in conjunction with oral medications to treat lumbosacral radiculopathy. Of note, the data supporting the use of these conservative treatment modalities is equivocal.54 After failure of conservative treatment modalities, interventional techniques, including ESIs and percutaneous disc decompression, are also commonly used. In refractory cases, where patients fail conservative interventional techniques, surgical decompression and spinal fusion may be needed.57
Consensus Point 5: The differential diagnosis of symptomatic LSS may include a variety of pathologies, and accurate diagnosis and dynamic stability assessment are essential for long-term treatment benefit. Grade A; Level of certainty high; Level of evidence II; Consensus strong
Percutaneous Image-Guided Lumbar Decompression (PILD)
Percutaneous image-guided lumbar decompression, as defined by the Centers for Medicare and Medicaid Services (CMS), involves minimally invasive techniques using instrumentation and image guidance to debulk the posterior elements of the spine (lamina and LF).58 PILD is an efficient, low risk, minimally invasive lumbar decompression procedure that removes a common cause of central stenosis to significantly improve mobility and reduce pain.59 Patients who are candidates for PILD have hypertrophied ligamentum flavum (HLF) of 2.5 mm or greater within the lumbar spinal canal, contributing to 50% to 85% central canal narrowing.60 This outpatient posterior lumbar procedure is designed to debulk a HLF, with the aim of alleviating NC in the presence of central canal narrowing. PILD was developed in 2005 as an alternative for cancer patients considered too high risk for open surgical decompression, and has evolved to label indications for direct decompression at spinal levels L1-S1 for symptomatic LSS with two level 1 RCTs,61,62 several level II prospective controlled studies,63–66 and a 5-year retrospective longitudinal observational durability study demonstrating statistically significant improvement in pain and mobility.67
The technique is performed percutaneously via a 5.1 mm port specifically designed for minimally invasive instruments used to debulk lamina and small portions of ligament. The patient is placed in a prone position with positioning aids to reduce lumbar lordosis and help gain access to the treatment levels. The technique has evolved from routine use of an epidurogram to define the anterior border of the LF to the use of bony anatomy, with support from a large single-center retrospective study.68 In a contralateral oblique fluoroscopic view, a bone rongeur is used to perform selective laminotomies of superior and inferior lamina to gain access to the interlaminar space. This is followed by a tissue sculptor via the same trochar to debulk sections of the LF. When there is no longer material to debulk and the instrument falls into the space created by the decompression of lamina and ligament, then the procedure is complete. This procedure can be performed unilaterally or bilaterally, and at multiple symptomatic levels through a single midline stab incision, and requires no general anesthesia, large incision, extensive surgical dissection, or surgical implants. The risk profile is identical to that of an epidural injection.
Indications
Lumbar spinal stenosis that is degenerative in nature can be caused from thickening of the LF, disc disease, osteoarthritic facet hypertrophy or a combination of all three.69 This pathology leads to the development of NC. PILD, by definition, treats LSS secondary to LFH with ligamentum thickness of ≥2.5 mm on MRI evaluation.70 While disc disease and facet hypertrophy can also contribute to LSS, PILD is not designed to address these pathologies; however, in clinical settings the reduction in spinal canal pressure from debulking the ligament has been shown to treat these multifactorial etiologies. The primary indication for PILD is central stenosis due to HLF and NC symptoms as a presenting complaint. Candidates for PILD must meet the following criteria:70
- Symptomatic LSS with the presence of NC
- Confirmation of stenosis on imaging
- Ligamentum flavum hypertrophy (LF greater than or equal to 2.5 mm).
Contraindications
Patients who have had prior instrumented spine surgery at the index level of treatment or disruption of the lamina are not candidates for PILD. These patients do not usually have lamina or ligament that can be debulked. Even though prior surgery at the level of treatment is a contraindication for PILD, there can be significant stenosis with LFH above or below the level of surgery. So PILD can be performed above or below the level of surgery if there is significant stenosis with LFH. Any localized infection at the site of the treatment area is an absolute contraindication. However, after infection has cleared the procedure can be performed. PILD is indicated for patients with less than a grade 2 spondylolisthesis. Anything greater than a grade 2 spondylolisthesis is a relative contraindication. Furthermore, patients with any coagulopathies should be evaluated for risk and benefit because of the increased risk of bleeding. Finally, the presence of a systemic infection is a relative contraindication and any systemic infection should be adequately treated before proceeding with the procedure.
Absolute contraindications for the procedure include:70
- Prior spine surgery at the index level of treatment.
- Presence of localized infection at the site of the procedure.
Relative contraindications include:70
- Presence of a higher than grade 2 spondylolisthesis.
- Presence of a bleeding diathesis/coagulation disorder.
- Presence of systemic infection.
Literature Review
To date there have been two level 1 RCTs, five prospective studies, two meta-analyses, four retrospective studies and three case series published, all demonstrating efficacy of PILD in decreasing the symptoms of NC with significant improvements in physical functionality, with an unparalleled safety profile.71
The first RCT involving PILD, conducted by Brown in 2012, was a double-blinded study with 38 subjects randomized to either PILD or lumbar epidural steroid injection (LESI) and followed for 12 weeks.61 Primary outcome measures were the Oswestry Disability Index (ODI), ZCQ, and VAS showing higher patient satisfaction with PILD vs LESI and sustained improvement for PILD throughout the 12-week duration of the study. This was the first RCT to show that the PILD procedure was more effective than ESI in providing symptomatic relief for patients with LSS.61
More recently, the level 1 ENCORE RCT involving over 300 patients randomized to PILD or ESI showed PILD to be statistically and significantly superior to ESI in the treatment of patients with NC central stenosis due to LFH at 1- and 2-year follow-up.62 Most patients enrolled in this study did have comorbid foraminal stenosis, facet hypertrophy, and/or disc bulging, which were found to be positive predictors of success with percutaneous decompression.6 There were no serious device- or procedure-related adverse events and there was no difference in safety between PILD and ESI, thereby providing level I evidence that PILD is as safe as ESI.62
Prior to these RCTs, an earlier prospective study by Deer and Kapural first described the technique of PILD and evaluated the safety of the procedure.63 This prospective study from 2010 involved 90 subjects and found the procedure to be a safe treatment option for patients with complication rates lower than those reported for minimally invasive LSS surgery. This was quickly followed by a second prospective study by Chopko and Caraway demonstrating clinical improvement in LSS patients as measured by the VAS, ODI, ZCQ and 12-item short form health survey (SF-12).64 The study included 78 subjects who were enrolled to undergo PILD, with statistically significant improvement across all outcome measures at 6 weeks. Also, in 2010, a two-site retrospective evaluation by Lingreen and Grider looked at 42 consecutive patients with significant improvement in VAS scores at 6 weeks and reduction by 40% to 86%.72 There was significant patient satisfaction with this procedure and patients felt that PILD was a viable option for the treatment of LSS prior to considering open surgical decompression.
Between 2011 and 2013 there were several studies that continued to demonstrate the safety and efficacy of PILD, including a prospective single-site study by Chopko with 14 subjects followed for 23 weeks that demonstrated 53% improvement in pain scores.65 This was followed shortly by a case series by Wong, who followed 17 patients over 1 year and demonstrated significant improvements in VAS and ODI similar to those in previous studies.73 Mekhail et al similarly followed 58 patients at 11 clinical sites retrospectively for 1 year and demonstrated significant improvements in VAS, ODI, ZCQ and SF-12 scores.74 Finally, Basu studied 27 subjects in a prospective study evaluating ODI, VAS, and ZCQ scores and reported similar results with improved scores and improved patient satisfaction.66 Therefore, as demonstrated by the numerous studies from level 1 RCTs to case studies, there is significant efficacy with PILD with respect to symptoms of NC and improvement in functionality, and a safety profile comparable to ESI.
A recent retrospective follow-up of the study by Mekhail et al analysed 75 patients treated at the Cleveland Clinic 5 years after their minimally invasive decompression procedure. Nine subjects had progressed to require open decompression. The study further evaluated opioid use and pain relief, finding that the initial results reported were durable throughout the 5-year period.67
Preliminary results of a prospective RCT comparing PILD to conventional medical management (CMM) for patients with LSS were recently released;75 CMM consisted of measures commonly prescribed for LSS, such as physical therapy, pain medications, ESI, facet joint blocks and ablations, back braces, walking aids and chiropractic care. At 6 months follow-up, PILD combined with CMM was superior statistically to CMM alone, with no adverse events reported in 181 patients.75
As the PILD therapy evolves so too have studies evolved from proof of efficacy to other subjects, such as patient selection or technical advances, which naturally arise as a therapy gains broader acceptance. With regard to patient selection and PILD, a recent study determined that subjects respond to PILD regardless of age.76 This manuscript describes the pooled statistical analysis from four high-quality studies selected from the 149 available studies evaluating PILD. There was no correlation between age and responsiveness to PILD as measured by VAS, ODI, standing time or walking distance.
A recent technical manuscript asked the question: “Is the epidurogram critical to safety of the procedure?”68 This question is particularly germane since, on occasion, the spinal degradation present in a patient does not lend itself to placing an epidural needle in the suggested cephalad-central position of the interlaminar space. On occasion, epidural access at the worst levels of spinal stenosis may be difficult to achieve at all. Pope et al address the issue of necessity and safety in this retrospective review of 147 subjects. There were no adverse events noted despite absence of a contrast layer in the epidural space at the operative site. This finding allows the experienced practitioner to proceed with some degree of confidence to continue the procedure despite difficulty or inability to obtain a working epidurogram.68
Consensus Point 6: PILD should be considered for the treatment of mild-to-moderate LSS in the presence of NC, with less than or equal to a grade 2 spondylolisthesis, and with a contribution of spinal narrowing with at least 2.5 mm of LFH. Grade A; Level of certainty high; Level of evidence 1-A
Interspinous Spacers
Designed as an alternative to lumbar fusion and/or decompression, interspinous spacers were developed to provide a less invasive surgical treatment for LSS with intermittent NC.77 These devices do not alter the bony anatomy of the spinal column, yet via indirect methods they can both stabilize and decompress the local anatomy and offer treatment for lumbar stenosis. As the name suggests, interspinous spacers are positioned between the spinous processes. This reduces lumbar extension at treated levels, but allows preserved lateral and rotational movement.78 By fixing the stenotic segment in a slightly flexed position, the interspinous spacer decreases the symptoms of NC. The first of these devices was given US Food and Drug Administration (FDA) approval in 2005.79 Since that time, several similar devices have been developed sharing the common goal of distracting the lumbar spinous processes to provide improved function for patients with symptomatic spinal stenosis who experience relief in the flexed position. Interspinous spacers can be used alone or in conjunction with a decompressive surgical procedure. One of the greatest benefits of this technology is that an interspinous spacer has a lower rate of complications compared to lumbar decompression or fusion for treatment of spinal stenosis.79 In addition, spacers can provide a more cost-effective treatment option for patients with symptomatic lumbar stenosis.80 Additionally, these devices can be placed using local anesthesia with sedation in an outpatient setting.
Indications
Interspinous spacers are approved by the FDA to treat skeletally mature patients suffering from pain, numbness, and/or cramping in the legs (intermittent NC) secondary to a diagnosis of moderate degenerative LSS, with or without grade 1 spondylolisthesis. Spinal stenosis is confirmed by x-ray, MRI and/or CT evidence of thickened LF, narrowed lateral recess, and/or central canal or foraminal narrowing. Interspinous spacers are indicated for patients with impaired physical function who experience relief of their symptoms in flexion. These patients must have undergone at least 6 months of nonoperative treatment.81 Spacers are approved for one or two adjacent lumbar levels from L1 to L5.82
Clear indications exist for the therapy and are supported by the literature. Identifying correct patients for the therapy is paramount to its success and to ensuring positive patient outcomes. Moderate degenerative LSS is defined in the literature as follows:
AND associated with the following clinical signs:
Contraindications
Contraindications to these devices are often rooted in the degree of pathology. If a patient has more than two levels of moderate stenosis, or severe stenosis at even one level, these devices should not be considered for treatment. In addition, advanced osteoporosis may present problems as the strength of the spinous processes may be compromised, putting the patient at risk for fracture at the location of the spacer. These devices are not able to be placed at levels that have been previously decompressed due to changes in anatomy at those levels.
According to the summary of safety and effectiveness data, one interspinous spacer has the following contraindications:83
• An allergy to titanium or titanium alloy;
• Spinal anatomy or disease that would prevent implantation of the device or cause the device to be unstable in situ, such as:
- Instability of the lumbar spine, e.g., isthmic spondylolisthesis or degenerative spondylolisthesis greater than grade 1 (on a scale of 1 to 4);
- An ankylosed segment at the affected level(s);
- Fracture of the spinous process, pars interarticularis, or laminae (unilateral or bilateral);
- Scoliosis (Cobb angle >10 degrees);
• Cauda equina syndrome defined as neural compression causing neurogenic bladder or bowel dysfunction;
• Diagnosis of severe osteoporosis, defined as bone mineral density (from DEXA scan or equivalent method) in the spine or hip that is more than 2.5 SD below the mean of adult normals;
• Active systemic infection, or infection localized to the site of implantation;
• Prior fusion or decompression procedure at the index level;
• Morbid obesity defined as a body mass index (BMI) greater than 40.
Literature Review/Grading of Evidence
The use of interspinous spacers for the treatment of LSS has become a very important area for scientific and clinical exploration. A PubMed search using lumbar stenosis and interspinous spacer as keywords yielded 109 results, most of which were commentaries and reviews. The authors selected systematic reviews, meta-analyses, RCTs, and real-world studies to create our recommendations for the use of interspinous spacers in the treatment of LSS.
In 2014, Wu et al published a systematic review and meta-analysis on dynamic interspinous spacers comparatively evaluated against traditional decompressive surgery.84 Analysis showed no difference between the interspinous spacers and decompression for low back pain (WMD: 1.2; 95% CI: −10.12, 12.53; P = 0.03; I2 = 66%), leg pain (WMD: 7.12; 95% CI: −3.88, 18.12; P = 0.02; I2 = 70%), ODI (WMD: 6.88; 95% CI: −14.92, 28.68; P = 0.03; I2 = 79%), Roland Disability Questionnaire (WMD: −1.30, 95% CI: −3.07, 0.47; P = 0.00; I2 = 0%), or complications (RR: 1.39; 95% CI: 0.61, 3.14; P = 0.23; I2 = 28%). However, the decompression cohort had a significantly lower incidence of reoperation (RR: 3.34; 95% CI: 1.77, 6.31; P = 0.60; I2 = 0%).84 The authors concluded that though no statistically significant differences were found in the percutaneous vs open surgery cohort, there is a greater cost for performing the intraspinous spacer technique vs open decompression for patients who have LSS. In 2016, Phan et al confirmed the earlier findings in another systematic review and meta-analysis using similar criteria.85 However, in 2019, Cairns et al performed an EMBASE and PubMed search to conclude that interspinous spacers were more cost effective compared to conservative medical management.86
Patel et al performed a multicenter RCT evaluating 391 patients who were treated with two different interspinous spacers for moderate LSS after failure of 6 months of CMM.87 Leg pain improved by 77%, and back pain improved by 68% at 2-year follow-up. ODI improved to study success parameters (minimum 15% improvement) in 65% of patients. The authors concluded that both devices achieved clinical success and one was not inferior to the other.87
In 2017, Nunley et al published 5-year retrospective data on patients implanted with an interspinous spacer and reported that 84% of patients demonstrated clinical improvement in the ZCQ; improvement in leg and back pain was seen in 80% of patients, and the success rate for the ODI was 65%.88 Furthermore, 75% of patients implanted with interspinous spacers did not require reoperation at the index level at 5 years.
In conclusion, there are many studies in the literature supporting the use of interspinous spacers for pain relief, improved mobility, and decreased opiate utilization.84–89 However, most of the studies are retrospective, albeit some have protracted follow-up of 5 years. There is a void of prospective RCTs comparing the efficacy of interspinous spacers to CMM or open surgery.
Consensus Point 7: Interspinous spacers should be considered for treatment of symptomatic spinal stenosis at the index level with mild-to-moderate spinal stenosis, with less than or equal to grade 1 spondylolistheses, in the absence of dynamic instability or micro-instability represented as fluid in the facets on advanced imaging. Grade A; Level of certainty high; Quality of Evidence 1-A
Interspinous Fusion
Introduction
Degenerative LSS is commonly of a multifactorial etiology, with contributions of varying degrees, from HLF, osteophytes, facet joint hypertrophy and degeneration of the disc space.90 This is often seen in conjunction with LSS, whether secondary to these degenerative factors or from congenital spinal stenosis.91 This cascade of degenerative changes and stenosis is largely the result of aging, with contributions from the aforementioned factors.
Several treatment options exist for those with spinal stenosis, as well as degenerative changes, ranging from conservative measures to surgical treatments. Conservative measures, or nonsurgical treatments generally include physical therapy, medications, and ESIs.92 These are generally reserved for those with mild or moderate symptoms but can also be performed for patients who demonstrate further disease progression. Open laminectomy or decompression of the neural structures, with or without transpedicular screw fixation, has been the most frequently used treatment for patients who fail conservative measures.93 However, spinal surgery may not be appropriate for all patients and has several drawbacks, including extended recovery periods from extensive muscle dissection and chronic back pain associated with postlaminectomy syndrome and persistent spinal pain syndrome. In addition, spinal surgery may be associated with adverse events such as cerebrospinal fluid leak, nerve injury, deep wound infections, misplaced hardware, and hardware failures.94,95 It is also well known that posterior lateral fusion is associated with altered spinal dynamics, which can lead to adjacent segment disease and degeneration.96 These drawbacks and limitations with more invasive open spinal procedures may limit the patients who can benefit, especially for those with medical comorbidities who may be deemed poor surgical candidates. Other patients are not considered candidates for an open surgical procedure because they may have mild or moderate findings on imaging or less severe symptoms. Hence, there is a group of patients suited to benefit from minimally invasive options with reduced procedural risks.
Definitions, Indications, and Contraindications
Indirect decompression with the use of interspinous process spacers (IPS) has shown positive outcomes and a favorable risk profile in the treatment of LSS. These devices are designed for use in patients with stenosis who display symptoms of NC that is relieved in spinal flexion as a means of limiting spinal extension.88 However, IPS use is limited in patients with flexion-associated pseudoclaudication who oftentimes also have findings of degenerative changes, spondylolisthesis, and multiple pain generators such as disc degeneration and facet joint hypertrophy, none of which are treated by indirect decompression. This has led to the development of minimally invasive devices for interspinous fixation (ISF) that can address both stenosis and degeneration. An ISF device stabilizes adjacent spinous processes, decompresses neural structures by blocking extension, and minimizes overload on adjacent spinal levels. Compared with open surgical decompression with or without fusion, ISF has the potential to offer a lower morbidity option to patients while addressing the same findings that would be treated during open spinal surgery.
Biomechanically, ISF gives immediate flexion-extension balance and provides effective stabilization for arthrodesis while preserving motion.97,98 ISF is a viable minimally invasive treatment option for those patients not suited for pedicle screw fixation or needing consideration earlier in the treatment algorithm. ISF can be used in combination with anterior column instrumentation, and in this setting, ISF augmenting anterior interbody placement has several advantages over pedicle screw fixation in terms of skin incisions, invasiveness, muscle dissection, operative times, perioperative outcomes, and favorable efficacy in reference to VAS and ODI in 1-year follow-ups,99 with preservation of the posterior elements, minimizing adjacent level disease. This has also held true in an elderly cohort demonstrating significant improvement in VAS with reliable fusion rates.100
Despite these findings, it has been unclear whether improvement would be obtained without anterior interbody fusion, that is, with ISF being used as a stand-alone device. The use of an IPS without fusion has proved efficacious and safe, and capable of maintaining sagittal alignment biomechanically within a cohort of those with LSS.88,101 However, an IPS did not directly address the degenerative process commonly found in those patients, as well as those unable to be treated with an IPS alone. Postacchini et al demonstrated in a prospective study that a stand-alone ISF combined with minimally invasive decompression in stenotic patients showing degenerative spondylolisthesis provided fusion in most patients.102 More importantly, at the 2-year follow-up patients had a highly significant improvement in all outcome measures, indicating a satisfactory clinical result, and none developed instability.
Several devices on the market have been in the surgeon’s treatment paradigm for use as ISF devices. These devices vary in their application and patient selection. They may be used with or without a decompression, as well as with or without anterior spinal fusion. The use of bone graft material is a defining factor in the labeling of ISF.
Literature Review
A PubMed literature search was performed that included the keywords lumbar stenosis and interspinous fusion. This yielded 127 results; all were reviewed and the most applicable studies for this manuscript included for assessment and grading.
The aforementioned 2016 Postacchini et al study evaluated 25 patients with degenerative lumbar stenosis and degenerative listhesis.102 Patients either underwent bilateral laminotomy or unilateral laminotomy with ISF and the two groups were compared. Unilateral laminotomy was performed to preserve the spinous processes and ISFs were then added to the procedure for fusion and to potentially mitigate postoperative worsening of the listhesis. Fusion occurred in 21/25 patients. Mean follow-up time was 34.4 months. The investigators reported a mean ODI decrease of 52%. The mean SF–36 bodily pain and physical function scores increased by 53% and 50%, respectively.
In 2020, Chin et al published a retrospective case series of 122 cases of lumbar decompression with interspinous fixation using a novel device.103 Two-year VAS and ODI showed improvement from 8.1±1.2 to 1.5±1.1 and 42.9±14.3 to 14.8±5.1, respectively.
Cuellar et al performed a prospective multicenter study evaluating interlaminar lumbar instrumented fusion, which is a subtype of ISF.104 Thirty-seven patients with single level degenerative lumbar stenosis were treated with lumbar decompression using a laminoplasty procedure followed by insertion of an allograft bone block and interspinous stabilization/fixation device. Follow-up was up to 24 months; 33 patients met the endpoint criteria (ODI and ZCQ) at 2 years. Sixty-seven percent of subjects had a 2 cm improvement on VAS and 94% of patients were off all narcotics and reported satisfaction with the procedure.
In 2011, Li et al reported on 18 patients who were treated with spinal fusion and dynamic interspinous fixation with a novel system.105 At 12 months, follow-up leg VAS, back VAS, and ODI functional scores were significantly improved over the preoperative baseline [back VAS: 1.50 ± 0.90 vs 7.20 ± 0.90; leg VAS: 1.10 ± 0.80 vs 5.20 ± 0.90; ODI functional score: (15.90 ± 5.80)% vs (52.50 ± 5.90)%]. The authors concluded that stabilization/fusion with this system provided improvement of pain and function. However, the authors also indicated that there was insufficient evidence in this study to conclude that this treatment is better than traditional fusion at the time the manuscript was published.
While not discriminating between fusion and nonfusion devices, a 2017 systematic review by Li et al assessing ISP devices concluded that there was a significant improvement in function and pain scores.106 Furthermore, the review suggested that interspinous device implantation is more effective than other conservative methods, but not superior to laminectomy in treating NC.
A multicenter RCT with 122 patients compared ISF with decompression to decompression alone.103 Two-year follow-up was performed for patients with moderate-to-severe spinal stenosis. The primary endpoint included a composite of four measures: ODI, secondary surgery or injections, neurological status, and adverse events related to the procedure or device. The primary endpoint was superior for the ISF with decompression group. Patients in the decompression-alone group were more likely to undergo a secondary intervention or injections. Another multicenter, RCT compared ISF with decompression to decompression with pedicle screw fusion.104 Subjects with moderate-to-severe lumbar stenosis were included and followed for 5 years. Composite endpoints included ODI, repeat surgery, further lumbar injections, or adverse events. When comparing both groups, the ISF with decompression group had 50.3% of the patients meeting all four endpoints, while only 44% did so in the pedicle screw fusion group. The two groups were similar in reoperation rates, as well as improvement in ODI and VAS. This further demonstrates the utility of ISF.
More recently, a retrospective review of safety and efficacy of ISF using a novel device was performed by Falowski et al, who studied 32 patients.107 The consecutive patient case series demonstrated the experience of four implanting interventional pain physicians who performed minimally invasive ISF in an outpatient ambulatory surgical center (ASC) for patients demonstrating low back pain and NC symptoms with imaging findings consistent with moderate-severe degenerative LSS at one or two levels. This was a retrospective review noting a significant reduction in VAS from 8.1 to 2.65 at 3-month follow-up, indicating a 67% reduction in overall pain. Furthermore, the safety review noted no significant adverse effects at 90 days and no reoperations or revisions.
Conclusion
There were no prospective RCTs evaluating the efficacy of ISF alone during the development of this manuscript. Some moderate-to-large scale retrospective reviews evaluated the efficacy of interspinous spacers with lumbar decompression;106,107 however, evidence supporting the use of ISF as a stand-alone procedure to benefit patients with lumbar stenosis remains limited. A multicenter single-arm prospective study is currently enrolling patients with degenerative disc disease in the presence of NC and spinal stenosis. The modest literature demonstrating lower intraoperative risk compared to other fusion techniques suggests that ISF devices should be considered in the treatment paradigm for LSS, especially in patients with significant medical comorbidities. Given that studies evaluating ISF alone are limited to retrospective work, the grading is commensurate with evidence while acknowledging that ISF in combination with other surgical interventions has shown promise.
Consensus Point 8: The MIST recommends consideration of ISF in patients with lumbar degenerative spine disease, in the presence of degenerative disc disease, with symptomatic mild-to-moderate LSS, with or without instability, with a grade 2 spondylolisthesis or less. Grade C; Level of certainty moderate; Level of evidence I-C
Intrathecal Drug Delivery Systems
Definitions
Intrathecal drug delivery systems are approved for treatment of patients with moderate-to-severe trunk and limb pain. With the discovery of opioid receptors in the dorsal horn of the spinal cord in 1976, intrathecal administration of medication allowed for bypassing the first-pass metabolism, facilitating more efficacious treatment at lower doses.108 These devices consist of a catheter that is implanted in the intrathecal space and connected to either a fixed-rate or programmable pump reservoir implanted in the subcutaneous tissue. The reservoir is then filled with single or multiple agents and delivery is programmed by the clinician to dispense medication.109
Indications
IDDS is currently a viable option for patients who have chronic pain and have failed both pharmaceutical management and appropriate interventions.110 Similar to spinal cord stimulation, IDDS is specifically recommended for patients who are experiencing moderate-to-severe pain of the trunk and limbs after other modalities of pain treatment have failed.111 While neuromodulation has replaced IDDS in the algorithm for the treatment of many complex pain conditions, the following disease conditions are currently recognized as indications: nonsurgical axial spine pain, postlaminectomy syndrome, abdominal/pelvic pain, extremity pain, complex regional pain syndrome type I and II, thoracic neuropathic/trunk pain, cancer pain, and pain where successful treatment by systemic opioids is limited by side effects.109 While patients with chronic malignant pain have been more extensively studied, recent evidence demonstrates efficacy for patients with nonmalignant pain conditions.110 There is currently a randomized multicenter prospective study investigating noncancer-related pain comparing intrathecal therapy to CMM, including spinal stenosis treatments. The study is currently enrolling patients, with a target completion date in 2021.
Currently, the on-label medications for intrathecal therapy are morphine and ziconotide. Despite this, over 80% of the pumps managed in the United States use off-label medications. The reader is advised to review the previous Polyanalgesic Appropriateness Consensus Conference (PACC) guidance regarding off-label intrathecal medications.109
Contraindications
Absolute contraindications to the implantation of an IDDS include active systemic infection, local infection at the site of proposed implantation, anatomic barrier for catheter placement, allergy to implant materials, and untreated opioid use disorder.112 Inability to stop anticoagulation, active bleeding disorder, inability to access medical care/follow-up, and inability to safely undergo general anesthesiology are often quoted as relative contraindications. While there are many other relative contraindications quoted in the literature, a true risk/benefit analysis should be conducted by an experienced physician. Further, reliable follow-up is necessary, as the pump needs to be maintained and therapy titrated with in-person appointments.
Literature Review
Although multiple studies have examined the use of IDDS for low back pain, there have been no studies specifically examining the modality in the treatment of back and leg pain resulting from spinal stenosis in a target, homogeneous population. Given the lack of studies dedicated to LSS and IDDS alone, the consensus committee determined to make inferences from the available data. To date, there have been studies of treatment of postlaminectomy syndrome and nonsurgical back and leg pain, many of which were likely secondary to LSS. Tomycz et al performed a retrospective analysis of 11 patients who were simultaneously implanted with IDDS and spinal cord stimulators (SCS).113 While all 11 patients (100%) stated that the dual system improved their quality of life, six patients (55%) felt that their relief from the IDDS was superior to SCS.113 Hayek et al performed a retrospective analysis of 57 patients with IDDS administration of hydromorphone and bupivacaine for postlaminectomy syndrome.114 At 24 months, pain scores had decreased from 8.42 to 4.3 (P<0.001). In patients with previous fusion, adjacent level disease and spinal stenosis are common, affecting the majority with posterior fusion at some interval after surgical treatment. As intrathecal therapy is commonly employed in this population, it follows that these patients can be managed well with intrathecal therapy, although no clinical studies address this specific spinal stenosis population.
Deer et al followed 166 patients with chronic low back pain who were trialed for IDDS.115 There was a 93% success rate and 136 (82%) of those patients were implanted. At 12 months 80% of patients implanted with IDDS for low back pain were satisfied with their therapy. While many of the foundational studies using IDDS for treatment of chronic pain do not subdivide lumbar spine pathologies in a fashion that would allow further investigation of the outcomes, one relatively recent prospective observational study did suggest that a subgrouping of patients with LSS were responsive to IDDS using opioid therapy. Grider et al reported that 12 of 58 subjects enrolled in the study carried the diagnosis of LSS based upon symptomatology and imaging.116 The LSS subjects did not differ from other spinal pathologies with regard to daily intrathecal opioid requirement, suggesting similar response to LSS vs lumbar degenerative disc disease or failed back surgery syndrome. While not conclusive, this study does offer directional outcomes specifically for patients with LSS when treated with IDD.
Evidence Ranking
Consensus Point 9: The MIST recommends IDDS be used in the treatment of LSS after anatomic considerations at the index level of treatment for minimally invasive decompressive options, and can be employed when more direct methods fail or are not suitable. Grade B; Level of certainty moderate; Level of evidence I-B
Open Decompression
Open decompression for LSS involves the resection of impinging bone, ligaments, and disc materials and traditionally has referred to laminectomy, which is often combined with medial facetectomy and foraminotomy.117 Open laminectomy has been modified in numerous ways over the past years to involve open decompression via smaller incisions; however, it remains unknown if such micro-decompressions are equivalent to open laminectomy.118 Laminectomy remains the gold standard, open decompression technique against which other open decompressions, such as percutaneous, microscopic, or endoscopic, are compared. Open decompression may be better defined as direct decompression and must be differentiated from indirect decompression, which involves enlarging the spinal canal and foramina by distraction and correction of global spinal alignment without removal of compressing tissues.119 Open and direct decompression can be accompanied by fixation or instrumented fusion when there is concern of instability. Complications of open decompression include cerebral spinal fluid leak, nerve root injury, epidural hematoma, epidural fibrosis, and iatrogenic instability.
Indications
Lumbar laminectomy alone or with fusion is one of most common operations performed by spinal surgeons. The primary indication for open decompression via lumbar laminectomy or via a less invasive approach is degenerative lumbar stenosis, especially central or lateral recess stenosis when NC and/or lower extremity radiculopathy symptoms do not respond to conservative treatments including epidural injections. Other indications for open decompression outside of degenerative stenosis include primary or secondary tumors, infection, trauma, and stenosis related to deformity.120
Contraindications
Contraindications for open decompression without associated fusion include spinal instability and coagulopathy. Relative contraindications for open decompression without associated fusion include coronal deformity (scoliosis), sagittal deformity (kyphosis), and spondylolisthesis, especially grade 2 or higher.
Literature Review
An analysis of five RCTs (643 participants) comparing surgical to nonsurgical care concluded that the evidence could not support that surgery was superior to nonoperative care.90 However, this study included a mix of both open decompression surgeries as well as indirect decompression surgery with spinous process spacers. In a randomized trial of lumbar laminectomy with or without fusion compared to nonsurgical management for LSS with degenerative spondylolisthesis, Weinstein et al showed that surgically treated patients had greater pain relief and functional improvement for 4 years.121 Athiviraham and Yen reported on a nonrandomized cohort of 125 consecutive patients with lumbar stenosis followed for 2 years.122 Most patients undergoing open decompression with or without fusion reported that they were better after surgery; however, residual symptoms were common. The majority of patients who declined surgery had persistent symptoms and 12.5% reported worsening of symptoms at 2 years.122 Most of the debate has focused on whether open decompression should be augmented with fusion. The remaining RCTs have compared open decompression alone to decompression with fusion to assess safety and efficacy.
Evidence Ranking
Consensus Point 10: The MIST recommends open decompression with or without fusion when the physician feels the risk:benefit ratio is favorable, and in the setting of a rapidly progressive neurological decline. Grade A; Level of certainty high; Level of evidence 1-A
Neurostimulation
Spinal cord stimulation is the delivery of electrical impulses to the dorsal column of the spinal cord to modulate the pain signal from traveling to the brain. This is proposed to occur through several mechanisms, and it is likely that the pain-relieving effects are a combination of these mechanisms.123 The procedure is typically performed in a two-step process. The first step is a trial, in which one or two temporary stimulation leads are placed percutaneously into the epidural space during an outpatient procedure. The leads are secured to the skin and left in place for 3 to 10 days, depending on physician preference. At the conclusion of the trial, the leads are removed and the patient reports about final pain and functional improvement. In most cases, success is defined as 50% or greater pain relief along with functional improvements. If the trial is successful and the patient desires implantation, the leads and implantable pulse generator (IPG) are implanted under the skin in a separate open surgical procedure.
Indications
The SCS procedure is FDA approved to treat intractable pain of the trunk and/or limbs. In the United States, the most common indications for SCS include chronic back and leg pain after spine surgery (FBSS), complex regional pain syndrome (CRPS) types I and II (causalgia), chronic radiculopathy, and peripheral neuropathy of multiple etiologies.124 However, SCS has been described in the treatment of other refractory painful conditions, including LSS.
Contraindications
Contraindication for SCS include uncontrolled psychiatric disorder, inability to comply with therapy, active local or systemic infection, immunosuppression, and anticoagulant use that cannot be temporarily halted for the trial or implant procedures.125
Literature Review
There is a relative paucity of data regarding the use of SCS for LSS related to back and leg pain. Chandler et al reported results from a retrospective cohort of 55 patients undergoing a SCS trial for LSS and associated leg pain.126 Twenty-one patients underwent permanent implantation via mini-laminotomy with a single paddle lead, with 67% reporting continued analgesia (greater than 50% subjective relief and/or decrease in medication or improvement in function) at 1.5 years. Twelve patients had a successful trial but choose not to proceed with permanent implant. These promising results warrant further research regarding the utility of SCS for certain patients with LSS.
Costantini et al performed a retrospective case series review of 69 patients with symptomatic back and leg pains attributed to LSS, all treated with paresthesia-based SCS.69 Data were collected from three independent registries at European sites. All patients had failed conservative management, including ESIs, and had declined or were refused for surgery. The diagnosis of LSS was made based on either MRI evidence of spinal canal narrowing, a history of NC, or both. Data were collected at baseline with a median follow-up of 2 years. The majority of patients had back and radicular pain (77%) and claudication (64%). The median follow-up was 24±17.8 months (range 1 to 72 months, mean 27 months). Visual analog scale improved from baseline 7.4±2.3 to 2.8±2.4 (P<0.05). Opioid use decreased from 29% of patients to 13%, NSAIDS from 75% to 49%, antidepressants from 33% to 20%, and antiepileptics from 32% to 9% (P<0.05). Oswestry disability index was not recorded for all patients (n = 28), but decreased from 34.3±7.6 to 15.7±13.1 at follow-up in this smaller cohort (P<0.05). There were six adverse events, including five lead migrations and one infection. The authors concluded that SCS appears effective in the treatment of LSS and should be considered before surgical decompression in high-risk patients.
Similar positive results were published by Kamihara et al.70 The authors described a retrospective case series of 91 patients who underwent a paresthesia-based SCS trial for LSS-associated leg pain. A total of 59 patients reported at least 50% pain relief during the trial (64.8%), and 41 patients desired permanent placement and were implanted (45.1%). The mean follow-up was 34.5±22.5 months. The authors defined success as a “good response group” defined as “SCS continued for 1 year or more after implantation” and this result was reported in 39 of 41 patients (95.1%). The significant limitation of this study is the lack of valid pain and/or functional outcome measures, which makes it difficult to assess whether the 95.1% success rate is valid.
Rare complications of spinal cord compression after SCS placement have been reported. A patient with known lumbar radiculopathy and spinal stenosis developed lower extremity weakness and absent toe proprioception after permanent SCS lead placement at the T8 level with insertion at the L1-L2 level.127 MRI after lead removal demonstrated severe stenosis at the T12-L1 level, and the patient regained neurologic function. This case highlights the importance of monitoring for asymptomatic thoracic spinal stenosis which can co-occur with lumbar stenosis in up to 30% of patients.128
Evidence Ranking
Consensus Point 11: The MIST recommends SCS be used in the treatment of LSS after anatomic considerations at the index level of treatment for minimally invasive decompressive options, and can be employed when more direct methods fail or are not suitable. Grade B; Level of certainty moderate; Level of evidence I-C
Epidural Steroid Injections
Definitions and Literature Search
The first descriptions of epidural injections for the treatment of lumbar spine-related pain appeared in the early 1900ʹs.129 Over the ensuing 100-plus years, lumbar epidural injection therapy has evolved to the current practice of image-guided (usually fluoroscopic) interlaminar or transforaminal ESIs. Lumbar epidural steroid injections (LESI) are commonly prescribed in the treatment algorithm for LSS. In most cases, they are considered as an option if a symptomatic patient fails to improve with conservative and noninvasive therapies such as oral medications, physical therapy, and activity modification.6
Multiple systematic reviews have been published regarding the use of LESI to treat LSS.48,130–132 The majority of these systematic reviews suggest at least short- to intermediate-term symptom improvement for patients with LSS. Similarly, many prospective clinical trials have been published on this subject. Most trials have demonstrated efficacy but there is considerable variability regarding epidural technique, medication, dosage, and duration of improvement. As a result, treatment efficacy for the modality has been difficult to determine, as foundational studies in support of the procedure come from different eras representing the evolution of evidence-based medicine and evidence-based study standards.
This section will outline the evidence to date in the literature with regard to treatment effect of application of medications delivered via the single-dose epidural route in the treatment of LSS. Studies from 1980 to present were considered. PubMed, Cochrane, EMBASE and Google Scholar databases were utilized and yielded 398 potential studies (60 manuscripts reviewed) of which nine studies met inclusion criteria of RCTs with homogenous populations for LSS. When study inclusion criteria were expanded to RCTs with a predominance of LSS subjects, an additional five studies were identified. Taken together, these studies represent the basis for the evaluation and subsequent recommendations.
Indications
When pain from clinically significant LSS and NC fails to be managed with noninterventional methods of pain relief, image-guided ESIs are commonly utilized as a safe and effective method of providing diagnostic and therapeutic benefit, which can last from 1 to 6 months. The institution of ESI in the modern treatment algorithm for LSS should be considered carefully for appropriately selected patients. In addition, while advocating for an ESI as an initial form of potentially therapeutic treatment, it is prudent to set patient expectations, and also be mindful to provide further insight into future minimally invasive treatment options from which the patient may benefit long term, based on their individual diagnostic work-up.6,22,48,62,90,91,130,133–136
Indications for ESI include confirmation of diagnosis with an accurate and positive history and physical examination findings, MRI and dynamic (flexion, extension, and oblique) x-ray imaging, and possible electrodiagnostic testing, all consistent with clinically significant LSS and NC. Patients should have demonstrated failure of more conservative forms of management. While traditionally ESIs have been studied and utilized predominantly for their therapeutic benefit, with recent advances in minimally invasive spine procedures, there has also been added utility of ESIs to provide diagnostic value in assessing candidacy for more advanced procedural options.61,131,132,135,137–143
Given the robust advancement in minimally invasive spine technology and evidence-based clinical efficacy with these options for treating LSS, repetitive ESIs for patients with clinically significant NC should be reserved for those patients who have a robust clinical response and/or are not candidates for higher level interventions or surgical decompression.
Contraindications
An ESI should give at least 3 months of adequate relief between therapeutic injections, depending on the degree of pain and dysfunction, where repeated use of ESIs in this population may be appropriately considered. Although it is reasonable to repeat ESI when patients have sustained pain relief with eventual recurrence of pain, it is important to understand that some payer guidelines (including CMS58) now stipulate that patients should have obtained a minimum of 3 months of pain relief with eventual recurrence of pain before it is reasonable to proceed with additional injection therapy. For patients exhibiting shorter-term relief of less than 3 months, the clinician may wish to consider other treatment options.6,22,48,57,61,62,74,90,91,130–135,137–146
Severe and uncontrolled comorbid factors may contraindicate the use of epidural steroids, particularly with uncontrolled diabetes or cardiovascular issues negating the use of corticosteroids, as well as active spinal or systemic infections and coagulopathies or patients on anticoagulants. In these instances, ESI without the use of steroids may be considered, as well as more advanced decompressive therapies within the treatment algorithm. In a double-blinded randomized prospective multicenter trial performed in 2014 with over 400 patients who had central spinal stenosis and moderate-to-severe leg pain and disability, scores to receive epidural injections using lidocaine with and without glucocorticoids revealed that after 6 weeks there was no improvement between interlaminar vs transforaminal, nor between glucocorticoid or not, to treat spinal stenosis, in patients who received one or two injections prior to the 6-week assessment. Similarly, the outcome was likely maintained at 12 months if relief occurred, suggesting that if it was achieved, it should be identified at 6 weeks.134 If no benefit was achieved, more mechanical therapy options may be needed.
Literature Review
As discussed already, we identified randomized comparative trials of epidural steroids to treat LSS. Methodology varied widely as did outcome measures, length of follow-up, and comparators.
Transforaminal ESI vs Interlaminar ESI
Lee et al compared interlaminar LESI to transforaminal ESI using 40 mg of triamcinolone in a 99-patient randomized comparative trial without a placebo control.138 Both treatment groups had significant improvement in the Roland 5-point pain scale, with the transforaminal group showing greater overall improvement than the interlaminar group at 2 weeks, 2 months, and 4 months. Problematically with this trial, only patients with axial back pain (no leg pain or NC symptoms) were included: accordingly, the patients in this trial did not have typical lumbar stenosis symptomatology.
Sencan et al performed a randomized comparative trial of intralaminar LESI (ILESI) vs bilateral transforaminal epidural steroid injection (TFESI) for 67 patients with NC in the setting of central canal lumbar stenosis.147 Each group received either fluoroscopic guided TFESI or ILESI with 80 mg of methylprednisolone plus bupivacaine and were followed for 3 months. Both groups had significant improvement in pain (NRS) and function (ODI) at all time points. In contrast to the trial by Lee et al,138 in this trial by Sencan et al,147 the ILESI group had overall greater pain and functional improvement compared to the TFESI group at the final 3-month follow-up. There was an overall progressive increase in NRS pain scores over the 3-month period.
Epidural vs No-Injection Control Group
Koc et al performed a small randomized trial of 29 patients with LSS, comparing no active treatment (control) to physical therapy and to ESI.137 The epidural technique was fluoroscopic guided interlaminar using 60 mg of triamcinolone plus local anesthetic. Patients in both the therapy and epidural groups had significant pain and functional improvement at all time points up to the final 6-month follow-up. At short-term follow-up (2 weeks), the epidural group had greater improvement than the therapy group and the control group. Each treatment group had only 10 patients. It is notable in this trial that even the control group with no active treatment had some improvement over time.
Epidural Local Anesthetic vs Epidural Glucocorticoid
Cuckler et al performed a randomized trial comparing non-image guided interlaminar epidural procaine vs 80 mg methylprednisolone in a mixed group of patients with pain from either lumbar disc herniation or LSS.148 There was no significant difference in the patients with LSS between the two treatment groups achieving the primary outcome of “75% improvement” at short-term follow-up (24 hours) or long-term follow-up (mean approximately 20 months). At long-term follow-up 22% of the steroid group were improved vs 14% of the local anesthetic group. The mixed patient populations, the use of non-image guided injections, and the lack of a standardized outcome measure significantly limits the generalizability of this trial.
Nam and Park in a small randomized comparative trial without a placebo control group compared transforaminal epidural lidocaine vs epidural triamcinolone 20 mg in patients with lumbar scoliosis plus symptomatic LSS.143 Both groups had improvements in VAS pain scores and ODI functional improvement at all follow-up points up to the final 3-month visit. The steroid group had significantly greater improvement than the local anesthetic group. Manchikanti et al, in a series of randomized double-blind controlled trials, examined the effect of fluoroscopic guided caudal ESI and LESI for the treatment of LSS in a total of 220 patients.135 In summary, the trials demonstrated that both caudal and lumbar ESI with local anesthetic only and with steroid showed significant pain improvement, with the interlaminar technique showing overall greater improvement than the caudal approach. The primary outcome was 50% or greater improvement in pain (NRS) and disability scores (ODI). Patients were allowed repeat injections if the effects of a prior successful injection waned, and each of the caudal or lumber ESI local or steroid group patients received an average of approximately 5 to 6 injections over the course of the study period.
Friedly et al performed a 400-patient, multicenter double-blind randomized trial comparing epidural local anesthetic plus steroid injection to epidural local anesthetic injection.134 The ESI technique (transforaminal vs interlaminar) was at the discretion of the procedural physician, as was the choice of steroid and dose (betamethasone, triamcinolone, dexamethasone, or methylprednisolone). At the 6-week follow-up, both groups had significant improvement in the primary outcome of Roland-Morris Disability Questionnaire score, but there was no significant difference between the two groups. At the 3-week time point, the steroid group had significantly greater improvement compared to the local anesthetic-alone group. Patients in the steroid group reported significantly greater satisfaction on the Swiss Spinal Stenosis Questionnaire compared to the local only group (67% of patients vs 54% of patients, respectively).
Fukusaki et al performed a comparative trial of non-image guided interlaminar epidural saline vs local anesthetic, vs local anesthetic plus 40 mg of methylprednisolone in 53 patients with NC in the setting of lumbar stenosis.142 All patients received a series of three injections over the first week of the trial. At 1-week follow-up, the local anesthetic group and the steroid group had a significant increase in the primary outcome of improved walking distance; however, by 1 month and 3 months, there was no significant improvement in any of the three groups.
Finally, Wei et al performed a randomized trial of 90 patients with unilateral leg pain in the setting of low-grade mild-to-moderate LSS.149 Subjects were randomized into one of three fluoroscopic guided transforaminal epidural groups: lidocaine only, lidocaine plus 10 mg etanercept (a TNF-alpha inhibitor drug), or lidocaine plus steroid (2 mL diprospan). All three groups had significant short-term improvement in VAS and ODI at 1-month follow-up. At 3 months, there was an increase in VAS and ODI and by 6 months these measures returned to baseline in the local-only group and the local-plus-steroid group. The local plus TNF-alpha group had greater improvement than the other two groups at 1 month follow-up and that improvement in VAS and ODI was sustained at the 3- and 6-month follow-up period.
Epidural Steroid Injection vs PILD
Brown performed a small randomized double-blind prospective trial comparing LESI with 80 mg triamcinolone to minimally invasive PILD in 38 patients.61 Sixteen of 21 patients in the minimally invasive group (76.2%) experienced the primary efficacy endpoint pain improvement outcome of a 2-point or greater improvement in VAS at 6-week follow-up relative to baseline vs only 6 of 17 ESI patients (35.3%). Six-week overall mean VAS did not show any significant improvement in the ESI group.
The MiDAS ENCORE trial, a multicenter prospective RCT, compared LESI to minimally invasive percutaneous image-guided lumbar decompression in 302 patients.139 The epidural group could receive up to four injections per year of 40 to 80 mg of triamcinolone or methylprednisolone. At 6 months, 62% of the minimally invasive group achieved the primary outcome endpoint of a 10-point or greater ODI improvement vs 35.7% in the ESI group. Similarly, 56% of the minimally invasive group achieved the secondary outcome endpoint of a 2-point or greater improvement in the numerical pain rating score vs 33.3% in the ESI group.
What can we conclude from the results of these investigations? It appears that ESIs can lead to temporary symptom improvement in patients with LSS, and that epidural local anesthetic injection without steroid may have a therapeutic effect as well. Beyond that, there remain many questions. Does the degree and/or severity of the stenosis affect the response? Does the location of the stenosis (central vs foramen vs lateral recess vs combinations) affect the response? Does the duration of symptoms affect the response? Given that many patients with LSS are elderly and have other medical comorbidities, do other medical problems such as diabetes mellitus affect the response? What is the optimal steroid dose? Can the injections be repeated and, if so, how often and at what interval? These are important questions that can be addressed in future studies on this topic. Many of the trials discussed here allowed repeat injections for patients who had initial temporary improvement. This would seem like a reasonable approach for most patients. On the other hand, repeat injections for patients who experience only short-term improvement should be discouraged. It is important to note that many payers and insurance providers now have limits on the number and frequency of repeat ESIs that are covered.
On the topic of stenosis severity, two trials suggest that more severe stenosis may be associated with a poorer response. Ghahreman and Bogduk, in a subgroup analysis of a RCT of TFESI, reported that patients with low grade nerve root compression responded more favorably to ESI compared to patients with high grade compression (75% of patients responding vs 26%, respectively).150 Similarly, another trial compared outcomes of ILESI in patients with moderate vs severe LSS, and both the number of patients responding to treatment as well as the percentage of overall pain relief was lower in patients with severe stenosis.151
A persistent question among practitioners concerns whether there is, in fact, benefit to proceeding directly to a more invasive treatment and bypassing the step of ESI for LSS. While this question has not been addressed with a RCT, a recent retrospective study evaluated the results of a treatment algorithm offering PILD upon presentation with LSS symptoms and LFH in 145 subjects.150 Seventy-five subjects had zero or one ESI, whereas 79 subjects had two or more ESIs. The authors of the six-center study concluded that multiple ESIs demonstrated no benefit and suggested that moving directly to PILD upon presentation with diagnostic criteria should be considered.
Consensus Point 12: Epidural steroid injections are recommended in the algorithm for the treatment of symptomatic lumbar spinal stenosis. Grade B; Level of certainty high; Level of evidence I-A
Consensus Point 13: Epidural steroid injection may be repeated when a patient has significant temporary improvement in symptoms. Be aware that the number and frequency of injections may be limited by insurance and payer rules and regulations. Grade B; Level of certainty moderate; Level of evidence I-B
Lumbar Spinal Stenosis Treatment Algorithm: A Comparison of MIST 1.0 and MIST 2.0
The MIST 1.0 served as the first guidance in identifying patients for treatment with both direct and indirect minimally invasive techniques to decompress spinal stenosis in the absence of surgical indications, such as motor weakness, multilevel disease, and translational instability. The MIST 1.0 focused on the architecture of the spinal stenosis as a pathway to determine the treatment algorithm, and since that publication, more data have been published on the multidimensional causative features of spinal stenosis and the treatment with percutaneous direct decompression. This has shifted the MIST 2.0 algorithm (Figure 1) to a more complete determination of the presence of spondylolisthesis and micro-instability (fluid in the facet joints). For indirect decompression with interspinous spacers, the presence of micro-instability or greater than a grade 1 spondylolisthesis at the index level is prohibitive, along with previous decompression at the adjacent levels from the index level, as removal of the spinous process prevents anchoring of the device. For direct percutaneous decompressive procedures, surgery at adjacent levels from the index level allows for treatment at the index level, as does the presence of anything less than a grade 2 spondylolisthesis. Furthermore, since MIST 1.0 there are new decompressive devices that allow for fusion. One has limited data as a stand-alone device in the presence of degenerative disc disease,107 which represents a minimally invasive open approach, and the other represents a lateral percutaneous approach with no published safety or efficacy data yet. Therefore, for the purposes of this algorithm, only the posterior approach is identified. Regarding the degree of spinal stenosis, there are numerous studies that demonstrate no correlation between the severity of spinal stenosis radiographically and the clinical presentation. It should be noted that these minimally invasive options, however, are for mild-to-moderate spinal stenosis. For severe spinal stenosis, referral is recommended, and minimally invasive approaches may be considered for appropriate candidates if they are not candidates for an open technique, with or without fusion.
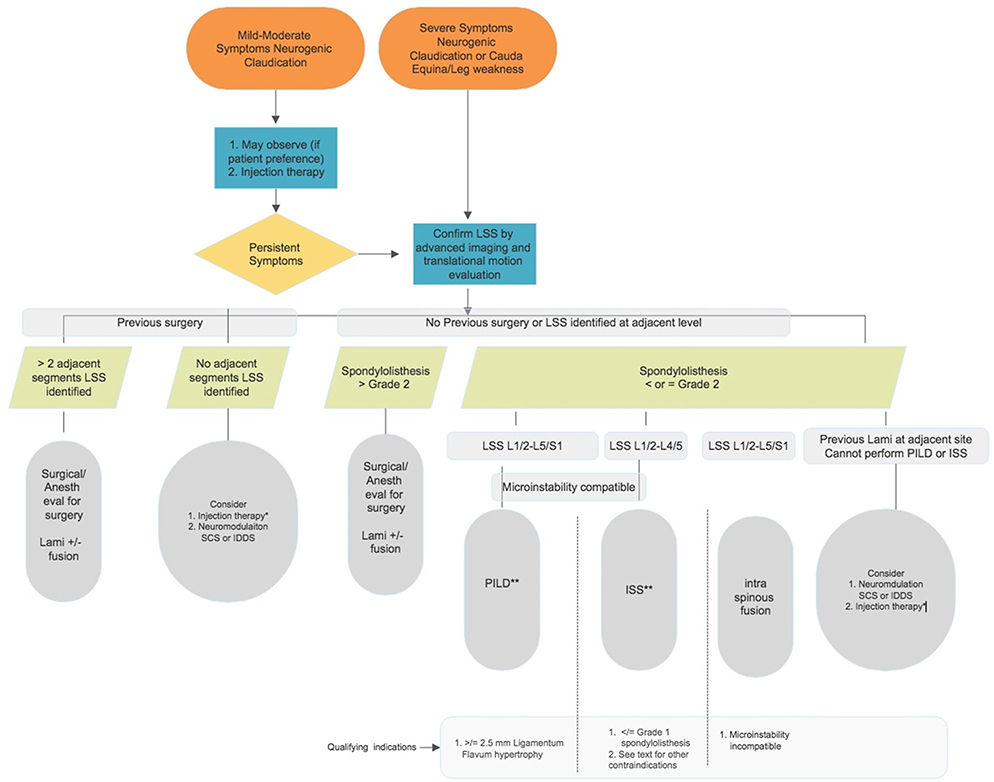 |
Figure 1 MIST 2.0 treatment algorithm. * Data would suggest up to three epidural injections within 6 weeks of initiation of treatment. **Although there are limited data on treatment of more than three spinal levels with minimally invasive spinal stenosis treatments, it is generally considered appropriate to seek a formal surgical consultation before proceeding. Special comment: Randomized controlled trial data suggest that the architecture of spinal stenosis (central, lateral recess, foraminal) was successfully treated with percutaneous direct and indirect decompressive strategies. Therefore, the distinction of stenosis architecture was removed from the MIST 1.0 original algorithm. Abbreviations: DRG, dorsal root ganglion; IDDS, intrathecal drug delivery system; ISS, interspinous spacer; LSS, lumbar spinal stenosis; PILD, percutaneous image-guided lumbar decompression; SCS, spinal cord stimulation. |
Conclusions
The treatment of LSS is evolving and new options have been brought to clinical practice in recent years that have facilitated less invasive and potentially lower risk treatments. The judicious use of both open surgery and minimally invasive pain treatments requires careful attention to evidence, and in the lack of evidence to consensus opinion of an informed group. The MIST group has examined the peer-reviewed literature and given consensus guidance to best practices. As the literature for minimally invasive procedures for LSS continues to develop and techniques such as spinal endoscopy continue to become more widely available, the MIST group intends to include them in future editions. This process is intended to create a living document and future versions of guidance will follow as additional studies are completed.
Acknowledgments
Sarah Staples, MA, ELS, assisted with manuscript preparation.
Disclosure
Dr Timothy R Deer reports personal fees, Consultant, Stock Options, Research from Vertos, personal fees, Consultant – Stock Options from Spinal Simplicity, during the conduct of the study; personal fees, Consultant, Research from Abbott, personal fees from Flowonix, personal fees, Consultant, Stock Options from SpineThera, personal fees, Consultant, Stock Options, Research from Saluda, Research from Mainstay, personal fees, Consultant, Research from Nalu, personal fees, Consultant, Stock Options from Cornerloc, personal fees, Consultant, Common Stock from Ethos, personal fees, Consultant, Stock Options, Research from SPR Therapeutic, personal fees from SI Bone, personal fees from Nevro, personal fees from Medtronic, personal fees, Consultant, Research from Boston Scientific, personal fees, Consultant, Stock Options, Research from PainTeq, personal fees from Tissue Tech, Research from Avanos, outside the submitted work. In addition, Dr Timothy R Deer has a patent Abbott pending to Abbott & Tim Deer. Dr Jason E Pope reports Consultant, Research, Advisory Board from Abbott, Consultant, Research, Advisory Board from Saluda, Consultant from Medtronic, Research from Boston Scientific, Consultant, Advisory Board from Biotronik, Consultant, Advisory Board, Stock Options from Vertos, Consultant, Equity from Spark, Consultant, Advisory Board, Research, Equity from Thermaquil, Consultant, Equity, Advisory Board from SPR Therapeutics, Advisory Board, Equity, Research from Painteq, Research, Advisory Board, Equity from Aurora Spine, Research, Consultant from Ethos, Research from AIS, Research, Consultant from Flowonix, Owner from Celeri Health, Owner from Neural Integrative Solutions, Owner from Pacific Research Institute, Consultant, Research from Mainstay, Consultant from WISE, Research from Muse, outside the submitted work. Dr Jonathan M Hagedorn reports personal fees from Boston Scientific, personal fees from Abbott, personal fees from Medtronic, personal fees from Nevro, personal fees from Saluda, outside the submitted work. Dr Steven Falowski reports grants, personal fees from Abbott, grants, personal fees from CornerLoc, grants, personal fees from Medtronic, Equity, Research from PainTeq, grants, personal fees from Aurora, personal fees from Vertos, grants, personal fees from Saluda, personal fees from SurgenTec, outside the submitted work. Dr Reda Tolba reports Consultant to Medtronic and Abbott. Dr Alex Escobar reports personal fees from Boston Scientific Vertiflex, personal fees from Vertos Medical, outside the submitted work. Dr Mark Malinowski reports personal fees, Consulting from Nalu Medical LLC, personal fees, Consulting from SI Bone, Inc., outside the submitted work. Dr Anjum Bux reports personal fees from Vertos, personal fees from Flowonix, personal fees from Boston Scientific, personal fees from AIS Healthcare, personal fees from Cornerloc, outside the submitted work. Dr Jennifer Hah reports Consultant from Nalu Medical, Consultant from SPR Therapeutics, grants from NIH NIDA, outside the submitted work. Dr Jacqueline Weisbein reports Research from Medtronic, Research and Professional Consulting Fees from Abbott, Consulting Fees, Advisory Board from Vertos, Consulting Fees from SI Bone, Advisory Board, Consulting Fees from Biotronik, Research & Consulting from Saluda, outside the submitted work. Dr Nestor D Tomycz reports Abbott consultant; SI-bone consultant. Dr Jessica Jameson reports personal fees from Abbott, personal fees from Nevro, personal fees from Saluda, personal fees from Control Rad, personal fees from Boston Scientific, personal fees from Vertos, personal fees from SI Bone, during the conduct of the study; personal fees from Abbott, personal fees from Nevro, personal fees from Saluda, personal fees from Boston Scientific, personal fees from Vertos, personal fees from SI Bone, personal fees from Control Rad, outside the submitted work. Dr Erika A Petersen reports she has received research support from Medtronic, Neuros Medical, Nevro Corp, ReNeuron, SPR, and Saluda, as well as personal fees from Abbott Neuromodulation, Medtronic Neuromodulation, Neuros Medical, Nevro, Saluda, Biotronik, and Vertos. She holds stock options from SynerFuse and neuro42. Dr Dawood Sayed reports personal fees, options from Vertos, grants from Boston Scientific, personal fees from Surgentec, options from Painteq, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Verbiest H. A radicular syndrome from developmental narrowing of the lumbar vertebral canal. J Bone Joint Surg Br. 1954;36-B(2):230–237. doi:10.1302/0301-620X.36B2.230
2. Social Security Administration. Disability evaluation under social security. Soc Secur Bull. 2010;70(3):70.
3. Kruger Jensen R, Secher Jensen T, Koes B, Hartvigsen J. Prevalance of lumbar spinal stenosis in general and clinical populations: a systematic review and meta-analysis. Eur Spine J. 2020;29(9):2143–2163. doi:10.1007/s00586-020-06339-1
4. Deyo RA, Mirza SK, Martin BI, et al. Trends, major medical complications, and charges associated with surgery for lumbar spinal stenosis in older adults. JAMA. 2010;303(13):1259–1265. doi:10.1001/jama.2010.338
5. Parker SL, Chotai S, Devin CJ, et al. Bending the cost curve—establishing value in spine surgery. Neurosurgery. 2017;80(3S):S61–69. doi:10.1093/neuros/nyw081
6. Deer TR, Grider JS, Pope JE, et al. The MIST guidelines: the lumbar spinal stenosis consensus group guidelines for minimally invasive spine treatment. Pain Pract. 2019;19(3):250–274. doi:10.1111/papr.12744
7. Institute of Medicine. Clinical Practice Guidelines We Can Trust. Washington DC: IOM; 2011.
8. Harris RP, Helfand M, Woolf SH, et al.; for the Methods Work Group, Third U.S. Preventive Services Task Force. A review of the process. Am J Prev Med. 2001;20(3):21–35. doi:10.1016/S0749-3797(01)00261-6
9. Deyo RA, Gray DT, Kreuter W, Mirza S, Martin BI. United States trends in lumbar fusion surgery for degenerative conditions. Spine. 2005;30(12):
10. Steurer J, Roner S, Gnannt R, Hodler J. Quantitative radiologic criteria for the diagnosis of lumbar spinal stenosis: a systematic literature review. BMC Musculoskelet Disord. 2011;121(1):175. doi:10.1186/1471-2474-12-175
11. Ciric I, Mikhael MA, Tarkington JA, Vick NA. The lateral recess syndrome: a variant of spinal stenosis. J Neurosurg. 1980;53(4):433–443. doi:10.3171/jns.1980.53.4.0433
12. Lee S, Lee JW, Yeom JS, et al. A practical MRI grading system for lumbar foraminal stenosis. AJR Am J Roentgenol. 2010;194(4):1095–1098. doi:10.2214/AJR.09.2772
13. Schroeder GD, Kurd MF, Vaccaro AR. Lumbar spinal stenosis: how is it classified? J Am Acad Orthop Surg. 2016;24(12):843–852. doi:10.5435/JAAOS-D-15-00034
14. Suri P, Rainville J, Kalichman L, Katz JN. Does this older adult with lower extremity pain have the clinical syndrome of lumbar spinal stenosis? JAMA. 2010;304(23):2628–2636. doi:10.1001/jama.2010.1833
15. Konno S, Kikuchi S, Tanaka Y, et al. A diagnostic support tool for lumbar spinal stenosis: a self-administered, self-reported history questionnaire. BMC Musculoskelet Disord. 2007;8(1):102. doi:10.1186/1471-2474-8-102
16. Sugioka T, Hayashino Y, Konno S, Kikuchi S, Fukuhara S. Predictive value of self-reported patient information for the identification of lumbar spinal stenosis. Fam Pract. 2008;25(4):237–244. doi:10.1093/fampra/cmn031
17. Katz JN, Dalgas M, Stucki G, et al. Degenerative lumbar spinal stenosis. Diagnostic value of the history and physical examination. Arthritis Rheum. 1995;38(9):1236–1241. doi:10.1002/art.1780380910
18. Hara N, Matsudaira K, Masuda K, et al. Psychometric assessment of the Japanese version of the Zurich Claudication Questionnaire (ZCQ): reliability and validity. PLoS One. 2016;11(7):e0160183. doi:10.1371/journal.pone.0160183
19. Marchand AA, Tétreau C, O’Shaughnessy J, et al. French-Canadian adaptation and validation of the Swiss Spinal Stenosis Questionnaire for patients with lumbar spinal stenosis. Spine. 2019;44(8):E487–E493. doi:10.1097/BRS.0000000000002896
20. Tomkins CC, Battié MC, Rogers T, et al. A criterion measure of walking capacity in lumbar spinal stenosis and its comparison with a treadmill protocol. Spine. 2009;34(22):2444–2449. doi:10.1097/BRS.0b013e3181b03fc8
21. Dyck P, Doyle JB. “Bicycle test” of van Gelderen in diagnosis of intermittent cauda equina compression syndrome. J Neurosurg. 1977;46(5):667–670. doi:10.3171/jns.1977.46.5.0667
22. Fritz JM, Delitto A, Welch WC, Erhard RE. Lumbar spinal stenosis: a review of current concepts in evaluation, management, and outcome measurements. Arch Phys Med Rehabil. 1998;79(6):700–708. doi:10.1016/S0003-9993(98)90048-X
23. Olszewski AD, Yaszemski MJ, White AA III. The anatomy of the human lumbar ligamentum flavum: new observations and their surgical importance. Spine. 1996;21(20):2307–2312. doi:10.1097/00007632-199610150-00001
24. Bridwell KH. Lumbar spinal stenosis. Diagnosis, management, and treatment. Clin Geriatr Med. 1994;10(4):677–701. doi:10.1016/S0749-0690(18)30323-9
25. Iversen MD, Katz JN. Examination findings and self-reported walking capacity in patients with lumbar spinal stenosis. Phys Ther. 2001;81(7):1296–1306. doi:10.1093/ptj/81.7.1296
26. Turner JA, Ersek M, Herron L, Deyo R. Surgery for lumbar spinal stenosis. Attempted meta-analysis of the literature. Spine. 1992;17(1):1–8. doi:10.1097/00007632-199201000-00001
27. Arbit E, Pannullo S. Lumbar stenosis: a clinical review. Clin Orthop Relat Res. 2001;384:137–143. doi:10.1097/00003086-200103000-00016
28. Jenis LG, An HS. Spine update. Lumbar foraminal stenosis. Spine. 2000;25(3):389–394. doi:10.1097/00007632-200002010-00022
29. Seppalainen AM, Alaranta H, Soini J. Electromyography in the diagnosis of lumbar spinal stenosis. Electromyogr Clin Neurophysiol. 1981;21(1):55–66.
30. Johnsson KE, Rosen I, Uden A. Neurophysiologic investigation of patients with spinal stenosis. Spine. 1987;12(5):483–487. doi:10.1097/00007632-198706000-00012
31. Jacobson RE. Lumbar stenosis: an electromyographic evaluation. Clin Orthop. 1976;115:68–71.
32. Hirsch LF. Diabetic polyneuropathy simulating lumbar disc disease. J Neurosurg. 1984;60(1):183–186. doi:10.3171/jns.1984.60.1.0183
33. Hartman J, Granville M, Jacobson RE. Radiologic evaluation of lumbar spinal stenosis: the integration of sagittal and axial views in decision making for minimally invasive procedures. Cureus. 2019;11(3):e2468.
34. Gao A, Wang Y, Miao Y, et al. Association between radiographic spinopelvic parameters and health-related quality of life in de novo degenerative lumbar scoliosis and concomitant lumbar spinal stenosis. Spine. 2020;45(16):E1013–1019. doi:10.1097/BRS.0000000000003471
35. Lang G, Vicari M, Siller A, et al. Preoperative assessment of neural elements in lumbar spinal stenosis by upright magnetic resonance imaging: an implication for routine practice? Cureus. 2018;10(4):e2440. doi:10.7759/cureus.2440
36. Alsaleh K, Ho D, Rosas-Arellano P, et al. Radiographic assessment of degenerative lumbar spinal stenosis: is MRI superior to CT? Eur Spine J. 2017;26(2):362–367. doi:10.1007/s00586-016-4724-9
37. Mir MM, John A, Naeem MA, Butt HR, Ali A. Prevalance and radiographical evaluation of lumbar spondylosis on magnetic resonance imaging. EAS J Radiol Imaging Techol. 2012;3(2):57–65. doi:10.36349/easjrit.2021.v03i02.005
38. Lee NJ, Mathew J, Kim JS, et al. Flexion-extension standing radiographs underestimate instability in patients with single-level lumbar spondylolisthesis: comparing flexion-supine imaging may be more appropriate. J Spine Surg. 2021;7(1):48–54. doi:10.21037/jss-20-631
39. Hallinan JTPD, Zhu L, Yang K, et al. Deep learning model for automated detection and classification of central, lateral recess and neuronal foraminal stenosis at lumbar spine MRI. Radiology. 2021;300(1):130–138. doi:10.1148/radiol.2021204289
40. Martin CN, Hughes RA. Epidemiology of peripheral neuropathy. J Neurol Neurosurg Psychiatry. 1997;62(4):310–318. doi:10.1136/jnnp.62.4.310
41. Italian General Practitioner Study Group (IGPSG). Chronic symmetric symptomatic polyneuropathy in the elderly: a field screening investigation in two Italian regions, I: prevalence and general characteristics of the sample. Neurology. 1995;45(10):1832–1836. doi:10.1212/WNL.45.10.1832
42. Al-Geffari M. Comparison of different screening tests for diagnosis of diabetic peripheral neuropathy in primary health care setting. Int J Health Sci. 2012;6(2):127–134. doi:10.12816/0005988
43. James C, Watson P, James B, Dyck M. Peripheral neuropathy: a practical approach to diagnosis and symptom management. Mayo Clin Proc. 2015;90(7):940–951. doi:10.1016/j.mayocp.2015.05.004
44. Deer T, Sayed D, Michels J, et al. A review of lumbar spinal stenosis with intermittent neurogenic claudication: disease and diagnosis. Pain Med. 2019;20(Suppl_2):S32–S44. doi:10.1093/pm/pnz161
45. Messiah S, Tharian AR, Candido KD, et al. Neurogenic claudication: a review of current understanding and treatment options. Curr Pain Headache Rep. 2019;23(5):32. doi:10.1007/s11916-019-0769-x
46. Kalichman L, Cole R, Kim DH, et al. Spinal stenosis prevalence and association with symptoms: the Framingham Study. Spine J. 2009;33:183–189.
47. Nadeau M, Rosas-Arellano MP, Gurr KR, et al. The reliability of differentiating neurogenic claudication from vascular claudication based on symptomatic presentation. Can J Surg. 2013;56(6):6. doi:10.1503/cjs.016512
48. Manchikanti L, Kaye AD, Manchikanti K, et al. Efficacy of epidural injections in the treatment of lumbar central spinal stenosis: a systematic review. Anesth Pain Med. 2016;5(1):e23139.
49. Hamburg N, Creager M. Pathophysiology of intermittent claudication in peripheral artery disease. Circ J. 2017;81(3):281–289. doi:10.1253/circj.CJ-16-1286
50. Spengel FA, Brown TM, Dietze S, et al. The Claudication Scale (CLAU-S). Dis-Manage-Health-Outcomes. 1997;2(Supplement 1):65–70. doi:10.2165/00115677-199700021-00013
51. Hinchliffe RJ, Forsythe RO, Apelqvist J, et al. Guidelines on diagnosis, prognosis, and management of peripheral artery disease in patients with foot ulcers and diabetes (IWGDF 2019 update). Diabetes Metab Res Rev. 2020;36(S1):e3276. doi:10.1002/dmrr.3276
52. Mignucci L, Bell G. Differential diagnosis of sciatica. In: Herkowitz H, Garfin S, Balderson R, Eismont F, Bell G, Wiesel S, editors. The Spine.
53. Bogduk N. On the definitions and physiology of back pain, referred pain and radicular pain. Pain. 2009;147(1–3):17–19. doi:10.1016/j.pain.2009.08.020
54. Alexander CE, Varacallo M. Lumbosacral radiculopathy. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 [Updated 2021 May 4]. Available from https://www.ncbi.nlm.nih.gov/books/NBK430837/.
55. Van der Windt DA, Simons E, Riphagen II, et al. Physical examination for lumbar radiculopathy due to disc herniation in patients with low-back pain. Cochrane Database Syst Rev. 2010;17(2):CD007431.
56. Kennedy DJ, Noh MY. The role of core stabilization in lumbosacral radiculopathy. Phys Med Rehabil Clin N Am. 2011;22(1):91–103. doi:10.1016/j.pmr.2010.12.002
57. Tang S, Mo Z, Zhang R. Acupuncture for lumbar disc herniation: a systematic review and meta-analysis. Acupunct Med. 2018;36(2):62–70. doi:10.1136/acupmed-2016-011332
58. Centers for Medicare and Medicaid Services. Percutaneous image guided lumbar decompression for lumbar spinal stenosis. Available from: https://www.cms.gov/Medicare/Coverage/Coverage-with-Evidence-Development/PILD.html.
59. Diwan S, Sayed D, Deer TR, Salomons A, Liang K. An algorithmic approach to treating lumbar spinal stenosis: an evidenced-based approach. Pain Med. 2019;20(Suppl 2):S23–S31. doi:10.1093/pm/pnz133
60. Hansson T, Suzuki N, Hebelka H, Gaulitz A. The narrowing of the lumbar spinal canal during loaded MRI: the effects of the disc and ligamentum flavum. Eur Spine J. 2009;18(5):679–686. doi:10.1007/s00586-009-0919-7
61. Brown LL. A double blind, randomized, prospective study of epidural steroid injection vs the MILD procedure in patients with symptomatic lumbar spinal stenosis. Pain Pract. 2012;12(5):333–341. doi:10.1111/j.1533-2500.2011.00518.x
62. Benyamin RM, Staats PS. MILD is an effective treatment for lumbar spinal stenosis with neurogenic claudication: MIDAS ENCORE randomized control trial. Pain Physician. 2016;19(4):229–242. doi:10.36076/ppj/2019.19.229
63. Deer TR, Kapural L. New image-guided ultra-minimally invasive lumbar decompression method: the MILD procedure. Pain Physician. 2010;13:35–41. doi:10.36076/ppj.2010/13/35
64. Chopko B, Caraway DL. MIDAS I (MILD decompression alternative to open surgery): a preliminary report of a prospective, multi-center clinical study. Pain Physician. 2010;13:369–378. doi:10.36076/ppj.2010/13/369
65. Chopko BW. A novel method for treatment of lumbar spinal stenosis and high risk surgical candidates: pilot study experience with percutaneous remodeling of the ligamentum flavum and lamina. J Neurosurg Spine. 2011;14(1):46–50. doi:10.3171/2010.9.SPINE091012
66. Basu S. MILD study: single site prospective IRB study. Clin J Pain. 2012;28(3):254–258. doi:10.1097/AJP.0b013e31822bb344
67. Mekhail N, Costnadi S, Nageeb G, et al. The durability of minimally invasive lumbar decompression procedure in patients with symptomatic lumbar spinal stenosis: long-term follow-up. Pain Pract. 2021;21(8):826–835. doi:10.1111/papr.13030
68. Pope JE, Deer TR, Falowski SM. A retrospective, single-center, quantitative analysis of adverse events in patients undergoing spinal stenosis with neurogenic claudication using a novel percutaneous direct lumbar decompression strategy. J Pain Res. 2021;14:1909–1913. doi:10.2147/JPR.S304997
69. Costantini A, Buchser E, Van Buyten JP. Spinal cord stimulation for the treatment of chronic pain in patients with lumbar spinal stenosis. Neuromodulation. 2010;13(4):275–280. doi:10.1111/j.1525-1403.2010.00289.x
70. Kamihara M, Nakano S, Fukunaga T, et al. Spinal cord stimulation for treatment of leg pain associated with lumbar spinal stenosis. Neuromodulation. 2014;17(4):340–345. doi:10.1111/ner.12092
71. Jain S, Deer T, Sayed D, et al. Minimally invasive lumbar decompression: a review of indications, techniques, efficacy and safety. Pain Manage. 2020;10(5):331–348. doi:10.2217/pmt-2020-0037
72. Lingreen R, Grider JS. Retrospective review of patient self-reported improvement and post procedure findings for MILD (Minimally Invasive Lumbar Decompression). Pain Physician. 2010;13:555–560.
73. Wong WH. MILD interlaminar decompression for the treatment of lumbar spinal stenosis: procedure description in case series with one year follow up. Clin J Pain. 2012;28(6):534–538. doi:10.1097/AJP.0b013e31823aaa9d
74. Mekhail N, Vallejo R, Coleman MH, Benyamin RM. Long term results of percutaneous lumbar decompression MILD for spinal stenosis. Pain Pract. 2012;12:184–193.
75. Deer T, Kim C, Wahezi SE, Qu H, Sayed D. Objective real-world outcomes of patients suffering from painful neurogenic claudication treated with the MILD procedure: interim report of a randomized controlled trial. J Pain Res. 2021;14:1687–1697.
76. Mekhail N, Costandi SJ, Armanyous S, et al. The impact of age on the outcomes of minimally invasive lumbar decompression for lumbar spinal stenosis. Med Dev. 2020;13:151–161.
77. Zucherman JF, Hsu KY, Hartjen CA, et al. A prospective randomized multi-center study for the treatment of lumbar spinal stenosis with the X STOP interspinous implant: 1-year results. Eur Spine J. 2004;13(1):22–31. doi:10.1007/s00586-003-0581-4
78. Lindsey DP, Swanson KE, Fuchs P, et al. The effects of an interspinous implant on the kinematics of the instrumented and adjacent levels in the lumbar spine. Spine. 2003;28(10):2192–2197. doi:10.1097/01.BRS.0000084877.88192.8E
79. Deyo RA, Martin BI, Ching A, et al. Interspinous spacers compared with decompression or fusion for lumbar stenosis: complications and repeat operations in the Medicare population. Spine. 2013;38(10):865–872. doi:10.1097/BRS.0b013e31828631b8
80. Tapp SJ, Martin BI, Tosteson TD, et al. Understanding the value of minimally invasive procedures for the treatment of lumbar spinal stenosis: the case of interspinous spacer devices. Spine J. 2018;18(4):584–592. doi:10.1016/j.spinee.2017.08.246
81. Guyer R, Musacchio M, Cammisa FP Jr, Lorio MP. ISASS Recommendations/coverage criteria for decompression with interlaminar stabilization - coverage indications, limitations, and/or medical necessity. Int J Spine Surg. 2016;10:41. doi:10.14444/3041
82. Decision memo for percutaneous image-guided lumbar decompression for lumbar spinal stenosis (CAG-00433N). Available from: https://www.cms.gov/medicare-coverage-database/view/ncacal-decision-memo.aspx?proposed=Y&NCAId=269.
83. Summary of Safety & Effectiveness Data (SSED). Superion® InterSpinous Spacer (ISS). Available from: https://www.accessdata.fda.gov/cdrh_docs/pdf14/p140004b.pdf.
84. Wu AM, Zhou Y, Li QL, et al. Interspinous spacer versus traditional decompressive surgery for lumbar spinal stenosis: a systematic review and meta-analysis. PLoS One. 2014;9(5):e97142. doi:10.1371/journal.pone.0097142
85. Phan K, Rao PJ, Ball JR, Mobbs RJ. Interspinous process spacers versus traditional decompression for lumbar spinal stenosis: systematic review and meta-analysis. J Spine Surg. 2016;2(1):31–40. doi:10.21037/jss.2016.01.07
86. Cairns K, Deer T, Sayed D, van Noort K, Liang K. Cost-effectiveness and safety of interspinous process decompression (Superion). Pain Med. 2019;20(Suppl 2):S2–S8. doi:10.1093/pm/pnz245
87. Patel VI, Whang PG, Haley TR, et al. Superion interspinous process spacer for intermittent neurogenic claudication secondary to moderate lumbar spinal stenosis: two-year results from a randomized controlled FDA-IDE pivotal trial. Spine. 2015;40(5):275–282. doi:10.1097/BRS.0000000000000735
88. Nunley PD, Patel VV, Orndorff DG, Lavelle WF, Block JE, Geisler FH. Five-year durability of stand-alone interspinous process decompression for lumbar spinal stenosis. Clin Interv Aging. 2017;6(12):1409–1417. doi:10.2147/CIA.S143503
89. Nunley PD, Deer TR, Benyamin RM, Staats PS, Block JE. Interspinous process decompression is associated with a reduction in opioid analgesia in patients with lumbar spinal stenosis. Pain Res. 2018;11:2943–2948. doi:10.2147/JPR.S182322
90. Zaina F, Tomkins-Lane C, Carragee E, Negrini S. Surgical versus non-surgical treatment for lumbar spinal stenosis. Cochrane Database Syst Rev. 2016;1:CD010264.
91. Siebert E, Pruss H, Klingebiel R, Failli V, Einhaupl KM, Schwab JM. Lumbar spinal stenosis: syndrome, diagnostics and treatment. Nat Rev Neurol. 2009;5(7):392–403. doi:10.1038/nrneurol.2009.90
92. Backstrom KM, Whitman JM, Flynn TW. Lumbar spinal stenosis-diagnosis and management of the aging spine. Man Ther. 2011;16(4):308–317. doi:10.1016/j.math.2011.01.010
93. Bridwell KH, Sedgewick TA, O’Brien MF, Lenke LG. Baldus. The role of fusion and instrumentation in the treatment of degenerative spondylolisthesis with spinal stenosis. J Spinal Disord. 1993;6(6):461–472. doi:10.1097/00002517-199306060-00001
94. Esses SI, Sachs BL, Dreyzin V. Complications associated with the technique of pedicle screw fixation. A selected survey of ABS members. Spine. 1993;18(15):
95. Jutte PC, Castelein RM. Complications of pedicle screws in lumbar and lumbosacral fusions in 105 consecutive primary operations. Eur Spine J. 2002;11(6):594–598. doi:10.1007/s00586-002-0469-8
96. Hilibrand AS, Robbins M. Adjacent segment degeneration and adjacent segment disease: the consequences of spinal fusion? Spine J. 2004;4(6):190S–194S. doi:10.1016/j.spinee.2004.07.007
97. Gonzalez-Blohm SA, Doulgeris JJ, Aghayev K, Lee WE, Volkov A, Vrionis FD. Biomechanical analysis of an interspinous fusion device as a stand-alone and as supplemental fixation to posterior expandable interbody cages in the lumbar spine. J Neurosurg Spine. 2014;20(2):209–219. doi:10.3171/2013.10.SPINE13612
98. Karahalios DG, Musacchio MJ. Lumbar interspinous devices: fusion and motion sparing. In: Holly L, Anderson P, editors. Essentials of Spinal Stabilization. Cham: Springer; 2017. doi:10.1007/978-3-319-59713-3_25.
99. Kim HJ, Bak KH, Chun HJ, Oh SJ, Kang TH, Yang MS. Posterior interspinous fusion device for one-level fusion in degenerative lumbar spine disease: comparison with pedicle screw fixation - preliminary report of at least one year follow up. J Korean Neurosurg Soc. 2012;52(4):359–364. doi:10.3340/jkns.2012.52.4.359
100. Vokshoor A, Khurana S, Wilson D, Filsinger P. Clinical and radiographic outcomes after spinous process fixation and posterior fusion in an elderly cohort. Surg Technol Int. 2014;25:271–276.
101. Falowski S, Sayed D, Deer T, Brescacin D, Liang K. Biomechanics and mechanism of action of indirect lumbar decompression and the evolution of a stand-alone spinous process spacer. Pain Med. 2019;20(S2):S14–S22. doi:10.1093/pm/pnz129
102. Postacchini F, Postacchini R, Menchetti PP, Sessa P, Paolino M, Cinotti G. Lumbar interspinous process fixation and fusion with stand-alone interlaminar lumbar instrumented fusion implant in patients with degenerative spondylolisthesis undergoing decompression for spinal stenosis. Asian Spine J. 2016;10(1):27–37. doi:10.4184/asj.2016.10.1.27
103. Chin KR, Pencle FJR, Benny A, Seale JA. Greater than 5-year follow-up of outpatient L4-L5 lumbar interspinous fixation for degenerative spinal stenosis using the INSPAN device. J Spine Surg. 2020;6(3):549–554. doi:10.21037/jss-20-547
104. Cuéllar JM, Field JS, Bae HW. Distraction laminoplasty with interlaminar lumbar instrumented fusion (ILIF) for lumbar stenosis with or without grade 1 spondylolisthesis: technique and 2-year outcomes. Spine. 2016;41(Suppl 8):S97–S105. doi:10.1097/BRS.0000000000001484
105. Li Z-H, Wang S-Y, Tang H, Ma H, Zhang Q-L, Ho T. Spinal fusion combined with dynamic interspinous fixation with COflex system for lumbar degenerative disease. Zhongguo Gu Shang. 2011;24(4):277–281.
106. Li M, Yang H, Wang G. Interspinous process devices for the treatment of neurogenic intermittent claudication: a systematic review of randomized controlled trials. Neurosurg Rev. 2017;40(4):529–536. doi:10.1007/s10143-016-0722-y
107. Falowski SM, Mangal V, Pope J, et al. Multicenter retrospective review of safety and efficacy of a novel minimally invasive lumbar interspinous fusion device. J Pain Res. 2021;31(14):1525–1531. doi:10.2147/JPR.S304957
108. Yaksh TL, Rudy TA. Analgesia mediated by a direct spinal action of narcotics. Science. 1976;192(4246):1357–1358. PMID: 1273597. doi:10.1126/science.1273597
109. Deer TR, Pope JE, Hayek S, et al. The Polyanalgesic Consensus Conference (PACC): recommendations on intrathecal drug infusion systems best practices and guidelines. Neuromodulation. 2017;20(2):96–132. doi:10.1111/ner.12538
110. Jain S, Malinowski M, Chopra P, Varshney V, Deer TR. Intrathecal drug delivery for pain management: recent advances and future developments. Expert Opin Drug Deliv. 2019;16(8):815–822. doi:10.1080/17425247.2019.1642870
111. Capozza MA, Triarico S, Mastrangelo S, Attinà G, Maurizi P, Ruggiero A. Narrative review of intrathecal drug delivery (IDD): indications, devices and potential complications. Ann Transl Med. 2021;9(2):186. doi:10.21037/atm-20-3814
112. Deer TR, Smith HS, Cousins M, et al. Consensus guidelines for the selection and implantation of patients with noncancer pain for intrathecal drug delivery. Pain Physician. 2010;13(3):E175–213. [PMID: 20495597]. doi:10.36076/ppj.2010/13/E175
113. Tomycz ND, Ortiz V, Moossy JJ. Simultaneous intrathecal opioid pump and spinal cord stimulation for pain management: analysis of 11 patients with failed back surgery syndrome. J Pain Palliat Care Pharmacother. 2010;24(4):374–383. doi:10.3109/15360288.2010.523066
114. Hayek SM, Veizi E, Hanes M. Intrathecal hydromorphone and bupivacaine combination therapy for post-laminectomy syndrome optimized with patient-activated bolus device. Pain Med. 2016;17(3):561–571. PMID: 26814257. doi:10.1093/pm/pnv021
115. Deer T, Chapple I, Classen A, et al. Intrathecal drug delivery for treatment of chronic low back pain: report from the national outcomes registry for low back pain. Pain Med. 2004;5(1):6–13. PMID: 14996232. doi:10.1111/j.1526-4637.2004.04011.x
116. Grider JS, Etscheidt MA, Harned ME, et al. Trialing and maintenance dosing using a low-dose intrathecal opioid method for chronic nonmalignant pain: a prospective 36-month study. Neuromodulation. 2016;19(2):206–219. doi:10.1111/ner.12352
117. Nerland US, Jakola AS, Solheim O, et al. Minimally invasive decompression versus open laminectomy for central stenosis of the lumbar spine: pragmatic comparative effectiveness study. BMJ. 2015;350:h1603. doi:10.1136/bmj.h1603
118. Thome C, Zevgaridis D, Leheta O, et al. Outcome after less-invasive decompression of lumbar spinal stenosis: a randomized comparison of unilateral laminotomy, bilateral laminotomy, and laminectomy. J Neurosurg Spine. 2005;3(2):129–141. doi:10.3171/spi.2005.3.2.0129
119. Yoshihara H. Indirect decompression in spinal surgery. J Clin Neurosci. 2017;44:63–68. doi:10.1016/j.jocn.2017.06.061
120. Binder DK, Schmidt MH, Weinstein PR. Lumbar spinal stenosis. Semin Neurol. 2002;22(2):157–166. doi:10.1055/s-2002-36539
121. Weinstein JN, Lurie JD, Tosteson TD, et al. Surgical compared with nonoperative treatment for lumbar degenerative spondylolisthesis. Four-year results in the Spine patient outcomes research trial (SPORT) randomized and observational cohorts. J Bone Joint Surg Am. 2009;91(6):1295–1304. doi:10.2106/JBJS.H.00913
122. Athiviraham A, Yen D. Is spinal stenosis better treated surgically or nonsurgically? Clin Orthop Relat Res. 2007;458:90–93. doi:10.1097/BLO.0b013e31803799a9
123. Caylor J, Reddy R, Yin S, et al. Spinal cord stimulation in chronic pain: evidence and theory for mechanisms of action. Bioelectron Med. 2019;5(2):1–41. doi:10.1186/s42234-019-0018-y
124. Lamer TJ, Deer TR, Hayek SM. Advanced innovations for pain. Mayo Clin Proc. 2016;91(2):246–258. doi:10.1016/j.mayocp.2015.12.001
125. Deer TR, Mekhail N, Provenzano D, et al. The appropriate use of neurostimulation of the spinal cord and peripheral nervous system for the treatment of chronic pain and ischemic diseases: the neuromodulation appropriateness consensus committee. Neuromodulation. 2014;17(6):515–550. doi:10.1111/ner.12208
126. Chandler GS 3rd, Nixon B, Stewart LT, Love J. Dorsal column stimulation for lumbar spinal stenosis. Pain Physician. 2003;6(1):113–118. doi:10.36076/ppj.2003/6/113
127. Wang D, Qureshi M, Smith J, Khetani N. Spinal cord compression related to spinal cord stimulator. Pain Med. 2018;19(1):212–214. doi:10.1093/pm/pnx123
128. Kim BS, Kim J, Koh HS, Han SY, Lee DY, Kim KH. Asymptomatic cervical or thoracic lesions in elderly patients who have undergone decompressive lumbar surgery for stenosis. Asian Spine J. 2010;4(2):65–70. doi:10.4184/asj.2010.4.2.65
129. Ter Meulen BC, Weinstein H, Ostelo R, Koehler PJ. The epidural treatment of sciatica: its origin and evolution. Eur Neurol. 2016;75(1–2):58–64. doi:10.1159/000443729
130. Bresnahan BW, Rundell SD, Dagadakis MC, et al. A systematic review to assess comparative effectiveness studies in epidural steroid injections for lumbar spinal stenosis and to estimate reimbursement amounts. Pm&r. 2013;5(8):705–714. doi:10.1016/j.pmrj.2013.05.012
131. Ammendolia C, Stuber K, de Bruin LK, et al. Nonoperative treatment of lumbar spinal stenosis with neurogenic claudication: a systematic review. Spine. 2012;37(10):E609– E616. doi:10.1097/BRS.0b013e318240d57d
132. Parr AT, Manchikanti L, Hameed H, et al. Caudal epidural injections in the management of chronic low back pain: a systematic appraisal of the literature. Pain Physician. 2012;15(3):E159–E198.
133. Malmivaara A, Slatis P, Heliovaara M, et al. Surgical or nonoperative treatment for lumbar spinal stenosis? A randomized controlled trial. Spine. 2007;32(1):1–8. doi:10.1097/01.brs.0000251014.81875.6d
134. Friedly JL, Comstock BA, Turner JA, et al. A randomized trial of epidural glucocorticoid injections for spinal stenosis. N Engl J Med. 2014;371(1):11–21. doi:10.1056/NEJMoa1313265
135. Manchikanti L, Cash KA, McManus CD, Pampati V, Fellows B. Results of 2-year follow-up of a randomized, double-blind, controlled trial of fluoroscopic caudal epidural injections in central spinal stenosis. Pain Physician. 2012;15(5):371–384. doi:10.36076/ppj.2012/15/371
136. Ammendolia C, Stuber KJ, Rok E, et al. Nonoperative treatment for lumbar spinal stenosis with neurogenic claudication. Cochrane Database Syst Rev. 2013;8:CD010712.
137. Koc Z, Ozcakir S, Sivrioglu K, Gurbet A, Kucukoglu S. Effectiveness of physical therapy and epidural steroid injections in lumbar spinal stenosis. Spine. 2009;34(10):985–989. doi:10.1097/BRS.0b013e31819c0a6b
138. Lee JH, An JH, Lee SH. Comparison of the effectiveness of inter-laminar and bilateral transforaminal epidural steroid injections in treatment of patients with lumbosacral disc herniation and spinal stenosis. Clin J Pain. 2009;25(3):206–210. doi:10.1097/AJP.0b013e3181878f9e
139. Staats PS, Benyamin RM. MiDAS ENCORE: randomized controlled clinical trial report of 6-month results. Pain Physician. 2016;19:25–38. doi:10.36076/ppj/2016.19.25
140. Wilson-MacDonald J, Burt G, Griffin D, Glynn C. Epidural steroid injection for nerve root compression: a randomized controlled trial. J Bone Joint Surg Br. 2005;87(3):352–355. doi:10.1302/0301-620X.87B3.15338
141. Manchikanti L, Buenaventura RM, Manchikanti KN, et al. Effectiveness of therapeutic lumbar transforaminal epidural steroid injections in managing lumbar spinal pain. Pain Physician. 2012;15:E199–E245. doi:10.36076/ppj.2012/15/E199
142. Fukusaki M, Kobayashi I, Hara T, Sumikawa K. Symptoms of spinal stenosis do not improve after epidural steroid injection. Clin J Pain. 1998;14(2):148–151. doi:10.1097/00002508-199806000-00010
143. Nam HS, Park YB. Effects of transforaminal injection for degenerative lumbar scoliosis combined with spinal stenosis. Ann Rehabil Med. 2011;35(4):514–523. doi:10.5535/arm.2011.35.4.514
144. Deer TR, Kim CK, Bowman RG 2nd, Ranson MT, Yee BS. Study of percutaneous lumbar decompression and treatment algorithm for patients suffering from neurogenic claudication. Pain Physician. 2012;15:451–460. doi:10.36076/ppj.2012/15/451
145. Weinstein JN, Tosteson TD, Lurie JD, et al. Surgical versus nonsurgical therapy for lumbar spinal stenosis. N Engl J Med. 2008;358(8):794–810. doi:10.1056/NEJMoa0707136
146. Carreon LY, Glassman SD, Howard J. Fusion and nonsurgical treatment for symptomatic lumbar degenerative disease: a systematic review of Oswestry Disability Index and MOS Short Form-36 outcomes. Spine J. 2008;8(5):747–755. doi:10.1016/j.spinee.2007.06.013
147. Sencan S, Edipoglu IS, Celenlioglu AE, Yolcu G, Gunduz OH. Comparison of treatment outcomes in lumbar central stenosis patients treated with epidural steroid injections: interlaminar versus bilateral transforaminal approach. Korean J Pain. 2020;33(3):226–233. doi:10.3344/kjp.2020.33.3.226
148. Cuckler JM, Bernini PA, Wiesel SW, et al. The use of epidural steroids in the treatment of lumbar radicular pain. A prospective, randomized, double-blind study. J Bone Joint Surg Am. 1985;67(1):63–66. doi:10.2106/00004623-198567010-00009
149. Wei P, Xu Y, Yao Q, Wang L. Randomized trial of 3-drug combination for lumbar nerve root epidural injections with a TNF-α inhibitor in treatment of lumbar stenosis. Br J Neurosurg. 2020;34(2):168–171. doi:10.1080/02688697.2020.1713990
150. Ghahreman A, Bogduk N. Predictors of a favorable response to transforaminal injection of steroids in patients with lumbar radicular pain due to disc herniation. Pain Med. 2011;12(6):871–912. doi:10.1111/j.1526-4637.2011.01116.x
151. Do KH, Kim TH, Chang MC. Effects of interlaminar epidural steroid injection in patients with moderate to severe lumbar central spinal stenosis: a prospective study. Ann Palliat Med. 2020;9(2):163–168. doi:10.21037/apm.2020.02.20
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.