Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Beliefs About Illness and Treatment Decision Modelling During Ill-Health in Arabic Families
Authors Arabiat D ![]() , Whitehead L
, Whitehead L ![]() , AL Jabery M
, AL Jabery M ![]() , Hamdan-Mansour A, Shaheen A
, Hamdan-Mansour A, Shaheen A ![]() , Abu Sabbah E
, Abu Sabbah E
Received 19 March 2021
Accepted for publication 9 June 2021
Published 8 July 2021 Volume 2021:14 Pages 1755—1768
DOI https://doi.org/10.2147/JMDH.S311900
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Diana Arabiat,1,2 Lisa Whitehead,1 Mohammad AL Jabery,1,3 Ayman Hamdan-Mansour,2 Abeer Shaheen,2 Eman Abu Sabbah2
1School of Nursing and Midwifery, Edith Cowan University, Perth, Australia; 2Faculty of Nursing, The University of Jordan, Amman, Jordan; 3School of Educational Sciences, The University of Jordan, Amman, Jordan
Correspondence: Diana Arabiat
School of Nursing and Midwifery, Edith Cowan University, 270 Joondalup Drive, Joondalup, WA, 6027 Email [email protected]
Background: The use of self-prescribed antibiotics and other unproven herbal remedies is common in the Arab world. Understanding how family members decide to manage illness is an important priority for health care providers.
Purpose: This paper presents a new model that can be viewed as an extension to the Health Belief Model and help clarifies the cognitive processes families use to manage illness in an Arab family in Jordan. It aims to generate an understanding of family beliefs about the causes of illness and appraisal of how best to manage illness in an Arab family.
Methods: A qualitative approach using a family interview method was used to collect data. Twenty-five families participated in semi-structured interviews designed to elicit representational models of illness and treatment-decisions.
Results: Thematic analysis revealed two forms of intertwined beliefs: core beliefs (fatalistic) and secondary beliefs (biomedical, supernatural and situational beliefs). Four key elements were identified as underpinning the involvement of family in treatment decision: perceived threat of illness, efficacy of treatment option, cost or availability and family prior experience.
Conclusion: An understanding of the health belief model and related cognitive appraisal processes used by families may assist health care providers to engage with and overcome some of the social, cultural, and structural variables that could influence how family members decide to manage illness in Jordan.
Keywords: family model, folk-remedies, health-beliefs, treatment-decision
Introduction
With the high reliance on use of folk/traditional remedies in Arab families,1 understanding how family members draw on biomedical models in the management of illness is important for health care providers striving to provide culturally competent care. It has been suggested that a person interested in folk remedies may use a complex system of traditional remedies mostly based on psychosocial interventions, mild herbs, ritualistic behaviour or household items.2,3 The use of folk remedies to manage illness is often influenced by family beliefs and the natural or social environment they live in.4,5 In this instance, understanding the relationship between health beliefs and traditional practices is important in conceptualising the capacity of families to manage illness during acute or chronic illness.
Historically, several theories have been suggested to explain this relationship, with the explanatory models of illness6 found to be the most accepted. Folk theories associated with the cultural formulations of explanatory models of illness have been part of much wider conceptual models used to explain lay model of ill-health. Kleinman’s explanatory model proposed that how people shape the experience of illness and the behaviour that follows constitute their “Folk Model of Illness”. The constellation of what has happened, why it has happened, and what should be done about it were considered important in understanding how individuals make sense of, and deal with their ill-health in terms of their own view of reality.7
Earlier studies have shown that biomedical models of illness that emphasise the roots of illness in anatomy, heredity, and disease processes, are more common in Western societies than elsewhere.8 Conversely, a “situational” model that describes psychosocial distress in the context of social and interpersonal situations may be a more common explanatory strategy in traditional societies and ethnic minorities.9
It is assumed that cultural and personal frameworks strongly influence treatment decisions in families.10 In a country like Jordan where family ties and cultural heritage are paramount and pervasive, health beliefs may influence health outcomes or may produce certain traditional practices that may shape self-management of illnesses.2
There is increasing recognition that families are often involved in decision-making during illness; however, little is known about how health beliefs influence decisions or behaviours related to managing an illness in the Arab world. Such knowledge will enable successful translation of culturally specific programs targeting health promotion and self-management of illness in Arab societies.4 For the Arab population, despite a small body of social and health science research on this population during the last few years, a gap exists in research on the cultural formulations of health and illness. A recently published studies of care practices and management of illnesses in Arab mothers demonstrated the importance of acknowledging traditional folklore and situating it within a family context.2 Understanding the underlying relationship of Arab culture to health beliefs and practices is a key factor in any treatment strategy that involves modifications of behaviours and other lifestyle intervention.4
Aims
This paper presents a new model that can be viewed as an extension to the Health Belief Model and help clarifies the cognitive processes families use to manage illness in an Arab family in Jordan. The aim of this study was to generate an understanding of family beliefs about the causes of illness within Arab families and family members’ appraisal of how best to manage illness.
Method
This study employed a qualitative descriptive research design involving semi-structured family group interviews.
Theoretical Framework
The theory underpinning the study was Kleinman’s explanatory model.7 It postulates that individual beliefs around illness, misfortune, and health are culturally determined and that individual’s health beliefs might be different from the ones held by their health providers.7,11 In Kleinman’s model, illness is culturally shaped and relates to how individuals perceive, experience, and cope with diseases.
The effect of cultural norms, Islamic values, as well as family dynamics tends to influence individual’s perception and experience of illness.12 For the purpose of this study, the Jordanian Arabic cultural context will be used to understand individual’s perceptions of disease in the following areas: how illness is caused, what causes it, why it started, why at a particular time, when did it happen, and what (happens) next.7 Understanding this interactive relationship will shed light on how health beliefs and health practices interact in relation to treatment and illness self-management in an Arab family.
Sample and Recruitment
A simple convenience sample was used to recruit a purposive sample of Arab families who lived in urban and metropolitan areas in Jordan. Potential participants were approached in the community setting through flyers posted in public places and social community settings. According to Zuna et al,13 the family unit in research is defined as “the collective number of individuals who consider themselves to be part of a family and who engage in the same activities together on a regular basis”. For this study, the family was the unit of analysis in this research and included family members living together or related by marriage or blood. In this study, first generation is defined as participants attending the family interview with their children and grandchildren, irrespective of the participant’s age; second generation is defined as parents attending the family interview with or without their children; and third generation as participants aged 18 years or older attending the family interview with their parents and/or grandparents. Identification of eligible families was limited to families who identified themselves as having an Arab background, able to speak and understand Arabic, and willingness to be part of a family group interview. Maximal variation was pursued on demographic factors, including socioeconomic status, level of education, age, and size of family to ensure that the sample was as representative as possible. Two research assistants with prior research experience (male and female) conducted all of the interviews with men and women interviewed at the same time. All interviews were conducted by one of the research assistants and lasted 1–2 hours.
Interviews
The family group interviews were conducted at a location chosen by and convenient to the participants and were mostly conducted at the participants’ home. All family members joined the interview in person, yet not all of the family unit decided to take part in the interview. The interview questions were designed to explore health-related beliefs and practices and the use of ethno-medical remedies among family members (see Supplementary File for the interview guide). The family group interviews varied in size from two participants to seven participants. All interview sessions were audiotaped and transcribed.
The data from all participants are presented as family level data. Twenty-five families from various geographic locations in Jordan agreed to participate in the study. Fifteen families had experienced at least one chronic condition such as cancer, type 2 diabetes or hypertension and 10 families experienced acute illness including allergies, eczema and viral infections. The family members’ age varied from 18 to 81 years, and the majority of participants were from two main cities in Jordan (Amman and Zarqa) and three from rural areas (Karak). Table 1 sets out participants’ demographic information by family case summary.
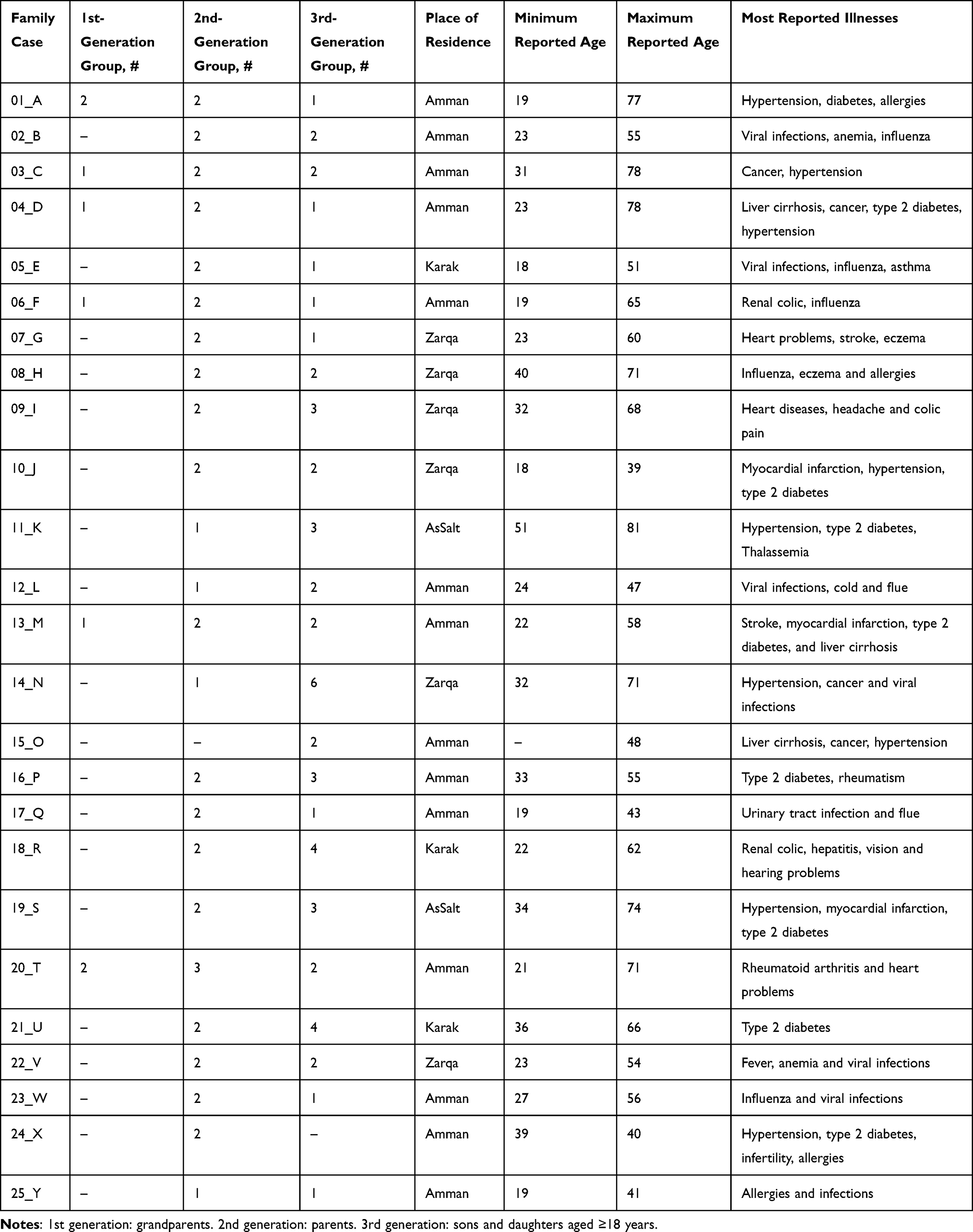 |
Table 1 Characteristics of the Sample of 107 Participants from 25 Extended Arab Families Attended the Interview |
Data Analysis
Thematic analysis was undertaken14 and the guidance developed by Knafl and Ayres15 drawn upon to analyse family data. Practical issues relating to interviewing families were considered16 and include preparation for the interviews, interviewer/family interactions during the interviews and closing the interview. Thematic analysis was used to determine the major recurring themes in the interviews, employing Boyatzis’s approach,14 where a theme is described as “a pattern found in the information that at a minimum describes and organises the possible observations and at maximum interprets the phenomenon, p. 3”.14 Analysis involved reducing the data to significant statements or quotes and identifying themes to draw together significant statements and coherent patterns. Analysis then moved on to compare themes across transcripts and explore relationships.
The family analysis approach set out by Knafl and Ayres15 was used to guide the analysis. Three questions were drawn on throughout the analysis to explore the meaning for family: how are these findings meaningful in investigating the family experience? Does the data represent family-level data? Do these data describe an individual perception of a family member that contributes to understanding the shared family experience? Family case studies were written up to capture and preserve both the individual viewpoint and family context of the data. By evaluating agreement among participants, homogeneity in responses between cases provided evidence for a shared, community-level folk model for the Arab community. We systematically compared individual and family themes on the causes of illness and behaviours following the onset of illness. The analysis was conducted by a team of two researchers and reviewed and discussed by a third.
Analysis of the family interview generated a series of structured narratives guided by the study questions. The following themes were highlighted throughout our analysis causes of illness, indicators to course of action, and decision to act (decision to use folk remedies and/or modern remedies).
In this study, research rigor was established through attention to the concepts of credibility, dependability, confirmability, and transferability.17 Credibility and trustworthiness of the findings were supported through the depth of the data collected with 25 families, the detailed descriptions of participants and the method used in writing case summaries. All narratives and transcripts were conducted in the participant’s native language for optimal clarification of beliefs and practices. To ensure dependability, the same interview guide was used for all family members, as well as an external researcher to secure dependability and reflexivity. Confirmability was generated through reflexivity and audit trials.
Ethical Consideration
This study was conducted in accordance with the Declaration of Helsinki. Prior to the interviews, the research assistants explained the study purpose to the participants and all family members provided informed consent that included publication of anonymized responses. Participants were informed of their right to withdraw from the study at any time and for any reason. Ethical approval was obtained from the Institutional Review Board (The University of Jordan, ethics approval dated 26/05/2016) before commencement of the study.
Results
Grounded in an initial analysis of the data that identified relevant coding categories and themes, the family case summary served to refine and extend the analytic categories and represent a family centered approach. The following steps were followed: First, substantive codes were inductively extracted from the data and applied to each interview. An example of codes that emerged at this stage were fatalistic beliefs, supernatural explanations, lay-referrals and self-medication (Table 2). This stage reduced the data to manageable units for further analysis. Secondly, two of the research team members individually reviewed the transcripts relating to each family group and prepared a brief background summary. The summaries were used to develop a guideline for completing detailed case summaries for each family, including analytic insights. An example of an analytic insight showed in one of the case summaries is presented below:
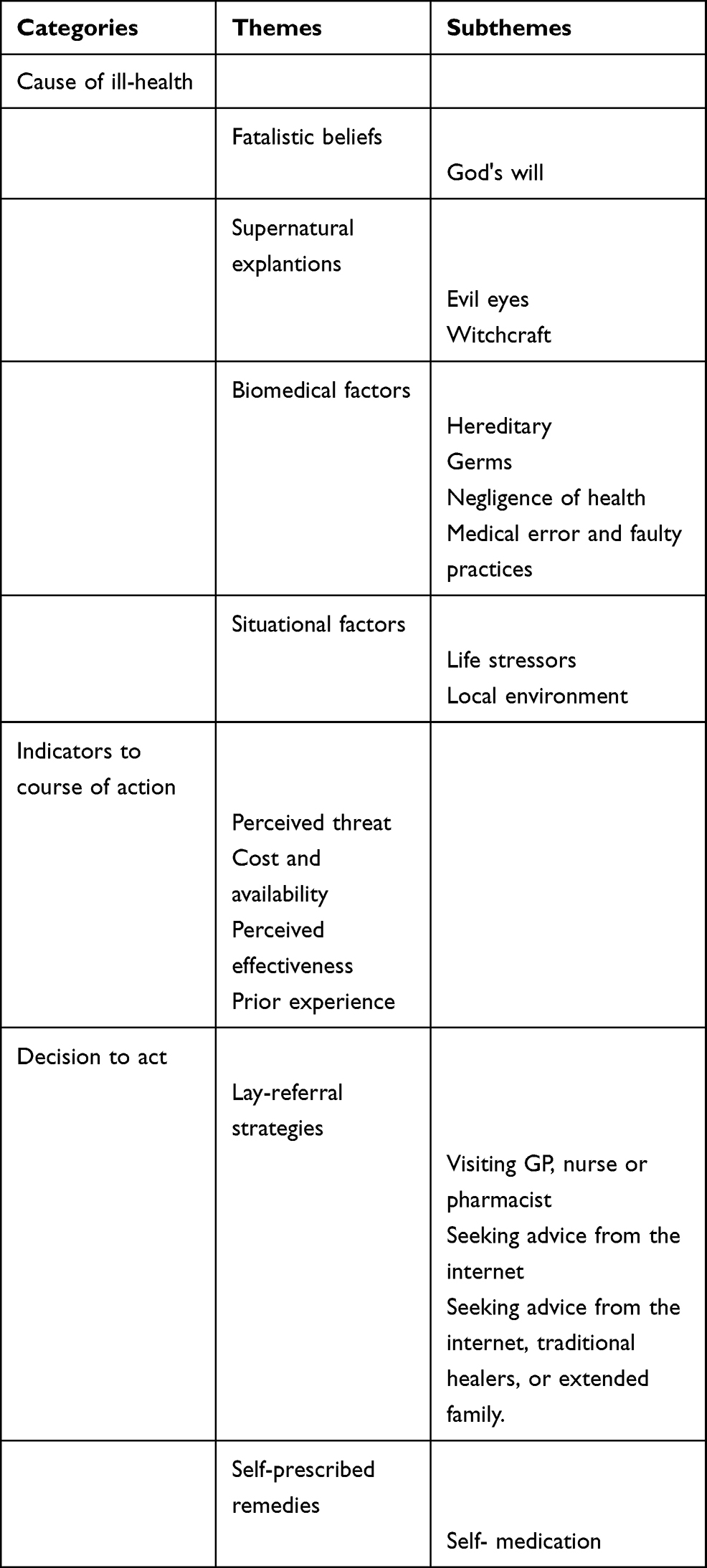 |
Table 2 Structure of Themes, Subthemes and Categories as Described by Families Prior to Their Use of Folk Remedies |
Brief Comment: View of Decision to Act
A mother (second generation) when asked “what do you do to restore your health when you are sick?” said,
I hate going to hospitals and doctors, but Ali (her son), God bless him, he always helps me following up my appointments with the GP to monitor my hypertension … I often drink herbal teas such as karkadeih (Scientific name: Roselle plants) and add medical plants such as garlic to my diet so I boost my health, but in combination with the tablet prescribed for my hypertension.
This statement illustrates the use of lay-referral strategies and self-prescribed remedies such as self-medication.
An Extended Comment
The quotation above illustrates the grandmother’s perception that she uses both folk remedies and modern remedies in managing illness. The case summaries presented in this study provided insight about whether family decisions to use folk remedies and/or modern remedies was based on their health beliefs, or prior experiences, and whether or not families were managing the illnesses using alternative practices. Case summaries assisted in identifying major analytic themes used in the identification and verification of thematic configurations across participating families. Examples of thematically coded data sorted by the case summaries for each family are provided in Table 3.
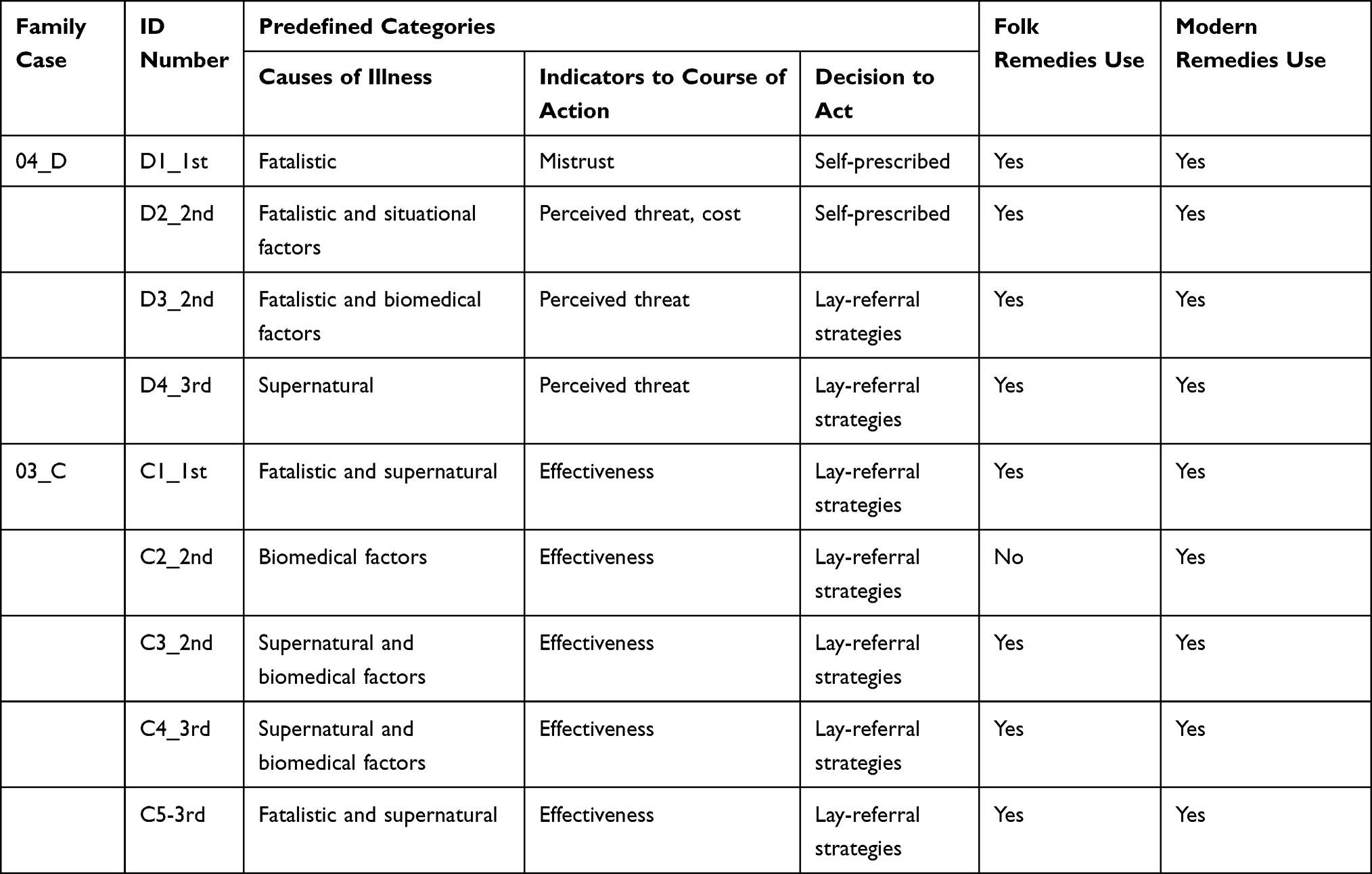 |
Table 3 Examples of Thematically Coded Data Sorted by Family Case Summary |
Throughout the major analytic categories, the beliefs regarding causes of illness and the social context in which families decide to self-manage their ill-health using folk and/or modern remedies were typical of the reflexive nature of qualitative research, and they were grounded in the data and contributed to further analysis. Overall, data pertaining to the beliefs about illness and symptoms management were generally multifaceted, including fatalistic beliefs, supernatural explanations, biomedical and/or situational factors. The main themes and illustrative quotes for the study findings are shown in Tables 4–6.
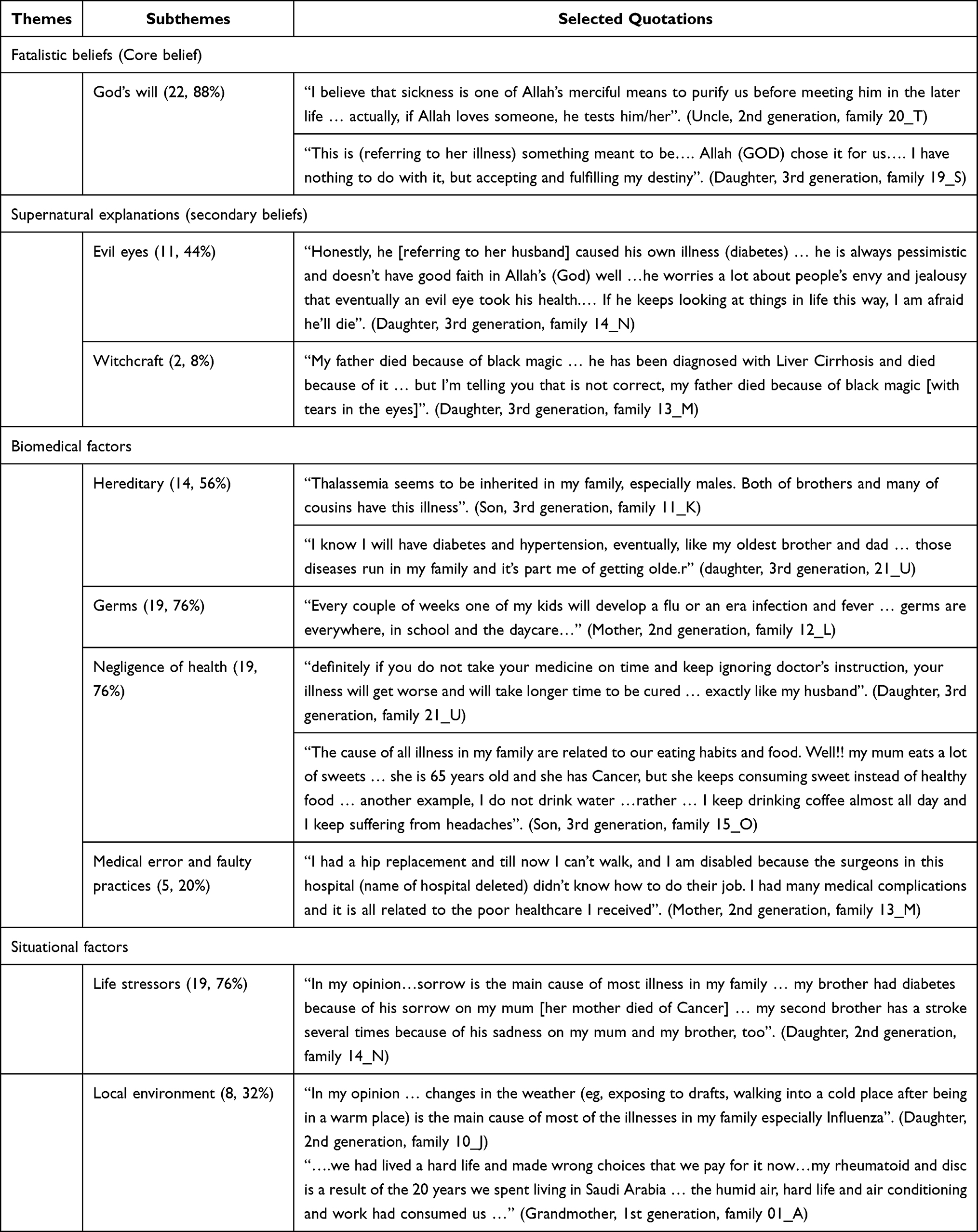 |
Table 4 Themes and Illustrative Quotations from Families Regarding the Cause of Illness at Family Level |
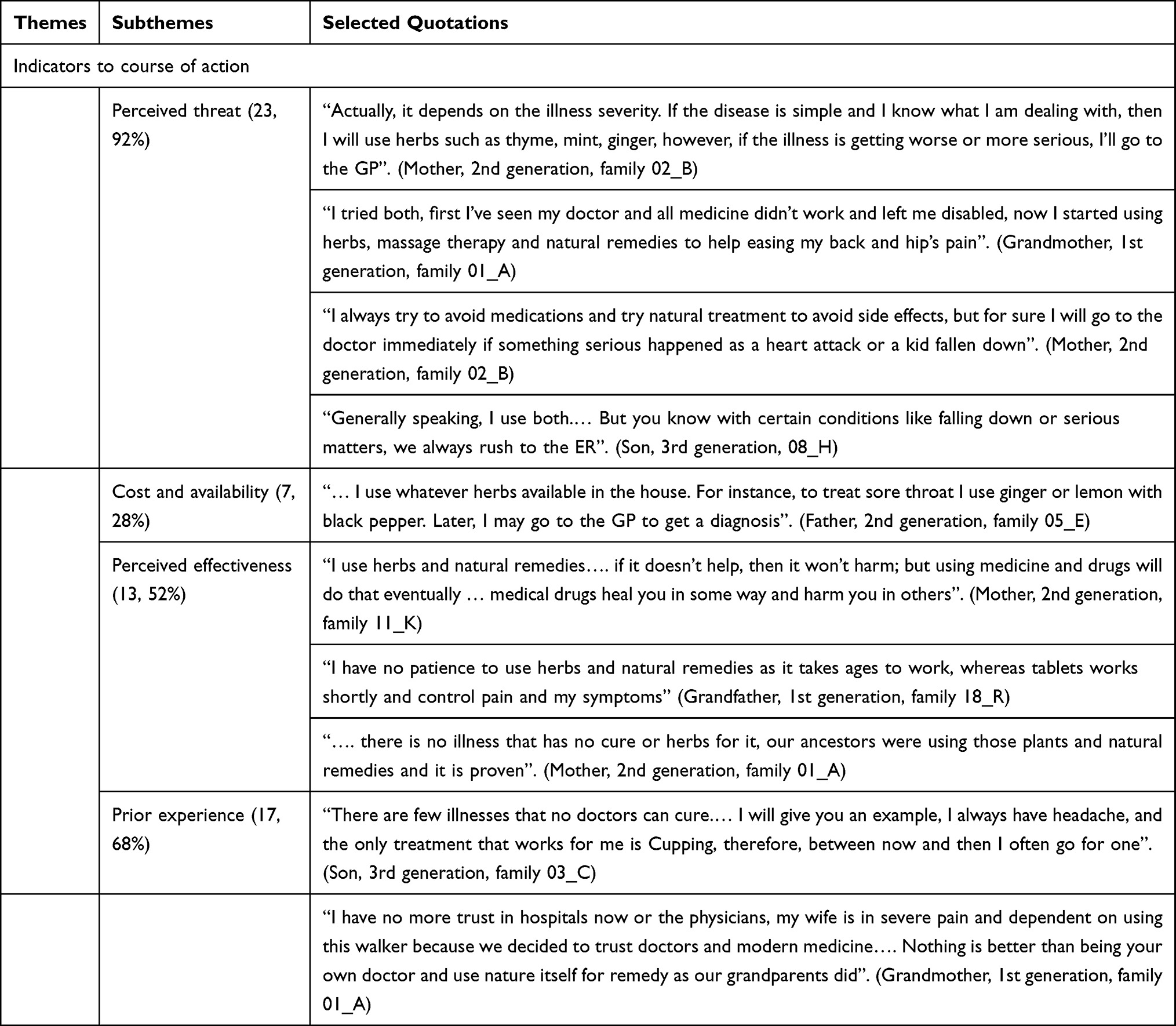 |
Table 5 Themes and Illustrative Quotations from Arab Families Regarding Indicators to Course of Action at Family Level |
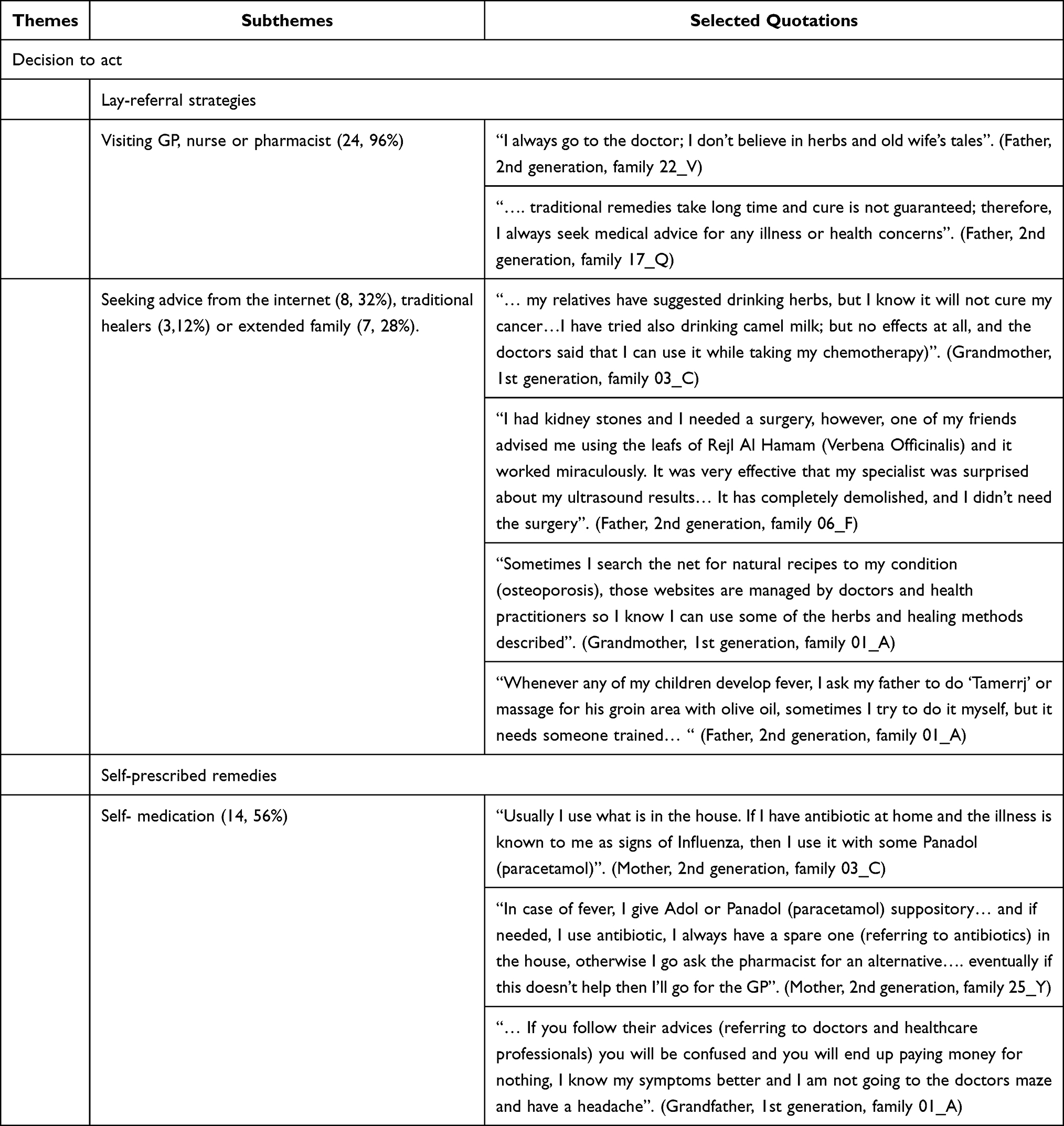 |
Table 6 Themes and Illustrative Quotations from Arab Families Regarding Decision to Act at Family Level |
The Treatment Decision Model
A treatment decision model evolved through analysis that describes how families, in this study conceptualised the cause of illness7 and key elements of family members’ appraisal of how best to manage illness (see Figure 1). The treatment decision model unfolded as follows: causes of illness, indicators to course of action, and decision to act (decision to use folk remedies and/or modern remedies).
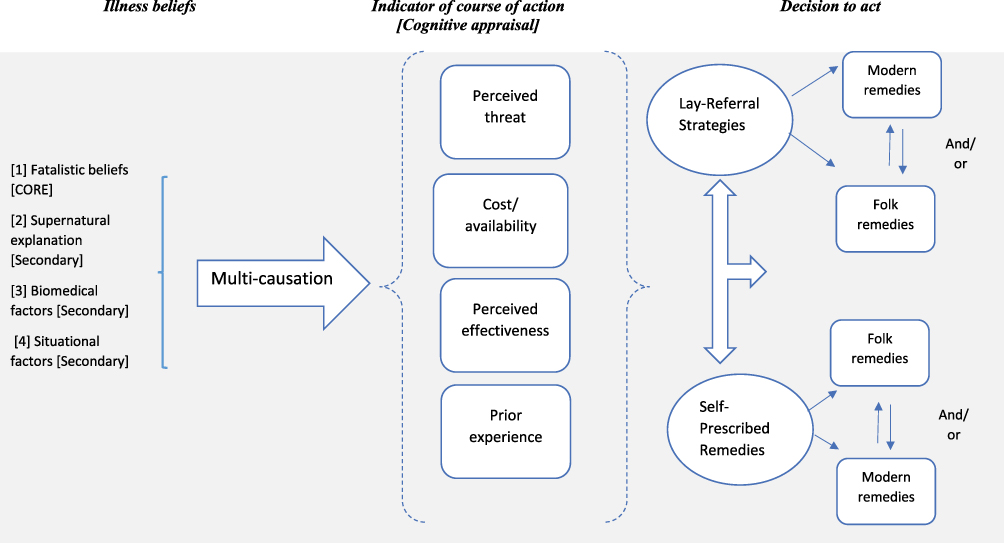 |
Figure 1 Health beliefs and treatment decision modelling during illness. |
Causes of Illness
Beliefs about the causes of illness were an assembly of several factors that family members used to try to explain why illness has happened. The main themes and illustrative quotes are shown in Table 4. We were able to identify four explanations of illness as part of much wider conceptual models used to make sense of illness between family members. This was through using fatalistic beliefs (God’s will) and/ or supernatural explanations including belief in an evil eye, or witchcraft to elucidate the cause of illness. Other beliefs included biomedical explanations where the roots of illness were emphasised in heredity factors, germs, faulty practices, and negligence of health, and finally, situational factors which are embedded in the context of life stressors and environment as common causes of illness. Each family member used two or three explanations for the cause of illness. For example, an illness can be caused by a germ or bad gene (reasons), yet it is considered to be “God’s will” that a germ is contracted or to inherit a gene (cause). This suggests two forms of intertwined beliefs: core beliefs (fatalistic) and secondary beliefs (biomedical, supernatural and situational beliefs).
Indicators of Course of Action
Each family has revealed an individual interpretation of illness within a family and possible reactions to this illness. This personal interpretation represents a general cognitive appraisal process for what to do during illness and how best to manage an illness within family. The main themes and illustrative quotes for the key elements underpinning treatment decisions among families are shown in Table 5.
The decision to see a doctor or to utilise self-prescribed remedies to manage illness included four key factors: First, evaluating the perceived threat of illness and possible outcomes. The majority of families (n = 23) illustrated that perception of illness severity as (simple or mild versus life threatening or emergency) were fundamental in helping to shape their treatment decisions and the use of folk and or modern remedies. Support for the decision to rely on modern remedies and attend a health clinic came mainly from subjective assessment that an illness was life threatening and fear of “death”. On the other hand, elements related with decisions to rely on folk remedies and/or self-medication were related to estimates of minor or low perceived threat (eg, short-term gastroenteritis, or common cold).
The second stage appraised the perceived effectiveness of treatment option (modern and/or folk remedies) in reducing severity of symptoms and treating the illness in a timely manner. Thirteen families described evaluating the extent to which illness could be managed by using folk remedies alone or in combination with modern remedies. Several family members described strong beliefs in the effectiveness of certain herbs and traditional practices such as hijama and cupping in treating their symptoms, while others described their concerns regarding the time it can take to achieve the desired outcome leading to the decision to use modern medicine. In addition, it was noted that some family members, in particular those with chronic illness in the family who perceived poor or low effectiveness of modern remedies reconciled modern remedies with folk remedies to manage illness.
The third stage was the decision to trust the family around the treatment option in light of family member’s previous experiences and knowledge about the illness or its symptoms. Central here were family members’ current and past experience with healthcare providers and management regimes. Almost 17 families stressed that they had lost trust in healthcare professionals and decided to rely on traditional remedies as first option for treatment to avoid unwanted side effects, medical errors, or faulty practices.
Finally, estimating the overall cost of the treatment option and its availability were described. As shown in Table 5, some families (n = 7) assessed the perceived financial consequences of attending a clinic or seeing their GP as not worthwhile. Participants described using self-prescribed antibiotics or herbs to self-manage their symptoms because it was readily available to them and at low-cost.
Decision to Act
Most families described using “lay-referral strategies” prior to deciding whether to rely on folk and or modern remedies. The term, “lay-referral” in this study is used to describe informal conversation and advice about any health concerns encountered. Lay referral in this study was an important method of getting families to use certain folk remedies, as well as it is considered as an important factor for choosing a particular health care professional for treatment.
As shown in Table 6, the extended family and social network of family members had an important role to play in family level decision around treatment. For example, while almost all families (n =24) acknowledged seeking medical advice from their general practitioner or healthcare provider at some point when feeling sick, fewer relied on traditional healers (n = 3) extended family member (n = 7) or social network (n = 8) for health advice. Furthermore, almost half of family members (n = 14) described using self-medication such as or over the counter medications (antibiotics can be accessed without a script in Jordan), in addition to other types of folk remedies to manage illness without informing their GP. Overall, our findings suggest that the link between illness beliefs and treatment decisions are tentative and not clear. While over half the family members believed that ill-health is caused by an evil eye or envy, these beliefs did not translate into treatment decisions such as going to traditional healer or relying on folk remedies alone).
Discussion
The current study used Kleinman “s framework7 to conceptualise a model that encompassed family beliefs about the causes of illness and key factors of family members” appraisal of how best to manage illness in an Arab family. To our knowledge, the current study is the first to provide conceptual modelling that explores and elaborates upon illness beliefs and treatment decisions using a family interview method.
As depicted in Figure 1, the treatment decision model is a conceptualisation of key factors of how the family interpreted illness within a family and how to it decided to manage it (cognitive appraisal). For example, a family’s initial appraisal can be that an illness is simple or mild and therefore can be managed by lay use of self-prescribed remedies, or an illness is life threatening or emergency and necessitates the use of lay referral strategies. Embodied within this model is cognitive appraisal that facilitates family ‘decision to use‘ modern remedies and/or “folk remedies” in managing illness. In this model, we propose that each family has its own lay model for both chronic and acute illness. Family decision to use folk remedies and or modern remedies in managing illness is conceptualised through the interplay of the four key factors together and are not necessarily tied to single cognitive domains or to a single key-factor.
In this study, a shared understanding of causes of illness was perceived to be a combination of fatalistic beliefs and/or situational and biomedical explanations (multicausal explanations). Causes of illness stated by families revealed strong beliefs about envy and the evil eye that are congruent with “supernatural explanation” yet cause of illness was seen in a more multifaceted way. These beliefs can be regarded as share beliefs within Arab families in Jordan, but it cannot be regarded as an exhaustive description of all illness beliefs. This finding may sound contradictory from the perspective of Kleinman’s theory of Explanatory Models,7 where illness beliefs are likely to fall under either supernatural/spiritual or bio-psychosocial domain. Yet, our findings are congruent with previous studies from Muslim societies18,19 that causes of illness are often embodied in multicausal explanations combining both spiritual and bio-psychosocial factors in explaining health and illness. This may reflect the modification of beliefs as a function of education or exposure to Western cultures.
Some of the health beliefs emerged as the expression of “God’s will”, commonly used in Muslim’s societies. For some participants, this may hold a deeper underlying meaning at play to determine thoughts and behaviours in an Arab family. Therefore, we suggest that fatalistic beliefs as “God’s will” are a core belief, while other interweaved beliefs are secondary or peripheral constructs. Core beliefs are important to identify, they are less likely to be challenged, distorted or modified during the participant’s life span.20,21
Overall, lay use of self-prescribed remedies (self-medication through modern or folk treatments) and the use of lay referral strategies (visiting a clinic or seeking other’s advice) relied on the evaluation of four key factors including perceived threat of illness, efficacy of treatment option, cost or availability and family prior experience. Some of these factors reaffirm Champion and Skinner22 notion presented in the Health Belief Model (HBM) where health decisions are made to reduce symptoms through evaluation of motivation to act; threat posed by the symptoms; benefits of an action to reduce the threat; and barriers or costs of the action. Therefore, the model proposed in this study can be viewed as an extension to the HBM described by Champion and Skinner.22 HBM theorises that for people to assume recommended behaviours, their perceived risk of disease and perceived benefits of action must outweigh the perceived barriers to the action. Those elements were used to address the challenges of habitual unhealthy behaviours such as smoking and overeating. However, our current model addresses specific cultural needs related to the choice between modern remedies vs folk remedies in Arab families in Jordan.
In this study, treatment decisions suggested a relationship between type and perceived severity of condition and decision to self-medicate. The accounts provided do not imply a sequential approach to action or to self-medicate; they are mutually reinforcing and are pursued in parallel. We argue that each family constructs causal models of ill-health with assumptions about how best to respond to illness, yet, it is less clear whether there is a relationship between illness beliefs and the decision to act. We argue that there is a trend in the evidence indicating association between illness beliefs and decisions to use folk or modern remedies. A further study to explore the proposed model further would allow further investigation of these relationships.
Whilst we were unable to associate treatment decisions with beliefs within our study, we would suggest that cultural values and norms influence family dynamics and beliefs systems within Arab family units and therefore the decision to use folk remedies and to self-medicate. This finding reflects in part the outcomes of an earlier study where the use of folk remedies and self-medication of children was not wholly attributed to Arab customs and traditions, but rather promoted through family, social media and virtual support groups for mothers in the Arab world.3 This suggests that family still influence beliefs and behaviours within the family unit, although influences outside of the family are also important.
Finally, whilst this study did not attempt to quantify findings on beliefs or practices, yet it revealed trends, for example, a high reliance on folk and alternative healthcare practices in Arab families in Jordan, high use of self-prescribed remedies among family members (folk herbs and/or self-prescribed antibiotics). This has also been described in other studies from Lebanon,23 and Jordan.24 The use of herbal remedies in the Middle Eastern region are historically linked to Arab family traditions, and/or the high floral diversity of Middle Eastern countries all year around.25 The high reliance on folk remedies may lead to a delay in seeking care, as well as potential risk of using non-medically approved remedies.
Strength and Limitations
Our findings are best understood in the context of Arab families in Jordan. While our study included a variety of demographic variables and representative data from different cities and backgrounds that makes our model transferable to the context of families in other Arab countries, further research is needed to explore whether the findings are applicable to other countries. It is important to acknowledge the possibility of selection bias related to use of convenience sampling as another limitation. Finally, we did not have equal samples of each family structure within our case family summaries, yet we believe our samples of each family structure were enough for detecting meaningful association between family members with relation to their beliefs and decisions to use folk and/or modern remedies.
Future research should address these shortcomings by replicating this study in different populations and by incorporating additional information about the context in which families are utilising self-prescribed remedies and its relationship with illness beliefs during acute and chronic illnesses. It will be interesting also to examine how did differences in health beliefs influence outcomes. Finally, due to limitations in the interview guide, we were unable to identify if some family members were more influential in decision-making than others, or if the decisions to use folk and herbal remedies were made as family or an individual unit. Future studies can refine and further developed our interview guide to elicit more specific information about this issue.
Conclusion
With the high reliance on folk and alternative healthcare practices in Arab families, understanding how family members decide to manage illness should be an important priority for health care professionals. The present study identified the specific key elements that contribute to the use of folk remedies guided by Kleinman.7 It also clarified the cognitive processes families use to manage illness in Jordan.
The findings highlight that though family members appear to share many health beliefs that are congruent with biomedical concepts, health beliefs among families in this study were often interwoven with beliefs that are fatalistic and situational in nature. Healthcare providers should be prepared to elicit and discuss the four key factors that were identified as underpinning the decision to use folk remedies or self-prescribed remedies such as non-prescribed antibiotics. Further attempts to understand the health belief model and related cognitive appraisal processes used by families may help assist families in making informed and safe treatment decisions.
Implications for Clinical Practice
The current conceptual model may have important implications for health interventions. A recent study26 suggested that health care professionals in Western countries who attempted to show respect toward other cultures fear that they may inhibit their natural inclinations and intuitions—sometimes compromising their clinical judgments. Therefore, health care professionals may feel hesitant to ask about cultural beliefs and assume belief patterns. This study highlights the importance of being curious and understanding how that individual/family make sense of the illness/treatment, and therefore how this influences their decision. An awareness of and understanding of the health belief model and related cognitive appraisal processes used by families in this study may assist nurses and other health care providers to engage with and overcome some of the social, cultural, and structural variables that could influence how family members decide to manage illness in an Arab family.
This study provides an initial set of evidence that can help to understand the illness beliefs and cognitive process underlying the decision to use folk and/or modern remedies in an Arab society. Therefore, this model can serve health promotion strategies directed for this population in any future studies. For example, it can inform the tailoring of interventions to the family’s culture and environment. While the Arab population is politically and religiously diverse, families share a common language and culture4 and given the self-prescribed remedies described above, it seems that self-prescribed modern remedies as antibiotics, which can be accessed without a script, provides an important mean for intervention and would perhaps be the most pervasive argument for intervention in Arab communities.
Data Sharing Statement
The data used to support the findings of this study have not been made available because of the sensitive nature of its content and concerns surrounding privacy and confidentiality of research participants. In addition, families participated in this study did not give consent for their data to be publicly shared. However, the anonymised raw data relevant to the study can be shared upon reasonable request on a case-by-case basis by contacting the following persons: Diana Arabiat, Associate Professor, Edith Cowan University, Australia, Email: ([email protected]).
Acknowledgments
We are grateful to all of the families who participated in the study, and we are grateful to the University of Jordan and Edith Cowan University for supporting the analysis and publication of this study.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded through the University of Jordan in Amman/ Jordan.
Disclosure
The authors declared no potential conflicts of interest in this work.
References
1. Alalwan TA, Mandeel QA, Al-Laith AA, Alkhuzai JA. Complementary practices of herbalists in the Kingdom of Bahrain. J Health Res. 2017;31(6):487–499. doi:10.14456/jhr.2017.60
2. Arabiat D, Whitehead L, AL Jabery M, Towell‐Barnard A, Shields L, Abu Sabah E. Traditional methods for managing illness in newborns and infants in an Arab society. Int Nurs Rev. 2019;66(3):329–337. doi:10.1111/inr.12505
3. Arabiat DH, Whitehead L, Al Jabery MA, Darawad M, Geraghty S, Halasa S. Newborn care practices of mothers in Arab societies: implication for infant welfare. J Transcult Nurs. 2019;30(3):260–267. doi:10.1177/1043659618794256
4. Bertran EA, Pinelli NR, Sills SJ, Jaber LA. The Arab American experience with diabetes: perceptions, myths and implications for culturally-specific interventions. Prim Care Diabetes. 2017;11(1):13–19. doi:10.1016/j.pcd.2016.07.004
5. Novak M, Costantini L, Schneider S, Beanlands H. Approaches to self‐management in chronic illness. In: Seminars in Dialysis. Vol. 26. No. 4. Oxford, UK: Blackwell Publishing Ltd; 2013 Mar:188–194. doi:10.1111/sdi.12080
6. de la Vega PB, Coe C, Paasche-Orlow MK, et al. “It’s like a mirror image of my illness”: exploring patient perceptions about illness using health mind mapping—a qualitative study. J Gen Intern Med. 2018;33(10):1692–1699. doi:10.1007/s11606-018-4557-9
7. Helman CG. Disease versus illness in general practice. J R Coll Gen Pract. 1981;31(230):548–552.
8. Hannan J. Minority mothers’ healthcare beliefs, commonly used alternative healthcare practices, and potential complications for infants and children. J Am Assoc Nurse Pract. 2015;27(6):338–348. doi:10.1002/2327-6924.12153
9. McCabe R, Priebe S. Explanatory models of illness in schizophrenia: comparison of four ethnic groups. Br J Psychiatry. 2004;185(1):25–30. doi:10.1192/bjp.185.1.25
10. Shahid S, Bleam R, Bessarab D, Thompson SC. “If you don’t believe it, it won’t help you”: use of bush medicine in treating cancer among Aboriginal people in Western Australia. J Ethnobiol Ethnomed. 2010;(1):1–9. doi:10.1186/1746-4269-6-18
11. Astin JA, Sierpina VS, Forys K, Clarridge B. Integration of the biopsychosocial model: perspectives of medical students and residents. Acad Med. 2008;83(1):20–27. doi:10.1097/ACM.0b013e31815c61b0
12. Begum S, Seppänen M. Islamic values in elderly care in Finland: the perspective of Muslim women caregivers. J Int Womens Stud. 2017;18(2):59–73.
13. Zuna N, Summers JA, Turnbull AP, Hu X, Xu S. Theorizing About Family Quality of Life. InEnhancing the Quality of Life of People with Intellectual Disabilities. Dordrecht: Springer; 2010:241–278.
14. Boyatzis RE. Mentoring for intentional behavioral change. In: The Handbook of Mentoring at Work: Theory, Research & Practice. Thousand Oaks: Sage; October 9, 2007:447–470.
15. Knafl KA, Ayres L. Managing large qualitative data sets in family research. J Fam Nurs. 1996;2(4):350–364. doi:10.1177/107484079600200402
16. Bennett JA, Cameron LD, Whitehead LC, Porter D. Differences between older and younger cancer survivors in seeking cancer information and using complementary/alternative medicine. J Gen Intern Med. 2009;24(10):1089–1094. doi:10.1007/s11606-009-0979-8
17. Elo S, Kääriäinen M, Kanste O, Pölkki T, Utriainen K, Kyngäs H. Qualitative content analysis: a focus on trustworthiness. SAGE Open. 2014;4(1):2158244014522633. doi:10.1177/2158244014522633
18. Arabiat DH, Al Jabery M, Abdelkader RH, Mahadeen A. Jordanian mothers’ beliefs about the causes of cancer in their children and their impact on the maternal role. J Transcult Nurs. 2013;24(3):246–253. doi:10.1177/1043659613481808
19. Tirodkar MA, Baker DW, Makoul GT, Khurana N, Paracha MW, Kandula NR. Explanatory models of health and disease among South Asian immigrants in Chicago. J Immigr Minor Health. 2011;13(2):385–394. doi:10.1007/s10903-009-9304-1
20. Årestedt L, Benzein E, Persson C. Families living with chronic illness: beliefs about illness, family, and health care. J Fam Nurs. 2015;21(2):206–231. doi:10.1177/1074840715576794
21. Bell JM, Wright LM. The illness beliefs model: advancing practice knowledge about illness beliefs, family healing, and family interventions. J Fam Nurs. 2015;21(2):179–185. doi:10.1177/1074840715586889
22. Champion VL, Skinner CS. The health belief model. Health Behav Health Educ. 2008;4:45–65.
23. Naja F, Alameddine M, Itani L, Shoaib H, Hariri D, Talhouk S. The use of complementary and alternative medicine among lebanese adults: results from a national survey. Evid Based Complementary Altern Med. 2015;2015:1–9. doi:10.1155/2015/682397
24. Wazaify M, Alawwa I, Yasein N, Al-Saleh A, Afifi FU. Complementary and alternative medicine (CAM) use among Jordanian patients with chronic diseases. Complement Ther Clin Pract. 2013;19(3):153–157. doi:10.1016/j.ctcp.2013.03.001
25. Saad B, Azaizeh H, Said O. Arab herbal medicine. Bot Med Clin Pract. 2008;4:31.
26. Casey S, Moss S, Wicks J. Therapists’ experiences of play therapy with Muslim families in Western Countries: the importance of cultural respect. Int J Play Ther. 2021. doi:10.1037/pla0000142
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.