")
Back to Journals » Psychology Research and Behavior Management » Volume 15
Beliefs About Body Weight and Practices of Regulating Food and Physical Exercise Patterns of Children Among Parents in Southern Ethiopia
Authors Zewude B , Siraw G , Melese B, Habtegiorgis T , Hizkeal A, Tadele M
Received 12 March 2022
Accepted for publication 19 July 2022
Published 27 July 2022 Volume 2022:15 Pages 1871—1883
DOI https://doi.org/10.2147/PRBM.S366132
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Bewunetu Zewude,1 Getahun Siraw,2 Belayneh Melese,3 Tewodros Habtegiorgis,1 Ashenafi Hizkeal,1 Mihret Tadele1
1Department of Sociology, College of Social Sciences and Humanities, Wolaita Sodo University, Wolaita Sodo town, Ethiopia; 2Department of Sociology, College of Social Sciences and Humanities, Dilla University, Dilla town, Ethiopia; 3Department of Civics and Ethical Studies, College of Social Sciences and Humanities, Wolaita Sodo University, Wolaita Sodo town, Ethiopia
Correspondence: Bewunetu Zewude, Email [email protected]
Background: The problem of childhood obesity is often associated with cultural values of body weight which includes the belief that voluptuous body size is a sign of good health status and better parental care. We examined the beliefs and behaviors of parents pertaining to preferred body weight of children, including practices of management of feeding and physical exercise patterns of children in southern Ethiopia.
Methods: Using cross-sectional survey study design, a structured questionnaire was distributed to randomly selected parents. Quantitative data were collected from 215 respondents, inserted into SPSS software, and analyzed by frequency and percentage distributions, charts, and multinomial logistic regression techniques.
Results: Most (59.1%) respondents want their child’s body weight to be normal/neither fat nor thin. In addition, 58.2% of the study participants held the opinion that average body size is an indication of good health status. Furthermore, 72.6% of respondents revealed that they control the amount of food their child consumes with the aim of preventing obesity/overweight. Moreover, 79.5% of respondents encourage their children to sometimes walk on foot, instead of always relying on vehicles while 87% of them replied that they regulate the amount of time their children spend watching TV. Above all, parents’ preference of voluptuous body size of children is significantly associated with age (OR=61.52.448, P < 0.001, 95%C.I: 57– 66.14), educational status (OR = 35.605, P < 0.001; 95%C.I: 6.050– 209.524), sex (OR = 0.237, P < 0.05; 95%C.I: 0.078-0.724) and grownup area (OR = 2.869, P < 0.05; 95%C.I: 1.062– 7.749).
Conclusion: Parents not only have adequate level of awareness regarding the health risks of children’s heavy body weight but also engage in the body weight management practices of their children such as by regulating the food consumption patterns of children, encouraging them to undertake physical exercises, and by being role models while doing physical exercises for themselves.
Keywords: childhood obesity, body weight, food consumption, physical exercise, regulation
Background
Overweight and obesity has become a major global public health problem and rising at a faster rate in urban areas of low- and middle-income countries due to the influence of demographic, epidemiological and nutrition transitions.1–4 Obesity was one of the leading risk factors for premature death contributing to 4.7 million deaths (8% of global deaths) in 2017.5 In sub-Saharan Africa, overweight/obesity levels are still lower than in high-income countries but certainly higher than they were two decades ago and increasing at an alarming rate.6 In this region, about 10.6% of school age children were overweight, of which 2.5% were obese.7 Studies conducted about the prevalence of obesity and overweight in Ethiopia,8–10 for instance, stated that Ethiopia is one of the sub-Saharan countries where 11.3% of children and adolescents were overweight or obese nationally in 2018.
Children and adolescents with overweight and obesity suffer from severe health consequences in childhood and are at high risk of becoming obese adults, suffer from social stigma and isolation, reducing attendance at school, and are vulnerable to increased risk of non-communicable diseases and reproductive disorders later in their life. Childhood obesity is also associated with increased morbidity of children and adolescents related to the risk of cardiovascular and other non-communicable diseases including diabetes.11 Moreover, the problem of obesity among children may jeopardize the wellbeing of parents, other family members, and parent–child relationship as well. For instance, Lee et al12 found that parents of children with obesity may experience weight stigma by association, a situation which directly affects parents, the children, and the parent–child relationship.
Among other factors, parents’ lack of awareness about nutritious food and failure to channel their children through healthy feeding practices, children’s habits of spending too much time at home and hence less time on physical activities, perhaps due to more television time have been identified as the causes for increased childhood obesity.13 Furthermore, Ang et al14 adds frequent intake of calorie-dense food stuffs, alterations of meal patterns, increased accessibility of fast foods and junk food items, busy work schedule of parents which leads to children being cared by care-providers increased rates of urbanization, car ownership and increased sedentary life styles as the other causes of childhood obesity. Moreover, Jeor et al15 contend that developmental, environmental, and psychosocial factors significantly contribute to physical inactivity, poor food consumption practices, and the resulting excessive weight gains among children which is also reinforced by families. According to Yazeedi et al16 children’s food consumption habit is associated with parental level of education, family income, and family nutrition and physical activity patterns, a result which indicates that family is a fundamental agent which plays a key role in shaping and influencing children’s life-style related behavior.
Whereas published researches regarding the knowledge and perception of parents about childhood obesity are hardly available in Ethiopia, the ones that were undertaken on related topics have principally emphasized on prevalence and determinants of obesity, focusing on the food and physical exercise behavior of the children, not their parents.7–9,17–21 On the other hand, studies undertaken on topics related to ours in areas outside of Ethiopia have mostly focused on the perception of obese parents or overweight children about childhood obesity. The present study fundamentally differs from such previous researches in that it took parents in the general population as its unit of analysis without considering their body weight status as the main criterion of inclusion. Doing so would be helpful in the sense that understanding the beliefs and patterns of practices about childhood obesity, feeding patterns, and cultural values of body weight held at societal level in general would have meaningful implications not only to comprehend the structural causes of the problem but also to address it effectively. In addition, individuals’ beliefs and routine practices about childhood obesity are the reflection of the general value system held at societal level. Moreover, members of a certain segment of the society (eg, obese parents) have little room to hold beliefs and engage in practices that are not parallel to the same situations at society level.
According to Caprio et al,11 the dynamic nature of culture suggests that additional research is needed to determine whether cultural patterns of shared understandings are the causes or consequences (or both) of childhood obesity. Therefore, this would justify the need to undertake related studies in areas where previous studies have not been conducted by collecting data from survey populations that reflect the characteristics of the general population. Furthermore, methodologically, most previous studies on beliefs about acceptable body size and parental perceptions of children’s body weight relied on qualitative methods alone and hence, our research differs by approaching the subject quantitatively. Above all, by including the perceptions of fathers in addition to that of the mothers, the present study differs from most previous related studies that focused on mothers alone for one or another reason. The purpose of this research was to examine the beliefs held by parents regarding body weight of children and the practices pertaining to regulating the patterns of food intake and physical exercises of children in Southern Ethiopia.
Materials and Methods
Research Design
Using quantitative research approach, a cross-sectional study was undertaken in which data were collected from a sample of parents having school-aged children in Southern Ethiopia. With both descriptive and explanatory study designs, we have examined the perceptions and practices of parents regarding children’s body weight, including the factors associated with preferences of children’s body weight.
Method and Procedures of Data Collection
Quantitative data were collected using survey research method through distributing a structured questionnaire. The questionnaire was developed first in English language by the researchers and later translated to the local language of the community where the data were collected. Then, it was given to two language editors who teach at Wolaita Sodo University and Dilla University. Following that, we have pilot tested the questionnaire taking 10% of the total sample size to ensure the validity of the instrument. Following the results of the pilot test, we have incorporated editorial and substantive findings into the questionnaire to enhance its validity. Training was given to data collectors regarding the purpose of the research, the variables in the questionnaire, and the procedure to be followed during data collection. A cooperation letter was secured from the concerned body of Wolaita Sodo University. After determining the sampling procedure and sample size, the data collectors contacted the research participants in their own location. In order to maintain the quality of data, selected parents were briefly oriented about the research, their role in the process, the content and themes of the questionnaire, and how they are supposed to answer the questions. Above all, data collectors were guiding and following-up the respondents during the entire processes of data gathering.
Instrument Design
The questionnaire used in this study was prepared by the researchers and then validated to help us address the research questions. It consisted mainly of four sections where the first section contains questions pertaining to the socio-demographic characteristics of respondents. This section consists of questions such as age, sex, educational status, and residential background of respondents. The aim of collecting such data was to examine the association between parents’ socio-demographic characteristics and their beliefs about acceptable body weight of children and their preferences of body size. The second section contains questions seeking responses about the perceptions regarding the acceptable body weight of children and body size preferences of research participants. It consists of questions such as 1) How do you want the body size/physical appearance of your child to be? 2) Do you believe that parents should help/do something to get their child become fat? 3) Do you think the body size of a child has something to do with health status? 4) Do you believe that physical strength of a child has something to do with body size/morphology, and 5) What do you feel if you find out that your child is increasingly getting overweight/obese? among other questions.
The third section of the questionnaire deals with questions that assess the perception and practices of respondents about regulating the food consumption behavior of children. Among others, it consists of questions such as 1) What is the common pattern of serving meals to a child at your home? 2) Do you regulate/control the food consumption practices of your child? 3) Do you often force/intimidate your child to finish all the food served to him/her on the dish? 4) When sending your child to school, do you often advice/warn him/her that s/he must finish the food you send with him or her? 5) Let us assume that your child did not finish all the food you sent with him/her to school, what do you do? and 6) Do you control the amount and type of food your child consumes to prevent overweight/obesity? Finally, the fourth section of the tool contains questions that aim to assess the beliefs about the relevance of physical exercises to controlling the body weight of children and the practices related to it. It contains questions such as 1) Do you encourage your child to sometimes walk on foot, instead of always relying on vehicles? 2) Do you regulate the amount of time your child should spend watching TV? 3) Do you believe that one has to do regular physical exercises to remain healthy? and 4) Do you believe that children should do some physical exercises to stay healthy? among other questions.
Sample and Sampling Procedure
A multi-stage cluster sampling technique was used to draw the sample of parents having one or more of school-aged children in the study area. In order to determine the sample size, the researchers applied Cochran’s (1977) formula for calculating sample size of unknown population as follows:

Where, n is the sample size, z is the selected critical value of desired confidence level, p is the estimated proportion of an attribute that is present in the population.
Then, the final sample units were chosen on the basis of probability proportionate to size sampling technique. The major inclusion criteria to participate in the study were having one or more school-aged children that is/are currently enrolled in primary level education in the study area and willingness to participate in the survey. Accordingly, in addition to those that were not willing to take part in the study, parents that do not have a child enrolled in a primary education level or those that have a child but teaching him/her at levels beyond primary level of education have been excluded. Among the seven administrative kebeles (the smallest administrative units in Ethiopia) found in Wolaita Sodo town, three were randomly selected. Then, the final sample units from each kebele were chosen on the basis of probability proportionate to size sampling technique. With a 5% contingency and consideration of possible non-response rate, 403 (384+19) copies of the questionnaires were duplicated and distributed. Respondents were contacted in their own houses after choosing the appropriate time in which participants can potentially be located at home. While visiting the homes, data collectors contacted either the fathers or the mothers, depending on their availability, after checking whether they have a child who attends primary level of education during the time of the study. From the distributed questionnaires, 295 were returned from which 215 were found to be correctly completed.
Data Analysis and Presentation
From the collected questionnaires, the ones that were fully completed and correctly filled were first sorted and hence, data clearing was undertaken. Then, the completed questionnaires were inserted into SPSS software for further processing. Data analysis was conducted using statistical techniques, including percentages, frequency distributions, charts, and multinomial logistic regression analysis. The first three statistical techniques were mainly used to present data regarding the frequency and percentage distributions of responses. It was, for instance, used to show the distribution of socio-demographic characteristics of respondents, parents’ beliefs about acceptable body weight of children and body size preferences in general, their perception and practices regarding regulation of food consumption patterns of children and physical exercises, among others. The multinomial logistic regression test was used to examine the association between socio-demographic characteristics of respondents and their values constituting body weight preferences.
Results
As presented in Table 1, the socio-demographic characteristics of the research participants reveal that most of the respondents (52.6%) were females. In addition, it is also shown that the majority (38.6%) of respondents constitute the age category of 26–33 while parents aged 58 and above comprised only 1.4%. Furthermore, the highest level of education that most respondents (28.8%) attained was primary education, followed by secondary education (24.7%). Moreover, 52.1% of respondents disclosed that they have grown up in an urban area.
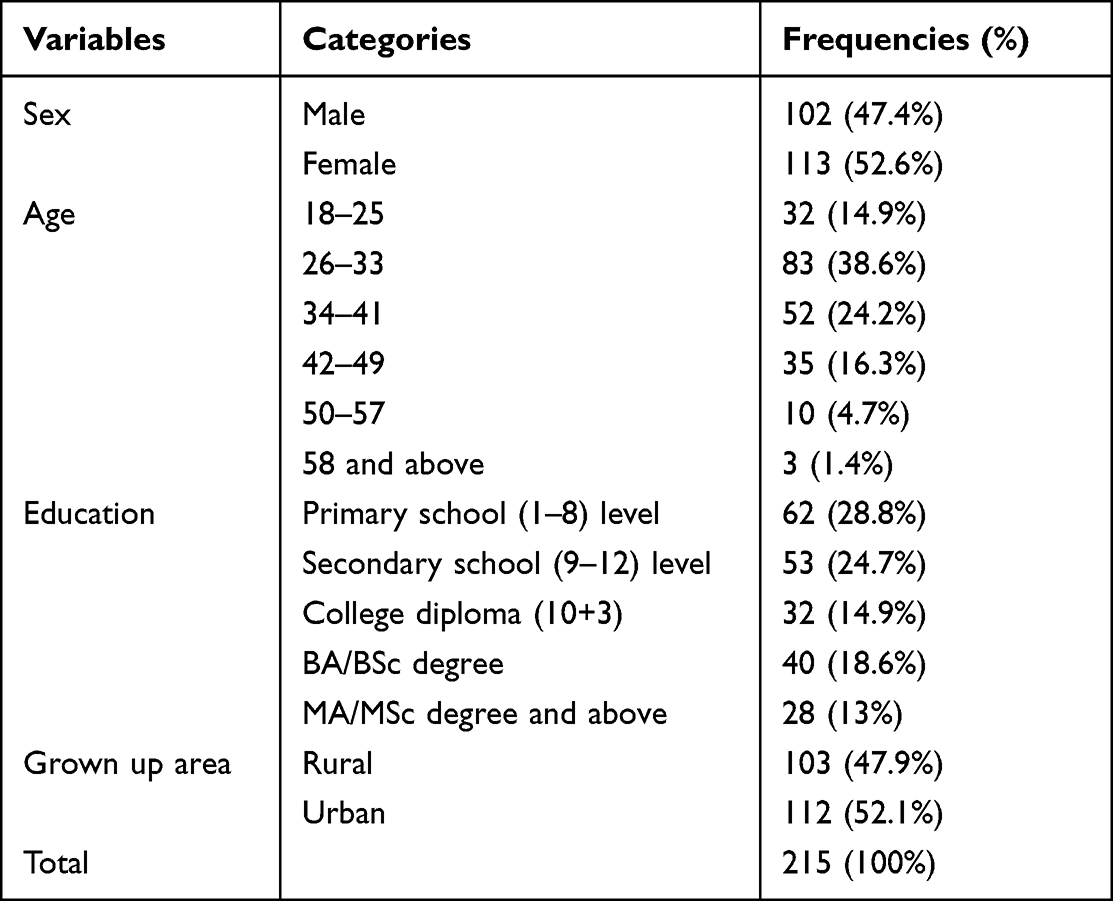 |
Table 1 Socio-Demographic Characteristics of Respondents |
Body Size Preferences and Beliefs Constituting Ideal Body Weight of a Child
Data pertaining to the body size preference of survey participants revealed that most (62.3%) respondents would like their own body size to be average/neither thin nor fat while 3.3% and 21.4% of them prefer very voluptuous and voluptuous body size, respectively. In addition, respondents were found to have no different preference of body size for men and women; 55.3% of respondents answered that both men and women should have average body size, as shown in Table 2. Most importantly, 59.1% of respondents replied that they want their child’s body size to be neither fat nor thin. Moreover, while 61.9% of respondents believe that parents should not do something to get their child become fat, the same percentage of respondents replied that they have never intervened to get their child obese. Furthermore, majority (52.1%) of respondents think that a child’s body size has something to do with health status and 57.2% believe that body size and physical strength are associated. It is also indicated that most (25.6%) of the respondents perceive that a child with an average body size is stronger. Above all, 68.4% of the research participants revealed that they would feel worried that their child may contract some kind of disease if they find out that their child is increasingly getting overweight/obese.
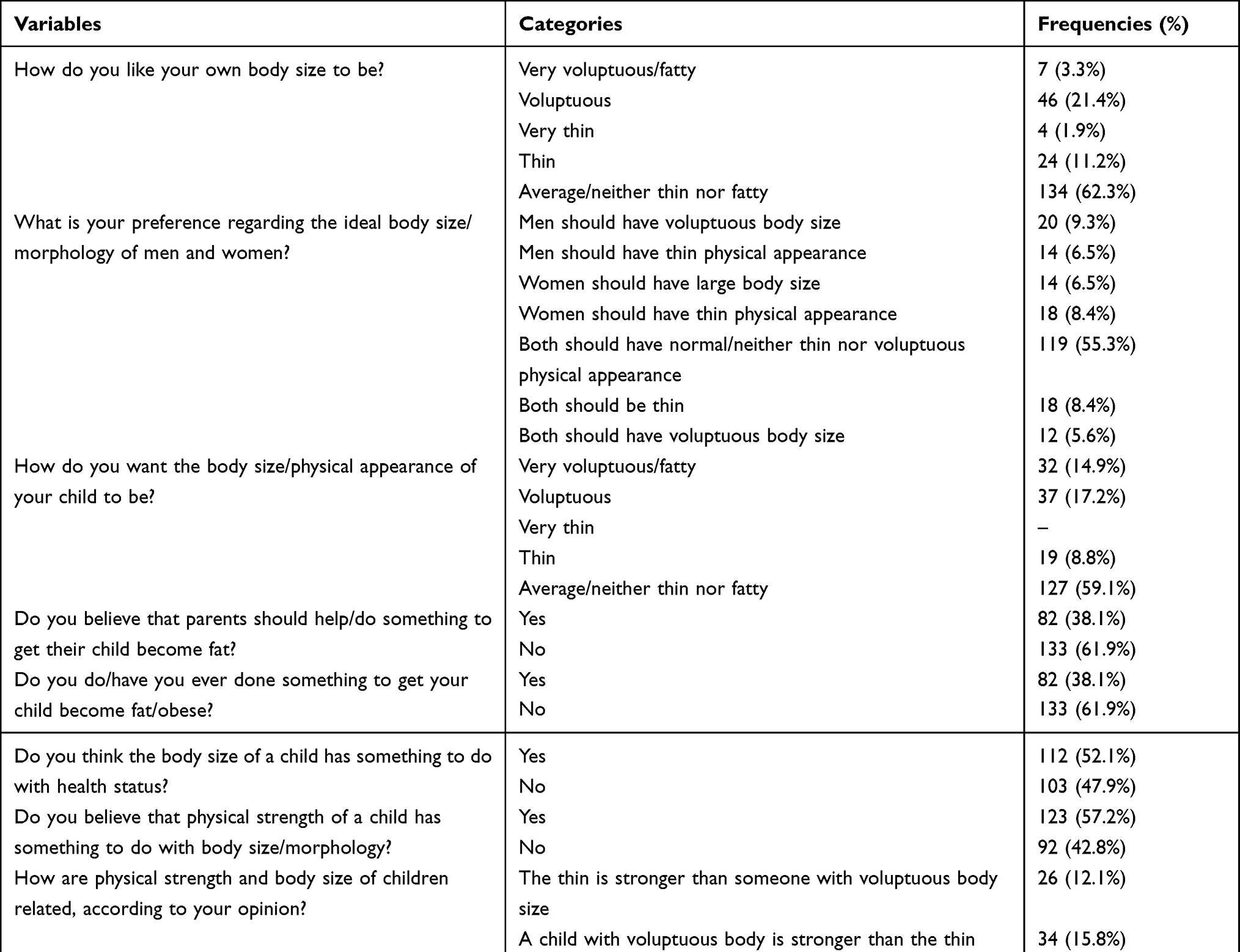 |
Table 2 Body Size Preferences and Beliefs About Appropriate Body Weight of a Child |
Data presented in Table 3 reveal that 53.5% of the respondents are highly concerned and 34% are concerned with the situation that their child is getting overweight or obese. In addition, the situation that a child is getting underweight is highly concerning and it is concerning for 50.2% and 44.7% of respondents, respectively, while 5.1% replied that it is not concerning for them. Moreover, the majority (90.2%) of respondents answered that it is not concerning if a child’s body weight always remains average but healthy. It is also shown that 56.7% and 70.7% of the survey participants replied that it is concerning when a child eats too much amount of food and too little amount of food, respectively.
 |
Table 3 Level of Concerns of Parents Regarding the Body Weight and Feeding Practices of Children |
According to the data presented in Figure 1, most (58.2%) of the study participants held the opinion that average body size – neither fatty nor tinny – is an indication of good health status, followed by 28.4% of respondents who agreed with the opinion that voluptuous body size can lead to chronic diseases, such as hypertension, and 23.6% of them who have accepted the opinion that body size has nothing to do with health condition.
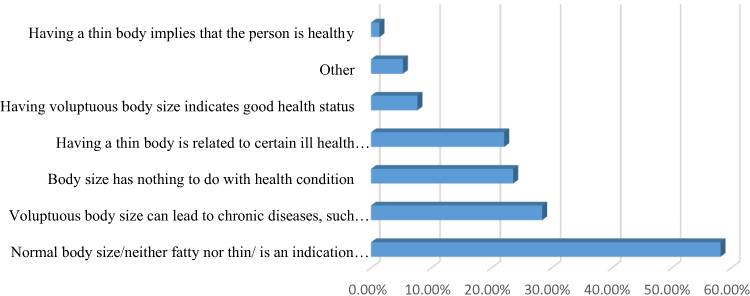 |
Figure 1 In your opinion, which of the following argument is/are acceptable? |
Perceptions and Experiences Related to Feeding Practices and Physical Exercise
Table 4 presents data pertaining to parents’ feeding practices of their school-aged children. Accordingly, it is found that the common patterns of serving meals to children has been three times a day (30.7%), followed by no limits or serving as needed by the child (27.4%), and four times a day (25.1%). Moreover, 93% of survey participants reported that they regulate the food consumption practices of their children. In addition, 72.6% of respondents revealed that they control the amount of food their child consumes with the aim of preventing obesity/overweight. It is also found that most (54.9%) of the respondents do not intimidate or compel their children to finish all the food served to him/her on the dish. Furthermore, while 53% of respondents replied that they focus on the food items that can help their child gain more body weight when preparing food, 76.3% of them answered that they often advice/warn their child that s/he must finish the food they send with him or her to school.
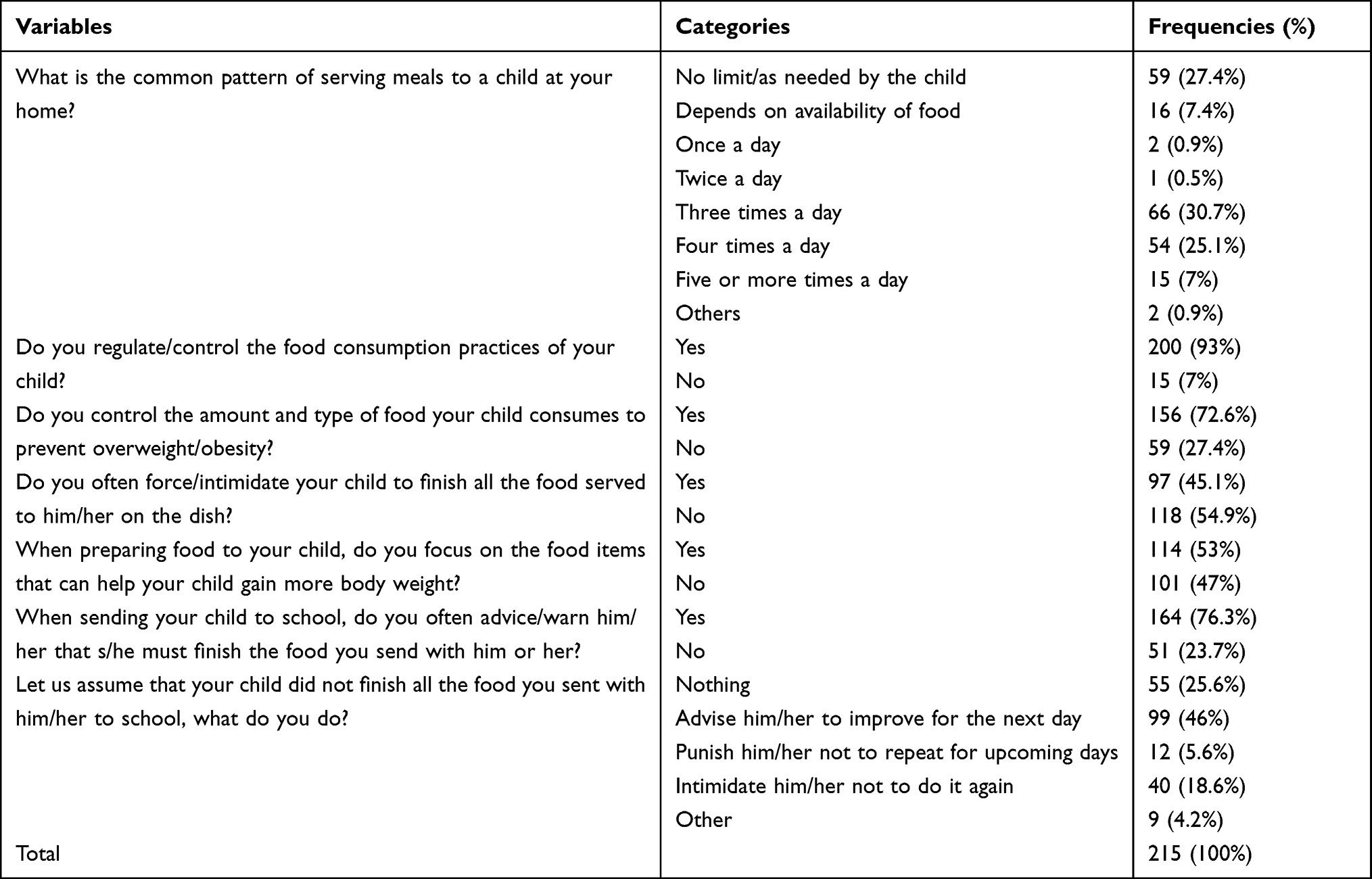 |
Table 4 Patterns of Feeding Children and Perceptions Regarding Child Feeding |
As shown in Figure 2, majority (77.7%) of our survey participants replied that they regulate the food consumption practices of their children by making sure that s/he eats on time, followed by encouraging/rewarding him/her to eat more amount of food (37.2%), and regulating that he/she is not over eating (17.2%).
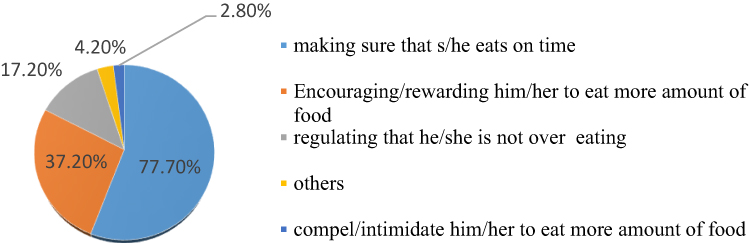 |
Figure 2 How do you regulate/control the food consumption practices of your child? |
According to the data presented in Table 5, it is found that 79.5% of respondents encourage their children to sometimes walk on foot, instead of always relying on vehicles. In addition, 87% of them replied that they regulate the amount of time their children spend watching TV. While 87.9% of the research participants believe that one has to do regular physical exercises to remain healthy, 78.6% reported that they do physical exercises. Furthermore, while 86% of respondents believe that children should do physical exercises to remain healthy, 82.8% of them disclosed that they encourage their children to do physical exercises.
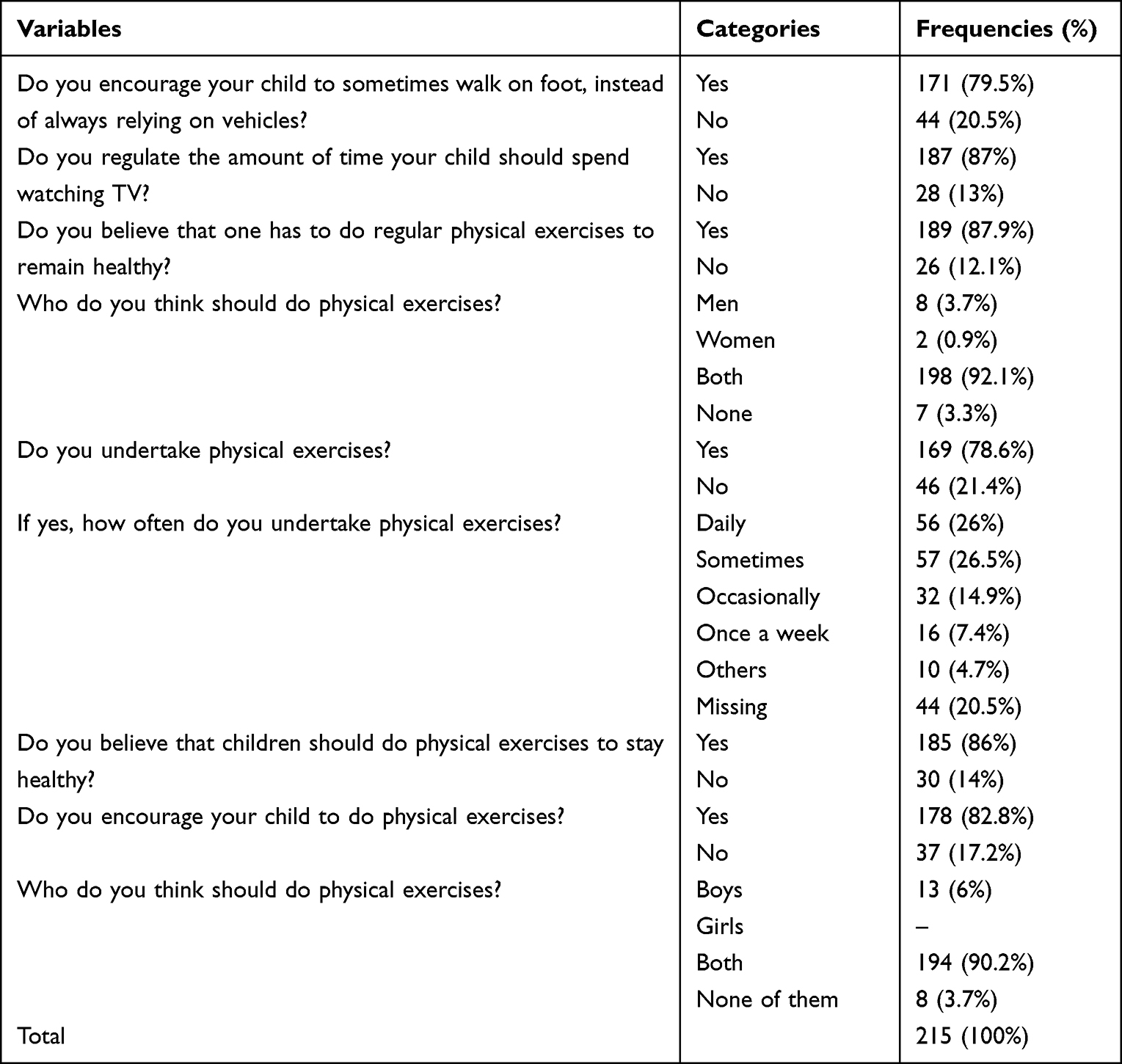 |
Table 5 Perceptions and Experiences About Children’s Physical Exercises |
Factors Associated with Body Size Preferences
Table 6 presents the results of multinomial regression analysis conducted to explain the association between children’s body size preferences of parents and their socio-demographic characteristics. Accordingly, it was found that parents’ preference of voluptuous body size of children is significantly associated with age (OR=61.52.448, P < 0.001, 95%C.I: 57–66.14), educational status of parents (OR = 35.605, P < 0.001; 95%C.I: 6.050–209.524), sex (OR = 0.237, P < 0.05; 95%C.I: 0.078-0.724) and grownup area (OR = 2.869, P < 0.05; 95%C.I: 1.062–7.749). In other words, the older the parents get, the better they are educated, being female (mother), and they grew up in an urban area, the more likely they are to prefer voluptuous body size of a child than preferring an average body size of a child. For instance, it is indicated that older parents prefer voluptuous body size of a child 15.632 times greater than preferring an average body size of a child. In addition, parents’ preference of very voluptuous body size of a child is significantly associated with educational status (OR = 5.331, P < 0.05; 95%C.I:1.052–6.487) and residential background of parents (OR = 2.613, P < 0.05; 95%C.I: 1.052–6.487) implying that parents that are better educated and those that have grown up in an urban area prefer very large body size of a child than an average body size.
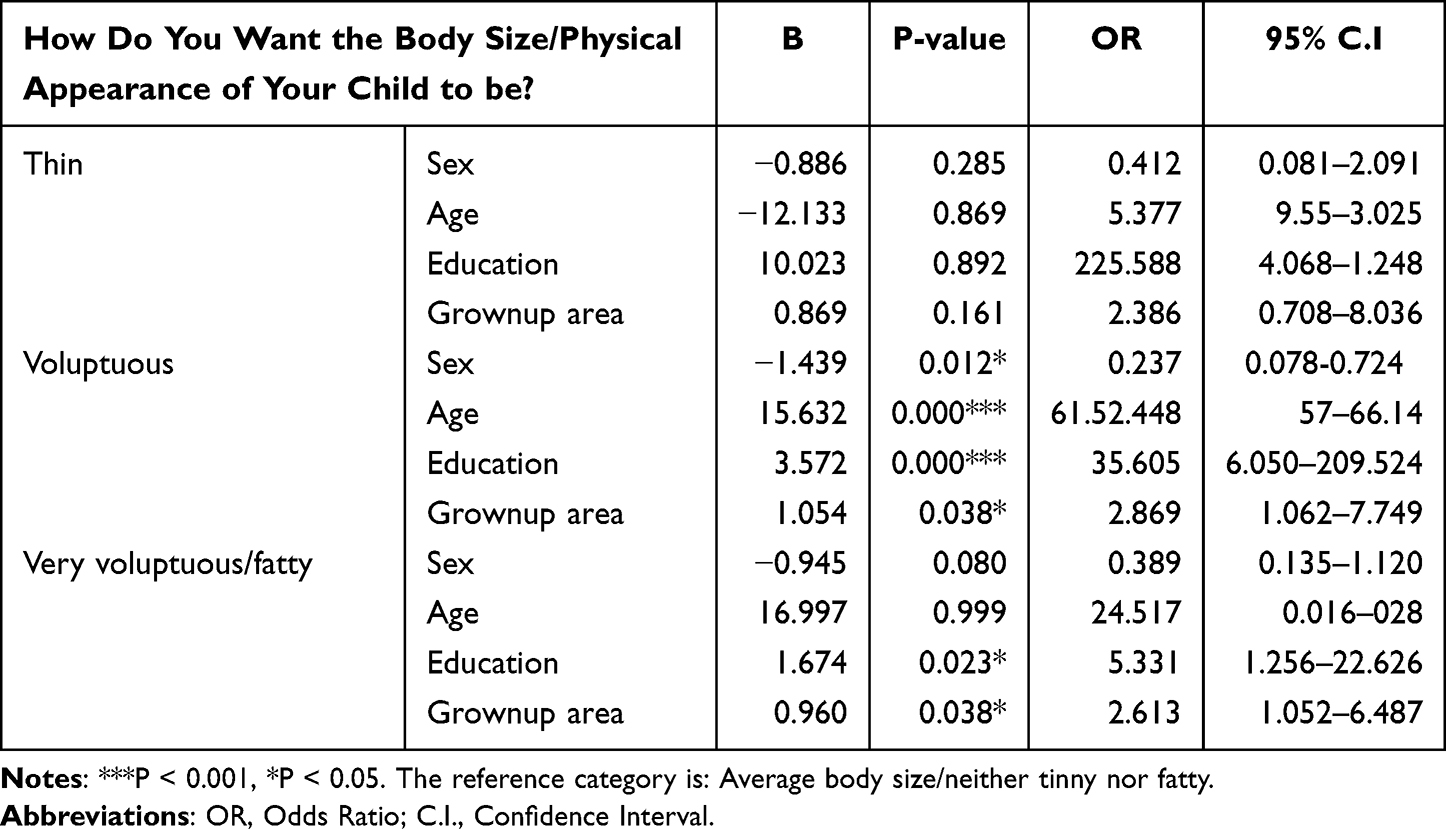 |
Table 6 Multinomial Regression Regarding Association Between Child’s Body Size Preferences of Parents and Socio-Demographic Characteristics |
Discussion
Until the onset of adolescence on which the major socializing agents would be peer groups and the media, parents play paramount role in terms of governing children’s body weight either by practicing appropriate feeding habits at home to be examples or by controlling their children’s food choices, exercise, and TV watching time.22 According to Gillison et al23 most parents do not feel happy when commented about the overweight status of their children mainly due to the belief that being overweight is important for the health of their children, interpretations of the comments as criticisms of one’s parenting style, or fearing that discussing about the issue may jeopardize the food consumption of their children. In a study undertaken in rural Northeastern North Carolina by Terry13 it was found that parents attributed the obesity situations of their children to the lack of affordable resources though they acknowledge childhood obesity as pathological that needs to be combated. The fact that most parents do not comply with weight management practices aimed at maintaining a normal body weight of children is exacerbated by their failure to recognize the obesity problem of their children.24 With this in mind, we have examined the perceptions and practices related to childhood obesity among parents in Southern Ethiopia. After gathering quantitative data from selected parents, we have analyzed it using descriptive and inferential statistical techniques.
The results of the present study indicated that most respondents want their child’s body size to be neither fat nor thin. It was also found that majority of the respondents are highly concerned with the situation that their child is getting overweight or obese. Moreover, most of the study participants held the opinion that average body size – neither fatty nor tinny – is an indication of good health status. These and other findings of our study would demonstrate that parents in the study area have a good level of awareness and held perceptions that can positively affect the health status of their children. This finding, nevertheless, is not consistent with the findings of most other researches previously undertaken on relevant topics in other areas of the world. For instance, according to Caamano et al25 over weight was socially accepted when it occurred in children and in married woman, mainly because it is a symbol of the good life that the head of the household provides. In addition, Naigaga et al26 also found a preference of large and overweight body size among Saharawi refugees. Moreover, the results of a study conducted among rural and urban Ghanaian adults by Agyapong et al27 revealed that study participants associate overweight with wealth and childbirth and attributed their current weight to hereditary and childbirth. Furthermore, Hashim et al28 found that most of the parents participated in their study preferred their child to be overweight and perceived that overweight and obese children can remain healthy. Above all, the findings of Brouwer29 revealed that parents believed the weight and body size of children is genetically predetermined and hence people should not bother about weight as long as a child remains healthy and active. The variation in the findings between our study and other previous researches might be attributed to differences in the socio-demographic characteristics of our survey population from which samples were generated. For instance, looking into the data, one would understand that respondents participated in our study had educational status that can be labeled from moderate to high level of achievement. In addition, the fact that our samples had an urban residential background and that urbanism is one way or the other related to better exposure to health information and access to education might have also contributed for the differences. On the other hand, the finding that parents in our study have better awareness about the fact that overweight and health status are negatively related is consistent with few studies previously undertaken by other authors. For instance, studies conducted by Allison et al.30 Akhtar-Danesh et al31 and Hashim et al28 found high awareness among parents regarding the fact that obesity can cause serious illness.
Although children are naturally predisposed to tasty foods and would like to avoid bitter ones, they are also equally responsive to parental control and the imposition in food choices and meal time patterns.32 Because the home environment plays a key role in influencing children’s food intake habits, parents can contribute in this regard by advising and encouraging the family members to eat certain types of food or by exposing them to the types of food items deemed healthy.33 In the present study, we found that the common patterns of serving meals to children has been three times a day (breakfast, lunch, and dinner – a food consumption pattern that is common to most people in Ethiopia) for most respondents, followed by no limits or serving as needed by the child, and four times a day. Moreover, majority of participants reported that they regulate the food consumption practices of their children. In addition, most respondents revealed that they control the amount of food their child consumes with the aim of preventing obesity/overweight. It is important to note that parents’ tendency of managing the feeding and physical exercise experiences of their children heavily relies on the value system surrounding their beliefs and practices regarding body size in general and children’s body weight in particular.29 Champion et al34 revealed that only very few mothers agreed in the importance of keeping their child happy than ensuring that their child ate healthy food. According to kromker et al35 parents’ lack of successful weight management strategies is more clearly associated with their children’s weight status than with lack awareness.
In this study, it is found that most of the respondents encourage their children to sometimes walk on foot, instead of always relying on vehicles. In addition, majority of them replied that they regulate the amount of time their children spend watching TV. Such promising experiences in terms of regulating both the food consumption and physical exercise patterns of children among our study participants might be linked not only to the positive perception most of them held towards both the need to control food consumption and physical exercises, but also that they themselves reportedly engaged in both endeavors which could have helped them to obtain certain experiential benefits. In a family-based randomized controlled weight control studies, Wrotnaik et al36 found that a weight loss of parents leads to weight loss of their children in which youth were found to benefit the most from parents who lose the most weight. Therefore, instead of focusing on the child alone, interventions aimed at improving the problem of child obesity at societal level should be developed at family-level because improvements underlying family life style will have positive influence on childhood obesity.37 It implies that for intervention efforts that aim to control the problem of child obesity to become successful in helping healthful practices both in and outside the home, it is necessary that they should involve working directly with families starting from the earliest stage of child development.32,36,37 Kromker et al35 found that parents’ level of self-efficacy for exercising and perceived benefits of healthy eating were negatively related to the weight status of their children, with self-efficacy for exercising being more strongly associated.
Results of a multinomial logistic regression analysis in our study have shown that parents’ preference of voluptuous body size of children is significantly associated with age, educational status of parents, sex, and grownup area. In addition, parents’ preference of very voluptuous body size of a child is significantly associated with educational status and residential background of parents implying that parents that are better educated and those that have grown up in an urban area prefer very large body size of a child than an average body size. The result of a systematic review of literatures on parental perceptions of childhood obesity by Aldolaim38 shows that parental perceptions of children’s weight is influenced by the belief about childhood obesity, parental weight status, and parental level of education. Moreover, Baughcum et al39 found that mothers believed a heavy infant was a healthier infant and they perceived that the possession of such heavy body weight of a child indicates an effective feeding practices and better parenting styles. Above all, Champion et al34 found that mothers who agreed or strongly agreed that children have unalterable food preferences were less likely than other mothers to have children who were overweight or obese.
Limitations
Our study has no many limitations. Of course, as most researches are not without gaps, one limitation we identified is methodological constraints. Obviously, studies pertaining to perceptions and beliefs about a certain health behavior can better address the intended objectives when supported by qualitative data, as it has been done by most previous studies conducted on related topics. In this research, nevertheless, we have solely relied on quantitative data which could have potentially affected the depth of the research. In addition, though the samples were selected based on the rules of probability sampling and hence, not done purposively, the socio-demographic profile of our research participants reveals that our observation units have educational status that ranges from primary level to Master’s degree and above. Perhaps, that could have resulted from the fact that respondents provided socially desirable responses. But, assuming that it is true, the study faced a fatal consequence of sampling bias which has a possibility of affecting the data. Therefore, future researches can better benefit from triangulating data using a mixed method. Above all, further studies that compare urban-rural dynamics of health behavior and health belief systems should also be undertaken to substantiate on the findings of the present study.
Conclusion
In this study, we have assessed knowledge and perceptions of parents about childhood obesity including practices related to regulating feeding and physical exercise patterns of their children. Accordingly, the results indicated that parents not only have adequate level of awareness regarding the health risks of children’s heavy body weight but also engage in the body weight management practices of their children such as by regulating the food consumption patterns of children, encouraging them to undertake physical exercises, and most importantly by being role models while doing physical exercises for themselves. We have noted not only that parents prefer an average body size of children but also there is a widely held assumption that children’s body condition of being neither overweight nor underweight results both physical strength and better health status. Therefore, the cultural value of considering large body size of a child as a socially accepted physical morphology of children and the belief that voluptuous body size is a sign of good health status is lacking among parents in the study area.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study was evaluated and approved by the Ethics Approval Committee of Wolaita Sodo University (WSU-HSC/1528/14). Research participants were first informed about the purpose of the research, including what role is expected from their side. Both verbal and written consents were gained from all research participants. In addition, a formal letter was obtained from college of social science and humanities of Wolaita Sodo University. This study was conducted in accordance with the Declaration of Helsinki.
Disclosure
The authors declare that there is no conflicts of interest.
References
1. Dagne S, Assefa Y, Abebe Z, Mesele M. Factors associated with overweight and obesity among adults in northeast Ethiopia: a cross-sectional study. Diabetes Metab Syndr Obes. 2019;12:391–399.
2. Wakayo T, Whiting S, Belachew T. Vitamin D deficiency is associated with overweight and/or obesity among schoolchildren in central Ethiopia: a cross-sectional study. Nutrients. 2016;8:190. doi:10.3390/nu8040190
3. Yosef T, Bogale B, Destaw A, Weldu A. The burden of overweight and obesity among long-distance truckers in Ethiopia. J Obesity. 2020;2020. doi:10.1155/2020/4242789
4. Mengesha A, Abate B, Kassaw M. Prevalence of overweight/obesity among the adult population in Ethiopia: a systematic review and meta-analysis. BMJ open. 2020;10:e039200.
5. Ritchie H, Roser M. Retrieved August 30, 2021, from obesity; 2017. Available from: https://ourworldindata.org/obesity.
6. Mekonnen T, Animaw W, Seyum Y. Overweight/obesity among adults in North Western Ethiopia: a community-based cross sectional study. Arch Public Health. 2018;76. doi:10.1186/s13690-018-0262-8
7. Fitsum K, Egata G, Demena M, Gebremichael B. Overweight/obesity and associated factors among second cycle primary school children in Kirkos Sub-City, Addis Ababa, Ethiopia. Glob Adv Health Med. 2021;10:21649561211017883. doi:10.1177/21649561211017883
8. Desalew A, Mandesh A, Semahegn A. Childhood overweight, obesity and associated factors among primary school children in Dire Dawa, eastern Ethiopia; a cross-sectional study. BMC Obes. 2017;4:20. doi:10.1186/s40608-017-0156-2
9. Gali N, Tamiru D, Tamrat M. The emerging nutritional problems of school adolescents: overweight/obesity and associated factors in Jimma Town, Ethiopia. J Pediatr Nurs. 2017;35:98–104. PMID: 28728777. doi:10.1016/j.pedn.2017.03.002
10. Gebrie A, Alebel A, Zegeye A, Tesfaye B, Ferede A. Prevalence and associated factors of overweight/ obesity among children and adolescents in Ethiopia: a systematic review and meta-analysis. BMc Obseity. 2018;5:1–12.
11. Caprio S, Daniels S, Drewnowski A, et al. Influence of race, ethnicity, and culture on childhood obesity: implications for prevention and treatment. Obesity Soc. 2012;16(12). doi:10.1038/oby.2008.398
12. Lee K, Arriola-Sanchez L, Lumeng J, Gearhardt A, Tomiyama J. Weight stigma by association among parents of children with obesity: a randomized trial. Acad Pediatr. 2021;22:754–760. doi:10.1016/j.acap.2021.09.019
13. Terry C. Parental perceptions of childhood overweight and obesity in four-year-olds in Northeastern North Carolina. Dissertation Submitted in Partial Fulfillment of the Requirements for the Degree of Doctor of Philosophy Public Health, Walden University; 2016.
14. Ang YN, Wee BS, Poh BK, Ismail MN. Multifactorial influences of childhood obesity. Curr Obes Rep. 2013;2:10–22. doi:10.1007/s13679-012-0042-7
15. Jeor S, Chaney SP, Sigman-Grant M, Williams C, Foreyt J. Family-based interventions for the treatment of childhood obesity. J Acad Nutr Diet. 2002;102(5):640–644.
16. Yazeedi B, Berry D, Crandell J, Waly M. Family influence on children’s nutrition and physical activity patterns in Oman. J Pediatr Nurs. 2020;56:E42–E48. doi:10.1016/j.pedn.2020.07.012
17. Ezo E, Gashawbeza B. Determinants of overweight among primary school children in Arba Minch Town, Southern Ethiopia, 2021. Adolesc Health Med Ther. 2021;12:99–110. doi:10.2147/AHMT.S339671
18. Tadesse Y, Derso T, Alene KA, et al. Prevalence and factors associated with overweight and obesity among private kindergarten school children in Bahirdar Town, Northwest Ethiopia: cross-sectional study. BMC Res Notes. 2017;10. doi:10.1186/s13104-016-2308-8
19. Sorrie MB, Yesuf ME, GebreMichael TG. Overweight/Obesity and associated factors among preschool children in Gondar City, Northwest Ethiopia: a cross-sectional study. PLoS One. 2017;12(8):e0182511. doi:10.1371/journal.pone.0182511
20. Anteneh ZA, Gedefaw M, Tekletsadek KN, Tsegaye M, Alemu D. Risk factors of overweight and obesity among high school students in Bahir Dar City, North West Ethiopia: school based cross-sectional study. Adv Prev Med. 2015;2015:294902. PMID: 26697231; PMCID: PMC4678054. doi:10.1155/2015/294902
21. Alemu E, Atnafu A, Yitayal M, Yimam K. Prevalence of overweight and/or obesity and associated factors among high school adolescents in Arada Sub city, Addis Ababa, Ethiopia. J Nutr Food Sci. 2014;4:2. doi:10.4172/2155-9600.1000261
22. Berry EM. He Obesity pandemic—whose responsibility? No blame, no shame, not more of the same. Front Nutr. 2020;7:2. doi:10.3389/fnut.2020.00002
23. Gillison F, Beck F, Lewitt J. Exploring the basis for parents’ negative reactions to being informed that their child is overweight. Public Health Nutr. 2013;17(5):987–997. doi:10.1017/S1368980013002425
24. Alexander S, Baur L. Childhood obesity: who’s to blame and who should pay? Expert Rev Pharmacoecon Outcomes Res. 2007;7(2):95–98. doi:10.1586/14737167.7.2.95
25. Caamaño MC, Ronquillo D, Kimoto R, et al. Beliefs and motives related to eating and body size: a comparison of high-BMI and normal-weight young adult women from rural and urban areas in Mexico. BMC Public Health. 2016;16:1014. doi:10.1186/s12889-016-3695-4
26. Naigaga DA, Jahanlu D, Claudius HM, Gjerlaug AK, Barikmo I, Henjum S. Body size perceptions and preferences favor overweight in adult Saharawi refugees. Nutr J. 2018;17(1):17. doi:10.1186/s12937-018-0330-5
27. Agyapong N, Annan R, Apprey C, Aduku L. Body weight, obesity perception, and actions to achieve desired weight among rural and urban Ghanaian adults. J Obes. 2020;2020:1–8. doi:10.1155/2020/7103251
28. Hashim MS, Abaid SS, Al-Saadi AM, Abutiheen AA. Perceptions and attitudes of parents towards overweight and obesity among their preschool-aged children in Karbala. J Med. 2020;13(1):2326–2334.
29. Brouwer B “She is active, eats well – i am not worried”- a qualitative study of parental challenges to managing childhood weight based on online parenting discussion forums. Master Degree Project in International Health, Uppsala University; 2017. Available from: https://www.diva-portal.org/smash/get/diva2:1112113/FULLTEXT01.pdf.
30. Sylvetsky-Meni AC, Gillepsie SE, Hardy T, Welsh JA. The impact of parents’ categorization of their own weight and their child’s weight on healthy lifestyle promoting beliefs and practices. J Obes. 2015;2015:7. doi:10.1155/2015/307381
31. Akhtar-Danesh N, Dehghan M, Morrison K, Fonseka S. Parents’ perceptions and attitudes on childhood obesity: a Q-methodology study. J Am Acad Nurse Pract. 2011;23(2):67–75. doi:10.1111/j.1745-7599.2010.00584.x
32. Lindsay AC, Sussner KM, Kim J, Gortmaker S. The role of parents in preventing childhood obesity. Future Child. 2006;16(1):169–186. doi:10.1353/foc.2006.0006
33. Golan M, Crow S. Targeting parents Exclusively in the treatment of childhood obesity: long-term results. Obes Res. 2004;12:357–361. doi:10.1038/oby.2004.45
34. Champion SL. Social Determinants of Childhood Overweight and Obesity in South Australian Families: Parenting, Work Patterns and Gender Roles. Unpublished thesis submitted in fulfillment of the requirements for the degree of doctor of philosophy. Australia: The University of Adelaide; 2013.
35. kromker D, Stolberg A, Muller C, Tian Z, Parlesak A. Is adolescent body weight associated with parental beliefs about overweight, attitudes towards food, and the home environment? J Food Res. 2015;4(2):104–118. doi:10.5539/jfr.v4n2p104
36. Wrotnaik BH, Epstein LH, Paluch RA, Roemmich JN. Parent weight change as a predictor of child weight change in family-based behavioral obesity treatment. Arch Pediatr Adolesc Med. 2004;158:342–347. doi:10.1001/archpedi.158.4.342
37. Gray LA, Hernandez Alava M, Kelly MP, Campbell MJ. Family lifestyle dynamics and childhood obesity: evidence from the millennium cohort study. BMC Public Health. 2018;18(1):500. doi:10.1186/s12889-018-5398-5
38. Aldolaim S. Parental perceptions of childhood obesity: systematic literature review. J Child Obes. 2019;4(1):70.
39. Baughcum A, Burklow K, Deeks C, Powers S, Whitaker C. Maternal feeding practices and childhood obesity: a focus group study of low-income mothers. Arch Pediatr Adolesc Med. 1998;152:1010–1014. doi:10.1001/archpedi.152.10.1010
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.