Back to Journals » International Journal of General Medicine » Volume 16
Behavioral Responses for Face Cleanliness Message to Prevent Trachoma Among Mothers Having Children Age 1–9 Years Old, in Fogera District, Northwest Ethiopia: An Application of Extended Parallel Process Model
Authors Muche N, Wasihun Y ![]() , Wondiye H
, Wondiye H ![]() , Bogale EK
, Bogale EK ![]() , Anagaw TF
, Anagaw TF ![]()
Received 10 April 2023
Accepted for publication 12 May 2023
Published 19 May 2023 Volume 2023:16 Pages 1927—1941
DOI https://doi.org/10.2147/IJGM.S412380
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Mihajlo Jakovljevic
Natnael Muche, Yosef Wasihun, Habtamu Wondiye, Eyob Ketema Bogale, Tadele Fentabil Anagaw
Department of Health Promotion and Behavioural science, school of Public Health College of Medicine and Health Science, Bahir Dar University, Bahir Dar, Ethiopia
Correspondence: Tadele Fentabil Anagaw, PO.BOX. 079, Tel +251-927692916, Email [email protected]
Background: Trachoma is an eye disease caused by bacteria called Chlamydia trachomatis. This infection causes papillary and/or follicular inflammation of the tarsal conjunctiva referred to as active trachoma. Active trachoma prevalence among 1 to 9 years old children is 27.2% in Fogera district (study area). Many people still require the implementation of the face cleanliness components of the SAFE strategy. Even if face cleanness is an important component to prevent trachoma, there is limited research done on this area. Therefore, the purpose of this study is to assess behavioral responses to face cleanliness messages to prevent trachoma among mothers having children aged 1 to 9 years old.
Methods: A community-based cross-sectional study was conducted with the guidance of an extended parallel process model in Fogera District from December 01 to December 30, 2022. A multi-stage sampling technique was used to select 611 study participants. Interviewer administered questionnaire was used to collect the data. Bivariable and multivariable logistic regression analysis was done to identify predictors of behavioral responses using SPSS V.23 significant variables were declared by AOR at a 95% confidence interval and a p-value < 0.05.
Result: Among the total participants, 292 (47.8%) were in danger control. Residence [AOR = 2.91; 95% CI: (1.44– 3.86)], marital status [AOR = 0.79; 95% CI: (0.667– 0.939)], level of education [AOR = 2.74; 95% CI: (1.546– 3.65)], family size [AOR = 0.57; 95% CI: (0.453– 0.867)], round trip to collect water [AOR = 0.79; 95% CI: (0.423– 0.878)], having information about face washing [AOR = 3.79; 95% CI: (2.661– 5.952)], Source of an information health facility [AOR = 2.76; 95% CI: (1.645– 4.965)], school [AOR = 3.68; 95% CI: (1.648– 7.530)], health extension workers [AOR = 3.96; 95% CI: (2.928– 6.752)], Women development army [AOR = 2.809; 95% CI: (1.681– 4.962)], knowledge [AOR = 2.065; 95% CI: (1.325– 4.427)] self-esteem [AOR = 1.013; 95% CI: (1.001– 1.025)], self-control [AOR = 1.132; 95%CI: (1.04– 1.24)], and future orientation [AOR = 2.16; 95% CI: (1.345– 4.524)] were found to be statistically significant predictors of behavioral response.
Conclusion: Less than half of the participants were in the danger control response. Residence, marital status, level of education, family size, face-washing information, source of information, knowledge, self-esteem, self-control, and future orientation were independent predictors of face cleanliness. Strategies of face cleanliness messages should give high attention to perceived efficacy with consideration of perceived threat.
Keywords: trachoma, face cleanliness, behavioral response, extended parallel process model
Introduction
Trachoma is an eye disease caused by bacteria called chlamydia trachomatis. This infection causes papillary and/or follicular inflammation of the tarsal conjunctiva, which is referred to as active trachoma. Active trachoma is subdivided into trachomatous inflammation—follicular (TF) and trachomatous inflammation—intense (TI).1
Recurrent infections of the conjunctiva lead to the development of scar tissue within the conjunctiva. Because of the contraction of the scar tissue, the eyelid is turned inward allowing the eyelashes to rub against and eventually abrade the cornea (trachomatous trichiasis), eventually leading to corneal opacity and blindness. Globally, trachoma is the leading cause of blindness, affecting people who lack access to clean water, sanitation, and adequate health care.2
In 1998, World Health Organization (WHO) set an objective to eliminate trachoma as a blinding disease by the year 20203 and endorsed the implementation of the SAFE strategy (Surgery to correct trichiasis, Antibiotics to treat active infection, Facial cleanliness to prevent the transmission of bacteria and Environmental improvement by increasing use of latrines and access to safe water).4,5
In practice, trachoma control programs largely focus on medical surgery and antibiotics interventions,6 whereas, face cleanliness and environmental improvement are poorly defined interventions. The predominant goal of face cleanliness and environmental improvement interventions is to break chlamydia trachomatis transmission.7 A clean face could be defined as an absence of ocular and dry nasal discharge that is a good predictor of whether the face has been washed.8
The ministry of health (MOH) Ethiopia recognized the burden of Neglected Tropical Diseases (NTDs) and developed a strategic plan for the period of 2021–2025 by prioritizing 12 diseases, where trachoma is put at the first line in the Amhara region. Behaviour change communication is the sole eradication and elimination strategy.9 Ministry of Health Targets 798 woreda for facial cleanliness interventions like face cleanliness assessments, face washing demonstrations at the HHs level and face cleanliness lessons at primary schools to eliminate trachoma.10
Trachoma control programs rely on health extension workers, community volunteers, primary school teachers, religious leaders, local government authorities, and local media to promote healthy behaviours that prevent trachoma.11
Models support describes the process of change that individuals go through those changes as they exchange information interpret and respond to different messages. The Extended Parallel Process Model (EPPM) is preferred as the model explains why fear appeals fail, incorporates fear as a central variable, and specifies the relationship between threat and efficacy in prepositional forms. Generally, it consolidates other theories by arguing that fear leads to message rejection or acceptance. Threat determines the degree or intensity of the responses, while efficacy determines the nature of responses.12 In this study, the Extended Parallel Processing Model (EPPM) was used as a guiding framework. EPPM is a communication model focusing on fear arousal and efficacy messages to activate and direct desirable behavioral responses to initiate behavioral change.13,14 The EPPM builds on the concept of perceived health threat (a combination of subjective perception of severity and susceptibility) and overall efficacy (a combination of perceived response efficacy and self-efficacy) that lead to message acceptance and, ultimately, desired behaviour changes in the population.15,16
The Extended Parallel Processing Model describes how rational considerations (efficacy beliefs) and emotional reactions (fear of a health threat) combine to determine behavioral decisions. Perceived susceptibility and Perceived severity are key variables related to beliefs about the threat and the other two Response efficacy and Self-efficacy are key variables related to beliefs about efficacy.17
The people must perceive that trachoma is severe and should think they are susceptible to Trachoma.17 Besides, they have to believe that the recommended preventive practice is effective in controlling Trachoma and believe that they can perform it to avert the spread of the disease. When perceptions of a threat are strong and perceived levels of efficacy are high, the model predicts self-protective behaviour. When perceptions of a threat are strong, but perceived levels of efficacy are low, the model predicts maladaptive denial or rejection of protective behaviours.13 With this context, this study will conduct to assess the behavioral response to face cleanliness messages to trachoma prevention and identify predictors of behavioral response among mothers of 1–9 years old children.
Globally, 2.2 billion people are living with vision impairment or blindness, of whom at least 1 billion have a vision impairment that could have been prevented.18 Trachoma is a public health problem in 44 countries or 136 million people around the world and is responsible for the blindness or visual impairment of about 1.9 million people. It causes about 1.4% of all blindness worldwide and yet, blindness from trachoma is irreversible.19 In recent estimates, the active disease affects about 84 million people, more than 10 million people have trichiasis, and 7.6 million people have been blinded.19 The cost of disability and potential loss in productivity alone has been estimated to be more than $2 billion per year.2
In Ethiopia, women are approximately three times more likely than men to be blinded by trachoma.20 Therefore, women are vulnerable to trachoma infection, as they are often the primary caregivers of children, and children are the primary victim of the problem.21 Active trachoma is common among children age 1 to 9 years old.22 Ethiopia has the highest burden of trachoma in the world. Even though elimination was expected, the average prevalence of trachoma among children age 1 to 9 years decreased from 26.6% in 2015 to 13.3% in 2020. As of December 2020, 798 Districts were endemic for trachoma, with about342800people with TT, and 72 million people living in 798 woreda where the prevalence of follicular trachoma in children aged 1–9 years was ≥5%. Thus, many people still require the implementation of the face cleanliness components of the SAFE strategy.10
A study has shown that active inflammatory trachoma is more common in children with unclean faces than in children with clean faces Facial cleanliness is part of the multi-pronged approach known as the SAFE strategy to eliminate trachoma.5 Studies have demonstrated the trachoma-protective effect of keeping children’s faces free of ocular and nasal secretions.23 Washing faces as often as needed is a crucial way to keep faces clean; current educational programs focus on the importance of face washing.24
Children harbour the bacteria that cause trachoma, and, while caring for them, women are exposed to infection more frequently than men.20 The trachoma program began in Amhara in 2001 in four districts of South Gondar and expanded to cover 19 districts in 2003. Following the 2007 Zonal-level baseline survey, SAFE interventions were gradually scaled up to all 152 districts between 2007 and 2010.25
The study was conducted in Fogera trachoma endemic district. Implementation of the full SAFE strategy for trachoma control in the districts started in 2003 based on trachoma prevalence survey that had identified trachoma as being a serious public health problem in the district. SAFE interventions were conducted following standards advocated by the WHO and included trachoma health education, promotion of facial hygiene, promotion of pit latrines, and advocacy for water provision. All communities within the program district were offered district-wide interventions with facial cleanliness.26
Even though the fight against Trachoma began in the South Gondar zone and prevention intervention has been implemented for the last 22 years, Fogera district remained endemic with a prevalence of TF 27.2% and TT 1.83% which is endemic and above the elimination threshold of WHO (TF <5% and TT <0.01% from the general population).27 The observational study has demonstrated and revealed an association between poor facial cleanliness, including the presence of flies on a child’s face, and trachoma.28 It is possible that improvements in hygiene, and especially facial cleanliness, will alter the transmission dynamics of trachoma and create favourable conditions to trachoma prevention and elimination.
Twenty-two years of intervention and unimproved prevalence and reduction of the infection in the study district motivated the researcher to know the level of behavioral response and the predictors of the response, for facial cleanliness messages in mothers of 1 to 9 years old children. To the knowledge of the researcher, there is no study done on behavioral responses to facial cleanliness messages since the face-washing component of the SAFE strategy aims to maintain clean faces in the community to reduce eye-seeking flies and person-to-person transmission of the trachoma organism.29 The face cleanliness component of SAFE strategies relies on human behaviour and the behaviour change of mothers is important to eliminate trachoma as a public health problem.30
Therefore, this study aimed to assess the behavioral responses to face cleanliness messages to prevent trachoma and its predictors among mothers of children 1–9 years of age with the guidance of EPPM to fill the aforementioned gap.
Methods and Materials
Study Area and Period
The study was conducted in the Fogera district, which is identified as one of the trachoma-endemic Districts in the South Gondar political administration. Fogera District is located at 625 km in the Northwest direction of Addis Ababa, the capital city of Ethiopia, where it is 60 km from Bahir Dar, the capital city of Amhara National Regional State. In Fogera, there are 9 government health center and 44 health posts. The District has 32 kebeles where 30 are rural and 2 are urban Kebeles (smallest unit of administration) with a 250,525 total population and 58,262 total households based on the District basic profile of 2022.31 Fogera District is implementing a school trachoma program in all 103 elementary schools and has a TT Surgery backlog of 1567 (8.5% of Zonal backlog) and could not maintain the elimination threshold after the implementation of the full SAFE strategy for two decades. This study was conducted from December 01 to December 30, 2022.
Study Design
Community-based cross-sectional study design was applied.
Source Population
All mothers having children age 1–9 years old in Fogera District.
Study Population
All selected mothers having children aged 1–9 years old in selected kebeles of Fogera District.
Inclusion Criteria
Mothers who had children age 1–9 years old and who were living in the kebele for at least six months during the data collection period were included in the study.
Variables of the Study
Dependent Variables
Behavioral Response (Danger Control and Fear Control).
Independent Variables
The independent variables include socio-demographic factors (age, marital status, family income, religion, occupation, residence), Knowledge, Self-esteem, Self-control, Future orientation, and Sources of information.
Operational Definition
Knowledge
The knowledge of the mothers was assessed by 13 knowledge questions. For each question, the participants were given three choices: yes, no and I do not know’. The yes item was given 1 value unlike the no and I don’t know items that were given 0 value. It had a minimum value of 5 and a maximum value of 13. A higher score indicates higher knowledge.
Self-Esteem
Self-esteem was mothers’ overall sense of self-worth or personal value.32 Self-esteem was measured by 5 points Likert scale from (strongly disagree - strongly agree). After the negatively worded statements of the questionnaire were reversely coded, the score was summed for each respondent. It had a minimum value of five and a maximum value of 19. A higher score indicates higher self-esteem. The overall scores of each individual were used to get its mean score.
Self-Control
Self-control was the ability of mothers to regulate their emotions, thoughts, and behaviour in the face of temptations and impulses.33 Self-control was measured by 5 points Likert scale that ranged from (strongly disagree - strongly agree). After reverse coding the negatively worded statements, the score was summed for each respondent. It had a minimum value of 6 and a maximum value of 20. A higher score indicates higher self-control. The overall scores of each individual were used to get its mean score.
Future Orientation
The extents to which mothers think about the future, anticipate future consequences, and plan before acting.34 Future orientation was measured by 5 points Likert scale that ranged from (strongly disagree – strongly agree). After reverse coding the negatively worded statements, the score was summed for each respondent. It had a minimum value of 3 and a maximum value of 15. A higher score indicates higher future orientation. The overall scores of each individual were used to get its mean score.
Perceived Severity
Perceived severity was a belief about the severity or seriousness of trachoma on one’s state of health affairs. It was measured by 5 points Likert scale (from strongly disagree - strongly agree). Since there was no negatively worded statement, the score was summed for each respondent. It had a minimum value of four and a maximum value of 15. A higher score indicates higher perceived severity. The overall scores of each individual were used to get its mean score.
Perceived Susceptibility
Perceived susceptibility was a belief of mothers’ self-perception of vulnerability to trachoma. It was measured by 5 points Likert scale (from strongly disagree - strongly agree). After reverse coding the negatively worded statements, the score was summed for each respondent. It had a minimum value of 4 and a maximum value of 15. A higher score indicates higher perceived susceptibility. The overall scores of each individual were used to get its mean score.
Self- Efficacy
A belief in one’s capability to do face washing to avert a threat.30 It will be measured by 5 points Likert scale (from strongly disagree - strongly agree). After reverse coding the negatively worded statements, the score was summed for each respondent. It had a minimum value of 4 and a maximum value of 15. A higher score indicates higher self-efficacy. The overall scores of each individual were used to get its mean score.
Response Efficacy
Response efficacy was an acceptance (beliefs) of the effectiveness of face cleanliness in decreasing the risk of trachoma. It was measured using 5 points Likert scale (from strongly disagree - strongly agree). Since there was no negatively worded statement, the score was summed for each respondent. It had a minimum value of 5 and a maximum value of 15. A higher score indicates higher response efficacy. The overall scores of each individual were used to get its mean score.
Perceived Threat
Perceived threat was a collective perceived threat and was measured by gaining the sum of both perceived severity and perceived susceptibility for each respondent. It had a minimum value of 10 and a maximum value of 29. A higher score indicates a higher perceived threat. The overall scores of each individual were used to get its mean score.
Perceived Efficacy
Perceived efficacy was a collective perceived efficacy and was measured by gaining the sum of both self-efficacy and response efficacy for each respondent. It had a minimum value of 11 and a maximum value of 28. A higher score indicates higher perceived efficacy. The overall scores of each individual were used to get its mean score.
Danger Control Response
Danger control response was an intended behavioral response when mothers of 1–9 children believed that their children were at risk for health risk that was trachoma (high perceived threat) and they believe they were able to effectively avert it from occurring (high perceived efficacy), they were motivated to control the danger or threat. It was a positive score obtained by subtracting the perceived threat score from the perceived efficacy score.
Fear Control Response
Fear control response was an unintended behavioral response when mothers of 1–9 children believed that they were at risk for a serious or significant threat.30 High perceived threat, but they believed that they were unable to perform the recommended response or they believed that the recommended response to be ineffective (low perceived efficacy), then they focused on controlling their fear about the treat. It was the negative score for fear control and a zero score for no response was obtained by subtracting the perceived threat score from the perceived efficacy score.35
Sample Size Determination
The sample size was calculated using a single population proportion formula. The assumptions used for sample size calculation were:
d = the margin of error between the sample statistics and the population parameter (=0.05)
Z α /2 = critical value at 95% confidence of certainty (=1.96)
P = 50% of the proportion (P) of the Danger control process (because there was no related research done related to this topic to the understanding of the principal investigator) = 0.5
q=1-p=(0.5)=384
The final sample size after considering the design effect of 1.5 and a 10% contingency of non-response rate was 634 mothers.
Sampling Techniques and Procedures
A multi-stage sampling technique was used to select study households (HHs). Fogera District was randomly selected among similar districts with similar endemic prevalence in South Gondar Zone. Fogera District has 32 (30 rural and 2 urban) kebeles. In the first stage, 10 Kebeles were selected from 32 Kebeles using a lottery method by considering the rule of thumb of 30% coverage of representative of the study population. 1 Kebele from urban and 9 kebeles from rural were selected to ensure representativeness. Systematic random sampling techniques were used to select 634 households. The number of HHs from each Kebele was determined proportionally. The total number of the study population was 7185 from the source population. Based on the number of the study population and sample size required from each Kebele, the interval between the HHs was calculated which was 11. Then, the first HH was selected by lottery method from 1 to 11 serial numbers of the sampling frame. Then, after getting the 1st sample separately for each Kebele, the remaining mothers were selected at each 11th interval to get a total of 634 study participants. Only one mother of the youngest child was selected as a study sample from each HH. In the case of non-response after the repeated visit (two times), the mothers were considered as non-response.
Data Collection Method and Instrument
A valid and reliable data collection tool was adapted and modified from related studies which were developed based on Extended Parallel Process Model (EPPM). The perception part was developed based on the risk behaviour diagnosis scale (RBDs) approach, adapted to the context of trachoma. The risk behaviour diagnosis scale (RBDs) was a Likert scale tool that allows rapid assessment of participants’ beliefs and behavioral responses to health threats showing that either each individual is in danger control or fear control category.36
The questionnaire was developed in four parts: the first was Socio-demographic with 13 items, the second was about communication factors having 3 items; the third part with 24 items, was about individual differences and the last part, with 12 items, was on a perception of the participants (perceived threat and perceived efficacy). The format of the tool was created using Epicollect5, a mobile data-gathering platform. The data was collected through a face-to-face interviewer-administered questionnaire. The questionnaire was developed in English then translated into Amharic (local language) then translated back to English to ensure consistency. There was one supervisor besides the principal investigator trained on integrated eye care worker and 4 nurses for data collection.
Data Management and Analysis
After the data was collected, the completed questionnaire was downloaded from epi collect-5 and saved as excel then the data was exported to a Statistical Package for Social Science (SPSS) version 23.0 for analysis. Descriptive statistics were used to characterize the socio-demographic status of study participants.
Bivariable and multivariable logistic regression analyses were done to identify predictors of behavioral responses. Independent variables with a P-value <0.25 in the bivariate analysis were entered into the multivariable logistic regression for controlled the possible effect of confounders using the forward likelihood variable selection method. The goodness-of-fit of the final models was checked using the Hosmer and Lemeshow test of goodness-of-fit for behavioral response and hence, in the final model, a p-value <0.05 was considered statistically significant. Significant independent variables were declared by adjusted odds ratio (AOR) at a 95% confidence interval.
Data Quality Assurance
As part of quality assurance, the questionnaire was prepared in the English language, translated to Amharic, and re-translated back to English by another person. To make sure that the questionnaire was appropriate and understandable; it was pre-tested on 5% of the sample size before the actual collection date in the kebele not included in the study. To assure the quality of the data, ensure clarity, wordings, understand ability, logical sequence, and skip patterns of the questions. Findings and experiences from the pre-test were utilized in modifying the data collection tool. The training was given to supervisors and data collectors for one day. During data collection, the supervisor and principal investigator were randomly checking sample questionnaires for their completeness and consistency. Regular supervision was given during the data collection period regularly to enhance the completeness and consistency of data and appropriate feedback was given to the interviewers timely. Supervisors’ daily checked completeness and consistency. The reliability test after the final data collection was checked for acceptable internal consistency with a Cronbach alpha of greater than 0.7.
Results
Socio-Demographic Characteristics
A total of 611 mothers were recruited making a response rate of 96.4%. Of the total participants, 530 (86.7%) were from rural areas and 482 (78.9%) were Orthodox. The mean age of the participants was 37.9 years, ±SD 4.6 with a range of 23 to 50 years (Table 1).
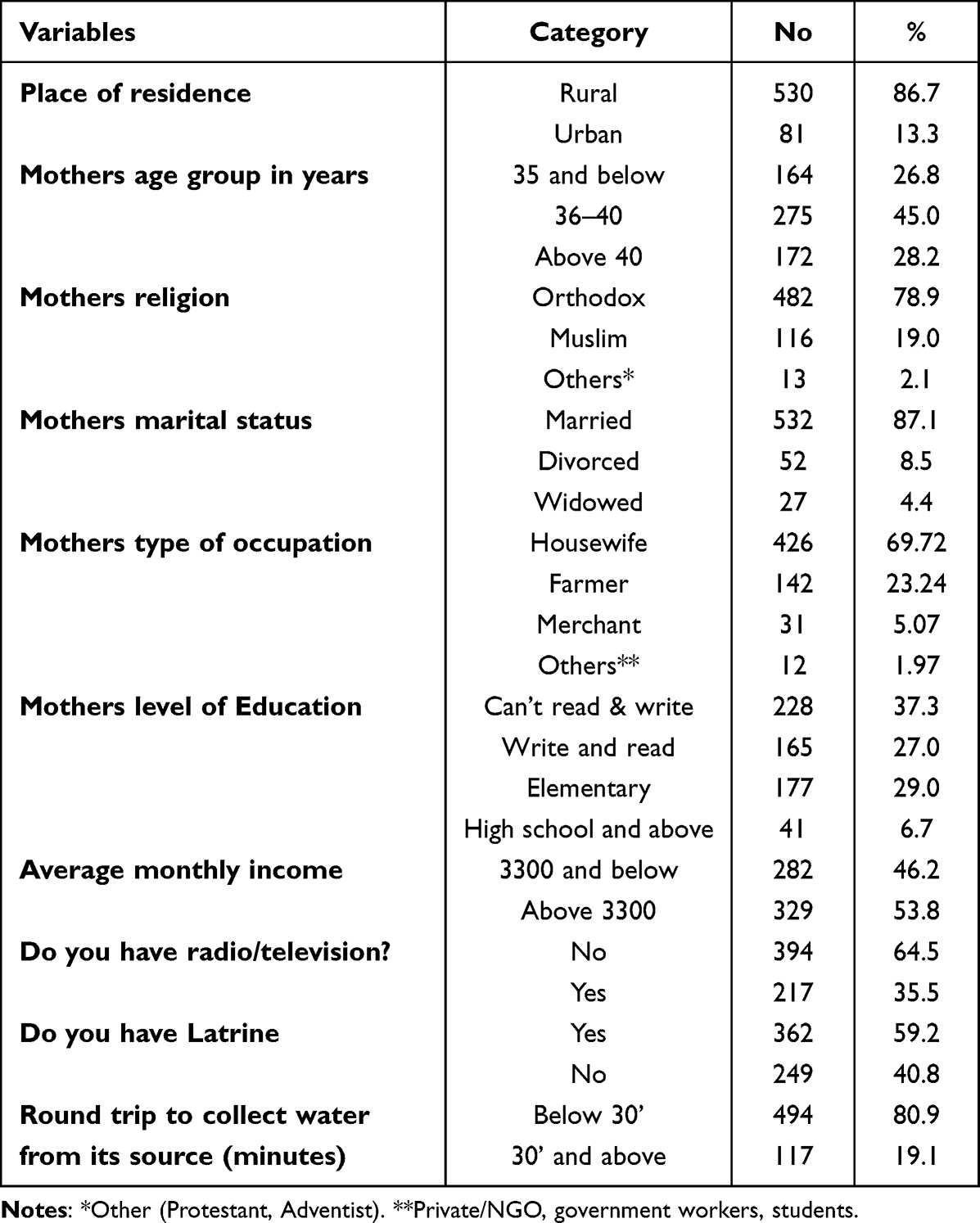 |
Table 1 Socio-Demographic Characteristics of Mothers Having Children Aged 1–9 Years in Fogera District, South Gondar Zone, Amhara Region, Northwest Ethiopia, 2022. (N = 611) |
Communication Factors
All of the participants 611 (100.0%) heard about trachoma. Among the total participants, 468 (76.6%) heard about face cleanliness and 196 (32.1%) heard about latrine utilization. Regarding, the source of information about face cleanliness to prevent trachoma 474 (77.6%) were health extension workers (Table 2).
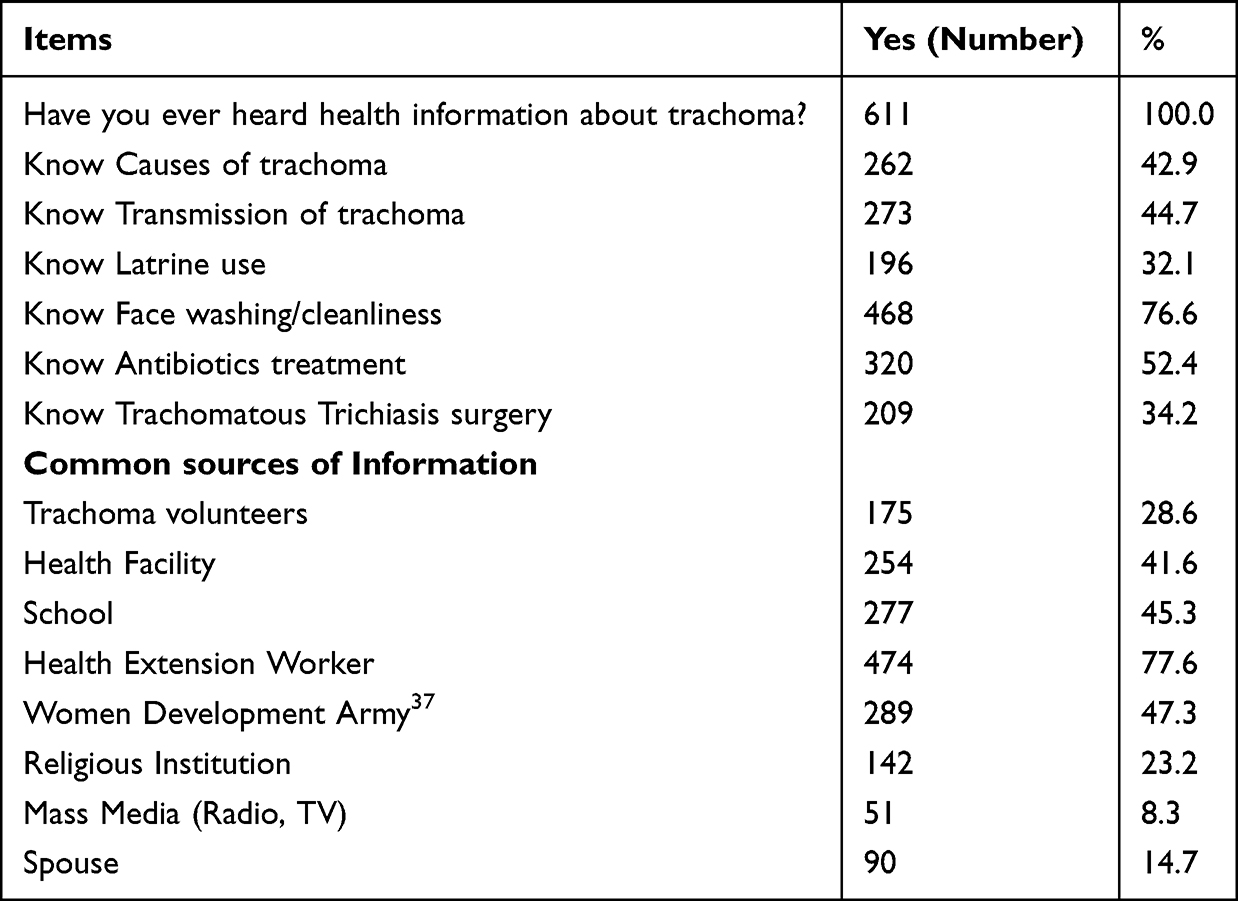 |
Table 2 Distribution of Mothers Communication Factors on Heard About Trachoma, Preferred Source of Information, Preferred Channels and Types of Message Appeals in Fogera District, South Gondar Zone, Amhara Region, Northwest Ethiopia, 2022 (n = 611) |
Knowledge Related to Trachoma
The overall knowledge of Mothers about trachoma was 411 (67.3%) (Figure 1).
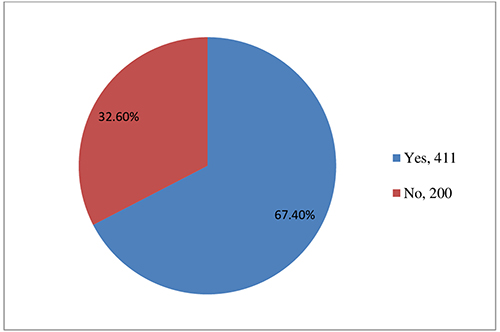 |
Figure 1 Knowledge of mothers related to Trachoma, January, 2023. |
Constructs of EPPM
The mean score with SD of perceived severity, perceived susceptibility, self-efficacy, and response efficacy of the participants were 10.20 (2.241), 10.77 (2.381), 10.55 (2.475), and 10.49 (2.12), respectively (Table 3).
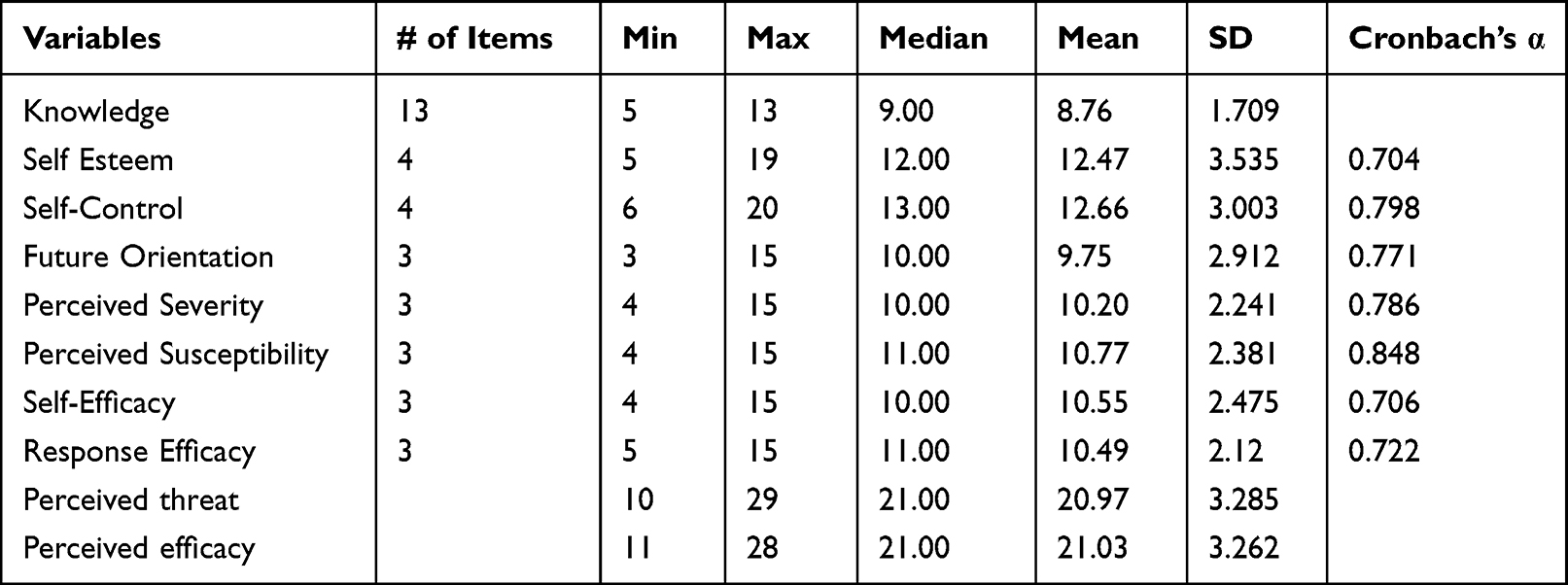 |
Table 3 Descriptive Statistics of Knowledge, Self-Esteem, Self-Control, Future Orientation, Perceived Threat and Perceived Efficacy of Mothers in Fogera District, South Gondar Zone, Amhara Region, Northwest Ethiopia, 2022 (n = 611) |
Audience Segmentation
The segmentation of participants was done using the mean. Above the mean was considered a high level and below the mean was used as a low level of threat and efficacy. Among the total participants, 136 (26.35%) were under high threat and high efficacy and 131 (21.44%) participants were under high efficacy and low threat (Table 4).
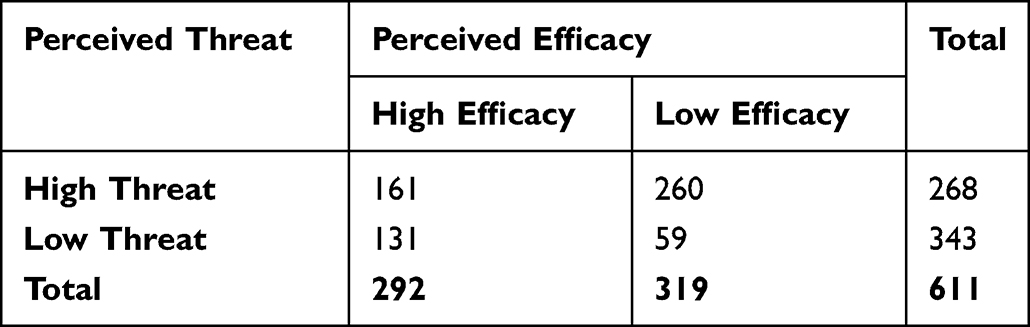 |
Table 4 Effects of Threat by Efficacy Interaction to Produce Danger Control and Fear Control Responses for Face Cleanliness Messages to Prevent Trachoma in Fogera District, South Gondar Zone, Amhara Region, Northwest Ethiopia, 2022 (n = 611) |
Behavioral Response for Face Cleanliness Messages to Prevent Trachoma
Among all participants, 292 (47.8%) (43.9–52.0) were in the danger control whereas 319 (52.2%) were in the category of fear control of the behavioral response for face cleanliness messages to prevent trachoma (Figure 2).
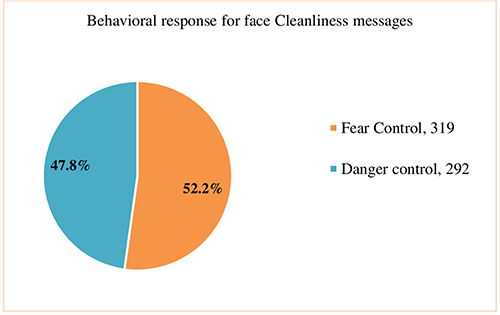 |
Figure 2 Behavioral response for Face Cleanliness Messages to prevent trachoma, January 2023. |
Factors Associated with Behavioral Response
In Bi variable analysis residence, age, religion, marital status, type of occupation, level of education, family size, average monthly income, latrine ownership, time of a round trip to collect water, information heard about face cleanliness, sources of information (health facility, school, health extension worker, religious institution, WDA), knowledge, self-esteem, self-control, and future orientation was a p-value of less than 0.25. These variables were entered into the multivariable logistic regression analysis.
In multivariable logistic regression analysis residence, marital status, level of education, family size, time of the round trip to collect water, information heard about face cleanliness, sources of information knowledge, self-esteem, self-control, and future orientation were statistically significant predictors of behavioral response for face cleanliness messages to prevent trachoma at 95% confidence interval with P-value less than 0.05.
The odds of being in the danger control category for face cleanliness were 2.91 times more likely among residents who were urban than rural [AOR = 2.91; 95% CI: (1.44–3.86)]. The odds of being in the danger control category for face cleanliness were 21% less likely among mothers who were divorced [AOR = 0.79; 95% CI: (0.667–0.939)].
The odds of being in the danger control category for face cleanliness were 2.74 times more likely among participants whose level of education was high school and above [AOR = 2.74; 95% CI: (1.546 −3.65)].
As the family size increased by 1, the odds of being in the danger control category for face cleanliness were less likely by 43% [AOR = 0.57; 95% CI: (0.453 −0.867)].
The odds of being in the danger control category for face cleanliness were 21% less likely among participants who waste ≥30 minutes collecting water on a round trip from its source [AOR= 0.79; 95% CI: (0.423 −0.878)].
The odds of being in the danger control category for face cleanliness were 3.79 times more likely among participants who have information about face washing than their counterparts [AOR = 3.79; 95% CI: (2.661 −5.952)].
The odds of being in the danger control category for face cleanliness was more likely among mothers who chose health facility as the preferred source of information by 2.76 times than their counterpart [AOR = 2.76; 95% CI: (1.645 −4.965)]. The odds of being in the danger control category for face cleanliness was more likely among mothers who chose the school as the preferred source of information by 3.68 times than their counterpart [AOR = 3.68; 95% CI: (1.648 −7.530)]. The odds of being in the danger control category for face cleanliness was more likely among mothers who chose health extension workers as the preferred source of information by 3.96 times than their counterpart [AOR = 3.96; 95% CI: (2.928 −6.752)].
As a unit increase in knowledge sum score, the odds of being in the danger control category of behavioral response for face cleanliness were 2.065 times more likely [AOR = 2.065; 95% CI: (1.325–4.427)]. As a unit increase in future orientation sum score, the odds of being in the danger control category of behavioral response for face cleanliness were 2.16 times more likely [AOR = 2.16; 95% CI: (1.345–4.524)]. The final model explains 83.2% of predictions of the outcome variable (behavioral response) with a goodness-of-fit of the model (x2/df = 31.04/34, p-value = 0.6133) (Table 5).
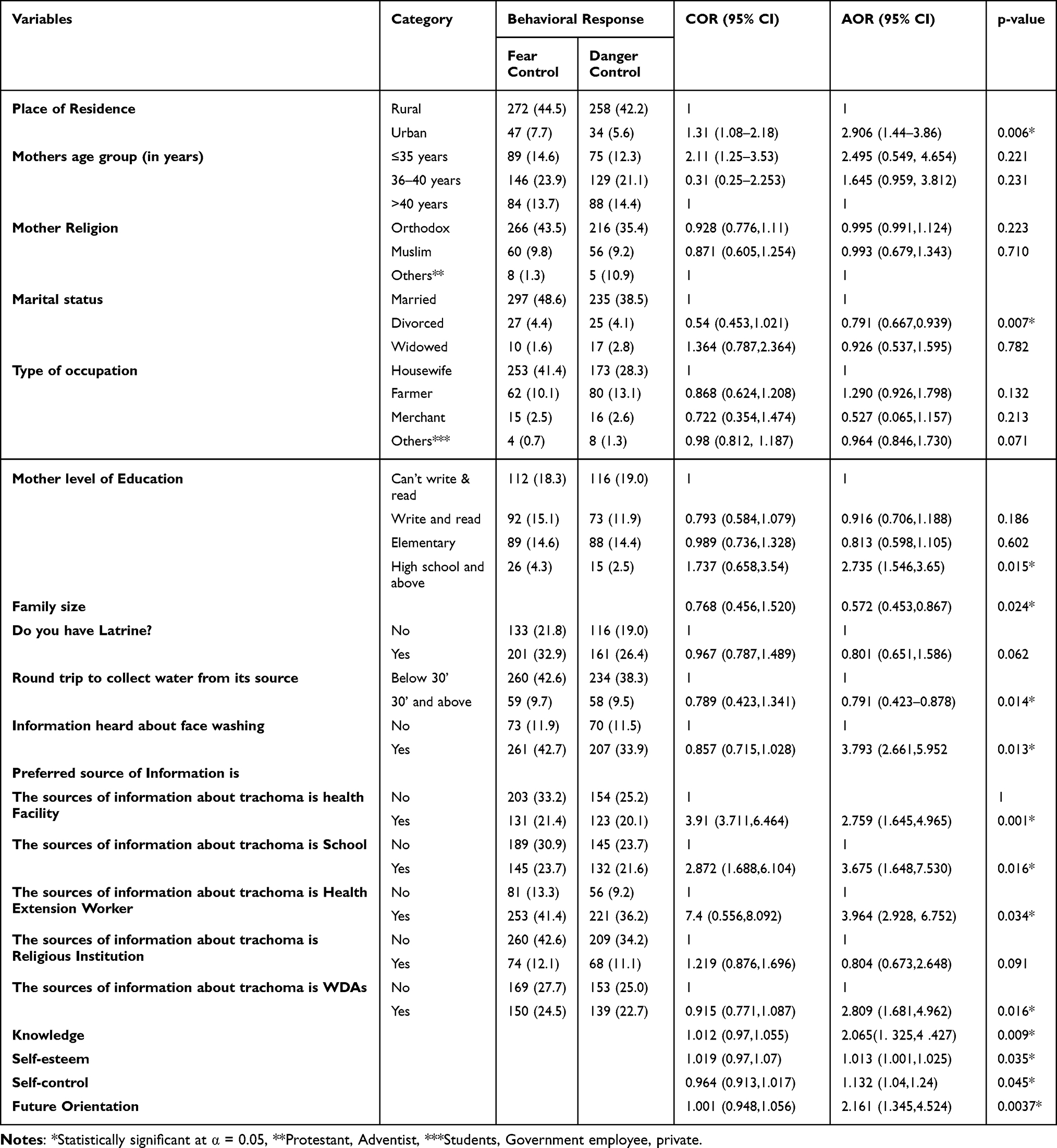 |
Table 5 Multivariable Binary Logistic Regression Analysis of Factors on Behavioral Response for Face Cleanliness Messages to Prevent Trachoma in Fogera District, South Gondar Zone, Amhara Region, Northwest Ethiopia, 2022 (n = 611) |
Discussion
The extended parallel process model was guiding this study to assess the behavioral response to face cleanliness messages to prevent trachoma among mothers who had children of age 1 to 9 years old.
The findings of this study indicated that 47.8% of participants were in the danger control behavioral response of face cleanliness, whereas 52.2% were in the fear control response. However, this study was lower than the study done in the Oromia region on the assessment of face-washing behavioral response showed that 52% of caregiver mothers washed their children’s faces.38 The discrepancy might be due to a perceived threat, and perceived efficacy levels. High-perceived efficacy with high-perceived threat and high-perceived efficacy with low perceived threat leads to danger control and in the other direction, a high-perceived threat with low perceived efficacy leads to a fear control response.12,39 This finding was also lower than the study conducted in Oromia on household caregivers (52% behavioral response of face washing),40 and lower than the study done in East gojjam with a behavioral response of 92% face washing practice of all children in the HHs.28 The difference might be due to the difference in mothers’ intention to adopt the recommended behaviour. A study in China using EPPM to evaluate the effectiveness of fear appeal messages stated that messages containing a high level of threat and efficacy increase women’s intentions to adopt recommended practices,14 but here the majority of 52.2% of mothers did not intend to adopt the recommended practice. The possible reason for low danger control could be that it might be the educational status of mothers the majority 37.5% cannot read and write since higher educational status leads to the acceptance of the message.
Another reason for the low level of danger control response might be the absence of well-designed fear appeal messages, since well-designed fear appeal messages can motivate people, and mothers might be exposed to these messages only once, which may not change the behaviour of mothers directly. However, the effectiveness of fear appeal messages might be realized by multiple interactions with the information instead of one exposure to the information.41
Urban residents were positive predictors of behavioral response. In this study, urban residents were more likely to be in danger control than rural residents were. This finding is contradicting the study done on Oromia.42 The difference might be the deployment of Health Extension Workers (HEWs). In this finding, two HEWs were deployed for each urban, but the later study showed as there was a lack of HEWs in urban than in rural. In this study, urban becomes a positive predictor might be due to factors of frequent supportive supervision by HEWs and distance from the health post. The other reason might be the urban had access to information through social media compared to the rural.
Divorced marital status was negatively associated with danger control. In this study divorced mothers were less likely to be in danger control than married mothers. The reason might be due to married mothers may receive assistance from their spouses and sharing of responsibilities.
High school and above the level of education was the positive predictor of behavioral response. In this study educational status of high school and above was more likely than cannot read and write. This study was similar to the study done in Ankober, Ethiopia,43 and the study conducted in Gonji Kollela district, Amhara.44 This might be because the more educated mothers may seek more information and have access to media exposure.
Family size was negatively associated with behavioral responses. This finding was similar to the study conducted by Gonji Kollela.44 The reason for this finding was that Trachoma is a disease of easily communicable among residents in poor housing conditions and the crowdedness of people sharing a living room.
More than 30 minutes round trip to collect water was negatively associated with the behavioral response of danger control. In this study, the participants who travel for more and equal to 30 minutes to collect water from its source were less likely to be in danger control. This finding is similar to the study done in the East Gojjam zone of the Amhara.28 The reason might be the time it takes and the saving of water instead of using water since saving water means saving time.
Having information about face washing was a positive predictor of danger control. In this study, having information about face washing was more likely than their counterpart. Health education and promotion in different settings play a good role to produce the intended outcome, especially for behavioral change.45,46
Health Facilities and Health extension workers for the preferred source of information had a positive significant association with the danger control behavioral response. In this study, mothers who chose health facilities and health extension workers as preferred sources of information were more likely to be in danger control than their counterparts. This was similar to the qualitative study done on talking health in Southwest Ethiopia among rural mothers, indicating Health Extension Workers (HEWs) were the preferred sources of information.47 This might be seeking health information found that HEWs as their most preferred and credible source for maternity information,48 the exchange of information between mothers and health extension workers were trusted and the belief their personal information was not disclosed, and the belief that health extension workers were the experts of health and are females.
Women Development Armies (WDAs) as a source of information were positive predictors of danger control. This study explained that sources of information from WDAs were more likely to be in danger control than their counterpart. The reason might be the easy accessibility of WDAs by their neighbour mothers and the trust they build.
Knowledge of the mothers had a positive association with the behavioral response of danger control. In this study, a unit increase in knowledge was more likely to be in the danger control category. This finding was similar to the study done in Oromia region (cross-sectional),42 and India (cross-sectional).49 Having knowledge about the perceived threat and perceived efficacy motivates mothers to accept the message and leads to the danger control outcome.
Self-esteem, self-control, and future orientation showed a positive association with the behavioral response. In this study, a unit increase in self-esteem, self-control, and future orientation sum score were more likely to be in the danger control category. Partly, this might be also due to higher perceived efficacy levels, mothers with higher knowledge, self-esteem, self-control, and futurity levels will have higher self-efficacy levels. This is also in line with the idea of the EPPM.12
Strengths and Limitations
The strengths of this study were the use of Epi collect-5 data collection software, which helps to collect with the smart cell phone, and it was very easy to use and fast to collect. The limitation of this study was a cross-sectional study in which it was not possible to identify the causality of the effect, lack of previous research studies on the related topic using EPPM and the study could not answer the reason why mothers are in danger control.
Conclusions
Less than half (47.8%) of the participants were in the danger control response, which is low, and yet, the majorities 52.2% were in the fear control category. This portrayed that the majority of participants had higher perceived threat (perceived severity and perceived susceptibility) than perceived efficacy (self-efficacy and response efficacy). Residence, marital status, level of education, family size, monthly income, time of the round trip to collect water, face washing information, source of information from the health facility, health extension workers, schools and women development army, knowledge, self-esteem, self-control, and future orientation were independent predictors of face cleanliness. Messages for face cleanliness strategy should better give high attention to perceived efficacy with consideration of perceived threat, hence this might meet the communication objectives of the health package messages for mothers.
Data sharing statement
All necessary data are available with the corresponding author and will be given upon reasonable request.
Ethical clearance and consent for participation
Ethical clearance was obtained from the institutional review board of Bahir Dar University, College of Medicine and Health Sciences with ethical review board (IRB) number; 549/2022, and assigned number; 003. Written informed consent was obtained from all study participants. Study participants have informed the write to withdraw at any point in data collection and data are confidentially secured. All methods were carried out in accordance with relevant guidelines and regulations complied with the Helsinki declaration.
Acknowledgment
We would like to acknowledge Bahir Dar University, Fogera district health office, data collectors, and study participants.
Author contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All authors declared no conflicts of interest in this work.
References
1. Burton MJ, Mabey DCW. The global burden of trachoma: a review. PLoS Negl Trop Dis. 2009;3(10):e460. doi:10.1371/journal.pntd.0000460
2. Trachoma; 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/trachoma.
3. Mariotti SPPR, Resnikoff S. Trachoma: looking forward to Global Elimination of Trachoma by 2020 (GET 2020). Am J Trop Med Hyg. 2013;69(5):33–35. doi:10.4269/ajtmh.2003.69.5_suppl_1.0690033
4. Emerson PM, Burton M, Solomon AW, et al. The SAFE Strategy for Trachoma Control: Using Operational Research for Policy, Planning, and Implementation. Organ BWH; 2006.
5. Taylor HRBM, Haddad D, West F, Wright H, Wright H. Trachoma. Lancet Elsevier Ltd. 2014;384:2142–2152. doi:10.1016/S0140-6736(13)62182-0
6. Stocks MEOS, Haddad D, Addiss DG, McGuire C, Freeman MC. Effect of water, sanitation, and hygiene on the prevention of trachoma: a systematic review and meta-analysis. PLoS Med. 2014;11(2):e1001605. doi:10.1371/journal.pmed.1001605
7. World Health Organization. Eliminating Trachoma: Accelerating Towards 2020. World Health Organization; 2016.
8. Gedefaw M, Shiferaw A, Alamrew Z, et al. Current state of active trachoma among elementary school students in the context of ambitious national growth plan: the case of Ethiopia. Health. 2013;5(11):1768–1773. doi:10.4236/health.2013.511238
9. Ministry of Health-Ethiopia. Health Sector Transformation Plan II (HSTP Ii) 2020/21-2024/25 (2013-2017 Efy); 2021.
10. Ministry of Health. The Third National Neglected Tropical Diseases Strategic Plan 2021-2025. 2021.
11. The Carter Center Ethiopia. Trachoma Control Program Health Education Materials Library; 2022. Available from: http://www.cartercenter.org/health/trachoma_education/index.html.
12. Witte KMG, Martell D. Effective Health Risk Messages: A Step-by-Step Guide. Sage; 2001.
13. Cho HWK, Witte K. Managing fears in public health campaigns: a theory-based formative evaluation process. Health Promot Pract. 2005;6(4):482–490. doi:10.1177/1524839904263912
14. Chen LYX. Using EPPM to evaluate the effectiveness of fear appeal messages across different media outlets to increase the intention of breast self-examination among Chinese women. Health Commun. 2018;06(1):1–8.
15. Health Communication Capacity Collaborative (HC3). The Extended Parallel Processing Model: An HC3 Research Primer [PDF]; 2015.
16. Witte K. Putting the fear back into fear appeals: the Extended Parallel Process Model. Commun Monogr. 1992;59(4):329–349. doi:10.1080/03637759209376276
17. Rimal RNMD, Morrison D. A uniqueness to personal threat (UPT) hypothesis: how Similarity Affects Perceptions of Susceptibility and Severity in Risk Assessment. Health Commun. 2006;20(3):209–219. doi:10.1207/s15327027hc2003_1
18. World Health Organization. World Report on Vision. Geneva: World Health Organization; 2019.
19. World Health Organization. WHO Alliance for the Global Elimination of Trachoma by 2020, Eliminating Trachoma: Accelerating Towards 2020. World Health Organization; 2021.
20. The Carter Center Ethiopia. Women and Trachoma, Achieving Gender Equity in the Implementation of SAFE; 2009.
21. Scott D, Chernet A, Astale T, et al. Population-Based Prevalence of Ocular Chlamydia trachomatis Infection among Infants in the Trachoma Endemic Amhara Region, Ethiopia. Am J Trop Med Hyg. 2022;106(1):62–65. doi:10.4269/ajtmh.21-0873
22. Cromwell EA, Courtright P, King JD, Rotondo LA, Ngondi J, Emerson PM. The excess burden of trachomatous trichiasis in women: a systematic review and meta-analysis. Trans R Soc Trop Med Hyg. 2009;103(10):985–992. doi:10.1016/j.trstmh.2009.03.012
23. Kea G. Selecting behavior change priorities for trachoma ‘F’ and ‘E’ interventions: a formative research study in Oromia, Ethiopia. PLoS Negl Trop Dis. 2019;13:1–19.
24. Tidwell JBFC, Gopalakrishnan A, Sheth E, et al. Integrating face washing into a school-based, handwashing behavior change program to prevent trachoma in Turkana, Kenya. Am J Trop Med Hyg. 2019;101(4):767–773. doi:10.4269/ajtmh.19-0205
25. Aisha EP, Zerihun M, Gessese D, et al. Progress to Eliminate Trachoma as a Public Health Problem in Amhara National Regional State, Ethiopia: results of 152 Population-Based Surveys. Am J Trop Med Hyg. 2019;10(6):1286–1295.
26. Ngondi J, Gebre T, Shargie EB, et al. Estimation of effects of community intervention with Antibiotics, Facial cleanliness, and Environmental improvement (A, F, E) in five districts of Ethiopia hyperendemic for trachoma. Trans R Soc Trop Med Hyg. 2015;103(1000):10.
27. The Carter Center Ethiopia. Trachoma Impact Survey (TIS); 2022.
28. Aiemjoy KSN, Gebresillasie S, Shiferaw A, et al. ‘If an Eye Is Washed Properly, It Means It Would See Clearly’: a Mixed Methods Study of Face Washing Knowledge, Attitudes, and Behaviors in Rural Ethiopia. PLoS Negl Trop Dis. 2016;10(10):e0005099. doi:10.1371/journal.pntd
29. HHS public access. Face Washing Promotion for Preventing Active Trachoma. HHS public access; 2015.
30. The International Coalition for Trachoma Control (ICTC). All You Need for F&E, a Practical Guide to Partnering and Planning; 2015.
31. Fogera Woreda Health Office. Total Population of the District, Basic Profile of 2015 EC; 2022.
32. Ntshuntshe ZGN, Livingstone Gqeba M, Majibha N. Self-Esteem: a Positive Way to Psychosocial Well-Being. Counseling Therapy. 2020. doi:10.5772/intechopen.92033
33. DeLisi M. Chapter 10: Low Self-Control is a Brain-Based Disorder. SAGE Publications Ltd; 2014; doi:10.4135/9781483349114
34. Nuttin J, Joseph N. Future Time Perspective and Motivation: Theory and Research Method. New York: Psychology Press; 2014.
35. Greenland K, White S, Sommers K, et al. Selecting behaviour change priorities for trachoma ‘F’and ‘E’interventions: A formative research study in Oromia, Ethiopia. PLoS neglected tropical diseases. 2019;13(10):e0007784.
36. Hailay G, Nega M, Tesfay T, et al. Knowledge, Attitudes, and Practices about Trachoma in Rural Communities of Tigray Region, Northern Ethiopia: Implications for Prevention and Control. Journal of Environmental and Public Health. 2020; 2020:8. doi:10.1155/2020/3270530
37. Gowda C, Dempsey AF. The rise (and fall?) of parental vaccine hesitancy. Hum Vaccin Immunother. 2013;9(8):1755–1762. doi:10.4161/hv.25085
38. Yibeltal Tebekaw MT, Tulu L, Endale H, Dodson S. Oromia WASH and Trachoma Programming Strategy: a Guide for Developing an Integrated, Evidence and Theory Based Water, Sanitation and Hygiene (WASH) and Trachoma F and E Programme. J Med. 2019:655.
39. Witte K, Cameron KA, McKeon JK, Berkowitz JM. Predicting risk behaviors: development and validation of a diagnostic scale. J Health Commun. 1996;1:317–341. doi:10.1080/108107396127988
40. Greenland KWS, Sommers K, Biran A, et al. Selecting behavior change priorities for trachoma ‘F’ and ‘E’ interventions: a formative research study in Oromia, Ethiopia. PLoS Negl Trop Dis. 2019;13(10):e0007784. doi:10.1371/journal.pntd
41. Smith SWRK, Kotowski MR, Glazer E, McFeters C, Keesecker NM, Law A. Using the EPPM to create and evaluate the effectiveness of brochures to increase the use of hearing protection in farmers and landscape workers. J Appl Commun Res. 2008;36(2):200–218. doi:10.1080/00909880801922862
42. Abera T, Tilahun W, Waqjira I. Trachoma prevention practice among mothers with child age of under-9 years and factors associated in a rural district of Oromia Region, Ethiopia: community-based cross-sectional study. World J Adv Res Rev. 2021;10:245–257. doi:10.30574/wjarr.2021.10.1.0136
43. Iea G, Jones L, Gelaye B. Access to the water source, latrine facilities, and other risk factors of active trachoma in Ankober, Ethiopia. PLoS One. 2009;4(8):e6702. doi:10.1371/journal.pone.0006702
44. Nigusie A, Berhe R, Gedefaw, M. Prevalence and associated factors of active trachoma among children aged 1–9 years in rural communities of Gonji Kolella district, West Gojjam zone, North West Ethiopia. BMC Res Notes. 2015;8(1):641. doi:10.1186/s13104-015-1529-6
45. Health-Ethiopia Mo. Second Generation Health Extension NTD Package, 2017. 2017:4–7
46. Ethiopia TCC. Zithromax Census Pad Registration, South Gondar; 2022.
47. Asfaw SMS, Abera M, Mamo A, et al. Talking health: trusted health messengers and effective ways of delivering health messages for rural mothers in Southwest Ethiopia. Arch Public Health. 2019;77(1):1–8. doi:10.1186/s13690-019-0334-4
48. Tsehay AB. Seeking Health Information in a Rural Context: Exploring Sources of Maternal Health Information in Rural Ethiopia [Master’s Thesis]. The University of Bergen; 2014.
49. Reddy BY, Kusuma L, Chandrakant S. Water and Sanitation Hygiene Practices for Under-Five Children. Community Med Health Educ. 2017;1:563.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.