Back to Journals » ClinicoEconomics and Outcomes Research » Volume 16
Behavioral Economic Strategies Increase Adverse Event Reporting in Pediatric Anesthesia
Authors Guan TK, Willer BL, Stevens J, Tobias JD ![]() , Olbrecht VA
, Olbrecht VA
Received 5 October 2024
Accepted for publication 28 November 2024
Published 7 December 2024 Volume 2024:16 Pages 841—845
DOI https://doi.org/10.2147/CEOR.S499363
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Tiffany K Guan,1 Brittany L Willer,2,3 Jack Stevens,4,5 Joseph D Tobias,2,3 Vanessa A Olbrecht2,3
1College of Medicine, The Ohio State University, Columbus, OH, USA; 2Department of Anesthesiology & Pain Medicine, Nationwide Children’s Hospital, Columbus, OH, USA; 3Department of Anesthesiology & Pain Medicine, The Ohio State University Wexner Medical Center, Columbus, OH, USA; 4Department of Pediatrics, Nationwide Children’s Hospital and The Ohio State University, Columbus, OH, USA; 5Center for Clinical Excellence, Nationwide Children’s Hospital, Columbus, OH, USA
Correspondence: Brittany L Willer, Nationwide Children’s Hospital, 700 Children’s Drive, Columbus, Ohio, 43205, USA, Email [email protected]
Introduction: Identification and reporting of severe adverse events (SAEs) during anesthesia care remains critical in identifying areas of improvement in perioperative patient care. Although many healthcare organizations rely on the self-reporting of SAEs, under-reporting may limit the identification of the true incidence of these events. To circumvent these barriers, many healthcare systems leverage the Electronic Medical Record (EMR) by incorporating an Anesthesia Information Management System (AIMS).
Methods: We followed the Institute for Healthcare Improvement’s Model of Improvement and implemented behavioral economic-based interventions to our perioperative practice including adding a deliberation-promoting “hard stop” that required the anesthesiologists to report the occurrence or absence of a “notable event” prior to closing a patient’s encounter in the EMR system.
Results: At baseline, 53% of SAEs were self-reported. The interventions resulted in a baseline shift to more than 75% self-reporting, a relative increase of 42%.
Conclusion: An increase in reporting of SAEs was achieved with simple interventions including modifications of the EMR which were done with limited financial impact or interruption in the work flow.
Keywords: adverse events, pediatric anesthesia, intraoperative care, quality and safety
Introduction
Patient safety became a national focus more than two decades ago when the Institute of Medicine published To Err is Human, a startling revelation of the frequency of medical errors and severe adverse events (SAEs) leading to patient harm.1 In pediatrics, SAEs account for more than 4400 pediatric deaths a year.2 Recent studies estimate that although there are 69.7 adverse events (AEs) per 1000 patient-days, only 6.6% of these events are self-reported.2 Low rates of self-reporting limit opportunities to promote feedback and identify areas of improvement in clinical practice, which serve to improve patient safety.3
To circumvent barriers to self-reporting SAEs in anesthesiology, many healthcare systems leverage the Electronic Medical Record (EMR) by incorporating an Anesthesia Information Management System (AIMS). AIMS identifies potential events using algorithm-based indicators that include vital signs, event stamps, and medication administrations captured in the anesthesia record. Although AIMS increases the capture of anesthesia-related SAEs, it does not replace self-reporting, underscoring the importance of engaging anesthesia providers in the process.4
Human behavior is complex, guided both by intrinsic factors and external cues.5 Behavioral economic “nudges” involve structuring the decision-making environment to facilitate the occurrence of a desired activity.6 Behavioral economics is increasingly being used to encourage healthcare providers to adhere to best practice guidelines.5 Our goal was to implement behavioral economics-based interventions to increase self-reporting of anesthesia-related SAEs at our institution from 53% to 85% over 10 months and sustain this for 4 months.
Methods
This initiative was performed at a pediatric hospital that performs more than 40,000 anesthetics per year. As a Quality Improvement initiative, this project is deemed IRB-exempt by the Review Board of Nationwide Children’s Hospital (Columbus, Ohio) and the need for informed consent was waived. We followed the Institute for Healthcare Improvement’s Model of Improvement and defined SAEs according to Wake-Up Safe.7 The data accessed complied with relevant data protection and privacy regulations. We collected SAE self-reporting rates before and after the implementation of behavioral economic-based interventions. The interventions included:
- Framing (softening terminology): We changed our EMR so that clinicians were asked to document “notable events” instead of “adverse events” in the post-operative note.
- Implementing a deliberation-promoting “hard stop”. This required the anesthesiologists to report the occurrence or absence of a “notable event” prior to closing a patient’s encounter in the EMR system.
- Simplifying: We added “Quick” notes to the anesthetic record to facilitate real-time capture of SAEs. These quick notes had pre-filled text options to expedite charting the event (Figure 1). Additionally, the documentation of a “Quick” note event automatically self-reported the incident at the end of the encounter.
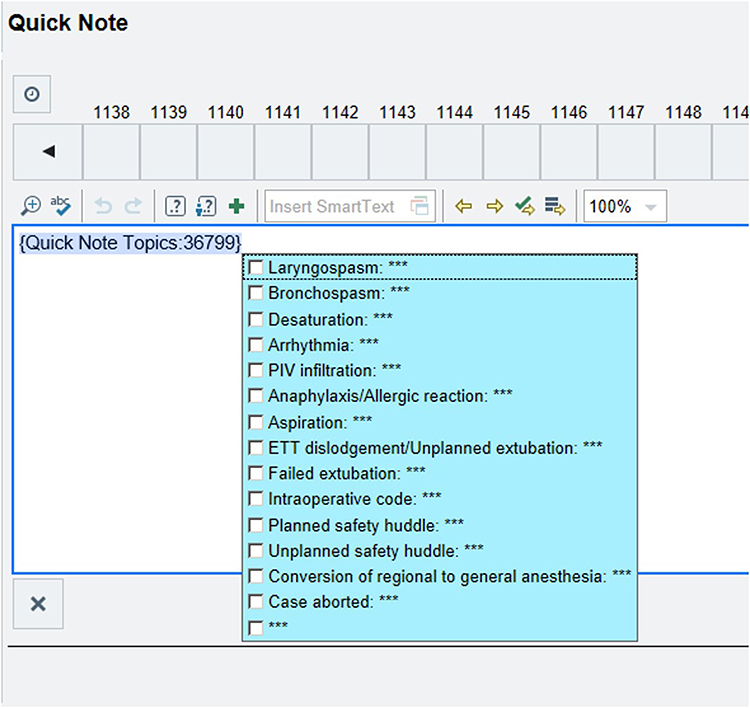 |
Figure 1 Pop-up screen from the notable event documentation that was added to electronic medical record to improve self-reporting of SAEs. |
Self-reporting of SAEs is the gold standard. In the absence of self-reporting, AIMS identifies potential events based on EMR algorithms that we have designed. AIMS identification of SAEs is sensitive, but not specific. Also, because of limitations of the algorithms, AIMS cannot identify all SAEs. Therefore, as part of our quality improvement process, manual chart review is used to verify potential events identified by AIMS. We compared self-reported SAEs to those captured by AIMS and manual chart review. We then generated a control chart. The numerator was self-reported SAEs and the denominator was total SAEs.
Results
At baseline, prior to the interventions, 53% of SAEs were self-reported. From January 2021 through March 2023, 259 SAEs were captured, with 165 (64%) of these being classified as self-reported. The interventions resulted in a baseline shift to more than 75% self-reporting, a relative increase of 42%. (Figure 2).
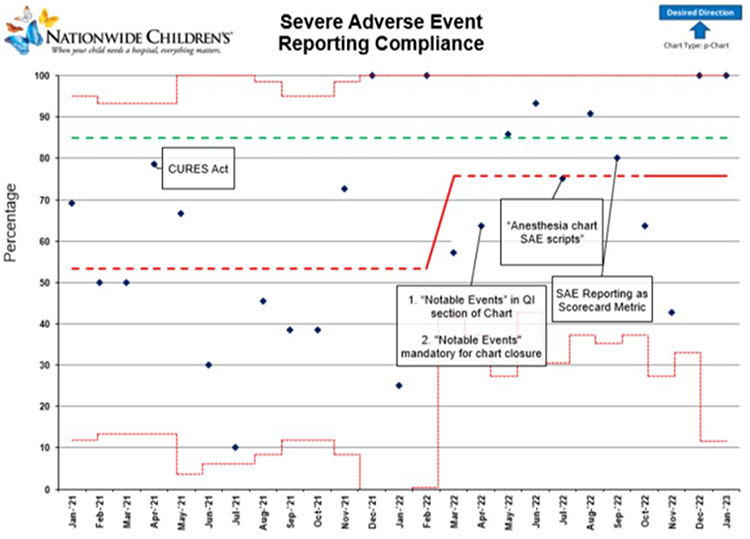 |
Figure 2 Control chart showing the proportion of SAEs self-reported over time from a baseline of 53% to more than 75% after the interventions. The dotted red line shows the baseline reporting rate of 53% which increased to slightly more than 75%. The CURES act allowed patients and families to have immediate and full access to the patient record. |
Discussion
In this initiative, we facilitated and encouraged self-reporting of anesthesia-related perioperative SAEs by using behavioral economics-based interventions embedded in the EMR. Our findings are consistent with a recent systematic review suggesting that behavioral economic “nudges” often enhance clinical performance.7 The preliminary results were promising, with an increased SAE self-reporting rate of 42% and an overall rate of more than 75%. However, despite these interventions there were still some months that fell below our goal suggesting that additional interventions may be needed.
Softening language (changing “adverse events” to “notable events” in the EMR) and simplification (making it quicker to document SAEs) were two of the strategies that likely contributed to our positive results. Regarding the former, Marshall et al similarly found that changing the harsher term “diagnostic error” to the less-threatening phrase “diagnostic learning opportunity” increased clinicians’ self- reporting of their diagnostic mistakes in a tertiary children’s hospital.8 Regarding the latter, Adusumalli et al found that simplifying the process for ordering cardiac rehabilitation services for adults with ischemic heart disease dramatically increased referral rates for that evidence-based therapy.9 Although our preliminary findings may have limited generalizability because they apply to only one tertiary pediatric hospital, our deployment of behavioral economic “nudges” through an EMR system could facilitate other institutions’ adoption of these strategies to determine if our promising results can be replicated elsewhere.
As with any prospective intervention, one must accept the potential limitations of quality improvement processes. This work was performed at a single center with a commonly-used EMR model. Therefore, our findings may not be generalizable. With a baseline SAE self-reporting of 53%, we chose a goal of improving reporting to 85% over 10 months and sustaining it for 4 months. However, one could argue that the goal should be 100% with a more prolonged maintenance beyond 4 months to demonstrate persistent efficacy. Additionally, we focused on implementing behavioral interventions to improve SAE reporting. In order to achieve the goal of 100% identification of SAEs, it is likely that other processes such as “word mining” of the EMR will be needed to identify adverse effects. For example, word mining of medication administrations can identify patients who received medications used to treat common SAEs (atropine for bradycardia, epinephrine for cardiovascular collapse, albuterol for bronchospasm). We did not include intraoperative death in this study because there were none during the study period. Because of complexities involved with how it is documented, we did not have a background algorithm to identify unplanned postoperative admissions or for the need for tracheal intubation.
In conclusion, the reporting and tracking of SAEs are critical components of anesthesia practice improvement. However, barriers exist that prevented SAE reporting, resulting in missed opportunities to enhance patient safety. Behavioral economics can be used to increase self-reporting of SAEs. We achieved preliminary success with simple modifications of the EMR which were done with limited financial impact or interruption in the work flow. While our study showed an increase in the reporting of SAEs with these EMR-based interventions, further efforts are needed to identify strategies that can enhance the effectiveness of SAE self-reporting. Additionally, we would recommend ongoing surveillance to ensure that these outcomes are sustained over time. The increase in self-reporting has allowed us to be more confident in the reporting of SAEs not captured by AIMS (unplanned tracheal reintubation). Barriers that prevent further pursuit are the limitations of behavioral economic strategies. Human behavior is extremely difficult to change and while you can make some changes, 100% sustainable changes is likely not possible.
Abbreviations
AE, adverse event; EMR, electronic medical record; AIMS, Anesthesia Information Management System; SAE, severe adverse event; IRB, institutional review board.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Institute of Medicine Committee on Quality of Health Care in America. To Err is Human: Building a Safer Health System. Washington, DC: National Academies Press (US); 2000.
2. Halvorson EE, Thurtle DP, Easter A, Lovato J, Stockwell D. Disparities in adverse event reporting for hospitalized children. J Patient Saf. 2022;18(6):e928–e933. doi:10.1097/PTS.0000000000001049
3. Jegathesan M, Vitberg YM, Pusic MV. A survey of mindset theories of intelligence and medical error self-reporting among pediatric housestaff and faculty. BMC Med Educ. 2016;16:58. doi:10.1186/s12909-016-0574-8
4. Tewfik G, Naftalovich R, Kaushal N, Zhang K. Adverse event and complication tracking in anaesthesiology: dependence on self-reporting despite implementation of electronic health records. Br J Anaesth. 2022;128(1):e28–e32. doi:10.1016/j.bja.2021.10.019
5. Wang SY, Groene O. The effectiveness of behavioral economics-informed interventions on physician behavioral change: a systematic literature review. PLoS One. 2020;15(6):e0234149. doi:10.1371/journal.pone.0234149
6. Stevens J. The promising contributions of behavioral economics to quality improvement in health care. Pediatr Qual Saf. 2017;2(3):e023. doi:10.1097/pq9.0000000000000023
7. Kurth CD, Tyler D, Heitmiller E, Tosone SR, Martin L, Deshpande JK. National pediatric anesthesia safety quality improvement program in the United States. Anesth Analg. 2014;119(1):112–121. doi:10.1213/ANE.0000000000000040
8. Marshall TL, Ipsaro AJ, Le M, et al. Increasing physician reporting of diagnostic learning opportunities. Pediatrics. 2021;147(1):e20192400. doi:10.1542/peds.2019-2400
9. Adusumalli S, Jolly E, Chokshi NP, et al. Referral rates for cardiac rehabilitation among eligible inpatients after implementation of a default opt-out decision pathway in the electronic medical record. JAMA Network Open. 2021;4(1):e2033472. doi:10.1001/jamanetworkopen.2020.33472
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.