Back to Journals » Patient Preference and Adherence » Volume 17
Behavior Change Techniques Improve Adherence to Physical Activity Recommendations for Adults with Metabolic Syndrome: A Systematic Review
Authors Peiris CL ![]() , Gallagher A, Taylor NF
, Gallagher A, Taylor NF ![]() , McLean S
, McLean S
Received 26 October 2022
Accepted for publication 20 December 2022
Published 15 March 2023 Volume 2023:17 Pages 689—697
DOI https://doi.org/10.2147/PPA.S393174
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Casey L Peiris,1 Amy Gallagher,2 Nicholas F Taylor,1,3 Sionnadh McLean2
1School of Allied Health, Human Services and Sport, La Trobe University, Melbourne, Victoria, Australia; 2Department of Allied Health Professions, Sheffield Hallam University, Sheffield, UK; 3Allied Health Clinical Research Office, Eastern Health, Box Hill, Victoria, Australia
Correspondence: Sionnadh McLean, Collegiate Campus, Sheffield Hallam University, L108, 36 Collegiate Crescent, Sheffield, S10 2BP, UK, Tel +447342 092 340, Email [email protected]
Background: Exercise and physical activity interventions improve short-term outcomes for people with metabolic syndrome, but long-term improvements are reliant on sustained adherence to lifestyle change for effective management of the syndrome. Effective ways of improving adherence to physical activity and exercise recommendations in this population are unknown. This systematic review aims to determine which interventions enhance adherence to physical activity and/or exercise recommendations for people with metabolic syndrome.
Methods: Electronic databases MEDLINE, PubMed, CINAHL, SPORTdiscuss and ProQuest were searched to July 2022. Risk of bias was assessed using the Cochrane risk of bias tool and overall certainty of evidence assessed using the Grading of Recommendation Assessment, Development and Evaluation approach.
Results: Four randomized controlled trials with 428 participants (mean age 49– 61 years) were included. There was very low certainty evidence from two trials that goal setting interventions may improve adherence to physical activity recommendations over three to six months. There was low certainty evidence from two trials that self-monitoring and feedback interventions increased adherence to physical activity interventions over 12 months for people with metabolic syndrome.
Conclusion: Clinicians and researchers may consider using behavior change strategies such as goal setting, monitoring and feedback in interventions for people with metabolic syndrome to increase adherence to physical activity and exercise recommendations over 3 to 12 months, but high-quality evidence is lacking.
Keywords: metabolic syndrome, adherence, long-term condition, behavior change, physical activity, exercise
Introduction
Metabolic syndrome is defined by the International Diabetes Federation (IDF), National Heart, Lung, and Blood Institute, American Heart Association, World Heart Federation, International Atherosclerosis Society, and International Association for the Study of Obesity as a cluster of three out of five risk factors: high waist circumference (central adiposity), high fasting blood glucose, low levels of high-density lipoprotein (HDL) cholesterol, high blood triglycerides and high blood pressure.1 Having metabolic syndrome doubles an individual’s risk of developing atherosclerotic cardiovascular disease and increases the risk five-fold for Type 2 Diabetes Mellitus.1,2 There is growing evidence that the inflammatory response to adipose tissue, through obesity and metabolic syndrome, is linked to an increased risk of developing cancer.3,4 Around a quarter of the world’s population is now suspected to have metabolic syndrome, leading to higher healthcare utilisation and costs.5–7 Diagnosing metabolic syndrome brings an opportunity for early intervention to prevent the development of chronic disease.
Changing lifestyle behaviors through diet and increased physical activity is the first-line treatment for 26 chronic conditions, including metabolic syndrome.8 Physical activity improves the individual components that define metabolic syndrome, and ultimately, reduces the prevalence of the syndrome9–12 likely due to its impact on low-grade systemic inflammation.13 Additionally, interventions combining physical activity and dietary changes reduce waist circumference, blood pressure, triglycerides and fasting glucose levels for people with metabolic syndrome.14
Although diet and physical activity interventions appear to improve metabolic outcomes for people with metabolic syndrome, maintenance of improvements are reliant on long-term adherence to recommendations for effective management of the syndrome.15 However, initiating and maintaining lifestyle changes can be difficult. It has been observed that only 10% of people at risk of metabolic syndrome were adherent to physical activity lifestyle recommendations.16 For people with metabolic syndrome who enrolled in exercise interventions, short-term attrition rates were as high as 50%.17 People with metabolic syndrome have been identified as having lower health literacy18 and, in turn, may struggle to execute healthy behaviors. The relationship observed between depression and metabolic syndrome may also limit long-term adherence to exercise interventions.19 Therefore, a significant challenge for health care professionals and people with metabolic syndrome, is sustaining long-term behavior change to prevent and manage chronic disease.
Adherence to physical activity has been identified as a therapeutic behavior that appears to be enhanced through behavior change strategies.20 Considering the cost burden of metabolic syndrome,5 investments that improve adherence should be considered well spent through health benefits and savings in future healthcare utilisation. Previous reviews have investigated the effectiveness of interventions for reducing the risk of developing cardiovascular disease and diabetes for people with metabolic syndrome,21 lifestyle modification programmes for managing and reversing metabolic syndrome,14,22 and the impact of adherence to recommendations on outcomes,15 but none have focussed on the key issue of increasing adherence to recommendations to ensure the effect is optimised and maintained over time. Therefore, this review aims to determine which interventions enhance adherence to physical activity and/or exercise recommendations for people with metabolic syndrome.
Method
This systematic review was designed and reported following the Cochrane Handbook for Systematic Reviews of Interventions version 6.22623 and is reported consistent with the PRISMA guidelines.24 This review was registered prospectively with PROSPERO international register for systematic reviews (CRD42022267433).
Search Strategy
A search strategy was developed using medical subject headings (MeSH) and their synonyms for the concepts of metabolic syndrome, adherence, and exercise/physical activity (Appendix/Supplement 1). Electronic health databases (MEDLINE, PubMed, CINAHL, SPORTdiscuss and ProQuest) were searched from inception until July 2022. A manual search of reference lists of primary studies and citation tracking of included trials through Google Scholar were also completed. The results of each search were downloaded into an online platform, Covidence25 and duplicates were removed. Initial screening of eligibility based on titles and abstracts to remove clearly ineligible trials was conducted by two reviewers (AG and CP) independently with discrepancies resolved by a third reviewer (SM). All papers not excluded were then reviewed in full-text independently by the two reviewers, with discrepancies resolved by consensus. The agreement of the reviewers was calculated using the Kappa statistic where, 0.21–0.4 represents fair agreement, 0.41–0.6 suggests moderate agreement, 0.61–0.8 is substantial and 0.81–0.99 suggests near perfect agreement.26
Inclusion/Exclusion Criteria
Articles were included if they were randomized controlled trials published in English and investigated adults (18+) with metabolic syndrome as defined by the NCEP ATP III or the IDF1 (or country specific adapted versions). Eligible interventions aimed to increase adherence to physical activity guidelines or prescribed physical activity or exercise that intended to improve metabolic syndrome, regardless of whether it was delivered by a healthcare professional (eg physiotherapist, nurse), trained lay representative (eg expert patient groups or arthritis self-management groups) or as part of a multi-disciplinary programme (which may have included other interventions eg diet). To be included, trials must have included a usual care or control group and used clearly defined and reproducible measures of adherence to exercise or physical activity or measures of physical activity where these had been used as a proxy measure of adherence. This includes patient-reported or clinician-reported measures, objective measures of physical activity or exercise diaries (if converted to an adherence measurement scale).
Trials were excluded if they aimed to increase adherence to medication or dietary intervention only or if they reported adherence or predictors of adherence but did not evaluate an intervention aimed at improving adherence.
Data Extraction
Data were extracted using the Data Collection Form for Cochrane Reviews: RCTs only form, completed by one reviewer (AG) and checked for accuracy by a second reviewer (CP). Data from included trials were extracted on population (number of participants, age, gender, and metabolic syndrome risk factors), intervention (type, duration, and frequency) and adherence outcomes (physical activity/exercise amount, physical activity/exercise frequency, numbers of participants meeting guidelines etc.). Study authors were approached for missing data when applicable.
Risk of Bias
The Cochrane updated risk of bias tool (RoB2)27 was used to evaluate the risk of bias of each trial by two researchers independently (AG and NT). Using a fixed set of domains, the RoB2 considers aspects of bias such as the randomisation process, deviations from intended interventions, missing outcome data, bias through measurement of the study outcome and the selection of the reported result.27 Assessment then produces an overall judgement for each selected trial as “low risk”, “high risk” or “some concerns” of bias. The agreement between reviewers was calculated using the Kappa statistic.
Data Analysis and Synthesis
Descriptive analyses were completed as data were unable to be pooled in meta-analyses due to heterogeneity of interventions, outcomes, and missing data.
The Grading of Recommendation, Assessment, Development, and Evaluation (GRADE) framework28 was used to establish the overall certainty of the body of evidence for each intervention type based on guidelines for reviews without meta-analyses.29 As all studies were randomized controlled trials, the grading began at “high” and was downgraded one place if: more than half of the studies had at least “some concern” regarding risk of bias (methodological limitations); the population, intervention or outcomes were dissimilar to our research question (indirectness); results were imprecise because of low sample size (<400) or wide confidence intervals within studies (imprecision); there was inconsistency in the direction and magnitude of results between studies (inconsistency); or if there was likelihood of reporting bias if there were only small positive studies.29,30 Initial grading was completed by two reviewers independently (AG, SM) and disagreements resolved by consensus through discussion with a third reviewer (CP).
Results
The initial database search recovered 1316 papers with 1131 remaining following removal of duplicates. The first screening process eliminated 1079 clearly irrelevant papers based on titles and abstracts and 22 papers went to full text review. There was slight agreement between reviewers (Kappa 0.16, 95% CI 0.07 to 0.25) when screening titles and abstracts due to uncertainty of one reviewer on the difference between determinants of adherence and interventions to enhance adherence. Following clarification of inclusion criteria, there was moderate agreement (Kappa 0.43, 95% CI 0.05 to 0.80) between reviewers on full-text review that four trials met inclusion criteria for the review (Figure 1).
 |
Figure 1 PRISMA flow of trials through the review. |
Study Characteristics
Four randomized controlled trials31–34 were included with 428 participants, of whom, 203 (47%) were male and 258 participated in interventions to enhance their adherence to physical activity or exercise recommendations (Table 1).
 |
Table 1 Trial Characteristics |
Three of the four trials provided health education,32–34 which was accompanied by telemonitoring of physical activity and provision of written or telephone feedback in one trial,32 goal setting and monitoring via a mobile application in another trial,34 and small group counselling sessions focussed on goal setting and behavior change in the third trial.33 Participants in the final trial had individual face-to-face or telephone counselling sessions focussed on nutrition and physical activity goal setting and behavior change.31
The control group participants of all four trials received health education on metabolic syndrome from healthcare professionals, and control group participants in one trial33 also received a take-home booklet surmising risk factors, goal setting techniques and emotional management strategies.
Risk of Bias Assessment
According to the RoB2, three of the included papers were considered of “some concern” and one of “high risk” in relation to perceived potential bias (Figure 2). Agreement between reviewers was fair (Kappa = 0.32, 95% CI. 0.50 to 0.60). Outcome assessors were unblinded in three of the four trials31–33 and all trials elicited some concern of bias due to lack of description of outcome measure selection, data analysis plan and reporting of results.
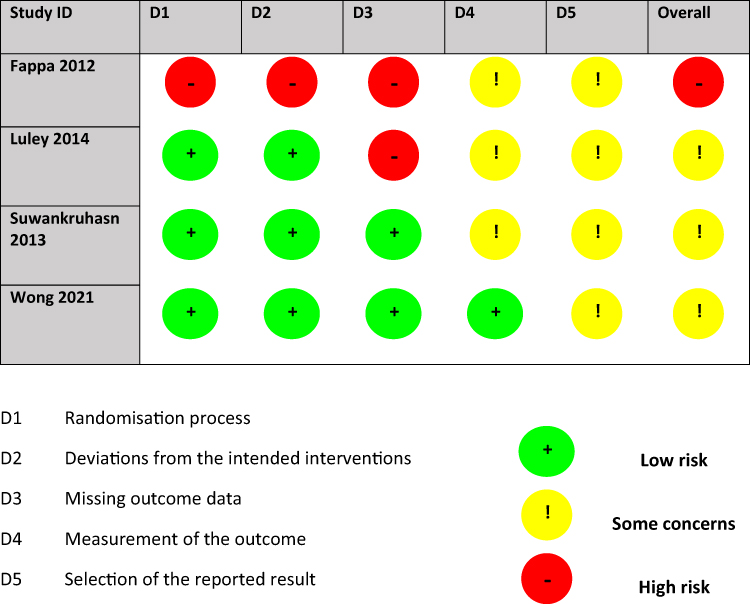 |
Figure 2 Risk of bias. |
Outcomes
One trial32 objectively measured physical activity levels using accelerometer data. Self-reported measures of physical activity used in the other trials were the Greek adjusted physical activity questionnaire (HAPAQ),31 the Physical Activity Log,33 and the Godin Shephard Leisure Time Physical Activity measure (GSLTPA)34 (Table 1).
Two trials31,32 did not report outcome data for physical activity despite measuring it and were not able to provide data despite requests from the reviewers, therefore, data were not able to be included in meta-analyses.
At three to four months, the attrition rate across three studies was 6% in the experimental groups and 13% in the control groups.32–34 At longer-term follow-up in one of these studies, attrition rates were 18% in the experimental group and 35% in the control group at 12-months.33 In the final study 41% of experimental group participants and 55% of control group participants were lost to follow-up at 6 months.31
Goal Setting
The interventions in two trials31,33 used goal setting counselling interventions delivered by dietitians to increase adherence to physical activity recommendations in 173 participants with metabolic syndrome. In one of the studies, participants self-selected physical activity goals during 6 × 2-hour small-group counselling sessions delivered over three months and found experimental group participants had significantly higher objectively measured physical activity levels at three- (ie post-intervention) and six-months (p<0.001).33 In the other study, seven 1:1 nutritional counselling sessions (20 to 60 minutes each) delivered over six months focussed on nutritional goals (and one pre-determined physical activity goal) found significant improvements in diet but no significant differences in physical activity at 6-months (ie post-intervention).31 Therefore, there was very low certainty evidence that goal setting interventions may improve adherence to physical activity recommendations over three to six months for people with metabolic syndrome (Table 2).
 |
Table 2 Summary of Findings |
Self-Monitoring and Feedback
Two trials32,34 used self-monitoring techniques and feedback to increase adherence to physical activity recommendations for 255 participants with metabolic syndrome. Telemonitoring plus regular feedback was reported to be effective at increasing adherence to physical activity recommendations over a 12-month period in one trial but raw data were not reported.32 Participants who used a mobile App with telemonitoring and feedback had moderate to large increases in exercise self-efficacy and moderate increases in physical activity compared to the control group at one (p = 0.029) and three (p = 0.038) months.34 Therefore, there was low certainty evidence that self-monitoring and feedback interventions increased adherence to physical activity interventions over 12 months for people with metabolic syndrome (Table 2).
Discussion
This systematic review of four trials with 428 participants found low certainty evidence that interventions involving monitoring and feedback increased adherence to physical activity recommendations in people with metabolic syndrome. There was very low certainty evidence that interventions involving goal setting and counselling may increase adherence. Results are somewhat congruent with literature in people with musculoskeletal disorders where self-management programmes including goal setting, monitoring and feedback35 and interventions aimed at increasing motivation36,37 have been found to increase adherence to exercise in people with musculoskeletal conditions while counselling and action coping plans did not improve adherence to long-term exercise and physical activity recommendations.36,37 With the exception of one study,31 attrition rates were lower in the included studies compared to what has previously been reported17 giving confidence that the behavior change interventions used were somewhat effective for maintenance.
This review focussed on adherence to exercise and physical activity, but all of the included trials also included a major focus on diet thus addressing pertinent lifestyle factors proven to have an impact on metabolic syndrome parameters. In one study31 participants increased their fruit consumption and their adherence to the Mediterranean diet while the remaining studies did not assess dietary intake34 or reported no significant differences.32,33 However, all studies reported improvements in metabolic outcomes likely from the combined effect of small changes in diet and physical activity. Half of the intervention group participants in two studies no longer had metabolic syndrome by the end of the intervention.31,32 Participants had reduced waist circumference,31,32,34 systolic blood pressure,33,34 fasting blood glucose,31–34 and triglycerides,31–33 and increased HDL-cholesterol.33 Therefore, with the addition of a dietary cointervention, the relatively small differences in physical activity adherence observed are likely to be clinically meaningful.
All of the included trials used strategies considered effective for behavior change. However, when used in isolation these may not address enough of the identified barriers. Previous research has identified that people with metabolic syndrome and low baseline levels of physical activity,38 higher body mass index,38,39 and older age38 were less likely to adhere to exercise and physical activity recommendations. On the other hand, people with access to walking routes and better self-rated health were more likely to adhere.40 In a qualitative study people with metabolic syndrome identified low motivation, low self-efficacy and lack of social support as barriers to adhering to exercise and physical activity recommendations.41 Because of the complex and multifaceted barriers to adherence in people with metabolic syndrome, future interventions may need to be more holistic to increase adherence.
If we consider the COM-B model of behavior change,42 effective interventions should address Capability, Opportunity and Motivation. For those who are sedentary or have mobility impairments, physical capability may need to be addressed with supervised exercise sessions. Compared to unsupervised and group exercise respectively, supervised and individual exercise have both been found to enhance adherence in people with musculoskeletal conditions.35 None of the included trials were delivered by exercise professionals (eg physiotherapists or exercise physiologists) and none included supervised exercise. Education and self-management strategies can enhance psychological capability and all included trials addressed this factor. Goal setting, monitoring and feedback were also features of all trials, which may have enhanced motivation. However, none of the included trials addressed opportunity by considering physical or social opportunities for physical activity. To enhance effectiveness, all components of the COM-B should be considered when designing interventions to address the multiple barriers that exist to ensure measurable improvements in lifestyle behaviors.
Limitations
This systematic review was conducted and reported following PRISMA guidelines and included independent screening and quality assessment. One limitation is the small number of randomized controlled trials identified and included and the lack of data reported within these trials which precluded meta-analysis. It is therefore difficult to draw strong conclusions from four randomized controlled trials.
Conclusion
This systematic review of four trials with 428 participants found that interventions involving goal setting, monitoring and feedback may have increased adherence to physical activity recommendations in adults with metabolic syndrome. Results should be interpreted with caution as there was low to very low certainty of evidence due to a lack of large, high-quality trials. Clinicians and researchers should consider using behavior change strategies such as goal setting, monitoring and feedback in interventions for people with metabolic syndrome to ensure short-term effects of lifestyle interventions on physical activity and exercise levels are maintained over time.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Alberti KG, Eckel RH, Grundy SM, et al. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation. 2009;120(16):1640–1645. doi:10.1161/CIRCULATIONAHA.109.192644
2. Grundy SM, Cleeman JI, Daniels SR, et al. Diagnosis and Management of the Metabolic Syndrome. Circulation. 2005;112(17):2735–2752. doi:10.1161/CIRCULATIONAHA.105.169404
3. Esposito K, Chiodini P, Colao A, Lenzi A, Giugliano D. Metabolic syndrome and risk of cancer: a systematic review and meta-analysis. Diabetes Care. 2012;35(11):2402–2411. doi:10.2337/dc12-0336
4. Garay-Sevilla ME, Gomez-Ojeda A, González I, Luévano-Contreras C, Rojas A. Contribution of RAGE axis activation to the association between metabolic syndrome and cancer. Mol Cell Biochem. 2021;476(3):1555–1573. doi:10.1007/s11010-020-04022-z
5. Boudreau DM, Malone DC, Raebel MA, et al. Health care utilization and costs by metabolic syndrome risk factors. Metab Syndr Relat Disord. 2009;7(4):305–314. doi:10.1089/met.2008.0070
6. O’Neill S, O’Driscoll L. Metabolic syndrome: a closer look at the growing epidemic and its associated pathologies. Obesity Reviews. 2015;16(1):1–12. doi:10.1111/obr.12229
7. Saklayen MG. The Global Epidemic of the Metabolic Syndrome. Curr Hypertens Rep. 2018;20(2):12. doi:10.1007/s11906-018-0812-z
8. Pedersen BK, Saltin B. Exercise as medicine – evidence for prescribing exercise as therapy in 26 different chronic diseases. Scandinavian J Med Sci Sports. 2015;25(S3):1–72.
9. Carroll S, Dudfield M. What is the Relationship Between Exercise and Metabolic Abnormalities? Sports Medicine. 2004;34(6):371–418. doi:10.2165/00007256-200434060-00004
10. Dieli-Conwright CM, Courneya KS, Demark-Wahnefried W, et al. Effects of Aerobic and Resistance Exercise on Metabolic Syndrome, Sarcopenic Obesity, and Circulating Biomarkers in Overweight or Obese Survivors of Breast Cancer: a Randomized Controlled Trial. J Clinical Oncol. 2018;36(9):875–883. doi:10.1200/JCO.2017.75.7526
11. Khan AA, Mundra PA, Straznicky NE, et al. Weight Loss and Exercise Alter the High-Density Lipoprotein Lipidome and Improve High-Density Lipoprotein Functionality in Metabolic Syndrome. Arterioscler Thromb Vasc Biol. 2018;38(2):438–447. doi:10.1161/ATVBAHA.117.310212
12. Wewege MA, Thom JM, Rye K-A, Parmenter BJ. Aerobic, resistance or combined training: a systematic review and meta-analysis of exercise to reduce cardiovascular risk in adults with metabolic syndrome. Atherosclerosis. 2018;274:162–171. doi:10.1016/j.atherosclerosis.2018.05.002
13. Della Guardia L, Codella R. Exercise tolls the bell for key mediators of low-grade inflammation in dysmetabolic conditions. Cytokine Growth Factor Rev. 2021;62:83–93. doi:10.1016/j.cytogfr.2021.09.003
14. van Namen M, Prendergast L, Peiris C. Supervised lifestyle intervention for people with metabolic syndrome improves outcomes and reduces individual risk factors of metabolic syndrome: a systematic review and meta-analysis. Metabolism. 2019;101:153988. doi:10.1016/j.metabol.2019.153988
15. Fappa E, Yannakoulia M, Pitsavos C, Skoumas I, Valourdou S, Stefanadis C. Lifestyle intervention in the management of metabolic syndrome: could we improve adherence issues? Nutrition. 2008;24(3):286–291. doi:10.1016/j.nut.2007.11.008
16. Alefishat EA, Abu Farha RK, Al-Debei MM. Self-Reported Adherence among Individuals at High Risk of Metabolic Syndrome: effect of Knowledge and Attitude. Med Princ Pract. 2017;26(2):157–163. doi:10.1159/000453037
17. Paley CA, Johnson MI. Abdominal obesity and metabolic syndrome: exercise as medicine? BMC Sports Sci Med Rehabil. 2018;10(1):7. doi:10.1186/s13102-018-0097-1
18. Peiris C, Harding K, Porter J, Shields N, Gilfillan C, Taylor N. Understanding the hidden epidemic of metabolic syndrome in people accessing community rehabilitation: a cross-sectional study of physical activity, dietary intake, and health literacy. Disabil Rehabil. 2022;1–9. doi:10.1080/09638288.2022.2065540
19. Pan A, Keum N, Okereke OI, et al. Bidirectional association between depression and metabolic syndrome: a systematic review and meta-analysis of epidemiological studies. Diabetes Care. 2012;35(5):1171–1180. doi:10.2337/dc11-2055
20. Sabate E. Adherence to Long Term Therapies. Evidence for Action. The World Health Organisation; 2003.
21. Dunkley AJ, Charles K, Gray LJ, Camosso-Stefinovic J, Davies MJ, Khunti K. Effectiveness of interventions for reducing diabetes and cardiovascular disease risk in people with metabolic syndrome: systematic review and mixed treatment comparison meta-analysis. Diabetes Obes Metab. 2012;14(7):616–625. doi:10.1111/j.1463-1326.2012.01571.x
22. Peiris CL, van Namen M, O’Donoghue G. Education-based, lifestyle intervention programs with unsupervised exercise improve outcomes in adults with metabolic syndrome. A systematic review and meta-analysis. Rev Endocr Metab Disord. 2021;22(4):877–890. doi:10.1007/s11154-021-09644-2
23. Higgins JPT, Thomas J, Chandler J, et al. Cochrane Handbook for Systematic Reviews of Interventions version 6.3. Cochrane. 2022;1:548.
24. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. 2021;10(1):89. doi:10.1186/s13643-021-01626-4
25. Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia. Available at www.covidence.org.
26. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159–174. doi:10.2307/2529310
27. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi:10.1136/bmj.l4898
28. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–926. doi:10.1136/bmj.39489.470347.AD
29. Murad MH, Mustafa RA, Schünemann HJ, Sultan S, Santesso N. Rating the certainty in evidence in the absence of a single estimate of effect. Evid Based Med. 2017;22(3):85–87. doi:10.1136/ebmed-2017-110668
30. Guyatt G, Oxman AD, Akl EA, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64(4):383–394. doi:10.1016/j.jclinepi.2010.04.026
31. Fappa E, Yannakoulia M, Ioannidou M, Skoumas Y, Pitsavos C, Stefanadis C. Telephone counseling intervention improves dietary habits and metabolic parameters of patients with the metabolic syndrome: a randomized controlled trial. Rev Diabet Stud. 2012;9(1):36–45. doi:10.1900/RDS.2012.9.36
32. Luley C, Blaik A, Götz A, et al. Weight loss by telemonitoring of nutrition and physical activity in patients with metabolic syndrome for 1 year. J Am Coll Nutr. 2014;33(5):363–374. doi:10.1080/07315724.2013.875437
33. Suwankruhasn N, Pothiban L, Panuthai S, Boonchuang P. Effects of a Self-management Support Program for Thai People Diagnosed with Metabolic Syndrome. Pacific Rim Int J Nursing Res. 2013;17(4):371–383.
34. Wong EML, Leung DYP, Tam HL, Wang Q, Yeung KW, Leung AYM. The Effect of a Lifestyle Intervention Program Using a Mobile Application for Adults with Metabolic Syndrome, versus the Effect of a Program Using a Booklet: a Pilot Randomized Controlled Trial. Clin Interv Aging. 2021;16:633–644. doi:10.2147/CIA.S303920
35. Jordan JL, Holden MA, Mason EE, Foster NE. Interventions to improve adherence to exercise for chronic musculoskeletal pain in adults. Cochrane Database Syst Rev. 2010;2010(1):Cd005956. doi:10.1002/14651858.CD005956.pub2
36. McLean SM, Burton M, Bradley L, Littlewood C. Interventions for enhancing adherence with physiotherapy: a systematic review. Man Ther. 2010;15(6):514–521. doi:10.1016/j.math.2010.05.012
37. Nicolson PJA, Bennell KL, Dobson FL, Van Ginckel A, Holden MA, Hinman RS. Interventions to increase adherence to therapeutic exercise in older adults with low back pain and/or Hip/knee osteoarthritis: a systematic review and meta-analysis. Br J Sports Med. 2017;51(10):791–799. doi:10.1136/bjsports-2016-096458
38. Abuissa H, Khanna A, Spertus J. Low rates of exercise in patients with metabolic syndrome after an acute coronary syndrome. Clin Cardiol. 2005;28(11):530–533. doi:10.1002/clc.4960281108
39. Jansen H, den Engelsen C, Rutten GE. Physical activity in patients with metabolic syndrome: at screening and three years thereafter. Metab Syndr Relat Disord. 2013;11(3):163–168. doi:10.1089/met.2012.0110
40. Colom A, Ruiz M, Wärnberg J, et al. Mediterranean Built Environment and Precipitation as Modulator Factors on Physical Activity in Obese Mid-Age and Old-Age Adults with Metabolic Syndrome: cross-Sectional Study. Int J Environ Res Public Health. 2019;16:5. doi:10.3390/ijerph16050854
41. Millstein RA, Huffman JC, Thorndike AN, et al. How Do Positive Psychological Constructs Affect Physical Activity Engagement Among Individuals at High Risk for Chronic Health Conditions? A Qualitative Study. J Phys Act Health. 2020;17(10):977–986. doi:10.1123/jpah.2019-0295
42. Michie S, Richardson M, Johnston M, et al. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med. 2013;46(1):81–95. doi:10.1007/s12160-013-9486-6
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Determinants of Non-Adherence to Exercise or Physical Activity in People with Metabolic Syndrome: A Mixed Methods Review
El Haddad L, Peiris CL, Taylor NF, McLean S
Patient Preference and Adherence 2023, 17:311-329
Published Date: 3 February 2023