Back to Journals » Advances in Medical Education and Practice » Volume 13
Basic Medical Sciences Knowledge Retention for Clinical Practice
Authors Goshu BT
Received 7 March 2022
Accepted for publication 28 April 2022
Published 9 May 2022 Volume 2022:13 Pages 475—482
DOI https://doi.org/10.2147/AMEP.S364631
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Bahiru Tenaw Goshu
Department of Anatomy, School of Medicine, University of Gondar, Gondar, Ethiopia
Correspondence: Bahiru Tenaw Goshu, Tel +251982076296, Email [email protected]
Background: The basis for studying the clinical sciences is the recall and comprehension of basic medical science facts. Do not, however, directly alter clinical information and as studies revealed that there are basic sciences knowledge retention of medical students gaps in clinical practice. The purpose of this study was to assess medical students’ basic medical sciences knowledge retention and a relevance of basic sciences knowledge for clinical for practice.
Methods: An institutional-based descriptive cross-section epidemiological study design was carried out in the University of Gondar from April to May of 2021. A total of 15 basic and clinical sets of questions were used for data collection. The data were entered and analyzed using SPSS version 20 to analyze data.
Results: A total of 191 medical students participated with response rate of 100%. Of these, 48.6% were male. Of all participant students, 69 (36.1%) have had the academic status of excellent with a commutative grade point average greater that 3.6 out of 4.0. Students who correctly responded for all categories of questions for basic and clinical sciences were 8.6± 2.7 and 5± 2.8 of second years, 5.5± 2.3 and 7.1± 1.2 of fourth years, 6.5± 1.4 and 6.7± 1.0 of fifth years, 5.3± 0.8 and 8.4± 2.5 of sixth years, respectively. As a representative year, the score of second year students’ performance for the basic sciences is a statistically significant with overall impact of the basic sciences (6.49± 2.5, F=12.51, P≤ 0.001) and clinical sciences (4.0± 1.9, F=14.73, P≤ 0.001).
Conclusion: It is proposed that basic sciences knowledge should be aligned with clinical sciences preparation so that students may grasp disease diagnosis and treatment concepts in an integrated manner.
Keywords: basic sciences, clinical sciences, knowledge retention, medical students
Introduction
Medical students develop their medical expertise on previously acquired basic medical sciences knowledge. Nonetheless, as medical students report, their recall and usage of basic sciences knowledge is not in standard of prediction, and curricula syllabus gives the impression of irrelevance to clinical practice.1 Medical students’ knowledge recall is considered a key issue.2 Unable to use what the students learned, and then the learned facts turn out to be inactive and inaccessible; finally, it leads to awareness difficulty.3–5
Regardless of the causal relation of basic and clinical knowledge, the strong link between preclinical and clinical year medical students’ knowledge of technical medical archives could be attributed to the reason that talented learners reached out each sets ofexposures.6 According to previous study, the general performance of medical students on written assessments tends to decline through time. This may vary with enduring rewards and the degree of early mastery implying that strong long-term memory is linked to competitive character learning behavior in the early stages and also the progressive use of various teaching methods.7
Basic medical science knowledge may be utilized to recall facts and to better grasp the causative pathways of disease processes, improving problem-solving excellence.8,9 Furthermore, to well comprehend the disease processes, knowledge offers a coherent theoretical foundation in which diagnostic information may be employed. A lack of assimilation of basic medical sciences with clinical sciences for practice may jeopardize the relevance of these disciplines.10,11
As a consequence, having a basic knowledge of medical science is essential for an enhanced conception of clinical sciences practice. As studies revealed that students with basic sciences knowledge have low recall habits.1,6,12
Furthermore, the medical students’ attitudes of basic science courses became progressively unfavorable. Despite this, research in India found medical students are enthusiastic about basic medical sciences.13,14
Therefore, most medical schools ambition is to change their curricula, thus it is thought that there was a need for particular medical evidence. Because they had been studying instances of applied fundamental technical know-how in the pre-medicine year as well as second year guides which were supposed to be accustomed to second year students. The current examination is aimed to check the degree of basic understanding of physiology and anatomy, as well as its influence on the level of clinical information standards amongst fifth and sixth year medical students. Moreover, it determines if basic technological standards are retained in the fourth, fifth, and sixth years. This will determine if senior students are provided with sufficient medical knowledge and insight into the causality of processes discovered, as well as the extent to which students’ comprehension may deteriorate with time. Therefore, the objective of this study was to assess medical students’ basic medical sciences knowledge retention and the relevance of basic sciences knowledge for clinical for practice.
Methods
Study Design, Setting and Period
An institution-based descriptive cross-sectional study design was conducted in University of Gondar medical students from April 25, 2021 to June 25, 2021. The University of Gondar has been serving the country since 1954. It has many programs. Of these, the school of medicine is one of the pioneer schools, which consists of about 1234 students.
Source and Study Population
Source Population
All second, fourth, fifth, and sixth years medical students at the University of Gondar were considered as the source population.
Study Population
All second, fourth, fifth and sixth years medical students at the University of Gondar who attended the classroom during data collection were considered as the study population.
Data Collection Procedure and Tools
Fifteen sets of open-ended questions were developed. The preliminary a part of the test consisted of questions about basic sciences, and the second part examined related clinical evidence. The order of questions was random, so that it would be much less obvious that they shaped 15 pairs. We created the questions in accordance to standard textbooks of anatomy and physiology. For clinical questions the clinical applications of textbooks chapters were used. A total of 30 questions were formed because it covered adequate understanding for analysis.
Each question pair represented an unmarried subject matter. The sample questions have been shaped in a way that the correct solution defined the physiological or anatomy history of the scientific query. Finally, there were seven anatomy and seven physiology questions in addition to one mixed question pair. Clinical related questions have been created in a way that basic sciences and clinical sciences questions were similarly familiar for all year’s categories of students. This became possible due to the fact the clinical standards practice was included through the anatomy and physiology textbooks for the second year.
Statistical Analysis
SPSS version 20.0 was used for data analysis. Mean standard deviation, frequency, ratio, and percentage, correlation coefficient, ANOVA, and coupled t-test were used. Level of statistical significance was at set at P<0.005.
Results
In this study, a total of 191 participants were joined, of these, 98 (51.3%) were females. Totally, in both sexes, 69 (36.1%) have had the academic status of excellent with cumulative grade point of greater than or equal to 3.6 out of 4.0 (Table 1).
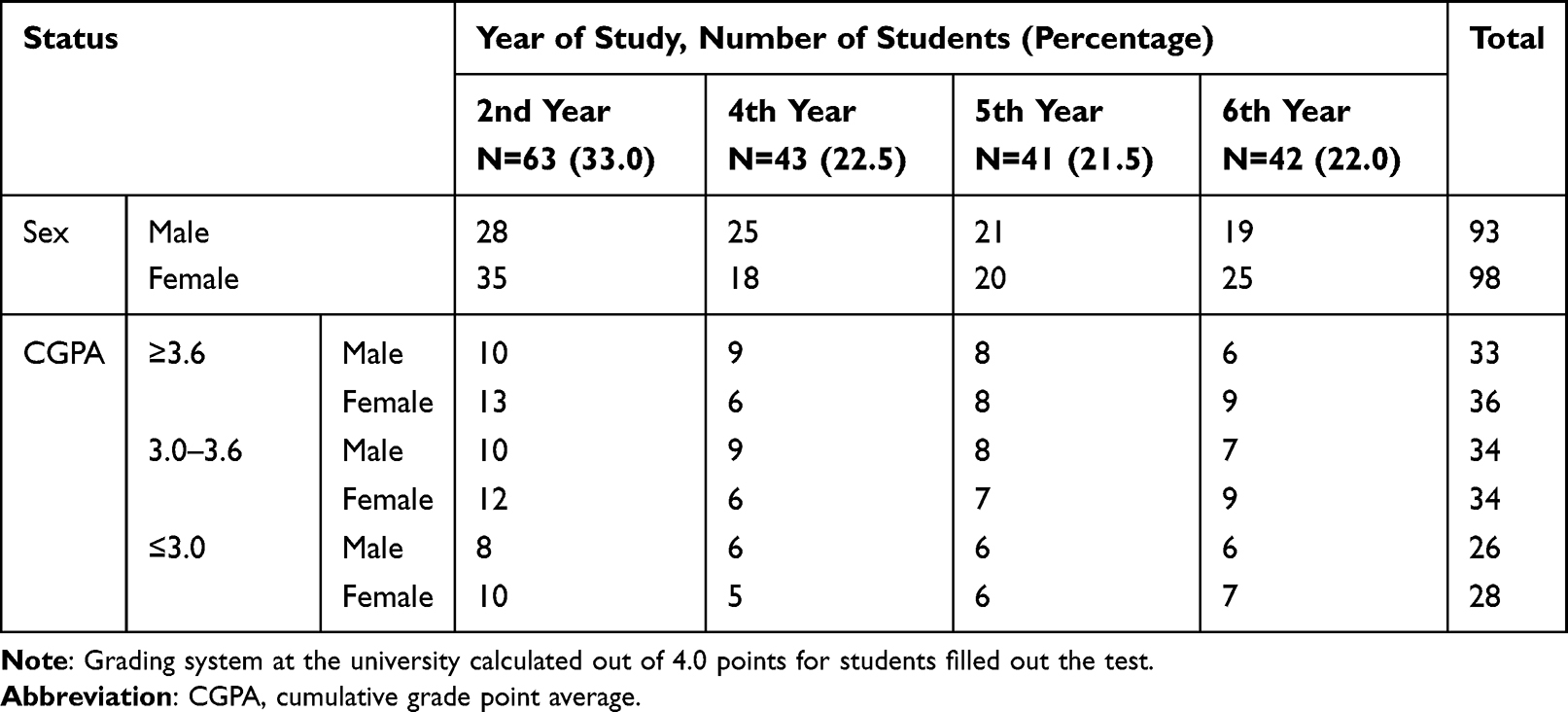 |
Table 1 Status of Medical Students Who Participated in this Research at the College of Medicine and Health Sciences, University of Gondar, Ethiopia, 2021 |
Mean number of accurate answers was 8.6±2.7 and 5.0±2.8, 5.5±2.3 and 7.1±1.2, 6.5±1.4 and 6.6±1.0, 5.3±0.8 and 8.4±2.5 for basic and clinical sciences questions responses of second, fourth, fifth, and sixth year students, respectively (Figure 1).
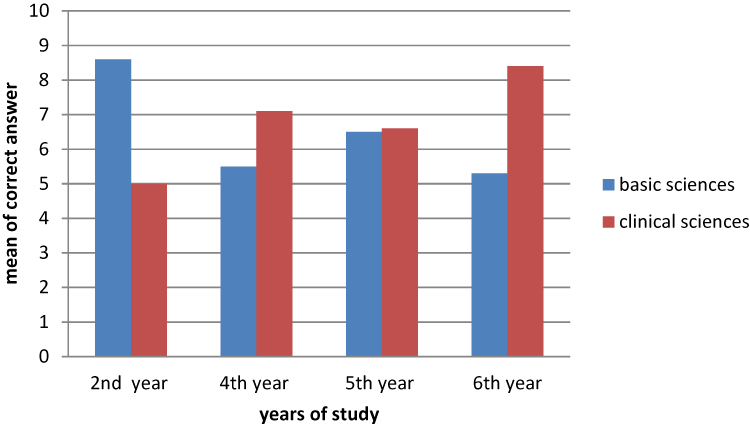 |
Figure 1 This figure revealed that the mean correctly answered questions of second, fourth, fifth, and sixth year’s medical students for basic and clinical oriented questions provided of University of Gondar, Ethiopia, 2021. |
There was a positive correlation between basic and clinical answers scores for second (r2=50.4%, P=0.0001) (Figure 2) and sixth year students (r2=42.6%, P=0.0001) (Figure 3), but a negative correlation for fourth year students (r2=18.8%, P=0.005), and no statistical significance correlation for fifth year students (r2=0%, P=0.819) (Figure 4). However, after reviewing the final data, no statistically significant link was found for all students (r2=0%, P=0.173). (Figure 5).
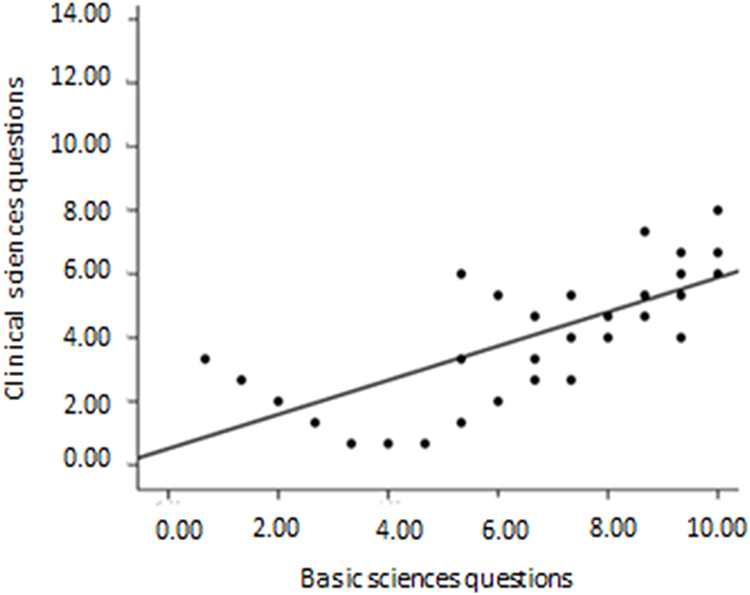 |
Figure 2 Basic and clinical questions answers scores of the second year students of the University of Gondar, Ethiopia, 2021. |
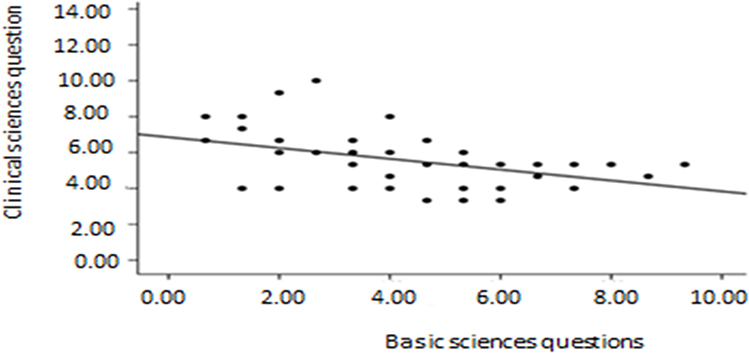 |
Figure 3 Basic and clinical sciences questions response scores of the sixth year students of the University of Gondar, Ethiopia, 2021. |
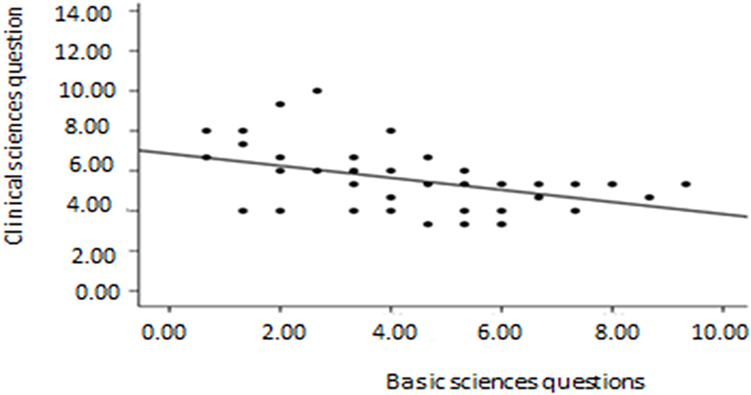 |
Figure 4 Basic and clinical sciences questions response scores of the fifth year students of the University of Gondar Comprehensive Specialized Hospital, Amhara, North West Ethiopia, 2021. |
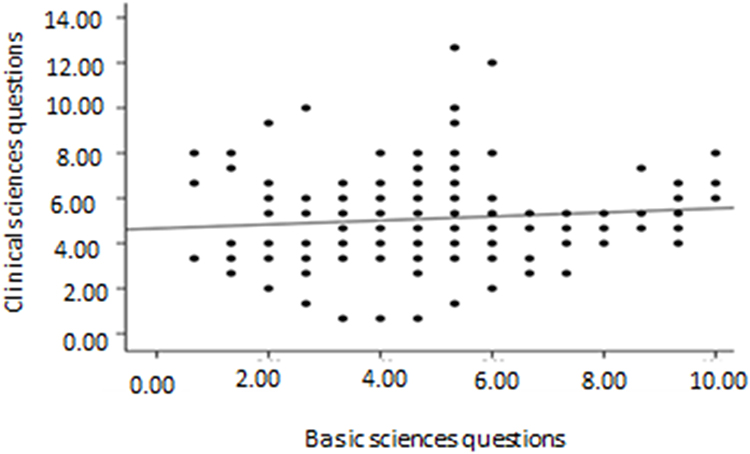 |
Figure 5 Basic and clinical questions response scores of all year medical students of the University of Gondar, Ethiopia, 2021. |
There was a statistically significant effect on test scores, suggesting that second and sixth year students performed better on the basic exam, while sixth year students performed better on the clinical test.
However, a statistically significant difference in scores, with fourth and sixth year students scoring lower on basic questions than second year students, but higher on clinical questions. In fifth-year students’ results, there was no statistically significant difference in clinical and basic sciences question scores (Table 2). Between male and female students, there was no difference in basic or clinical knowledge. When comparing basic question scores (5.01±2.48 and 5.10±1.99, respectively) and clinical question scores (5.43±2.03 and 5.14±2.03 respectively), there were no statistical differences between and within subjects’ ANOVA according to gender differences: females’ mean scores and males’ mean scores.
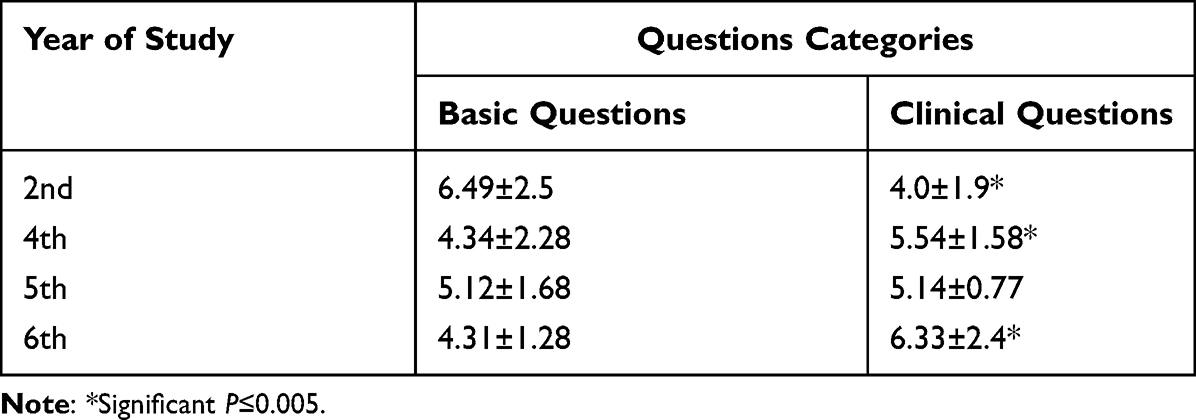 |
Table 2 Second, Fourth, Fifth, and Sixth Year Students Correct Response Mean Scores for Basic Sciences and Clinical Sciences Questions, University of Gondar, Ethiopia, 2021 |
Discussion
This topic has not before been addressed in Ethiopia, and it is especially vital for experts to exploring dynamic curriculum in various institute, as well as introducing alternative research interest area. The current findings revealed that clinical sciences practice is frequently nonheritable, despite a complete hold of its underlying basic science support. Hence, the present findings demonstrated that clinical year students earned enhanced scores on clinical questions, but they did not perform as well on basic sciences questions.
These results call into question that basic sciences had an impact on the triple-crown response to clinical sciences inquiries. If such a link existed, it would be ahead getting more quantifiable essential basic sciences knowledge. Clinical facts are not always recalled alongside the corresponding fundamental data, but remembered independently. The possible reason for unfortunate essential information in clinical year students might be due to lack of in-depth contents of clinical textbook for basic sciences facts and early exposure for basic sciences and a gradual decline in recall.
Conversely, clinical year students are bombarded with numerous scientific data that must be learned, and they look to be losing their grasp on basic concepts as time goes on. The loss of data does not appear to be linked to final test grades, the quality of the assessment made by learners, or even gender differences. Previous research has shown that medical performance may be improved. Pearson correlation between clinical and basic sciences, therefore, immeasurable basic responses on written data exams across all year students frequently decreases over time, which most likely varies with in-progress.7
According to Giles et al,15 when compared to audibly provided teaching aids, visual content was processed more quickly initially, but after four months, there was no variance in these two methods. The atmosphere in early learning classrooms was centered on techniques and comprehension rather than memorizing, with plenty of time to explain particularly difficult materials and purposely successful engagement with practice. This indicates that while cramming is negative in the long run, it might help you earn higher test scores in the short-term.16
Determinant variables in post-secondary information retention, such as taking subsequent courses (reinforcement) and initial “active” learning were recognazed. Initial learning is certainly insufficient for long-term retention, but it is important for elements such as distributed, growing, elaborative rehearsal of knowledge based on recollection. The content does not need to be recognized or represented. Data loss should not be attributed just to a lack of factual content; rather, it should be linked to the program’s inability to increase data over time, as each initial learning and spaced usage are critical for memory.17–21
As a result of the well-organized information, active learning method users will be facilitated as future medical school advancement of course deliveries and clinical practice. Even though certain clinical reasoning studies found that there was no evidence that those practitioners utilized basic medical science knowledge for routine clinical practice,8 basic science was more memorable because of its abstract coherence, and it assisted students in reconstructing the alternatives of particular illness classes after the original symptom lists were lost.22
Clinical management might serve as an example of the use of fundamental data. In this discipline, light-emitting diode data from fundamental sciences is amplified to get a better knowledge of pathophysiological mechanisms.7 It is important to note that, as prior research has shown, strong memory is linked to over-learning in the first portion and, as a result, the regular updating and transmission of learning resources across extended periods of time.18
Research has discovered that a primary concentration on definition of terms and understanding rather than recall, as well as appropriate time to be taught (particularly of hard content) and purposeful successful participation with activities (practice), are all important factors in promoting early learning.23 The priority ascribed to basic medical science knowledge by the two participants may also play a role in the distinction between second and clinical year students.24
The discovery that clinical data is not fundamentally static in terms of comprehending underlying processes necessitates future research efforts aimed at uncovering components required for triple-crown execution of health care service.18 The factors such as variation in curricula, learning methods, and students ‘attention have an influence in relationship between basic and clinical medical sciences. The goal would be a collaborative research work with aim of incorporating all medical sciences.26
Although medical sciences (basic and clinical) knowledge among fifth year students were no significant statistically, the preclinical (basic) medical science knowledge score was lower than that of second-year students, but higher than that of fourth and sixth years. Statistically nonsignificant variation in knowledge in all categories of questions could be due to personal variation and courses overburden wherever the students learning clinical sciences, all of which require a lot of effort.24–26 Medical schools should have a closed internal control system in place, with a highly objective committee judging and establishing educational requirements for their pupils. Because the final word criteria have been discussed, written, and rewritten, the academic efficacy is tied to the teaching offered and to the health service quality provided to customers.27
Conclusion
This study has provided baseline data to propose that basic sciences knowledge should be aligned with clinical sciences preparation so that students may grasp disease diagnosis and treatment concepts on an integrated manner. Therefore, medical school curriculum should integrate basic and clinical sciences course starting from scratch.
Ethical Considerations
Ethical clearance was gained from the University of Gondar, school of medicine, proposal review committee (reference number 589/05/2021). All respondents of this study provided an informed consent and has gained consent from respondents after a detailed explanation of the purpose, benefit, and risk of the study.
Acknowledgments
My appreciation goes to school of medicine, University of Gondar providing this opportunity to carry out this research work. I want to express my gratitude to study participants.
Disclosure
The author reports no conflicts of interest in this work.
References
1. D’ Eon MF. Knowledge loss of medical students on first year basic science courses at the University of Saskatchewan. BMC Med Educ. 2006;6:5. doi:10.1186/1472-6920-6-5
2. Cate O, Snell L, Mann K, Vermunt J. Orienting teaching toward the learning process. Acad Med. 2004;79:219–228. doi:10.1097/00001888-200403000-00005
3. Sanson-Fisher R, Rolfe I. The content of undergraduate health professional courses: a topic largely ignored? Med Teach. 2000;22:564–567. doi:10.1080/01421590050175532
4. Ellis JA, Semb GB, Cole B. Very long-term memory for information taught in school. Contemp Educ Psychol. 1998;23:419–433. doi:10.1006/ceps.1997.0976
5. Harden RM. Approaches to curriculum planning. Med Educ. 1986;20:458–466. doi:10.1111/j.1365-2923.1986.tb01193.x
6. Lazić E, Dujmović J, Hren D. Retention of basic sciences knowledge at clinical years of medical curriculum. Croat Med J. 2006;47(6):882–887.
7. Halpern DF. Thought and Knowledge: An Introduction to Critical Thinking. Mahwah, NJ: Lawrence Erlbaum Associates; 2003.
8. Woods NN, Brooks LR, Norman GR. The value of basic science in clinical diagnosis: creating coherence among signs and symptoms. Med Educ. 2005;39(1):107–112. doi:10.1111/j.1365-2929.2004.02036.x
9. Woods NN, Brooks LR, Norman GR. The role of biomedical knowledge in diagnosis of difficult clinical cases. Adv Health Sci Educ Theory Pract. 2007;12:417–442. doi:10.1007/s10459-006-9054-y
10. Woods NN, Neville AJ, Levinson AJ, Howey EH, Oczkowski WJ, Norman GR. The value of basic science in clinical diagnosis. Acad Med. 2006;81(Suppl):S124–S127. doi:10.1097/00001888-200610001-00031
11. Ginzburg SB, Brenner J, Cassara M, Kwiatkowski T, Willey JM. Contextualizing the relevance of basic sciences: small-group simulation with debrief for first- and second-year medical students in an integrated curriculum. Adv Med Educ Pract. 2017;8:79–84. doi:10.2147/AMEP.S124851
12. Norman G. The essential role of basic science in medical education: the perspective from psychology. Clin Invest Med. 2000;23(1):47–51.
13. Alam A. How do medical students in their clinical years perceive basic sciences courses at King Saud University? Ann Saudi Med. 2011;31:58–61. doi:10.4103/0256-4947.75780
14. Gupta S, Gupta AK, Verma M, Kaur H, Kaur A, Singh K. Students’ perceptions of basic science subjects. Int J Appl Basic Med Res. 2014;4:16–19.
15. Giles RM, Johnson MR, Knight KE, Zammett S, Weinman J. Recall of lecture information: a question of what, when, and where. Med Educ. 1982;16:264–268. doi:10.1111/j.1365-2923.1982.tb01262.x
16. Sissons JC, Swartz RD, Wolf FM. Learning, retention and recall of clinical information. Med Educ. 1992;26:454–461. doi:10.1111/j.1365-2923.1992.tb00205.x
17. Patel VL, Groen GJ, Scott HM. Biomedical knowledge in explanations of clinical problems by Medical students. Med Educ. 1988;22:398–406. doi:10.1111/j.1365-2923.1988.tb00774.x
18. Bransford JD, Brown AL, Cocking RR, editors. How People Learn: Brain, Mind, Experience, and School. Washington, DC: National Academy Press; 2000.
19. Baddeley A. Human Memory: Theory and Practice.
20. Regehr G, Norman GR. Issues in cognitive psychology: implications for professional education. Acad Med. 1998;71:988–1001. doi:10.1097/00001888-199609000-00015
21. Gardiner JM, Gawlik B, Richardson-Klavehn A. Maintenance rehearsal affects knowing, not remembering; elaborative rehearsal affects remembering, not knowing. Psych Bulletin Rev. 1994;1:107–110. doi:10.3758/BF03200764
22. Zanchetti A. The basic importance of the physiological approach in clinical medicine: the experience in the area of hypertension. Arch Ital Biol. 2005;143:97–102.
23. Rudland JR, Rennie SC. The determination of the relevance of basic sciences learning objectives to clinical practice using a questionnaire survey. Med Educ. 2003;37:962–965. doi:10.1046/j.1365-2923.2003.01671.x
24. Koens F, Rademakers JJ, Ten Cate OT. Validation of core medical knowledge by postgraduates and specialists. Med Educ. 2005;39:911–917. doi:10.1111/j.1365-2929.2005.02246.x
25. Gonnella JS, Hojat M, Erdmann JB, Veloski JJ. Assessment Measures in Medical School, Residency, and Practice: The Connections. New York: Springer; 1993.
26. O’Brien K, Crespo L, Wallach P, Elnicki M. Internal Medicine Clerkship Directors’ opinion regarding clinical input in the preclinical years: the 2002 CDIM basic science survey results. Teach Learn Med. 2006;18:105–109. doi:10.1207/s15328015tlm1802_3
27. Bligh J. Learning about science is still important. Med Educ. 2003;37:944–945. doi:10.1046/j.1365-2923.2003.01703.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Impact of Audience Response System in Enhancing Teaching of Anatomy and Physiology for Health Sciences Students at King Saud bin Abdulaziz University for Health Sciences
Baashar A, Kumar RS, Akhtar SMI, Alyousif SM, Alhassan AI, Townsi N
Advances in Medical Education and Practice 2023, 14:421-432
Published Date: 25 April 2023