")
Back to Journals » Vascular Health and Risk Management » Volume 19
Barriers to Participation in Cardiac Rehabilitation Among Patients with Coronary Heart Disease After Reperfusion Therapy: A Scoping Review
Authors Sugiharto F , Nuraeni A , Trisyani Y , Melati Putri A , Aghnia Armansyah N
Received 12 June 2023
Accepted for publication 17 August 2023
Published 31 August 2023 Volume 2023:19 Pages 557—570
DOI https://doi.org/10.2147/VHRM.S425505
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Pietro Scicchitano
Firman Sugiharto,1 Aan Nuraeni,2 Yanny Trisyani,2 Azalia Melati Putri,1 Nuraulia Aghnia Armansyah1
1Faculty of Nursing, Universitas Padjadjaran, Sumedang, Jawa Barat, Indonesia; 2Department of Critical Care and Emergency Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, Jawa Barat, Indonesia
Correspondence: Firman Sugiharto, Faculty of Nursing, Universitas Padjadjaran, Jl. Raya Ir. Soekarno KM. 21, Hegarmanah, Jatinangor, Sumedang, West Java, 45363, Indonesia, Tel +6282218235600, Fax +6282287793411, Email [email protected]
Abstract: Patients with coronary heart disease (CHD) experience many barriers to participate in cardiac rehabilitation (CR) programs. Several studies identify barriers that can affect participation in CR among patients with CHD after reperfusion therapy. However, there has yet to be a review specifically in this population. This review aims to identify the literature systematically that analyzes the barriers that affect the participation of CHD patients after reperfusion therapy in implementing the CR program. This study used the Preferred Reporting Item for PRISMA Extension for Scoping Reviews (PRISMA-ScR) with databases PubMed, ScienceDirect, EBSCO-hosted Academic Search Complete, Scopus, Taylor & Francis, and Sage Journals. The keywords used in English were “coronary artery disease OR myocardial infarction OR cardiovascular disease OR heart disease” AND “Barrier OR obstacle”, AND “percutaneous coronary intervention OR PCI OR angioplasty OR coronary artery bypass graft surgery OR CABG” AND “cardiac rehabilitation OR rehabilitation OR recovery”. The inclusion criteria in this review were full-text articles in English, articles with a descriptive, cross-sectional, and cohort design with a minimum of 100 participants that discussed barriers to participation in patients with CHD after undergoing reperfusion therapy, and the CR phases such as I, II, III, and IV have also been identified. Based on the initial search, there are 23 relevant studies out of 7400. The results of this study reported that most of the participants from the studies analyzed had a low level of participation in CR (≤ 50%). We classify the factors that affect the level of CR participation into five categories: individual factors, health history, environmental, logistical, and health system. The most reported barriers in each category were age, comorbidities, lack of support from friends, family and health workers, distance or travel time, and cost and economic status. Professional health workers, especially nurses, can identify various barriers that patients feel so that they can increase their participation in attending CR.
Keywords: cardiac rehabilitation, coronary heart disease, patient participation, reperfusion
Introduction
Coronary heart disease (CHD) is still a significant health problem with high morbidity and mortality rates in various countries.1 Globally, as many as 244.1 million people were living with ischemic heart disease (IHD) in 2020.2 Based on data recorded in 2020, the death rate caused by this disease reached 112.37 per 100,000 with the highest IHD mortality rate occurring in North Africa and Middle East, Eastern Europe and Central Asia regions.2 Unfortunately, according to World Health Organization (WHO), this mortality rate is expected to continue to increase to 24.2 million people in 2030.3
Reperfusion therapy is one of the solutions to reduce the morbidity and mortality of patients with CHD.2 This therapy aims to restore blocked blood flow through the coronary arteries with good standard and quality.2 Over the past ten years, several evidence has supported using reperfusion therapy to reduce morbidity and mortality in CHD patients.4 However, despite the many benefits of this therapy, patients undergoing reperfusion therapy often experience adverse cardiovascular events (MACE), which increase the length of hospitalization and lead to death.5,6 Thus, ensuring adequate precautions are taken to reduce complications and improve the prognosis of CHD patients who have undergone reperfusion therapy is essential.7–9
Cardiac rehabilitation (CR) is an interdisciplinary and comprehensive secondary prevention care model that effectively reduces mortality and MACE rates in patients with CHD after reperfusion therapy.10,11 Previous reviews have proven that CR can significantly be reduced all-cause mortality by 13%-26%, cardiac death by 20%-36%, recurrent infarction by 25–47%, and some by other risk factors.12 CR can also delay the development of atherosclerosis, even reverse plaque formation and prevent arterial blockage by a thrombus.13
CR programs consist of physical training and education focused on risk factor management, lifestyle and its modification, nutritional therapy, psychological support, and pharmacotherapeutic adherence.14 The European Society of Cardiology, the American Heart Association, and the American College of Cardiology recommend that patients with CHD after reperfusion therapy undergo a CR program.15 However, the application of CR still needs to be improved due to low patient participation.10,11,13,16
Participation and compliance in the implementation of CR are essential for patients with CHD, especially for those who have undergone reperfusion therapy.16–19 Hence, low participation rates in CR programs worry cardiologists and healthcare workers.20 Currently, the participation of patients with CHD in CR programs is lower than expected.20,21 The CR program dramatically influences the quality of life and patient prognosis.20,22–24 As explained in two previous cross-sectional studies, low CR participation can be related to various factors, including age, gender, lack of knowledge, cost, transportation, self-efficacy, motivation, social support, type of exercise, travel time, and CR schedule.11,25 However, obtaining comprehensive data related to CR barriers requires review, and as far as researchers have identified, reviews related to this matter are still scarce.
Several reviews have found barriers related to participation in CR. However, the literature review regarding barriers to patients with CHD participating in CR after undergoing reperfusion therapy still needs to be explored. Differences in barriers to CR participation in developing and developed countries are not yet clear. However, several previous studies stated that barriers related to gender roles, especially women, distance to health service locations, and ability to drive have been suggested to explain the variability of CR participation in a developing country.26 Besides, studies conducted in developed countries report age, personal barriers (health beliefs, limited time, and knowledge), previous medical history, and the health insurance program as barriers that influence CR participation.27,28 Recent systematic review found that patients with comorbidities20 and women had lower CR participation rates.29 However, previous reviews still had some limitations, that is (a) the previous research only focused on the female population;29 (b) previous systematic reviews did not evaluate the quality of the included studies;20,29 and (c) the characteristics of the participants from the articles analyzed are still heterogeneous.20 Because there has not been a review specifically identifying this population, this study aims to identify barriers to participation in the CR program in patients with CHD who have undergone reperfusion therapy. Furthermore, the extent to which the research has succeeded in identifying these barriers can provide recommendations for strategies and improvement of CR services to improve the participation of CR in patients with CHD after undergoing reperfusion therapy.
Materials and Methods
Design
The design used in this study is a scoping review. A Scoping review is a flexible methodological technique for exploring new, rapidly developing topics.30 This design has a more comprehensive conceptual range so that it can explain a variety of relevant study results. The framework of scoping review consists of 5 core stages, namely identifying research questions, identifying relevant study results, selecting studies, mapping data, compiling, summarizing and reporting results.30
Eligibility Criteria
The process of selecting articles for this review was carried out by five reviewers based on the PRISMA Extension for Scoping Reviews (PRISMA-ScR) (see Figure 1).31 Research questions and eligibility criteria for research articles use the PCC (Population, Concept, and Context) approach.
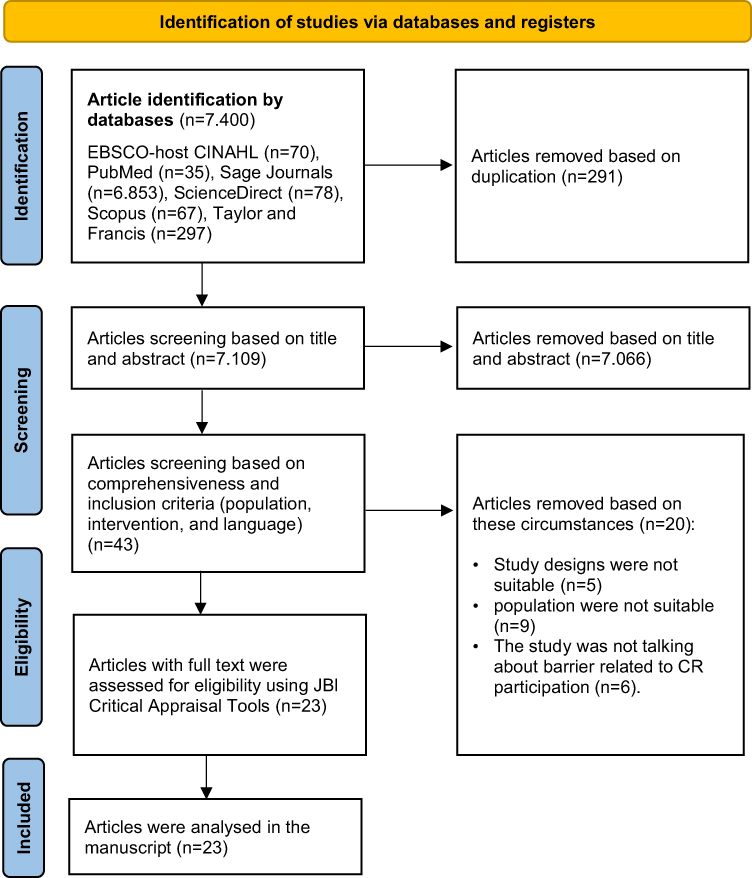 |
Figure 1 PRISMA flow diagram. Notes: Adapted from Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Creative Commons.31 |
P (Population): Patients with CHD
C (Concept): Patients with CHD who have undergone reperfusion therapy (PCI, Angioplasty, and CABG)
C (Context): Barriers to participation in cardiac rehabilitation programs.
This review excluded non-English language studies, inaccessible full-text publications and secondary research. The inclusion criteria in this review were full-text articles in English, articles with a descriptive, cross-sectional, and cohort design that discussed barriers to participation in patients with CHD after undergoing reperfusion therapy, the CR phases such as I, II, III, and IV have also been identified, as this criterion may present different barriers to participation. In addition, another inclusion criterion of this review is a minimum of 100 patients participating in the study. This aims to reduce bias in the results of the research. Then, this study has no limit on the year of publication because it looks at the barrier to participation in a comprehensive cardiac rehabilitation program.
Data Collection and Analysis
Search Strategy
The literature search process was carried out systematically using six primary databases: PubMed, ScienceDirect, EBSCO-hosted Academic Search Complete, Scopus, Taylor & Francis, and Sage Journals. The keywords used were “coronary artery disease OR myocardial infarction OR cardiovascular disease OR heart disease” AND “barrier OR obstacle” AND “percutaneous coronary intervention OR PCI OR angioplasty OR coronary artery bypass graft surgery OR CABG” AND “cardiac rehabilitation OR rehabilitation OR recovery”. For each term verified by MeSH (Medical Subject Headings), synonyms are used to retrieve all possible relevant articles. In addition, the author uses the Boolean operators “AND” and “OR” to trim or expand the search results for various tenses.
Study Selection and Quality Appraisal
Three independent authors selected studies that met the eligibility criteria. The authors checked for duplication in the initial selection process using Mendeley’s reference manager. It then checks the title, abstract and full text for relevance to the research topic and establishes inclusion and exclusion criteria by three authors to review independently screened records. In the final process, the authors checked each complete text with the Joanna Briggs Institute (JBI) critical assessment checklist.32 Following the assessment, we eliminated any studies with a JBI score < 70%. Furthermore, the first, second and third authors provide a decision if there is a discrepancy in the selection results. We experienced no differences of opinion regarding the feasibility of the study.
Data Extraction and Analysis
Data extraction was carried out using an extraction table to describe all results related to the topics discussed. Information is presented in tables relating to the characteristics of each study: study design, country, age (mean ± SD), participants, and findings (barriers, participation rate, types, phase of CR, and PR measuring tool). All included studies were primary studies with descriptive, cohort and cross-sectional designs. Therefore, data analysis was carried out thematically with a descriptive exploratory approach. The process of data analysis begins with the identification and presentation of the data obtained in tabular form based on the articles reviewed. After obtaining the data, all authors analyzed and explained each finding based on the barriers to participation in CR programs in patients with CHD who had undergone reperfusion therapy.
In the participation level, the authors divided the participation rate into three categories, namely low (≤50%), moderate (51–75%), and high (>75%). It was categorized as low if less than or equal to 50% of respondents participated in the CR. In addition, it is said to be moderate if the participation rate ranges from 51% to 75%, and then it is categorized as high if more than 75% of the respondents participated in the CR. CR participation in this study was based on the total number of participating patients and at least one CR session.
Results
Study Selection
The initial stage of identification from several databases obtained 7400 studies. Next, the authors screened the studies based on title, abstract, and inclusion criteria so that the remaining 43 studies. Furthermore, the authors screened 43 full-text articles and excluded 20 studies based on inclusion criteria. Then, the authors assess the quality of the article using JBI critical appraisal tools. As a result, the authors included 23 studies in this review after a quality assessment of the articles to be analyzed. Figure 1 depicts the number of studies retrieved using the PRISMA flow chart diagram.
Study Characteristics
The authors identified a cohort and cross-sectional study in the CHD population undergoing reperfusion therapy. Most of the studies analyzed in this review were cohort studies (n = 16). Almost all of the articles analyzed came from developed countries, including Australia (n=3), USA (n=4), Czech Republic (n=1), Canada (n=3), Belgium (n=1), China (n=2), United Kingdom (n=2), Portugal (n=1), Korea (n=3), Norway (n=1), Singapore (n=1), and one study was conducted in developing countries namely, Malaysia (n=1) (see Table 1). The participants (n=297,791) of the study analyzed were patients with CHD who had undergone reperfusion therapy with an average age of 54–68.9 years. The results of the JBI analysis show that most of the studies analyzed used cross-sectional and cohort methods. This method has the disadvantage of identifying confounding factors, and strategies to address these often need to be included. In addition, in the cohort studies analyzed, some studies still need to include and explain follow-up treatment strategies.
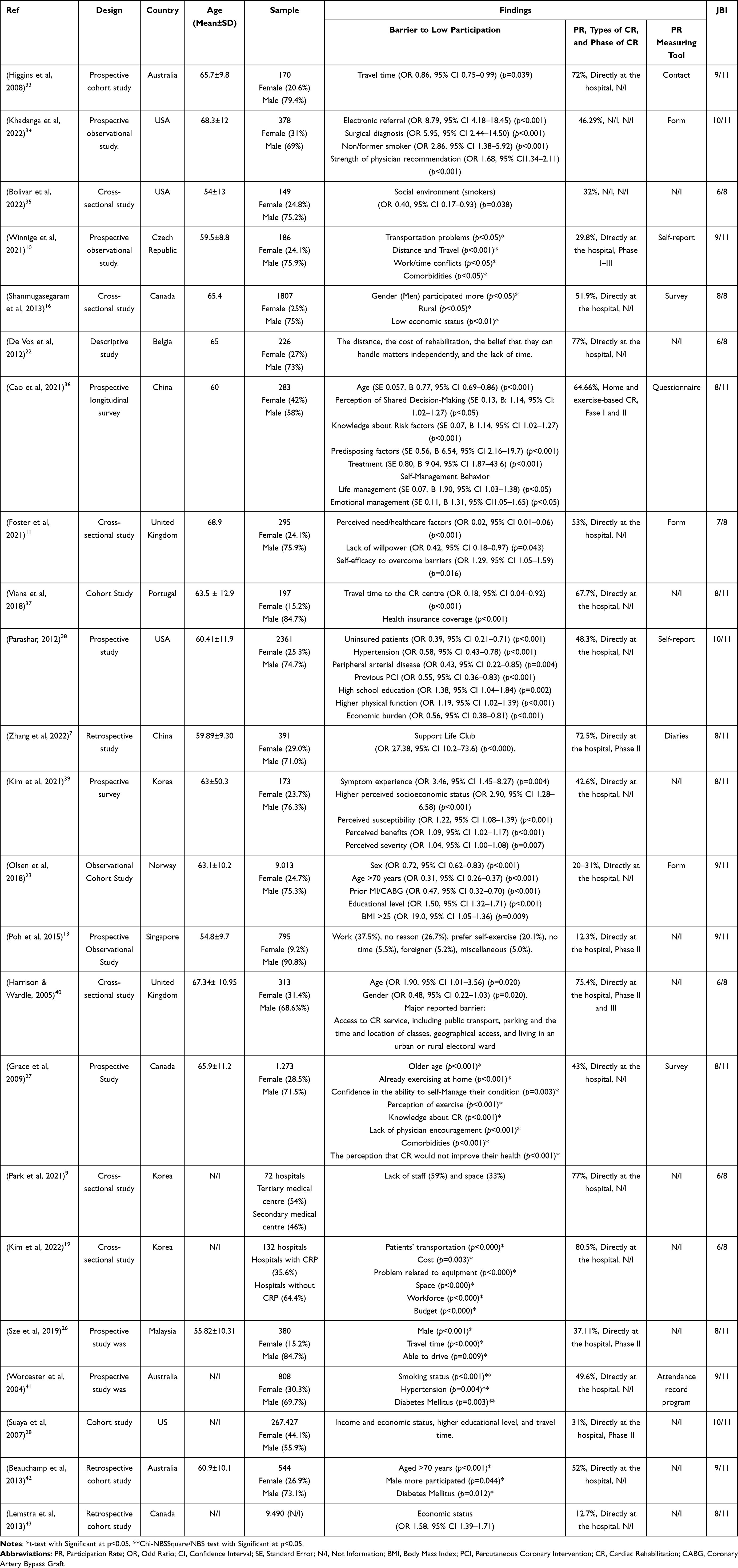 |
Table 1 Characteristics of Study |
Participation in Cardiac Rehabilitation
Based on the review results, the 23 studies analyzed did not categorize the participation rate of patients with CHD in attending CR. However, in the participation level section, the authors divide the participation rate into three categories they are low respondents participation in CR (≤50%), moderate (51–75%), and high (>75%) (see Table 2). Based on the categorization of participation rates in CR, it shows that most of the studies analyzed show a low participation rate (n=12),10,13,23,26–28,34,35,38,39,41,43 moderate participation rate (n=7),7,11,16,33,36,37,42 and a high participation rate CR (n=4).9,19,22,40
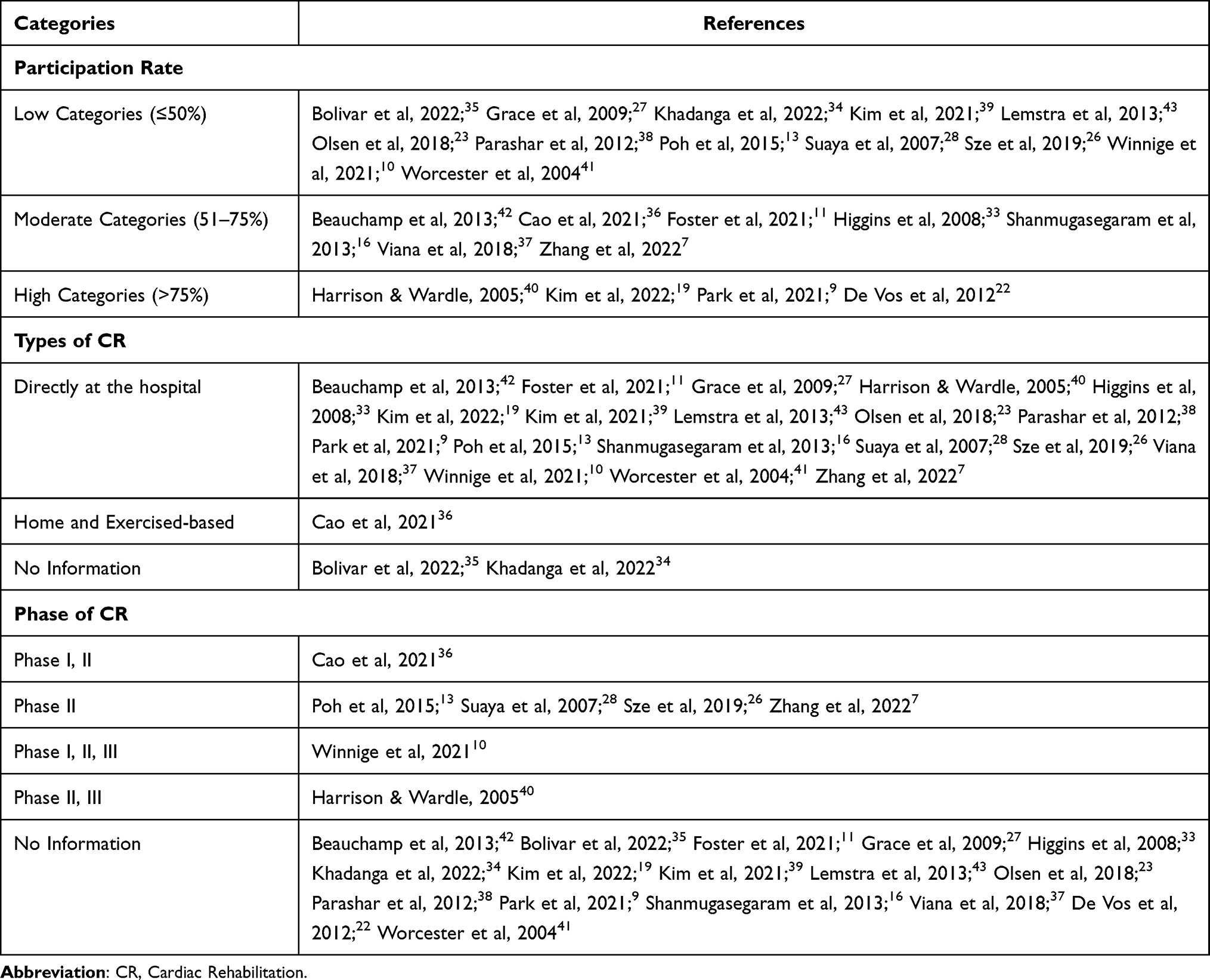 |
Table 2 Categories of Participation in Cardiac Rehabilitation |
Furthermore, most CR program types undertaken by participants from the studies were carried out in hospitals7,9–11,13,16,19,23,26–28,33,37–43 and only the study by Cao et al, 2021 which report home and exercise-based CR with most of the participants had a moderate participation rate (64.66%).36 Furthermore, two studies did not mention the type of CR program.34,35 In addition, most of the studies did not include the specific CR phase category of the participants,9,11,16,19,22,23,27,33–35,37–39,41–43 some others are divided into phase II,7,13,26,28 phase I, II,36 Phase I, II, III,10 and Phase II, III.40
Barriers to Participation in Cardiac Rehabilitation
Barriers to participation in CR among patients with CHD after reperfusion therapy are classified into five categories: barriers from the individual, health history, environment, logistics, and health system (see Table 3). Variables from individual barriers include age, gender, health perceptions and beliefs, lack of time, work conflict, knowledge, self-management behavior, educational level, and lack of motivation. Meanwhile, barriers to the health history category include prior revascularization, prior MI, surgical diagnosis, comorbidities, and physical status.
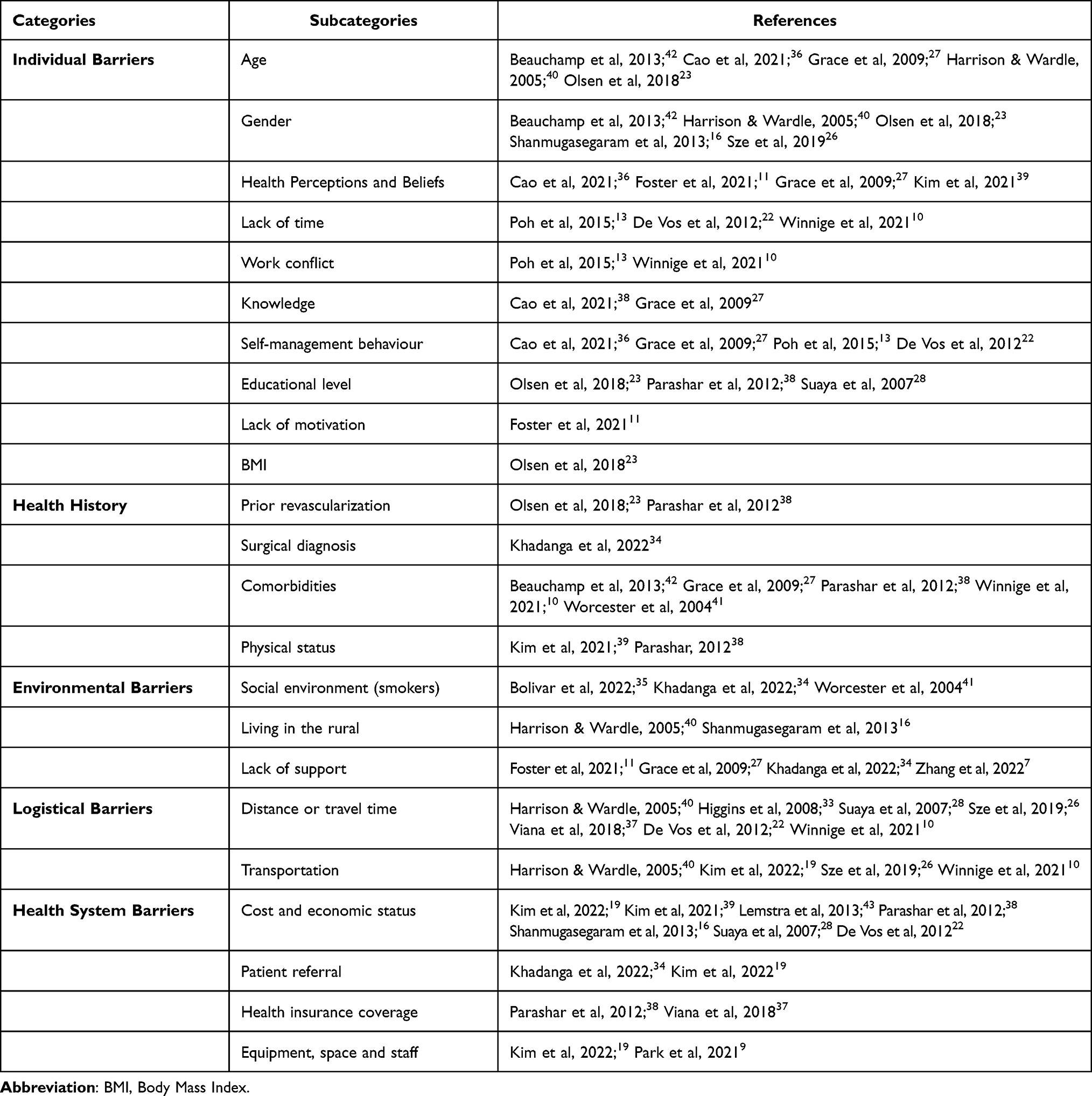 |
Table 3 A Barrier to Low Participation in Cardiac Rehabilitation |
Furthermore, the identification results related to barriers originating from the environment, including being in a smoker’s environment, living in a rural area, and lacking support from family, friends, and health workers. Next, included in the category of logistical barriers include distance or travel time and transportation. Finally, the barriers identified in the health system category include cost and economic status, patient referrals, health insurance coverage, equipment, room, and staff.
Discussion
This review aims to identify barriers to participation in CR programs among patients with CHD after reperfusion therapy. The results of this study indicate that most of the studies analyzed still have a low participation rate (≤50%).10,13,23,26–28,34,38,39,41,43 In addition, some studies mention the CR phase category (I, II, III) but do not specifically discuss the barriers experienced for each CR phase.7,10,13,26,28,36,40 This review focuses on the barriers influencing patient participation in the CR program regardless of each phase. The small number of studies originating from developing countries makes this study unable to generalize the barriers that affect patient participation in CR programs in developing countries. The low participation is caused by several factors, which are classified in this study into five categories: individual, health history, environmental, logistical, and health system.
The results of this review indicate that one study assesses the participation rate of home-based CR programs with moderate participation rates (64.66%).36 Although these results are not sufficient to generalize, home-based CR programs also have good participation and the same efficacy as hospital-based CR. A recent cohort study showed that participation in home-based CR was associated with fewer hospitalizations than hospital-based CR.44 This is because patients who carry out CR at home have good participation and adherence and do not consider the distance and costs that must be incurred.44 Specifically, the obstacles experienced by participants in implementing home-based CR come from individual factors, namely knowledge, self-management behavior, perception of shared decision-making and age.36 However, in general, many other barriers may affect CR participation among patients with CHD after undergoing reperfusion therapy.
Individual barriers become independent barriers that cause low participation in CR. Several studies have shown that older patients have significantly more significant CR barriers to enrollment and participation than younger patients.23,27,36,40,42 Several barriers that contribute to the low participation rate of elderly CR tend to be absenteeism, co-morbidity, poorer understanding and perception of the benefits of CR, inadequate transportation, and caregiver responsibilities at home.11,27,36 Meanwhile, younger patients experience more barriers to CR participation due to work responsibilities and lack of time.13,22,27 In addition, women have a much lower CR completion rate than men.16,23,40 This is because factors such as transportation and family responsibilities influence women to participate in CR.23
Knowing how CR benefits one’s heart health is another critical factor influencing participation in a CR program.27,36 Knowledge is closely related to one’s level of education. Those with at least a high school education are more likely to participate in CR.38 Knowledge of CR will influence self-management behaviour, so this is a critical factor in self-care and must be considered by medical staff and healthcare providers to increase patient compliance with CR.22,36
The patient’s previous medical history, including comorbidities, surgical diagnosis, and physical status, also influences the patient’s participation in the CR program.28,38 Patients with a surgical diagnosis tend to participate better in CR than patients with a non-surgical diagnosis.34 However, another study showed that patients after PCI had better participation in CR.38 This may be due to differences in patient experience and knowledge regarding the symptoms they are experiencing. Comorbidities more experienced by the elderly (diabetes, angina, and heart failure) can hinder the patient’s exercise in CR sessions related to the experience of pain, shortness of breath, limited mobility, and disability.27 On the contrary, the results of other studies show that patients who experience these symptoms are more likely to attend CR programs.45 Experience with symptoms, especially in newly diagnosed patients with CHD, can trigger sensitivity and a tendency to take their health condition seriously.23 On the other hand, patients who experience chronic illness after MI are reported to be non-adherent to the treatment given due to the influence of various factors, including psychosocial support.17,46 Therefore, it is essential to readjust the exercise program to the patient’s physical capacity and provide psychosocial support to increase participation in the CR program.
Environmental barriers are additional barriers that influence low participation in CR. In particular, the utilization rate of CR among the rural population is still relatively low.16,40 This is because of geographical barriers such as CR location, distance, transportation access, parking fees, road quality and bad weather conditions. In addition, patients in rural areas are also more likely to be active smokers. Previous studies said smoking is associated with decreased CR participation in cardiac patients and if the patient has many smokers in his social environment.34,35,41 This is because other smokers can cause smoking cessation difficulties by increasing access to cigarettes, providing cues to smoke, and supporting positive norms around smoking.45,47 Lack of support in the patient’s environment can also affect the participation rate of CR.7,11,27,34 Multidisciplinary support from doctors, nurses, rehabilitation therapists, family, friends, and partners is needed to strengthen their motivation to increase CR adherence.
Travel time exceeding the recommended average (<30 minutes) was reported as the most significant barrier to CR program participation in various countries.10,22,26,28,33,37,40 The location of CR facilities, generally in the centre of big cities, makes reaching difficult, especially for patients from rural areas.10,21,37 This is supported by previous findings, which state that CR program patients have a shorter travel time than patients who do not participate.33 The most frequent CR barriers were the distance from the hospital/rehabilitation centre, travel costs, and lack of information about the CR program.48 Ease of access to transportation, including parking facilities, is known to determine patient participation in the CR program.19,49 Elderly patients with severe health problems also find it challenging to travel and optimize the use of CR services due to technical constraints on travel. In addition, the inability to drive, as reported by many patients in Sze et al study, resulted in lower CR participation.26
The Health System is another essential factor that becomes a barrier for patients to attend the CR program. The findings of this review show that cost and economic status are the most common barriers patients have.16,19,22,28,38,39,43 Patients with low socioeconomic status feel burdened in paying for the entire program. Thus, individuals with economic difficulties are less likely to participate in CR. This is also supported by some individuals’ lack of health insurance coverage.37,38 Then another factor from the health system is the lack of patient referrals.19,34 The findings in this study indicate that a specific strategy needed to increase CR participation is automated electronic referrals.19,34 Optimal CR referrals significantly affect patient participation in attending CR.19,34 Meanwhile, another barrier that also influences the low participation of CR is the need for more supporting facilities (equipment, space, staffing) in hospitals without CR compared to hospitals with CR.9,19 This is an essential obstacle in supporting patient participation in attending CR in small hospitals in their area, especially patients who live in rural areas.16,40
Strengths and Limitations
This Scoping review has strengths and limitations. First, we have yet to be able to integrate the results through meta-analysis due to the limitations of the data presented from the studies included (there is no correlation value, effect size, and variance of standard error). Second, most of the studies were conducted in developed countries, and only one study was conducted in a developing country, so this review cannot provide a general picture regarding the differences in barriers experienced by CHD patients who come from each country. Third, regarding sample size, we included studies with a minimum of 100 patients or more to reduce the possibility of bias or unreliable results. In addition, the results of critical appraisal analysis with JBI showed that many of the studies analyzed need to be clarified and include triggering factors and strategies to overcome these factors. Thus, the authors increased the standard of the JBI score (70%) for each study analyzed. Lastly, most of the studies analyzed in this study did not mention or explain the CR phase, so researchers found it difficult to categorize barriers based on the CR phase. Therefore, the results of this study cannot be generalized to all phases of CR because each phase has different obstacles.
Conclusions
Barriers that contribute to low participation are classified into five categories, and they are barriers from the individual, health history, environment, logistics, and health system. The most reported barriers in each category were age, comorbidities, lack of support from friends, family and health workers, distance or travel time, and cost and economic status. The complexity of barriers contributing to the participation of patients with CHD in CR programs can be an essential consideration for healthcare providers to evaluate and improve the quality and accessibility of CR services.
The findings from this review suggest that health workers must pay attention to the barriers experienced by patients in participating while participating in the CR program so that they can find solutions to overcome these problems and implementation of CR can be provided optimally. Further studies assessing participation and adherence in home- and exercise-based CR programs in patients with CHD after reperfusion therapy are warranted, given that only one study addressed this program. In addition, studies related to this topic still need to be carried out, especially in developing countries, so that it can increase the generalization aspect in future review studies.
Acknowledgments
All authors thank to Universitas Padjadjaran, Bandung, West Java, Indonesia, who has facilitated the database for us in this study.
Disclosure
The authors had no conflicts of interest in this research.
References
1. Virani SS, Alonso A, Benjamin EJ, et al. Heart disease and stroke statistics—2020 update: a report from the American Heart Association. Circulation. 2020;141(9):e139–e596. doi:10.1161/CIR.0000000000000757
2. American Heart Association. 2023 heart disease and stroke statistics update fact sheet [Internet]; 2023. Available from: https://professional.heart.org/en/science-news/heart-disease-and-stroke-statistics-2023-update.
3. World Health Organization (WHO). Cardiovascular diseases (CVDs) [Internet]; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds).
4. Fröhlich GM, Meier P, White SK, Yellon DM, Hausenloy DJ. Myocardial reperfusion injury: looking beyond primary PCI. Eur Heart J. 2013;34(23):1714–1722. doi:10.1093/eurheartj/eht090
5. Zhang Y, Huo Y. Early reperfusion strategy for acute myocardial infarction: a need for clinical implementation. J Zhejiang Univ Sci B. 2011;12(8):629–632. doi:10.1631/jzus.B1101010
6. Sugiharto F, Trisyani Y, Nuraeni A, Mirwanti R, Melati Putri A, Aghnia Armansyah N. Factors associated with increased length of stay in post primary percutaneous coronary intervention patients: a scoping review. Vasc Health Risk Manag. 2023;19(June):329–340. doi:10.2147/VHRM.S413899
7. Zhang S, Zuo H, Meng X, Hu D. Support Life Club: a new model based on social media group chats and social activities that can improve adherence and clinical outcomes in patients receiving cardiac rehabilitation. Patient Prefer Adherence. 2022;16(July):1907–1917. doi:10.2147/PPA.S368615
8. Soldati S, Di Martino M, Rosa AC, Fusco D, Davoli M, Mureddu GF. The impact of in-hospital cardiac rehabilitation program on medication adherence and clinical outcomes in patients with acute myocardial infarction in the Lazio region of Italy. BMC Cardiovasc Disord. 2021;21(1):1–13. doi:10.1186/s12872-021-02261-6
9. Park MS, Lee S, Ahn T, et al. Current status of cardiac rehabilitation among representative hospitals treating acute myocardial infarction in South Korea. PLoS One. 2021;16(12 December):1–12. doi:10.1371/journal.pone.0261072
10. Winnige P, Filakova K, Hnatiak J, et al. Validity and reliability of the Cardiac Rehabilitation Barriers Scale in the Czech Republic (CRBS-CZE): determination of Key Barriers in East-Central Europe. Int J Environ Res Public Health. 2021;18(13113):1–14.
11. Foster EJ, Munoz SA, Crabtree D, Leslie SJ, Gorely T. Barriers and facilitators to participating in cardiac rehabilitation and physical activity in a remote and rural population: a cross-sectional survey. Cardiol J. 2021;28(5):697–706. doi:10.5603/CJ.a2019.0091
12. Turk-Adawi KI, Grace SL. Narrative review comparing the benefits of and participation in cardiac rehabilitation in high-, middle- and low-income countries. Heart Lung Circ. 2015;24(5):510–520. doi:10.1016/j.hlc.2014.11.013
13. Poh R, Ng HN, Loo G, et al. Cardiac rehabilitation after percutaneous coronary intervention in a multiethnic asian country: enrollment and barriers. Arch Phys Med Rehabil. 2015;96(9):1733–1738. doi:10.1016/j.apmr.2015.05.020
14. Ji H, Fang L, Yuan L, Zhang Q. Effects of exercise-based cardiac rehabilitation in patients with acute coronary syndrome: a meta-analysis. Med Sci Monit. 2019;25:5015–5027.
15. Simon M, Korn K, Cho L, Blackburn GG, Raymond C. Cardiac rehabilitation: a class 1 recommendation. Cleve Clin J Med. 2018;85(7):551–558. doi:10.3949/ccjm.85a.17037
16. Shanmugasegaram S, Oh P, Reid RD, Mccumber T, Grace SL. Cardiac rehabilitation barriers by rurality and socioeconomic status: a cross-sectional study. Int J Equity Health. 2013;12(1):1. doi:10.1186/1475-9276-12-72
17. Kosobucka A, Michalski P, Pietrzykowski Ł, et al. Adherence to treatment assessed with the adherence in chronic diseases scale in patients after myocardial infarction. Patient Prefer Adherence. 2018;12:333–340. doi:10.2147/PPA.S150435
18. Dunlay SM, Witt BJ, Allison TG, et al. Barriers to participation in cardiac rehabilitation. Am Heart J. 2009;158(5):852–859. doi:10.1016/j.ahj.2009.08.010
19. Kim C, Sung J, Han JY, et al. A comparison of barrier factors between hospitals with and without cardiac rehabilitation programs in Korea: a Nation-Wide Survey Research. J Clin Med. 2022;11(9):2560.
20. Ruano-Ravina A, Pena-Gil C, Abu-Assi E, et al. Participation and adherence to cardiac rehabilitation programs. A systematic review. Int J Cardiol. 2016;223:436–443. doi:10.1016/j.ijcard.2016.08.120
21. Turk-Adawi KI, Oldridge NB, Tarima SS, Stason WB, Shepard DS. Cardiac rehabilitation enrollment among referred patients: patient and organizational factors. J Cardiopulm Rehabil Prev. 2014;34(2):114–122. doi:10.1097/HCR.0000000000000017
22. De Vos C, Li X, Van Vlaenderen I, et al. Participating or not in a cardiac rehabilitation programme: factors influencing a patient’ s decision. Eur J Prev Cardiol. 2012;2(20):341–348.
23. Olsen SJ, Schirmer H, Bønaa KH, Hanssen TA. Cardiac rehabilitation after percutaneous coronary intervention: results from a nationwide survey. Eur J Cardiovasc Nurs. 2018;17(3):273–279. doi:10.1177/1474515117737766
24. Zeymer U, Ludman P, Danchin N, et al. Reperfusion therapies and in-hospital outcomes for ST-elevation myocardial infarction in Europe: the ACVC-EAPCI EORP STEMI Registry of the European Society of Cardiology. Eur Heart J. 2021;42(44):4536–4549. doi:10.1093/eurheartj/ehab342
25. Fraser MJ, Leslie SJ, Gorely T, Foster E, Walters R. Barriers and facilitators to participating in cardiac rehabilitation and physical activity: a cross-sectional survey. World J Cardiol. 2022;14(2):83–95. doi:10.4330/wjc.v14.i2.83
26. Sze CL, Siop S, Lim L. Enrollment and attendance to cardiac rehabilitation after percutaneous coronary intervention in Sarawak: a prospective study. Int J Recent Technol Eng. 2019;8(1C2):900–903.
27. Grace SL, Shanmugasegaram S, Gravely-Witte S, et al. Barriers to Cardiac Rehabilitation: does age make a difference? J Cardiopulm Rehabil Prev. 2009;29(3):183–187. doi:10.1097/HCR.0b013e3181a3333c
28. Suaya JA, Shepard DS, Normand SLT, Ades PA, Prottas J, Stason WB. Use of cardiac rehabilitation by medicare beneficiaries after myocardial infarction or coronary bypass surgery. Circulation. 2007;116(15):1653–1662. doi:10.1161/CIRCULATIONAHA.107.701466
29. Motrico E, Rubio-valera M, Conejo-cero S, Pastor L, Moreno-peral P. Barriers for nonparticipation and dropout of women in cardiac rehabilitation programs. J Womens Health. 2017;26(8):849–859.
30. Peterson J, Pearce PF, Ferguson LA, Langford CA. Understanding scoping reviews: definition, purpose, and process. J Am Assoc Nurse Pract. 2017;29(1):12–16. doi:10.1002/2327-6924.12380
31. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:1–11.
32. Joanna Briggs Institute (JBI). JBI’s critical appraisal tools [Internet]. Joanna Briggs Institute; 2022. Available from: https://jbi.global/critical-appraisal-tools.
33. Higgins RO, Murphy BM, Goble AJ, et al. Cardiac rehabilitation program attendance after coronary artery bypass surgery: overcoming the barriers Rosemary. Med J Aust. 2008;188(12):712–714. doi:10.5694/j.1326-5377.2008.tb01852.x
34. Khadanga S, Savage PD, Gaalema DE, Ades PA. Predictors of Cardiac Rehabilitation Participation. J Cardiopulm Rehabil Prev. 2022;41(5):322–327. doi:10.1097/HCR.0000000000000573
35. Bolívar HA, Elliott RJ, Middleton W, et al. Social smoking environment and associations with cardiac rehabilitation attendance. J Cardiopulm Rehabil Prev. 2022;41(1):46–51. doi:10.1097/HCR.0000000000000518
36. Cao Q, Xu L, Wen S, Li F. Investigating the influence of the shared decision-making perception on the patient adherence of the home-and exercise-based cardiac rehabilitation after percutaneous coronary intervention. Patient Prefer Adherence. 2021;15:411–422. doi:10.2147/PPA.S292178
37. Viana M, Borges A, Araújo C, et al. Inequalities in access to cardiac rehabilitation after an acute coronary syndrome: the EPiHeart cohort. BMJ Open. 2018;8(1):1–11. doi:10.1136/bmjopen-2017-018934
38. Parashar S, Spertus JA, Tang F, et al. Predictors of early and late enrollment in cardiac rehabilitation, among those referred, after acute myocardial infarction. Circulation. 2012;126(13):1587–1595. doi:10.1161/CIRCULATIONAHA.111.088799
39. Kim JS, Kim GS, Kang SM, Chu SH. Symptom experience as a predictor of cardiac rehabilitation education programme attendance after percutaneous coronary intervention: a prospective questionnaire survey. Eur J Cardiovasc Nurs. 2021;20(3):183–191. doi:10.1177/1474515120940534
40. Harrison WN, Wardle SA. Factors affecting the uptake of cardiac rehabilitation services in a rural locality. Public Health. 2005;119(11):1016–1022. doi:10.1016/j.puhe.2005.01.016
41. Worcester MUC, Murphy BM, Mee VK, Roberts SB, Goble AJ. Cardiac rehabilitation programmes: predictors of non-attendance and drop-out. Eur J Cardiovasc Prev Rehabil. 2004;11(4):328–335.
42. Beauchamp A, Worcester M, Ng A, et al. Attendance at cardiac rehabilitation is associated with lower all-cause mortality after 14 years of follow-up. Heart. 2013;99(9):620–625. doi:10.1136/heartjnl-2012-303022
43. Lemstra ME, Alsabbagh W, Rajakumar RJ, Rogers MR, Blackburn D. Neighbourhood income and cardiac rehabilitation access as determinants of nonattendance and noncompletion. Can J Cardiol. 2013;29(12):1599–1603. doi:10.1016/j.cjca.2013.08.011
44. Nkonde-Price C, Reynolds K, Najem M, et al. Comparison of home-based vs center-based cardiac rehabilitation in hospitalization, medication adherence, and risk factor control among patients with cardiovascular disease. JAMA Netw Open. 2022;5(8):E2228720. doi:10.1001/jamanetworkopen.2022.28720
45. Hitchman SC, Fong GT, Zanna M, Thrasher JF, Laux FL. The relation between number of smoking friends, and quit intentions, attempts, and success: findings from the International Tobacco Control (ITC) Four Country Survey. Psychol Addict Behav. 2014;28(4):1–7. doi:10.1037/a0036483
46. Wu JR, Moser DK, Chung ML, Lennie TA. Predictors of medication adherence using a multidimensional adherence model in patients with heart failure. J Card Fail. 2008;14(7):603–614. doi:10.1016/j.cardfail.2008.02.011
47. Cambron C, Lam CY, Cinciripini P, Li L, Wetter DW. Socioeconomic status, social context, and smoking lapse during a quit attempt: an ecological momentary assessment study. Ann Behav Med. 2020;54(3):141–150. doi:10.1093/abm/kaz034
48. Antoniou V, Pasias K, Loukidis N, et al. Translation, cross-cultural adaptation and psychometric validation of the greek version of the Cardiac Rehabilitation Barriers Scale (CRBS-GR): what are the barriers in South-East Europe? Int J Environ Res Public Health. 2023;20(5):4064. doi:10.3390/ijerph20054064
49. De Angelis C, Bunker S, Schoo A. Exploring the barriers and enablers to attendance at rural cardiac rehabilitation programs. Aust J Rural Health. 2008;16(3):137–142.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.