")
Back to Journals » Risk Management and Healthcare Policy » Volume 15
Barriers to Delivery of Enteral Nutrition in Intensive Care Settings in Saudi Arabia: A Comparative Study of the Perceptions of Health Care Providers Working in Adult and Paediatric ICUs
Authors Zaher S
Received 19 October 2022
Accepted for publication 30 November 2022
Published 15 December 2022 Volume 2022:15 Pages 2357—2370
DOI https://doi.org/10.2147/RMHP.S394035
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Sara Zaher1,2
1Clinical Nutrition Department, Faculty of Applied Medical Sciences, Taibah University, Madinah, Kingdom of Saudi Arabia; 2National Nutrition Committee (NNC), Saudi Food and Drug Authority (Saudi FDA), Riyadh, Saudi Arabia
Correspondence: Sara Zaher, Clinical Nutrition Department, Faculty of Applied Medical Sciences, Taibah University, P.O. Box 344, Madinah, 42353, Kingdom of Saudi Arabia, Email [email protected]; [email protected]
Background and Aims: Achieving optimal nutrition prescription is challenging in critically ill patients. Many factors can hinder the adequate delivery of enteral nutrition (EN) in intensive care units (ICUs). In this study, we aim to describe EN barriers and compare the perceptions of health care practitioners working in adult and paediatric ICUs regarding these barriers.
Methods: In this cross-sectional study, data were collected via online survey. All physicians, dietitians, and nurses working in adult or paediatric ICUs across Saudi Arabia were eligible to participate. The survey contained 24 potential EN barriers and participants were asked to rate their importance on a scale from 1 to 5. A total Likert rating score of the 24 items was later calculated.
Results: We recruited 244 health care providers working in adult and paediatric ICUs. The most important perceived barriers were “Delay in physician ordering EN initiation” (3.33 ± 1.32), and ‘Waiting for dietitians to assess patients’ (3.22 ± 1.20). There was a statistical difference between the responses of health care providers based on their work settings for the following items; “Nurses failing to progress feeds according to feeding protocol” (p=0.006) and ‘Feeding being held too far prior procedures or operating-room visits’ (p=0.021). Profession significantly influenced the total Likert rating score of the 24 items (r=− 0.234, p=0.001).
Conclusion: This study identified some barriers of EN delivery in ICUs and showed that participants’ perceptions regarding these barriers were influenced by their roles. These findings shed light on the nutritional practices in Saudi hospitals and identify areas of improvement in EN practice and advancements in the field of critical care nutrition in the region.
Keywords: enteral nutrition, EN barriers, PICU, ICU
Introduction
Nutrition therapy is a vital element of the care process of critically ill adult and paediatric patients. The prognostic impact of nutrition therapy in the critically ill population has previously been documented in the literature;1–5 however, achieving optimal nutrition remains a challenge in this population. Although nutrition support either enterally or parenterally has substantially improved the patient’s nutritional intake, underfeeding continues to be documented in intensive care settings worldwide.6–8
Underfeeding is determined when a patient receives less than 70% of their prescribed requirements during the first 7 days of intensive care unit (ICU) admission.9,10 The current international nutrition guidelines uniformly recommend the preferential use of enteral nutrition (EN) for critically ill patients where possible.11,12 The development of EN and implementation of feeding protocols have markedly improved nutrient delivery in the hospitalised critically ill population.13,14 However, there are a substantial number of critically ill children and adults worldwide who still cannot achieve adequate nutritional intake via the enteral route for many reasons.7,8,15,16 These include: delayed initiation of EN, under-prescription of the requirements by physicians, and frequent interruption of EN due to fear of aspiration, high residual volume, or diarrhoea;17–19 some of these reasons might be preventable.17–19
Although many international studies have investigated feeding practices in ICUs, this field is new in the Middle East and limited research has been conducted in this area. Therefore, there is an urgent need for nutrition-based studies to advance the field of critical care nutrition in the region. Previous data in the region recorded a high incidence of underfeeding among critically ill adult patients, and we have shown that the time of EN initiation plays a key role in determining the time to achieving full requirements.7 In this study, we aim to describe in detail other barriers of EN delivery in critically ill adult and paediatric patients as perceived by physicians, dietitians, and nurses working in intensive care settings. Furthermore, we aim to compare the perceptions of health care providers working in adult and paediatric ICUs regarding the barriers of EN.
Methods
Study Design and Participants
In this cross-sectional study, all physicians, dietitians, and nurses working in adult or paediatric ICUs across Saudi Arabia were eligible to participate. The study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee at Taibah University (Certificate no. 2020/57/204/CLN). A participant information sheet was included in the first page of the online survey. Participants’ consent was obtained by including a mandatory question confirming that they agreed to participate in the study.
Data were collected via online survey, which was promoted on various social media platforms (eg, Twitter and WhatsApp). Chain-referral sampling was then performed where the head of ICU departments were contacted to achieve adequate convenience sampling of medical staff working in adult and paediatric ICUs across the kingdom of Saudi Arabia. Data collection was initiated on 15 October 2021 and continued for 3 months.
Survey Development
The survey tool was adapted from Cahill et al (2016)20 and was reviewed and modified by the researcher, including adding more questions about the demographics of the participants and rewriting some of the questions to improve clarity. The survey was then pilot tested on 10 dietitians, 5 doctors, and 5 nurses, and was adjusted accordingly. The data of the 20 participants used in the pilot testing were excluded from the analysis. The survey collected information about the participants’ demographic information and barriers to adequate EN delivery as perceived by physicians, dietitians, and nurses working in adult and paediatric ICUs. The questionnaire contained 24 items, and the respondents were asked to rate the items’ importance as barriers to delivery of EN in their ICUs from 1 (not at all important), 2 (slightly important), 3 (important), 4 (Fairly important) to 5 (very important). The barriers of EN were categorised into 5 domains: Domain 1 included 2 questions about guidelines and recommendations, Domain 2 included 7 questions about EN delivery to patients, Domain 3 included 3 questions about ICU and paediatric ICU (PICU) resources, Domain 4 included 7 questions about critical care providers’ attitudes and behaviours, and Domain 5 included 5 questions about dietitian resources in intensive care settings. The Cronbach’s alpha obtained indicated an excellent internal reliability of the instrument (0.944).
Statistical Analysis
Data were downloaded and analysed using the Statistical Package for Social Sciences software version 23 (SPSS Inc.) (SPSS 23, SPSS Inc., Chicago, IL, USA). The Shapiro–Wilk test was used to assess the normality of continuous variables. Continuous variables were presented as mean ± standard deviation (SD) and median (interquartile range [IQR]). Frequencies and percentages were also presented to describe the data. Mean (±SD) and median (IQR) were calculated to determine the most and least important barriers to EN in adult and paediatric ICUs. Cronbach’s alpha test of reliability was used to assess the reliability of the measured enteral feeding barriers in the questionnaire. A total Likert rating score of the 24 items was calculated for each participant for use in the statistical analysis.
The Kruskal–Wallis test was performed to compare the median Likert rating scores of the 5 domains. The Mann–Whitney U-test was performed to compare the perceptions of health care providers working in adult ICUs and those working in PICUs regarding the importance of each item as a barrier to EN delivery.
A stepwise linear regression analysis was performed to identify factors that influenced the perceptions of the health care providers regarding the barriers of EN in ICU settings. The calculated total score (120) for each participant was used as the outcome variable in the regression models. The independent variables used in the models were gender (female coded as 1 and male coded as 2), education level (diploma coded as 1, intern coded as 2, Bachelor’s coded as 3, Master’s coded as 4, residency coded as 5, fellowship coded as 6, and doctorate coded as 7), years of experience as a numerical variable, type of health care facility (medical city coded as 1, military hospital coded as 2, ministry of health hospital coded as 3, national guard hospital coded as 4, private hospital coded as 5, specialised hospital coded as 6, and university teaching hospital coded as 7), region (Central coded as 1, Eastern coded as 2, Northern coded as 3, Southern coded as 4, and Western coded as 5), profession (dietitians coded as 1, nurses coded as 2, and doctors coded as 3), and setting (adult ICU coded as 1 and PICU coded as 2).
Results
A total of 244 health care providers working in adult and paediatric ICUs across Saudi Arabia participated in this study; 47 were physicians, 61 were dietitians, and 136 were nurses. Most of the participants were females (n=177, 72%). Most of the responses were received from the Western region, and their mean years of experience in intensive care settings was 5 ± 3.7 years. The characteristics of the study participants are presented in Table 1.
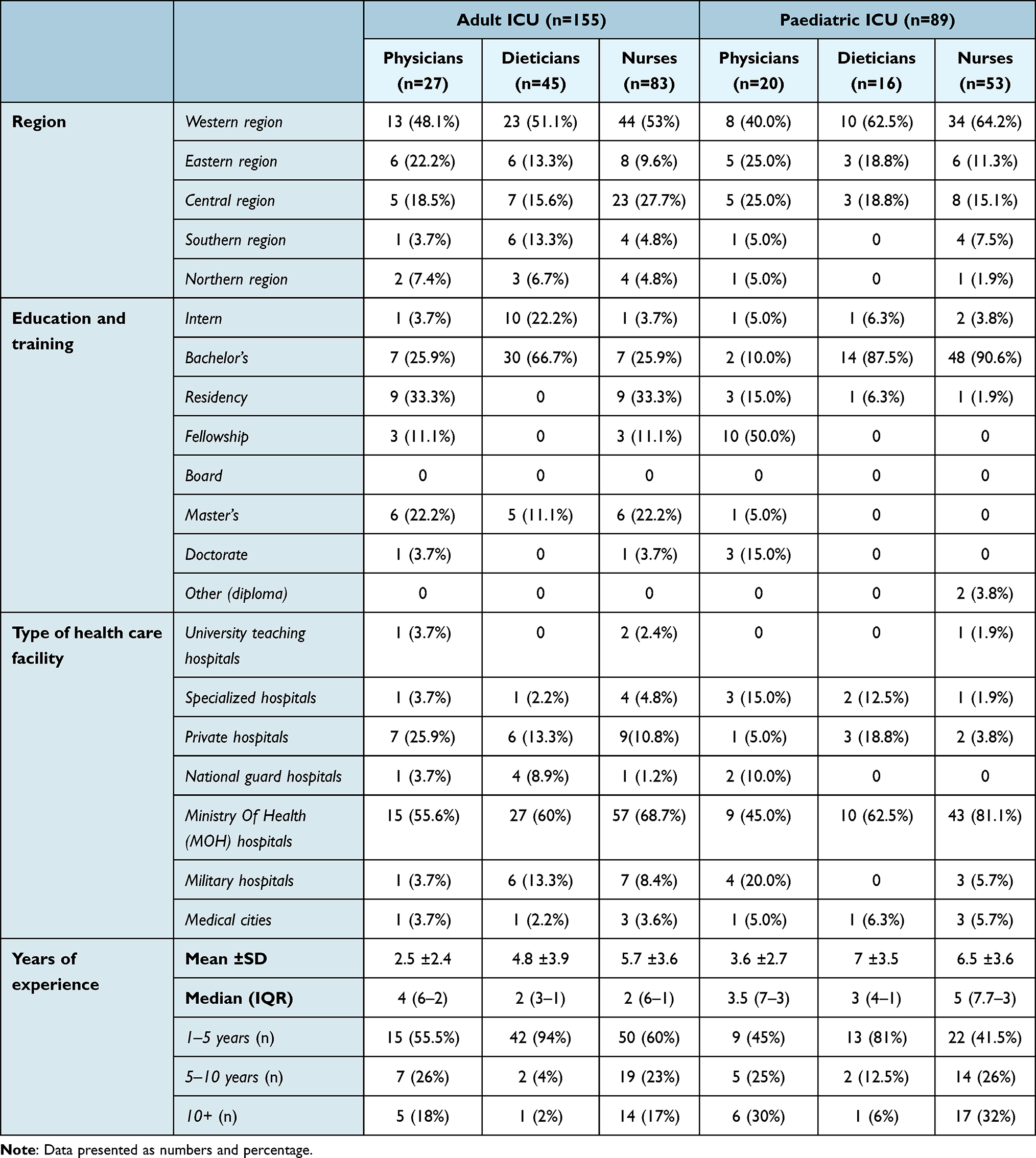 |
Table 1 General Characteristics of the Study Participants |
We calculated the mean (±SD) and the median (IQR) to determine the most and least important barriers to EN in adult and paediatric ICUs. The results showed that the most important barrier was “Delay in physician ordering initiation of enteral nutrition” [3.33 ±1.32, 3 (2–5)]which was included in the “delivery of EN” domain. The mean score of this item as indicated by the dietitians was [3.9 ±1.4, 5 (3–5)], by physicians was [3.09 ±1.1, 3 (2–4)] and by nurses was [3.06 ±1.3, 3 (2–4)]. The second most important barrier was “Waiting for the dietitian to assess the patients” [3.22 ±1.2, 3 (2–4)] which was included in the “dietitian support” domain. The mean score of this item as indicated by the dietitians was [3.5 ±1.4, 4 (2–5)], by physicians was [3.2 ±1.1, 3 (2–4)] and by nurses was [2.79 ±1.1, 3 (2–3)].The least important barriers were “Non-ICU physicians requesting patients not be fed enterally” [3.01 ±1.2, 3 (2–4)] preceded by “General belief among ICU team that provision of adequate nutrition does not impact on patient outcome” [3.03 ±1.3, 3 (2–4)]; both barriers were included in the “critical care providers attitude and behaviour” domain. A Kruskal–Wallis test was performed to compare the median Likert ratings of the 5 domains, and no significant differences were observed between the domains (Table 2).
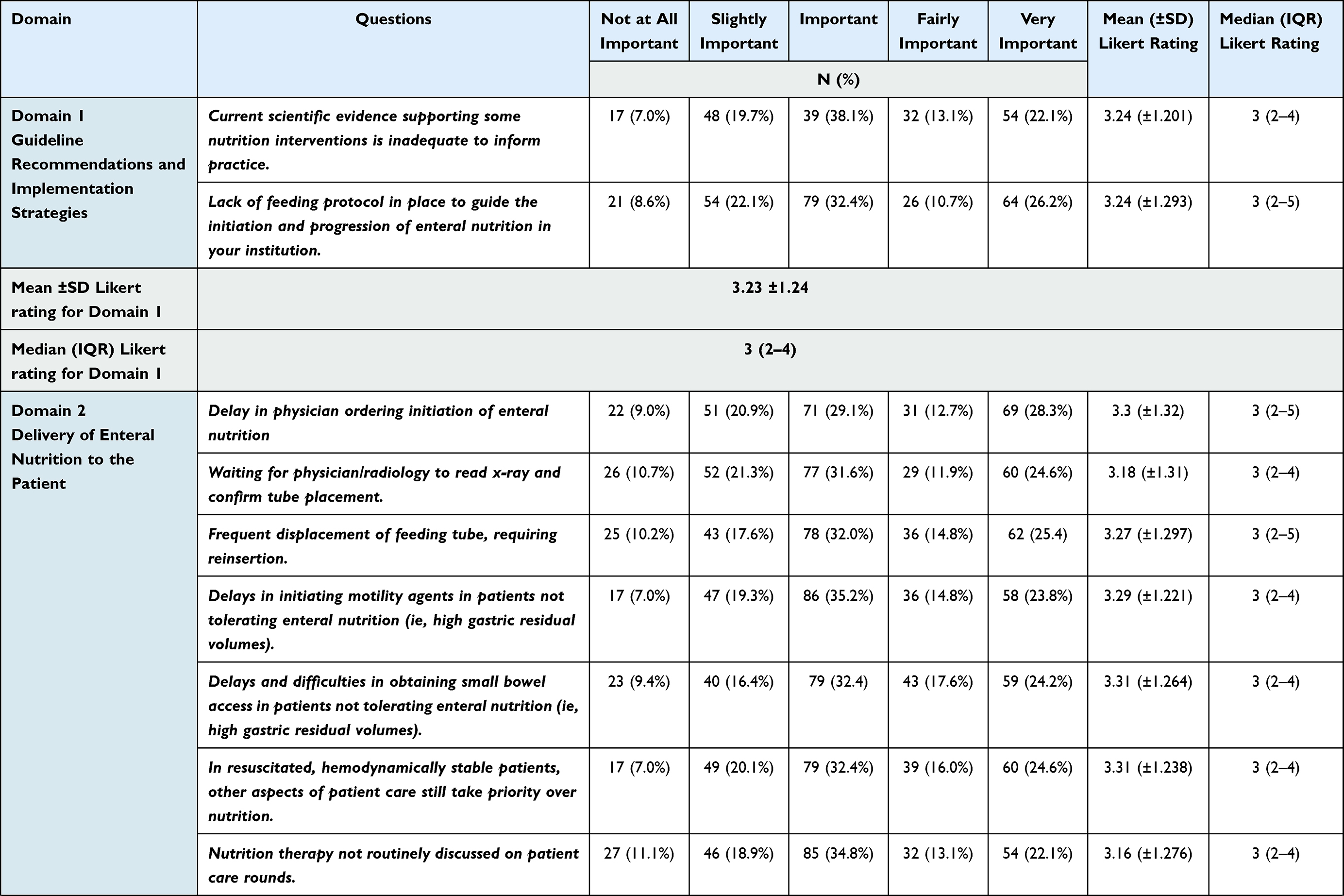 | 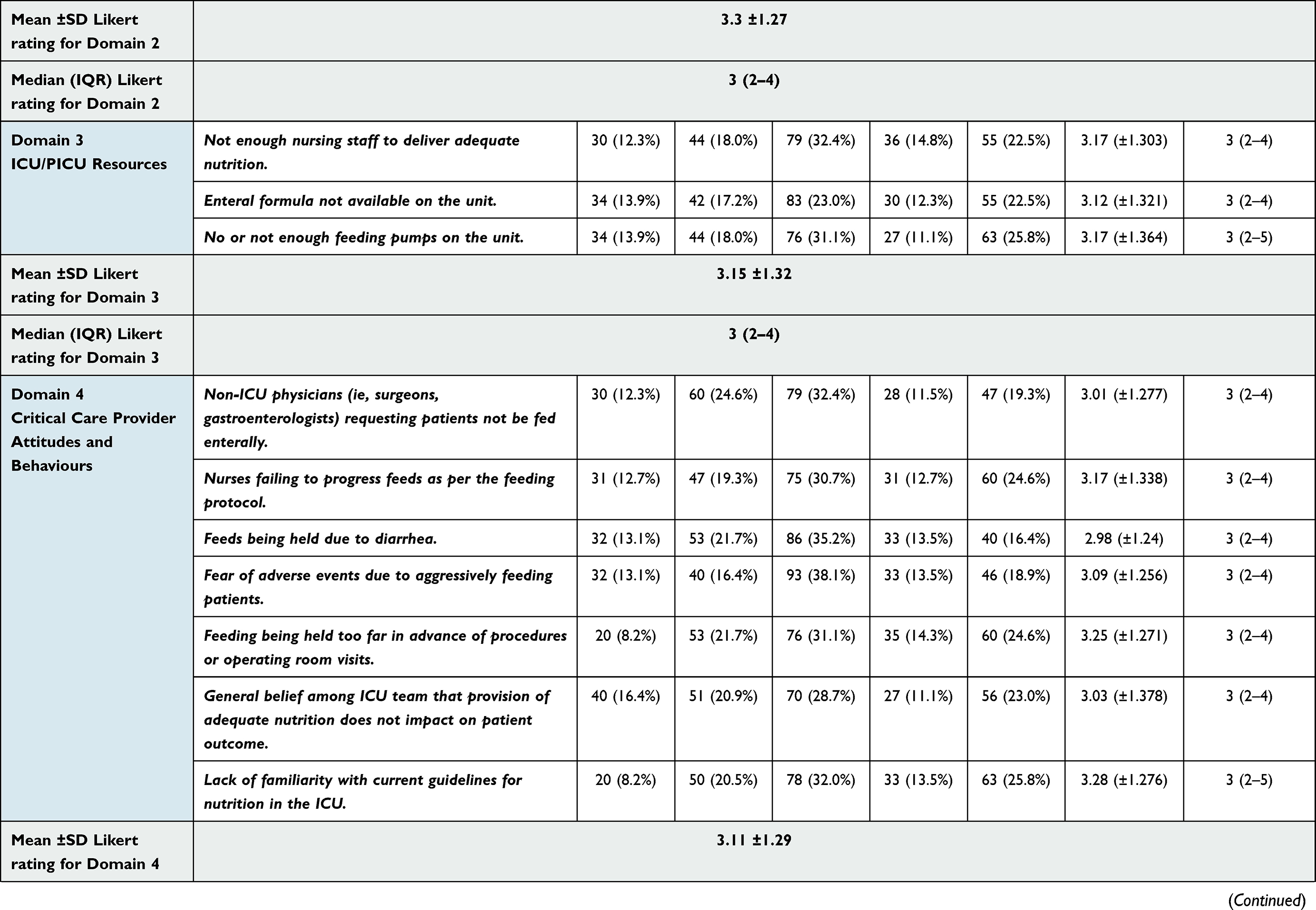 | 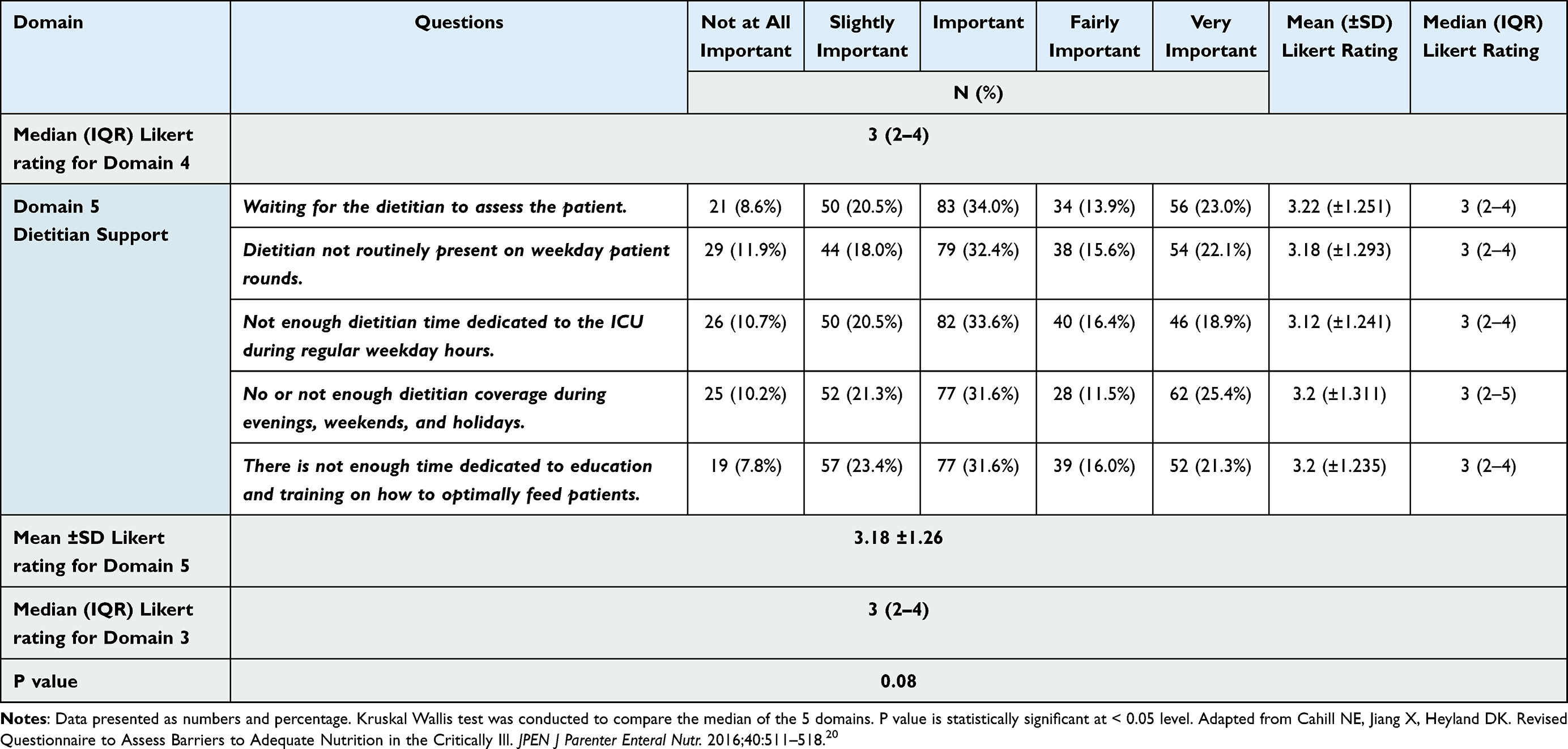 |
Table 2 Description of Enteral Feeding Barriers as Perceived by the Medical Staff Working in Adults and Paediatric ICUs |
To compare the perceptions of health care providers regarding the importance of each item as a barrier to EN based on their work setting (adult or paediatric ICU), a series of Mann–Whitney U-tests were performed. No significant differences were recorded between the responses of health care providers working in adult ICUs and those working in PICUs for most items, p> 0.05. However, a significant difference was recorded in the responses of the participants based on their work settings for the following items: “Nurses failing to progress feeds as per the feeding protocol” (p=0.006) and “Feeding being held too far in advance of procedures or operating room visits” (p=0.021). The results showed that “Nurses failing to progress feeds as per the feeding protocol” was perceived as more important EN barrier by participants working in adult ICU [3.34 (±1.3)] compared to those working in PICUs 2.88(±1.3). Similarly, “Feeding being held too far in advance of procedures or operating room visits” was also perceived as more important EN barrier by participants working in adult ICU [3.39 (±1.2)] compared to those working in PICUs 3.01(±1.3) (Table 3).
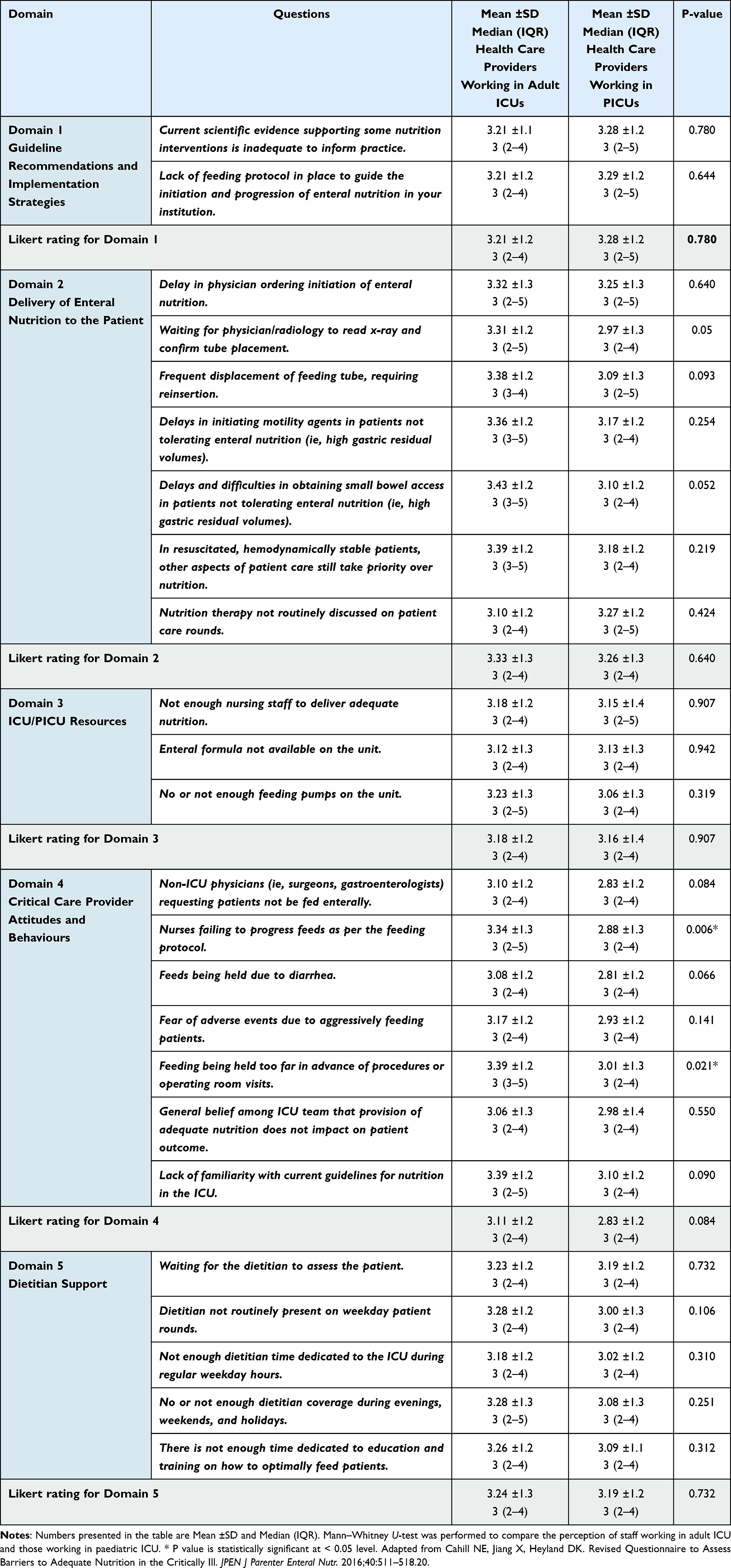 |
Table 3 Comparison Between the Perception of Health Care Providers Working in Adult and Paediatric ICU Regarding the Importance of the Following Items as Barriers to Achieve Adequate EN |
We then calculated the total Likert rating scores of the 24 items for each participant. The results showed that physicians had a median (IQR) Likert rating score of 71 (55–81), while dietitians scored 87 (69–102), and nurses scored 76 (65–88). A statistical difference was recorded between the total scores of different health care professions; the dietitians had statistically higher scores than the physicians and nurses (p<0.001).
The median (IQR) total Likert rating score of the 24 items was 78 (68–90) for health care providers working in adult ICUs and 72 (59–88) for those working in PICUs. No statistical difference was observed in the total scores between participants based on their work settings (adult vs paediatric ICU) (p=0.059).
A stepwise linear regression analysis was performed to identify factors influencing the health care providers’ perceptions regarding EN barriers in ICU settings. In the regression analysis, profession statistically influenced the total Likert rating scores of the participants (r=−0.234, p=0.001) (Table 4). In the sub-analysis of health care providers working in PICUs, gender statistically influenced the total Likert rating scores of the participants (r=−0.289, p=0.006) (Table 4).
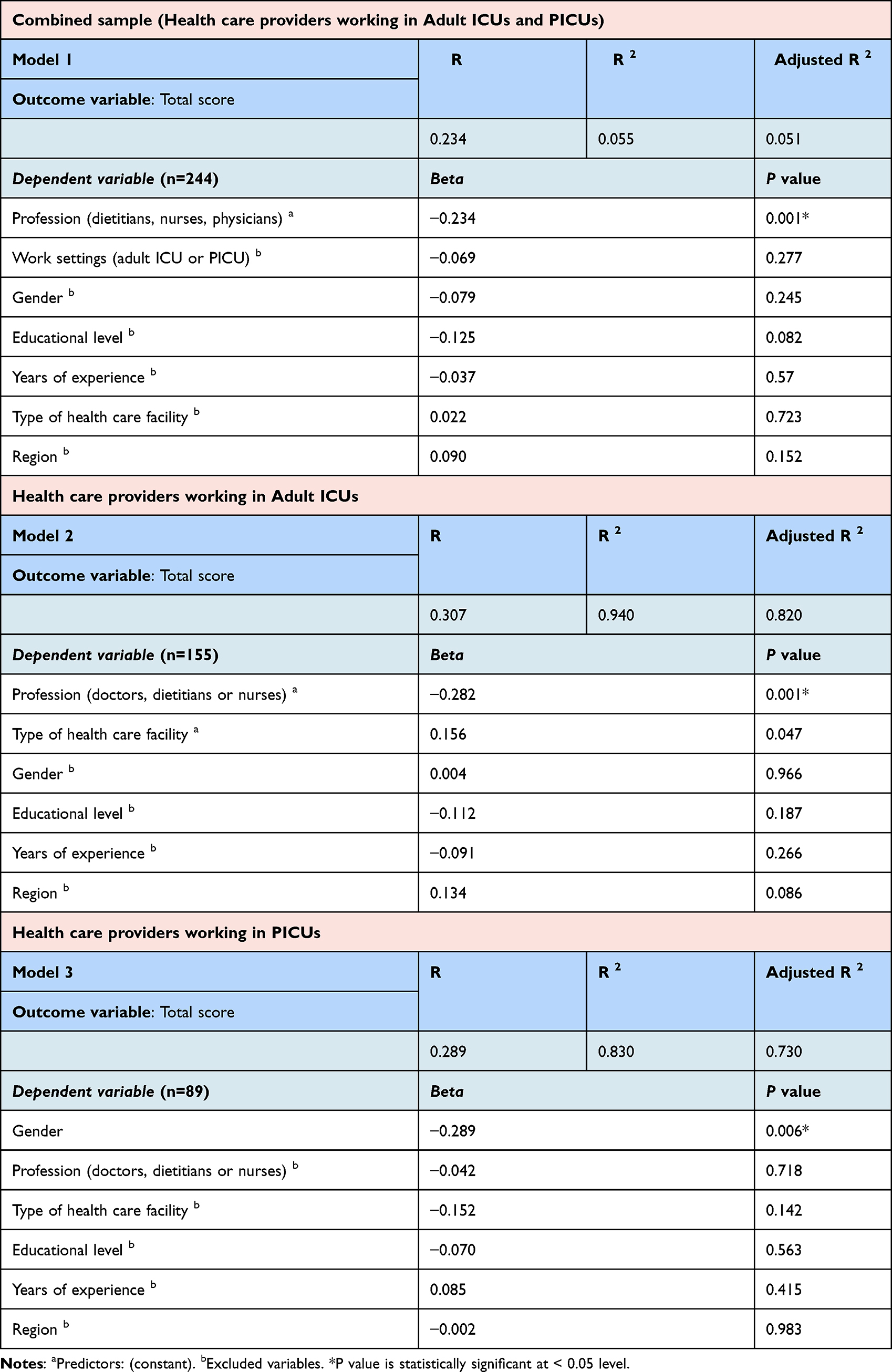 |
Table 4 Regression Analysis to Identify the Factors Influenced the Perception of Health Care Providers Regarding the Barriers to Achieve Adequate EN in ICU Settings |
Finally, we allowed for free-text responses to record any barriers that were not mentioned in the survey, two participants indicated that the nurses fear of aspiration could be a potential barrier to initiate and advance EN.
Discussion
The current study is the first to investigate the perceived barriers to EN in both adult and paediatric ICUs across Saudi Arabia; it included all three professional groups responsible for EN delivery in intensive care settings. Overall, this study showed that delayed ordering of EN initiation by physicians and waiting for dietitians to assess patients were considered the most important barriers to EN delivery in both adult and paediatric ICUs. Furthermore, the current study indicated that the perceptions of health care providers working in adult ICUs regarding barriers to EN were similar to those working in PICUs. However, the participants’ characteristics, such as profession (physicians, dietitians, and nurses) and gender, influenced their perceptions regarding EN barriers in intensive care settings.
The current study indicated that delayed ordering of EN initiation by physicians was perceived as the most important barrier to adequate delivery of EN by health care providers working in adult and paediatric ICUs. It has been previously reported that physicians were reluctant to initiate EN early; this is mainly because of the common perception that early EN is associated with increased risk of aspiration pneumonia.21,22 In addition, it is likely that other procedures took priority over EN, which may have hindered the optimal delivery of enteral feeding. Physicians have a key role in improving nutrition care in intensive care settings as the physician usually commences the initial feeding order, and this is considered the first step of the nutrition delivery process. Studies have shown that the use of physician opinion leaders as agents of change has resulted in improvements in the patient care process.23,24 Therefore, it is crucial that physicians understand the importance of nutrition in improving the clinical outcomes of critically ill adults and children. According to the participants from all disciplines included in this study, waiting for dietitians to assess patients was also considered a significant barrier to EN delivery in both adult and paediatric ICUs. Many studies have emphasised the role of the dietician in managing and minimising malnutrition in hospitalised patients, reducing the incidence of underfeeding, and improving the overall outcomes.25–27 Furthermore, research has shown that the availability of dedicated registered dietitians in ICUs improves the compliance to EN orders and substantially improves protein delivery to critically ill patients.26 Overall, these findings highlight the role of the multidisciplinary team in improving nutrition delivery in intensive care settings.
In the current study, the general responses of health care providers working in adult ICUs and PICUs regarding the barriers of EN were not significantly different for most items; however, there was a significant difference in their perceptions of certain barriers. The failure of nurses to advance feeding according to the feeding protocol was considered a more significant barrier to enteral feeding by health care providers working in adult ICUs than those working in PICUs. The discrepancy in the perceptions of health care providers based on their work setting could be related to the different levels of nutritional training provided to nurses in adult and paediatric ICUs. It is likely that nurses working in PICUs receive more nutritional training and therefore have better EN practices. For example, in the United Kingdom, nutrition training is a required for PICU nursing and medical staff.28 In contrast, Morphet et al highlighted a significant EN knowledge deficit in nurses working in adult ICUs.29
Holding feeds for an extended time prior to medical procedures was perceived as a more significant barrier to enteral feeding by health care providers working in adult ICUs than staff working in PICUs. Prolonged periprocedural cessation of EN has frequently been reported in adult ICUs.30,31 There are many reasons for the variation in the duration of delaying EN between different ICUs. For instance, lack of proper feeding protocols leads to a unnecessary feeding interruptions or delays in feeding restart after procedures.30 Furthermore, the clinical load in adult ICUs in Saudi Arabia is likely heavier than in PICUs, which might affect the timing of the procedures and consequently impacts the feeding schedule. The prolonged period of EN cessation after procedures in ICU settings might also be due to insufficient staff awareness that this practice can prevent the delivery of the planned nutritional requirements.31 Frequent and prolonged interruption of EN can be minimised by improving the nutrition knowledge of the health care practitioners who are responsible for making decisions regarding patient feeding in intensive care settings. To support and maintain good EN practices, regular nutritional education and training sessions should be provided to all health care providers involved in the nutrition care process.
Studies have shown that nutrition therapy is influenced by the practitioner roles due to competing priorities when caring for patients.25,28,32 In the current study, dietitians assigned higher scores to all the questions, indicating that they were more aware than other professions of the importance of these items as barriers to EN delivery in ICUs. These findings highlight the importance of involving all three professional groups in EN practice training and education. Although dietitians play a key role in assessing and providing the patient’s nutritional requirements, they are nonetheless part of a multidisciplinary team. Therefore, effective communication between health care providers is crucial to ensure proper implementation of nutrition care plans.
There were some limitations to our study that should be highlighted. Our sample size was relatively small, and the response rate from some professions was low. It was challenging to obtained the desired number of participants as we needed a specific group in a specific setting. However, our sample size was close to that of other studies performed in ICU settings in other countries. In addition, we recruited participants from all the regions of the kingdom, providing a general representation of the perspectives of health care providers working in ICUs regarding the barriers of EN. The tool used in this study was validated for adult ICUs, and there might be other barriers specifically encountered in PICUs that were not explored in this study. For example, Rogers et al reported that fluid restriction was the main barrier to achieving adequate EN in children with congenital heart disease.33 We allowed for free-text responses to record any barriers that were not mentioned in the survey. The survey-based nature of this study, as compared with direct prospective observation, was considered another limitation. However, most of the previously studies that investigated EN barriers in ICU settings worldwide collected their data through surveys.
Conclusion
This study highlighted the important of certain factors as barriers to EN delivery in intensive care settings as perceived by health care providers. The perceptions of the participants were influenced by their roles, mostly due to competing priorities when caring for patients. Highlighting and identifying EN barriers in intensive care settings will help to optimise nutrition care in this population. The standardisation of feeding protocols could minimise the discrepancies in the perceptions of health care providers regarding some avoidable barriers of EN, such as delaying EN initiation. Conducting educational sessions on preventable EN barriers should be included in the training of health care providers working in adult and paediatric ICUs to ensure best EN practices. The findings of this study shed light on the nutritional practices in Saudi hospitals and identify areas for improvement in EN practice, eventually helping to advance the field of critical care nutrition in the region. Future studies should focus on direct of observation of the factors hindering the delivery of EN in intensive care settings.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee at Taibah University (Certificate no. 2020/57/204/CLN). A participant information sheet was included in the first page of the online survey. Participants’ consent was obtained by including a mandatory question confirming that they agreed to participate in the study. Informed consent for publication was also obtained from participants.
Acknowledgments
Grateful acknowledgment to my students and my colleagues at the department of Clinical Nutrition, Taibah University for their help in distributing the survey. I would also like to thank all intensive care staff who participated in the study for completing the survey.
Author Contributions
The author made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Lew CCH, Wong G, Cheung K., et al. Association between malnutrition and 28-day mortality and intensive care length-of-stay in the critically ill: a Prospective Cohort Study. Nutrients. 2017;10(1):10. doi:10.3390/nu10010010
2. Cole H, Barlow R, Edwards S, et al. Impact of nutritional status on length of hospital stay. Clin Nutr ESPEN. 2017;22:137. doi:10.1016/j.clnesp.2017.07.054
3. Koontalay A, Suksatan W, Sadang JM, Prabsangob K. Optimal nutritional factors influencing the duration of mechanical ventilation among adult patients with critical illnesses in an intensive care unit. J Multidiscip Healthc. 2021;14:1385–1393. doi:10.2147/JMDH.S319553
4. Bagri NK, Jose B, Shah SK, et al. Impact of malnutrition on the outcome of critically ill children. Indian J Pediatrics. 2015;82(7):601–605. doi:10.1007/s12098-015-1738-y
5. de Souza Menezes F, Leite HP, Koch Nogueira PC. Malnutrition as an independent predictor of clinical outcome in critically illchildren. Nutrition. 2012;28:267–270. doi:10.1016/j.nut.2011.05.015
6. Salciute-Simene E, Stasiunaitis R, Ambrasas E, et al. Impact of enteral nutrition interruptions on underfeeding in intensive care unit. Clinical Nutrition. 2021;40(3):1310–1317. doi:10.1016/j.clnu.2020.08.014
7. Zaher SA, AL‐Subaihi R, AL‐Alshaya A, et al. Pilot Study to Investigate Enteral Feeding Practices and the Incidence of Underfeeding Among Mechanically Ventilated Critically Ill Patients at a Specialist Tertiary Care Hospital in Saudi Arabia. J Parenteral Enteral Nutrition. 2021;45(6):1327–1337. doi:10.1002/jpen.2019
8. Heyland DK, Dhaliwal R, Wang M, Day AG. The prevalence of iatrogenic underfeeding in the nutritionally ‘at-risk’ critically ill patient: results of an international, multicenter, prospective study. Clin Nutr. 2015;34(4):659–666. doi:10.1016/j.clnu.2014.07.008
9. Singer P, Blaser AR, Berger MM, et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clinical Nutrition. 2019;38(1):48–79. doi:10.1016/j.clnu.2018.08.037
10. Tatucu-Babet OA, Ridley EJ. How much underfeeding can the critically ill adult patient tolerate? J Intensive Med. 2022;2:69–77. doi:10.1016/j.jointm.2022.01.002
11. Hill A, Elke G, Weimann A. Nutrition in the intensive care unit—a narrative review. Nutrients. 2021;13(8):2851. doi:10.3390/nu13082851
12. Compher C, Bingham AL, McCall M, et al. Guidelines for the provision of nutrition support therapy in the adult critically ill patient: the American Society for Parenteral and Enteral Nutrition. J Parenteral Enteral Nutrition. 2022;46(1):12–41. doi:10.1002/jpen.2267
13. Compton F, Bojarski C, Siegmund B, van der Giet M. Use of a nutrition support protocol to increase enteral nutrition delivery in critically ill patients. Am J Crit Care. 2014;23(5):396–403. doi:10.4037/ajcc2014140
14. Brierley-Hobson S, Clarke G, O’Keeffe V. Safety and efficacy of volume-based feeding in critically ill, mechanically ventilated adults using the ‘Protein & Energy Requirements Fed for Every Critically ill patient every Time’ (PERFECT) protocol: a before-and-after study. Crit Care. 2019;23:105. doi:10.1186/s13054-019-2388-7
15. Zaher S, White D, Ridout J, et al. Association between enteral macronutrient delivery and inflammatory response in critically ill children. Clin Nutr. 2019;38(5):2287–2296. doi:10.1016/j.clnu.2018.10.001
16. Kim H, Shin JA, Shin JY, Cho OM. Adequacy of nutritional support and reasons for underfeeding in neurosurgical intensive care unit patients. Asian Nurs Res. 2010;4:102–110.
17. Kim H, Shin JA, Shin JY, Cho OM. Adequacy of nutritional support and reasons for underfeeding in neurosurgical intensive care unit patients. Asian Nurs Res. 2010;4:102–110. doi:10.1016/S1976-1317(10)60010-2
18. Peev MP, Yeh DD, Quraishi SA, et al. Causes and consequences of interrupted enteral nutrition: a prospective observational study in critically ill surgical patients. JPEN J Parenter Enteral Nutr. 2015;39(1):21–27. doi:10.1177/0148607114526887
19. Keehn A, O’Brien C, Mazurak V, et al. Epidemiology of interruptions to nutrition support in critically ill children in the pediatric intensive care unit. J Parenteral Enteral Nutrition. 2015;39(2):211–217. doi:10.1177/0148607113513800
20. Cahill NE, Jiang X, Heyland DK. Revised questionnaire to assess barriers to adequate nutrition in the critically ill. JPEN J Parenter Enteral Nutr. 2016;40:511–518. doi:10.1177/0148607115571015
21. Artinian V, Krayem H, DiGiovine B. Effects of early enteral feeding on the outcome of critically ill mechanically ventilated medical patients. Chest. 2006;129:960–967. doi:10.1378/chest.129.4.960
22. Lee H, Koh SO, Kim H, et al. Avoidable causes of delayed enteral nutrition in critically ill children. J Korean Med Sci. 2013;28(7):1055–1059. doi:10.3346/jkms.2013.28.7.1055
23. Jain MK, Heyland D, Dhaliwal R, et al. Dissemination of the Canadian clinical practice guidelines for nutrition support: results of a cluster randomized controlled trial. Crit Care Med. 2006;34(9):2362–2369. doi:10.1097/01.CCM.0000234044.91893.9C
24. Flodgren G, Parmelli E, Doumit G, et al. Local opinion leaders: effects on professional practice and health care outcomes. Cochrane Database Syst Rev. 2011;(8):CD000125. doi:10.1002/14651858.CD000125.pub4
25. Mirhosiny M, Arab M, Shahrbabaki PM. How do physicians and nurses differ in their perceived barriers to effective enteral nutrition in the intensive care unit? Acute and Critical Care. 2021;36:342–350. doi:10.4266/acc.2021.00185
26. Arney BD, Senter SA, Schwartz AC, Meily T, Pelekhaty S. Effect of registered dietitian nutritionist order-writing privileges on enteral nutrition administration in selected intensive care units. Nutr Clin Pract. 2019;34:899–905. doi:10.1002/ncp.10259
27. O’Flynn J, Peake H, Hickson M, Foster D, Frost G. The prevalence of malnutrition in hospitals can be reduced: results from three consecutive cross-sectional studies. Clin Nutr. 2005;24:1078–1088. doi:10.1016/j.clnu.2005.08.012
28. Tume LN, Eveleens RD, Verbruggen SCAT, et al. Barriers to delivery of enteral nutrition in pediatric intensive care: a world survey. Pediatr Crit Care Med. 2020;21(9):e661–e671. doi:10.1097/PCC.0000000000002382
29. Morphet J, Clarke AB, Bloomer MJ. Intensive care nurses’ knowledge of enteral nutrition: a descriptive questionnaire. Intensive Crit Care Nurs. 2016;37:68–74. doi:10.1016/j.iccn.2016.07.001
30. Passier RHA, Davies AR, Ridley E, et al. Periprocedural cessation of nutrition in the intensive care unit: opportunities for improvement. Intensive Care Med. 2013;39(7):1221–1226. doi:10.1007/s00134-013-2934-8
31. Uozumi M, Sanui M, Komuro T, et al. Interruption of enteral nutrition in the intensive care unit: a single-center survey. J Intensive Care. 2017;5(1):52. doi:10.1186/s40560-017-0245-9
32. Chapple L-A, Chapman M, Shalit N, et al. Barriers to nutrition intervention for patients with a traumatic brain injury: views and attitudes of medical and nursing practitioners in the acute care setting. JPEN J Parenter Enteral Nutr. 2018;42(2):318–326. doi:10.1177/0148607116687498
33. Rogers EJ, Gilbertson HR, Heine RG, Henning R. Barriers to adequate nutrition in critically ill children. Nutrition. 2003;19:865–868. doi:10.1016/S0899-9007(03)00170-9
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.