Back to Journals » Patient Preference and Adherence » Volume 17
Barriers to Accessing Effective Treatment and Support for Menopausal Symptoms: A Qualitative Study Capturing the Behaviours, Beliefs and Experiences of Key Stakeholders
Received 12 July 2023
Accepted for publication 31 October 2023
Published 15 November 2023 Volume 2023:17 Pages 2971—2980
DOI https://doi.org/10.2147/PPA.S430203
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Katie Barber,1,2 Alexandra Charles3
1Clinical Lead Community Gynaecology, Oxfordshire, UK; 2Clinical Director, Oxford Menopause Ltd, Oxford, UK; 3Women’s Health, Besins Healthcare, London, UK
Correspondence: Katie Barber, Email [email protected]
Background: Historically, menopausal symptoms have been hugely under-treated and under-reported, with many women struggling to manage intrusive, bothersome symptoms which can significantly affect quality of life. In the past couple of years, awareness of the impact of the menopause has risen in the public health agenda but many women are still not receiving adequate information and support.
Aim: To gain an in-depth understanding of the barriers that impact women’s access to treatment and uptake of hormone replacement therapy (HRT).
Design and Setting: Qualitative study with perimenopausal and menopausal women, general practitioners (GPs) and gynaecologists in the UK.
Methods: Sixty-minute in-depth interviews conducted with 20 menopausal women, 30 GPs and 10 gynaecologists. Data from the interviews were analysed thematically.
Results: Barriers to seeking help for menopausal symptoms include: a lack of knowledge of the full range of symptoms, stigma, embarrassment and the belief that it is part of normal ageing. Previous negative experience in accessing advice or treatment discouraged women from pursuing help. There are substantial differences in the beliefs and attitudes towards the menopause amongst GPs and often a lack of confidence in prescribing HRT. Secondary care services can consequently be overwhelmed by an explosion in uncomplicated referrals which could be effectively managed in primary care.
Conclusion: There are barriers at each point in the management pathway: from women not feeling empowered to seek medical advice, to some women feeling their symptoms are dismissed by healthcare professionals (HCP); or HCPs not recognising some of the less common menopausal symptoms, not offering options for treatment, both hormonal and non-hormonal, or offering onward specialist referral for complex issues outside their expertise. There are multiple opportunities to address these gaps in knowledge, including the use of HCP education and culturally appropriate leaflets to reach a wider range of perimenopausal and menopausal women.
Keywords: menopause, treatment barriers, patient research, hormone replacement therapy
Introduction
Menopausal symptoms have been under-treated and under-reported for years.1 A recent survey of 4014 UK women conducted in early 2022, commissioned by Channel 4 to support the findings of a 2021 documentary on the menopause, confirmed that this is very much still the case. The majority of women, 77%, experience one or more symptoms they describe as “very difficult” and 10% of women have left their jobs because of menopausal symptoms.2
Almost half of women have not approached their GP for help or advice about the menopause.2 Of those who have, 30% experienced delays in diagnosis and 40% were offered hormone replacement therapy (HRT).2 This is despite 2015 guidance from the National Institute for Health and Care Excellence (NICE) being clear that HRT, with discussion of risks and benefits, is considered a first-line management option for those without any contraindications.3
A UK government survey of almost 100,000 women in 2021 found that 91% did not feel they had enough information about the menopause and 36% did not feel comfortable talking about it with a healthcare professional (HCP).4
In order to understand the complete, holistic picture of the barriers preventing women with menopausal symptoms accessing support and appropriate treatment, we conducted in-depth qualitative research with women, GPs and gynaecologists. We used a qualitative methodology to enable us to cross-refer and explore issues raised by different stakeholders with each other and to enable us to fit the different pieces together to identify the issues and how they might be addressed.
Previous research has concentrated on quantifying the number of women who experience menopausal symptoms, the impact of their symptoms, and whether they seek healthcare advice, are offered and, ultimately, take HRT.5–9 This study aimed to complement and enrich these findings by digging beneath the surface to understand why so few women request help or are offered treatment. The study focuses on the barriers that prevent women from approaching GPs, the barriers preventing GPs from offering treatment and why women refuse HRT. Finally, it aims to understand the role that secondary care specialist gynaecologists play.
Methods
Design
The study used a qualitative methodology with in-depth 60-minute interviews either face to face or virtually to explore and understand the perspectives of menopausal women, GPs and gynaecologists with respect to the management of menopausal symptoms.
Participants and Recruitment
Women reporting menopausal symptoms were recruited from a large opt-in consumer panel that is designed to be representative of the general population in the UK. Gynaecologists and GPs were recruited from opt-in panels of HCPs who had consented to be contacted to participate in research. Both panels are regularly maintained with demographic characteristics updated to ensure appropriate sample selection. Sampling from these databases was based on a number of criteria: Women aged between 45 and 60 who had their last menstrual period more than 12 months ago and were experiencing at least 2 menopausal symptoms. A total of 20 women were recruited from three groups: those who were diagnosed and treated with HRT; women diagnosed but not taking HRT; and women undiagnosed not on HRT. Thirty GPs and 10 gynaecologists were recruited from different geographic regions of England (London, the South East, the South West, East and West Midlands and the North), Scotland, Wales and Northern Ireland. All gynaecologists were consultant-grade and spent at least 70% of their time in direct patient care.
Data Collection
Two semi-structured interview schedules were designed to ensure that critical topics were covered in both the women and HCP interviews. Topics covered in the interviews with women included: symptoms of the menopause, attitudes to seeking healthcare advice and knowledge and beliefs about HRT. In addition to these topics, HCPs were also asked about media coverage, pressures on the NHS and referral procedures. All interviews were conducted by 2 trained interviewers who received specific training relating to the objectives of this research. In order to facilitate frank, open discussions, all interviews with women were conducted by a female interviewer. The interviews were recorded and subsequently transcribed for analysis.
Data Analysis
A grounded theory-influenced approach was used to ensure a systematic process was followed in developing knowledge and theory.10 Analysis started in parallel with data collection. Two trained researchers worked independently to identify and code statements of interest and draw out recurring themes. Both researchers had received training in qualitative methodology as part of their post-graduate degrees (MSc in Health Psychology, PhD in medicine (patient outcomes)) and many years of experience as qualitative researchers in healthcare. Both researchers received the same training for this project. Memos were written about emerging categories, to summarise a point, to critique information and to relate emergent theories to existing literature. In accordance with the grounded theory approach, data were constantly compared until “theoretical saturation” was reached and no new categories of themes emerged. Researchers compared and discussed their findings to ensure reliability and reduce bias.
Ethical Considerations
The study was conducted according to the guidelines of the Declaration of Helsinki. The study outline was reviewed by Reading Independent Research Ethics Committee in the UK.
Results
Sample
Twenty interviews were conducted with three cohorts of menopausal women. Six had been diagnosed with the menopause and were taking HRT, six had been diagnosed with the menopause and were not taking HRT and eight women were undiagnosed but experiencing symptoms and were not on HRT. Interviews were also undertaken with 30 GPs and 10 gynaecologists.
Demographics
Participating women were aged between 47 and 59 years (mean age 53.95, SD 3.69) and 15 of the 20 self-identified their ethnicity as white British. Five identified as either: Indian, Irish, African, white and black Caribbean. Eleven women had been educated to college or university level, 4 had postgraduate degrees, 4 had finished education at 18 with secondary education-level qualifications and 1 had left school aged 16 years.
Impact of the Menopause: Menopausal Women
All women viewed the menopause as a natural phase of life rather than a medical condition. Some women in each cohort had positive associations with the menopause such as “liberation”, “transformation” and “wisdom”. However, in all three cohorts most women felt that the term “menopause” has negative connotations associated with old age, their body “shutting down”, loss of fertility, becoming less attractive/invisible to society and for many it created a sense of mourning. Due to this stigma, women avoided using the term.
Hot flush severity was described as embarrassing and severity ranged from “uncomfortable” to “unbearable” or “horrendous”. This, plus night sweats and difficulty sleeping, had a large negative impact on life – at home, at work and in relationships.
Barriers to Accessing Treatment: Menopausal Women
The barriers that emerged to seeking help, accessing and accepting treatment and support are listed in Table 1.
 |
Table 1 Barriers for Women to Seek Help and Access Support |
Barriers to Seeking Help
Lack of knowledge about the range of symptoms was revealed as a major barrier to seeking help. All women knew hot flushes and cessation of periods occurred at the menopause. However, problems with memory and concentration were experienced by 19/20 women but to varying degrees and were unlikely to be attributed to the menopause in the untreated groups of women. Though experienced by nearly all women, there were mixed beliefs and knowledge on whether the following symptoms were due to the menopause: reduced libido, vaginal dryness and discomfort, headaches, mood changes, palpitations, joint stiffness, reduced muscle mass, tiredness and weight gain. These symptoms were misattributed to other causes.
Women often normalised their symptoms, putting them down to work or family stress, lockdown during the COVID-19 pandemic, or existing medical conditions or pre-existing symptoms that had simply worsened.
Many women did not seek help because they did not want to “waste a doctor’s time” or they thought the GP would not be able to do anything as “the menopause happens to everybody”. Stigma and embarrassment also prevented many women from discussing their symptoms.
Women from African and Asian backgrounds were less likely to medicalise the menopause and seek help from a doctor.
Barriers to Accessing/Accepting Treatment and Support
Where women sought help for suspected menopause or fertility, diagnosis was relatively quick and straightforward if they had typical symptoms, but it was more convoluted when they sought help for individual troublesome symptoms. This was particularly true if they had not thought of the menopause being the cause of non-specific symptoms such as mood changes and difficulty sleeping. HCPs were unlikely to ask about other symptoms of the menopause in these situations. This limited information exchange led to such non-specific symptoms either being dismissed by the HCP or attributed to depression for which they were prescribed antidepressants or cognitive behavioural therapy (CBT).
Some women diagnosed and treated with HRT reported a positive experience at their first appointment, but others had a negative experience, feeling disbelieved and ignored. Those diagnosed with the menopause but not treated with HRT did not revisit the discussion despite seeing their GP since the appointment as they felt it was a low priority for GPs;
It would’ve been nicer to have a continued discussion because it is an ever-changing thing …and I don’t feel because of the timing I’ve had that opportunity.
All women were concerned about the potential increased risk of cancer with HRT prior to seeking help, and this concern caused delays in making an appointment or taking treatment after it was prescribed. For many women, this was resolved through information provided by the GP, the media or their own research. One woman discussed “outdated” information: “There’s so much negativity and I think so many women are basing a decision on medication on a flawed study.”
However, others still had remaining concerns about cancer, which they described as a “niggle at the back of my mind”. This was overcome due to perceived necessity for treatment and trust in the GP.
Women with a menopause diagnosis but not on HRT had decided against HRT before seeing the GP. This was due to either the risk of breast cancer, a “just get on with it” attitude, apprehension around taking medication, negative labelling due to being on HRT, or concerns that periods would restart and the menopausal symptoms would revert to being as severe as they were previously as soon as they stopped treatment. In general, these women described a lack of exploration of these concerns by their GP and felt they had not received clear guidance regarding risks and benefits of HRT. Some undiagnosed women assumed symptoms would be over soon despite admitting no knowledge of the timeline.
Few women who were diagnosed were given information about the menopause at the point of diagnosis. Information that was provided ranged from basic leaflets to a website and app. Reception of the information was varied. Some women found this very helpful whereas others felt unsupported. They wanted the GP to give them the information rather than direct them elsewhere. Some undiagnosed women would consider HRT if they were more aware of the pros and cons and if their symptoms increased in severity.
There was some confusion about the term HRT and whether it was a direct replacement of their natural hormones or whether it contains additional “unnatural” hormones. Some women were told by their GP that they were better off without treatment because they would be “introducing a hormone into your body.”
Barriers to Offering Treatment: GPs
Barriers to GPs diagnosing the menopause and recommending treatment with HRT are listed in Table 2.
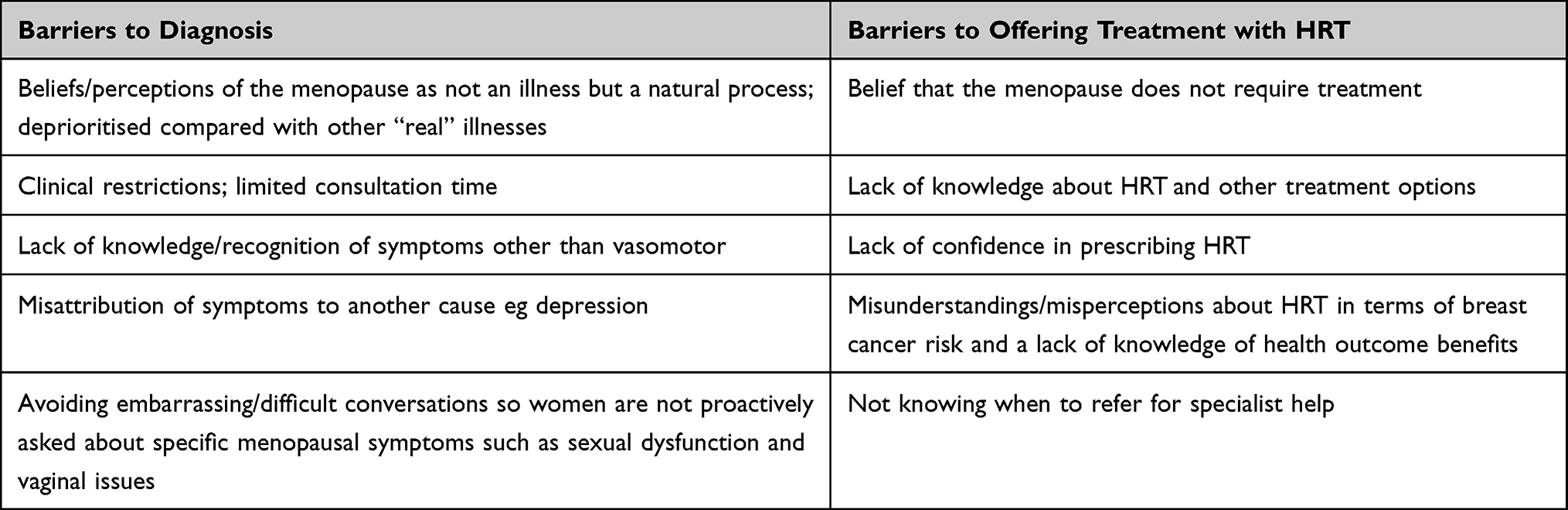 |
Table 2 GP Barriers to Diagnosis and Offering HRT |
Barriers to Diagnosis by GPs
There were two opposing, strongly held positions. One group of GPs believed that whilst the menopause is a natural process, the severity and impact of symptoms in some women results in a medical condition requiring treatment. The other group of GPs perceived that medicalising the menopause potentially exposes large numbers of women to the risks of HRT for what is a limited benefit in most cases. In this second group, there was a concern that celebrity ‘campaigns’ have been responsible for a huge upsurge in women seeking treatment with HRT. This group of GPs believe the increased demand is not appropriate and is putting too much pressure on the NHS. In particular, there has been a recent increase in younger women wanting to have a blood test to check whether they are menopausal.
Whilst most stakeholders had positive reactions to the media coverage, GPs were the most likely to express negative attitudes. Some GPs felt that media campaigns sensationalise and simplify the menopause and can be overly negative towards GPs and their handling of menopausal patients. One described feeling disbelief about media stories from women saying they have to “fight their GP” for HRT; believing instead that there is often just a delay in prescribing due to exploration of risk factors and ensuring safe prescribing.
With restrictions on the number of appointments and consultation time, despite the impact on women’s quality of life and the impact on longer-term health which they report (eg osteoporosis and cardiovascular health), most GPs do not consider the menopause to be a clinical priority. It is important because of the distress it causes, rather than for any clinical risk:
In terms of priorities obviously it’s hard to justify in a stretched primary care service those conditions [menopause] to have the same quality as more serious illness.
GPs were less likely to diagnose the menopause in women who are experiencing less common symptoms or symptoms that might be indicative of some other condition, eg low mood, atrophic vaginitis, spotting, tiredness and general aches and pains. GPs sometimes misattributed these less common symptoms to another cause such as depression or a gynaecological condition. They reported that when symptoms are more vague or generalised, women may present multiple times before these symptoms are recognised as the menopause.
Some male GPs acknowledged that it can be awkward and embarrassing talking to women during the diagnostic process about the symptoms they experience.
Barriers to GPs Offering Treatment with HRT
GPs who were more concerned about using HRT or believed that the menopause was over-medicalised, recommended the option of doing nothing and waiting for the symptoms to resolve in their own time. One group of GPs offered lifestyle advice eg weight loss and smoking cessation as a matter of course, before they offered treatment. Others provided lifestyle advice alongside active treatment. Other GPs recommended women discuss over-the-counter products, including natural products, with a pharmacist before they would prescribe HRT.
Most GPs were uncomfortable with prescribing HRT for longer than 5 years as this had been the historical duration of treatment,11 whereas the new Menopause Practice Standards (29 June 2022) state that “duration of treatment should be individualised. No arbitrary limits should be placed on the dose of HRT, duration of usage or age of women taking treatment.”12
There was variation across GPs in their knowledge about HRT and other treatment options, including some misunderstandings with regard to benefits and risks, particularly breast cancer risk. Thresholds for referral to specialists also varied, particularly depending on whether GPs lacked confidence in prescribing HRT.
Barriers to Providing Expert Help: Gynaecologists
Barriers to women receiving care and HRT from gynaecologists are listed in Table 3.
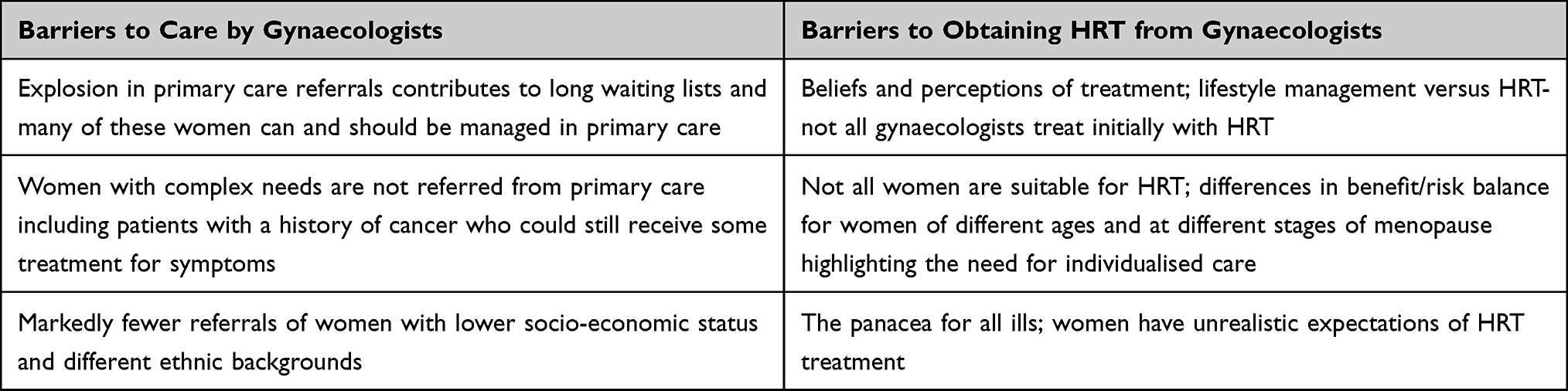 |
Table 3 Barriers to Care and HRT from Gynaecologists |
Barriers to Care by Gynaecologists
Gynaecologists reported an “explosion” in the number of women seeking help for the menopause. This included women who are premenopausal and have an increased awareness and recognition of symptoms such as sleep disruption; and women who are postmenopausal and “feel they have missed out”. Gynaecologists believed GPs were less confident in prescribing for these groups of women and this was contributing to longer waiting lists. In addition, they reported a growing number of referrals from GPs wanting specialist care for women with comorbidities such as obesity and gynaecological conditions. Gynaecologists were also receiving referrals for women who were not satisfied with prescribed HRT, wanted a second opinion, had experienced bleeding on HRT, and women with significant symptoms who did not want to take HRT.
Gynaecologists were therefore seeing more women whom they thought would be more appropriately managed in primary care, at the expense of women with more complex needs who should be referred. Women whom gynaecologists felt should be referred for specialist advice but were not, included women with a history of cancer or thrombosis. Gynaecologists reported that they were diagnosing the menopause in up to 50% of their caseload who had been referred for other reasons such as help with fertility, change in endometriosis symptoms and other gynaecological conditions.
Gynaecologists and GPs generally felt that the majority of women seeking help for the menopause and requesting HRT were white, social grade AB, well-educated women. This was even more apparent in private clinics. They believed this may be due to women from lower socioeconomic groups being less educated about the menopause and its treatment. Both GPs and gynaecologists saw fewer women from African and Asian ethnic groups and believed that the possible explanations for this included: differences in the cultural significance and meaning of the menopause; differing degrees of medicalisation of the menopause; the expectation that women will follow intergenerational cultures; media coverage portraying the menopause as a white, middle-class issue; and inherent racial bias and language barriers in seeking medical help – especially when a friend or family member is the translator.
Barriers to HRT Treatment by Gynaecologists
Whilst gynaecologists recognised that the menopause is a natural part of ageing, many felt it was a medical condition that needs to be treated, drawing parallels with other medical conditions that occur naturally eg osteoporosis and pregnancy. However, views on the symptom of “brain fog” were divided. Some gynaecologists were adamant that this was a common and highly impactful symptom. In contrast, others did not believe that brain fog is a true symptom of the menopause but is rather a natural part of ageing.
The majority believed treatment to be a necessity and some likened women’s refusal to have HRT when they needed it to women who refuse an epidural in labour: “Women will feel failure if they have an epidural, while you’re not a hero for having pain.”
Gynaecologists had differing views on which women and at what age women are suitable for HRT. Treatment also depended on the individual woman’s situation and perception of the balance of benefit and risks: “Some women think ‘I’m happy to run the risk because I cannot afford to live that quality of life that I once had of being really miserable and unhappy”. There was agreement among gynaecologists that women referred by their GP had the expectation that they would be prescribed HRT. Gynaecologists often found this frustrating, especially when HRT was not appropriate. They also found that some women had unrealistic expectations of HRT, and “see taking HRT as a thing that will fix that [problem in their life such as relationship breakdown], and it won’t”.
Discussion
Lack of knowledge about the menopause and the risks and benefits of HRT by women and GPs were the main barriers identified that are preventing women from accessing adequate support for the menopause. All three stakeholder groups recognised the need for high-quality educational materials for women, however there was often a disconnect between HCPs and women as to whose responsibility it was to share or access these materials.
There is clearly variation in care offered to women for the menopause. It is highly dependent on GPs’ attitudes and beliefs about the menopause and whether it is a condition that should be treated. Even amongst gynaecologists, the consensus was that NICE guidelines and the Menopause Practice Standards are not strictly followed and are largely outdated; treatment decisions on the whole were made based on individual patient needs.
Strengths and Limitations
A major strength of this study is that it captures a truly holistic picture of menopause from the perspectives and experiences of all key stakeholders and purposefully includes women who had sought help and those who had not to better understand help seeking behaviour. Whilst the qualitative nature of the study inherently means there was a small sample size which may bias the results, the broad findings are in keeping with those of larger surveys conducted in the UK but enriched by the individual comments. Although attempts were made to include a diverse sample of participants in each stakeholder group, the views may not be representative of all menopausal women or HCPs. The undiagnosed group may include women with symptoms due to a condition other than the menopause. In future, it may be useful to consider including GPs with additional specialist menopause knowledge/qualifications to expand the data and provide a different viewpoint.
Comparison with Existing Literature
The findings from this study confirm previous research around women’s experiences of menopause; the symptoms they experience and the impact these can have on their quality of life.6–9 What this study adds is an understanding that the barriers to accessing effective support for these symptoms are still prevalent, are fuelled by misperceptions and lack of knowledge, and operate at all levels of the healthcare system. The Women’s Health Strategy for England published in August 2022, which drew on survey responses from almost 100,000 women and over 400 written submissions from organisations and experts in healthcare, also found that accessing appropriate services for menopause care is difficult.4 Management of the menopause was the third most important topic that women wanted to be improved. Due to these findings, the UK Menopause Taskforce was established in February 2022. It aims to focus on 4 areas:
- healthcare provision
- education and awareness for the population and healthcare professionals
- workplace support
- research, evidence and data
With regard to healthcare provision, this study highlights the strains that primary and secondary care are currently facing. The oversubscription of primary care services is already recognised, with GPs feeling overwhelmed by the number of appointments that are being taken up by HRT requests since the Channel 4 documentary aired in May 2021.13 Without an increase in funding, the NHS is needing to adapt quickly to respond to this unmet need.
Although there are a number of potential short and long-term risks associated with HRT, it was concerns about the association between HRT and increased risk of breast cancer that were most frequently mentioned and remain barriers to treatment for women and some GPs as highlighted in this study. This can in part be attributed to media-fuelled misinformation and overgeneralisation of data from some key studies including the first set of findings from the Women’s Health Initiative in 200214 and a meta-analysis published in the Lancet in 2019.15 However, based on a thorough review of the most recent data including the 2020 long-term follow-up of the placebo-controlled, randomised Women’s Health Initiative (WHI) Study,16 the British Menopause Society has published a summary of current knowledge about HRT and breast cancer risk17 which concludes that:
- In women with a low underlying risk of breast cancer (ie most of the population), the symptomatic benefits of HRT use for up to five years will exceed potential harm17
- Where breast cancer risk with HRT is estimated to be elevated, the degree conferred is considered small17
- Most women will not be diagnosed with breast cancer as a result of their exposure to HRT17
The summary of product characteristics (SmPC) for most oestrogen-only or combined oestrogen-progestogen HRT preparations contraindicate women with known, past or suspected breast cancer and highlight a potential increased risk of breast cancer that is dependent on the duration of treatment and other risk factors. A recently published nested case–control study based on analysis of data from the primary care records of 98,611 women aged 50–79 with a primary diagnosis of breast cancer between 1998 and 2018, and 457,498 age and general practice matched female controls found lower incremental risk associations between longer term HRT and breast cancer and more noticeable decline in risks once HRT was stopped than in previous studies.18
Conclusions
Many women suffer menopausal symptoms that have a considerable impact on their daily lives, emotional well-being, relationships and sense of self-worth. These are women who could have a better experience if the menopause were recognised, and they had access to effective treatment. Barriers to accessing effective treatment include:
- Women’s help seeking behaviour and attitudes towards treatment, specifically HRT
- Some GPs’ beliefs about the menopause, the seriousness of the symptoms and their impact on women’s lives, difficulty in asking embarrassing/difficult questions, beliefs and misperceptions of HRT and lack of confidence and time
- Gynaecologists’ beliefs/attitudes towards HRT and when to use it and tempering women’s unrealistic expectations of HRT
Implications for Research and Practice
In some areas, the NHS is proactively addressing the increase in demand for support and treatment through provision of dedicated menopause clinics and primary care women’s health “hubs”, whilst other practices have devolved elements of responsibility to practice nurses.19 Gynaecologists reported using “Advice and Guidance” to consult on more generic cases. This service allows GPs to seek advice on cases as part of a shared management approach, without making a full referral to secondary care. Recent difficulties in supply of some HRT products have involved pharmacists working more closely on the menopause (eg sourcing products) and one consequence may be that pharmacists will become more involved in the management of the menopause, especially given the expanding role of pharmacists within Primary Care Networks (PCN).
Non-Caucasian women and/or those of lower socioeconomic status are currently less likely to be diagnosed with the menopause, contributing to large health inequalities and missed opportunities. Despite HCPs’ awareness of this, none reported pro-actively trying to identify and initiate conversations with these women. Some gynaecologists suggested language can be a barrier – they recommended using Language Line rather than a friend/family member to translate, to ensure the reliability of communication. HCPs could also recommend women read resources produced by reputable sources such as the British Menopause Society that have been written in different languages.
Despite the spotlight on the menopause over the past few years, the attitude that the menopause is simply a normal, natural part of getting older and therefore not clinically important remains a barrier both to help-seeking and prescription of treatment. As awareness improves from the multi-faceted approach recommended by the UK Menopause Taskforce, hopefully these attitudes will be changed.
Ethics
This study was submitted to Reading Independent Ethics Committee, an independent research ethics committee for review in December 2021. Having reviewed the study outline and interview guides, they confirmed that no formal ethical review was required for this research. All women and healthcare professionals provided written consent to participate in the study and consent for publication of the results and the study was conducted according to the guidelines of the Declaration of Helsinki.
Acknowledgments
With thanks to the women, GPs and gynaecologists who participated in the study.
Fiona Hammond, Charlotte Griffin and the research team at Hamell Communications provided assistance with study design, analysis and reporting and were responsible for study management. Alison Carr from Hamell Communications provided medical writing support for this article.
Funding
This study was funded by Besins. Hamell Communications received payment from Besins for assistance with the study design, data collection, analysis and reporting.
Disclosure
Alexandra Charles is an employee of Besins Healthcare UK Limited. Dr Katie Barber has received honoraria from Besins relating to the design and execution of this study but received no payment for authorship of this paper and reports personal fees from Gedeon Richter, personal fees from Theramex, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Joint Royal College of Obstetricians and Gynaecologists, Faculty of Sexual and Reproductive Health and British Menopause Society. APPG on Menopause inquiry: assessing the impacts of menopause and the case for policy reform; 2021. Available from: https://www.rcog.org.uk/media/rokly5ip/appg-menopause-fsrh-bms-rcog-joint-response-sept-2021.pdf.
2. The Fawcett Society. Menopause and the workplace; 2022. Available from: https://www.fawcettsociety.org.uk/Handlers/Download.ashx?IDMF=9672cf45-5f13-4b69-8882-1e5e643ac8a6.
3. National Institute for Health and Care Excellence. NICE guideline 23: menopause: diagnosis and management; 2015. Available from: https://www.nice.org.uk/guidance/ng23/chapter/Recommendations#managing-short-term-menopausal-symptoms.
4. Department of Health & Social Care. Policy paper: women’s Health Strategy for England; 2022. Available from: https://www.gov.uk/government/publications/womens-health-strategy-for-england/womens-health-strategy-for-england#menopause.
5. Monteleone P, Mascagni G, Giannini A, Genazzani AR, Simoncini T. Symptoms of menopause — global prevalence, physiology and implications. Nat Rev Endocrinol. 2018;14(4):199–215. doi:10.1038/nrendo.2017.180
6. Hoga L, Rodolpho J, Gonçalves B, Quirino B. Women’s experience of menopause: a systematic review of qualitative evidence. JBI Database Syst Rev Implement Rep. 2015;13(8):250–337. doi:10.11124/01938924-201513080-00018
7. Whiteley J, daCosta DM, Wagner JS, Alvir J, Shah S. The Impact of Menopausal Symptoms on Quality of Life, Productivity, and Economic Outcomes. J Womens Health. 2013;22(11):983–990. doi:10.1089/jwh.2012.3719
8. Marlatt KL, Beyl RA, Redman LM. A qualitative assessment of health behaviors and experiences during menopause: a cross-sectional, observational study. Maturitas. 2018;116:36–42. doi:10.1016/j.maturitas.2018.07.014
9. Huang D, Goodship A, Webber I, et al. Experience and severity of menopause symptoms and effects on health‑seeking behaviours: a cross‑sectional online survey of community dwelling adults in the United Kingdom. BMC Women’s Health. 2023;23:373. doi:10.1186/s12905-023-02506-w
10. Glaser B, Strauss A. The Discovery of Grounded Theory: Strategies for Qualitative Research. London: Weidenfeld and Nicolson; 1968.
11. Martin KA, Manson JE. Approach to the patient with menopausal symptoms. J Clin Endocrinol Metab. 2008;93:4567. doi:10.1210/jc.2008-1272
12. British Menopause Society. Menopause Practice Standards; 2022. Available from: https://thebms.org.uk/wp-content/uploads/2022/07/BMS-Menopause-Practice-Standards-JULY2022-01D.pdf.
13. Howard S. GPs caught in media menopause spotlight. BMJ. 2022;379:02841. doi:10.1136/bmj.o2841
14. Rossouw JE, Anderson GL, Prentice RL; Writing Group for the Women’s Health Initiative Investigators. et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the women’s health initiative randomized controlled trial. JAMA. 288;2002:321–333. doi:10.1001/jama.288.3.321
15. Collaborative Group on Hormonal Factors in Breast Cancer. Type and timing of menopausal hormone therapy and breast cancer risk: individual participant meta-analysis of the worldwide epidemiological evidence. Lancet. 2019;394:1159–1168. doi:10.1016/S0140-6736(19)31709-X
16. Chlebowski RT, Anderson GL, Aragaki AK, et al. Association of menopausal hormone therapy with breast cancer incidence and mortality during long-term follow-up of the women’s health initiative randomized clinical trials. JAMA. 2020;324(4):369–380. doi:10.1001/jama.2020.9482
17. British Menopause Society. Fast Facts. HRT and breast cancer risk; 2022. Available from: https://thebms.org.uk/wp-content/uploads/2022/12/12-BMS-TfC-Fast-Facts-HRT-and-Breast-Cancer-Risk-NOV2022-A.pdf.
18. Vinogradova Y, Coupland C, Hippisley-Cox J. Use of hormone replacement therapy and risk of breast cancer: nested case-control studies using the QResearch and CPRD databases. BMJ. 2020;371:m3873. doi:10.1136/bmj.m3873
19. NHS Somerset. Somerset NHS menopause service; 2022. Available from: https://nhssomerset.nhs.uk/health/local-services/menopause-service/.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Innovative Drug Delivery Systems for Management of Menopausal Symptoms: A Systematic Review
Bostani Khalesi Z, Abedinzade M, Golshekan M
International Journal of Women's Health 2025, 17:5425-5438
Published Date: 13 December 2025