Back to Journals » International Journal of Women's Health » Volume 9
Barriers and facilitators to cervical cancer screening among Pakistani and Somali immigrant women in Oslo: a qualitative study
Authors Gele AA, Qureshi SA, Kour P ![]() , Kumar B, Diaz E
, Kumar B, Diaz E
Received 7 April 2017
Accepted for publication 10 June 2017
Published 6 July 2017 Volume 2017:9 Pages 487—496
DOI https://doi.org/10.2147/IJWH.S139160
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Abdi A Gele,1,2 Samera A Qureshi,1 Prabhjot Kour,1 Bernadette Kumar,1 Esperanza Diaz1,3
1Norwegian Center for Minority Health Research, 2Department of Health, Institute of Nursing and Health Promotion, Oslo and Akershus University College, Oslo; 3Department of Global Public Health and Primary Care, University of Bergen, Bergen, Norway
Abstract: Norway has a low incidence and mortality rate of cervical cancer, which is mainly due to the high participation rate of women in cervical cancer screening. However, the attendance of cervical cancer screening was reported to be low among immigrant women. For this reason, we conducted a qualitative study to obtain better insight into perceived barriers and challenges to cervical cancer screening among Somali and Pakistani women in the Oslo region. A convenient sample of 35 (18 Pakistani, 17 Somali) women were recruited for the study in collaboration with Somali and Pakistani community partners. Focus group discussions were used to explore barriers and facilitators to cervical cancer screening, whereas the Ecological Model was used as the framework for the study. The study found three levels of barriers to cervical cancer screening. The individual level included a lack of understanding of the benefits of the screening. The sociocultural level included the stigma attached to the disease and the belief that women who are unmarried are sexually inactive. The system-related level included a lack of trust toward the health care system. Based on the study results, and using a common denominator approach for the immigrant groups included, the study recommends three communication strategies with the potential to improve women’s participation in cervical cancer screening: 1) in-person communication and information material at health centers; 2) verbal communication with women through seminars and workshops to educate them about their risk of cancer and the importance of screening and 3) the initiation of better recall through SMS and letters written in native languages. Finally, an intervention study that compares the aforementioned strategies and proves their effectiveness in increasing immigrant women’s participation in cervical cancer screening is recommended.
Keywords: cervical cancer, immigrant women, Somali and Pakistani women, preventive health
Background
Although cervical cancer is the third most common cancer in women globally,1 it is the most common cancer among women in many developing countries.2 Somalia is one of the countries with the highest incidence (34.8/100,000) and mortality rate (22/100,000) of cervical cancer in the world, which contrasts sharply with the incidence and mortality rate in Norway of 9.8 and 2.3/100,000 women, respectively.3 Similarly, the mortality rate of cervical cancer among women in Pakistan is twice as high as that in Norway (4.7/100,000).3 This difference is also apparent between immigrant women from high-incidence countries residing in the west and the general population.4,5 The disparities in the incidence of cervical cancer between immigrant women and mainstream women have been attributed to immigrant women’s low attendance for cancer screening tests.6,7 Cervical cancer is one of the few preventable cancers if detected early; therefore, screening of women is imperative for the prevention of cervical cancer. This paper explores the perception on cervical screenings among Pakistani and Somali immigrant women in the Oslo region of Norway.
The immigrant population in Norway has increased over the last few decades, accounting for ~16% (884,000) of the total population.8 Immigrants from Somalia and Pakistan are the two largest non-western immigrants in Norway, constituting 4.7% (41,513) and 4.3% (38,186) of the total immigrants, respectively.8 A low participation of immigrant women in cervical cancer screening has been reported in the literature.7 A recent review among South Asian immigrants in the UK, the USA and Canada reported low cervical cancer screening among women.9 The reported barriers to screening included personal barriers such as a lack of knowledge, low self-perceived risk and personal beliefs associated with religion and language issues, while systemic barriers were included with limited access to health care.7,9 A study of Pakistani women in Lahore reported a very low uptake in the screening program (2.6%), which was primarily attributed to a lack of knowledge.10 Similarly, a low participation in cervical cancer screening rates was reported among Somali women in both the USA and the Netherlands.11,12 Among the barriers reported by these studies include embarrassment due to female genital mutilation, a perceived low susceptibility of Human Papilloma Virus and cancer and a general distrust toward the health system.
The Norwegian health care system offers a cervical cancer screening test to all women between the ages of 25 and 69 years. A letter written in Norwegian was sent to all women in this age group, inviting them to make an appointment with their General Practitioner (GP) for cervical screening. As with any other consultation, women have to pay approximately €25 for the GP visit. The participation rate of this program has been reported to be 74%.13 However, more than half the women diagnosed with cervical cancer have never attended the screening test.14 Evidence shows that regardless of their country of origin, immigrant women in Norway have lower rates of participation in cervical screening, compared to Norwegian-born women.15 Despite increased attempts at different health-related interventions to reach the immigrant populations,16,17 the barriers to cervical screening continue to exist. This has created a demand for context-specific cervical cancer screening interventions to better reach immigrant women, whose risk of having the disease is higher than that of the majority of the population.4 Nonetheless, immigrants in Norway are culturally and linguistically diverse people from over 200 countries. It may not be feasible or necessary to develop and implement interventions tailored to each individual minority group in order to raise participation in cervical cancer screening. Thus, a possible solution would be to find a common denominator approach to target several immigrant groups. Women from Somalia and Pakistan form two of the largest immigrant groups in Norway, but differ in many ways, including culturally, in their migration status and in their history in Norway. Both groups are predominantly Muslim; however, Pakistanis are economic immigrants, while Somalis are predominantly refugees. In addition, Pakistani community is the oldest immigrant group in the country, whereas most Somalis came to Norway after 1990. Therefore, we conducted a qualitative study in order to acquire better insight into perceived barriers and challenges to cervical cancer screening, with the aim of identifying common features that in turn could be used to develop a culturally adapted intervention for immigrant women from different communities to help increase their participation in cervical cancer screening.
Methodology
Sample
A qualitative study using focus group discussions (FGDs) was conducted in Oslo from February to June of 2016. We used FGDs because they can encourage participation of people reluctant to be interviewed on their own, or who feel they do not have anything to say about the topic.18 FGDs are also considered important in providing a dynamic environment in which participants motivate each other’s view and have been proven effective when exploring sensitive topics.19 Moreover, FGDs were found to be important in research focusing on minority groups.18 The aim was to explore Pakistani and Somali immigrant women’s perceptions toward cervical cancer screening regarding its cultural relevance, appropriateness and acceptability. A convenient sample of 35 (18 Pakistani, 17 Somali) women were recruited in collaboration with Somali and Pakistani community partners. Two Pakistani and Somali research assistants recruited the women and conducted the FGDs. The inclusion criteria were being from Pakistan or Somalia, being aged 25–69 years old and consenting to participate in the study. We followed the common research ethics principles in carrying out this study, including informed consent, in which the right to refuse, as well as withdrawal and confidentiality, was explained to each participant. Subsequent to this, written or verbal consent was obtained from the participants. This study was not subject to the application for ethical clearance by the Regional Committees for Medical and Health Research Ethics, as it is an evaluation of quality of services only. Moreover, the study did not collect any personally identifiable information such as address, name or any other sensitive information. In addition, the study used FGDs, where participants discussed their views on the barriers and facilitators to cervical cancer screening. Therefore, we believe that there is no ethical dilemma associated with the study.
Data collection
A total of six FGDs were conducted, including three FGDs with Pakistani women and three with Somali women. The FGDs were conducted in different venues, based on women’s preferences. The FGDs were conducted in Urdu and Somali, and were tape recorded with the participants’ permission. Each focus group included five to six women and lasted for 2 hours. Among the questions explored during the FGDs were women’s perceptions about the Norwegian health system and their experience with the system. In addition, their experiences regarding gynecologic examinations and with pap smears and how they felt about them were explored. Finally, the perceived barriers to gynecologic examinations and their view of how to overcome these barriers were discussed.
Data analysis
All six focus groups were transcribed and translated into English, with the Ecological Model used as the framework for this study.20 The model allows the researcher to understand the range of factors that may put people at risk for a disease or protect them from experiencing the disease.21 This framework approach was implied for the thematic analysis of the data. The interviewers transcribed the interviews; the first and third authors systematically read the transcripts and then reread them to identify themes of importance. The interrelationship and occurrence were further compared between all transcripts.22 The coding process involved recognizing an important theme and encoding it prior to interpretation. The codes were identified in each transcript by the first and third authors, which was followed by a discussion by all authors about the identified codes. The themes that were identified through coding were divided into categories based on the participants’ common experience with barriers and facilitators to cervical cancer screening.
Results
A total of 35 women were recruited for the FGDs, including 18 women of Pakistani descent and 17 of Somali descent. The age of the Pakistani participants ranged from 25 to 70; all were married and had some level of formal education. Some of them had no children, whereas some had up to five children. The length of stay in Norway ranged between 1 and 35 years, with most of them having lived in Norway for more than 10 years. Regarding Somali women, 3 of them were single, while the remaining 14 were married. Their age ranged from 26–50 years. Most of the participants had a formal education, while some women had no formal education. The length of stay in Norway ranged from 5 to 24 years (Table 1).
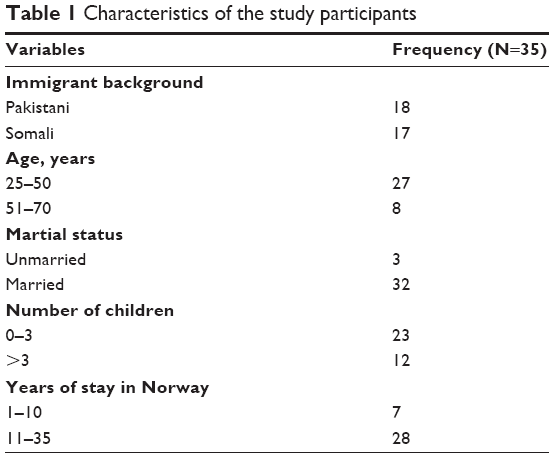 | Table 1 Characteristics of the study participants |
The Ecological Model has been used as a comprehensive framework while analyzing the data (Figure 1). Four main themes emerged from the data. Three represented barriers to cervical cancer screening, while the fourth represented facilitators to cervical cancer screening. The three themes that represented barriers to screening were identified, with data analysis based on the Ecological Model. The fourth theme was derived from our findings and added into the model in order to present participants’ perspectives of what they believed could help improve their participation with cervical cancer screening.
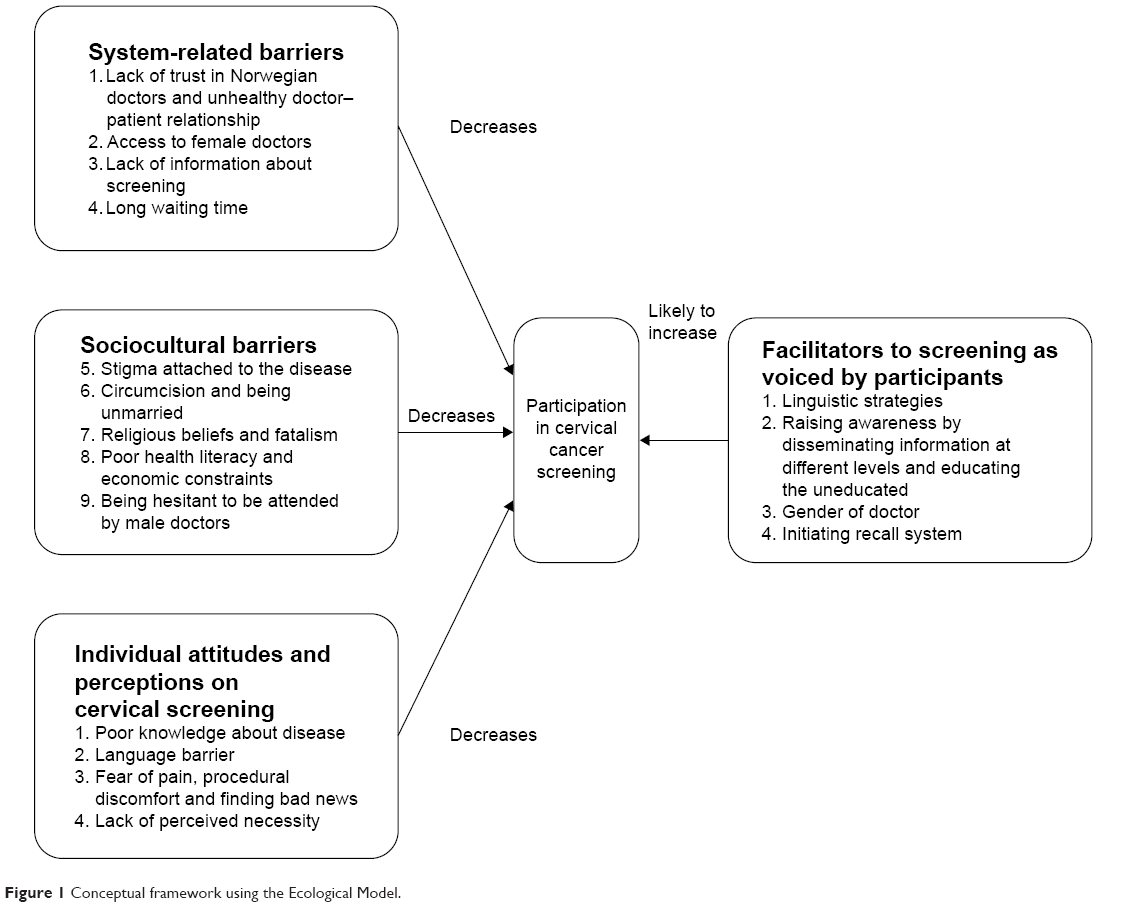 | Figure 1 Conceptual framework using the Ecological Model. |
Individual attitudes and perceptions on cervical screening
Poor knowledge about disease
Women’s description of cervical screening reflected that they had limited knowledge about the disease and its prevention. Although most of the study participants had a formal education, they showed poor knowledge about the disease:
I never had a gynecological examination here in Norway. I have no knowledge about pap smears. My GP has never talked to me about this, and I have never received any letter. I have never been screened. [Pakistani woman]
Language barrier
Language was one of the dominant barriers to cervical cancer screening, as reported by the study participants. Generally speaking, health providers often communicate in Norwegian with users, and most of the participants reported that they do not speak good Norwegian. Some women reported that they use their husbands as translators, which may limit their openness and violate their rights to privacy. Using family member as a translator is an indication of their lack of understanding of their rights to a professional translator:
I could not communicate properly with my GP due to a language problem, and I had to take my husband with me. The doctor did not tell me that I had a right to have a translator. [Pakistani woman]
Fear of pain, procedural discomfort and finding bad news
Many women reported that they do not go for a cervical screening because they are afraid of the disease and that they would instead prefer to die without knowing that they have cancer. This fear was accompanied by the fact that many women feel uncomfortable with the screening procedure, especially the sitting position while receiving the test:
I have received the letters for cervical screening, but I never sought the test. I am very allergic to hospitals and I panic and get anxious, so I try to stay away as much as possible. I have heard about mammographic screening and I am very scared about it, that what if I remain stuck to the machine. [Somali woman]
They get embarrassed when they sit on the chair and open their legs while the doctor is inspecting. [Somali woman]
Lack of perceived necessity
Most of the women in both groups have the opinion that the test should only be done in women who have some symptoms of illness. They think that only those who suspect themselves of having the disease should seek the screening. This is a clear indication of women’s lack of knowledge of the primary aim of cervical cancer screening as a preventive measure:
When I have no problem of any kind then why should I have a pap-smear. The test should be taken only when I have some complaint. [Pakistani woman]
Sociocultural barriers
Both Pakistani and Somali women had sociocultural prejudices that prevented them from participating in cervical cancer screening. These barriers included a stigma about the disease, female circumcision (for Somalis only), being unmarried, as well as the religious belief of being Muslim and not at risk for the disease. In addition, reluctance in discussing the issues related to their sexual life with their families was mentioned.
Stigma attached to the disease
Women from both communities reported stigma and a fear attached to the cancer. They related cervical cancer with sexual health and were reluctant to publicly talk about sexual health. Some stated that they never wanted to know if they had cancer, especially Somali women who constantly stated that they “hate the disease” and hence do not like talking about it:
Most of the Somalis that I talk to don’t get themselves tested. They get the letters about testing, but they threw them in the trash. They hate the disease since it can be fatal. They stay silent about it, and it is hard to get them tested. [Somali woman]
I did not go since I hated cancer, and do not want to hear anything related to it. [Somali woman]
Circumcision and being unmarried
Some of the Somali women mentioned that female circumcision is a barrier to undergoing a screening test, particularly if they are unmarried. This was due to the fact that the women who are circumcised and unmarried are considered to be sexually inactive in the community. They also reported that being circumcised and closed, they are afraid of pain, which they associate with the screening procedure:
It is quite hard to get tested on girls who are circumcised and are unmarried since they don’t like it. [Somali woman]
Religious beliefs
Some of the participants reported that being Muslim is a protective factor for cancer and other terminal diseases; as a result, they do not undergo a cervical cancer screening test. This perception was mentioned to be based on a fear of cancer, thus resulting in denial of an individual’s susceptibility to such a terminal disease, rather than based on any religious teaching. This fear may stem from a lack of accurate information about cancer and the presence of misinformation about the screening within the community:
Somalis think that Muslims won’t easily get that disease and don’t go to hospitals. They think that they are healthy and don’t need testing. [Somali woman]
We pray to Allah that we don’t get the disease … people think that Muslims don’t get that disease. [Somali woman]
Poor health literacy and economic constraints
Some of the participants were of the view that they dealt with the economic problems of their families, which took priority over their health problem. They mentioned that they did not feel the need to seek any health care until they felt sick:
I think we do not prioritize our health. Paying the monthly bills are more important for us and that’s what we care about most. It has to do with our lack of knowledge as well, as we do not realize how serious the problem can be. [Pakistani woman]
Being hesitant to be attended by male doctors
Most of the participants stated that they are hesitant in talking about cervical cancer in front of male members. Moreover, they feel shame in being genitally examined by male doctors, which may serve as a barrier in seeking cervical cancer screening:
Once I had some gynecological problems. I went for a check-up, but there was a male doctor at the health center. I felt very awkward and asked for a female but she was not available. It was not a good experience. I go for mammographic screening, but never for a pap smear. I do not discuss these issues at home with my husband. [Pakistani woman]
System-related barriers
Another important aspect that was identified as a barrier to cervical screening was system-related factors. These factors included a lack of trust in the health system, limited access to female doctors, long waiting times, a lack of information and a poor patient–doctor relationship.
Lack of trust in the health system
Both Somali and Pakistani participants showed some level of distrust toward the health system, which may be related to their past negative experiences in the system and a fear of misdiagnosis. The level of distrust was expressed more by Somali women compared to Pakistanis:
I don’t know how to trust these doctors. I know a boy, who was told that he has cancer in the throat and went through some medications here. But when he went to Germany for further consultations, he was told that he had no cancer, and that is a problem. [Somali woman]
I am not at all satisfied with the Norwegian doctors. They do not listen, when I try to tell them about my health problems, they say just one thing at a time. They do not give me enough time. [Pakistani woman]
Some of the participants also mentioned that they do not share a healthy relationship with their GPs. This was attributed to the fact that GPs do not listen and do not give them enough time to discuss their problems.
Health personnel do not listen to all our problems. They should use simple Norwegian. My daughter had some problems but a temporarily employed doctor attended to her. He kept insisting that there is no problem and the condition got worse and worse. [Pakistani woman]
Most of the participants mentioned that they do not get enough information from their GPs about the cervical cancer screening. As a result, many women may feel that screening is not important. They also reported that they were only informed about the screening when they became pregnant, but not before.
I gave birth to two children. But I did not know about the screening before I became pregnant. The doctor told me about the cancer of the cervix when I became pregnant, then I got tested. [Somali woman]
Access to female doctors
Almost all the participants delineated their discomfort with male doctors, particularly when it involves a genital examination. Women reported sometimes demanding a female doctor, but their demands are not always met. As a result, they may not go to the follow-up visits:
I developed some problem during my labor and had to go to the emergency room. The majority of the staff were male and the gynecologist was a male. I asked for a female doctor, but one was not available. This experience was very uncomfortable for me. [Pakistani woman]
Lack of information about screening
Most of the participants stated there is a lack of information about cervical screenings and a subsequent lack of knowledge about cancer prevention. They reported that they receive letters written in Norwegian, which is difficult for many of them to understand and follow:
A lack of awareness about cancer is quite common. The information letter, which was received, is also difficult to understand. [Pakistani woman]
Facilitators to cervical screening as voiced by the participants
Linguistic strategies
Most of the participants preferred information letters written in their native language to overcome the language barrier to cervical cancer screening. They mentioned that having a bilingual staff and translators would help them to better understand the disease, which may increase their participation in cervical screenings:
The letters should be written in an easy language … preferably in Urdu … and explain the test so that women do not have any fear about the test. [Pakistani woman]
To explain the disease and … to get information about this disease in Somali language so that women can understand about it. [Somali woman]
Raising awareness by disseminating information at different levels
Another important strategy mentioned by most of the participants was to educate women about the disease and give them information about the risks related to cervical cancer, the benefits of screening and their right to have a translator. The participants also mentioned the awareness of the cervical screening should be made available at health centers, religious places and through social media. Women also pointed out the importance of GPs in the provision of information about cervical cancer and the importance of screening:
Information about the test should be given by the GP because women have the most contact with GPs. [Pakistani woman]
… Lectures and seminars should be arranged in mosques and community centers, where doctors and health personnel can talk about cervical cancer screening and answer questions. But if it is in Norwegian, then there should be a translator as well. They should also explain everything to overcome fears. [Pakistani woman]
Initiating recall system
Last, the participants mentioned that there should be a recall system for increasing participation in cervical screening. The recall system mentioned by the participants included telephone calls and sending letters in women’s native languages. A few of the participants also mentioned that the test should be made mandatory, and that women should be informed on a regular basis to undergo screening.
I think it is important that the doctors tell women about the testing and how important it is, and to remind them frequently. [Somali woman]
Attendance is low because it is not obligatory to women. Women should not be allowed to decide whether to attend the screening or not, but it should be made compulsory with a specific time and a place written in the letter. [Pakistani woman]
Discussion
This study explored the challenges and opportunities in participation in cervical cancer screening among Somali and Pakistani women in the Oslo region of Norway, a topic that has not been previously documented in the literature. The results show individual, sociocultural and system-related barriers, in addition to a facilitator for cervical cancer screenings among women. The study used a common denominator approach; thus, the findings will help to develop a culturally adapted intervention that may be applicable not only for Somali and Pakistani immigrant women, but also for other immigrant groups to help raise their participation in preventive cervical screening tests.
The study used the Ecological Model for the analysis, and crafted a framework that illustrates the link and relationship between various factors affecting the participation of women in cervical cancer screening (Figure 1). The Ecological Model for health promotion pays attention to both individual and social environmental factors as targets for health promotion interventions. The model assumes that changes in the social environment will likely produce changes in individuals.23 The framework indicates that the health problem cannot be looked upon without understanding the larger context that has created it, which makes it imperative to understand the physical and social environment that strongly shapes the pattern of the health problem, as well as our response to them.24 The principles that guide the development of culturally adapted health interventions to immigrants have been developed over the past few years.12,25 Netto et al have given five principles for adapting the interventions for minorities: 1) the use of community resources to publicize the intervention and increase accessibility; 2) identify and address barriers to access and participation; 3) develop communication strategies that are sensitive to language use and information requirements; 4) work with cultural or religious values that either promote or hinder behavioral change and 5) accommodate varying degrees of cultural identification.25 The barriers and facilitators found in this study strongly support Netto’s five principles of culturally adapted intervention for minorities.
Individual attitudes such as a lack of understanding of the benefit of the screening were found to serve as barriers to cervical cancer screening. This finding is consistent with previous findings which reported that immigrant women have a limited knowledge about cervical cancer and the benefits of preventive screening tests.6,26 A study conducted on Vietnamese in the USA reported that participants were of the view that a screening test is not necessary until they feel symptoms that push them to seek care.27 Prior research reported that many Somalis have no reference for the notion of prevention and the long-term management of chronic diseases.28 Further, consulting with their GPs for chronic disease screening and illness prevention is unfamiliar to most Somalis because they are accustomed to only seeking health care when they fall ill.29 Furthermore, this study found that language is a prominent communication barrier in cervical cancer information and screening, which is in line with the findings of other studies among Somali immigrants in the Netherlands and elsewhere.7,15
Sociocultural barriers included stigma attached to the disease, which was cited by women as one of the impediments to undergoing a preventive cervical screening test. Study participants considered the disease to be the subject of embarrassment and shame, which is also found in prior research.30,31 Although sociocultural barriers such as fear, embarrassment and shame were raised by many Pakistani women, the potential for these emotions to be barriers seemed more prominent among Somali women. There is ample evidence that Asian and African women are more likely to report fear, embarrassment and shame as being responsible for delayed help-seeking regarding cancer symptoms and screening.32–34 The stigma of cancer has also been reported from ethnic minorities in the UK.35,36 Although there is a need for a large quantitative study that investigates those barriers to a larger extent, our finding supports the fact that any intervention targeted toward an increased screening of Pakistani and Somali women should help address those barriers.
Similarly, and consistent with our findings, previous research among immigrants showed that women who are unmarried are expected to not be sexually active because of the cultural acceptability and religious norms, and hence are not expected to undergo any cervical screening.26,31 Circumcision has also been reported as a barrier to cervical screening tests, as described by Somali women. Moreover, similar findings were reported from Somalis in the Netherlands.26 This perception may be explained by the fact that 98% of Somali women have experienced female genital mutilation, particularly the type three form, which involves cutting the tissues and stitching the labia together, leaving only a narrow opening for urine to pass. Therefore, a “closed” woman is considered safe from sexually transmitted diseases; consequently, they may rarely go for screenings.26 Another explanation could be that women may fear that the examination of their closed genitals may cause them pain. On the other hand, women who participated in this study demonstrated less interest in preventive health and put more of a focus on economic constraints faced by their families, which served as barriers to seeking cervical cancer screening. A study of Norwegian and Danish immigrant women in Sweden indicated that, given the competing needs faced by immigrant women, they largely neglected their health,37 which is also in accordance with our findings.
Not only did the individual and sociocultural barriers, but also the barriers related to the health system, which were very pronounced as described by the study participants, decrease the participation in preventive cervical screening tests. The lack of trust in the Norwegian health system was attributed to a poor relationship between patients and GPs, which stems from language, cultural and gender-related barriers. The GPs are the first contact point and the prime source of health information among women, and thus play an important role in women’s perceptions of cervical cancer screening.38 It is, therefore, imperative to ensure that smear takers and GPs are culturally competent to help reduce or eliminate the negative experience of minority women in cervical cancer screening.38 Some participants reported resorting to their husbands to be the translators of information, which violates the anonymity of their private information. In Norway, women with an immigrant background who are not proficient enough in Norwegian have the right to an interpreter, and this right needs to be exercised and enforced by all levels of the health system.
Recent research indicated a lower screening uptake and higher diagnosis of cervical cancer among women with an immigrant background.4,15 Another study clearly presented the role that language barriers play in health disparities, and particularly to immigrant women’s cervical cancer screening uptake.38 This study contributes important knowledge by presenting multiple factors with the potential to increase immigrant women’s uptake in cervical cancer screening. Among them is an increased access to translators. Previous studies have recommended measures to equip health care providers with the linguistic and interpreter resources they need to overcome barriers to cervical screening among immigrant women.38 We, therefore, argue that having a translator or bilingual staff at health centers will allow immigrant women to better communicate and, hence, attain more knowledge on the benefits of cervical cancer screening.
One of the important factors that can increase participation of Pakistani and Somali women in cervical cancer screening is to raise awareness of cancer prevention by disseminating information through different channels. First, information should be given to women at their initial contact with the health centers by the GPs and other health professionals at primary health care centers. In addition, information material about the disease and screening, such as brochures, pamphlets and guides, which is written in both the Somali and Pakistani languages, should be made available at the health centers. This should be supported by making female doctors available for women during screening. However, since the availability of female doctors may not sometimes be possible, women should be informed that, regardless of gender, the responsibility of the doctor is to put their health first. Second, health professionals with a cultural and linguistic competence should provide information about the risk of cervical cancer and the importance of screening to women. Because women under study came from oral societies, direct communication with women is the most preferred information channel among them. Prior studies among immigrant women have also made similar suggestions.37 Finally, using social media such as SMS and social websites, in addition to sending letters written in the native languages of women to establish recalls will increase the level of participation of cervical cancer screening among immigrant women.
Our study should be viewed in light of the following limitations. First, the reported results are the perspectives of 35 participants, so it is unclear whether this is the view of the majority of Somali and Pakistani women in Norway. However, women who participated in the study were very open to sharing their beliefs and opinions, and because the FGDs were conducted in their native language, women got a chance to express their views. Furthermore, the study participants were a highly diverse group regarding their level of education, age, marital status and ethnicity, which may have increased the representativeness of the information provided by the women. In conclusion, the study presents barriers and facilitators to cervical cancer screening among women with a very high risk of cervical cancer and a low participation of cervical cancer screening. We highlighted the beliefs, cultural insights and experiences that determine or shape the decisions of these women about participation in cervical screening. Based on the study results, we recommend three communication strategies with the potential to improve women’s participation in cervical cancer screening: 1) in-person communication and information material at health centers; 2) verbal communication with women through seminars and workshops to educate them about their risk of cancer and the importance of screening and 3) the initiation of better recalls through SMS and letters written in native languages. Finally, an intervention study that compares the aforementioned strategies and investigates their effectiveness in increasing immigrant women’s participation in cervical cancer screening is recommended.
Acknowledgments
The authors wish to thank Ubah Abshir for collecting data from the Somali participants, as well as the Somali and Pakistani communities in Oslo for collaborating with the study team. Last, thanks are also due to the participants of the study for their participation and help. We also wish to thank the Norwegian Cancer Association and the Norwegian Center for Minority Health Research (NAKMI) for funding the study.
Disclosure
The authors report no conflicts of interest in this work.
References
Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61(2):69–90. | ||
World Health Organization. 10 Facts on cancer. WHO. Available from: http://www.who.int/features/factfiles/cancer/facts/en/. Accessed March 10, 2017. | ||
World Health Organization; 2012. Globocan 2012: Estimated Cancer Incidence Mortality and Prevalence Worldwide in 2012. Available from: http://globocan.iarc.fr/ia/World/atlas.html. Accessed March 10, 2017. | ||
Azerkan F, Sparén P, Sandin S, Tillgren P, Faxelid E, Zendehdel K. Cervical screening participation and risk among Swedish-born and immigrant women in Sweden. International Journal of Cancer. 2012; 130(4):937–947. | ||
Arnold M, Razum O, Coebergh JW. Cancer risk diversity in non-western migrants to Europe: an overview of the literature. Eur J Cancer. 2010;46(14):2647–2659. | ||
Ghebre RG, Sewali B, Osman S, et al. Cervical cancer: barriers to screening in the Somali community in Minnesota. J Immigr Minor Health. 2015;17(3):722–728. | ||
Johnson CE, Mues KE, Mayne SL, Kiblawi AN. Cervical cancer screening among immigrants and ethnic minorities: a systematic review using the Health Belief Model. J Low Genit Tract Dis. 2008; 12(3):232–241. | ||
Statistics Norway. Immigrants and Norwegian-born to immigrant parents, 2013. Available from: http://www.ssb.no/en/befolkning/statistikker/innvbef/aar/2013-04-25#content. Accessed March 10, 2017. | ||
Crawford J, Ahmad F, Beaton D, Bierman AS. Cancer screening behaviours among South Asian immigrants in the UK, US and Canada: a scoping study. Health Soc Care Community. 2016;24(2):123–153. | ||
Imam SZ, Rehman F, Zeeshan MM, et al. Perceptions and practices of a Pakistani population regarding cervical cancer screening. Asian Pac J Cancer Prev. 2008;9(1):42–44. | ||
Morrison TB, Flynn PM, Weaver AL, Wieland ML. Cervical cancer screening adherence among Somali immigrants and refugees to the United States. Health Care Women Int. 2013;34(11):980–988. | ||
Verdonk P, de Boer F, Abma TA. “A Somali girl is Muslim and does not have premarital sex. Is vaccination really necessary?” A qualitative study into the perceptions of Somali women in the Netherlands about the prevention of cervical cancer. Int J Equity Health. 2015;14(1):68. | ||
Skare GB, Lönneberg S. Årsrapporten 2013–2014. Masseundersøkelsen mot livmorhalskreft. Oslo: Kreftregisteret. Institutt for populasjonsbasert kreftforsknin. [Skare GB & Lönneberg S. Annual Report 2013–2014. Mass Survey against Cervical Cancer. Oslo: Cancer Registry. Department of Population-Based Cancer Research]. 2015. Available from: https://www.kreftregisteret.no/globalassets/publikasjoner-og-rapporter/livmorhalskreft/arsrapport/livmorhals_2015.pdf. Accessed March 10, 2017. Norwegian. | ||
Cancer registry of Norway, Cervix cancer. Cancer registry of Norway, Oslo. 2016. Available from: https://www.kreftregisteret.no/globalassets/publikasjoner-og-rapporter/livmorhalskreft/arsrapport/aarsrapport-livmorhalsprogrammet-2015.pdf. Accessed March 10, 2017. | ||
Møen KA, Kumar B, Qureshi S, Diaz E. Differences in cervical cancer screening between immigrants and non-immigrants in Norway: a primary healthcare register-based study. Eur J Cancer Prev. In press 2016. | ||
Resnicow K, Baranowski T, Ahluwalia JS, Braithwaite RL. Cultural sensitivity in public health: defined and demystified. Ethn Dis. 1999; 9(1):10–21. | ||
Razum O, Spallek J. Addressing health-related interventions to immigrants: migrant-specific or diversity-sensitive? Int J Public Health. 2014;59:893–895. | ||
Kitzinger J. Qualitative research. Introducing focus groups. BMJ. 1995;311(7000):299–302. | ||
Upvall MJ, Mohammed K, Dodge PD. Perspectives of Somali Bantu refugee women living with circumcision in the United States: A focus group approach. Int J Nurs Stud. 2009;46(3):360–368. | ||
McLeroy KR, Bibeau D, Steckler A, Glanz K. An ecological perspective on health promotion programs. Health Educ Q. 1988;15(4):351–377. | ||
Centre for Disease Control and Prevention. Ecological Model. Available from: https://www.cdc.gov/violenceprevention/overview/social-ecologicalmodel.html. Accessed March 10, 2017. | ||
Merriam SB, Tisdell EJ. Qualitative research: A guide to design and implementation. San Francisco, CA, USA: John Wiley & Sons. 2015. | ||
Fielding JE, Teutsch S, Breslow L. A framework for public health in the United States. Public Health Reviews. 2010;32:174–189. | ||
Liu JJ, Davidson E, Bhopal RS, et al. Adapting health promotion interventions to meet the needs of ethnic minority groups: mixed-methods evidence synthesis. Health Technol Assess. 2012;16(44):1–469. | ||
Netto G, Bhopal R, Lederle N, Khatoon J, Jackson A. How can health promotion interventions be adapted for minority ethnic communities? Five principles for guiding the development of behavioural interventions. Health Promot Int. 2010;25(2):248–257. | ||
Ma, GX, Gao W, Fang CY, et al. Health beliefs associated with cervical cancer screening among Vietnamese Americans. J Womens Health (Larchmt). 2013;22(3):276–288. | ||
Morrison TB, Wieland ML, Cha SS, Rahman AS, Chaudhry R. Disparities in preventive health services among Somali immigrants and refugees. J Immigr Minor Health. 2012;14(6):968–974. | ||
Pavlish CL, Noor S, Brandt J. Somali immigrant women and the American health care system: discordant beliefs, divergent expectations, and silent worries. Soc Sci Med. 2010;71(2):353–361. | ||
Shelton RC, Jandorf L, Thelemaque L, King S, Erwin DO. Sociocultural determinants of breast and cervical cancer screening adherence: An examination of variation among immigrant Latinas by country of origin. J Health Care Poor Underserved. 2012;23(4):1768–1792. | ||
Redwood-Campbell L, Fowler N, Laryea S, Howard M, Kaczorowski J. ‘Before you teach me, I cannot know’: immigrant women’s barriers and enablers with regard to cervical cancer screening among different ethnolinguistic groups in Canada. Can J Public Health. 2011;102(3): 230–234. | ||
Robb K, Wardle J, Stubbings S, et al. Ethnic disparities in knowledge of cancer screening programmes in the UK. J Med Screen. 2010; 17:125–131. | ||
Forbes LJ, Atkins L, Thurnham A, et al. Breast cancer awareness and barriers to symptomatic presentation among women from different ethnic groups in East London. Br J Cancer. 2011;105:1474–1479. | ||
Williams M, Kuffour G, Ekuadzi E, et al. Assessment of psychological barriers to cervical cancer screening among women in Kumasi, Ghana using a mixed methods approach. Afr Health Sci. 2013;13: 1054–1061. | ||
Thomas VN, Saleem T, Abraham R. Barriers to effective uptake of cancer screening among Black and minority ethnic groups. Int J Palliat Nurs. 2005;11:562,564–571. | ||
Randhawa G, Owens A. The meanings of cancer and perceptions of cancer services among South Asians in Luton, UK. Br J Cancer. 2004; 91:62–68. | ||
Azerkan F, Widmark C, Sparén P, Weiderpass E, Tillgren P, Faxelid E. When life got in the way: How danish and norwegian immigrant women in Sweden reason about cervical screening and why they postpone attendance. PloS one. 2015;10(7):e0107624. | ||
Marlow LAV, Waller J, Wardle J. Barriers to cervical cancer screening among ethnic minority women: a qualitative study. J Fam Plann Reprod Health Care. 2015;41(4):248–254. | ||
Jacobs EA, Karavolos K, Rathouz PJ, Ferris TG, Powell LH. Limited English proficiency and breast and cervical cancer screening in a multiethnic population. Am J Public Health. 2005;95(8):1410–1416. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.