Back to Journals » Advances in Medical Education and Practice » Volume 16
Barriers and Facilitators of Simulation-Based Education in Stroke Nursing Management at a Regional Referral Hospital in Southwestern Uganda: A Qualitative Study
Authors Najjuma JN, Bajunirwe F ![]() , Mbalinda SN
, Mbalinda SN ![]() , Ssedyabane F
, Ssedyabane F ![]() , Mwebembezi G
, Mwebembezi G ![]() , Moore S, Kaddumukasa M
, Moore S, Kaddumukasa M ![]() , Atukunda EC
, Atukunda EC ![]()
Received 8 May 2025
Accepted for publication 25 July 2025
Published 4 August 2025 Volume 2025:16 Pages 1317—1329
DOI https://doi.org/10.2147/AMEP.S535086
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh Arja
Josephine Nambi Najjuma,1 Francis Bajunirwe,1 Scovia Nalugo Mbalinda,2 Frank Ssedyabane,1 Gerald Mwebembezi,1 Shirley Moore,3 Mark Kaddumukasa,2 Esther C Atukunda1
1Faculty of Medicine, Mbarara University of Science and Technology, Mbarara, Uganda; 2College of Health Sciences, Makerere University, Kampala, Uganda; 3Frances Payne Bolton School of Nursing, Case Western Reserve University, Cleveland, OH, USA
Correspondence: Josephine Nambi Najjuma, Faculty of Medicine, Mbarara University of Science and Technology, P. O Box 1410, Mbarara, Uganda, Email [email protected]
Introduction: Simulation-based education (SBE) improves skills and knowledge among health professionals. Stroke nursing necessitates swift decision-making, elevated levels of clinical competence, and interdisciplinary collaboration. SBE improves these competencies but encounters implementation challenges. The objective of this study was to explore the barriers and facilitators of SBE implementation for stroke care for nurses at a referral hospital in Uganda.
Methods: From March to July 2024, a descriptive qualitative study was carried out at Mbarara Regional Referral Hospital and Mbarara University of Science and Technology using focus group discussions (FGDs), and key-informant interviews (KIIs). The FGDs were carried out with nursing students. The KIIs participants included purposively selected nurses, nurse educators, and other health care providers involved in stroke care and bedside teaching. The study was guided by the Consolidated Framework for Implementation Research (CFIR) and used deductive thematic analysis to identify barriers and facilitators for simulation-based stroke education (SBSE).
Results: We conducted 4 FGDs, and 12 KIIs. The FGDs participants’ mean age was 24 years and 36 years for other participants in KIIs. The barriers to SBSE included anticipated high cost for simulation methods, the anticipated high costs to translate lessons learned to real hospital setting, resistance to change from established routines. The high patient-to-nurse ratios and lack of stroke-specific structured training are also barriers. The facilitators included strong institutional administrative support for simulation methodology, availability of training facilities at the simulation center, and prior exposure to simulation methodologies.
Conclusion: Strong administrative support exists for SBSE. However, for successful implementation, there is a need to address the resource limitations, address anticipated resistance to change, and foster a culture of continuous learning and improvement within healthcare institutions. Future interventions should strategically address identified barriers while leveraging facilitators can enhance the success of SBSE stroke nursing care in resource-limited settings.
Keywords: stroke, education, simulation, nurses, Uganda
Introduction
Globally, stroke is the leading cause of death and a serious cause of long-term acquired physical disability in adults.1,2 The incidence of stroke is increasing in Sub-Saharan Africa (SSA).3 In Uganda, stroke affects relatively young individuals, and it accounts for 15% of hospital admissions and constitutes a major contributor to mortality.4 Statistics at Mbarara Regional Referral Hospital (MRRH) reported a thirty-day mortality rate of 38.1% for patients with stroke,5 and most of these patients were cared for by a team of healthcare providers, largely made up of nurses.
Stroke management requires adequate nursing knowledge, and a unique skill set to reduce the rapid development of associated complications, disability, and dysfunction.6 In stroke units, nurses are involved in all aspects of stroke care from admission to discharge and sometimes post-discharge care.7 Effective stroke management in nursing involves a multifaceted approach that includes acute care, secondary prevention, rehabilitation, and patient/family education.8 To provide the required and appropriate stroke patient nursing care, nurses must be equipped with the proper patient-centered skill set and approaches to effectively prevent and manage catastrophic complications and deaths that arise from stroke.9 These approaches should be enshrined within both pre-service and in-service nurse training.
Nurse education in stroke care is vital in delivering high-quality and efficient care, as nurses not only make up the largest bulk of health professionals, they also oversee most of the management of stroke.10 Noteworthy, some nurses may receive generalized training. However, with the increasing number of stroke patients, there is a need to develop stroke-specific training for nurses.11 Through tailored training, nurses can acquire and improve competencies to better their management skills and improve the outcomes of patients with stroke.10,12 The lack of stroke-specific nursing education may result poor patient outcomes, including inadequate management and or prevention of complications, long hospital stays among others.
Therefore, interactive teaching methodologies have been recommended to provide nurses with opportunities to actively participate in the learning process.13–15 Among the active learner-centered approaches, simulation-based education (SBE) has been highly recommended by nurse educators.14,16 Implementation SBE in low- and middle-income settings (such as Uganda) may encounter specific challenges such as poor stakeholder buy in, and resource constraints,16 but it could also yield educational benefits.17 SBE is a crucial component of nursing education, particularly in high-stakes time-sensitive fields like stroke. SBE improves of competencies such as knowledge, clinical skills, teamwork, critical thinking, problem-solving skills, patient safety, effective communication, role clarity, and confidence among nursing and other healthcare teams14,17–19 without compromising patient safety20 to improve procedural accuracy and adherence to protocols. Even though SBE has known benefits, not much is known about factors that affects its use in stroke care in Sub-Saharan Africa. Also, there is limited clarity on how institutions and stakeholders will adopt and implement this innovative educational approach. The Consolidated Framework for Implementation Research (CFIR) is a recognized and commonly used frame-work,21–23 and was chosen for its ability to assess contextual factors, conceptualize, and distinguish between the contextual determinants of implementation success.24 Thus, this study aimed to identify barriers and facilitators to using SBE to train nurses in stroke management at Mbarara Regional Referral Hospital, Uganda. The context-specific barriers and facilitators will inform the implementation of SBE for stroke nursing care.
Methods
Study Design and Setting
We conducted an exploratory qualitative study from March to July 2024 at Mbarara University of Science and Technology (MUST) and Mbarara Regional Referral Hospital (MRRH) in Uganda. MRRH is the teaching hospital for MUST. MUST and MRRH are in Mbarara City, southwestern Uganda, approximately 260 km from Kampala – the capital city. The department of nursing is part of the Faculty of Medicine at MUST. Nurse educators are involved in bedside teaching, and care of patients at MRRH. MUST nursing students participate in the care of patients with stroke, as part of their learning.
Study Participants and Recruitment
We interviewed nurses and other healthcare professionals who are involved in the management of stroke patients at MRRH. These healthcare providers work at the Accident and Emergency ward, Intensive care unit, medical, and or surgical wards. They are also involved in bedside teaching for the nurses. These healthcare professionals included physicians, neurosurgeons, intern doctors, residents, and rehabilitation therapists. We also included active nurse educators at MUST through in-depth interviews. We included both male and female participants. All participants were above 18 years old. We also interviewed Bachelor of Nursing Science students from MUST who were in clinical years using Focus Group Discussions (FGD). And had rotated on the wards where stroke patients are admitted. The nursing students also had prior exposure to simulation. These students had rotated on the wards or units where stroke patients receive care from and attended lectures that provide content for stroke nursing management, including medical-surgical nursing and critical care nursing. Each FGD consisted of 5 participants and a total of 20 nursing students in their final and semi-final year participated in the study.
Sampling Procedure
We purposively selected active clinical educators and clinical-year nursing students and recruited them as the study participants. Potential candidates were approached for written informed consent. Participant recruitment continued until the saturation point was reached as used previously.25
Data Collection
Data were collected using key informant interviews with the different professionals involved in stroke management and bed side teaching at MRRH, and nurse educators from MUST. We also conducted focus group discussions with nursing students. Data collection was conducted by a trained research assistant who was not known to the study participants to allow free expression of their opinions. The interviewer was also not part of the research investigators. The interviewer was assisted by a note taker who also served as a timekeeper. All interviews were audio recorded, conducted in English in a room with no interruptions, to allow for uninterrupted discussions. The same interviewer conducted the KII and FGD for consistence. The data collection took place from March to July 2024.
A semi-structured interview guide was designed using the Consolidated Framework for Implementation Research (CFIR) tool.23 We adopted questions from the five domains of the CFIR. The CFIR domains are: intervention characteristics, inner setting, outer setting, characteristics of individuals and process of implementation.23 The interview guides consisted of questions from CFIR constructs that were relevant to the study. The semi-structured interview guide was designed and adopted by the JNN and was reviewed by the team before it was used for data collection.
Data Management and Analysis
Data were transcribed verbatim by the notetaker and checked by the interviewer against the audio recordings for correctness of information. The transcription process was assisted by the field notes. Data analysis began with open coding which involved reading the transcripts line-by-line, to familiarize with the data. The data were then categorized in codes. Categories composed of codes that have similar information. Categories were then compared to confirm that they were not overlapping to make the final number of codes. Codes and descriptions were used in the transcripts to ensure the anonymity and confidentiality of the participants. The data analysis process was led by a research assistant (GA) who developed the codes. The team (JNN, GA, JT AND FS) had several meetings to compare the results and discuss the analysis process and to resolve discrepancies, in the codes and these were discussed in these team meetings. Audio files and transcripts are stored on a password-protected computer and only accessed by the research team. Thematic analysis was used to analyze the data with the help of NVivo (Version 12; QSR international). Codes were developed in line with the CFIR domains (the intervention characteristics, the outer setting, the inner setting, the characteristics of the individuals involved, and the process of implementation). Member checking was done to ensure data trustworthiness, transcripts were validated within the organization.
Ethical Considerations
All methods were carried out in accordance with the relevant guidelines and regulations. Before the data collection. Ethical clearance for the study was obtained from Uganda National Council of Science and Technology (HS3535ES) and the MUST Research Ethics Committee (MUST-2023-1157). All participants provided written informed consent before taking part in the research activities. Participants also provided informed consent for audio-recording of the interviews and publication of anonymized responses/direct quotes. Each participant was given a unique identifier that was used for identification. Only participant identification numbers were included in the transcripts. All study data was collected in password protected laptop that is only accessed by the study team. All study participants gave consent to publish.
Trustworthiness
The criteria for trustworthiness and authenticity guided the study.26 These include credibility, transferability, Dependability/consistency, conformability/neutrality. The data collection team spent more than 30 minutes with the participants in the FGD to create rapport before the data collection started. The appointments for data collection and the time given was to the participants in the KIIs gave them time to ask create rapport with the team and encourage a smooth and easy sharing. The note taker kept a detailed journal throughout the study where feeling and expressions were recorded. The study was well thought through by describing the research design and methods used in the study. An experienced, qualitative researcher with a nursing background and a research assistant comprised the data collection team. The audio recordings were transcribed verbatim, and member checking was done for accuracy. The peer review system provided constructive criticism to the methodology and analysis of the work.
Positionality
The lead researcher is a nurse and a member of the MUST simulation center team. The most of the other study investigators are health care providers and or educators and are aware of SBE. The investigators did not carry out the data collection instead, an experienced qualitative researcher with 5-year experience and a nurse led the data collection. The investigators-maintained awareness of their opinion and disregarded them during the analysis.
Results
Participants Demographics
Twelve (12) health care providers or educators (2 females and 10 males) were interviewed. Their highest level of education ranged from diploma to Masters degrees. They had all worked for more than one year in the wards where stroke patients are admitted and their age ranged from 27 to 51 years. (Table 1) (We do not include the participants role as this might expose the identity of the participants). We conducted 4 FGD with a total of 20 nursing students. These included 12 males and 8 females; average age of FGD participants was 24 years (Table 2).
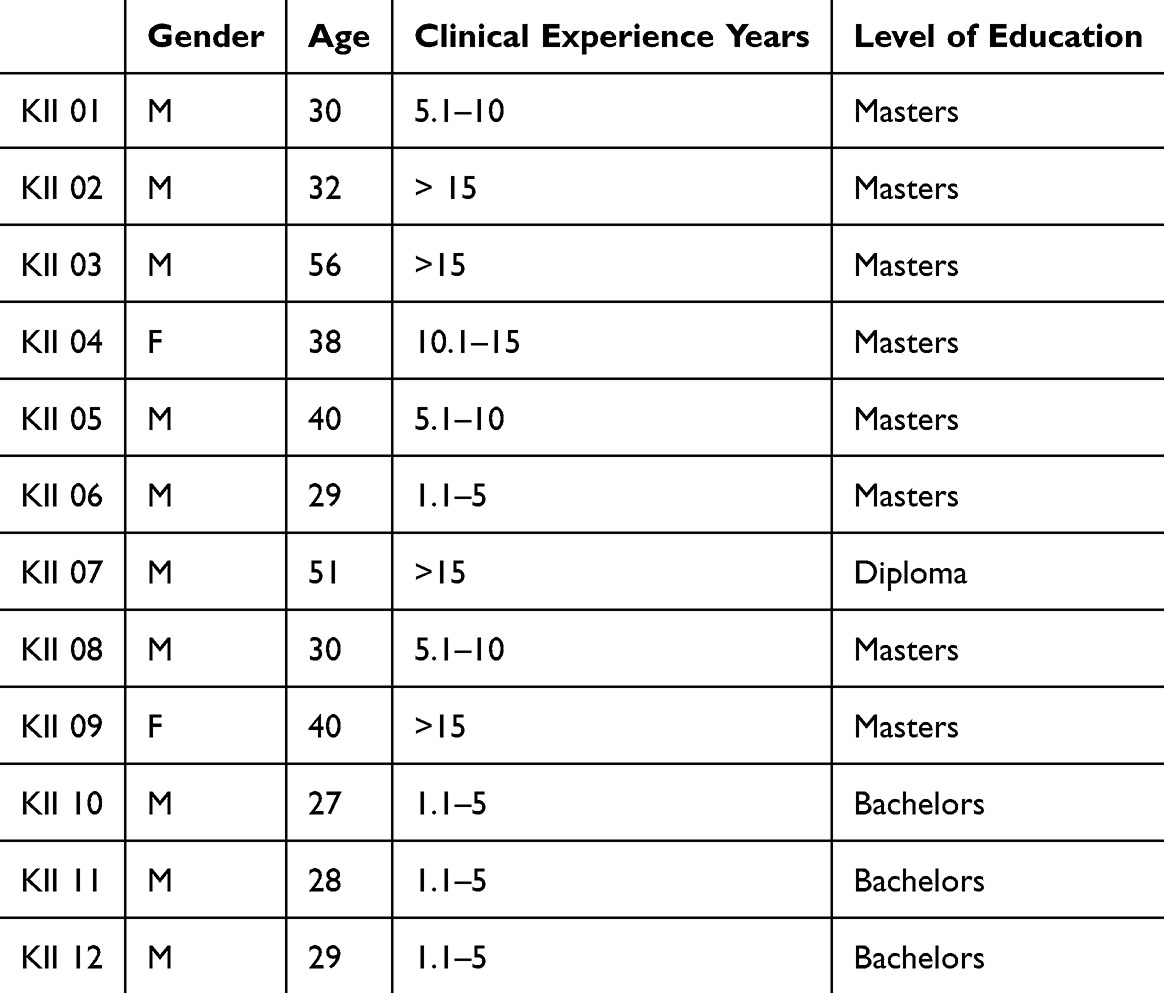 |
Table 1 Characteristics of Key Informant Interview Study Participants |
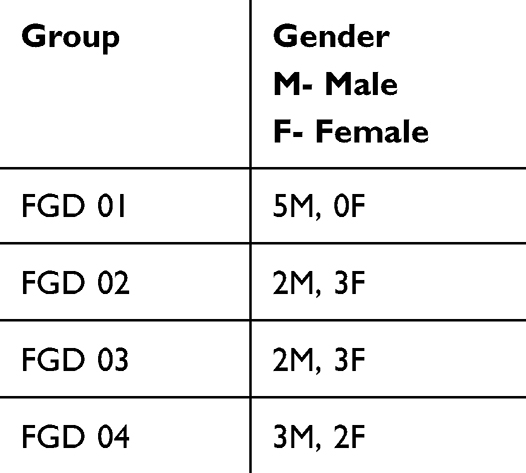 |
Table 2 Characteristics of Focus Group Discussion Study Participants |
Table 1 shows the characteristics of the key informant interviews. We do not include their professions, marital status, current role, and religion in the table as this might disclose their identity.
Interviews and FGD Results
The qualitative data was described in the five constructs of the CFIR model (Table 3). The data from the transcripts of interviews and focus group discussions about barriers and facilitators of simulation-based education for nurses in stroke management the following themes merged.
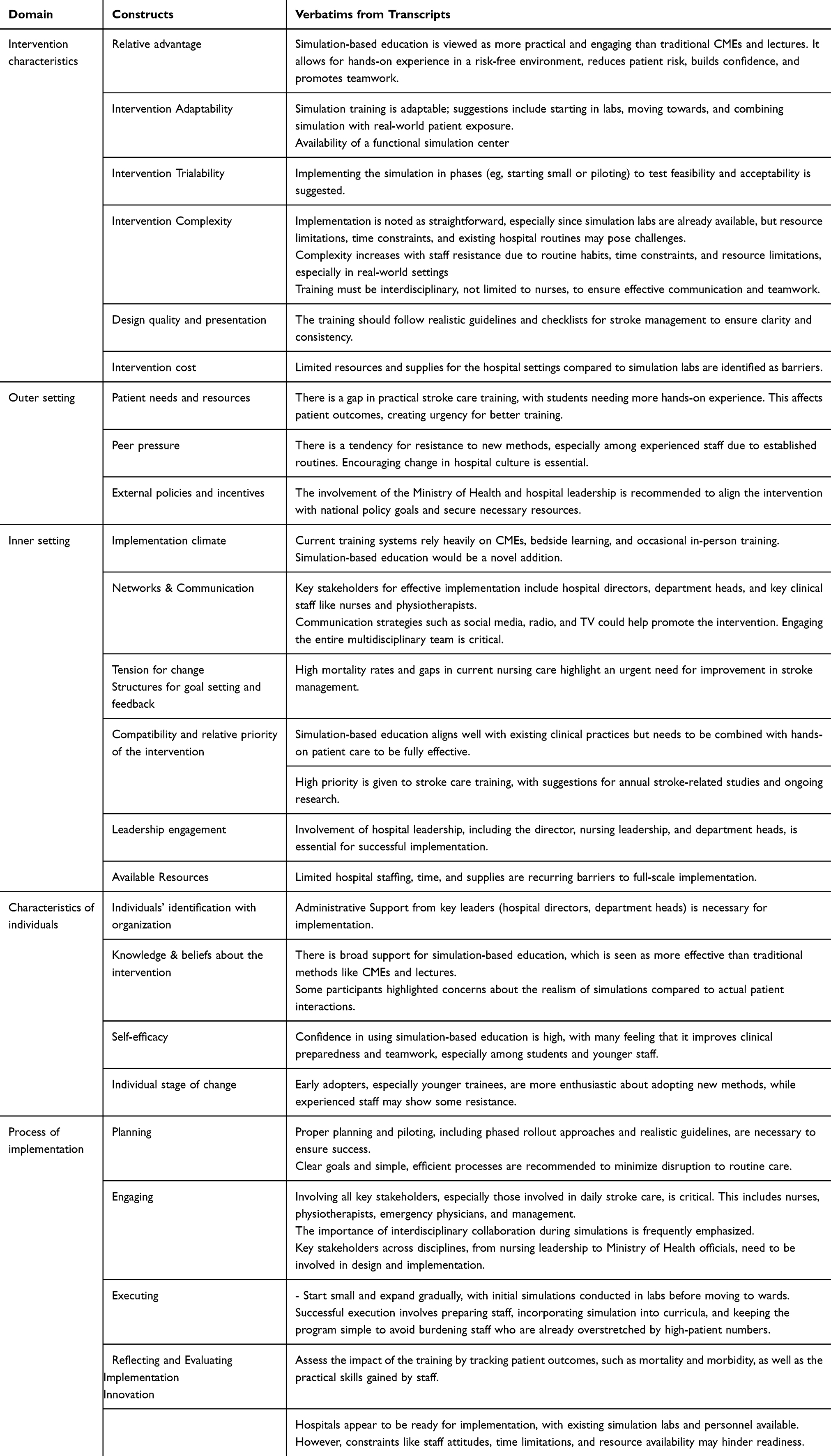 |
Table 3 CFIR Constructs for Implementing SBSE for Stroke Nursing |
Barriers to Simulation-Based Education in Nursing Stroke Management
Resource Constraints for Simulation and Translation to Care (Intervention Characteristics)
The intervention cost was noted as a barrier. Participants mentioned that the cost of the resources to run a simulation intervention might not always be readily available. It was emphasized that the cost of resources that are required to implement the skills learnt from the simulation session to the hospital setting are sometimes higher than the current funding limits.
Implementation simulations will need more costs, compared to the traditional bedside training that doesn’t need costs though the challenge remains that you teach as they go. (KII, 004, Male)
Because in a lab. I somehow implement it…But down there in a hospital. It doesn’t work. So that would make it very difficult. Because if you are doing a simulation session. I believe you must do the ideal. What is supposed to be done? Not improvise. And down at the referral, everything we are trained to do is to improvise. So, it would pose a challenge. Participant 5, FGD 3, Male
Anticipated Resistance to Change and Staffing (Outer Settings)
Participants observed potential resistance from experienced nurses to new learning methods because they are used to being set in routines, and this may pose challenges. Some participants mentioned that this might be coupled with the established routines that might hinder the adoption of new approaches like simulation training. The nurses serve on a specific duty time and leave immediately the hospital once their duty time ends. There must be an interruption of this routine for simulation training to take place.
…And truly, it’s going to be uneasy to bring out those experienced nurses and do the simulation and then try to undo the things. …. KII 09, Male
The high numbers of patients compared to the nurses available on the ward was also identified as a barrier. Limited staffing in the hospital and the busy schedules of healthcare workers compounded by high patient numbers pose a challenge, making it difficult to allocate sufficient time for simulation training without disrupting patient care.
Because in sim labs, you always have what you need somehow to be provided. But when you go down there, there are no supplies to try and implement that. So, a modification that can come into simulation is as we’re training them, we’ll try to seek out what is ongoing so that we can teach the people we are training how to improvise with what they have on hand. KII 09, Male
Facilitators to Simulation-Based Education in Nursing Stroke Management
Prior Exposure to Simulation (Inner Setting)
Interviewees noted that simulation training is more engaging and practical compared to traditional Continuing Medical Education (CME) sessions. They suggested that simulations could bridge the gap between theoretical knowledge and real-world application.
I think simulation might be better. Because it is hands-on. According to the experience that I have in caring for these stroke patients, it’s hands-on. I think simulation is better. But you begin with the theory that is the CMEs, then you just go into simulation. Because people will have to enjoy it as I have told you. Most today’s nurses and doctors do things without rationale. KII 03, Male
I would go with simulation because if you are to look at simulation sessions, we are having hands-on in a safe environment, and therefore there they can be able to acquire the basic knowledge about stroke and the best knowledge about the management for this patient such that the moment they go to the wards they have baseline knowledge to start on the management and assessment. Participant 2, FGD 2, Male
Participants with prior exposure to simulation expressed strong support for simulation-based training, highlighting its relative advantage over other teaching methods including the effectiveness in promoting teamwork, providing hands-on experience, and achieving learning objectives.
I have been through simulation sessions, and they are very good compared to the other alternatives because they link the in-class lectures and also the videos watched to the real-life situation as they give a picture and a hands-on experience. Though it is not on the real patient it gives that confidence, skills and also being at ease and alert in case a person is encountered by any stroke condition and management. Participant 01, Male FGD 01
Another participant who had been exposed to simulation-based learning as both a learner and facilitator emphasized that it is close to what is seen in the hospital setting.
I’m lucky to have been part of simulation training and I must say this is as close as we get to reality because sometimes when you’re just told or you see someone doing something without you having experience, it can bring in fear of handling this patient…But when we simulate the care of this patient, it’s easy to translate it into reality. KII 09, Male
Recommendations for Implementation
Participants also shared proposals to incorporate stroke management simulation training into medical and nursing curricula for successful implementation and sustainability.
So, we make sure we incorporated this one into the curriculum, in that all the medical professions at MUST they study rehabilitation medicine. And it is taught by this department such that each professional knows what to do and what their fellows do. And this one has facilitated the nursing care, vis-a-vis, physio care, physician care, and whatsoever. KII 06, Male
It’s easy to implement it…It’s just that we have to incorporate it into the academic program so that we start pitching or throwing in these ideas as early as possible. They say you cannot teach an old dog new tricks. It is the same. And truly, it’s going to be uneasy to bring out those experienced nurses and do the simulation and then try to undo the thing. It takes a longer process. KII 09, Male
Lack of Stroke-Specific Structured Training (Characteristics of Individuals)
Participants highlighted the lack of formal training specifically tailored to stroke care as a barrier to simulation-based education. Many nurses rely heavily on on-the-job learning or sporadic CME sessions, indicating a need for more structured educational opportunities.
I don’t remember a particular training per se except for being on the ward round and in class where you’re told about the condition of stroke. They show you a patient presenting before you and you’re told what to do. So that is from really class, the teaching, the tutorials but there was no specific training relating to that. KII 09, Male
Nurses highlighted that some initiatives which include bedside teaching, classroom tutorials, video presentations, occasional Continuing Medical Education (CME) sessions for nurses, and learning opportunities during ward rounds with other health professionals could be leveraged to share knowledge about stroke management training for nurses.
I have had training about stroke in class. Those are some good years back. However, I’ve gotten the opportunity to attend several CMEs about stroke. You know, because nurses, we have an arrangement in the hospital where nurses prepare CMEs. KII 07, Male
Available Resources and Recommendation for Implementation (Process of Implementation)
Communication through various channels (social media, print media, TV, meetings) was recommended to raise awareness about the benefits of simulation training and encourage participation among staff.
Now, community, TV, and radio. The health workers. If you can.If you can, still TV and radio; health workers, because we are not only looking at the Mbarara health workers. We are looking at other health workers out there who are managing stroke patients. So, TV, radio. If you can publish something in the papers, and journals and distribute them, the message can reach. Then for students who are still in the learning institutions, talk to them, physically. KII 07, Male
Social media. You can put those adverts on social media, on Instagram, on X, on radios, TVs. KII 012, Male
For easy planning, engagement, execution, and evaluation, it was mentioned that starting with small-scale pilot programs could be one way of gradually introducing simulation training. This allows for testing acceptability and feasibility before broader implementation.
…then the other recommendation is to start small and a little bit slow. Because by starting slow, as you say, let’s start from below the Lab for the beginning of the training. Then I’ll see later. KII 002, Male
Assuming am right, to suggest the pilot intervention simulation of three phases of care I think it is too much to bite. Is the analysis of this data going to be comparative? So let me give an example, in a simulation intervention of admission, you are going to be looking at the time, to see the time frame in which the nursing care is being given, because you want it to be timely. You want to see how the catheterization and others are being done at that phase. KII 04, Female
Some respondents advocated for combined learning methods that combines simulation with traditional teaching methods. This includes integrating simulations into existing curricula earlier on to enhance learning outcomes.
If it’s a simulation uh…one, simulations are more practical. So, they add knowledge in terms of real-time or yeah real-time experiences and patients. So, it can work better than that. However, other traditional methods can still stand like ward round discussions and teachings because these are real patients on the ward. So, I would say the simulation program can be there, just to add on, to supplement already basic problems we have. I don’t think it can replace; I don’t think it can replace the ways I’ve talked about above; me I think it can only supplement that. KII 012, Male
As compared to a lecture session because sometimes you might be in a lecture but then in the lecture room you have the lecturer who is lecturing you for you a student you’re seated somewhere, uh the longer the lecture takes the more your attention span decreases and then you don’t pick much from it […] but when you’re having a simulation session you are alert throughout the thing throughout the session…compared to when you’re having a lecture and maybe a CME. So, I think the simulation part of learning is much better compared to the others. KII, 011, Female
There was a consensus among nurses and educators on the importance of making simulations as realistic as possible. Utilizing high-fidelity mannequins and real-life scenarios can enhance the learning experience.
They should make it as real as possible. They should imitate the real world-like nature as possible… and they should follow the current guidelines of stroke management because they are outlined, by NIH, like the NIH Stroke Score, there are protocols for stroke. So, you should bring them on board during these simulation programs. KII 012, Male
There is something we saw we were in a training, for it the dummy feels like a real person. If you’re putting in a catheter, you feel as if you’re okay if you’re to put NG tube it feels like it’s a person unlike ours here the other one has a patent esophagus and everything so it’s more of a it is also simulation but for it feels like it’s a real person. KII 011, Male
Regularly scheduled simulation sessions were recommended to reinforce skills and ensure ongoing education. Participants suggested that these should be integrated into the existing training framework rather than treating them as standalone events.
I think to improve the simulation sessions is first of all providing more time to the sim sessions and conducting them over a long time while exposing these participants to the same case multiple times. Participant 3, FGD 04, Male
KII participants proposed conducting assessments after simulation training and patient outcomes such as reduction in mortality and morbidity to assess the effectiveness of the intervention in stroke management for both nurses and stroke patients.
I remember mentioning retrospective. You see how many stroke patients were admitted, how long, they stayed in the hospital, how many succumbed to pressure sores, and how many went home with contractures. So now, the time you started the simulation program, then you see those who come, how many will go home with pressure sores, contractures and how many days will they stay in the hospital. KII 03, Male
Ultimately, it’s a reduction in mortality and morbidity. Especially when you note that in a certain year, this percentage of patients were dying due to stroke-related complications. In the following scene, we now have this percentage reduction. So that’s an indicator we can use to decide to implement a national simulation-based training, for instance. So have a satellite center that shows this other issue. KII 09, Male
Many respondents emphasized the need for interprofessional training that includes not only nurses but also doctors, physiotherapists, and other healthcare professionals. This approach is seen as essential for fostering teamwork, communication of the teams, collaboration, and improving patient care.
I think there should be mix should be mixed groups where we have nurses and nursing students, physiotherapy students, ok and medical students… Not having only one group. And same should be also emphasized on the ward. Where nursing students should isolate themselves in one corner and medical students in another corner. So, it should mix up and give nursing students ok this um ok. Participant 4, FGD 2, Female
I think we are going into an interdisciplinary kind of healthcare. So, I think we are going into an interdisciplinary kind of care. So, I think having teams would be nice because we’ve already said that it is teams that take care of this patient. KII 008, Female
Engaging key stakeholders including department heads, nursing leaders, and hospital administration was identified as crucial for successful implementation. Their support can facilitate resource allocation and promote a culture of collaboration.
The head of the hospital the director, will inform the administration, because the hospital administrator will be the one signing off those things that we will need to buy and use, that is the gloves and the like. Then you come to the heads of departments, area managers because they are the heads of those people to be trained, ward in-charges. Because the cleaners are under the ward in-charges. KII 03, Male, Nurse
If the training is to be successful, right? The first thing to do is to involve these influential leaders, the director, heads of department, and the heads of the nursing team. Sell the idea to them. Tell them what exactly you want to do. And tell them the importance and the impact of what you think. That’s the first convincing, you have to make. And once they are convinced, like I told you, things can move. KII 02, Male
Discussion
In this study, we explored the barriers and facilitators simulation-based stroke training among nurses at Mbarara Regional Referral Hospital (MRRH) from healthcare providers and nurse educators. Participants articulated the complex landscape of barriers and facilitators to training nurses in stroke management using the simulation methodology at MRRH in Uganda. The results offer valuable insights into the barriers in implementing effective simulation training program and highlight potential strategies for improvement.
One of the primary barriers identified was resistance to change among experienced nurses. This resistance is often rooted in established routines and a lack of familiarity with innovative training methodologies such as SBE. Similar challenges have been documented in other countries where entrenched practices and attitudes hinder the adoption of new educational strategies.27 This resistance underscores the need for change management strategies and targeted interventions to promote openness to new learning approaches among seasoned healthcare professionals. Resource limitations also emerged as a significant challenge. Participants reported scarcity of supplies and inadequate staffing as critical barriers to conducting effective simulation sessions. Healthcare providers frequently face overwhelming patient loads28 and insufficient resources to implement new training programs effectively.29 This resonates with findings from other research indicating that healthcare environments often struggle with resource allocation for training initiatives.17,30
The disparity between the ideal training environment and the reality of clinical practice poses a significant challenge in translating learned skills into patient care. Addressing these logistical challenges is essential for creating a sustainable training program.21 Furthermore, the lack of formal stroke-specific training programs for nurses regarding stroke management was cited. Many nurses rely on on-the-job learning rather than formal training, which can lead to inconsistencies in care delivery. This finding is consistent with research indicating that structured training programs are essential for improving clinical competencies in LMICs.31
The lack of standardized, stroke-specific education for nurses highlights a critical area for improvement in the Ugandan healthcare system. Participants strongly supported simulation-based education (SBE) as an effective method for enhancing nursing skills in stroke management. The consensus among healthcare professionals and nursing students was that simulation training bridges the gap between theoretical knowledge and practical application, fostering confidence and competence in real-world scenarios. This aligns with previous research that highlights SBE as a transformative approach to nursing education, promoting critical thinking and teamwork.13,32–34
This enthusiasm for SBE suggests that, if implemented effectively, it could be a powerful tool for enhancing stroke care competencies among nurses at MRRH. Moreover, leveraging existing training opportunities within the hospital, such as bedside teaching and Continuing Medical Education (CME) sessions, can provide a foundation for integrating stroke-specific education into nursing curricula. This approach not only utilizes available resources but also addresses the educational gaps identified in nursing practices related to stroke care. By building upon familiar educational structures, the integration of new training methodologies may face less resistance and achieve greater acceptance among staff. Engaging key stakeholders such as hospital director, department heads, and nursing leaders was also highlighted as crucial for resource allocation and fostering a collaborative culture within the hospital.
This finding underscores the importance of a systems-based approach to implementing educational interventions, where support from leadership can facilitate the necessary organizational changes to accommodate new training programs.16,24 The proposal to incorporate stroke management and simulation training into academic curricula reflects a proactive approach to ensuring sustainability in nursing education. By embedding these competencies early in training programs, future nurses will be better equipped to manage stroke patients effectively from the outset of their careers.13 This finding, however, contradicts a letter from Turkey about integrating medical simulation into the Turkish undergraduate curriculum where overcrowded curricula and limited resources posed challenges to implementing simulation programs effectively.30 The authors argued that without adequate funding and support, the integration of essential simulation training becomes unrealistic, demonstrating a need for a well-organized process and collaboration of both academic staff and administration to make it work. Also, the authors highlight that their program was able to receive more funding from the university, this might not be possible in Uganda a low resource setting. This difference shows how important it is to align resources and get stakeholders on board. Without these things, even highly valued interventions like SBE may fail.
A notable finding from this study was the strong advocacy for an interdisciplinary approach to stroke care training. Participants emphasized the importance of including not only nurses but also physicians, physiotherapists, and other healthcare professionals in simulation-based training. This aligns with current best practices in stroke care, which emphasize a team-based approach to patient management.7 Implementing multidisciplinary training could foster better collaboration and communication skills among healthcare provider teams, which can be translated into improved bedside performance,35 ultimately leading to improved patient outcomes.
The emphasis on making simulations as realistic as possible, utilizing high-fidelity mannequins and real-life scenarios, aligns with best practices in simulation-based education.14 This focus on realism enhances learning and potentially easing the transition of skills from simulated environments to actual patient care.36 Regular simulation sessions can help maintain competencies and ensure that stroke care knowledge remains current among nursing staff. This approach is supported by literature demonstrating the positive impact of repeated simulation exposure on clinical skills and confidence.18,20
These findings pave way for the development of the Uganda’s national stroke training policy and other chronic disease simulation standards in settings like Uganda.
Study Strength and Limitations
Our study had several strengths. The participants provided rich and varied descriptions of their contextual experiences, facilitators, and proposed solution to the barriers. The researchers were involved data collection. We used the CFIR model to optimize study design, data collection, and analysis.24
Our study also had limitations. The qualitative nature of the research, while offering rich, contextual data, may limit generalizability to other settings. However, the Focus group discussion moderator was proficient and unbiased to allow the participants to share their views freely. The participants in the FGD were also from the same class and familiar to each other to allow for free sharing.
Conclusions
The study contributes to the greater understanding of the barriers and facilitators for implementing the simulation-based education for nursing stroke care at a large hospital in Uganda. Curriculum integration, multidisciplinary training, and educator/facilitator preparations will facilitate the implementation of SBE for stroke nursing. However, for successful implementation there will be need to address resource limitations, address resistance to change, and fostering a culture of continuous learning and improvement within healthcare institutions. Resource scarcity is a persistent challenge in LMIC healthcare systems, which could limit the scalability and sustainability of simulation-based programs. Addressing the barriers while leveraging existing facilitators will be essential in implementing a simulation-based intervention for nurses. The insights gained from this study contribute to a growing body of literature advocating for improved nursing education in LMICs, ultimately aiming to reduce the burden of stroke-related morbidity and mortality. The study focused primarily on the perspectives of healthcare providers, nursing students, and educators. This study lays the groundwork for pilot interventions and informs national and institutional training strategies. Future studies could include the voices of patients and their families to gain a more comprehensive understanding of the impact of nurse training on stroke care quality. Longitudinal studies tracking the implementation and outcomes of simulation-based training programs for stroke care would provide valuable data on the long-term efficacy of these interventions.
Abbreviations
CME, Continuous Medical Education; CFIR, Consolidated Framework for Implementation Research; FGD, Focus Group Discussion; LMICS, Low-Middle Income settings; MRRH, Mbarara Regional Referral Hospital; MUST, Mbarara University of Science and Technology; SBE, Simulation-Based Education; SSA, Sub Saharan Africa; UNCST, Uganda National Council for Science and Technology.
Data Sharing Statement
The authors confirm that the data supporting the results of this study are available with the article. Raw data that supports the findings of this study are available on request from the corresponding author.
Acknowledgments
We would like to acknowledge the participants who agreed to participate in this study. We acknowledge Ms. Tebulwa B. Joanita and Ms. Sarah Mwijukye for their contribution towards the data collection of this work.
Funding
This study did not receive direct funding.
Disclosure
The authors declare no conflict of interest in this work.
References
1. Okekunle AP, Jones S, Adeniji O, et al. Stroke in Africa: a systematic review and meta-analysis of the incidence and case-fatality rates. Int J Stroke. 2023;18(6):634–644. doi:10.1177/17474930221147164
2. Feigin VL, Nichols E, Alam T, et al. Global, regional, and national burden of neurological disorders, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(5):459–480. doi:10.1016/S1474-4422(18)30499-X
3. Mbonde AA, Chang J, Musubire A, et al. An analysis of stroke risk factors by HIV serostatus in Uganda: implications for stroke prevention in sub-Saharan Africa. J Stroke Cerebrovasc Dis. 2022;31(7):106449. doi:10.1016/j.jstrokecerebrovasdis.2022.106449
4. Kaddumukasa M, Najjuma J, Mbalinda SN, et al. Reducing stroke burden through a targeted self-management intervention for reducing stroke risk factors in high-risk Ugandans: a protocol for a randomized controlled trial. PLoS One. 2021;16(6):e0251662. doi:10.1371/journal.pone.0251662
5. Olum S, Muyingo A, Wilson TL, et al. Stroke mortality outcomes in Uganda. J Stroke Cerebrovasc Dis. 2021;30(5):105661. doi:10.1016/j.jstrokecerebrovasdis.2021.105661
6. Kassaw Asres A, Cherie A, Bedada T, Gebrekidan H. Frequency, nursing managements and stroke patients’ outcomes among patients admitted to Tikur Anbessa specialized hospital, Addis Ababa, Ethiopia a retrospective, institution based cross-sectional study. Intl J Africa Nurs Sci. 2020;13:100228. doi:10.1016/j.ijans.2020.100228
7. Summers D, Leonard A, Wentworth D, et al. Comprehensive overview of nursing and interdisciplinary care of the acute ischemic stroke patient: a scientific statement from the American Heart Association. Stroke. 2009;40(8):2911–2944. doi:10.1161/STROKEAHA.109.192362
8. Camicia M, Lutz B, Summers D, Klassman L, Vaughn S. Nursing’s role in successful stroke care transitions across the continuum: from acute care into the community. Stroke. 2021;52(12):e794–e805. doi:10.1161/STROKEAHA.121.033938
9. Bvumbwe T, Mtshali N. Nursing education challenges and solutions in Sub Saharan Africa: an integrative review. BMC Nurs. 2018;17(1):3. doi:10.1186/s12912-018-0272-4
10. Jarva E, Mikkonen K, Tuomikoski AM, et al. Healthcare professionals’ competence in stroke care pathways: a mixed‐methods systematic review. J Clin Nurs. 2021;30(9–10):1206–1235. doi:10.1111/jocn.15612
11. Owolabi MO, Thrift AG, Martins S, et al. The state of stroke services across the globe: report of World Stroke Organization–World Health Organization surveys. Int J Stroke. 2021;16(8):889–901. doi:10.1177/17474930211019568
12. Jones SP, Miller C, Gibson JM, Cook J, Price C, Watkins CL. The impact of education and training interventions for nurses and other health care staff involved in the delivery of stroke care: an integrative review. Nurse Education Today. 2018;61:249–257. doi:10.1016/j.nedt.2017.11.024
13. Cant RP, Cooper SJ. Simulation-based learning in nurse education: systematic review. J Adv Nurs. 2010;66(1):3–15. doi:10.1111/j.1365-2648.2009.05240.x
14. Demiray A, Ilaslan N. Standardized patient simulation usage in nursing education and evaluation of outcomes by Kirkpatrick Model. Sch J Appl Sci Res. 2019;2:10–18.
15. Kapucu S, Bulut H. Turkish nursing students’ views of their clinical learning environment: a focus group study. Pak J Med Sci. 2011;27(5):1149–1153.
16. Najjuma JN, Bajunirwe F, Twine M, et al. Stakeholder perceptions about the establishment of medical simulation-based learning at a university in a low resource setting: a qualitative study in Uganda. BMC Med Educ. 2020;20(1):379. doi:10.1186/s12909-020-02301-3
17. Data S, Dubé MM, Bajunirwe F, et al. Feasibility of an interprofessional, simulation-based curriculum to improve teamwork skills, clinical skills, and knowledge of undergraduate medical and nursing students in Uganda: a cohort study. Simulation Healthcare. 2020.
18. Cant RP, Cooper SJ, Lam LL. Hospital nurses’ simulation-based education regarding patient safety: a scoping review. Clin Simul Nurs. 2020;44:19–34. doi:10.1016/j.ecns.2019.11.006
19. Mehta T, Strauss S, Beland D, Fortunato G, Staff I, Lee N. Stroke simulation improves acute stroke management: a systems-based practice experience. J Grad Med Educ. 2018;10(1):57–62. doi:10.4300/JGME-D-17-00167.1
20. Roots A, Thomas L, Jaye P, Birns J. Simulation training for hyperacute stroke unit nurses. Br J Nurs. 2011;20(21):1352–1356. doi:10.12968/bjon.2011.20.21.1352
21. Muhumuza A, Najjuma JN, MacIntosh H, et al. Understanding the barriers and enablers for postgraduate medical trainees becoming simulation educators: a qualitative study. BMC Med Educ. 2023;23(1):28. doi:10.1186/s12909-022-03995-3
22. Breimaier HE, Heckemann B, Halfens RJG, Lohrmann C. The consolidated framework for implementation research (CFIR): a useful theoretical framework for guiding and evaluating a guideline implementation process in a hospital-based nursing practice. BMC Nurs. 2015;14(1):43. doi:10.1186/s12912-015-0088-4
23. Safaeinili N, Brown‐Johnson C, Shaw JG, Mahoney M, Winget M. CFIR simplified: pragmatic application of and adaptations to the Consolidated Framework for Implementation Research (CFIR) for evaluation of a patient‐centered care transformation within a learning health system. Learn Health Syst. 2020;4(1):e10201. doi:10.1002/lrh2.10201
24. Means AR, Kemp CG, Gwayi-Chore M-C, et al. Evaluating and optimizing the consolidated framework for implementation research (CFIR) for use in low- and middle-income countries: a systematic review. Implement Sci. 2020;15(1):17. doi:10.1186/s13012-020-0977-0
25. Braun V, Clarke V. To saturate or not to saturate? Questioning data saturation as a useful concept for thematic analysis and sample-size rationales. Qual Res Sport Exerc Health. 2019;1–16.
26. Lincoln YS, Guba EG. But is it rigorous? Trustworthiness and authenticity in naturalistic evaluation. New Directions Program Eval. 1986;1986(30):73–84. doi:10.1002/ev.1427
27. Ehilawa PI, Woodier N, Dinning A, et al. Using simulation-based interprofessional education to change attitudes towards collaboration among higher specialty trainee physicians and registered nurses: a mixed methods pilot study. J Interprof Care. 2023;37(4):595–604. doi:10.1080/13561820.2022.2137481
28. Adam A, Sunny CO, Isabel K, et al. The health workforce status in the WHO African Region: findings of a cross-sectional study. BMJ Global Health. 2022;7(Suppl 1):e008317. doi:10.1136/bmjgh-2021-008317
29. Aldosari AM, Alsalman AA, Albathali GM, et al. The impact of nurse-to-patient ratios on patient outcomes. J Namibian Studies. 2022;31:453–463.
30. Kitapçıoğlu D, Aksoy ME. Integrating medical simulation programs into the Turkish undergraduate medical curriculum. Adv Med Educ Pract. 2016;7:29–30. doi:10.2147/amep.S99596
31. Virani SS, Alonso A, Benjamin EJ, et al. Heart disease and stroke statistics—2020 update: a report from the American Heart Association. Circulation. 2020;141(9):e139–e596. doi:10.1161/CIR.0000000000000757
32. Lim CY, Song MR. Sustained effect of simulation-based resuscitation education on knowledge, self-confidence, and performance ability of neonatal intensive care unit nurses. J Continuing Educ Nurs. 2024;55(2):79–86. doi:10.3928/00220124-20231109-05
33. Ho MH, Yu LF, Lin PH, et al. Effects of a simulation-based education programme on delirium care for critical care nurses: a randomized controlled trial. J Adv Nurs. 2021;77(8):3483–3493. doi:10.1111/jan.14938
34. Tong K, McMahon E, Reid-McDermott B, Byrne D, Doherty AM. SafePsych: improving patient safety by delivering high-impact simulation training on rare and complex scenarios in psychiatry. BMJ Open Qual. 2021;10(3):e001533. doi:10.1136/bmjoq-2021-001533
35. Colman N, Figueroa J, McCracken C, Hebbar KB. Can simulation based-team training impact bedside teamwork in a pediatric intensive care unit? J Pediatr Intensive Care. 2019;8(4):195–203. doi:10.1055/s-0039-1688928
36. Kim TE, Reibling ET, Denmark KT. Student perception of high fidelity medical simulation for an international trauma life support course. Prehospital Disaster Med. 2012;27(1):27–30. doi:10.1017/s1049023x11006790
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.