")
Back to Journals » Patient Preference and Adherence » Volume 17
Barriers and Facilitators of Adherence to Oral Anticancer Medications Among Women with Breast Cancer: A Qualitative Study
Authors Onwusah DO , Ojewole EB , Manyangadze T, Chimbari MJ
Received 12 April 2023
Accepted for publication 29 August 2023
Published 6 November 2023 Volume 2023:17 Pages 2821—2839
DOI https://doi.org/10.2147/PPA.S416843
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Deborah Obehi Onwusah,1 Elizabeth Bolanle Ojewole,1 Tawanda Manyangadze,2,3 Moses John Chimbari2,4
1Discipline of Pharmaceutical Sciences, School of Health Sciences, College of Health Sciences, University of KwaZulu-Natal, Durban, KwaZulu-Natal, South Africa; 2Discipline of Public Health Medicine, School of Nursing and Public Health, College of Health Sciences, University of KwaZulu-Natal, Durban, KwaZulu-Natal, South Africa; 3Geosciences, School of Geosciences, Disasters and Sustainable Development, Faculty of Science and Engineering, Bindura University of Science Education, Bindura, Mashonaland Central, Zimbabwe; 4Department of Public Health, School of Medical and Health Sciences, Great Zimbabwe University, Masvingo, Zimbabwe
Correspondence: Deborah Obehi Onwusah, Discipline of Pharmaceutical Sciences, School of Health Sciences, College of Health Sciences, University of KwaZulu-Natal, Private Bag X54001, Durban, KwaZulu-Natal, 4000, South Africa, Email [email protected]
Purpose: Despite the life-saving benefits of oral anticancer medications (OAMs) to women with breast cancer (BC), adherence remains suboptimal and, in many cases, not well documented. The study examined barriers and facilitators of adherence to OAMs among women receiving BC treatment in Nigeria.
Patients and Methods: The study was framed within the World Health Organization (WHO) Multidimensional Model of Adherence. We conducted qualitative in-depth interviews of 16 purposively sampled women in two tertiary hospitals in Southern Nigeria. The interviews were audio-recorded and transcribed verbatim. The interview data were analyzed using the Framework Method.
Results: The key barriers to OAM adherence mentioned were socioeconomic factors (high cost of medication) and therapy-related factors (medication side effects). The key facilitating mechanisms for adherence to OAMs mentioned included; (i) patient-related psychosocial factors such as self-encouragement and self-discipline in sticking to the prescription, taking the medication at a particular time each day, receiving practical support from family members; and (ii) healthcare team/system factors such as obtaining an adequate supply of the medication at the pharmacy.
Conclusion: Barriers and facilitators to OAM adherence are multidimensional. The study findings highlight the potential benefit of a multifaceted intervention (such as patient education and monitoring or strategies promoting cost-containment and side effects management) to optimize adherence. Therefore, our findings may inform the designing and evaluating of context-specific adherence measures and multifaceted intervention strategies targeting key barriers and approaches that enable adherence to enhance patient outcomes.
Keywords: medication adherence, oral antineoplastic agents, breast cancer, women’s experiences
Introduction
Breast cancer (BC) is the most common cancer and a significant health burden in women worldwide, including Nigeria. BC incidence and survival vary in different regions, with higher incidences for developed countries in Europe and Northern America than in Africa. The global 2020 reports for the estimates of cancer incidence and mortality worldwide showed that in Belgium and the USA, the reported age-standardized incidence rates (ASR) were 113.2 and 90.3 per 100,000, respectively. In Africa, Nigeria (ASR: 49.0 per 100,000) ranked second to Mauritius (ASR: 66.2 per 100,000). However, mortality is relatively low in developed countries compared to Africa. The age-standardized mortality rates reported for Belgium and the USA were 15.1 and 12.4 per 100,000, respectively. In Africa, Nigeria ranked highest with an age-standardized mortality rate of 25.5 per 100,000, compared to 20.0 per 100,000 for Mauritius, indicating lower survival from BC in Nigeria.1,2
The common modalities for breast cancer treatment include surgery, chemotherapy and radiotherapy.3 Traditional chemotherapy has mainly been administered intravenously when the patient presents to an outpatient infusion centre or inpatient hospital setting to receive their infusions.4 In recent years, oral anticancer medications (OAMs) comprising the traditional endocrine, cytotoxic, and targeted therapies have been used as primary treatment for many cancers, including breast cancer.5 About 70–80% of breast cancers are hormone receptor-positive (HR+) as they express estrogen (ER) and progesterone (PR) receptors. Oral endocrine therapy (OET), also called hormonal therapy, is standard adjuvant therapy for HR+ BC. OET include selective estrogen receptor modulators (SERMs, eg, tamoxifen) or aromatase inhibitors (AIs) (eg, anastrozole, letrozole and exemestane). OET is prescribed to prevent recurrence and mortality and is recommended for a standard duration of 5 years and sometimes for a longer duration. Despite proven benefits, non-adherence and early therapy discontinuation before the recommended five years are common.6–8 The human epidermal growth factor receptor 2 (HER2/neu) gene plays a role in BC development. BC with HER2 protein overexpression (gene amplification) is called HER2-positive BC. BC without HER2 protein overexpression is called HER2-negative BC. HER2-positive BC tends to grow faster and is more likely to spread and recur than HER2-negative BC. Targeted therapies are used to treat HER2-positive BC (eg, trastuzumab, pertuzumab, lapatinib). Trastuzumab is the standard treatment for high-risk early-stage HER2-positive BC.9,10 The oral nonendocrine therapies include cytotoxic therapies (eg, capecitabine, cyclophosphamide) and targeted therapies (eg, lapatinib, trastuzumab).5,11
Medication adherence which describes medication-taking behavior, is defined as “taking medication as prescribed regarding the daily amount, dosage, and frequency”, and persistence refers to “the duration of time from initiation to discontinuation of therapy”.12 The clinical efficacy of OAMs in improving treatment outcomes and survival and the associated reduction in patients’ care burden attributed to ease of administration make many patients prefer oral to intravenous medication administration.5,13 To optimize treatment with OAMs, full (100%) adherence is necessary to maintain therapeutic doses and ensure greater treatment efficacy.14 While adherence to OAMs reduces the risk of early disease relapse and death, non-adherence is related to poorer health outcomes, low quality of life, and higher healthcare utilization and costs.15–17
Notwithstanding this, adherence to recommended OAM regimens is sub-optimal and has been reported to vary widely. A systematic review showed that the mean adherence rate for endocrine therapy at five years was 66.2% (SD = 17.3%) at the implementation phase, and the mean persistence was 66.8% (SD = 14.5%). By the fifth year, adherence declined by an average of 25.5% (SD = 9.3%).8 Another systematic review reported that for tamoxifen and AIs, adherence rates varied from 41% to 72%.18 Adherence rates of oral nonendocrine medications such as capecitabine ranged from 10% to 100%.19–22
In Africa, including Nigeria, achieving optimal adherence to OAMs remains a problem in treating women with breast cancer, as suboptimal adherence to OAMs is common. A recent scoping review of primary quantitative studies on adherence to OAMs in women with BC reported variable rates of non-adherence ranging from 4.3% to 65.4% for endocrine therapy, 80.9% for cytotoxic chemotherapy including capecitabine, cyclophosphamide, and prednisolone, and 32.7% for combined therapies.23 The review showed that in routine clinical settings in Nigeria, the reported non-adherence rate for tamoxifen was 24.5% at one year of treatment. The overall non-adherence rate was 80.9% for chemotherapy, including cyclophosphamide, capecitabine and prednisolone.23 Despite the variable rates of non-adherence to OAMs among breast cancer patients, limited information is available regarding the factors influencing adherence to OAMs in Nigeria.
Medication adherence is a complex and dynamic behavior influenced by multiple interacting factors.24 Hence, adherence to OAMs may vary with time for women with breast cancer due to many factors influencing medication-taking behavior. A systematic review of qualitative studies of breast cancer patients’ experiences of adherence and persistence to oral endocrine therapy showed that factors that promoted medication adherence included women feeling they had no option and fear of cancer recurrence. Persistence was facilitated by support and information. Severe side effects, insufficient information and lack of support contributed to non-adherence and non-persistence.25 Most of the reviewed qualitative studies explored patients’ experiences concerning oral endocrine therapy in developed countries, including the USA. None of the reviewed qualitative studies was conducted in Africa, including Nigeria.
The review of primary quantitative studies from Africa23 reported several barriers and facilitators associated with OAM adherence. Barriers that were significantly associated with OAM adherence include Islamic religion, concurrent comorbidities, mastectomy, anastrozole treatment, side effects, limited awareness of insurance coverage, and seeking treatment from traditional healers. Facilitators significantly associated with OAM adherence include thorough therapeutic communication regarding treatment, neoadjuvant chemotherapy, and adequate social support. However, the barriers and facilitators associated with OAM adherence were reported in a few quantifiable studies and were inconsistent across studies.
The review23 revealed that few observational studies from Nigeria26–28 assessed factors influencing adherence to OAMs among women with BC. Financial difficulties, medication costs, younger age, and feeling well after starting chemotherapy contributed to poor adherence to OAMs.27 Patients having a job, living in an urban area, having received a mastectomy, receiving cosmesis, and not having evidence of disease at the last clinic visit promoted patient compliance to treatment and medication.28 However, the evidence is inconsistent, and the reasons for these observations are unclear. To date, qualitative studies assessing factors influencing adherence to OAMs in women with breast cancer in the Nigerian setting are scarce. Qualitative studies provide more in-depth insights into women’s experiences on adherence to OAM regimens than can be achieved with quantitative studies. This study used qualitative methods to examine barriers and facilitators influencing adherence to prescribed oral anticancer medications among women diagnosed with stage I–III breast cancer.
Materials and Methods
Study Design and Setting
This qualitative study applied a qualitative description design.29,30 This approach was selected as we sought to provide straightforward, focused, and detailed descriptions of participants’ experiences of barriers and facilitators influencing OAM adherence.30 The study used semi-structured, face-to-face interviews31 with women with breast cancer prescribed OAMs. We adopted the Framework Method,32,33 and the World Health Organization (WHO) Multidimensional Adherence Model informed the analysis framework.24,34 The study was conducted at the outpatient oncology and surgical clinics of two tertiary hospitals in southern Nigeria between August 2019 and September 2019.
Ethics and Informed Consent
The study was approved by the ethics committee at the University of KwaZulu-Natal, South Africa (reference number BFC021/19), the National Health Research Ethics Committee of Nigeria, and health research ethics committees in each participating hospital. We conducted the study in accordance with the Nigerian National Code for Health Research Ethics and the Declaration of Helsinki. All participants provided written informed consent before the study commencement. The participants written informed consent included the publication of anonymized responses.
Participant Selection
We recruited participants based on the criterion of data saturation. Other similar studies have recommended a minimum sample size of between 12 and 13 participants.35,36 In our case, saturation was achieved on the 16th participant. Purposive sampling was applied to recruit eligible participants who were identified from the patient’s medical records based on the following inclusion criteria: aged 18 years and above, who were pre- or postmenopausal, had stage I, II, or III invasive BC at diagnosis based on the American Joint Committee on Cancer breast cancer staging system,37 had been prescribed and were currently taking OAMs (endocrine or nonendocrine) for at least one month at the time of study commencement, and could understand and speak English or the local language of communication. Eligible participants were grouped into two purposive sampling categories, defined by their prescribed OAM type (endocrine and nonendocrine medications), assessed from patient medical records. Participants were then sampled within these categories. Those selected were invited through telephone calls and face-to-face meetings by members of the cancer care team (surgeon, oncologist, or nurse) to participate in the study. Women who indicated they were interested in receiving more information about the study were contacted by the researcher (DOO), who explained the interview process and asked the women if they were currently taking their prescribed OAM. Interviews with women who were willing to participate in the study were scheduled at agreed dates and times. As interviews continued, recruitment was directed at the unfilled OAM category. We also made an attempt to ensure that the sample was diverse in age and socioeconomic background.38,39 Relevant demographic and clinical information of each patient was recorded using a pretested data collection form.
Data Collection Procedure
We conducted face-to-face, in-depth interviews using a semi-structured interview schedule with predetermined open-ended questions developed based on previously published qualitative research,40 and the study’s objectives (Supplementary File 1). The interview questions were based on the WHO Multidimensional Adherence Model.24,34 The model was developed to provide a comprehensive assessment of factors influencing adherence to inform intervention design. The model is based on the principle that adherence is a multidimensional phenomenon determined by the interplay of five sets of factors or dimensions, encompassing the demographic and socioeconomic, disease, health care team/system, therapies/medication, and patient-and-close relatives-related factors.24,34 The interview schedule contained two sections: section A gathered relevant socio-demographic and clinical information. Section B included open-ended questions that examined women’s experiences of taking OAMs (endocrine and nonendocrine), as well as barriers and facilitators to OAM adherence. The interview schedule was not piloted. It was cross-checked by and discussed with the clinical oncologist of the study sites before and during the study. The first author (DOO, a female clinical pharmacist), a novice researcher in qualitative research, had received training before the study commenced and conducted this qualitative study as a requirement of a PhD in Pharmacy. Before each interview, the researcher (DOO) introduced herself and obtained written informed consent from the participant; and a relationship with the participant was established through informal talk. The researcher conducted individual interviews with patients in a private room within the hospital to ensure confidentiality. According to the participant’s preference, most of the interviews were conducted in English, one in Nigerian Pidgin English and another in the local Yoruba language. A bilingual translator – a staff of the health facility and a native Yoruba speaker translated into Yoruba for the participant who preferred the local language. Probing questions were asked to prompt further information and explore the answers in-depth, and the interviews were audio-recorded with the participant’s permission. Interviews were transcribed verbatim and anonymized. Transcripts were not returned to participants for comment or correction. The duration of the interviews was between 21 and 58 minutes (mean length of interview 36.14 minutes, standard deviation 11.45 minutes). Field notes were taken, examined and added to the text before analysis. We recruited participants until saturation was achieved in each OAM category, where further interviews did not offer any new or pertinent information. The participants’ oncologists (and other staff at the clinic) were not provided with information on patient participation to remove possible bias.
Data Analysis
We used NVivo version 12 (QSR International, Burlington, MA, USA) to analyze data.41 Thematic analysis was performed based on the Framework approach, and the WHO Adherence Model informed the analysis framework.32,33 We developed the framework through an iterative process that incorporated the study aim, the WHO Adherence Model and detailed reading of interview transcripts. The Framework approach allowed the inclusion of both apriori (WHO Adherence Model) factors and emergent codes. Consistent with the Framework approach, an overview of the entire data set was initially obtained. The initial familiarization step was done during the interview process. As part of the familiarization process, the researchers read through each transcript before coding to ensure the main themes were not missed. After familiarization, two investigators (DOO, THA) individually coded two interviews, then compared and discussed results to develop a coding index which was then applied to the rest of the interviews. Differences in coding were resolved by discussion. The inter-coder reliability coefficient (Cohen’s Kappa) was 0.93. The coding index was developed by identifying recurrent themes introduced into the interviews through the interview schedule. The coding index was used to construct thematic matrices or charts according to key constructs and dimensions from the WHO Adherence Model in the software package NVivo version 12. Each dimension and its associated constructs were plotted on a separate thematic chart.32,38,42 Tables highlighting key thematic content, barriers and facilitators within each dimension of the WHO Adherence Model were produced. The broader research team members (EO, TM, MJC) reviewed the allocation of the codes to the WHO Adherence Model constructs and dimensions. The entire research team (DOO, EO, TM, MJC) held detailed discussions to resolve discrepancies in the allocation of codes until a consensus was reached. The dimensions were perceived to either facilitate or present barriers to OAM adherence. The most influential dimensions for OAM adherence were identified based on the following criteria (i) when participants expressed firm views or beliefs within the dimension, which was discussed at great length or extensively (ii) when participants frequently expressed views or beliefs within the dimension (iii) when participants expressed conflicting or opposing views within the dimension.38 Member checks were performed with the participants who reviewed the preliminary results of their interview for accurate reflection of the researchers’ account of their experience.43,44 We have provided illustrative quotes to supplement narrative descriptions. The study applied the Consolidated Criteria for Reporting of Qualitative Research (COREQ) checklist.45
Results
Participant Characteristics
A total of 20 women with BC were approached to participate in the study. Of this, only 16 women were included and interviewed. Reasons for non-participation included time factor (n =1), no interest (n=1), and data collection having reached saturation (n = 2). The participants were between 34 and 68 years of age (mean 47.6 years, standard deviation 8.8). The mean duration of BC was 2.7 years (range 4 months to 10 years), while the mean duration for OAM use was 0.97 years (range 1 month to 6 years). Ten participants received oral endocrine medications, and six received oral nonendocrine medications. Most of the patients had stage II BC (43.75%), had hormone receptor-positive/HER2-negative (ER+/PR+/HER2-) BC (56.25%), were offered other treatment modalities, including surgery, adjuvant chemotherapy and radiation therapy (81.25%) in addition to the OAM. About 50.0% had at least one comorbid illness, and 43.75% received a prescription for at least one medication for their comorbid condition (Table 1). The results presented reflect the diverse sample and how the barriers and facilitators differ by stage of BC (I, II and III).
 |
Table 1 Participants’ Socio-Demographic and Clinical Characteristics (n = 16) |
Barriers to Adherence to OAMs
We aligned the identified barriers to OAM adherence to the five WHO adherence model’s recommended dimensions: demographic and socioeconomic, patient and close relatives, therapy/medication, disease, and healthcare team/system barriers (Table 2).
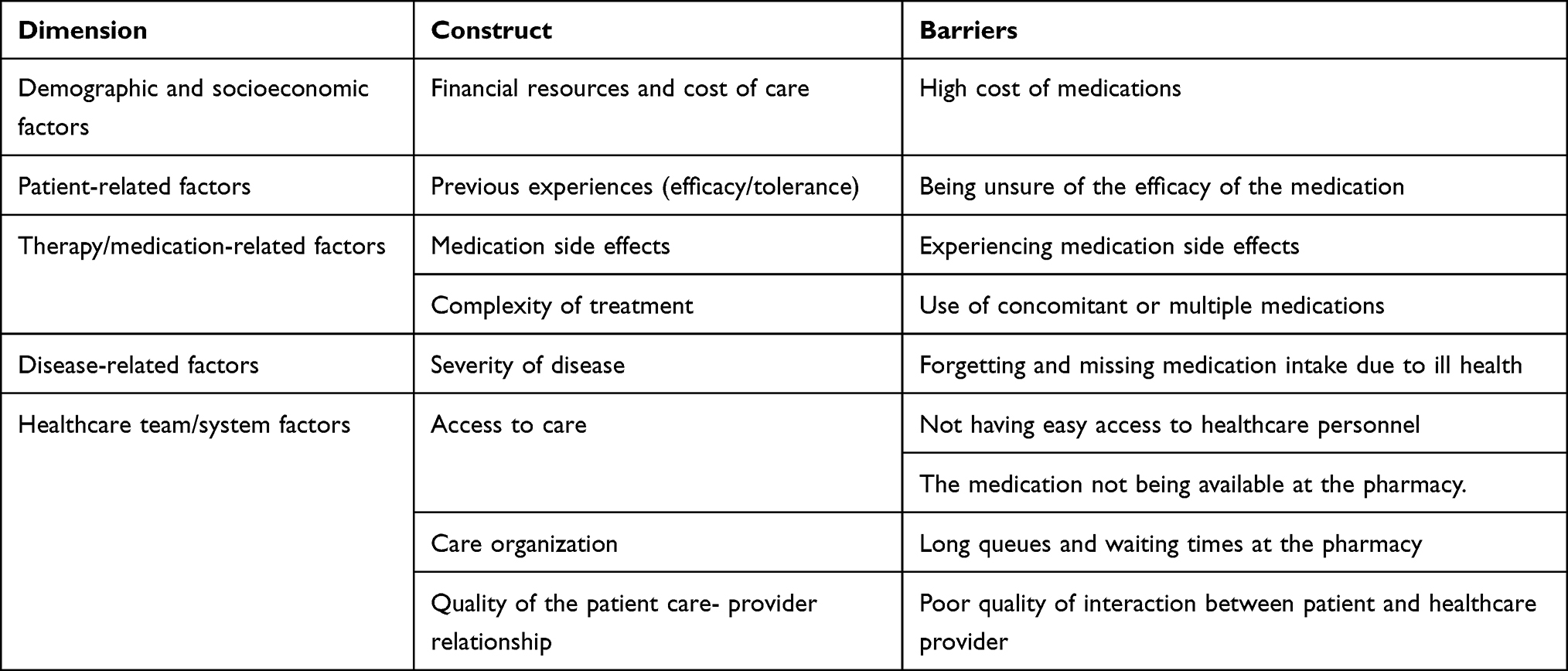 |
Table 2 Barriers to Oral Anticancer Medication Adherence |
Demographic and Socioeconomic Barriers
The high cost of medication was a central theme in the socioeconomic dimension. Treatment cost was a frequently mentioned barrier, with patients expressing concern about the high cost of prescribed OAM, as stated below.
… I have to wait for money … It takes 3 or 4 days. I will not be taking it [medication]… because of the money. The cost of the medicine is very high. (P8, Tamoxifen, Stage II)
… There are a lot of us who are having difficulties when it comes to finance … Cancer drugs are too expensive, and a lot of people who do not even have jobs, how do we afford this kind of expensive treatment? … And the money is not forthcoming, I don’t have it … my most difficult challenge is getting the drug … in affording the drug, buying the drug, that is my primary problem. (P9, Tamoxifen, Stage II)
Patient and Close Relatives-Related Barriers
Patient-related barriers were mentioned by some patients and consisted of one central theme, namely, being unsure of the medication efficacy, as stated below.
Well, I thought it was working, but when I started having that recurrence, I asked myself the benefit of [the medication]. That was when I started to doubt the efficacy… I can’t say for sure, but I feel maybe it’s of some lower quality. (P5, Tamoxifen, Stage I)
Therapy/Medication-Related Barriers
Medication-related barriers consisted of two themes that patients mentioned: experiencing medication side effects and using concomitant or multiple medications.
Some patients reported that they had experienced substantial side effects while taking OAMs. The most common side effects reported were hot flashes, fatigue and dizziness.
Oh, the major one is … I’m always sweating… Since I started taking it, even right now, I’m sweating … The sweating alone is enough side effect to stop me from taking it, but what can I do? The sweating alone is just enough side effect… because at times when I want to go out, I look at my dresses, and I will be like, ‘Oh, with this tamoxifen that is making me sweat a lot, I can’t go out with this dress’ even my dress code has changed… (P10, Tamoxifen, Stage I)
It’s like my eyes [are] turning me… that dizziness… I was asking if I will be taking two [tablets] instead of three … since [the medication makes me dizzy]. I feel weak. (P14, Capecitabine, Stage III)
… The difficulty is the side effect, and I noticed that when I take three tablets, it makes me very uncomfortable I feel dizzy. (P16, Capecitabine, Stage II)
Other therapy/medication-related barriers mentioned by patients included treatment complexity, such as the use of concomitant medications (that further intensified the experience of side effects); or the use of multiple medications, which contributed to patients skipping or missing medication doses due to the tiring routine of frequent medication intake and concerns about taking many medications as stated by some patients.
Use of concomitant or multiple medications
… I take [oral capecitabine] after my chemo [intravenous chemotherapy] … you know chemo [intravenous chemotherapy] itself is the type of drug that weakens someone. Yes, the weakness, the intravenous, so anytime I take [oral capecitabine] within that period, it … [made] me weaker. I take it in addition to chemo [intravenous chemotherapy], so it gives me fatigue. (P1, Capecitabine, Stage III)
Several days. It’s like there was a time I was sick, … about either 3 or 4 days. At times I might feel that these … drugs [are] too much; let me finish this one first. (P5, Tamoxifen, Stage I)
Disease/Illness-Related Barriers
The illness-related barrier identified included patients forgetting and missing medication intake due to ill health, as stated below.
But there was once I did not take it just one day, I did not take it … I was sick, I was very down with pains, I was really weak, so I slept. I slept off only to wake up in the middle of the night; early morning the next day, I realized I did not take it. (P9, Tamoxifen, Stage II)
Healthcare Team/System-Related Barriers
The identified healthcare team/system barriers included four main themes: (i) ease of access to healthcare personnel, (ii) medication unavailability at the pharmacy, (iii) quality of the interaction between patient and healthcare provider, and (iv) long queues and waiting times at the pharmacy. The following are statements from some participants about each theme.
Going back to that … pharmacy [in the hospital] is far, and sometimes when I go there, the man [who] is supposed to attend to me is not around… (P1, Capecitabine, Stage III)
…What can I say, besides at times when you call them, they don’t take your calls. (P10, Tamoxifen, Stage I)
… Sometimes when I go there [pharmacy] … the drug is not available … (P1, Capecitabine, Stage III)
At times, I have to look for it [medication] before I can get it to buy; it is scarce at times. (P2, Tamoxifen, Stage I)
I went back. they told me to pick other brands. I said no. So, I referred back to my doctor. So, my doctor said that one [medication brand] was scarce. (P5, Tamoxifen, Stage I)
… I called the nurses, I told them about it, I called my doctor… He did not pick his calls. So I called the other younger doctors, one of them said, okay, he will get back to me; I waited for days, he did not get back to me; I called he was not picking his calls. But I called severally he did not pick; I sent text messages, he did not respond. (P9, Tamoxifen, Stage II)
I went to [a private pharmacy] to get my [medication] … I was already tired after work, so when I got there, I had to line up to give them my prescription and pay. Then they gave me the receipts, which I took to the counter again to collect a number, after which I had to wait for the drugs. (P1, Capecitabine, Stage III)
Facilitators of Adherence to OAMs
We categorized the identified facilitators of OAM adherence to three WHO adherence model recommended dimensions: patient and close relatives, disease, and healthcare team/system-related factors (Table 3).
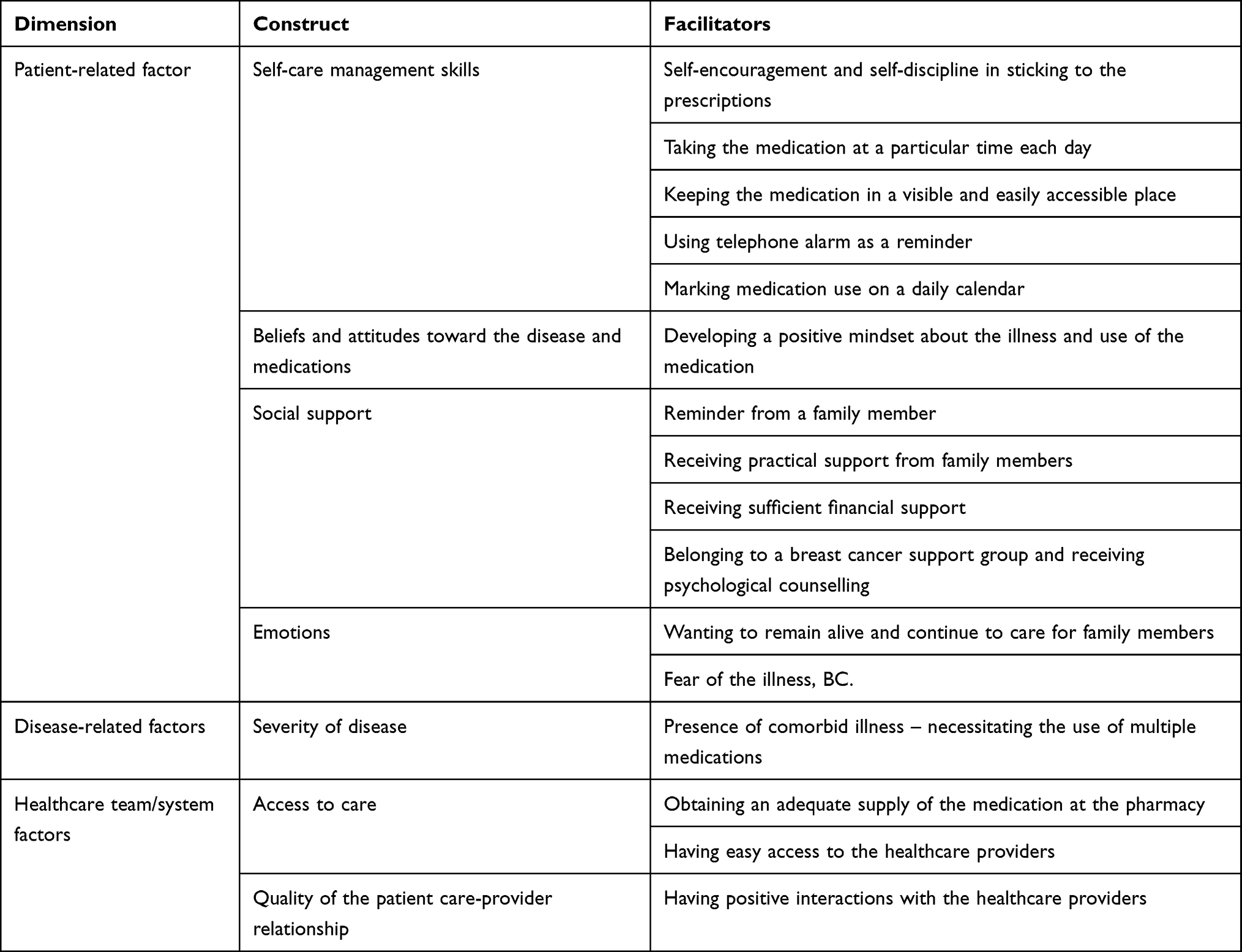 |
Table 3 Facilitators of Oral Anticancer Medication Adherence |
Patient and Close Relatives-Related Factors
There were twelve main themes identified in this dimension: (i) self-encouragement and self-discipline in sticking to the prescription (ii) taking the medication at a particular time each day (iii) keeping the medication in a visible and easily accessible place (iv) using telephone alarm as a reminder (v) marking medication use on a daily calendar (vi) developing a positive mindset about the illness and use of the medication (vii) reminder from a family member (viii) receiving practical support from a family member (ix) receiving sufficient financial support (x) belonging to a breast cancer support group and receiving psychological counselling (xi) wanting to remain alive and continue to care for family members (xii) Fear of the illness, BC.
Patients’ utilized various self-care management strategies to help them use their medications as prescribed. Patients’ capacity and confidence in their ability (self-efficacy) to self-manage their condition and use the prescribed medication, and the value they assigned to treatment, promoted their medication-taking behaviour, as stated by some patients.
… I live with the awareness that I’m a cancer patient…under treatment, so that helps me remember to take my medication … I don’t get overly anxious, so with that, I have been able to manage whatever I have experienced on this journey of cancer. (P9, Tamoxifen, Stage II)
Because I know it [medication] is what I can use to get sound health. I am helping myself; I don’t let anything disturb me from taking my medications; the help I do myself is to make sure I am punctual taking my medication. (P2, Tamoxifen, Stage I)
If you [patient] like yourself, you must use it [medication]…, they [doctors] don’t need to advise you [patient] before using it [medication], it is a must that you [patient]. use it [medication]. (P3, Letrozole, Stage II)
After taking my dinner and I relax for a while, then I take my medications…I take my medications every night. I take it anytime I take my dinner; I was told dinner should not exceed 7 pm, so after taking my meal around 7 pm or 7:30 pm after 30 minutes, I will take my medications. (P2, Tamoxifen, Stage I)
It’s at nine at night I take it [medication] … I take it last thing at night. (P9, Tamoxifen, Stage II)
I should be making it a point of duty to be taking it every morning because the issue of taking it morning today, tomorrow you [patient] … [take at another time]. One might forget one day; you go to bed without taking it. So … I should discipline myself to be taking it every morning. (P7, Tamoxifen, Stage III)
… It’s just always on my table, yes always on; if you open my door now, you will see it on my table, you will see it on my table, why? Because I don’t want to put it in one secret place and then … that will now make to forget to take it, so it’s always on my table. (P10, Tamoxifen, Stage I)
I have to set the alarm… for the drugs so that I will not forget it. So as soon as that alarm rings, my baby will leave anything she is doing, she will run and go and get a cup and water, … go and carry the medicine where I used to keep it, and she will bring it to me. So I had to set that alarm so that I don’t forget again. (P9, Tamoxifen, Stage II)
… I mark it [daily medication intake] on the calendar, and today I’ve not marked it. Any day I take it [medication], I mark it [calendar]. Then the next day, I know I didn’t take that day when I had not marked it [calendar]. The calendar is on my wall. (P11, Tamoxifen, Stage I)
Talking about my oral medication, it makes me very weak; it gives me terrible headache. I have a very positive view about my condition. So when these weaknesses come, I try not to dwell on my condition because I have seen that anxiety, even we’ve been taught scripturally, the bible says ‘Good heart is medicine’, so I try to be very positive. (P9, Tamoxifen, Stage II)
The truth is that … It’s a matter of mindset. I have this positive mindset that in as much as there is life, there is hope. In as much as the drugs are available, I get them. (P5, Tamoxifen, Stage I)
Then my daughter will always be there … she will give me water … mummy take your drugs… sometimes when I say ‘hold it, she will say ‘take it, take it. (P14, Capecitabine, Stage III)
In as much as I am able to afford the drug, I think God will continue to use my child to give me the needed support… (P9, Tamoxifen, Stage II)
Family members have been of help. Before, I wasn’t even walking, but they move me about on a wheelchair; they’ve been of great help. (P16, Capecitabine, Stage II)
When my children are around, they help me to prepare food, take care of my laundry, so it is easy for me to take my drugs. (P1, Capecitabine, Stage III)
They [family] normally give me money for everything, so I won’t say it’s money… anytime I want to buy it [medication] in [name of Pharmacy] (P1, Capecitabine, Stage III)
The founder of [name] the breast cancer support group, a non-governmental organization… brought me to this hospital, called and directed me to the doctor… gave me his numbers, then called him, sent me to him… paid for my… lab tests, everything for me to get set for the chemo… pay for the drugs for them to bring them here for me to take … (P11, Tamoxifen, Stage I)
When I remember some things about life, I want to take my medications so that I stay to take care of my children… Anytime I look at the situation on the ground, my children, I don’t want to leave them, so I used to try as much as possible to take my medication and do what is needful. (P1, Capecitabine, Stage III)
Knowing the condition I’m in, I would not want to take such a risk. I don’t want to take that kind of chance. I’m struggling to make sure I get better, so that’s why I wouldn’t want to miss my drug. (P9, Tamoxifen, Stage II)
Disease/Illness-Related Factors
The identified illness-related factor that facilitated patients’ medication adherence included the presence of comorbid illness, which required patients’ use of multiple medications and thus guided patients’ decisions to take medications as recommended by the clinician, as stated.
… My doctor always counsels me on these hypertensive drugs I am taking … [in addition to the anticancer medication]. I know I take it [medication] daily … I caution myself to be religious in taking them [medications] since they are daily drugs, I ensure that I take them [medications]. (P7, Tamoxifen, Stage III)
Healthcare Team/System-Related Factors
Three themes were identified in this dimension as adherence facilitators, namely (i) obtaining adequate medication supply at the pharmacy, (ii) having easy access to healthcare providers, and (iii) having positive interactions with healthcare providers.
Participants reported that obtaining an adequate supply of the medication at the pharmacy facilitated medication adherence.
… I don’t wait for my medication to finish entirely before calling my friend that provides for me to get some. When I’m on the last pack, … I will now ask him that I’m on the last pack, and then he will bring more for me, at times six-packs … (P10, Tamoxifen, Stage I)
Normally, I used to buy enough like three months … ahead, so before then I will be able to buy again. (P11, Tamoxifen, Stage I)
Some patients reported that having easy access to and positive interactions with healthcare providers promoted their medication adherence.
What makes it easier for me, it’s just I have a pharmacist’s number and then I call him…two to three days before time … I’m coming to the hospital on [day] for my chemo, please make my drugs ready, how much is it, he will let me know and then. the medications are always ready once I come I just pick them (P16, Capecitabine, Stage II)
I don’t find things difficult; I’m very free with my doctors. (P11, Tamoxifen, Stage I)
…I think the doctors know what they are doing. (P1, Capecitabine, Stage III)
Discussion
This study examined the barriers and facilitators of adherence to oral endocrine and nonendocrine medications among women diagnosed with breast cancer. To date, to our knowledge, no similar studies have been conducted in Nigeria. Moreover, a diverse sample of participants allowed exploring the common and unique themes relating to OAM adherence in this patient cohort. The study findings identified socioeconomic factors (high cost of medication) and therapy-related factors (medication side effects) as critical barriers to OAM adherence. Similarly, factors identified as main facilitators of OAM adherence included psychosocial factors related to the patient, such as (i) self-encouragement and self-discipline in sticking to the prescription, (ii) taking the medication at a particular time each day, (iii) receiving practical support from family members; and healthcare team/system factors including obtaining an adequate supply of the medication at the pharmacy. The main themes identified as key barriers and facilitators of adherence to OAMs are discussed below.
Barriers to Medication Adherence
Socioeconomic Barriers
Most participants experienced difficulties in being able to afford and use their medications as prescribed. However, this difficulty was most frequently reported by patients with stage II BC on oral tamoxifen for long-term use. They attributed this difficulty to the high cost of medication and their inability to afford medication without the required financial support. Some BC patients experienced financial hardships due to high treatment costs, including medication costs. Treatment cost is an important barrier to medication taking, particularly in African countries.46–48 This finding aligns with studies from developed countries, including the United States and the United Kingdom,49–52 but contrasts with a previous study from the United States.53 In Nigeria, BC patients might face specific adherence barriers caused by medication unaffordability due to limited financial resources arising from inadequate financial support, unemployment, or lack of health insurance coverage. Thus, the challenge of medication unaffordability and use could influence poor medication adherence, contributing to treatment failure and low survival observed in this population.54 This indicates the need to provide required financial support and free or subsidized anticancer medications for patients. Perhaps all aspects of BC treatment should be included in the Nigerian National Health Insurance Authority (NHIA). Low co-payment can reduce medication costs, enabling patients to afford prescribed medication to improve treatment outcomes, including survival.
Therapy/Medication-Related Barriers
Medication side effects, including fatigue, dizziness, and hot flashes, contributed to poor adherence to OAM, as reported in other BC studies.19,55 Some women who experience side effects may not seek appropriate support and may decide to change the dosage regimen without informing the clinician or stopping the medication altogether. Medication discontinuation due to side effects can contribute to disease progression, relapse or recurrence, and reduced survival. A systematic review of qualitative studies showed that healthcare providers (HCPs) do not adequately provide support or utilize opportunities for monitoring adherence to and managing symptoms of adjuvant endocrine therapy.55 Thus, suggesting the need for HCPs to educate and support patients about expected medication side effects at the start of treatment.
Furthermore, the use of concomitant medications contributed to patients’ experience of severe side effects and impacted adherence. Most patients reported concerns about medication side effects across BC stages (I, II and III) and OAM types. However, patients with stage II and III TNBC reported severe side effects related to intravenous chemotherapy combined with oral capecitabine for their treatment. These findings are consistent with other studies.56,57 Also, using multiple concurrent medications, including medications for other illnesses and the OAM, negatively impacted adherence for some patients. Some patients with stage I BC on oral tamoxifen for long-term use reported skipping or deciding not to take some of their medications due to concerns about the tiring routine of medication intake or having to take many medications for treatment. Other studies have also shown similar findings.5,58
Facilitators of Medication Adherence
Patient and Close Relatives-Related Factors
According to the patients, most factors that enabled medication adherence were psychosocial. The use of self-talk by patients provided needed self-encouragement. Also, self-discipline and the awareness of living with cancer and receiving treatment helped them cope with the illness and remember to take their medication. Evidence has shown that illness perceptions and medication beliefs are vital psychosocial determinants impacting oral anticancer treatment adherence. Patients’ perceptions of illness determine coping behavior, which in turn determines the outcome. Patients with adequate awareness or understanding of the nature of their condition and its required medical management (high illness perceptions) are more likely to devise adaptive and constructive mechanisms. This understanding assists them in coping with the illness, thereby promoting higher levels of medication adherence. In contrast, low illness coherence (understanding) is associated with lower medication adherence. Also, patients with high perceived necessity of the medication (positive medication beliefs) were more adherent than those with low perceived necessity (negative medication beliefs).59 Taking the medication at a specific time each day helped patients remember to adhere. Women who incorporated their medication-taking into their daily routines (eg waking up, at mealtimes, at bedtime) were more adherent. Once they could develop a consistent routine, taking the medication became a habit. A previous qualitative study in other settings showed that women with an established routine for taking medication were more adherent and persistent than those with no routine.38 Patients who received adequate practical support from family members found taking their medication as prescribed easier. Family members support to patients was through assisting them in purchasing the prescribed medicines, physically moving patients around to get treatment, and helping patients access medicine so they can use it appropriately. Other studies have indicated similar findings on the provision of social support and adherence to medication.60,61
Healthcare Team/System-Related Factors
Obtaining an adequate supply of medication at the pharmacy ensured that prescribed medication was available for patients to use and reduced the number of delayed or missed doses, thereby enabling medication adherence. Poor supply of medication due to medicines shortages or scarcity hindered medication adherence resulting in poor treatment outcomes as reported in other studies.62,63 This indicates the need for HCPs and policymakers to minimize the impact of medicine shortages by ensuring the continued availability of medications in health facilities to improve access to and use of medications and optimize patient outcomes.
Strengths and Limitations
To our knowledge, this study is the first to use qualitative methods to interview women in Nigeria about their experiences with adherence to oral endocrine and nonendocrine medications. The study applied the Framework Method and the WHO Multidimensional Adherence Model for thematic analysis of the interview data. Participants were recruited from two tertiary hospitals across southern Nigeria. They were diverse in age, marital status, ethnicity, level of education, and stage of BC at diagnosis and expressed a wide range of views. The diversity of patients’ experiences on adherence to OAMs based on the stage of BC provides insight into the varying barriers and facilitators of adherence that are common and unique to the patient categories in this study cohort.
However, the study does have limitations. All the participants were women with BC on OAMs still receiving treatment at tertiary hospitals. Thus, the present study findings may not generalize to women with BC who are either not receiving treatment or are receiving treatment outside of a tertiary hospital. Future studies should involve women with BC who become lost to follow-up to determine if they experience other challenges to treatment not reported in this study. Furthermore, this study did not fully explore some factors related to the illness, such as fear of BC progression and lack of knowledge about the illness. Thus, future research should include further questions about factors not fully explored in this study. Most patients had stage II BC, had multiple comorbidities, resided in an urban area, and had low financial resources. Hence, the themes identified may not readily be transferable or generalizable to other settings outside southern Nigeria. However, the purpose of this study was to obtain an in-depth insight into barriers and facilitators of OAM adherence experienced by this patient population.
Although the interview schedule was not pilot tested, it was checked by study supervisors and cross-checked by and discussed with the clinical oncologist of the study sites before and during the study. Conducting the interviews in a hospital setting might have caused participants to feel more reserved. However, the interviews were conducted in a private room in the hospital, and participants were assured of confidentiality and anonymity, which perhaps minimized participants feeling potentially more reserved. Moreover, clinic staff, including healthcare providers, were not informed of participants who consented to the study to prevent potential bias. Although transcripts were not returned to participants, member checks were performed with the participants who assessed the preliminary findings of their interview for the accuracy of the researchers’ account of their experiences, which enhanced the validity of our findings. However, when feasible, future research can pilot test the interview schedule, perform interviews in a setting that may minimize participants feeling more reserved (eg, participant home) and return transcripts to participants to improve study rigour further. Despite these limitations, our study findings provide valuable insights into the barriers and facilitators influencing adherence to OAMs as experienced by participants.
Implications for Practice, Policy, and Research
The findings may inform and motivate policymakers and oncology practitioners to design and evaluate programs or strategies that promote adherence in women with BC. Medication adherence programs for BC patients could be designed to improve medication-taking behavior. However, there is a need first to identify patients’ challenges and the factors potentially contributing to non-adherence. The high cost of care was identified as a major burden for most BC patients who could not afford treatment and medication without the necessary support. Therefore, strategies that promote cost containment or reduction in treatment costs, including medication costs for patients and the healthcare system, may improve adherence. Such strategies may mitigate the challenges of medication unaffordability caused by lack of financial support, unemployment, and low income, so that medications are available at affordable costs, enabling patients to obtain adequate medication supply, reduce dose delays, and missed or skipped doses.
Furthermore, strategies that promote side effects management could be developed to improve BC patients’ care. Clinicians could provide adequate explanations regarding expected medication side effects to patients at the start of treatment and perhaps avoid patients reducing medication doses without consulting clinicians or abandoning treatment altogether. This strategy may build patients’ confidence in treatment, minimize concerns about unexpected medication side effects, and encourage medication adherence.
Barriers and facilitators to OAM adherence occur at multiple dimensions. Hence, identifying the multifaceted factors contributing to non-adherence may guide decisions on adherence-enhancing strategies, with a focus on individual patient needs and medication types. Clinicians should routinely assess OAM adherence using context-specific measures to support patients in identifying potential barriers and recommend or employ context-specific facilitators or design a multifaceted intervention (eg, patient education and monitoring or strategies that promote cost-containment and side effects or symptom management) to optimize adherence. Patient adherence to OAMs is critical to successful treatment outcomes for BC patients. Therefore, these findings may improve the care of BC patients as they provide valuable insights regarding barriers and facilitators to OAM adherence which may inform and guide service improvement initiatives or inform intervention development, which may be tested in experimental studies. Ultimately, these efforts could enhance care quality and outcomes, including quality of life and survival in this patient population. Future research may be conducted across different healthcare settings by stages of BC, patients’ multimorbidity and demographic profiles. These research efforts could improve BC patient outcomes and advance the evidence base in Nigeria.
Conclusion
Barriers and facilitators influencing adherence to OAMs are multidimensional. Therefore, multifaceted strategies are required to support patients in optimizing adherence and treatment outcomes. In Nigeria, treatment cost, including medication cost, is a key barrier to ensuring optimal adherence. Some patients reported not taking their medication for days due to medication unaffordability caused by financial constraints. Insufficient medication supply and use may contribute to suboptimal adherence, treatment failure and reduced survival, which is common in this patient population. Therefore, developing and evaluating strategies promoting cost containment, availability and affordability of OAMs may ensure sufficient medication supply and minimize delays in medication intake. Perhaps all aspects of BC treatment, including free medication provision or reduced patient co-payments, may be included in the Nigerian National Health Insurance Authority (NHIA) to reduce the financial burden patients experience during treatment.
Furthermore, providing sufficient information regarding expected side effects at treatment commencement and prompt and adequate management of medication side effects when they occur may improve adherence. Hence, healthcare professionals should routinely assess, identify, monitor, educate and support patients with potential adherence challenges and barriers. Therefore, our findings may inform the designing and evaluating of context-specific measures to assess adherence and multifaceted intervention strategies targeting key barriers and approaches that enable adherence to enhance patient outcomes.
Data Sharing Statement
The datasets generated and/or analyzed that support the present study’s findings are available from the corresponding author upon reasonable request.
Acknowledgments
We thank the study participants for their time and the staff of the participating hospitals for their assistance with the study. We acknowledge TH Ajadi, who helped develop the coding index for this study.
Funding
The University of KwaZulu-Natal College of Health Sciences PhD scholarship (Award No. 636726) funded this research. IREX funding through the UASP alumni small grants program is acknowledged for providing a platform for the development of this publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Ferlay J, Ervik M, Lam F, et al. Global cancer observatory: cancer today. Lyon, France: International Agency for Research on Cancer; 2020. Available from: https://gco.iarc.fr/today.
3. McDonald ES, Clark AS, Tchou J, Zhang P, Freedman GM. Clinical diagnosis and management of breast cancer. J Nucl Med. 2016;57(2):9S–16S. doi:10.2967/jnumed.115.157834
4. Engle JA, Lohr L. Interventions to promote adherence to oral chemotherapy in clinical practice. Oncol Times. 2017;39(22):1–10.
5. Greer JA, Amoyal N, Nisotel L, et al. A systematic review of adherence to oral antineoplastic therapies. Oncologist. 2016;21(3):354–376. doi:10.1634/theoncologist.2015-0405
6. Paranjpe R, Trivedi M, Abughosh S. Identifying adherence barriers to Oral Endocrine Therapy (OET) among breast cancer patients. Value Health. 2018;21:S35. doi:10.1016/j.jval.2018.04.293
7. Krauss K, Stickeler E. Endocrine therapy in early breast cancer. Breast Care. 2020;15(4):337–346. doi:10.1159/000509362
8. Yussof I, Mohd Tahir NA, Hatah E, Mohamed Shah N. Factors influencing five-year adherence to adjuvant endocrine therapy in breast cancer patients: a systematic review. Breast. 2022;62:22–35. doi:10.1016/j.breast.2022.01.012
9. Masoud V, Pagès G. Targeted therapies in breast cancer: new challenges to fight against resistance. World J Clin Oncol. 2017;8(2):120–134. doi:10.5306/wjco.v8.i2.120
10. Tang M, Schaffer A, Kiely BE, et al. Treatment patterns and survival in HER2-positive early breast cancer: a whole-of-population Australian cohort study (2007–2016). Br J Cancer. 2019;121(11):904–911. doi:10.1038/s41416-019-0612-5
11. Weingart SN, Brown E, Bach PB, et al. NCCN task force Report: oral chemotherapy. J Natl Compr Canc Netw. 2008;6(Suppl 3):S1–14. doi:10.6004/jnccn.2008.2003
12. Cramer JA, Roy A, Burrell A, et al. Medication compliance and persistence: terminology and definitions. Value Health. 2008;11(1):44–47. doi:10.1111/j.1524-4733.2007.00213.x
13. Jacobs JM, Pensak NA, Sporn NJ, et al. Treatment satisfaction and adherence to oral chemotherapy in patients with cancer. J Oncol Pract. 2017;13(5):e474–e485. doi:10.1200/JOP.2016.019729
14. Spoelstra SL, Rittenberg CN. Assessment and measurement of medication adherence: oral agents for cancer. Clin J Oncol Nurs. 2015;19(3):47–52. doi:10.1188/15.S1.CJON.47-52
15. McCowan C, Wang S, Thompson AM, Makubate B, Petrie DJ. The value of high adherence to tamoxifen in women with breast cancer: a community-based cohort study. Br J Cancer. 2013;109(5):1172. doi:10.1038/bjc.2013.464
16. Cahir C, Barron TI, Sharp L, Bennett K. Can demographic, clinical and treatment-related factors available at hormonal therapy initiation predict non-persistence in women with stage I-III breast cancer? Cancer Causes Control. 2017;28(3):215–225. doi:10.1007/s10552-017-0851-9
17. Inotai A, Ágh T, Maris R, et al. Systematic review of real-world studies evaluating the impact of medication non-adherence to endocrine therapies on hard clinical endpoints in patients with non-metastatic breast cancer. Cancer Treat Rev. 2021;100:102264. doi:10.1016/j.ctrv.2021.102264
18. Murphy CC, Bartholomew LK, Carpentier MY, Bluethmann SM, Vernon SW. Adherence to adjuvant hormonal therapy among breast cancer survivors in clinical practice: a systematic review. Breast Cancer Res Treat. 2012;134(2):459–478. doi:10.1007/s10549-012-2114-5
19. Bhattacharya D, Easthall C, Willoughby KA, Small M, Watson S. Capecitabine non-adherence: exploration of magnitude, nature and contributing factors. J Oncol Pharm Pract. 2012;18(3):333–342. doi:10.1177/1078155211436022
20. Bourmaud A, Henin E, Tinquaut F, et al. Adherence to oral anticancer chemotherapy: what influences patients’ over or non-adherence? Analysis of the OCTO study through quantitative-qualitative methods. BMC Res Notes. 2015;8(1):291. doi:10.1186/s13104-015-1231-8
21. Partridge AH, Archer L, Kornblith AB, et al. Adherence and persistence with oral adjuvant chemotherapy in older women with early-stage breast cancer in CALGB 49907: adherence companion study 60104. J Clin Oncol. 2010;28(14):2418. doi:10.1200/JCO.2009.26.4671
22. Vacher L, Thivat E, Poirier C, et al. Improvement in adherence to Capecitabine and Lapatinib by way of a therapeutic education program. Support Care Cancer. 2020;28(7):3313–3322. doi:10.1007/s00520-019-05144-x
23. Onwusah DO, Ojewole EB, Chimbari MJ. Adherence to oral anticancer medications among women with breast cancer in africa: a scoping review. JCO Glob Oncol. 2023;9:e2100289. doi:10.1200/GO.21.00289
24. Lehmann A, Aslani P, Ahmed R, et al. Assessing medication adherence: options to consider. Int J Clin Pharm. 2014;36(1):55–69. doi:10.1007/s11096-013-9865-x
25. Clancy C, Lynch J, OConnor P, Dowling M. Breast cancer patients’ experiences of adherence and persistence to oral endocrine therapy: a qualitative evidence synthesis. Eur J Oncol Nurs. 2020;44:101706. doi:10.1016/j.ejon.2019.101706
26. Oguntola AS, Adeoti ML, Akanbi OO. Non-adherence to the use of tamoxifen in the first year by the breast cancer patients in an african population. East Cent Afr j Surg. 2011;16(1):1
27. Adisa AO, Lawal OO, Adesunkanmi ARK. Paradox of wellness and nonadherence among Nigerian women on breast cancer chemotherapy. J Cancer Res Ther. 2008;4(3):107. doi:10.4103/0973-1482.42640
28. Anele A, Bowling M, Eckert G, Gonzalez EL, Kipfer H, Sauder C. Treatment of breast cancer: imo State Nigeria versus Indiana, USA women–comparative analytic study. J West Afr Coll Surgeo. 2014;4(4):39.
29. Willis DG, Sullivan-Bolyai S, Knafl K, Cohen MZ. Distinguishing features and similarities between descriptive phenomenological and qualitative description research. West J Nurs Res. 2016;38(9):1185–1204. doi:10.1177/0193945916645499
30. Kim H, Sefcik JS, Bradway C. Characteristics of qualitative descriptive studies: a systematic review. Res Nurs Health. 2017;40(1):23–42. doi:10.1002/nur.21768
31. Harrell MC, Bradley MA. Data Collection Methods: Semi-Structured Interviews and Focus Groups. USA: RAND Corporation; 2009:TR-718–USG.
32. Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multidisciplinary health research. BMC Med Res Methodol. 2013;13(1):117. doi:10.1186/1471-2288-13-117
33. Smith J, Firth J. Qualitative data analysis: the framework approach. Nurse Res. 2011;18(2):52–62. doi:10.7748/nr2011.01.18.2.52.c8284
34. Sabaté E.World Health Organization Adherence to Long-Term Therapies: Evidence for Action. Geneva, Switzerland: World Health Organization; 2003.
35. Ando H, Cousins R, Young C. Achieving saturation in thematic analysis: development and refinement of a codebook. Compr Psychol. 2014;3(4). doi:10.2466/03.CP.3.4
36. Francis JJ, Johnston M, Robertson C, et al. What is an adequate sample size? Operationalizing data saturation for theory-based interview studies. Psychol Health. 2010;25(10):1229–1245. doi:10.1080/08870440903194015
37. Giuliano AE, Edge SB. Hortobagyi GN. Eighth Edition of the AJCC Cancer Staging Manual: breast Cancer. Ann Surg Oncol. 2018;25:1783–1785.
38. Cahir C, Dombrowski SU, Kelly CM, Kennedy MJ, Bennett K, Sharp L. Women’s experiences of hormonal therapy for breast cancer-exploring influences on medication-taking behaviour. Support Care Cancer. 2015;23(11):3115–3130. doi:10.1007/s00520-015-2685-x
39. Vasileiou K, Barnett J, Thorpe S, Young T. Characterising and justifying sample size sufficiency in interview-based studies: systematic analysis of qualitative health research over a 15-year period. BMC Med Res Methodol. 2018;18(1). doi:10.1186/s12874-018-0594-7
40. Ho SC, Jacob SA, Tangiisuran B, van Wouwe JP. Barriers and facilitators of adherence to antidepressants among outpatients with major depressive disorder: a qualitative study. PLoS One. 2017;12(6):e0179290. doi:10.1371/journal.pone.0179290
41. QSR International Pty Ltd. NVivo Qualitative Data Analysis Software. Version 12. QSR International Pty Ltd; 2018.
42. Ritchie J, Lewis J, Nicholls CM, Ormston R. Qualitative Research Practice: A Guide for Social Science Students and Researchers.
43. Candela AG. Exploring the function of member checking. Qual Rep. 2019;24(3):619–628.
44. Thomas DR. Feedback from research participants: are member checks useful in qualitative research? Qual Res Psychol. 2017;14(1):23–41. doi:10.1080/14780887.2016.1219435
45. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
46. Vanderpuye V, Olopade OI, Huo D. Pilot survey of breast cancer management in sub saharan Africa. J Glob Oncol. 2017;3(3):194–200. doi:10.1200/JGO.2016.004945
47. Mattila PO, Babar ZUD, Suleman F. Assessing the prices and affordability of oncology medicines for three common cancers within the private sector of South Africa. BMC Health Serv Res. 2021;21(661). doi:10.1186/s12913-021-06627-6
48. Gany F, Ayash C, Raad N, et al. Financial and food security challenges of Egyptian women undergoing breast cancer treatment. Support Care Cancer. 2020;28(12):5787–5794. doi:10.1007/s00520-020-05426-9
49. Vyas A, Descoteaux A, Kogut S, et al. Predictors of adherence to oral anticancer medications: an analysis of 2010–2018 US nationwide claims. J Manag Care Spec Pharm. 2022;28(8):831–844. doi:10.18553/jmcp.2022.28.8.831
50. Zaorsky NG, Khunsriraksakul C, Acri SL, et al. Medical service use and charges for cancer care in 2018 for privately insured patients younger than 65 years in the US. JAMA Network Open. 2021;4(10):e2127784–e2127784. doi:10.1001/jamanetworkopen.2021.27784
51. Cheng H, Lin L, Liu T, Wang S, Zhang Y, Tian L. Financial toxicity of breast cancer over the last 30 years: a bibliometrics study and visualization analysis via CiteSpace. Medicine. 2023;102(12):e33239. doi:10.1097/MD.0000000000033239
52. Longo CJ, Fitch MI, Banfield L, Hanly P, Yabroff KR, Sharp L. Financial toxicity associated with a cancer diagnosis in publicly funded healthcare countries: a systematic review. Support Care Cancer. 2020;28(10):4645–4665. doi:10.1007/s00520-020-05620-9
53. Wells KJ, Pan TM, Vázquez-Otero C, et al. Barriers and facilitators to endocrine therapy adherence among underserved hormone-receptor-positive breast cancer survivors: a qualitative study. Support Care Cancer. 2016;24(10):4123–4130. doi:10.1007/s00520-016-3229-8
54. Okoronkwo IL, Ejike-Okoye P, Chinweuba AU, Nwaneri AC. Financial barriers to utilization of screening and treatment services for breast cancer: an equity analysis in Nigeria. Niger J Clin Pract. 2015;18(2):287–291. doi:10.4103/1119-3077.151070
55. Peddie N, Agnew S, Crawford M, Dixon D, MacPherson I, Fleming L. The impact of medication side effects on adherence and persistence to hormone therapy in breast cancer survivors: a qualitative systematic review and thematic synthesis. Breast. 2021;58:147–159. doi:10.1016/j.breast.2021.05.005
56. Huo X, Li J, Zhao F, et al. The role of capecitabine-based neoadjuvant and adjuvant chemotherapy in early-stage triple-negative breast cancer: a systematic review and meta-analysis. BMC Cancer. 2021;21(1):78. doi:10.1186/s12885-021-07791-y
57. Zhang Z, Ma K, Li J, et al. The clinical value of chemotherapy combined with capecitabine in triple-negative breast cancer—a meta-analysis. Front Pharmacol. 2021;12:3241.
58. Wulaningsih W, Garmo H, Ahlgren J, et al. Determinants of non-adherence to adjuvant endocrine treatment in women with breast cancer: the role of comorbidity. Breast Cancer Res Treat. 2018;172(1):167–177. doi:10.1007/s10549-018-4890-z
59. Kaptein AA, Schoones JW, van der Meer PB, et al. Psychosocial determinants of adherence with oral anticancer treatment: ‘we don’t need no education’. Acta Oncol. 2021;60(1):87–95. doi:10.1080/0284186X.2020.1843190
60. Toledo G, Ochoa CY, Farias AJ. Exploring the role of social support and adjuvant endocrine therapy use among breast cancer survivors. Support Care Cancer. 2020;28(1):271–278. doi:10.1007/s00520-019-04814-0
61. Bright EE, Stanton AL. Prospective investigation of social support, coping, and depressive symptoms: a model of adherence to endocrine therapy among women with breast cancer. J Consult Clin Psychol. 2018;86(3):242–253. doi:10.1037/ccp0000272
62. Martei YM, Grover S, Bilker WB, et al. Impact of essential medicine stock outs on cancer therapy delivery in a resource-limited setting. J Glob Oncol. 2019;5:
63. Eniu A, Cherny NI, Bertram M, et al. Cancer medicines in Asia and Asia-Pacific: what is available, and is it effective enough? ESMO Open. 2019;4(4):e000483. doi:10.1136/esmoopen-2018-000483
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.