Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 12
Barriers and Facilitators for HIV Testing Practice Among Ethiopian Women Aged 15-24 years: Analysis of the 2016 Ethiopian Demographic and Health Survey
Authors Diress G ![]() , Ahmed M
, Ahmed M ![]() , Adane S
, Adane S ![]() , Linger M
, Linger M ![]() , Alemnew B
, Alemnew B ![]()
Received 3 October 2020
Accepted for publication 24 December 2020
Published 5 January 2021 Volume 2020:12 Pages 963—970
DOI https://doi.org/10.2147/HIV.S280590
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Gedefaw Diress,1 Mohammed Ahmed,1 Seteamlak Adane,1 Melese Linger,1 Birhan Alemnew2
1Department of Public Health, College of Health Science, Woldia University, Woldia, Ethiopia; 2Department of Medical Laboratory Science, College of Health Science, Woldia University, Woldia, Ethiopia
Correspondence: Gedefaw Diress Tel +251913756945
Email [email protected]
Background: In developing countries, youth women are most at risk of HIV infection. Center for Disease Control recommends that people who participate in high-risk behaviors get tested for HIV at least annually. In 2016, the Ethiopian Ministry of Health set goals to identify 90% of the people living with HIV by 2030. But undiagnosed HIV infections are still high in the country. To alleviate the problem, it is vital to identify the factors that hinder HIV testing practice. Therefore, this study aimed to identify the facilitators and barriers of HIV testing practice among Ethiopian youth women.
Methods: The analysis was done on 6401 women aged 15– 24 years using data from the 2016 Ethiopia Demographic Health Survey (EDHS). The main outcome variable was self-reported HIV testing practice. Multivariable logistic regression was used to identify the facilitators and barriers of HIV testing practice.
Results: In this study, 37.7% [95% CI: (33.6, 39.1)] of youth women were tested for HIV in their life. Being married (AOR=4.7; 95% CI: (3.67, 6.01)), divorced [AOR=6.2; 95% CI: (3.98– 9.54)], having primary level of education [AOR=2.4;95% CI: (1.79– 3.13)], and secondary level of education [AOR=4.0; 95% CI: (2.87– 5.63)], being rich [AOR=2.3;95% CI: (1.39– 3.91)] and being in the highest wealth index catagory [AOR=2.6;95% CI: (1.30– 5.16)] increase the odds of HIV testing. However, lack of media acccess [AOR = 0.7; 95 CI %: (0.54– 0.87)], lack of comprehensive HIV knowledge [AOR = 0.68; 65% CI: (0.53– 0.86)] and having discriminatory attitude towards PLHIV[AOR=0.79;95% CI: (0.64– 0.97)] decrease the odds of HIV testing.
Conclusion: The practice of HIV testing among youth populations was low as compared to national recommendations. Lack of media access, lack of comprehensive knowledge about HIV, and having discriminatory attitudes were the barriers to HIV testing practice. Marriage, secondary or higher education attainment, and high wealth index category were the facilitators for HIV testing. Improving HIV-related knowledge, improving media access, and minimizing discriminatory attitudes are strongly recommended to promote HIV testing practice.
Keywords: HIV testing, youth, demographic health survey, Ethiopia
Introduction
Globally, in 2017, approximately 3.9 million youths (15–24 years) were infected with HIV1 and it was increased by 30% between 2005 −2016.1,2 In Sub-Saharan Africa (SSA), young and adolescent are particularly vulnerable to HIV and other sexually transmitted infections; of all youth women living with HIV worldwide, 80% of women live in SSA.3–5 In 2017, the national HIV prevalence in Ethiopia was estimated to be 1.16%.6 Currently, in Ethiopia, 62% of the total people living with HIV (PLHIV) were female.7 One-third of the Ethiopian total population are young peoples, and approximately half of them were females.7 Youth and adolescents are extremely affected by HIV/AIDS and other sexually transmitted infections6,8 but the majority of youth did not know their HIV serostatus. Therefore, undiagnosed HIV infections are still high among sexually active segments of the population.9
Identifying 90% of the people infected with HIV was the first and crucial goal established by the Ethiopian Ministry of Health in 2016 because of the increasing number of new HIV infections.10,11 The goal will be achieved by improving HIV testing practice.12 Timely HIV testing is crucial for early diagnosis and enrollment to HIV chronic care which reduced the probability of transmission and HIV-related mortality.13,14 It is also important to promote HIV prevention among the negatives.9
The majority of youth in SSA including Ethiopia have not been tested for HIV. Past evidence revealed that only 32–55% of youth have been tested for HIV in their life.15–18 Similarly, a recent population-based survey in Ethiopia showed only 40% of women previously tested prior to the survey8 which implies a significant number of HIV seropositive people did not know their HIV-positive serostatus. Therefore, identifying the barriers and enablers to uptake HIV testing is crucial to improve HIV testing practice among population groups who participate in high-risk behaviors.
Previous studies have identified age, residence, education status, wealth index, used condom at last sex, consistent condom use, access to general medical care, access to HIV testing, knowledge of HIV, and substance use19–25 as factors that affect HIV testing. But the identified factors vary from population to population and from country to country. Most of the studies in Ethiopia have focused only on pregnant mothers whose HIV testing practice and health-seeking behaviors were different from the young and adolescent populations. Therefore, information regarding barriers to HIV testing specific to the youth population was limited in Ethiopia.8
Most of the previous studies did not assess the effect of discriminatory attitudes towards PLHIVon HIV testing practice except a study done in Kenya reported as an obstacle to HIV testing.26 The current study also tried to answer this information gap. Furthermore, nationwide information regarding HIV testing is needed to accelerate progress towards the three 90s goals in the country. Therefore, this study aimed to identify barriers and facilitators for HIV testing practice on youth women in Ethiopia using data from a national-based household survey to inform future policymakers for designing gender and age-specific interventions.
Materials and Methods
Data Sources and Study Population
This analysis used secondary data from the 2016 EDHS. Data were obtained from the DHS program website: https://www.dhsprogram.com. In 2016 EDHS, five questionnaires were used: the Household Questionnaire, the Woman’s Questionnaire, Men’s Questionnaire, the Biomarker Questionnaire, and the Health Facility Questionnaire. However, in this analysis, the authors used only women’s data. In 2016 EDHS, 15683 reproductive-age women have participated in the survey. After excluding women beyond the youth age group, we restrict our analytical sample to 6401 women aged 15–24 years. A detailed explanation of the methodology of 2016 EDHS is found somewhere else.8
Description of 2016 EDHS
In 2016 EDHS, the sampling frame was the 2007 Ethiopia Population and Housing Census. The census consists of 84,915 enumeration areas. One enumeration area was covering on average 181 households. During 2016 EDHS, Ethiopia has nine geographical regions and two administrative cities. The sample of 2016 EDHS was selected in two stages. Each region was stratified into urban and rural areas, yielding 21 sampling strata. Samples of enumeration areas were selected independently in each stratum in two stages. All reproductive-age women (15–49 years) who were either permanent residents or visitors who stayed in the selected household the night before the survey were eligible to be interviewed.
Study Variables and Measurements
The main outcome variable was HIV testing practice. Age, residence, educational status, wealth index, media exposure, Internet use, substance use, condom use at last sex, number of sexual partners, self-reported history of sexually transmitted infections, HIV-related stigma, and comprehensive knowledge on HIV were the independent variables.
In 2016 EDHS, comprehensive knowledge on HIV/AIDS was measured using the following five items. 1) Having just one uninfected faithful partner can reduce the chance of getting HIV, 2) Consistent use of condoms during sexual intercourse can reduce the chance of getting HIV, 3) healthy-looking person can have HIV, 4) HIV can be transmitted by mosquito bites and 5) a person can become infected by sharing food with a person who has HIV. Having a comprehensive knowledge of HIV was defined if respondents responded to all five questions correctly.
Access to media was classified depending on the answer to how often women read a newspaper, listened to the radio, or watched television. Women who answered at least once a week to any of these media were considered to have access to media. Substance use was measured based on the response to whether or not participants chew chat, drink alcohol, or smoke cigarettes. HIV-related discrimination was computed from two questions: would you buy vegetables from a vendor with HIV and Children with HIV should be allowed to attend school with children without HIV. Women who respond “yes” for the above two questions categorized as “non-stigma and discriminatory attitude” and who responded “no” or “I don’t know” for one or more questions categorized as “have stigma and discriminatory attitude”
Statistical Analysis
Participant characteristics were summarized using frequency and weighted percentage. A multivariable logistic regression model was used to determine the predictors of HIV testing uptake. All possible variables were included in the final regression model regardless of the p-values at the bivariable regression model. Adjusted odds ratios with 95% CI were used to measure the association between the independent and outcome variable. All statistical techniques used a complex sampling design applied in the 2016 EDHS.
Results
Participant Sociodemographic Characteristics
From the total participants, about 55% were found in the age group between 15 and 19 years. The majority of respondents (76.1%) were rural residents. Within this sample, 43.0% of youth women were Orthodox religion followers. About 57% were single in marital status and 20% of youth women did not attend formal education. Nearly 9.0% of youths women ever chewed chat. Only 24.3% of women had a comprehensive knowledge of HIV and only 7.5% of youth women used the Internet (Table 1).
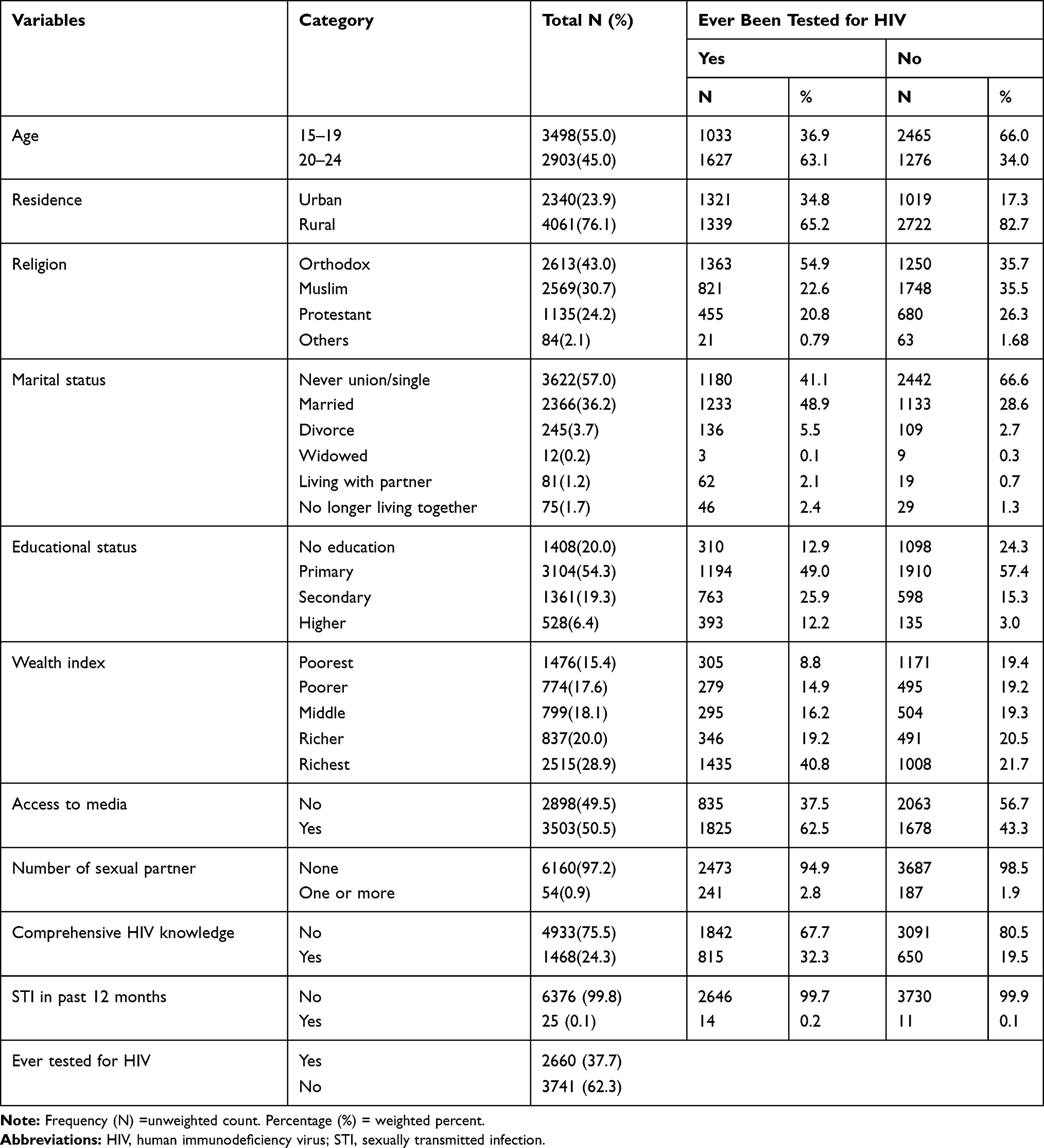 |
Table 1 Background Information of Participants (N=6401) |
HIV Testing Practice
The magnitude of HIV testing uptake in youth women was 37.7% (95% CI;35.3–40.2). Among HIV-tested women, the majority (63%) were in the age group between 20 and 24 years, and 65% were from rural residents. Nearly two-thirds of HIV-tested participants had media access but only one-third of women had a comprehensive knowledge of HIV (Table 1).
Barriers and Facilitators for HIV Testing
Marital status, wealth index, level of education, media exposure, comprehensive knowledge of HIV, and discriminatory attitude were significantly associated with HIV testing in the multivariate analysis model.
In this study, the odds of being tested for HIV were 5 times [AOR=4.7; 95% CI: (3.67–6.01)] higher among married women, 6.2 times [AOR=6.16; 95% CI: (3.98–9.54)] higher among divorced than single. The odds of being tested for HIV were higher among women with a primary level of education [AOR= 2.4; 95% CI: (1.79–3.13)] and secondary level of education [AOR=4.0; 95% CI (2.87–5.63)] when compared to those with no formal education.
Women found in the richer wealth index group were 2.3 times at higher odds of testing for HIV as compared to the lowest group. Similarly, women found in the richest level of wealth index were 3 times more likely to be tested for HIV (AOR=2.60;95% CI: (1.30–5.16)). Youth women with a lack of media access had a 31% reduction in the odds of testing uptake [AOR = 0.69; 95 CI %: (0.54–0.87)]. Similarly, participants with poor comprehensive HIV knowledge had a 32% [AOR = 0.68; 95% CI: (0.53–0.86)] lower probability of HIV testing as compared to their counterpart. Similarly, women who have discriminatory attitudes have lower HIV testing practice [AOR=0.79;95% CI: (0.64–0.97)] compared to those who have no discriminatory attitude (Table 2).
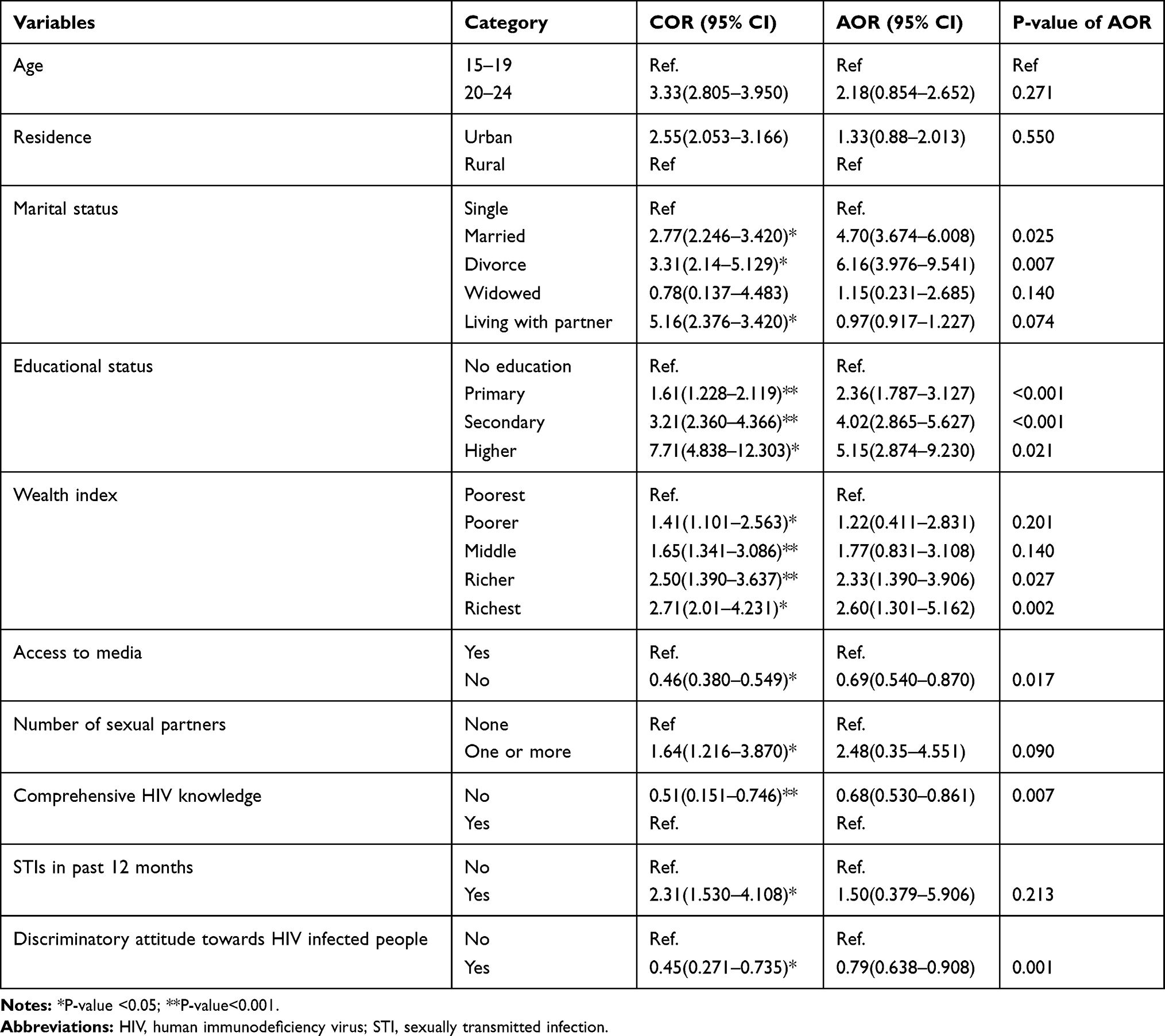 |
Table 2 Bivariable and Multivariable Analysis to Show Factors Associated with HIV Testing Among Youth Women Ethiopia |
Discussion
Using national survey data, we found that only one-third of women (15–24 years) were tested for HIV in their lifetime which is similar to previous studies in Africa15,27 but much lower than a study done in Zimbabwe.18 The current study is restricted to youth women age 15–24 years which may account for the differences in findings. Most of the HIV testing programs in Ethiopia targets key populations which include adolescents and young age groups. Although youths were identified as a target group for HIV testing in Ethiopia, the current finding suggests that a substantial number of youth women were unaware of their HIV status. Persons with unknown HIV status might enhance ongoing HIV transmission. To accelerate progress toward achieving the three 90s goal, the Ethiopian Ministry of Health and its partners should increase HIV testing coverage in communities particularly in the adolescents and young population.
Comparable to prior research from Zimbabwe and Uganda18,28 married women had a higher probability of being tested for HIV than never in a union. In Ethiopia, HIV testing before marriage for couples has been introduced as one approach to improving HIV testing coverage prior to the 2016 EDHS. This might initiate married women to know their HIV status better than single. In addition, women who are married might be tested during pregnancy. Finally, it might be because women with relationships might perceive their own risk of being infected with HIV.
In this study educational attainment is an important facilitator of HIV testing. A high educational level is associated with good HIV testing practice because of continued exposure to HIV prevention information that is more freely available in the school system than in the community.22,29 Educated women were found to be more knowledgeable on the benefit of testing like prevention of mother-to-child transmission30 which might initiate women to be tested for HIV. Finally, education might improve testing practice through improved recognition of the significance of knowing one’s HIV status and greater control over the decision to test. Thus, HIV testing approach should be emphasized among uneducated youth women.
Existing evidence has recommended that wealth index is vital in influencing HIV testing practices.31 Good economic status might be related to improved awareness of risks and reduce financial barriers to testing. This study also revealed that the highest wealth index (richer and richest) was associated with an increased likelihood of testing for HIV. Even if the test was free of charge in all government health institutions in Ethiopia, youth prefer private health institutions for their confidentiality.8 Lack of money might be a barrier for HIV testing in private health institutions as pointed in the past evidence.32
The other important finding is that good media access is positively associated with HIV testing which is supported by previous studies done in East Africa.33,34 Media exposure increases awareness about the importance of HIV testing and improves the understanding of the prevention approach which might initiate women to be tested for HIV. This finding points to the need for governmental and non-governmental organizations to use several types of media in convincing youths to constantly learn about the benefit of HIV testing and to know their HIV status. The current finding also showed that women who have no comprehensive HIV knowledge were less likely to be tested for HIV. This suggests that creating awareness about HIV in societies leads to an increase in the practice of HIV testing. This finding was supported by previous studies done in different parts of the world.30,35,36 In opposite to this, there was no association in a previous study conducted in Zimbabwe.18
As previously documented, this study shows that women who had a discriminatory attitude were less likely to be tested for HIV.8,37 The attitudes and perceptions related to HIV mode of transmission can be an important barrier to HIV testing and can operate on an individual level and institutional levels such as in healthcare services.30,38
The current study has several strengths such as a large nationally representative sample size, availability of detailed data on confounders, and standardized and high-quality data collection tool. However, there are several limitations to consider. First, we cannot assign causality because the data were cross-sectional. Secondly, in the original survey, data were collected based on self-report which might result in social desirability biases.
Conclusion
In Ethiopia, HIV testing for the youth population is a public health priority as the new infection is significantly high among this age group. However, HIV testing practice among youth is still low in our study. Being married, secondary level of education and high wealth index category were facilitators for HIV testing. Lack of media access, lack of comprehensive knowledge about HIV, and having discriminatory attitudes were the barriers to HIV testing practice. Therefore, promotion of education improves HIV-related knowledge, strengthens mass media awareness campaigns and minimizes discriminatory attitudes may be the possible means to increase HIV testing practice in Ethiopia. Future researchers should consider institutional level factors like lack of staff training and maintenance of confidentiality.
Abbreviations
AOR, adjusted odds ratio; COR, crude odds ratio; EDHS, Ethiopia Demographic Health Survey; HIV, human immunodeficiency virus; PLHIV, people living with HIV; SPSS, Statistical Package for Social Science.
Data Sharing Statement
The data can be available from the corresponding author and DHS database.
Ethical Approval and Consent to Participate
The investigators have accessed the EDHS survey data from the DHS program website: https://www.dhsprogram.com and then the researchers have maintained the confidentiality of the data.
Consent for Publication
Not applicable
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. WHO. Adapting and Implementing new recommendation on HIV patient monitoring. 2017.
2. All in to #End Adolescent AIDS. Available from: http://www.unaids.org/sites/default/files/media_asset/20150217_ALL_IN_brochure.pdf.
3. Bonnenfant YT, Hindin MJ, Gillespie D. HIV diagnosis and sexual risk behavior intentions among couple VCT clients in Ethiopia. AIDS Care. 2012;24(9):1078–1086. doi:10.1080/09540121.2012.663883
4. Bradley H, Tsui A, Kidanu A, Gillespie D. HIV infection and contraceptive need among female Ethiopian voluntary HIV counseling and testing clients. AIDS Care. 2010;22(10):1295–1304. doi:10.1080/09540121003692227
5. Enquselassie F, Girma S. HIV prevalence among clients with possible clinical signs of HIV infection: using the provider initiated testing and counseling approach. Ethiop Med J. 2009;47(3):187–194.
6. ETHIOPIA POPULATION-BASED HIV IMPACT ASSESSMENT(EPHIA) 2017-2018.
7. Central Statistical Agency. Population Projections for Ethiopia 2007-2037. 2013.
8. Central StatisticalAgency (CSA)[Ethiopia]. Ethiopia Demographic and Health Survey(EDHS). ICF; 2016.
9. National guidelines for comprehensive HIV prevention care and treatment, Ethiopia, MOH. 2017.
10. UNAIDS. 90-90-90: On the Right Track Towards the Global Target. Geneva: Switzerland; 2016.
11. HIV Prevention in Ethiopia National Road Map 2018-2020.
12. Cohen M, Chen Y, McCauley M, Gamble T, Hosseinipour M, Nea K. Prevention of HIV-1 Infection with early antiretroviral therapy. NEJM. 2011;365.
13. Fox J, White PJ, Macdonald N, et al. Reductions in HIV transmission risk behaviour following diagnosis of primary HIV infection: a cohort of high-risk men who have sex with men. HIV Med. 2009;10(7):5–8. doi:10.1111/j.1468-1293.2009.00708.x
14. Egger M, May M, Chene G, et al. Prognosis of HIV-1-infected patients starting highly active antiretroviral therapy: a collaborative analysis of prospective studies. Lancet. 2002;360(9327):119–129. doi:10.1016/S0140-6736(02)09411-4
15. Meehan SA, Sloot R, Draper HR, Naidoo P, Burger R, Beyers N. Factors associated with linkage to HIV care and TB treatment at community-based HIV testing services in Cape Town, South Africa. PLoS One. 2018;13(4):e0195208. doi:10.1371/journal.pone.0195208
16. Staveteig S, Croft TN, Kampa KT, Head SK. Reaching the ‘first 90ʹ: gaps in coverage of HIV testing among people living with HIV in 16 African countries. PLoS One. 2017;12(10):4–9. doi:10.1371/journal.pone.0186316
17. Brima N, Burns F, Fakoya I, Kargbo B, Conteh S, Copas A. Factors associated with HIV prevalence and HIV Testing in Sierra Leone: findings from the 2008 Demographic Health Survey. PLoS One. 2015;10(10):e0137055. doi:10.1371/journal.pone.0137055
18. Takarinda KC, Madyira LK, Mhangara M, et al. Factors associated with ever being HIV-tested in Zimbabwe: an extended analysis of the Zimbabwe Demographic and Health Survey (2010-2011). PLoS One. 2016;11(1):e0147828. doi:10.1371/journal.pone.0147828
19. Musheke M, Ntalasha H, Gari S, et al. A systematic review of qualitative findings on factors enabling and deterring uptake of HIV testing in Sub-Saharan Africa. BMC Public Health. 2013;13(1). doi:10.1186/1471-2458-13-220.
20. Oginni A, Obianwu O, Socio-demographic Factors AS. Associated with Uptake of HIV Counseling and Testing (HCT) among Nigerian Youth. AIDS Res Human Retroviruses. 2014;30.
21. Schwarcz S, Richards TA, Frank H, et al. Identifying barriers to HIV testing: personal and contextual factors associated with late HIV testing. AIDS Care. 2011;23(7):8–12. doi:10.1080/09540121.2010.534436
22. Chimoyi L, et al. HIV-related knowledge, perceptions, attitudes, and utilisation of HIV counselling and testing: a venue-based intercept commuter population survey in the inner city of Johannesburg, South Africa. Global Health Sci Pract. 2015.
23. Gwadz M, Cleland CM, Kutnick A, et al. Factors associated with recent HIV testing among heterosexuals at high risk for HIV infection in New York City. Front Public Health. 2016;4:76. doi:10.3389/fpubh.2016.00076
24. Murphy DA, Mitchell R, Vermund SH, Futterma D. Factors associated with HIV testing among HIV-Positive and HIV-negative high-risk adolescents. Pediatrics. 2002;110(3):e36–e36. doi:10.1542/peds.110.3.e36
25. Asaolu IO, Gunn JK, Center KE, Koss MP, Iwelunmor JI, Ehiri JE. Predictors of HIV Testing among Youth in Sub-Saharan Africa: a cross-sectional study. PLoS One. 2016;11(10):e0164052. doi:10.1371/journal.pone.0164052
26. Nall A, Tiffany Chenneville L, Rodriguez M, O’Brien JL. Factors affecting HIV testing among youth in Kenya. Int J Environ Res Public Health. 2019;16(8):1450. doi:10.3390/ijerph16081450
27. Staveteig S, Shanxiao W, Head SK, Bradley SE, Demographic EN. Patterns of HIV testing uptake in Sub-Saharan Africa. DHS Comparative Rep. 2013.
28. Bwambale FM, Ssali SN, Byaruhanga S, Kalyango JN, Karamagi CA. Voluntary HIV counselling and testing among men in rural western Uganda: implications for HIV prevention. BMC Public Health. 2008;8. doi:10.1186/1471-2458-8-263
29. Hargreaves J, et al. The association between school attendance, HIV infection and sexual behaviour among young people in rural South Africa. J Epidemiol Community Health. 2008;62.
30. Hamra M, Ross MW, Orrs M, D’Agostino A. Relationship between expressed HIV/AIDS-related stigma and HIV-beliefs/knowledge and behaviour in families of HIV infected children in Kenya. Trop Med Int Health Care Women Int. 2006;11:499–521.
31. Manirankunda L, Loos J, Alou TA, Colebunders R, Nöstlinger C. “It’s better not to know”: perceived barriers to HIV voluntary counseling and testing among sub-Saharan African migrants in Belgium. AIDS Educ Prev. 2009;21(6):582–593.
32. Conserve DF, Iwelunmor J, Whembolua G-L, Sofolahan-Oladeinde Y, Michelle Teti PJ, Surkan P. Factors associated with HIV testing among Men in Haiti: results from the 2012 Demographic and Health Survey. Am J Men’s Health. 2017;11:5. doi:10.1177/1557988316635247
33. Lompo ML, Bago J-L. How does exposure to mass media affect HIV testing and HIV-related knowledge among adolescents? Evidence From Uganda. Glob J Health Sci. 2018;10:1. doi:10.5539/gjhs.v10n9p1
34. Onsomu EO, Moore D, Abuya BA, Valentine P, Duren-Winfield V. Importance of the media in scaling-up HIV testing in Kenya. SAGE Open. 2013;3(3):2158244013497721. doi:10.1177/2158244013497721
35. Obermeyer CM, Osborn M. The utilization of testing and counseling for HIV: a review of the social and behavioral evidence. Am J Public Health. 2007;97(10):1762–1774. doi:10.2105/AJPH.2006.096263
36. Yahaya L, Jimoh A, Balogun O. Factors hindering acceptance of HIV/AIDS voluntary counseling and testing (VCT) among youth in Kwara State, Nigeria. Afr J Reprod Health. 2010;14(3):159–164.
37. Chimoyi L, Tshuma N, Muloongo K, Setswe G, Sarfo B, Nyasulu PS. HIV-related knowledge, perceptions, attitudes, and utilisation of HIV counselling and testing: a venue-based intercept commuter population survey in the inner city of Johannesburg, South Africa. Glob Health Action. 2015;8:26950. doi:10.3402/gha.v8.26950
38. Manirankunda L, Loos JAT, Colebunders R. C. N. “It’s better not to know”: perceived barriers to HIV voluntary counseling and testing among sub-Saharan African migrants in Belgium. AIDS Educ Prev. 2009;21(6):579–595.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.