Back to Journals » Patient Preference and Adherence » Volume 20
Barriers and Facilitating Factors for Preoperative Non-Invasive Positive Pressure Ventilation Compliance in Chinese Patients with Obesity Hypoventilation Syndrome: A Qualitative Study
Authors Qiu H, Zhang X ![]() , Lv N, Zhang G, Ma K
, Lv N, Zhang G, Ma K
Received 11 January 2026
Accepted for publication 29 June 2026
Published 9 July 2026 Volume 2026:20 594905
DOI https://doi.org/10.2147/PPA.S594905
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Dr Johnny Chen
Huifang Qiu,1 Xiaohong Zhang,2 Na Lv,1 Guoping Zhang,1 Kai Ma1
1Thyroid and Metabolic Surgery for Weight Loss Department, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, Taiyuan, 030032, People’s Republic of China; 2Nursing Department, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, Taiyuan, 030032, People’s Republic of China
Correspondence: Xiaohong Zhang, Nursing Department, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, Taiyuan, 030032, People’s Republic of China, Tel +8613453443366, Email [email protected] Na Lv, Thyroid and Metabolic Surgery for Weight Loss Department, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, Taiyuan, 030032, People’s Republic of China, Tel +8613453412879, Email [email protected]
Aim: To explore factors influencing compliance with Non-invasive Positive Pressure Ventilation therapy in patients with obesity hypoventilation syndrome (OHS) prior to bariatric surgery, and to identify enabling factors and barriers using the capability, opportunity, and motivation-behavior model (COM-B model).
Design: A qualitative descriptive design.
Methods: Using purposive sampling, 13 patients with OHS who underwent bariatric metabolic surgery in the general surgery department of a tertiary hospital in Taiyuan from March to September 2025 were selected. Face-to-face semi-structured in-depth interviews were conducted, and the interview data underwent content analysis to extract themes.
Results: This study summarizes from three main factors: capability, opportunity, and motivation, and extracts the three major facilitating factors and barrier factors for patients with OHS to use Non-invasive Positive Pressure Ventilation (NIPPV) before weight loss surgery. Among them, facilitating factors include: Capability factors (positive perceptions and internalization of health awareness for positive pressure ventilation), Opportunity factors (family support, motivational effects of and peer support, assistance and supervision from professionals), and Motivation factors (urgency of ensuring surgical safety, strong motivation for rehabilitation, fear of severe health consequences, positive feedback from symptom improvement). Barrier factors include: Capability factors (the physiological burden of obese patients, lack of self-efficacy in changing past habits, insufficient cognitive ability), Opportunity factors (insufficient professional support, unfavorable rehabilitation environment), Motivation factors (uncomfortable wearing experience, fatigue while wearing, anxious mind and sense of shame).
Conclusion: The use of NIPPV before weight loss surgery in patients with OHS is influenced by their capability, opportunity, and motivation. Patients with OHS are highly reliant on authoritative information. Clinical medical staff can leverage “peer support”, focus on the spontaneous motivational role of positive pressure ventilation in patients with OHS, and use positive feedback incentive mechanisms to improve the enthusiasm and compliance with positive pressure ventilation, thereby helping patients with OHS achieve better ventilation outcomes.
Practice Implications: Clinical interventions should target the above multidimensional factors, focusing on strengthening patient cognitive education and self-efficacy, optimizing family and social support systems, improving wearing comfort, and alleviating psychological burden, thereby effectively enhancing preoperative adherence to NIPPV.
Keywords: obesity hypoventilation syndrome, weight loss metabolism, positive pressure ventilation, compliance, facilitating factors, barriers, qualitative research
Introduction
With the rapid development of the national economy and the improvement of people’s living standards, the number of obese individuals has been increasing daily. Consequently, the public health burden associated with obesity-related diseases such as cardiovascular diseases, metabolic disorders, and sleep-disordered breathing has become increasingly severe.1 Obesity Hypoventilation Syndrome (OHS) refers to insufficient alveolar ventilation in obese individuals (body mass index (BMI) ≥30 kg/m2) during wakefulness, characterized by arterial blood carbon dioxide partial pressure (PaCO2) ≥45 mmHg. This condition must be distinguished from other chronic respiratory diseases, OHS is a clinical syndrome that is a type of sleep-disordered breathing.2 According to literature reports,3 the prevalence of OHS in obese populations is 1.1%, while among patients scheduled for weight-loss surgery, the proportion with preoperative OHS is 8%.4 The prevalence of OHS among patients with obesity and obstructive sleep apnea (OSA) is 10% to 20%.5 Without timely treatment, patients may develop hypertension, heart failure, pulmonary hypertension, respiratory failure, and poor sleep quality, increasing their risk of death. The mortality rate within two years can reach as high as 24%.6 Currently, the primary treatment approaches for OHS include weight management (considered when BMI ≥ 40 or BMI ≥ 35 with complications), improvement of sleep-disordered breathing, and medication therapy.7
Weight-loss metabolic surgery is an effective treatment for obese patients, significantly improving OHS. However, patients with OHS are at increased risk of perioperative complications due to obesity-related respiratory compromise.8 Preoperative NIPPV should be administered to patients with OHS for at least 4 hours, or even up to 6 hours. It can effectively improve ventilation and oxygenation, alleviate respiratory muscle fatigue, reduce the incidence of pulmonary complications and perioperative risks of atrial fibrillation, alleviate symptoms related to preoperative sleep and respiratory disorders, and significantly enhance the outcomes of bariatric surgery while reducing the incidence of complications and surgical risks; it is also effective when used for a short period of time.9,10 However, data indicate that patients with OHS have poor compliance with preoperative NIPPV support, with non-compliance rates approaching 50%.11 A large number of patients either use the device for insufficient periods or discontinue use altogether. Obese and overweight patients face even greater challenges due to their specific physiological and psychological characteristics (such as large neck circumference, skin issues, low self-esteem, and claustrophobia), and may even develop a psychological aversion to positive pressure ventilation from the outset, refusing to use it, making it difficult to improve compliance.9
Current research on obese patients primarily focuses on the postoperative period—such as diet, exercise, follow-up, and weight loss outcomes—and lacks studies on preoperative preparation. Furthermore, most adherence research has focused on OSA rather than OHS; studies on OHS patients have also been predominantly quantitative, with most analyzing factors influencing the use of non-invasive ventilators. There is insufficient exploration of the factors that facilitate or hinder patients’ subjective experiences, and a lack of relevant qualitative research. In addition, while quantitative methods can measure what has occurred (such as compliance rates), qualitative methods are needed to understand the causes and mechanisms—capturing personal experiences, beliefs, and contextual factors that surveys cannot capture. The COM-B model is a theoretical framework used to analyze the determinants of behavior and its underlying mechanisms. It comprises three behavioral components: capability (physical skills and strength, knowledge and understanding), opportunity (cultural background, social relationships, and time, place, and resources), and motivation (planning, evaluation, desire, and emotions). The model posits that for behavior to occur, three basic conditions—ability, opportunity, and motivation—must be met. Behavioral change can only be achieved when an individual possesses all three simultaneously, and the behavior itself also exerts a reciprocal influence on these three components.12 Therefore, this study employs a descriptive qualitative research methodology, using the COM-B model to guide the content analysis of interviews, in order to thoroughly explore the real-life experiences of obese and overweight patients NIPPV. By examining multiple perspectives, the study aims to fully identify the facilitating and hindering factors associated with preoperative positive pressure ventilation in patients with OHS, with the goal of providing a scientific basis for clinical healthcare professionals to implement relevant behavior change strategies.
Objects and Methods
Sample/Participants
Using purposive sampling, patients with OHS undergoing bariatric metabolic surgery admitted to the General Surgery Department of a Grade III Class A hospital in Taiyuan City between March and September 2025 were selected as study subjects. Inclusion criteria include:① Diagnosed with OHS; ② Age ≥ 18 years; ③ Meets Chinese diagnostic criteria for obesity and surgical indications specified in the Chinese Guidelines for Surgical Treatment of Obesity and Type 2 Diabetes (2014); ④ First-time weight-loss metabolic surgery patients; ⑤ Able to communicate effectively and actively participate in interviews; ⑥ Informed consent for this study. Exclusion criteria include:① Patients with severe complications such as heart failure, serious infections, or malignant tumors; ② Unable to communicate normally due to mental or other issues. Detachment Criteria:① Patients who died during follow-up; ② Those who withdrew from the study for various reasons. This study took individual differences among the interviewees fully into account. The sample size was determined based on the principle of achieving saturation in theme extraction during data analysis, with preliminary coding conducted after every three interviews. The results showed that no new themes or codes emerged after the 10th interviewee; to ensure stability, we conducted interviews with three additional participants (for a total sample size of 13) and confirmed that no new concepts or relationships appeared. A total of 13 patients with OHS who underwent bariatric surgery were interviewed. The general characteristics of the study subjects are presented in Table 1. This study has been reviewed and approved by the Ethics Committee of Shanxi Bethune Hospital. Ethics Committee of Hospital in July 2024 (Approval Number: YXLL-2024-134), and was conducted in accordance with the Declaration of Helsinki. All participants provided written informed consent, which explicitly included permission for their anonymized responses and direct quotes to be used in publication.
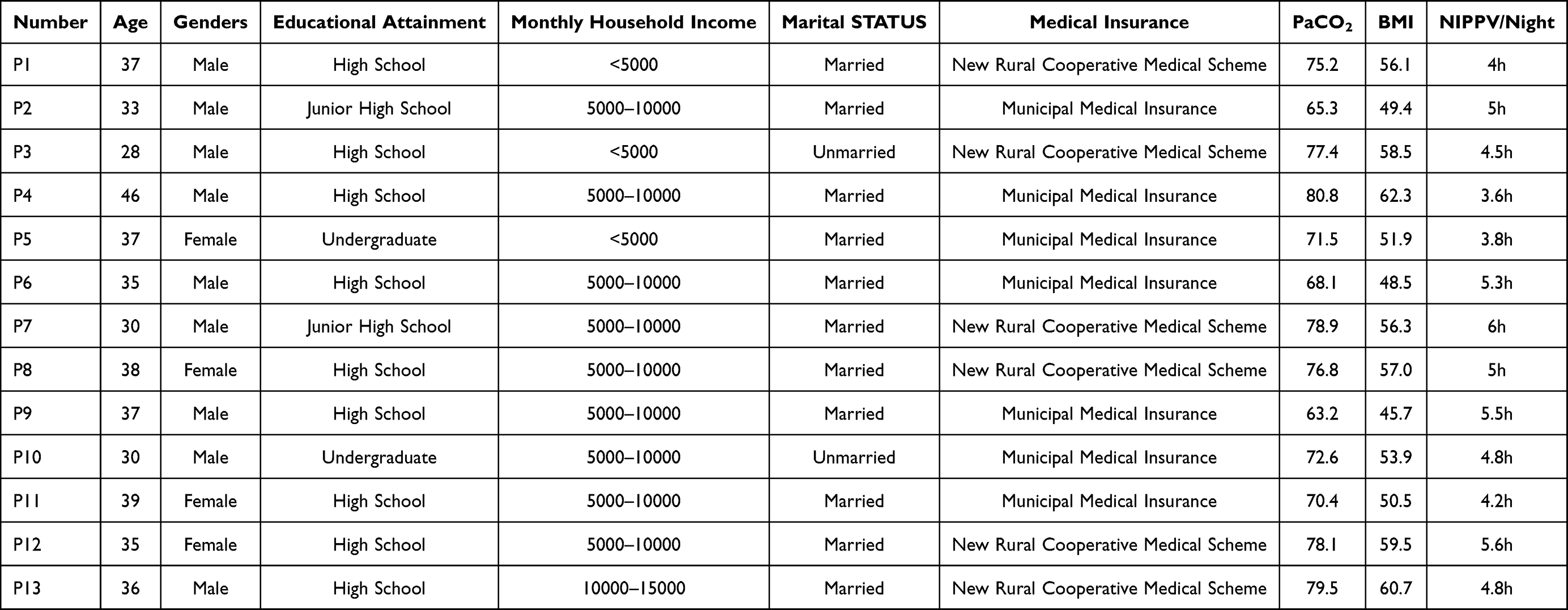 |
Table 1 General Characteristics of Study Participants (n=13) |
Research Methods
Interview Guide
This study employed a descriptive qualitative research methodology, utilizing theory-based interview techniques combined with a literature review. An initial interview outline was developed based on discussions within the research team. Two patients with OHS who had undergone bariatric surgery and met the inclusion criteria were selected for preliminary interviews, which were used to finalize the interview outline and revise and refine the interview guide accordingly. Data saturation was achieved when no new or surprising information emerged from further data collection. Specifically: capability ① Have you previously used a non-invasive ventilator to assist with breathing? How was your experience with it, and how did it feel? Can you describe your experience with positive pressure ventilation? ② Can you describe the benefits you perceive from using a non-invasive ventilator? Motivation ③ Can you describe the reasons or circumstances that led you to start using a non-invasive ventilator to assist with breathing? ④ Can you describe what motivates you to continue using the non-invasive ventilator? Opportunity ⑤ What factors might cause you to stop using the non-invasive ventilator or prevent you from continuing to use it?
Data Collection
This study conducted interviews in the preoperative consultation room, with each session lasting approximately 30 minutes. The interviews were conducted by two nursing graduate students from the research team who had received specialized training in qualitative research and possessed sufficient expertise in qualitative research methods and interview techniques. To ensure the quality of the interviews, a strong relationship of trust was established with the participants prior to the interviews to guarantee the authenticity and rigor of the results. Prior to the interview, the researchers introduced themselves to the participants, explained the purpose, content, and specific methods of the interview, and assured them that the principles of confidentiality and voluntariness would be strictly observed. After obtaining the patient’s consent, the entire interview was audio-recorded to ensure the accuracy and completeness of the recorded data. A semi-structured interview method was employed, beginning with open-ended questions and adjusting the content appropriately based on the interview context to ensure that participants could express their genuine feelings and thoughts. During the interview, adhere to the requirements and principles of the interview process, avoid leading questions, and simultaneously record the interviewee’s nonverbal expressions.
Qualitative Analysis
Within 24 hours of the interview, the researcher promptly transcribed the interview data. The interview data were analyzed and organized using NVivo 12.0 software. Content analysis was employed, following Braun and Clarke’s thematic analysis method. The entire process included: (1) repeatedly reading the transcripts to familiarize oneself with the data and annotating key points and ideas; (2) conducting line-by-line open coding; (3) merging similar codes to preliminarily form themes; ④ reviewing and adjusting the thematic structure against the original data; ⑤ clearly defining the connotations of each theme, defining items based on the COM-B model, and integrating the data into meaningful interpretations of the research content according to internal connections and logical relationships; ⑥ selecting representative quotations to draft the results report, with researchers mapping and interpreting each theme and its corresponding textual content to form the final research findings. Throughout this process, the two researchers coded the data independently and resolved discrepancies through discussion. To ensure credibility, we provided interviewees with audio recordings and transcripts for review. Additionally, we incorporated peer review, in which two researchers who did not participate in data collection independently performed open coding on 20% of the interview transcripts, achieving 89% inter-coder agreement. We maintained a complete audit trail (including original recordings, transcripts, coding logs, and analysis memos) to demonstrate the chain of reasoning from data to conclusions. If two researchers disagreed during data analysis, they consulted a third senior researcher to reach consensus and finalize the themes.
Results
Based on the COM-B model—which analyzes the facilitators and barriers affecting adherence to positive pressure ventilation among patients with OHS from the perspectives of capability, opportunity, and motivation—a framework analysis was conducted, resulting in eight subthemes each for facilitators and barriers. The relationships among these three elements under the two main themes are illustrated in Figure 1.
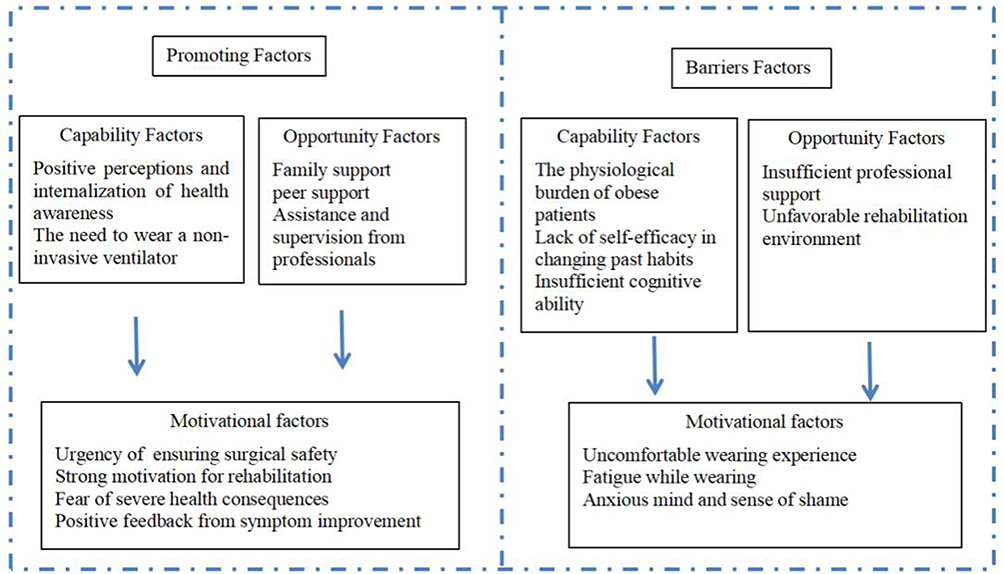 |
Figure 1 Conceptual Framework of Facilitating Factors vs Barrier Factors. |
Theme 1: Facilitating Factors
Capability Factors
Positive Perceptions and Internalization of Health Awareness for Positive Pressure Ventilation
Most patients with OHS undergoing weight-loss surgery recognize the positive impact of using a non-invasive ventilator on their health and postoperative recovery, and have gradually incorporated this into their own health awareness. This recognition motivates them to use the ventilator proactively and serves as a key driving force in helping them stick with the treatment.
P7:I am aware of this myself. I even bought a small ventilator for home use. It helps reduce the number of apneas during the night.
P13:After getting used to wearing it for a while, it really does feel more comfortable I sleep better at night—no more waking up gasping for air in the middle of the night—and I feel more alert the next day.
Understanding your own needs can significantly improve compliance with NIPPV.
P1:I think Positive pressure ventilation before surgery effectively ensures the smooth progress of the procedure. It serves as a protective measure for the surgery, so I can stick with wearing it.
Opportunity Factors
Family Support
Some patients reported that their families provided significant emotional support by encouraging them to use Positive pressure ventilation for respiratory assistance, offering positive emotional value.
P2:My sleep apnea and snoring have been getting worse and worse. My spouse often wakes me up in the middle of the night, worried that I might stop breathing, and even bought me a portable breathing device online.
Motivational Effects of and Peer Support
Against the backdrop of rapid information development, peer support has transcended geographical boundaries, and remote interaction formats can effectively motivate patients to Positive pressure ventilation for assisted breathing.
P1:Since I first started learning about bariatric surgery, I have consulted with many doctors and joined WeChat groups for people with obesity. One member shared that she used a non-invasive ventilator before her surgery; at first, it was very uncomfortable and she felt like she could not breathe, but once she got the hang of it, she realized it was really necessary… She often encourages us, her fellow patients, to follow the doctors’ instructions.
P13:My fellow patient in the clinic was admitted before me. He’s been using the ventilator for two days now and has been consistent with it. I can stick with it too.
Assistance and Supervision from Professionals
Some patients expressed trust and reassurance when healthcare providers personally assisted them in wearing non-invasive ventilators. They were willing to follow the professionals’ guidance and demonstrated greater perseverance in wearing the device throughout the night under supervision.
P2:Although it did feel uncomfortable at first, the hospital is definitely more professional, so I am willing to follow the medical staff’s instructions… I will still be able to overcome my fear and keep wearing it.
P5:I do not know why the ventilator was removed in the middle of the night; on several occasions, the medical staff came by during their rounds and put it back on for me.
The attitude and competence of medical staff directly impact patient confidence. Patient initial guidance and prompt problem-solving significantly enhance patients’ sense of security.
P13:That nurse was especially patient, teaching me several times until I felt comfortable.
Motivational Factors
Urgency of Ensuring Surgical Safety
Ensuring surgical safety is the primary motivation for patients to Positive pressure ventilation for respiratory support.13 In this study, patients were willing to actively comply with medical staff instructions.
P8:The doctor said my blood oxygen saturation is too low now and I need to wear a non-invasive ventilator to adjust it. Otherwise, the surgery could be dangerous.
Strong Motivation for Rehabilitation
Rehabilitation motivation serves as the purpose and rationale for patients undergoing positive pressure ventilation. It acts as the driving force influencing patients to initiate and adhere to positive pressure ventilation therapy. Patients undergoing weight reduction and metabolic improvement surgery often employ psychological techniques such as self-affirmation to enhance their motivation for positive pressure ventilation. They believe thorough preoperative preparation can effectively reduce postoperative complications and promote recovery.
P5:I told myself I must persist with positive pressure ventilation to ensure better postoperative recovery.
Fear of Severe Health Consequences
Some patients’ compliance stems from fear of disease progression.
P1:I am afraid of this surgical approach, so I even bought insurance. I definitely hope the surgery goes smoothly. I will do anything that ensures my surgery proceeds without issues without hesitation.
P6:Wearing a non-invasive ventilator before surgery improves my blood oxygen levels while removing carbon dioxide, which is crucial for the procedure. This undoubtedly eases my anxiety about the surgery.
Positive Feedback from Symptom Improvement
Some patients report significant relief from symptoms like breathing difficulties and nighttime awakenings after Positive pressure ventilation, with improved sleep quality reflected in better daytime naps and reduced fatigue.
P5:I used to wake up gasping for air every night, feeling dizzy and weak the next day. Since Positive pressure ventilation, I can sleep through the night. Now I have energy even when walking during the day—it just makes me determined to keep using it.
Theme 2: Barriers Factors
Capability Factors
The Physiological Burden of Obese Patients
The physical burden poses the greatest challenge for patients with OHS undergoing weight-loss surgery when Positive pressure ventilation for respiratory support. Excess facial fat and unique anatomical structures lead to airway collapse and reduced intrathoracic pressure, making gas exchange laborious—the primary reason most patients with OHS refuse Positive pressure ventilation14.
P8:My face is large and chubby, so wearing the ventilator feels uncomfortable It frequently triggers alarms, and the mask leaks air, requiring constant adjustments. It feels like a burden.
P4:The airflow impact is too strong, making it hard to adapt to the ventilator’s rhythm. It might be related to my weight—exhaling feels laborious, which actually makes me feel more suffocated.
Lack of Self-Efficacy in Changing Past Habits
After receiving an OHS diagnosis, psychological and behavioral barriers further diminish patients’ motivation and persistence in altering established habits. This stems from a lack of drive to change past patterns and insufficient self-efficacy in actively adopting new respiratory support methods.
P3:I’d never used one before, and suddenly having this foreign object requires constant vigilance while sleeping. I cannot rest soundly and find it quite bothersome.
Insufficient Cognitive Ability
The use of NIPPV for respiratory support prior to bariatric surgery is underestimated. Patients place greater emphasis on the immediate success of the procedure, failing to recognize the importance of preoperative non-invasive ventilator therapy and its long-term benefits for postoperative recovery.
P9:I know I have severe sleep apnea, but I’ll recover quickly after surgery. As long as the surgery is successful, that’s all that matters. Preoperative Positive pressure ventilation isn’t very meaningful.
P8:I’ve never heard of Positive pressure ventilation. I didn’t know wearing a ventilator could alleviate sleep apnea.
P10:It’s not that I don’t want to keep wearing it. My surgery is the day after tomorrow—will wearing it for just a day or two even make a difference?
Opportunity Factors
Insufficient Professional Support
Some patients with OHS undergoing weight-loss surgery reported that medical staff tended to focus more on educating them about how to wear non-invasive ventilators and their benefits, while providing fewer details about potential risks.
P1:Because the nurse’s explanation was rather vague, and I didn’t get a clear answer after asking, I didn’t know the risks of refusing to Positive pressure ventilation.
P6:I felt uncomfortable and asked the staff to adjust the machine’s pressure. They said they weren’t trained to do so and wouldn’t adjust it arbitrarily, insisting that a respiratory specialist was needed.
Unfavorable Rehabilitation Environment
Patients undergoing bariatric surgery for weight loss may face environmental constraints when wearing non-invasive ventilators preoperatively, including space, personnel, and facilities. ① Peer pressure: Some interviewees expressed difficulty tolerating the unusual looks from roommates, which weakened their resolve to Positive pressure ventilation.
P8:Every time I put on the ventilator equipment, other patients and their families would give me strange looks. Though no harsh words were spoken, this behavior made me uncomfortable—I didn’t want to be seen as different.
② Mismatch of equipment: The lack of specialized non-invasive ventilator masks for obese patients means standard masks do not fit properly, leading to issues like mask slippage and poor facial seal. This significantly hinders their willingness to use the device.
P2:The main problem is the mask constantly slipping off and leaking air. Just when I finally get coordinated with the ventilator, any interruption is frustrating and makes me feel annoyed.
Motivational Factors
Uncomfortable Wearing Experience
Most patients may experience discomfort while Every time I put on the ventilator equipment, such as labored breathing, irregular breathing patterns, shortness of breath, stuffiness, mask pressure, and noise disturbance. These discomforts can reduce their willingness to use the ventilator, leading to withdrawal and reluctance to continue therapy.
P13:During use, I felt suffocated, like being held underwater, desperately trying to breathe—it was terrifying.
P1:I sweat easily anyway, but the ventilator mask made me feel even hotter and sticky, extremely uncomfortable.
P5:The headgear caused headaches, and I woke up with marks all over my face”. The fit between the device and the patient directly impacts the treatment experience.
P6:“We adjusted the pressure several times, but it either felt like I couldn’t breathe or the airflow ‘pushed’ against me uncomfortably.
Fatigue While Wearing
Some patients report experiencing fatigue on both physical and psychological levels during wear, which subsequently becomes one of the obstacles to consistent use.
P10:I have been wearing it as the medical staff advised, but I cannot guarantee I will wear it all night—I am just too tired.
P12:I just don’t want to wear it; I’m physically and mentally exhausted, and I can’t bring myself to use the ventilator.
Anxious Mind and Sense of Shame
Some patients, especially younger ones, feel ashamed about using ventilators, viewing it as a sign of “terminal illness” that damages their self-image.
P3:I already felt inferior because of my weight. Wearing a ventilator made me feel embarrassed—I didn’t want my partner to see me like that”. Others develop psychological resistance, commonly experiencing a “sense of confinement”. Wearing it at night feels restrictive and can trigger anxiety.
P11:Wearing the ventilator means I can’t even sleep on my side. It’s so restrictive, it’s frustrating.
Discussion
Patients with OHS Undergoing Weight-Loss Surgery Exhibit a Higher Demand for Positive Pressure Ventilation Support Preoperatively, yet the Specialized Technical Support Provided by Healthcare Personnel Remains Inadequate
Among opportunity factors, a good environment can promote the occurrence of positive behaviors in individuals. This study found that three levels of social support systems—professional support, peer support, and family support play an important role in OHS patients wearing non-invasive ventilators. Three out of the 13 participants believed that information from clinical healthcare providers to be the most authoritative and valuable, and thus were more willing to follow their professional advice.15 However, clinical healthcare providers lack specialized technical proficiency in operating non-invasive ventilators. Moreover, most professionals provide only generic guidance when encouraging patients with OHS to use these devices, failing to present cautionary examples that illustrate the potential risks involved. Therefore, healthcare professionals should be provided with access to relevant specialized knowledge and technical training to master the operational adjustments of non-invasive ventilators. Additionally, clinical staff should enhance their knowledge and methods of disease education, combining positive guidance with negative examples to develop targeted, comprehensive educational models. This approach promotes positive preoperative cognition and internalization of health awareness regarding non-invasive ventilator use among patients with OHS, thereby improving their compliance. This study also found that patients with OHS are more inclined to peer support, and related research indicates that peer support is higher than family support.16 It may be because patients with OHS place greater emphasis on personal self-esteem, preferring to confide in peers rather than family members. Among peers, they find mutual comfort, encouragement, and shared experiences. Therefore, healthcare providers should strengthen peer support pathways. While promoting offline peer support, they should actively build online platforms to establish “virtual peer” support channels, creating a more open and diverse social support network for these patients.
Enhancing Rehabilitation Motivation to Boost Engagement Among Patients with OHS Undergoing Weight-Loss Surgery, Thereby Improving Ventilator Compliance
Motivation refers to the brain activity process that stimulates and guides an individual’s behavior. Rehabilitation motivation serves as the core driver for patients with OHS using non-invasive ventilation, enhancing adherence to obesity-related treatment modalities.17 This study found that although patients are not consciously aware of wearing a respirator and do not understand the benefits of wearing it, they will actively cooperate with medical staff to persist in wearing the respirator out of motivation for rehabilitation (P5), Consistent with the findings of Alencar et al.17 It may be that having a motivation encourages patients to take further action. In order to quickly get rid of their disease condition and achieve a higher quality of life, they choose surgery despite years of ignoring OHS, hoping to extend their lifespan. It is suggested that clinical healthcare personnel, when developing educational guidance, can focus on the positive effects of wearing a non-invasive ventilator and postoperative rehabilitation, in order to enhance patients’ motivation for recovery and thereby improve patients’ compliance with wearing the non-invasive ventilator before surgery.
Stimulate Positive Feedback Perception in Patients with OHS to Enhance Weight Loss Metabolism and Increase Their Motivation to NIPPV
The perception of positive feedback can give patients enough motivation. This study found that most patients with OHS who Positive pressure ventilation for respiratory support before surgery could perceive positive feedback from wearing the ventilator. The physical benefits in turn motivated patients to experience a sense of accomplishment, forming a virtuous cycle that increased their willingness to wear the ventilator. Related research also indicates that positive feedback has a motivating effect on patients.18 This may be due to the fact that patients have personally experienced positive results; firsthand comparisons provide a more intuitive perspective and are more likely to motivate them. It is recommended that clinical healthcare providers develop self-management record cards for patients with OHS. By documenting and tracking the actual duration of NIPPV, physical and mental status, and changes in symptoms (such as sleep duration and the number of times the patient wakes up gasping for air), and providing regular feedback on treatment outcomes, this approach helps patients intuitively perceive the positive effects of NIPPV, reinforces their understanding of the treatment’s value, and better helps patients with OHS gain confidence and motivation after using the device, thereby increasing their willingness to use it.
Improve the Comfort of NIPPV, Alleviate Patients’ Physical Discomfort, and Enhance Compliance with Noninvasive Ventilation Therapy
Ability refers to the relevant knowledge, skills, health literacy, and other factors that an individual possesses to guide behavior in participating in related activities. This studies have shown that adherence among patients with OHS is low, consistent with the findings of a meta-analysis by Luo Ying et al19 The physical discomfort experienced by patients is a major factor hindering their use of non-invasive ventilators prior to surgery.20 This may be related to symptoms such as breath-holding, stuffiness, and mask pressure experienced by some patients, as well as their doubts and uncertainty regarding the effectiveness of NIPPV.21 Therefore, to address facial pressure and heat issues, wide-brimmed masks or breathable materials suitable for obese patients can be selected,22 and pressure-relieving pads can be used to protect pressure points. For respiratory resistance issues, progressive pressure adjustment (starting at low pressure and gradually increasing to the target value) can be employed to help patients adapt to the airflow rhythm. In addition, targeted health guidance can be provided. On one hand, explain to patients the reasons for experiencing breathlessness and uncoordinated breathing, instruct them on how to alleviate symptoms, and demonstrate the proper way to breathe and precautions when NIPPV. On the other hand, actively offer psychological support to patients, enhance their ability to cope with the distress of physical symptoms, and increase their willingness to use the non-invasive ventilator.
Correct Patients’ Misconceptions About NIPPV and Help Them Overcome Fatigue, Anxiety, and Feelings of Shame Associated with Wearing a Ventilator
The good cognition ability possessed by the patient can motivate the individual to initiate behavior. The results of this study indicate that 4 out of 13 participants lacked a positive perception of preoperative NIPPV, some patients in the early stages of treatment were unaware of the benefits of preoperative NIPPV and did not take it seriously,23 which is consistent with the findings of Wu24 et al The primary reason lies in patients’ current focus on surgical success rates and outcomes, as well as the surgeon’s technical proficiency. They believe surgical success alone suffices, unaware of the impact of low oxygen saturation on surgical factors. Some patients also recognize that NIPPV can effectively alleviate fatigue. Therefore, healthcare providers should provide relevant exercise plans and guidance to patients as early as possible. Knowledge about non-invasive ventilator use can be disseminated through face-to-face educational lectures or digital means such as video conferences and online platforms. In addition, this study also revealed that some patients experienced anxiety, fatigue, and feelings of shame regarding the preoperative use of non-invasive ventilators, leading them to adopt an avoidance attitude. Research indicates that cognitive interventions can effectively alleviate feelings of fatigue and shame.25,26 Therefore, clinicians need to understand the factors influencing patients’ ability to use non-invasive ventilators and pay attention to their psychological state. Cognitive therapy can be employed to correct patients’ misconceptions regarding the use of non-invasive ventilators, emphasizing the importance and necessity of such devices for patients with OHS. This approach aims to enhance patient motivation, help them overcome psychological barriers to the greatest extent possible, and boost their confidence.
Limitations
This study is a qualitative study. The study population consisted of representative individuals. The study design was single-center, with a small sample size, and all participants were from the same hospital. At the same time, Our sample was predominantly male, which, while consistent with the higher prevalence of OHS in men, may mean that gender-specific barriers or facilitators were not fully captured. Due to differences in cultural background, this may have limited the richness and generalizability of the findings; therefore, the generalizability of the results may be affected to some extent. Additionally, there is a lack of objective compliance data. In the future, we will aim for more balanced gender representationbuilding on this foundation, we plan to integrate quantitative research and conduct multicenter studies across different regions and cultural contexts to further explore the factors influencing the use of non-invasive ventilators by patients with OHS.
Conclusions
Based on the COM-B model, this study conducted semi-structured in-depth interviews with 13 patients with OHS who were prescribed NIPPV prior to bariatric surgery. The study aimed to identify the factors promoting and hindering NIPPV use, providing guidance for improving patient compliance with preoperative NIPPV and laying the groundwork for future empirical research. This study found that NIPPV in patients with OHS prior to bariatric surgery is influenced by multiple factors. This suggests that healthcare professionals should reinforce the facilitating factors, actively enhance their professional skills, pay attention to patients’ needs, provide support, and fully mobilize their motivation. Clinicians may consider brief family-inclusive training sessions during NIPPV initiation to address practical support gaps. At the same time, attention should be paid to the barriers to NIPPV therapy. This involves correcting behavioral and cognitive biases, eliminating psychological resistance and social prejudice, improving physical comfort, and motivating rehabilitation to stimulate patient willingness.
Ethical Approval
The procedures of this study were reviewed and approved by Ethics Committee of Shanxi Bethune Hospital. The participation was voluntary; the informed consent, including the permission to publish the results of the research, was obtained. All data used in this research manuscript were obtained legally in accordance with the Protocol on Access to Genetic Resources and the Fair and Equitable Sharing of Benefits Arising from Their Utilization (Nagoya Protocol). This study was approved by the Ethics Committee of Shanxi Bethune Hospital on July 24, 2024, with document number YXLL-2024-134. All participants were informed of the study’s purpose and provided verbal consent prior to interviews, the verbal informed consent process was acceptable and approved by the Ethics Committee of Shanxi Bethune Hospital. To ensure confidentiality, all interview data, related descriptions, and documentation were stored on password-protected computers, with backup files kept on a secured portable hard drive.
Acknowledgments
All the authors wish to thank all of the participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Shanxi Bethune Hospital Nursing Research Fund (2023YH25).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Swinburn BA, Kraak VI, Allender S, et al. The global syndemic of obesity, undernutrition, and climate change: the lancet commission report. Lancet. 2019;393:791–13. doi:10.1016/S0140-6736(18)32822-8
2. Mokhlesi B, Masa JF, Brozek JL, et al. Evaluation and management of obesity hypoventilation syndrome. an official American thoracic society clinical practice guideline. Am J Respir Crit Care Med;2019. e6–e24. doi:10.1164/rccm.201905-1071ST
3. Borel JC, Guerber F, Jullian-Desayes I, et al. Prevalence of obesity hypoventilation syndrome in ambulatory obese patients attending pathology laboratories. Respirology. 2017;22:1190–1198. doi:10.1111/resp.13051
4. Chau EHL, Lam D, Wong J, et al. Obesity hypoventilation syndrome: A review of epidemiology, pathophysiology, and perioperative considerations. Anesthesiology. 2012;117:188–205. doi:10.1097/ALN.0b013e31825add60
5. Mokhlesi B. Obesity hypoventilation syndrome: A state-of-the art review. Respir Care. 2010;55:1347–1362. doi:10.4187/respcare.10551347
6. Jennum P, Kjellberg J. Health, social and economical consequences of sleep-disordered breathing: a controlled national study. Thorax. 2011;66:560–566. doi:10.1136/thx.2010.143958
7. Kakazu MT, Soghier I, Afshar M, et al. Weight loss interventions as treatment of obesity hypoventilation syndrome. A systematic review. Ann Am Thorac Soc. 2020;17:492–502. doi:10.1513/AnnalsATS.201907-554OC
8. Niu X, Zhang Y, Feng N. Perioperative airway protection strategies for morbidly obese patients undergoing laparoscopic gastric volume reduction surgery. J Laparoscopic Sur. 2024:73–78.
9. Ma S, Yang C, Wang B, et al. Study on the efficacy and influencing factors of weight-loss metabolic surgery in improving obesity hypoventilation syndrome. Abdom Surg. 2024:319–324.
10. Yang C, Wang W, Huo H, et al. Guideline introduction and understanding for diagnosis and treatment of obstructive sleep apnea in the perioperative period of bariatric metabolic surgery. Chin J Obes Metab Dis. 2018:62–64.
11. Gervès-Pinquié C, Bailly S, Goupil F, et al. Positive airway pressure adherence, mortality, and cardiovascular events in patients with sleep apnea. Am J Respir Crit Care Med. 2022;206:1393–1404.
12. Terri E. Assessing and managing nonadherence with continuous positive airway pressure (CPAP) for adults with obstructive sleep apnea. 2025[updated September 24, 2025]. Available from: https://www.uptodate.com/contents/assessing-and-managing-nonadherence-with-continuous-positive-airway-pressure-cpap-for-adults-with-obstructive-sleep-apnea.
13. Michie S, van Stralen MM, West R. The behaviour change wheel: A new method for characterising and designing be haviour change interventions. Implement Sci. 2011;6:42. doi:10.1186/1748-5908-6-42
14. Bengtsson C, Grote L, Ljunggren M, Ekström M, Palm A. Nasal polyposis is a risk factor for nonadherence to CPAP treatment in sleep apnea: the population-based discovery study. J Clin Sleep Med. 2023;19:573–579. doi:10.5664/jcsm.10390
15. Cui T, Lui J, Chen B, et al. Knowledge, attitudes, practices, and burnout related to respiratory support among healthcare professionals in central China: a structural equation modeling study. BMC Med Educ. 2025;25:735. doi:10.1186/s12909-025-07302-8
16. Jian L. Study on the intervention of narrative companion support nursing combined with precision nursing on stigma and social adaptability of colorectal cancer stoma patients. Prim Med Forum. 2026;30(12):120–122.
17. Alencar M, Sauls R, Johnson K, et al. Health and wellness coaching can improve usage of positive airway pressure therapy in participants with obstructive sleep apnea and obesity. Am J Lifestyle Med. 2024;19:899–907. doi:10.1177/15598276241244719
18. Xiao R, Zhou Y. A qualitative study on factors promoting and hindering physical activity participation among pregnant women with gestational diabetes mellitus during pregnancy. Chin J Nurs. 2025;1683–1689.
19. Luo Y, Ning L, Shi F, et al. A meta-analysis of adherence to continuous positive airway pressure therapy and its influencing factors in patients with obstructive sleep apnea. Mod Med. 2024;52(9):1434.
20. Zhou X. The effect of full-course seamless penetration nursing on the adverse psychological state and treatment compliance of patients using non-invasive ventilators for the first time. Prim Med Forum. 2024;28(08):129–133.
21. Fujita Y, Yamauchi M, Hamada E, et al. Evaluation of continuous positive airway pressure adherence and its contributing factors. Respir Med. 2024;234:107815. doi:10.1016/j.rmed.2024.107815
22. Hu Z. Nursing progress of nasal and facial pressure injuries in patients undergoing non-invasive positive pressure ventilation. Contemp Nurse. 2021;28(05):8–9.
23. Briand R, Lebouvier T, Lanvin L, et al. Continuous positive airway pressure compliance in patients with mild cognitive impairment. Sleep Breath. 2024;28:1165–1172. doi:10.1007/s11325-024-02995-5
24. Wu W, Fang L, Qian Y, et al. The impact of a multidisciplinary collaborative health management program on out-of-hospital noninvasive ventilator support for obese patients with obstructive sleep apnea-hypopnea syndrome. Res Chin Foreign Med. 2026;5(06):35–37.
25. Zhao X, Wang X, Li Z. Effects of flaxseed on lipid metabolism, inflammation, and fatigue in overweight and obese children. Chin J Food Hyg. 2024;260–266.
26. Ramsamy G, Mosbah H, Faure JP, Plault V, Albouy M, Esnard C. How to reduce the adverse effects of weight stigma on the quality of life: a preferred reported items for systematic reviews and meta-analyses (PRISMA). Front Psychol. 2024;15:1421609. doi:10.3389/fpsyg.2024.1421609
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
A Qualitative Study on Barriers and Facilitators to Postpartum Cardiovascular Disease Risk Screening in Women with Hypertensive Disorders of Pregnancy: Perspectives from Patients and Healthcare Providers
Zhang Y, Jiang Y, Sun S, Jiang L, Yu W, Hu J, Ji X
International Journal of Women's Health 2025, 17:5329-5342
Published Date: 11 December 2025
Healthcare Professionals’ Perspectives on Perinatal Mental Health Care in the United Arab Emirates: A Qualitative Study of Barriers and Facilitators at the Patient, Family, and Societal Levels
ElKhalil R, Bayoumi R, Menon P, Qurniyawati E, Ahmed LA, Al-Rifai RH, Masuadi E, Elbarazi I
International Journal of Women's Health 2026, 18:597512
Published Date: 11 June 2026