")
Back to Journals » Patient Preference and Adherence » Volume 17
Barrier Factors of Adherence to Dupilumab Self-Injection for Severe Allergic Disease: A Non-Interventional Open-Label Study
Authors Hosoya K , Komachi T, Masaki K , Suzaki I , Saeki H , Kanda N , Nozaki M, Kamide Y, Matsuwaki Y, Kobayashi Y, Ogino E, Osada SI , Usukura N, Kurumagawa T, Ninomia J, Asako M, Nakamoto K, Yokoi H, Ohyama M , Tanese K, Kanzaki S, Fukunaga K, Ebisawa M, Okubo K
Received 7 October 2022
Accepted for publication 10 March 2023
Published 27 March 2023 Volume 2023:17 Pages 861—872
DOI https://doi.org/10.2147/PPA.S389865
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Kei Hosoya,1 Taro Komachi,2,* Katsunori Masaki,3,* Isao Suzaki,4 Hidehisa Saeki,5 Naoko Kanda,6 Makoto Nozaki,7 Yosuke Kamide,8 Yoshinori Matsuwaki,9 Yoshiki Kobayashi,10 Eriko Ogino,11 Shin-Ichi Osada,12 Norihiro Usukura,13 Toshikazu Kurumagawa,14 Junya Ninomia,15 Mikiya Asako,16 Keitaro Nakamoto,17 Hidenori Yokoi,18 Manabu Ohyama,19 Keiji Tanese,3 Sho Kanzaki,3 Koichi Fukunaga,3 Motohiro Ebisawa,8 Kimihiro Okubo13
1Nippon Medical School, Musashi Kosugi Hospital, Kanagawa, Japan; 2Department of Otolaryngology, Nippon Medical School, Chiba Hokusoh Hospital, Inzai, Chiba, Japan; 3Keio Allergy Center, Keio University Hospital, Tokyo, Japan; 4Department of Otorhinolaryngology, Head and Neck Surgery, Showa University, School of Medicine, Tokyo, Japan; 5Department of Dermatology, Nihon Medical School, Tokyo, Japan; 6Department of Dermatology, Nippon Medical School, Chiba Hokusoh Hospital, Inzai, Chiba, Japan; 7Wakaba-Hifuka Clinic, Tokyo, Japan; 8National Hospital Organization Sagamihara National Hospital, Clinical Research Center for Allergy and Rheumatology, Kanagawa, Japan; 9Matsuwaki Clinic Shinagawa, Tokyo, Japan; 10Allergy Center, Kansai Medical University, Hirakata, Japan; 11Kyoto Nose and Allergy Clinic, Kyoto, Japan; 12Department of Dermatology, Nippon Medical School Tama Nagayama Hospital, Tokyo, Japan; 13Department of Otolaryngology, Head and Neck Surgery, Nippon Medical School Hospital, Tokyo, Japan; 14Minamiosawa Medical Plaza, Tokyo, Japan; 15Nagase Clinic of Dermatology, Tokyo, Japan; 16Department of Otolaryngology, Head and Neck Surgery, Kansai Medical University, Osaka, Japan; 17Department of Respiratory Medicine, Kyorin University Faculty of Medicine, Tokyo, Japan; 18Department of Otolaryngology, Head and Neck Surgery, Kyorin University Faculty of Medicine, Tokyo, Japan; 19Department of Dermatology, Kyorin University Faculty of Medicine, Tokyo, Japan
*These authors contributed equally to this work
Correspondence: Kei Hosoya, Nippon Medical School, Musashi Kosugi Hospital, 1-383 Kosugimachi, Nakahara-ku, Kawasaki, Kanagawa, 211-8533, Japan, Tel +81-44-733-5181, Fax +81-44-711-8713, Email [email protected]
Purpose: The status of dupilumab self-injection at home is not well understood. We therefore aimed to identify the barriers to adherence to dupilumab self-injection.
Patients and Methods: This non-interventional open-label study was conducted between March 2021 and July 2021. Patients with atopic dermatitis, bronchial asthma, and chronic rhinosinusitis with nasal polyps receiving dupilumab, from 15 sites, were requested to complete a self-administered questionnaire regarding the frequency and effectiveness of dosing as well as their use and satisfaction with dupilumab. Barriers to adherence were assessed using the Adherence Starts with Knowledge-12.
Results: We included 331 patients who used dupilumab for atopic dermatitis (n = 164), chronic rhinosinusitis with nasal polyps (n = 102), and bronchial asthma (n = 65). The median efficacy of dupilumab scored 9.3 on the visual analog scale. Overall, 85.5% of the patients self-injected dupilumab, and 70.7% perfectly complied with the established injection dates. The pre-filled pen was significantly superior to the conventional syringe in terms of usability, operability, ease of pushing the plunger, and patient satisfaction. However, the pre-filled pen caused more pain during self-injection than did the syringe. Multivariate logistic regression analysis showed that adherence decreased with longer dupilumab treatment duration (p = 0.017) and was not associated with age, sex, underlying disease, or device type. There was a difference in responses related to “inconvenience/forgetfulness” between the good and poor adherence groups.
Conclusion: The pre-filled dupilumab pen was superior to the syringe in terms of usability, operability, ease of pushing the plunger, and satisfaction. Repetitive instructions are recommended for preventing poor adherence to dupilumab self-injection.
Keywords: atopic dermatitis, biologics, bronchial asthma, chronic rhinosinusitis
Introduction
Allergic diseases have become a major health problem in modern society, with an increasing incidence worldwide because of considerable changes in sanitation, lifestyle, and diet.1,2 The global incidence rates of atopic dermatitis (AD), adult bronchial asthma (BA), and chronic rhinosinusitis are approximately 3%,3 15%,4 and 12%,5 respectively. In addition to frequent hospitalizations and unscheduled hospital visits due to disease exacerbations, people with allergic diseases are forced to bear a substantial economic burden, reduced quality of life due to symptoms, time loss and medical expenses incurred by regular hospital visits, and reduced work productivity.6 Although treatments for allergic diseases have improved over time, numerous patients remain refractory to treatment. In such instances, biologics have been reported to be effective7–9 and can be considered an innovative treatment method.6
Symptomatic management of allergic diseases often requires not only oral medications, but also a combination of oral medications and topical medications (for AD), inhalants (for BA), nasal sprays (for chronic rhinosinusitis), and other local anti-allergy medications. However, topical medications are more laborious to administer than oral medications, and patients may experience difficulty in following instructions, leading to poor adherence. In a study by Storm et al, one-third of patients with psoriasis and eczema attending a dermatology clinic did not have their prescriptions refilled.10 On the other hand, in a study conducted by Braido et al, approximately half of the patients with BA did not use their inhalers correctly.11 Furthermore, because poor adherence greatly diminishes treatment effectiveness,12,13 improving adherence is important for preventing exacerbation and managing symptoms.
The Adherence Starts with Knowledge-12 (ASK-12) is a 12-item questionnaire designed to assess patient-specific behaviors and barriers related to treatment adherence.14 The ASK-12 is a shortened version of the ASK-20, with fewer questions to increase ease of use in a clinical setting. In addition, questions specific to oral medications have been eliminated and the shortened version can be used for various drug dosage types, including topical, inhaled, nasal, and injectable medications.15
Additionally, a patient’s affinity with the administration device, such as satisfaction with inhalers for BA, affects adherence.16 Pain at the site of self-injection plays an important role in adherence to treatments involving self-administration of injectable medications, such as in diabetes and rheumatoid arthritis.17,18 Home self-injection is now also possible for allergic diseases, with dupilumab for AD, BA, and chronic rhinosinusitis with nasal polyps (CRSwNPs); omalizumab for BA and chronic urticaria; and mepolizumab for BA and eosinophilic granulomatosis with polyangiitis.
There are three methods for dupilumab administration: self-injection syringe, syringe with an aid device, and pre-filled pen (Figure 1).19 The syringe and pre-filled pen are filled with 300 mg (2 mL) of dupilumab and utilize a 27-gauge needle measuring 13 mm. The needle of the pre-filled pen is inserted subcutaneously at a depth of 6 mm. With the pre-filled pen, dupilumab is injected at a fixed rate when the button is pressed. The aid device secures the injection site to the body and conceals the needle.
 |
Figure 1 Injection devices. (A): Pre-filled syringe; (B): Aid device; (C) Pre-filled pen. |
Few real-world reports have been published on the impact of the device and disease characteristics on adherence to dupilumab self-injection. Thus, this study aimed to identify barriers to adherence by using the ASK-12 and an original questionnaire for investigating adherence to and satisfaction with self-injection of dupilumab.
Materials and Methods
Ethics Statements
This study was performed in accordance with the principles stated in the Declaration of Helsinki and was approved by the Nippon Medical School Tama Nagayama Hospital Ethical Review Committee (ethical review approval number: 681), and permission to conduct the study was obtained from each participating institution. Informed consent was obtained from each participant enrolled in this study.
Study Design and Patients
This non-interventional open-label study was conducted between March 2021 and July 2021 in 10 hospitals (> 200 beds) and five clinics of cooperating facilities. Patients with AD, BA, and CRSwNPs attending these facilities, who used dupilumab during the study period according to the Japanese guidelines for their respective diseases,20,21 who were aged 12 years or older, and who answered the Japanese version of the ASK-12 as well as 20 additional questions were included in this study. Patients with missing answers to any question were excluded, and those who could not read the questionnaires (eg, foreigners) were not asked to participate.
Questionnaires
The self-reported ASK-12 questionnaire consisted of queries regarding “inconvenience/forgetfulness” (Q1–3), “health beliefs” (Q4–7), and “behavior” (Q8–12). Answers were scored using a five-point Likert scale. Scores for Q1–7 ranged from 1, indicating “strongly disagree”, to 5, indicating “strongly agree.” For Q8–12, the scale for frequency ranged from 1 point for “never”, to 5 points, for “in the last week.” The total ASK-12 score ranged from 12 to 60 points. The 20 additional questions consisted of five categories: (1) frequency and effectiveness of dupilumab administration; (2) history of self-injection; (3) whether patients self-injected, how they self-injected, if they delayed self-injection, and the scheduling of self-injection; (4) self-injection devices used and patients’ satisfaction with them; and (5) open-ended statements about dissatisfaction with the devices and areas of improvement. Questions about the self-injection devices were asked using a visual analog scale (VAS; score range, 0–10) for operability, ease of pushing the plunger, pain, and fear of self-injection using the device. Regarding the device size and ease of gripping, both scores were set on a 5-point scale, from 1 for “very small” and “very hard to grip”, 3 for “just right”, and 5 for “very large” and “very easy to grip.” For usability and satisfaction, a 5-point scale was also set, where 1 indicated “very dissatisfied” and 5 indicated “very satisfied.”
Statistical Analysis
Data are presented as median and interquartile range. The Mann–Whitney U-test was used to compare continuous data between two groups, whereas the Kruskal–Wallis test was used to compare data among three groups. Post hoc Bonferroni adjustment was applied. Fisher’s exact and chi-square tests were used to compare categorical data between groups. Spearman’s rank correlation coefficient was used to assess correlations between the VAS score and duration of treatment.
Multiple logistic regression analysis was performed using SPSS Statistics for Mac OS, version 27.0 (IBM Corporation, Armonk, NY, USA). A p-value < 0.05 (two-tailed) was set as the level for statistical significance.
Results
In this study, 375 patients were enrolled, and 331 patients (164 with AD, 65 with BA, and 102 with CRSwNPs) were analyzed after excluding 44 patients with missing information (Table 1). Overall, 38.4% of the enrolled patients were female, and the median age was 47.0 years. In patients with AD, BA, and CRSwNPs, the median subjective efficacies of dupilumab, expressed as VAS scores, were 9.4, 9.1, and 9.2, respectively, which were all favorable, without significant differences among diseases. The median duration of dupilumab use was 364.0 days, and there was a slight correlation between duration of dupilumab use and its efficacy (p = 0.0271, r = 0.1215) (Figure 2). The injection frequency was significantly higher in the AD than in the BA group (p = 0.0037). The proportion of patients who self-injected was 13.3%. The median total score on each ASK-12 was 30.0 for all three diseases, with no significant differences between diseases (p = 0.6184).
 |
Table 1 Patient Characteristics |
 |
Figure 2 Correlation of visual analogue scale (VAS) score with the efficacy and duration of dupilumab use. p = 0.0271, r = 0.1215. |
The background characteristics of patients who self-injected dupilumab are shown in Table 2. Self-injection was performed by 85.5% of patients. Among patients with a history of self-injection, 97.7% chose or continued to self-inject dupilumab. There was no relationship between age and the choice or continuation to self-inject. Overall, 70.7% of the patients were adherent (never forgot an injection). The adherence rate in the AD group was 59.4%, which was significantly lower than that in the other two groups (p = 0.0002) (Table 2). Injection was delayed for < 2 weeks in 95.2% of patients (n = 80), 2–4 weeks in 3.6% (n = 3), and > 2 months in 1.2% (n = 1). Worsening of symptoms due to delayed injection occurred in 11.9% (< 2 weeks: 8 AD patients; 1 BA patient; 2–4 weeks: 1 CRSwNP patient) and became severe in 1.2% (> 2 months: 1 AD patient) of the participants (data not shown).
 |
Table 2 Characteristics of Patients Who Self-Inject Dupilumab |
Figure 3 shows the preferred injection sites for dupilumab, the type of device used, and the number of days that the device was used. Multiple responses were allowed for the injection site. The abdomen was the most common injection site (81.7%, 254/311), followed by the thigh (16.1%, 50/311) (Figure 3A and B). Overall, the pre-filled pen was the most used device (61.5%, 174/283). The syringe was most frequently used in the AD group (47.1%, 65 cases), whereas the pre-filled pen was most frequently used in the BA group (44.9%, 62 cases) and CRSwNP group (78.7%, 70 cases), showing significant differences in terms of the type of instrument used and disease (p < 0.001, chi-square test; data not shown). The median duration of dupilumab use was significantly shorter in patients using the pre-filled pen than in those using other forms (272.5 days; vs syringe, p < 0.0001; vs syringe with an aid device, p = 0.0006) (Figure 3C).
 |
Figure 3 Graphs showing (A) self-injection site, (B) injection device, and (C) duration of dupilumab use. **** p < 0.0001, ***p = 0.0006. |
As shown in Figure 4, patients were asked to rate the operability of self-injection, ease of pushing the plunger, pain, and fear of self-injection using a VAS. The pre-filled pen was significantly superior to the syringe in terms of ease of operability (9.1 vs 8.0, p < 0.0001) and pushing the plunger (9.1 vs 7.0, p < 0.0001); however, it was significantly inferior in terms of pain (5.1 vs 3.4, p = 0.0193). Among participants who self-injected, 24.4% (69/283) completed the free text field. Of these participants, 30.4% (21/69) stated that the rapid injection speed caused the pain associated with using the pre-filled pen (data not shown). There were no significant differences in terms of the device’s size or ease of gripping. The pre-filled pen was significantly superior to the syringe in terms of usability (4.0 [4.0] vs 4.0 [3.0–4.0], p = 0.0003) and satisfaction (4.0 [4.0] vs 4.0 [3.0–4.0], p = 0.0001) (Figure 5).
 |
Figure 4 Evaluation of each device. (A) Operability; (B) Ease of pushing the plunger; (C) Pain; (D): Fear of self-injection. The pre-filled pen fared significantly better in terms of operability and ease of pushing the plunger, but fared significantly worse in terms of pain. **** p < 0.0001, ***p < 0.001, *p = 0.0193. |
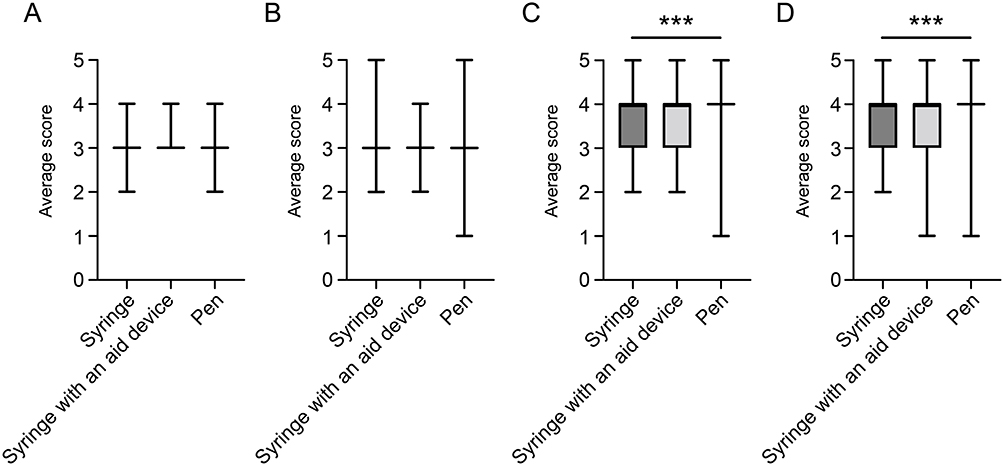 |
Figure 5 Evaluation of each device. (A) Size; (B) Grip; (C) Usability; (D) Patient satisfaction. The pre-filled pen fared significantly better in terms of usability and patient satisfaction. (C) ***p = 0.0003, (D) ***p = 0.0001. |
As shown in Table 3 and Table 4, the ASK-12 scores were analyzed separately for the good adherence group (200 patients), who did not miss a dose, and for the poor adherence group (83 patients), who missed or delayed a dose at least once. The total ASK-12 score was significantly higher in the poor adherence group than in the good adherence group (p < 0.0001) (Table 3). Significant differences in responses to Q1, 2, 3, 8, and 9 were found between the groups. Further comparison of clinical characteristics revealed that the poor adherence group included younger participants (43.0 vs 47.0 years, p = 0.0047), used dupilumab for a longer duration (585.0 vs 319.5 days, p < 0.0001), more frequently used a syringe (syringe, 41.0% vs syringe with an aid device, 9.6% vs pre-filled pen, 49.4%, p = 0.0267), and more commonly included patients with AD (AD group, 67.5% vs BA group, 15.7% vs CRSwNP group, 16.9%, p = 0.0002) (Table 4). The VAS scores for pain related to self-injection did not differ significantly between the groups.
 |
Table 3 The Scores of ASK-12 Items in Patients with Good or Poor Dupilumab Adherence |
 |
Table 4 Comparison of Clinical Characteristics Between the Good and Poor Adherence Groups |
Multiple logistic regression analysis was performed for age, sex, duration of dupilumab use, disease, and type of device used, to explore factors associated with non-adherence (Table 5). The use of an aid device was excluded from the analysis due to the small number of patients who used such devices. The analysis showed that a longer duration of dupilumab use was associated with poor adherence (odds ratio, 1.002; 95% confidence interval: 1.000–1.004, p = 0.017). Patients also managed their injection schedules in various ways, including using smartphones and home and work calendars (Figure 6A). The good adherence group used multiple, rather than single methods to manage their schedules (p = 0.0015) (Figure 6B).
 |
Table 5 Multivariate Logistic Regression Analyses of Factors for Poor Adherence |
 |
Figure 6 Schedule management for self-injection. (A) Smartphones and calendars at home or work were often used to manage self-injection schedules. (B) The poor adherence group used one method for managing self-injection, whereas the good adherence group used multiple management methods (**p = 0.0015). |
Discussion
Patients with AD, BA, and CRSwNPs reported therapeutic efficacy with dupilumab. The injection intervals were longest in the AD group and shortest in the BA group. The pre-filled pen was most frequently used (61.5%). Although the pre-filled pen caused more pain than the syringe-type device, it was superior in terms of usability and satisfaction. In the good adherence group, 70.7% of patients self-injected without missing a dose, showed different responses to the “inconvenience/forgetfulness” questions in the ASK-12, and used other methods by which they managed their injection schedules, as compared with patients in the poor adherence group. Multivariate logistic regression analysis illustrated that long-term use of dupilumab was associated with decreased adherence; however, decreased adherence was not associated with age, sex, underlying disease, or type of device used.
Dupilumab is a biological agent that inhibits interleukin (IL)-4 and IL-13, using an IL-4 receptor alpha antibody, and has been reported to improve symptoms and decrease the frequency of exacerbations in patients with severe AD, BA, and CRSwNP.7–9 In Japan, healthcare insurance has covered dupilumab use since April 2018 for AD, and since March 2019 for BA, with self-injection devices and corresponding aid devices available since May 2019. Since March 2020, dupilumab has been accepted as indicated for CRSwNPs, and in November 2020, the pre-filled pen became available as an alternative to the syringe-type device. In this study, patients with AD, BA, and CRSwNP did not significantly differ in their assessment of their treatment responses to dupilumab, with a high median VAS score of 9.3 for the three diseases. The r-value for the correlation between the number of days of treatment and the rated treatment effect was 0.1215, indicating that patients were aware of the effect of dupilumab from the beginning of its use, and that awareness of the effect slowly increased along with continued treatment. For AD and BA, the dosing interval for dupilumab is 2 weeks. However, we found that dosing intervals were extended in clinical practice, particularly in AD cases. The high cost of dupilumab may cause patients to extend dosing intervals as long as symptoms do not flare. A prolonged dosing interval is associated with the formation of neutralizing antibodies; therefore, patients should avoid extending the dosing interval at their discretion, without the agreement of their physicians.22
Overall, 61.5% of patients used the pre-filled pen, which was reportedly more painful to use than the syringe. However, it was superior to the syringe in terms of ease of operation, pushing the plunger, and usability. There was no significant difference in the fear of injection among users of a syringe with a visible needle during injection, a syringe with an aid device that conceals the needle, and a pre-filled pen with no visible needle. This result suggests that the pain during injection is not psychological. A syringe allows the users to adjust the injection rate by themselves, whereas the pre-filled pen uses a constant injection rate, and 30.4% of the respondents noted in the free text that the rapid injection rate was the cause of the pain following injection. Since there is currently only one type of pre-filled dupilumab pen, we believe that a type with a slower speed should be manufactured and its use compared.
Tischer et al reported that ease of grip correlated with ease of injection.23 Although there was no difference in the device size and ease of gripping in our study, the pre-filled pen was the most satisfactory according to the participants, because of its operability and ease of pushing the plunger. In insulin therapy for diabetes, use of a pre-filled pen was reported to improve adherence and thus to provide better glycemic control than a syringe.24 In patients with BA, patient-preferred inhalers are recommended when selecting a device.25 Hence, we believe that patients should be able to choose whether the injection device is in the form of a pen or syringe.
In this real-world study, 70.1% of the participants were in the good adherence group for dupilumab use. Elsewhere, consistent use of dupilumab for AD at 12 months was reported to be 77.3%.26 Adherence to omalizumab for BA treatment was previously reported to range from 47% to 91%.12,27–29 In a randomized controlled trial and field study conducted by Caminati et al, the dropout rate for omalizumab for BA was examined and found to be up to 45.5%, with a lack of therapeutic efficacy being the main reason for treatment discontinuation.30 Our validation revealed that patients treated with dupilumab experienced high treatment efficacy, which we believe contributed to their high adherence.
The total ASK-12 score was significantly higher in the poor adherence group than in the good adherence group, particularly for Q1–3, which are related to “inconvenience/forgetfulness.” It was also clear that patients with good adherence managed their injection schedules through multiple ways. We believe that confirming and suggesting methods for schedule management during outpatient care may improve adherence. Moreover, our study revealed that pain during self-injection did not play a role in adherence. However, a previous study on adherence in patients with rheumatoid arthritis reported that injection-site pain and skin perception affected patient adherence.31 In contrast, in this study, pain related to injection with the pre-filled pen did not appear to have an impact on adherence. Because comparison of the good and poor adherence groups showed that multiple factors, such as age, duration of dupilumab use, syringe use, and prevalence of patients with AD, were involved, multiple logistic regression analysis was conducted to explore factors related to non-adherence, in addition to analyzing the risk factors among these multiple factors. Dupilumab was approved for different diseases at different times, and the pre-filled pen was only adopted later on. The results showed that the duration of dupilumab use was a factor in poor adherence. Therefore, similar to the inhalation instructions given to BA patients, giving patients regular instructions and reminders of dupilumab self-injection by physicians and pharmacists are important.32,33
Age and sex were not factors associated with poor adherence in this study; however, a decrease in adherence among young-onset patients has been reported for inhaled steroids for severe BA and for self-injection for diabetes.16,34,35 Therefore, when examining young-onset patients, it is advisable to consider that adherence may decrease in future.
This study had several limitations. First, the epidemiological incidence of each disease and the respective disease rates in this study did not match. This may be due to the proportion of patients with severe disease and the fact that other biologics have been marketed for BA prior to dupilumab. Second, the questionnaire was self-administered; therefore, it was unclear whether the prescribing physician instructed the patients to extend the dosing interval, permitted the extension after patient request, or if it was done at the discretion of the patient. Moreover, the results of the self-administered questionnaire lacked objective evaluation. Finally, data in this study were obtained from patients who felt that dupilumab was effective and continued to use it. Previous studies indicated that most patients improved within <1 to 2 months after treatment, but some showed gradual improvement of the disease after this period.7,9,36 Moreover, it is possible that patients in whom dupilumab was not efficient enough were not included in this study. In future, development of injection pens that cause less pain may improve adherence to self-injection, with a reduced patient burden.
Conclusion
In this study, a pre-filled pen was superior to a syringe in terms of usability, operability, ease of pushing the plunger, and patient satisfaction for self-injection of dupilumab for allergic conditions. Furthermore, it is likely that poor adherence to dupilumab self-injection could be prevented by repetition of instructions.
Abbreviations
AD, atopic dermatitis; ASK-12, Adherence Starts with Knowledge-12; BA, bronchial asthma; CRSwNPs, chronic rhinosinusitis with nasal polyps; IL, interleukin; VAS, visual analog scale.
Data Sharing Statement
An anonymized dataset from this trial is available from the corresponding author (email: [email protected]) upon publication. The investigator may only use the data for the purpose outlined in the request, and redistribution of the data is prohibited.
Ethics Approval and Informed Consent
This study was performed in accordance with the principles stated in the Declaration of Helsinki and was approved by the Nippon Medical School Tama Nagayama Hospital Ethical Review committee (Ethical Review Approval No. 681), and permission to conduct the study was obtained from each participating institution. Informed consent was obtained from each patient enrolled in this study.
Acknowledgement
This work was supported by JSPS KAKENHI Grant Number JP19K18820.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval for the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
KH, TKo, KM, IS, HS, NK, MN, YKa, YKo, YM, YH, EO, SO, TKu, KN, HY, NO, KT, SK, KF, ME, and KO received honoraria from Sanofi K.K. KH also reports grants from MEXT KAKENHI Grant. YKa also reports payment for lectures from Sanofi K.K, Glaxo Smith Kline K.K, AstraZeneca K.K. YM also reports personal fees from Olympus, clinical trial funding from Regeneron Pharmaceuticals. EO also reports grants/personal fees from Sanofi K.K, Novartis Pharma K.K, clinical trial funding from Regeneron Pharmaceuticals, GlaxoSmithKline K.K. KN also reports grants/personal fees from Grant-in- Aid for Scientific Research, GSK, AstraZeneca, Sanofi, Novartis, Kyorin Pharmaceutical. ME also reports personal fees from Viatris. MA has been an advisory board member for Sanofi. MO received lecture fees from Sanofi K.K. and Eli Lilly Japan K.K, as well as advisory fees from Eli Lilly Japan K.K. and Pfizer Japan, Inc. The authors report no other conflicts of interest in this work.
References
1. Platts-Mills TAE. The allergy epidemics: 1870–2010. J Allergy Clin Immunol. 2015;136(1):3–13. doi:10.1016/j.jaci.2015.03.048
2. Noval Rivas M, Chatila TA. Regulatory T cells in allergic diseases. J Allergy Clin Immunol. 2016;138(3):639–652. doi:10.1016/j.jaci.2016.06.003
3. Nutten S. Atopic dermatitis: global epidemiology and risk factors. Ann Nutr Metab. 2015;66(suppl 1):8–16. doi:10.1159/000370220
4. Enilari O, Sinha S. The global impact of asthma in adult populations. Ann Glob Health. 2019;85:1. doi:10.5334/aogh.2412
5. DeConde AS, Soler ZM. Chronic rhinosinusitis: epidemiology and burden of disease. Am J Rhinol Allergy. 2016;30(2):134–139. doi:10.2500/ajra.2016.30.4297
6. Sastre J, Dávila I. Dupilumab: a new paradigm for the treatment of allergic diseases. J Investig Allergol Clin Immunol. 2018;28(3):139–150. doi:10.18176/jiaci.0254
7. Bachert C, Han JK, Desrosiers M, et al. Efficacy and safety of dupilumab in patients with severe chronic rhinosinusitis with nasal polyps (Liberty NP SINUS-24 and Liberty NP SINUS-52): results from two multicentre, randomised, double-blind, placebo-controlled, parallel-group Phase 3 trials. Lancet. 2019;394(10209):1638–1650. doi:10.1016/S0140-6736(19)31881-1
8. Paller AS, Bansal A, Simpson EL, et al. Clinically meaningful responses to dupilumab in adolescents with uncontrolled moderate-to-severe atopic dermatitis: post-hoc analyses from a randomized clinical trial. Am J Clin Dermatol. 2020;21(1):119–131. doi:10.1007/s40257-019-00478-y
9. Blauvelt A, de Bruin-Weller M, Gooderham M, et al. Long-term management of moderate-to-severe atopic dermatitis with dupilumab and concomitant topical corticosteroids (Liberty AD Chronos): a 1-year, randomised, double-blinded, placebo-controlled, phase 3 trial. Lancet. 2017;389(10086):2287–2303. doi:10.1016/S0140-6736(17)31191-1
10. Storm A, Andersen SE, Benfeldt E, Serup J. One in 3 prescriptions are never redeemed: primary nonadherence in an outpatient clinic. J Am Acad Dermatol. 2008;59(1):27–33. doi:10.1016/j.jaad.2008.03.045
11. Braido F, Baiardini I, Blasi F, Pawankar R, Canonica GW. Adherence to asthma treatments: “We know, we intend, we advocate”. Curr Opin Allergy Clin Immunol. 2015;15(1):49–55. doi:10.1097/ACI.0000000000000132
12. Campisi R, Crimi C, Intravaia R, et al. Adherence to omalizumab: a multicenter “real-world” study. World Allergy Organ J. 2020;13(2):100103. doi:10.1016/j.waojou.2020.100103
13. Rolnick SJ, Pawloski PA, Hedblom BD, Asche SE, Bruzek RJ. Patient characteristics associated with medication adherence. Clin Med Res. 2013;11(2):54–65. doi:10.3121/cmr.2013.1113
14. Hahn SR, Park J, Skinner EP, et al. Development of the ASK-20 adherence barrier survey. Curr Med Res Opin. 2008;24(7):2127–2138. doi:10.1185/03007990802174769
15. Matza LS, Park J, Coyne KS, Skinner EP, Malley KG, Wolever RQ. Derivation and validation of the ASK-12 adherence barrier survey. Ann Pharmacother. 2009;43(10):1621–1630. doi:10.1345/aph.1M174
16. Plaza V, Giner J, Calle M, et al. Impact of patient satisfaction with his or her inhaler on adherence and asthma control. Allergy Asthma Proc. 2018;39(6):437–444. doi:10.2500/aap.2018.39.4183
17. Peyrot M, Rubin RR, Kruger DF, Travis LB. Correlates of insulin injection omission. Diabetes Care. 2010;33(2):240–245. doi:10.2337/dc09-1348
18. Aronson R. The role of comfort and discomfort in insulin therapy. Diabetes Technol Ther. 2012;14(8):741–747. doi:10.1089/dia.2012.0038
19. Sanofi. [homepage on the Internet (in Japanese)], Available from: https://e-mr.sanofi.co.jp/products/dupixent.
20. Katoh N, Kataoka Y, Saeki H, et al. Efficacy and safety of dupilumab in Japanese adults with moderate-to-severe atopic dermatitis: a subanalysis of three clinical trials. Br J Dermatol. 2020;183(1):39–51. doi:10.1111/bjd.18565
21. Fujieda S, Matsune S, Takeno S, et al. The effect of dupilumab on intractable chronic rhinosinusitis with nasal polyps in Japan. Laryngoscope. 2021;131(6):E1770–E1777. doi:10.1002/lary.29230
22. Worm M, Simpson EL, Thaçi D, et al. Efficacy and safety of multiple dupilumab dose regimens after initial successful treatment in patients with atopic dermatitis: a randomized clinical trial. JAMA Dermatol. 2020;156(2):131–143. doi:10.1001/jamadermatol.2019.3617
23. Tischer B, Mehl A. Patients’ and nurses’ preferences for autoinjectors for rheumatoid arthritis: results of a European survey. Patient Prefer Adherence. 2018;12:1413–1424. doi:10.2147/PPA.S169339
24. Campbell RK. Recommendations for improving adherence to type 2 diabetes mellitus therapy—Focus on optimizing insulin-based therapy. Am J Manag Care. 2012;18:S55–S61.
25. Global Initiative for Asthma. Available from: https://ginasthma.org/.
26. Silverberg JI, Guttman-Yassky E, Gadkari A, et al. Real-world persistence with dupilumab among adults with atopic dermatitis. Ann Allergy Asthma Immunol. 2021;126(1):40–45. doi:10.1016/j.anai.2020.07.026
27. Broder MS, Chang EY, Ory C, Kamath T, Sapra S. Adherence and persistence with omalizumab and fluticasone/salmeterol within a managed care population. Allergy Asthma Proc. 2009;30(2):148–157. doi:10.2500/aap.2009.30.3190
28. Janson SL, Solari PG, Trzaskoma B, Chen H, Haselkorn T, Zazzali JL. Omalizumab adherence in an observational study of patients with moderate to severe allergic asthma. Ann Allergy Asthma Immunol. 2015;114(6):516–521. doi:10.1016/j.anai.2015.04.010
29. Lafeuille MH, Gravel J, Zhang J, Gorsh B, Figliomeni M, Lefebvre P. Association between consistent omalizumab treatment and asthma control. J Allergy Clin Immunol Pract. 2013;1(1):51–57. doi:10.1016/j.jaip.2012.08.006
30. Caminati M, Senna G, Stefanizzi G, et al. Drop-out rate among patients treated with omalizumab for severe asthma: literature review and real-life experience. BMC Pulm Med. 2016;16(1):128. doi:10.1186/s12890-016-0290-5
31. Salaffi F, Di Carlo M, Farah S, Carotti M. Adherence to subcutaneous Anti-TNFα agents in patients with rheumatoid arthritis is largely influenced by pain and skin sensations at the injection site. Int J Rheum Dis. 2020;23(4):480–487. doi:10.1111/1756-185X.13803
32. Ovchinikova L, Smith L, Bosnic-Anticevich S. Inhaler technique maintenance: gaining an understanding from the patient’s perspective. J Asthma. 2011;48(6):616–624. doi:10.3109/02770903.2011.580032
33. Baba R, Nakachi I, Masaki K, et al. Repetitive instructions at short intervals contribute to the improvement of inhalation technique. Asia Pac Allergy. 2020;10(2):e19. doi:10.5415/apallergy.2020.10.e19
34. Masaki K, Miyata J, Kamatani T, et al. Risk factors for poor adherence to inhaled corticosteroid therapy in patients with moderate to severe asthma. Asian Pac J Allergy Immunol. 2020. doi:10.12932/AP-311219-0731
35. Mariye T, Girmay A, Birhanu T, et al. Adherence to insulin therapy and associated factors among patients with diabetes mellitus in public hospitals of Central Zone of Tigray, Ethiopia, 2018: a cross-sectional study. Pan Afr Med J. 2019;33:309. doi:10.11604/pamj.2019.33.309.17547
36. Busse WW, Maspero JF, Rabe KF, et al. Liberty Asthma QUEST: phase 3 randomized, double-blind, placebo-controlled, parallel-group study to evaluate dupilumab efficacy/safety in patients with uncontrolled, moderate-to-severe asthma. Adv Ther. 2018;35(5):737–748. doi:10.1007/s12325-018-0702-4
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.