Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Bandura’s Self-Efficacy Model Used to Explore Participants’ Experiences of Health, Lifestyle, and Work After Attending a Vocational Rehabilitation Program with Lifestyle Intervention – A Focus Group Study
Authors Linge AD ![]() , Bjørkly SK
, Bjørkly SK ![]() , Jensen C, Hasle B
, Jensen C, Hasle B
Received 17 August 2021
Accepted for publication 26 November 2021
Published 24 December 2021 Volume 2021:14 Pages 3533—3548
DOI https://doi.org/10.2147/JMDH.S334620
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Anita Dyb Linge,1 Stål Kapstø Bjørkly,2 Chris Jensen,3,4 Bente Hasle1
1Faculty of Social Science and History, Volda University College, Volda, Norway; 2Faculty of Health Sciences and Social Care, Molde University College, Molde, Norway; 3Norwegian National Advisory Unit on Occupational Rehabilitation, Rauland, Norway; 4Department of Public Health and Nursing, Norwegian University of Science and Technology (NTNU), Trondheim, Norway
Correspondence: Anita Dyb Linge
Faculty of Social Science and History, Volda University College, Mailbox 500, Volda, 6101, Norway
Tel +47 988 73 835
Email [email protected]
Purpose: We aimed to use the self-efficacy model to examine the participants’ experience, attitudes, and viewpoints regarding the association between work, health and lifestyle factors that influence work participation after completing a new one-year multidisciplinary vocational rehabilitation (VR) programme with a lifestyle intervention for people on or at risk of sick leave due to obesity or obesity-related problems.
Materials and Methods: This case study was based on focus group (FG) interviews with 11 previous participants. The interviews were conducted 2 to 4 years after they completed the program, between August and September 2019. The analysis followed Braun and Clarke’s six-phase reflexive thematic analysis (RTA) approach.
Results: The main theme “Work participation enhances quality of life” was prominent and related to mastery experience. Four sub-themes directly and indirectly affect work participation. The first sub-theme is “My attitude to life”, influenced by mastery experiences. Next, “Body size matters”, related to physiological and affective states. “Good physical capacity profit in everyday life” is associated to physiological and affective states, and the last “Support from the surroundings” influenced by vicarious experience and Verbal Persuasion.
Conclusion: This study’s main finding highlights how participants value work participation as a meaningful activity that positively influences their work self-efficacy. Future VR programs should pay attention to interventions focusing on the workplace, cognitive approaches to develop skills for coping strategies, lifestyle change purposing BMI reduction, physical activity, and support from the surroundings.
Clinical Trials: Technical information about the study on Clinical Trials NCT03286374.
Keywords: obesity, self-efficacy, vocational rehabilitation, occupational health
Introduction
People with obesity may have a good quality of life and physical functioning.1 However, people with obesity experience poorer health-related quality of life (HRQoL) when compared with the non-obese population.1 Obesity (body mass index [BMI] ≥ 30 kg/m2) is a multifactorial chronic disease associated with severe health complications, functional impairment and lower self-esteem.2 Causes of obesity result from a combination of genetic, biological, psychological, behavioural, familial, social, cultural, and environmental conditions.3–5 For many people with obesity, humiliation, stigmatization, discrimination, and bullying may be experienced daily in many areas of their social life, including the workplace.2,6,7 Moreover, obesity may also affect work participation through reduced job productivity and physical functioning,1,8 absenteeism from work, and sick leave.8,9 Statistics for the Scandinavian countries indicate that Denmark, reported a yearly 1, 8 million extra days of work absence and close to 1.100 cases of disability pension related to obesity.10 A study on Swedish women concludes that 10% of the total cost regarding social security are caused by overweight and obesity.11 A report from OECD through Statistics Norway shows that persons in the age between 50 to 59 with obesity have three times as much work absence than those without.12 Previously published studies indicate that working people of all ages with obesity may struggle to enter and remain in the workforce,8 contributing to adverse financial and social consequences, lower self-confidence, a depressed mood, and feelings of isolation.13,14 Further, publications indicate also that weight reduction may improve work ability and work participation.15–17 To manage health and functional capacity problems and adjust contextual factors, people in Norway can receive help through governmental-funded vocational rehabilitation (VR).18,19 VR aims not to cure illness but to promote work participation despite sickness and health complaints. Return to work (RTW) (ie return, maintain or stay at work) is often the outcome measure and the final goal; however, it explains only a small part of rehabilitation’s complex picture.14,20 For employees, job satisfaction, mental function and work-home balance are important outcomes of the RTW process.21 Previous research has indicated that people attending VR programmes may enhance work ability and reduce sick leave.15,22,23
In Norway, traditional VR programmes tend to last no more than 4 weeks and occasionally up to 12 weeks.18 This short duration contrasts sharply with the time people with obesity need to make lifestyle changes, which preferably would be more than 6 months.24 Therefore, in 2015, a new, temporary, multidisciplinary VR programme for people on or at risk of sick leave due to obesity or obesity-related problems, for example as diabetes, muscle and skeletal disorders, hypertension and mental health problems was established at a specialised rehabilitation centre, Muritunet, in Norway. The major differences between the traditional and the new VR program are the length and the behavioural- and dietary intervention. The inpatient VR programme was established with several follow-ups over an entire year to enable the participants to work with processes contributing to health benefits and increased RTW (Figure 1).
 |
Figure 1 A schematic overview above the vocational rehabilitation program’s In- and Outpatient stays with lifestyle intervention. |
The multidisciplinary team engaged in the rehabilitation program comprised a labour consultant, health care professionals and a sports educator; they all had complementary roles and collaborated to assess and treat the participants. Each participant developed a plan with goals for work activity, diet, physical activity, and coping strategies for the rehabilitation period. The rehabilitation program consisted of practical and theoretical intervention components in groups and individually. During the 4-week inpatient stay, the participants had, on average 17 hours of individual consultations with a labour consultant, medical doctor, dieticians, physiotherapist, psychiatrist, or nurse, all educated in Motivational interviewing.25 They also had 48 hours of group activity and lectures divided as follows: 14 hours of cognitive behaviour theory and practice, 20 hours of physical activity, 9.5 hours of education on food, 2.5 hours of work-related education, and 2 hours of lectures about obesity. After the four weeks of inpatient stay, the participants received an additional 4 hours of individual consulting, 6 hours of cognitive behaviour therapy and practice, 2 hours of food education and 4 hours of physical activity aiming to further support lifestyle change.
Self-Efficacy
The new VR programme lasted longer, had dietary and behavioural interventions, and was based on cognitive behaviour therapy principles to enhance work self-efficacy and lifestyle change. Self-efficacy is a dynamic construct that explains the development of motivation and coping strategies and may be a useful approach for understanding the self-management aspects of RTW and lifestyle change.14,26 Self-efficacy is defined as “belief in one’s abilities to organise and execute the courses of action required to produce a given attainment”.27 Self-efficacy is an important cognitive, motivational factor for predicting functional recovery and an individual’s probability of successfully participating in and completing treatment and maintaining appropriate behaviour.14,23,27 Self-efficacy belief can vary, often substantially, across different domains of functioning. This implies that an increase of self-efficacy in one domain may be interpreted as a result of increased self-efficacy in other domains.27
The four sources of self-efficacy are: Mastery Experience, Vicarious Experience, Verbal Persuasion, and Emotional and Physiological states. The first and most important source of increasing self-efficacy is having a direct experience of mastery. The second component is vicarious experiences. This comes from observations of people around us, particularly from persons we consider role models. Verbal persuasion is the third element. Positive communication and feedback from influential persons in our lives, such as family, teachers, and colleagues, can strengthen our self-belief. The last source for improved self-efficacy is emotional and physiological states. These four sources influence each other and can contribute to improving our confidence in our skills. Belief in personal efficacy promotes a key factor of healthy development,26 and high self-efficacy will generally contribute to better performance.27 The level of self-efficacy can predict behaviour change and the likelihood of successfully embracing and coping with life.14,27 How people live their lives depends on previous experiences, how they evaluate their abilities concerning the approval of others, how support from others can strengthen their belief to achieve what they seek, and how the emotional state affects the body’s physiological responses.27 Peoples’ self-efficacy is rooted in a system consisting of individual factors and environmental and social systems. In a group, working together may be essential for achieving collective social goals.27
Self-efficacy is a good predictor of behaviour and behaviour change. Still, the concept cannot be used as an exhaustive explanation of “the beliefs about whether actions affect outcomes”,27 further explained as outcome expectancy. Outcomes, for example, BMI loss and work participation in this study, arise from action and depend a lot on an individual’s judgment of how well they will perform in a given situation. Unrealistic high expectancy outcomes can be demoralising in combination with low skills to accomplish tasks and activities. In contrast, high expectancy in combination with good skills can motivate one to a desired behaviour.27 A mix between self-efficacy and outcome expectancy can contribute to good behavioural outcomes and strengthening emotional abilities.27
VR with a lifestyle intervention is new and unexplored. Only a few studies have focused on the association between multifactorial lifestyle risk and work ability20,28 and factors that generate work participation for people with obesity.29 By examining the work dimension’s interpretation, we can explore a more holistic picture of the complexity of obesity and work participation. The participants’ own voices on what they experience as facilitating or inhibiting their lifestyles and work participation are vital for this insight. Therefore, the present study aimed to use the four sources of self-efficacy to examine the participants’ experience, attitudes, and viewpoints regarding the association between work, health and lifestyle factors that influence work participation 2 to 4 years after completing the new VR programme with lifestyle intervention.
Materials and Methods
Study Design
This qualitative case study was based on focus group (FG) interviews with persons who had attended the new one-year multidisciplinary VR programme. The interviews were conducted between August and September 2019, 2 to 4 years after they completed the VR program. An invitation was given to participants who had achieved weight loss during the VR program and worked part or full-time at the 12-month follow-up. On average, the participants had achieved −11.9 kg weight loss during the VR program, stretching from −17.2 to −6.8 kg. The participants lived in a geographical area nearby each other.
Participants
In total, 18 individuals between 18 and 64 years were telephoned, and 12 orally consented to participate. As well, the participants received a written letter with information about the study (purpose, date, time, and place for the interview). Based on geographical destinations, the participants were divided into three FGs. On the same day as FG interview number two, one male participant could not come. Therefore, the total number of participants reported in this study is 11 (Table 1).
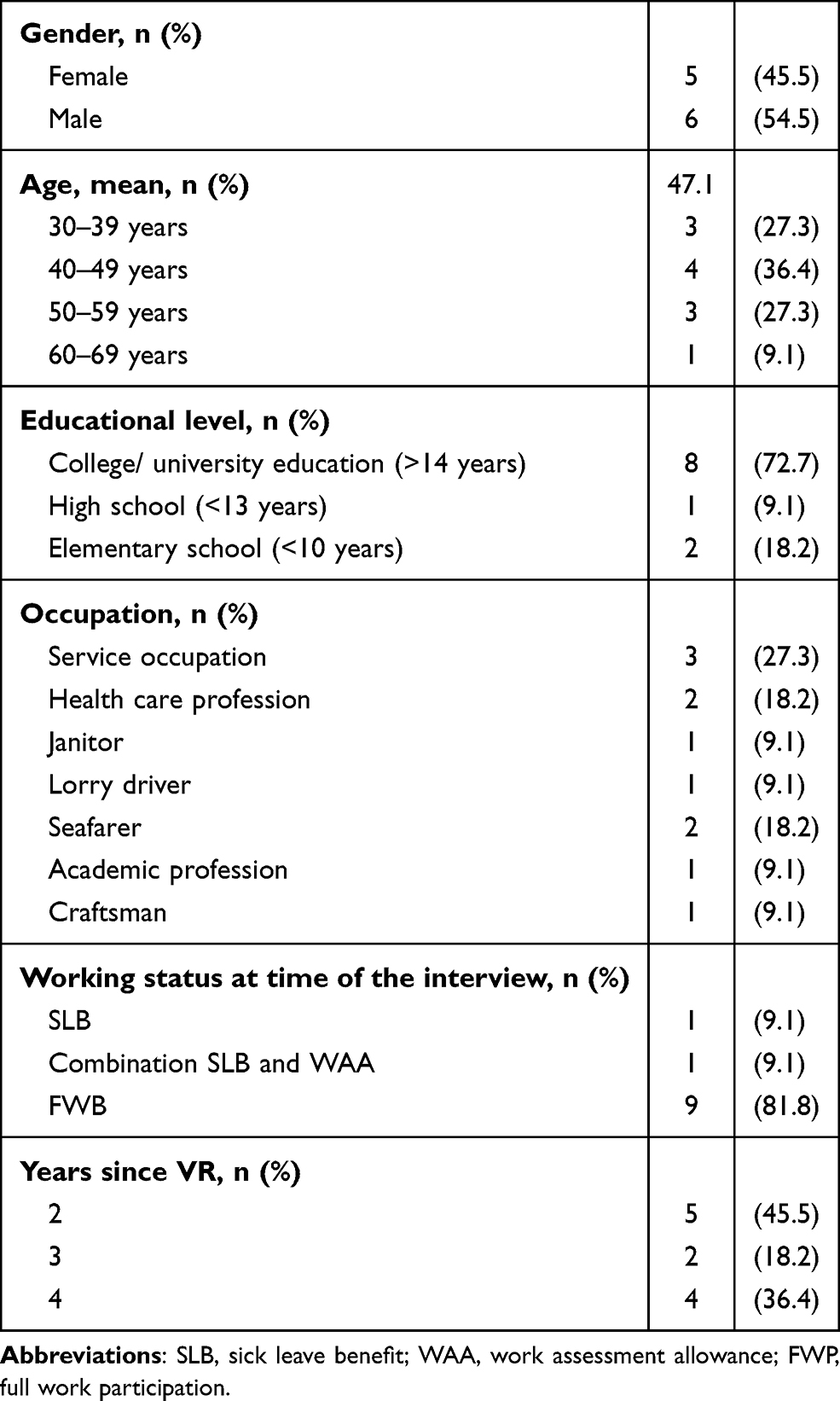 |
Table 1 Characteristics of the Participants |
The study sample included 6 men and 5 women aged 35 to 62 years. At the time of the interview, 2 of the participants were single and 9 married. Eight of the participants worked full-time, 2 were working part-time, and 1 female participant was temporarily on sick leave due to an operation. Seven participants had extended work experience of more than 20 years, and the rest had between 11 to 20 years of work experience. Since attending the VR program, 6 participants had lost or maintained their body weight, and 5 were “going up and down.”
Interviews
A semi-structured interview guide was developed to capture the participants’ experiences, attitudes, and viewpoints on the association between health, lifestyle, and work participation (Appendix 1). The interviews were based on open-ended questions. The questionnaires were first tested on a selected and consenting individual with a BMI of more than 30 who participated in a lifestyle change program at Muritunet, a specialised rehabilitation centre. This resulted in small changes to the interview guide. Second, in a VR program at Muritunet, two groups of volunteers tested the modified interview guide and, subsequently, the questionnaires were adjusted to ensure validity.
The first and last author in this article conducted all three FGs. Each interview took from 1.5 to 2 hours and was conducted in a suitable meeting room big enough for six persons. The FG interview started with presenting the study’s purpose, group rules, expectations, and the participants’ possibility of clearing up any ambiguities. A short presentation for the members was conducted before introducing topics in the interview. To keep control over the FG interview, the main author controlled the discussion and interaction. The last author kept track of what was taking place, taking notes and contributing with questions and input in the dialogue.30 After approval from the participants, the interviews were digitally recorded.
After the interviews, the authors summarised the experiences and observations. After each interview, the digital data were reviewed and orthographically transcribed.31 Each transcript was compared with digital files at least twice.
Reflexive Thematic Data Analysis
The analysis followed Braun and Clarke’s six-phase reflexive thematic analysis (RTA) approach, which involves familiarising data, data coding, searching for themes, reviewing themes, defining, and naming themes and producing the report.31–33 The process was characterised by an exchange of views, creative thinking, sharing, and discussing notes and models between the first and last authors. RTA allows identifying broad themes among the participants’ experiences on what affects their work participation.34 Analysing data was not a straightforward process but rather a process in which we moved back and forth between the different writing phases.
The RTA process started with familiarising ourselves with the data and identifying essential information relevant to the study’s aim before exchanging opinions. The first and last authors started with a hard copy (paper and pen) method, first separately and then together. The next phase included importing transcript interviews to NVivo version 12 for Windows. This process consisted of an analysis of data which were accompanied by observational and causal notes.31 In this phase, data “opened up” and provided more profound meaning. An inductive approach contributed to coding the essence of what was interesting, first on hard copy and then in NVivo. NVivo allowed matching the code of the part of the interview to that to which it refers. The data amount was reduced throughout the coding process and briefly organized the interview content into meaningful categories relevant to answering the study aim.33 Included data described knowledge from the VR program and substantiated participants’ experiences with work participation. Codes in this section provided the building blocks of the analysis.31,33 Data were then sorted into themes, and meaning-based patterns were identified by looking into the codes and their associated extracts.33 Going back and forth through the data contributed to establishing coherent and distinctive themes,31 and the themes names were based on the theme’s content, interest, and essence.
Writing “what we did” and “what we found” hopefully provides transparency to aid in understanding the messy process involved in transforming focus group research into a coherent and informative presentation. Quotations in this article of what the participants said demonstrate the findings, give the participants a voice, and demonstrate the interpretative adequacy of the analysis.31,33
Results
One main theme and four sub-themes emerged from the analysis and consisted of information affecting the participants’ self-efficacy concerning work participation. The findings are presented according to the four sources of self-efficacy by Bandura,27,35 a theoretical framework used as a lens for how this study labelled the findings36 (Table 2).
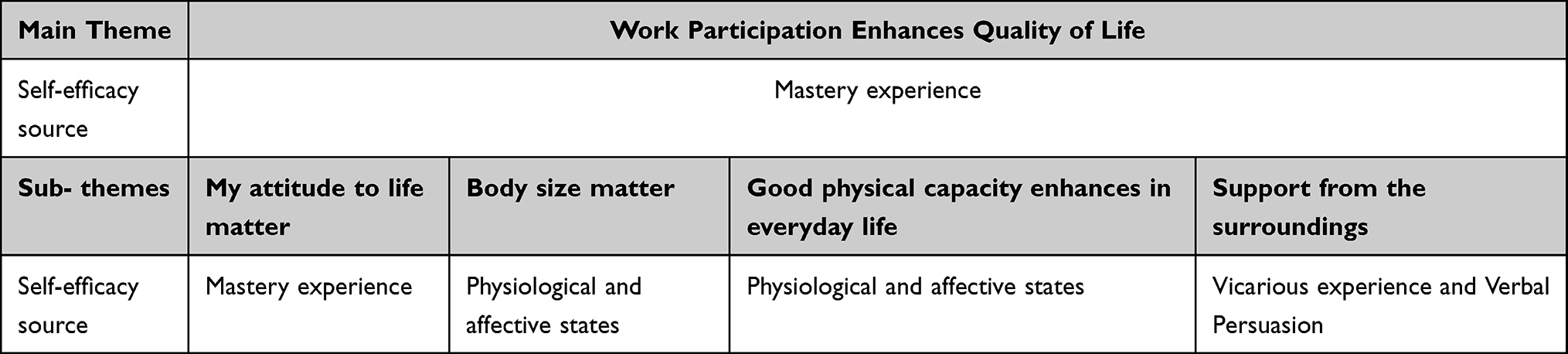 |
Table 2 Overview of Findings and Related Self-Efficacy Source |
Due to the modest amount of published literature about factors that generate work participation for people with obesity, the framework of self-efficacy can contribute as a valuable approach for the study context and depth of the topics of work and obesity.37 The main theme is “Work participation enhances quality of life”, and the four sub-themes are “My attitude to life”, “Body size matters”, “Good physical capacity enhances in everyday life”, and the last, “Support from the surroundings”.
The main and the first sub-theme are presented within the source of mastery experience, and the third and fourth, within the source of physiological and affective states. The last theme is presented with the source vicarious experience and verbal persuasion. The amount of information within these sources highlights how important they are for the participants’ general self-efficacy concerning health, lifestyle, and work participation.
Work Participation Enhances Quality of Life: Mastery Experience
Work participation enhances quality of life was unlike the other themes as it was prominent in all focus groups interviews and, therefore, the main theme. This theme contains information about job satisfaction, facilitated work, good relationship with employers and colleagues, and the consequences of lack of recognition.
Most of the participants had worked many years in the same profession or with the same employer. It struck us how they all were proud of what they do. The participants talked warmly about their devotion and dedication to their jobs. They had important tasks, and one skipper told us:
I love to be in charge, to manoeuvre the boat and to do the job right. That is my quality of life. I love my job, and I’m a sailor. For me, work is a way of life.
One of the women working with children said it is
Nice to get to work, and the kids wrap around my neck. During the periods I have been on sick leave, I miss the social life, to be with the other colleagues and have the possibility to talk to the others.
They stated that “it is important to enjoy the work” and that “a job with well-being compensates for much in life.” Being part of a good team was highlighted for “well-being at work.” One of the women said, “We colleagues kid with each other”. Another woman said: “I need jokes and laughter around me at work. Nonsense gives me a good laugh”. Working together in a team, sharing life experiences, and having fun together was crucial for job satisfaction. These statements were typical for all the participants and were analysed as the core theme of all three focus groups’ interviews. Good communication and relationship with employers and colleagues may support their self-efficacy in interaction with others.
During the interviews, the participants discussed what promotes and inhibits work participation. An employer can make things easier or harder in the workplace.
There is not always need for big changes, but it was helpful when Fridays were celebrated with fruit instead of cake. Not just because of me but in general.
Another employer had organised physical activity and signed up for organised physical activity called “Stikk UT.” The company offered this to all their employees. Some participants had employers who contributed to job satisfaction and a healthy lifestyle as an inclusive practice for all, which supported their work self-efficacy. An attitude like this might help alleviate the stigma individuals who are overweight usually encounter. Sometimes greater accommodations are required, illustrated in the craftsman example where his employer “facilitated that I did not have to travel that much, and I worked less overtime.” Working shifts contributed to a less healthy lifestyle, and some participants had access to modified jobs with the same employer when, as one said, “I got sleeping problems due to the night shift which affected my eating habits and my lifestyle”.
However, not all the participants had good experiences with their employers. One of them found that shift work and “unconventional working hours lead to sleeping problems and anxiety.” One informant experienced a lack of recognition of his health problems and related the following:
After I got on sick leave, my first contact with my employer was after six months. My employer called me one hour before a dialogue meeting with NAV. My problem, I could not sleep due to shift work, became stressed, and my employer did not show any interest in facilitating the work, which affected both my work ability and lifestyle.
Not experiencing support from his employer was understood as a means of exclusion and affected his lifestyle. Not being heard when struggling at work was associated with loss of motivation, work absence and decreased work self-efficacy to exercise control over troublesome situations.
The main theme contains information about what work participation means for the participants and what can be done to maintain work participation. Regardless of which focus group, participants shared information about work participation’s joy and satisfaction, based on their past and present experiences. Even when a workload included heavy physical tasks, as one cleaning lady talked about, her satisfaction in being a part of and having important tasks in a work community was strong: “I love to be at work, it is my family, there is humour and a fantastic place to be”. Her satisfaction did not, however, keep her from adding to the theme of how a large body makes work hard.
The participants emphasised with employers who facilitated working hours and a healthy lifestyle. They conversed positively about employers who served fruit instead of cake, organised or facilitated physical activity during working hours or leisure times, and facilitated and individualised organised working conditions for the workers. Participants highlighted good leaders who promoted a healthy work culture and was a source of well-being and job satisfaction. Having a need for modified work not being accommodated was a factor that led to sick leave and consequent troubling lifestyle change processes.
My Attitudes to Life: Mastery Experiences
The first sub-theme associated with work participation included findings about how participants’ thoughts, feelings, and the ability to conduct tasks and activity successfully affected their lives in general. This sub-theme provides insight into what promotes and inhibits choices related to life in general and work participation.
Besides participation in work, the participants continued working on their lifestyle change process, including weight loss, which might be challenging to achieve and maintain. In all focus group interviews, the topic of “weight cycling,” which describes repeated periods of unhealthy food intake, inactivity and loss of faith and motivation, was recurring. It seems that “weight cycling” greatly impacted the participants’ lives, both in their lifestyles and, equally importantly, in their coping strategies in general. Participants who expected weight cycling managed to recognise and mobilise previously experienced strategies to return to a lifestyle characterised by healthy food, structure in everyday life and positive self-efficacy. Also, they had the strong belief: “I know I can!”, build on previous experiences in combination with high outcome expectancy. Another characteristic was that instead of cutting out food, they replaced unhealthy with healthy food. They maintained a balance between allowing and denying themselves food and sweets, like, for example, one of the women who described one of her coping strategies:
I have learned to eat food, and I taste sweets. I have stopped eating sweets, I taste it. I look forward to tasting and have stopped having a bad conscience about tasting”. She had learned that previous food patterns and feelings about eating decreased her self-efficacy and had now learned a coping strategy which affected her positively.
Three of the informants did not manage to overcome the negative weight cycling and expressed a wish to have “the strength to succeed and stay there.” Previous experience with diets that failed, lack of coping strategies and external factors contributed to failure in their projects. One reported having lost her “motivation on vacation and could not stop the unhealthy lifestyle - there were no future goals.” One of the sailors said that his “loss of faith” was associated with several factors. It was connected to the culture at work with “inappropriate food patterns”, “an inhibitory sports injury, and a new girlfriend. Getting a girlfriend is not good if you want to lose weight [laughter].” In some periods, especially in cases where the lifestyle-change process failed, many of the participants’ felt unsuccessful and withdrew themselves from others, both from work colleagues and in private: “I withdraw myself from others when I fail in my project and am more social when I succeed - my own choice.” It seems that negative strategies among the participants were characterised by no future goals, lower self-efficacy, and a higher sense of failure when they failed in life.
Letting go of a miserable conscience and learning to deal with emotions and messy thoughts was another experience involved in being able to handle the workload and which contributed to increased self-efficacy. One of the women said:
I had messy thoughts all the time both at work and in private. Then I realised that this was not good for me. In the last year, I haven’t had that messy thinking. I have discovered that I still reach the finish line.
This echoed what another woman pointed out:
I have a less lousy conscience now. I have learned not to worry too much. In my group, we talk a lot about eating our emotions. I have become good at putting thoughts and worries away, and then I do not get so scared. I do not dull my fears by eating them up.
Accepting “who you are and what you can do” is the last experience the participants’ highlighted. High expectations recurred as a factor for stress. Two participants in different focus groups both engaged in the theme of being “good enough”. They had changed their attitudes to life in general by not letting their big bodies dominate their thoughts. Both had lost weight and learned from previous thoughts and feelings, redefined and strengthened their self-efficacy, and accepted “who you are and what you can do”. One of the women said that she had “learned that I am good enough”, and these two participants supported other group members that had not succeeded by encouraging them: “One should be happy for the one thing you achieve and not focus on the other things you have not done.”
Body Size Matters: Physiological and Affective States
The second sub-theme contained findings regarding how body size promotes or inhibits work participation. The participants started by explaining why body weight reduction was important for them regarding work participation. Three of the men, mainly sailors, faced the threat of losing their jobs because of their obesity or obesity-related diseases:
We could have lost our medical certificate. We go to the seafarer’s doctor every other year. We struggled with overweight and had problems. We could have lost our jobs if we had not lost weight.
One lorry driver experienced that his doctor “threatened to take my driver license due to my uncontrolled blood sugar; I have diabetes.”
Both men and women experienced how body weight reduction had positive effects regarding work execution. They experienced that body weight reduction contributed to easier job performance. For some, being able to wear normal clothing sizes rather than custom-made work clothing was a relief. These positive effects of body weight reduction contrasted with the experiences of a cleaning lady who gained body weight after the VR programme. She talked openly about how her body size affected her work participation and health:
I have low-back pain, and today, I am attending a treatment program for this problem. I am 50% on sick leave. Walking around with heavy body weight on my stomach is not ideal for my back.
Regardless of body weight reduction, the participants talked about how their body size affected work participation through increased security risk due to safety equipment not being customised for people with obesity. The lorry driver talked about his fear when he was walking on the top of a truck:
When you have a high BMI as I do, I am afraid of the balance. I must balance on the roof of the vehicle, between two low rails. The thin rails to pull up that should hold me on the top will be unsafe if I fall.
Body size affects security at work directly and indirectly because it may also exclude some from participation in fire drills and first aid training. The participants experienced their body size exposed in these situations and found this excessive attention unpleasant. One of the women who had gained weight said:
I did not want to participate. Imagine, getting laid down and being pulled along the floor. You are revealed for how heavy you are…. Also, we had a first aid course at work. We were going to create a situation where I would faint. I did not want to lie down, and others would turn me over in a stable side position.
Another woman in the focus group supported her: “I agree with her. Pulled in a fire blanket… then I would leave.” These stories can describe how self-image is at play at work due to obesity. The participants’ emotional reactions to activities, tasks, and situations due to body size seemed to affect their judgment of their ability to complete tasks in different areas. Low self-images affect self-efficacy and may be a result of how other employees think of people with obesity. Especially among health care workers, the participants experienced stigma, which affected their work participation indirectly and directly:
Often when I go to the medical doctors, they tell me to lose weight and then my problems will be solved. You will not be taken very seriously when you have a big body.
Another example was from a lady working as a nurse:
I have struggled a lot with my hips. The orthopaedic surgeon could give me new hips but recommended that I lose weight for a successful outcome. So now I have fixed them, hip replacements. When I read the description of the operation, it was a revelation that my hip problems were due to a congenital hip defect. It was a relief; this was not just self-inflicted.
Some have also experienced violation from others like the man in this quotation:
I was on the mountain one day, and there was a girl who had sprained her ankle. There were six persons from the Red Cross that carried her down. One group member told me that I should not injure my ankles on the mountain because they could not bear to carry me down.
Besides stigma, one of the women talked about experiences of discrimination due to obesity:
I have experienced that people think I am pregnant because of my stomach. Once, when I was at a job interview, I’m sure that I did not get the position because they thought I was pregnant. The girl who got the position had less education than I. I guess they thought I was pregnant, and then they could not hire me because I was soon going on maternity leave.
One of the men said that he has worked “high up in organisations” and experienced how “people with obesity have been deselected, even though they have had wonderful qualifications.” He concluded: “If you are too obese, you lose respect!”
The participants talked about how body weight reduction improved individual health with normal blood pressure, more stable blood sugar, and increased activity level. These improvements led to their renewing their medical certificates to continue working on Norwegian ships and mobile offshore units and as a lorry driver. Besides health improvements, body weight reductions contributed to relief among three participants regarding their being able to wear workwear in normal sizes and how much easier it was to do their jobs with trouble-free access to difficult places. Without body weight reduction, health complaints maintained and negatively affected work participation. Obesity may contribute to security risks at work because of a lack of safety requirements and of people avoiding exposing themselves to safety training courses. The participants experienced stigma and discrimination both at work and in private from healthcare workers, colleges, and unknown people in their surroundings. Discrimination can be random or, in worst cases, systematic within an organisation. Stigma affected all areas of their lives and affected the participants’ thoughts and feelings. With an underlying tone of seriousness, the participants talked about discrimination and stigma whimsically.
Good Physical Capacity Enhances in Everyday Life: Physiological and Affective States
The third sub-theme contains findings on the physical capacity that enhances participants’ work participation and mental and physical health. Two to four years after they completed the VR, physical capacity and activity seemed to be more important to participants than their body weight reduction. They talked about the physical endurance needed for a functional body and how important this was, like one lady in this quotation said: “Losing body weight was not the most important thing for me. I was not that obese. Getting in better shape to cope with the day was essential for me.” Achieving this goal was described as “liberating”. High physical capacity was experienced as a factor for better mood, greater endurance, and the feeling of confidence. These factors contributed to coping with work demands and in everyday life and building self-efficacy. Mainly, lifestyle changes were kept, despite gained weight for some. One of the young men related:
Always go for a morning walk and maybe once again during the day. Suddenly it becomes “Oh, Saturday I can go for a long walk!” Very nice! Walking has become an activity I want to do and not something I have to do. I have even changed to a new job which contributed to being “paid to be sweaty”.
One of the women experienced that she “lost motivation.” She had gained weight and said it was hard to work:
I get body pain; my body hurts all over. I know that if I’m good at exercising, then I have the strength to carry my body, and then I do not get so much pain. It does not matter if I have high body weight, but whether I have a functional body.
In addition, other participants had experienced that low physical endurance contributed to lower energy level, less social contact with others, and increased health complaints, which, in total, may affect work participation. It seems that low physical endurance and capacity may influence the participants about how they feel and think of themselves.
One participant had health barriers that made physical activity difficult. Nevertheless, she had managed to find pleasure in activities by adapting physical activity requirements based on a functional level assumption:
I cannot walk in the mountains. I have learned that walking around the corner is also a form of exercise. Walking around the “corner” takes only 10 minutes. Suddenly I may have walked for 15 minutes. It is more than nothing. It does not have to be an exhausting activity.
Two of the female informants had additional responsibility for children with special challenges. This was a contributing factor to sick leave. The additional obligations for children also prevented physical activity. After participating in VR, one of them chose to reduce work participation from 100% to 80% to prioritise physical activity. The motivation for physical activity was also shown by the other mothers who applied for 30% disability benefits due to health complaints. In that way, she managed both continuous work participation and physical activity but accepted less income. These mothers found a balance between family obligations and taking care of their health. One of the women talked about her new lifestyle and expressed: “I use my trips as a break. Then I think of everything and nothing. No children were quarrelling or bullying each other. That’s good for me.”
Most participants exercised several times a week with swimming, hiking, running, bicycling, weight training, walking and interval exercise. Physical capacity contributed to the participants’ increased energy level, strength, and social contact both at work and in general. It seems that most of the participants preferred to exercise during the morning because they experienced that early activity contributes to reasonably healthy choices for the rest of the day. The activity level positively influenced their image of health, ability to handle the workloads, and participation in family and social activity.
Support from the Surroundings: Vicarious Experience and Verbal Persuasion
The last sub-theme contains information about how support from colleagues, family and others may promote and inhibit the participants success in life. The participants regarded their colleagues and employer as essential factors for support. During the interviews, stories were told about how colleagues’ support was valued and motivated their work participation. Some, like this lady, had experienced that her colleagues and employer had supported her: “They applauded me! When I got back to work after sick leave, I had no fear.” Furthermore, working in groups was highlighted: “Nice to be a part of the team, we are good in teams. I know we are doing a good job.”
Not everyone had an extended framework consisting of supportive colleagues. The lorry driver worked most of the time alone, driving his lorry. His working frame did not facilitate extended physical contact with other colleagues. He stopped along the road in diners to meet other lorry drivers, and they exchanged experiences and sharing from their everyday life. He talked about a “lorry-driver culture”: “We are meeting at the dinner, and then it is about being the biggest liar [Laughter].” He is not a “talker” and likes to listen, but he still finds this “lorry driver culture” supportive.
Besides employers and colleagues, the participants highlighted family and friends’ support that affected their attitudes to life and lifestyle. Families provided support through working with the participant to implement new routines for the whole family regarding food habits and exercise. “A lucky man” talked proudly about his wife: “My wife supports me. She makes healthy food, and we exercise together… it helps me a lot that she is with me.” This support is essential for continuing a healthy lifestyle and for faith and motivation. A supportive family seems essential in a healthy lifestyle and handling health concerns. One of the women had an opposite experience where the family had another food habit than she and shared no interest in her process:
I experienced that it was challenging to come home after VR and have to arrange the food myself. My husband and two children were not in the process as I. I sat with my crispbreads while they enjoyed themselves with delicious food. It didn’t take that long a time before I started eating the food the family ate.
Another inhibiting factor was family members who secretly ate sweets and unhealthy food but forgot to throw out the packaging. When her husband “was eating potato chips when we were sitting on the couch,” one of the women decided, “I had to go to bed because I could not sit and watch him.” The family’s ability to support the participants’ seems to influence their ability to master the activity needed for faith, motivation, and success.
For two of the mothers who still had children living at home, a family situation where the partner is working long periods away from home results in little support in their daily life, which was experienced as exhausting and, in the end, affected their life in general and thereby their work participation.
Discussion
Methodological Considerations
The present study aimed to use the four sources of self-efficacy to examine participants’ experience, attitudes, and viewpoints regarding the association between work, health and lifestyle factors that influenced work participation 2 to 4 years after they had participated in the new VR programme with lifestyle intervention. Before the interview, the participants received both written and oral information about the aim and subjects of the FG. The participants’ voices on what they see as promoting and inhibiting factors in the related fields of obesity and work participation is vital for insight into this relatively unexplored area.
The strength of this study has been the choice of a FG interview to gain insight into participants’ experiences since the aim of qualitative methods is to seek the participants’ experiences of social phenomena. As such, these methods can identify nuances and complexity not otherwise accessible.38
Another strength is that the FG led to a certain level of empowerment of the participants.31 The participants came up with new topics that were meaningful to them, which they discussed and which contributed to a meaning-creating process. In addition, they exchanged experiences and explored each other’s opinions which, for some, gave inspiration and motivation for their lifestyle and work participation.
The timing of the interview- 2 to 4 years after completing the VR programme with the lifestyle intervention is another strength. Following the participants’ experiences through VR and the time afterwards has been crucial for obtaining information that contributes to a broad picture about their diverse life experiences regarding health, lifestyle, and work.
Findings indicate that the participants differed in work- and family status, body weight and health complaints. These differences provide insight into those participants who had and did not have body weight reduction as well as into working participants and participants temporarily outside the workforce on promoting or inhibiting factors affecting their health, lifestyle, and work participation.
The last strength was that the first and last author collaborated through the process by conducting the interviews, going through the interviews after each FG, analysing and discussing the findings in the data, and establishing themes presented in this article.
Two FGs had four participants, and the last had three. The information from the one FG with four participants was narrower than the other two. The reason might be the combination of different personalities in the group: two participants were modest, one talked more than the others, and gender distribution was three men and one woman. In addition, this was the first FG for the first author who was inexperienced in leading an FG. In total, this may have affected the FG and execution.
Another limitation in the other two FGs was that some participants spoke more than others, leading the moderators to intervene in the dialogue to promote the modest participants. This may have influenced the group dynamic and the overall contribution to data.
Discussion of Results
Even though Bandura’s four sources of self-efficacy are discussed separately, it is important to have in mind that the sources influence each other, contributing together to participants’ self-efficacy regarding health, lifestyle and work participation. The data reported provides an opportunity to hear the participants’ attitudes on what promotes and inhibits their self-efficacy towards work participation.
Work Participation Enhances Quality of Life: Mastery Experience
The participants experienced working together in teams as an important source for continued and remaining work participation. Furthermore, their experience of employers who provided tailored work promoted a healthy lifestyle and a positive job culture. When the participants succeed with a lifestyle change, RTW, or other tasks at work, they will, according to mastery experience, obtain truly, genuine and objective evidence for their ability to succeed.27 Our findings support existing literature regarding workplace modification contributing to healthier nutrition, physical activity, working hours, and preventing one participant from taking sick leave due to night shifts.39–42
As the participants had spent a quarter of their life at work, they had extensive work participation and experience about how work affects them. Participants emphasised job satisfaction as an important factor for their well-being at work and RTW, which is highly influenced by past and present experiences, which is also supported in the literature.14,21,43,44 Unconventional working hours and unmodified work are associated with loss of motivation and work absence. Not being heard can reduce their self-efficacy by undermining their efforts in difficult situations resulting in loss of faith in required skills to stay-at-work.27 In addition, failure to succeed will reduce self-efficacy if a failure occurs in the early lifestyle change and RTW process. Promoting and inhibiting factors in the main theme are especially significant because they are based on mastery experiences, the most influential source of efficacy information.27,35 These findings support existing literature where working conditions can contribute to illness, disability, and absence.45,46
It is important to address the feeling of joy, social inclusion, and devotion to work as important sources of work self-efficacy. The participants’ stories about work are strongly associated with past and present mastery experience.13,35,47,48
My Attitude to Life: Mastery Experience
Attitude to life influences both at work and in other areas of life. Job satisfaction and the wish to maintain work that requires a medical certificate contribute positively to losing body weight. Adapted coping strategies affected the participants’ lifestyles and how they solved stress connected with work participation. Further, strategies contributed to balancing between allowing and denying, knowing how to deal with messy thoughts and feelings, and accepting that I am good enough. Increased self-efficacy, built by previous experiences, seems to establish a strong belief in their outcome expectancy “I know I can” contributing to positive activity performance. Another interesting finding is how some of the participants had, in the process, managed to describe adjustments customised to their needs that enabled them to maintain or return to work. They found their value as employees and claimed adjustments to ensure a balance between health and work demands. Attitudes and strategies, in general, seem to affect how the participants’ chooses to accomplish tasks and activity, and these again affect how they cope with life. Our findings merge with systematic reviews where higher self-efficacy are associated with sustained work participation despite health problems.13,43 Negative strategies among the participants were characterised by no future goals, lower self-efficacy, and a higher sense of failure when they failed with lifestyle change, and these findings also support other studies.13,43
In the interviews, the participants described life with its ups and downs. When life is tough, everything is complicated, and when life is good, they feel strong and unbeatable. Stories about dealing with these ups and downs provided insights into what promotes and inhibits choices associated with life in general and work participation. Seem to be better able to make choices in situations that arise and to accomplish tasks and activities.27
Body Size Matters: Physiological and Affective States
Body size influenced work participation, and structure and working frames affected the participants’ lifestyle and body weight loss. Body weight reduction among the participants gave health benefits that contributed to the renewal of a driver’s licence and medical certificate, made it easier to carry out work tasks, allowed wearing workwear in normal sizes and extended social contact. Loss of body weight increased participants’ ability to work and enhanced work self-efficacy and is supported by previous studies that indicated that weight loss positively affects work capacity, mood, working memory, and body image, and this can contribute to increased self-efficacy.26,49,50
Body size is negatively associated with work participation due to musculoskeletal disorders, stigma, and discrimination, and this has been supported in a meta-analysis of 29 longitudinal studies where health problems were an important barrier for maintaining paid employment.2,7 Our findings of the participants’ experiences of body size are also supported in systematic reviews, such as persons with obesity being hired less frequently than those with average body weight and receiving less frequent promotions than individuals of average body weight51 and on the association between obesity and musculoskeletal disorders.2 The participants’ stories indicated that body size may have influenced how they judged their self-efficacy concerning work participation and life in general. Emotional reactions to activities, tasks, and situations due to body size seemed to affect their judgment of their ability to complete tasks in different areas.27
Good Physical Capacity Enhances in Everyday Life: Physiological and Affective States
Physical capacity is highlighted as an essential factor for most of the participants. Physical activity contributes to protecting and reducing medical conditions such as heart disease, high blood pressure, diabetes, stress, depression, anxiety, and lower BMI, all important factors both for health and work participation.52 Participants’ physical endurance profited them in activity at work and at leisure time, and several of the participants appreciated a job with physical activity requirements that contributed to increasing their physical capacity. It seems that physical activity at work and in private, contributes to coping with work demands and building self-efficacy. Previous research indicates that better health (ie better general physical and mental health) reduces sick leave, results in earlier return to work following sick leave, and reduces the risk of work disability for people with chronic diseases.22 Our findings support existing literature indicating that physical activity increases mobility and lower extremity function, as well as reduces arthritis pain, energy level and well-being.1,5 In addition, the participants thought it was important to customise activity to their life situations and to find a suitable balance between their own needs adapted to the family’s, a finding that also supports existing literature.45 It seems that improvement in physical endurance and capacity may increase personal efficacy through how individuals feel and think of themselves.27
Support from the Surroundings: Vicarious Experience and Verbal Persuasion
Colleagues, employers, and families are highlighted as important contributions for support for work participation and life in general. Support from colleagues and employers may be crucial for a healthy work environment and work culture, important factors for job satisfaction and successful RTW. It seems that the participants’ increased self-efficacy after participating in the VR programme, together with perceived support, had a positive impact on them. This study’s findings support existing literature on colleagues’ and employers’ roles as facilitators and that positive attitude and self-efficacy may contribute positively to maintaining or increasing work participation.19,53–56
Having social support from one’s family can help in coping with health concerns, and this study’s findings highlights supportive family as an important factor in a healthy lifestyle where new habits occur and continue. In addition, support from the family affects the total life situation, which affects the participants’ work ability. In contrast, lack of support affects participants’ physical activity, body weight (such as weight cycling), and may contribute to lower self-efficacy. It seems that positive appraisal from acquaintances and observing people around them raised participants’ belief in their ability to master the activity needed for faith, motivation, and success. Assumptions concerning self-efficacy increase or decrease depending on whom the participants imitate and through positive or negative assessment from others.27 Our findings are similar to the existing literature for people with nonspecific musculoskeletal disorder.22,43,44
Conclusions
The present study aimed to use the four sources of self-efficacy to examine participants’ experiences, attitudes, and viewpoints regarding associations between work, health, and lifestyle factors that might influence work participation with a focus group design 2 to 4 years after completing the new VR programme with lifestyle intervention. One main theme and four sub-themes emerged from the analyses and were highlighted as important for the participants’ self-efficacy and work participation. Job satisfaction seems to occur from a healthy work culture and from employers who modify work and contribute to a healthy lifestyle at work. The participants with high job satisfaction seem to have had a resilient sense of self-efficacy in overcoming obstacles at work through effort and perseverance.
Factors like positive attitudes, efficient coping strategies, a high self-efficacy, and acceptance that “I am good enough” seem to characterise those who lose weight and stay there. It seems that increased self-efficacy combined with a high outcome expectancy such as “I know I can” makes them stronger in overcoming weight cycling and other obstacles in a lifestyle change process and work participation.
Participants’ body size influenced their work performance, and several of the participants experienced stigma and discrimination. Lower self-images seem to lead to avoidance of fire drills and first aid courses and requests for security equipment made for people with obesity. The participants’ body size seems to impact how they judge themselves and influences their self-efficacy concerning work participation and life in general.
Two to four years after completing the VR programme, good physical capacity was more important than weight reduction. Physical activity and physical endurance were highlighted as a source of personal efficacy regarding how they felt and thought about themselves.
Colleagues, employers, and families form a supportive network contributing to a healthy lifestyle and work participation. Participants who cooperate and collaborate with their network and receive verbal support increased their belief in mastering the activities needed for success in lifestyle and work participation.
In this study Mastery Experience and Physiological and Affective States are the two most influential sources of Bandura’s self-efficacy model. This study’s finding indicates that VR programmes should be aware that the level of self-efficacy can predict behaviour change and the likelihood of successfully embracing and coping with life.
The main finding, “work participation enhances quality of life” highlights how participants value work participation as a meaningful activity and positively influence their work self-efficacy. Future VR programs should pay attention to interventions focusing on the workplace, cognitive approaches to develop skills for coping strategies, lifestyle change purposing BMI reduction, physical activity, and support from the surroundings.
Abbreviations
VR, Vocational Rehabilitation; FG, Focus group; BMI, Body Mass Index; RTA, Reflexive thematic analyze; HRQoL, Health-Related Quality of Life; RTW, Return To Work; NAV, Norwegian Labour and Welfare Administration; CASP, Critical Appraisal Skills Programme; REC, Norwegian Regional Committee for Medical and Health Research Ethics Central Norway.
Ethics Approval and Informed Consent
There is a range of approaches to judging the quality of qualitative analysis. In this article, Critical Appraisal Skills Programme (CASP) for qualitative research checklist has been followed.57 This study was approved by the Norwegian Regional Committee for Medical and Health Research Ethics Central Norway (REC) 2017/573 and is registered in Clinical Trials NCT03286374. All written consents to participate in this study followed the laws and guidelines for proper health research and treatment in the Specialised Health Care services in Norway and are in accordance with the Helsinki Declaration. In addition to the written consent, the participants provided verbal informed consent that anonymised findings shared during the FG interviews could be published.
Acknowledgments
The authors thank all the participants who agreed to participate in the FG interviews. They provided their time and effort to give insightful information about their life situation regarding their lifestyle and work ability.
Author Contributions
All authors (A.D.L, C.J, S.K.B and B.H) made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas. Further, they have drafted or written, or substantially revised, or critically reviewed the article and agreed on the journal to which the article will be submitted. In addition, they have reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage. All authors agreed to take responsibility and be accountable for the contents of the article.
Additional information:
ADL. The main investigator designed the study protocol (in close collaboration with B.H), collected data, held responsibility for database quality assessment, analysed and thematised findings (in close collaboration with B.H), integrated theory and finding (in close collaboration with S.K.B) and wrote the first draft of the manuscript and its successive revisions.
SKB. He has made a significant contribution to the integrated theory and finding (in close collaboration with A.D.L).
BH. She has made a significant contribution to the design of the qualitative study, being a moderator in the FG interviews, going through and analysed the interviews together with ADL.
All authors (A.D.L, CJ, SKB, and BH) have agreed to ensure that issues related to the accuracy or integrity of any part of the work, even those in which they were not personally involved, are investigated, resolved and resolution properly documented.
Funding
The Central Norway Regional Health Authority funded this study. Volda University College provided PhD funding for Anita Dyb Linge.
Disclosure
The authors, Anita Dyb Linge, Chris Jensen, Stål Bjørkly and Bente Hasle declare that they have no conflict of interest in this study.
References
1. Rejeski WJ, Williamson D. Effects of lifestyle interventions on health related quality of life and physical functioning. In: Wadden TA, Bray G, editors. Handbook of Obesity Treatment. Guildford Press; 2018:223–240.
2. Colditz GA, Dart H. Epidemiology and health and economic consequences. In: Wadden TA, Bray G, editors. Handbook of Obesity Treatment. Guildford Press; 2018:3–24.
3. Hayes MR. Gut-to-brain mechanisms of body weight regulation. In: Handbook of Obesity Treatment. Vol. 24. Guilford Press; 2018:chap 2.
4. Marlatt LK, Ravussin E. Energy expenditure and obesity. In: Handbook of Obesity Treatment.
5. Wadden TA, Bray GA. Handbook of Obesity Treatment. Guilford Publications; 2018.
6. Tronieri JS, Wadden TA. Behavioral assessment of patients with obesity. In: Handbook of Obesity Treatment. Vol. 2nd. Guilford Press; 2018:253–280.
7. van Rijn RM, Robroek SJW, Brouwer S, Burdorf A. Influence of poor health on exit from paid employment: a systematic review. Occup Environ Med. 2014;71(4):295–301. doi:10.1136/oemed-2013-101591
8. Bajorek Z, Bevan S. Obesity and Work. Vol. 526. Institute for Employment Studies; 2019:0–27.
9. Neovius K, Neovius M, Kark M, Rasmussen F. Association between obesity status and sick-leave in Swedish men: nationwide cohort study. Eur J Public Health. 2012;22(1):112–116. doi:10.1093/eurpub/ckq183
10. Juel K, Sørensen J, Brønnum-Hansen H. Risikofaktorer Og Folkesundhed I Danmark [Risk factors and public health in Denmark]. The National Institute of Public Health; 2006:347.
11. Narbro K, Jonsson E, Larsson B, Waaler H, Wedel H, Sjostrom L. Economic consequences of sick-leave and early retirement in obese Swedish women. Int J Obes Relat Metab Disord. 1996;20(10):895–903.
12. OECD/EU. Health at a Glance: Europe 2016. OECD Publishing; 2016.
13. de Wit M, Wind H, Hulshof CTJ, Frings-Dresen MHW. Person-related factors associated with work participation in employees with health problems: a systematic review. Int Arch Occup Environ Health. 2018;91(5):497–512. doi:10.1007/s00420-018-1308-5
14. Ekberg K, Ståhl C. Employment as a key rehabilitation outcome. In: Bültmann U, Siegrist J, editors. Handbook of Disability, Work and Health. Springer International Publishing; 2020:364–384.
15. Linge AD, Jensen C, Laake P, Bjørkly SK. Lifestyle and work-related factors associated with work ability and work participation for people with obesity: a prospective observational study after vocational rehabilitation. Diabetes Metab Syndr Obes. 2021;14:2943–2954. doi:10.2147/dmso.s311462
16. Svärd A, Lahti J, Mänty M, et al. Weight change among normal weight, overweight and obese employees and subsequent diagnosis-specific sickness absence: a register-linked follow-up study. Scand J Public Health. 2020;48(2):155–163. doi:10.1177/1403494818802990
17. Mancini A, Borel AL, Coumes S, Wion N, Arvieux C, Reche F. Bariatric surgery improves the employment rate in people with obesity: 2-year analysis. Surg Obes Relat Dis. 2018;14(11):1700–1704. doi:10.1016/j.soard.2018.06.026
18. Norwegian Labour and Welfare Administration (NAV). Vocational rehabilitation (Arbeidsrettet rehabilitering). NAV; February 12, 2021.
19. Lippel K. Regulatory contexts affecting work reintegration of people with chronic disease and disabilities: an international perspective. In: Bültmann U, Siegrist J, editors. Handbook of Disability, Work and Health. Springer; 2020:
20. Linge A, Jensen C, Laake P, Bjørkly S. Changes to body mass index, work self-efficacy, health-related quality of life, and work participation in people with obesity after vocational rehabilitation: a prospective observational study. BMC Public Health. 2021;21(1):936. doi:10.1186/s12889-021-10954-y
21. Hees HL, Nieuwenhuijsen K, Koeter MW, Bültmann U, Schene AH. Towards a new definition of return-to-work outcomes in common mental disorders from a multi-stakeholder perspective. PLoS One. 2012;7(6):e39947. doi:10.1371/journal.pone.0039947
22. Sewdas R, de Wind A, Abma FI, Boot CRL, Brouwer S. Personal and environmental factors influencing work participation among individuals with chronic diseases. In: Bültmann U, Siegrist J, editors. Handbook of Disability, Work and Health. Springer International Publishing; 2020:385–398.
23. de Vries H, Fishta A, Weikert B, Rodriguez Sanchez A, Wegewitz U. Determinants of sickness absence and return to work among employees with common mental disorders: a scoping review. J Occup Rehabil. 2018;28(3):393–417. doi:10.1007/s10926-017-9730-1
24. Wadden TA, Butryn ML, Wilson C. Lifestyle modification for the management of obesity. Gastroenterology. 2007;132(6):2226–2238. doi:10.1053/j.gastro.2007.03.051
25. Miller WR, Rollnick S. Motivational Interviewing: Helping People Change. Guilford Press; 2012.
26. Gomez‑Rubalcava S, Stabbert K, Phelan S. Behavioral treatment of obesity. In: Bültmann U, Siegrist J, editors. Handbook of Obesity Treatment.
27. Bandura A. Self-Efficacy: The Exercise of Control. W H Freeman/Times Books/ Henry Holt & Co; 1997:ix, 604–ix, 604.
28. Oellingrath IM, De Bortoli MM, Svendsen MV, Fell AKM. Lifestyle and work ability in a general working population in Norway: a cross-sectional study. BMJ Open. 2019;9(4):e026215. doi:10.1136/bmjopen-2018-026215
29. Sharples AJ, Cheruvu CV. Systematic review and meta-analysis of occupational outcomes after bariatric surgery. Obes Surg. 2017;27(3):774–781. doi:10.1007/s11695-016-2367-x
30. Malterud K. Qualitative research: standards, challenges, and guidelines. Lancet. 2001;358(9280):483–488. doi:10.1016/S0140-6736(01)05627-6
31. Braun V, Clarke V. Successful Qualitative Research: A Practical Guide for Beginners. Sage; 2013.
32. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
33. Braun V, Clarke V, Hayfield N, Terry G. Thematic analysis. In: Liamputtong P, editor. Handbook of Research Methods in Health Social Sciences. Singapore: Springer; 2019:843–860.
34. Braun V, Clarke V. Reflecting on reflexive thematic analysis. Qual Res Sport Exerc Health. 2019;11(4):589–597. doi:10.1080/2159676X.2019.1628806
35. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215. doi:10.1037/0033-295x.84.2.191
36. Collins CS, Stockton CM. The central role of theory in qualitative research. Int J Qual Methods. 2018;17(1):1609406918797475. doi:10.1177/1609406918797475
37. Guba EG, Lincoln YS. Competing paradigms in qualitative research. In: Handbook of Qualitative Research. Sage Publications, Inc; 1994:105–117.
38. Malterud K. Focus Groups as a Research Method in Medicin and Health Science (Fokusgrupper Som Forskningsmetode for Medisin Og Helsefag). Universitetsforlaget; 2012.
39. Kristman VL, Boot CRL, Sanderson K, Sinden KE, Williams-Whitt K. Implementing best practice models of return to work. In: Bültmann U, Siegrist J, editors. Handbook of Disability, Work and Health. Springer International Publishing; 2020:589–613.
40. Schultz IZ, Stowell AW, Feuerstein M, Gatchel RJ. Models of return to work for musculoskeletal disorders. J Occup Rehabil. 2007;17(2):327–352. doi:10.1007/s10926-007-9071-6
41. Young AE, Roessler RT, Wasiak R, McPherson KM, Van Poppel MN, Anema J. A developmental conceptualization of return to work. J Occup Rehabil. 2005;15(4):557–568. doi:10.1007/s10926-005-8034-z
42. Franche RL, Krause N. Readiness for return to work following injury or illness: conceptualizing the interpersonal impact of health care, workplace, and insurance factors. J Occup Rehabil. 2002;12(4):233–256. doi:10.1023/a:1020270407044
43. de Vries HJ, Brouwer S, Groothoff JW, Geertzen JHB, Reneman MF. Staying at work with chronic nonspecific musculoskeletal pain: a qualitative study of workers’ experiences. BMC Musculoskelet Disord. 2011;12(1):126. doi:10.1186/1471-2474-12-126
44. Figueredo J-M, García-Ael C, Gragnano A, Topa G. Well-being at work after return to work (RTW): a systematic review. Int J Environ Res Public Health. 2020;17(20):7490. doi:10.3390/ijerph17207490
45. Mather L, Bergström G, Blom V, Svedberg P. High job demands, job strain, and iso-strain are risk factors for sick leave due to mental disorders: a prospective Swedish Twin study with a 5-year follow-up. J Occup Med Environ Med. 2015;57(8):858–865. doi:10.1097/jom.0000000000000504
46. Rugulies R, Christensen KB, Borritz M, Villadsen E, Bültmann U, Kristensen TS. The contribution of the psychosocial work environment to sickness absence in human service workers: results of a 3-year follow-up study. Work Stress. 2007;21(4):293–311. doi:10.1080/02678370701747549
47. Cancelliere C, Donovan J, Stochkendahl MJ, et al. Factors affecting return to work after injury or illness: best evidence synthesis of systematic reviews. Chiropr Man Therap. 2016;24(1):32. doi:10.1186/s12998-016-0113-z
48. Shaw WS, Reme SE, Linton SJ, Huang YH, Pransky G. 3rd place, PREMUS best paper competition: development of the return-to-work self-efficacy (RTWSE-19) questionnaire–Psychometric properties and predictive validity. Scand J Work Environ Health. 2011;37(2):109–119. doi:10.5271/sjweh.3139
49. Burke LE, Ewing LJ, Ye L, et al. The SELF trial: a self-efficacy-based behavioral intervention trial for weight loss maintenance. Obesity (Silver Spring, Md). 2015;23(11):2175–2182. doi:10.1002/oby.21238
50. Myers CA, Martin CK. Weight loss and changes in psychosocial status and cognitive function. In: Wadden TA, Bray GA, editors. Handbook of Obesity Treatment. Vol. 2nd. Guildford Press; 2018:208–223.
51. Puhl RM, Heuer CA. The stigma of obesity: a review and update. Obesity (Silver Spring, Md). 2009;17(5):941–964. doi:10.1038/oby.2008.636
52. Gregg EW, Flores MR. The impact of intentional weight loss on major morbidity and mortality. In: Handbook of Obesity Treatment.
53. de Vries G, Hees HL, Koeter MWJ, Lagerveld SE, Schene AH. Perceived impeding factors for return-to-work after long-term sickness absence due to major depressive disorder: a concept mapping approach. PLoS One. 2014;9(1):e85038. doi:10.1371/journal.pone.0085038
54. Rydström I, Dalheim Englund L, Dellve L, Ahlstrom L. Importance of social capital at the workplace for return to work among women with a history of long-term sick leave: a cohort study. BMC Nurs. 2017;16:38. doi:10.1186/s12912-017-0234-2
55. Loisel P, Buchbinder R, Hazard R, et al. Prevention of work disability due to musculoskeletal disorders: the challenge of implementing evidence. J Occup Rehabil. 2005;15(4):507–524. doi:10.1007/s10926-005-8031-2
56. Etuknwa A, Daniels K, Eib C. Sustainable return to work: a systematic review focusing on personal and social factors. J Occup Rehabil. 2019;29(4):679–700. doi:10.1007/s10926-019-09832-7
57. Critical Appraisal Skills Programme. CASP qualitative studies checklist. Available from: https://casp-uk.net/wp-content/uploads/2018/03/CASP-Qualitative-Checklist-2018_fillable_form.pdf.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.