")
Back to Journals » International Medical Case Reports Journal » Volume 15
Balantidium coli; Rare and Accidental Finding in the Urine of Pregnant Woman: Case Report
Authors Almaw A , Berhan A , Solomon Y , Malkamu B , Eyayu T , Workineh L , Mekete G , Yayehrad AT
Received 6 January 2022
Accepted for publication 12 March 2022
Published 22 March 2022 Volume 2022:15 Pages 105—109
DOI https://doi.org/10.2147/IMCRJ.S355536
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Andargachew Almaw,1 Ayenew Berhan,1 Yenealem Solomon,1 Birhanemaskal Malkamu,1 Tahir Eyayu,1 Lemma Workineh,1 Getachew Mekete,2 Ashagrachew Tewabe Yayehrad3
1Department of Medical Laboratory Science, Debre Tabor University, Debre Tabor, Ethiopia; 2Department of Anesthesia, Debre Tabor University, Debre Tabor, Ethiopia; 3Department of Pharmacy, Bahir Dar University, Bahir Dar, Ethiopia
Correspondence: Andargachew Almaw, Tel +251925987855, Email [email protected]
Background: Balantidium coli is a ciliated protozoan parasite, which causes intestinal and extraintestinal infections in humans. It is transmitted feco-orally by ingesting infective cysts with food and water. Urinary balantidiasis may occur through contamination (direct spread from the anal area), secondarily to rectovaginal fistula and following immune suppression. Data about cases of urinary balantidiasis are rare in the world. Currently, there are no documented reports of urinary balantidiasis in Ethiopia. As our understanding, there are only eleven documented reports of urinary balantidiasis globally. However, cases of urinary balantidiasis among pregnant women have not been documented yet. The aim of this report is to alarm health professionals for considering the occurrence of such rare cases and conduct diagnosis.
Case Presentation: A 24-year old pregnant woman was admitted due to severe preeclampsia and preterm delivery at Debre Tabor Comprehensive Specialized Hospital, gynecology ward. Her urine was presented to inpatient laboratory for routine urinalysis. We detected unusual and ciliated parasite from her urine sediment characterized by its active and rotary motility through its cilia and possessing macro- and micro-nuclei, several food vacuoles and ingested red blood cells inside the cytoplasm. Hematuria, many white blood cells and epithelial cells were also detected from the urine sediment, which suggests genito-urinary tract infection due to this parasite. This rare parasite finding was confirmed to be B. coli.
Conclusion: The route of transmission and extraintestinal existence from this woman’s urine was unclear. It might be due to feco-oral transmission and spread to the genitourinary tract through direct anal contact. Moreover, it might be associated with immune suppression as she is pregnant woman.
Keywords: Balantidium coli, urine, pregnant, Ethiopia
Background
Balantidium coli (B. coli) is the largest intestinal protozoan parasite found to infect gastrointestinal tract of humans. It is the only ciliated protozoan parasite that infects humans and other primates.1 Although the infection occurring due to B. coli mostly remains asymptomatic, it may invade the intestinal mucosa and result in fatal balantidial dysentery (balantidiasis) resembling that of E.histolytica.1
B. coli infection encompasses worldwide distribution. However, the prevalence of the disease among humans is highly limited because of its asymptomatic nature in most cases. In humans, the infection is found mostly in areas of tropical and subtropical regions and developing countries; with poor environmental and sanitary conditions.2 Evidences indicate that, the parasite is mainly endemic in Philippines, Papua New Guinea, Pacific Islands, Central and South America, and central Asia.2–5
The prevalence of B. coli in human hosts may vary from 0.02% to 1%.2,6,7 These low frequencies may not represent the real occurrence and prevalence of the parasite as it usually remains asymptomatic and under reported. Higher prevalence of the infection among humans was reported from different regions including Latin America, the Philippines, Papua New Guinea, and the Middle East, with about 29% reports among pig farmers.2,5,8,9 The main mode of transmission for B. coli is feco-oral route, usually occurring via ingestion of food and water contaminated with the cyst stage.2 It has been postulated that trophozoites might also be infective if ingested immediately within few hours after passage.10 The disease is mainly zoonotic with pigs, rodents, wild boars, sheep, goats, camels and horses serving as reservoirs of the infection. Pigs and wild boars are considered to be the most important reservoirs.2,11–14
However, the parasite may cause extra intestinal infections especially in immune suppressed individuals through dissemination into appendix,15 liver,16 peritoneum,17 lung,18 and genitourinary tract.19 In females, the genitourinary tract infections like uterine infection, vaginitis, and cystitis may occur through direct spread from the anal area and secondary to the rectovaginal fistula.20 This paper reports rare, accidental and asymptomatic urinary balantidiasis from urine sediment of pregnant woman admitted in Debre Tabor Comprehensive Specialized Hospital, North West Ethiopia and requested for routine urinalysis.
Case Report
A 24 years old pregnant woman was admitted in Debre Tabor Comprehensive Specialized Hospital gynecology ward due to severe preeclampsia and preterm delivery. She did not have signs and/or symptoms of balantidiasis. She had no history of smoking, drinking alcohol, and other underlying chronic diseases. However, her caregiver health professional sent urine sample for routine urinalysis test to the inpatient laboratory department.
The urine physically appeared to be somewhat dark and turbid with little foam. The chemical examination (Agape ™ Urine Reagent Strips test kit) results revealed; Specific gravity of 1.01, pH=6.0, Albumin=1+, blood=3+ (hematuria), and Leucocyte=2+ (leucocyturia) which may be indicative of urinary tract infection (UTI). From the microscopic examination of centrifuged (3600RPM for 3 minutes) urine sediment, we found motile and ciliated parasite together with many white blood cells /high power field (HPF) and many epithelial cells/low power field (LPF). The processing of urine was conducted within five minutes after passage. The urine sediment repeated in the next morning revealed similar result.
The ciliated parasite appeared to be ovoid with rapid motility in circular fashion under the microscope slide. The entire body of the parasite was enclosed with short and uniform cilia which aided its motility. But, the cilia around the mouth appeared to be longer and clearly visible than the others. The parasite possessed the mouth part that was found at pointed anterior end (cytostome) and rounded posterior end (cytopyge). In addition, the body of the parasite contained several food vacuoles, macro- and micro-nuclei, and some red blood cells inside the cytoplasm. This parasite with unique morphological characteristics was confirmed by medical parasitologists and experienced microscopists jointly to be B. coli. We did not have gone to further staining of the parasite as we easily and correctly confirmed it with microscopy.
However, this was incidental and strange finding from the urine and it has never been detected here even from stool. The stool sample was collected from the patient. The stool physically appeared formed. But, it was found negative for the parasite. Finally, the finding was reported to the concerning health care giver for intervention and additional information was collected if she had contact with risk factors. But, she had no history of contact with pigs. She came from rural area where goats, sheep and other domestic animals are always in close contact with humans. She also had history of feeding raw vegetables. In addition, there are monkeys around the area which might have contaminated the vegetables she ingested.
Discussion
Balantidiasis is zoonotic disease transmitted by ingestion of food and water contaminated with cyst stage (feco-oral). After ingestion, the cysts release the pathogenic trophozoites which live in the large intestine and reproduce by binary fission.1 Many of the infected individuals may remain asymptomatic or few may develop different gastrointestinal symptoms. In some occasions, the trophozoites may disseminate to extraintestinal sites through blood circulation and metastasis through invasion and perforation of intestinal mucosa.21
This pregnant woman did not have history of contact with pigs. But, the risk factor for her case may be her usual close contact with domestic cattle22,23 and her history of feeding raw vegetables which is one of the transmission mechanisms.24 The parasite might have invaded urinary tract of this woman by direct spread through the anal area or metastasis via blood stream.21 Hematuria and leucocyturia from her urine might have been due to B. coli.
Moreover, it has been estimated that immune suppression is among the important factors favouring the spread of urinary balantidiasis. Different reports have documented cases of urinary balantidiasis due to immune suppression following the underlying disease conditions.9,21, Similarly, immunity declines during pregnancy. In addition to the above suggestions from her history, this pregnant woman might have acquired urinary balantidiasis due to her immune suppression. The stool sample collected from the patient, which appeared formed in consistency revealed negative result. She has history of dysentery three weeks ago and has taken treatments of amoebiasis.
B. coli in urine (urinary balantidiasis) is a rare finding. This is the first case report of urinary balantidiasis among pregnant women in Ethiopia and in the world. Currently, there are about eleven documented cases of urinary balantidiasis reported globally. Single cases reported from Iran,21 Italy,25 Slovenia26 and Thailand27 while, seven cases were reported from India (Table 1).20,28–32
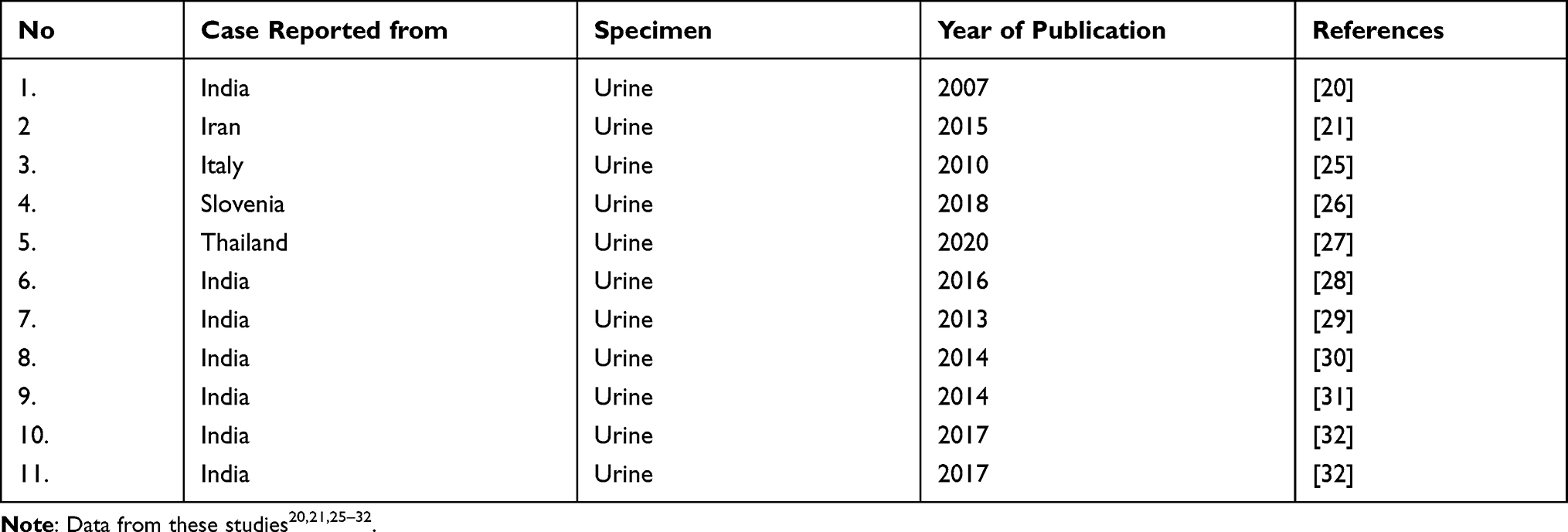 |
Table 1 Documented Case Reports of Urinary Balantidiasis |
Conclusion
B. coli is ciliated protozoan parasite with worldwide distribution. It is transmitted feco-orally through ingestion of infective cysts with food and water. It invades the intestine and causes intestinal infection, mainly balantidial dysentery. It may also cause extraintestinal infections of liver, lung, peritoneum and genitourinary tract. Urinary infections occur through direct spread from the anal area and secondarily to rectovaginal fistula. In addition, the spread of urinary balantidiasis is associated with immune suppressed states like pregnancy. The parasite can be easily detected from urine sediment by light microscope through its characteristic ciliated and rapid rotary movement.
Ethical Consideration
Approval letter for publication was obtained from Medical Laboratory Science department academic council (DAC).
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report.
Funding
No funding is available.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ponce-Gordo F, Jirků-Pomajbíková K. Balantidium coli. In: Rose JB, Jiménez-Cisneros B, editors. Water and Sanitation for the 21st Century: Health and Microbiological Aspects of Excreta and Wastewater Management (Global Water Pathogen Project). UNESCO-International Hydrological Programme (Michigan State University); 2017. doi:10.14321/waterpathogens.30
2. Schuster FL, Ramirez-Avila L. Current world status of Balantidium coli. Clin Microbiol Rev. 2008;21:626–638. doi:10.1128/CMR.00021-08
3. Fletcher SM, Stark D, Harkness J, Ellis J. Enteric protozoa in the developed world: a public health perspective. Clin Microbiol Rev. 2012;25:420–449. doi:10.1128/CMR.05038-11
4. Kline K, McCarthy JS, Pearson M, Loukas A, Hotez PJ. Neglected tropical diseases of Oceania: review of their prevalence, distribution, and opportunities for control. PLOS Negl Trop Dis. 2013;7:1755. doi:10.1371/journal.pntd.0001755
5. Owen IL. Parasitic zoonoses in Papua New Guinea. J Helminthol. 2005;79:1–14. doi:10.1079/JOH2004266
6. Boonjarsapinyo S, Boonmars T, Kaewsamut B, et al. A cross sectional study on intestinal parasitic infections in rural communities, Northeast Thailand. Korean J Parasitol. 2013;51:727–734. doi:10.3347/kjp.2013.51.6.727
7. Walzer PD, Healy GR. Balantidiasis. In: CRC Handbook Series in Zoonoses. Section C. Parasitic Zoonoses. CRC Press, Inc; 1982:15–24.
8. Solaymani-Mohammadi S, Rezaian M, Anwar MA. Human balantidiasis in Iran: an unresolved enigma? Trends Parasitol. 2005;21:160–161. doi:10.1016/j.pt.2005.02.001
9. Yazar S, Altuntas F, Sahin I, Atambay M. Dysentery caused by Balantidium coli in a patient with non-Hodgkin’s lymphoma from Turkey. World J Gastroenterol. 2004;10:458–459. doi:10.3748/wjg.v10.i3.458
10. Pomajbíková K, Petrželková KJ, Profousová I, Modrý D, Modrý D. Discrepancies in the occurrence of Balantidium coli between wild and captive African great apes. J Parasitol. 2010;96:1139–1144. doi:10.1645/GE-2433.1
11. Hindsbo O, Nielsen CV, Andreassen J, et al. Age-dependent occurrence of the intestinal ciliate Balantidium coli in pigs at a Danish research farm. Acta Vet Scand. 2000;41:79–83. doi:10.1186/BF03549657
12. Ismail HA, Jeon HK, Yu YM, Do C, Lee YH. Intestinal parasite infections in pigs and beef cattle in rural areas of Chungcheongnam-do, Korea. Korean J Parasitol. 2010;48:347. doi:10.3347/kjp.2010.48.4.347
13. Weng YB, Hu YJ, Li Y, et al. Survey of intestinal parasites in pigs from intensive farms in Guangdong Province, People’s Republic of China. Vet Parasitol. 2005;127:333–336. doi:10.1016/j.vetpar.2004.09.030
14. Yin DM, Lv CC, Tan L, et al. Prevalence of Balantidium coli infection in sows in Hunan province, subtropical China. Trop Anim Health Prod. 2015;47:1637–1640. doi:10.1007/s11250-015-0904-6
15. Dodd LG. Balantidium coli infestation as a cause of acute appendicitis. J Infect Dis. 1991;163:1392. doi:10.1093/infdis/163.6.1392
16. Kapur P, Das AK, Kapur PR, Dudeja M. Balantidium coli liver abscess: first case report from India.. J Parasit Dis. 2014;40:138–140. doi:10.1007/s12639-014-0464-0
17. Ferry T, Bouhour D, De Monbrison F, et al. Severe peritonitis due to Balantidium coli acquired in France. Eur J Clin Microbiol Infect Dis. 2004;23:393–395. doi:10.1007/s10096-004-1126-4
18. Sharma S, Harding G. Necrotizing lung infection caused by the protozoan Balantidium coli. Can J Infect Dis. 2003;14:163–166. doi:10.1155/2003/829860
19. Rivasi F, Giannotti T. Balantidium coli in cervico-vaginal cytology. A case report. Pathologica. 1983;75:439–442.
20. Umesh S. Balantidium coli on urine microscopy. Natl Med J India. 2007;20:270.
21. Soleimanpour S, Babaei A, Roudi AM, Raeisalsadati SS. Urinary infection due to Balantioides coli: a rare accidental zoonotic disease in an addicted and diabetic young female in Iran. JMM Case Rep. 2015;3:e000102.
22. Levine ND. Veterinary Protozoology. Iowa State University Press, Ames; 1985.
23. Levine ND. Protozoan Parasites of Domestic Animals and of Man. Smithsonian Institution; 1961.
24. Nyirenda SS, Bukowa KM, Banda WR, et al. Parasitic contamination of common vegetables sold in Lusaka, Zambia. J Food Qual Hazards Control. 2021;8:112–118.
25. Maino A, Garigali G, Grande R, Messa P, Fogazzi GB. Urinary balantidiasis: diagnosis at a glance by urine sediment examination. J Nephrol. 2010;23:732–737.
26. Tanja PZ, Yu WK, Natasa KK. Urinary balantidiasis: a rare incidental finding in a patient with psoriasis. J Antimicrob Agents. 2018;4:177. doi:10.4172/2472-1212.1000177
27. Martviset P, Sirisabhabhorn K, Pumpa S, Rhongbutsri P, Taylor A, Taylor WRJ. Urinary balantidiasis in a patient with systemic lupus erythematosus and lupus nephritis: a case report. J Med Case Rep. 2020;14(1):63. doi:10.1186/s13256-020-02389-7
28. Kaur S, Gupta A. Urinary balantidiasis: a rare incidental finding in a patient with chronic obstructive pulmonary disease. J Cytol. 2016;33:169–171. 4. doi:10.4103/0970-9371.188063
29. Bandyopadhyay A, Majumder K, Goswami BK. Balantidium coli in urine sediment: report of a rare case presenting with hematuria. J Parasit Dis. 2013;37:283–285. doi:10.1007/s12639-012-0163-7
30. Karuna T, Khadanga S. A rare case of urinary balantidiasis in an elderly renal failure patient. Trop Parasitol. 2014;4:47–49. doi:10.4103/2229-5070.129165
31. Khanduri A, Chauhan S, Chandola I, Mahawal B, Kataria V. Balantidiosis: a rare accidental finding in the urine of a patient with acute renal failure. J Clin Diagn Res. 2014;8:DD03–DD04. doi:10.7860/JCDR/2014/7033.4343
32. Gupta S, Bharati P, Sinha KP. Balantidium coli: rare urinary pathogen or faecal contaminant in urine? Case study and review. J Dent Med Sci. 2017;16:88–90.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.