Back to Journals » Infection and Drug Resistance » Volume 15
Bacterial Contamination and Susceptibility Pattern Among Blood and Blood Components Using Divergent and Non-Divergent Collection Methods at Armed Forces Comprehensive Specialized Hospital, Addis Ababa, Ethiopia
Authors Tsegaye W, Bitew A, Gize A ![]()
Received 29 January 2022
Accepted for publication 25 March 2022
Published 8 April 2022 Volume 2022:15 Pages 1677—1686
DOI https://doi.org/10.2147/IDR.S360515
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Wondwossen Tsegaye,1 Adane Bitew,2 Addisu Gize3
1Department of Diagnostic Medical Laboratory and Radiology, Defense University, Bishoftu, Ethiopia; 2Department of Medical Laboratory Sciences, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 3Department of Microbiology, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
Correspondence: Addisu Gize, Email [email protected]
Background: Understanding the proportion of blood and blood products contamination during transfusion is important in developing infection control strategy in the health system. Therefore, this study was aimed to determine bacterial contamination and susceptibility patterns among blood and blood components at Armed Forces Comprehensive Specialized Hospital, Addis Ababa, Ethiopia.
Methods: A cross-sectional study was done on blood and blood components collected with both diverging and none-diverging methods. Simple random sampling method was applied to select blood and blood product units from the record form and 10 mL of sample was drawn from each blood and blood product. Culturing from collected blood and blood products and antimicrobial sensitivity tests were done. The collected data were entered and analyzed by SPSS statistical software version 20. Binary and multiple logistic regression analysis were done to see different factors and p-values less than 0.05 were taken as statistically significant.
Results: A total of three hundred seventy six (376) units of blood and blood product samples, 188 from non-diverging and 188 from diverging blood donor collection methods were included. Among different blood group types, O+ blood and the majority of components were stored from one to five days. The overall bacterial contamination among blood and blood components were n = 17 (4.5%). Among them, n = 14 (7.4%) and n = 3 (1.6%) were collected with a non-diverging and diverging method, respectively. Staphylococcus epidermidis was the most dominant isolate. Most bacterial isolates were susceptible to different antimicrobial agents; however, Pseudomonas aeruginosa showed resistance for gentamicin. The non-diverging collection units of blood and components were significantly associated with bacterial contamination. Of all, n = 5/17 (29.4%) isolated bacteria were multidrug resistant.
Conclusion: The bacterial contamination of blood and blood components collected with diverging method was lower and recommended to use this collection method from donors.
Keywords: bacterial contamination, diverging and non-diverging method, blood culture, susceptibility pattern
Introduction
After the discovery of blood circulation, the first recorded thriving blood transfusion was from dogs to dogs and then, lamb to human being. In the 1800s, the blood transfusion was started among human beings then after the outcome became successful.1 The need for blood and blood products transfusion demand was very increase significantly after the discovery of practical anticoagulation and the ABO blood groups at the start of the 20th century.2
Blood transfusion is a medical mediation planned to offer protected blood products for those who need them.3 Nevertheless, Transfusion Transmitted Infection (TTI) can be transferred from blood products to recipients. Common TTI causative agents and bacteria can be screened from blood.4 Bacterial contamination of blood products could be the causation for morbidity and mortality when transfused them to patients.5
In the half of 1990s, it was documented in the case report about bacterial transmission and this interest depicted by the blood community.6 Either skin commensals or gastrointestinal tract flora which accounts for 75% are the principal gram-positive aerobic pathogens.7
Blood products may be infected during blood collection, inadequate disinfection of donor skin, processing and accidents on blood bags. In addition to that, they can also be infected from asymptomatic bacteremia in the donor.8 In developed countries, the incidence of bacterial contamination and its related transfusion transmitted bacterial infection (TTBI) has been greatly condensed as a result of proper donor screening,9 use of enhanced donor skin decontamination method and diverting the first blood volume.10 As opposed to developed countries, developing countries do not put into practice the above measures.8
African’s, bacterial contamination; gained through collection and processing, is 2500 times higher than developed countries. Moreover, visual examination of blood bags for hemolysis is the most common means of detecting for bacterial contamination.11
The studies done in Ethiopia showed significant and variable prevalence of bacterial contaminations and their antimicrobial susceptibility pattern among whole blood collected by the non-diverging method11,12 but not with diverging method. To this end, the aim of the current study was to determine bacterial contamination of blood products collected by two different donor blood collection methods.
Materials and Methods
Study Settings
A cross-sectional study was conducted from January 2017 to April 2018 at Armed Forces Comprehensive Specialized Hospital (AFCSH), Addis Ababa, Ethiopia. The hospital provides medical service to members of the Ethiopian defense forces, their family and community. AFCSH has 15 wards with 600 beds. There are 378 healthcare professionals with different levels and field of training. Based on the 2016/17 annual report, the hospital provides services for 100,005 outpatients and 4229 inpatients as well as 962 deliveries and 295,549 Laboratory investigations. On average, about 8–12 units of blood and blood components are transfused daily. In 2016/17, the maximum annual required blood and blood components were 4818 units of blood and blood components. The hospital has the access to received blood and blood components that were collected by diverging method from Ethiopia National Defense Forces Blood Bank Service (ENDFBBS) and non-diverging one from Ethiopia National Blood Bank Service (ENBBS).
All blood and blood components collected from ENBBS and ENDFBBS for transfusion purpose during the study period were the source and those delivered from ENBBS and ENDFBBS for were study population.
All units of blood and blood components which were ready for transfusion were included, units which have expired dates and those bags which showed any leakage were excluded from the study.
Study Variables
Bacterial contamination in blood, blood components, and susceptibility pattern were the dependent variable and, diverging and non-diverging method of blood collection from the donors’, storage time, types of blood and blood components were some of independent variables.
Operational Definition
Blood components: specific parts which can get from donated whole blood such as PRBC, FFP and Platelets.
Diverging method: a blood collection method applied by changing the first 30–40 milliliters flow of venipuncture blood direction into diverging pouch to reduce fragments and contamination from the skin and air.Non-diverging method: a donor blood collection method which used to collect blood without changing the first flow of venipuncture blood direction.
Multidrug resistant (MDR): bacteria resistant for more than two different antibiotics classes.
Sample Size Determination and Techniques
The sample size was calculated based on two population proportion formula. The value of P1 was taken as 15.33%11 from the previous study on whole blood and P2 as 50%. Considered 95% confidence interval and commonly used values for Cp, power; C0.05, 95%, were 13. We took 47 units from whole blood, 47 units from Packed Red Blood Cells (PRBC), 47 units from Fresh Frozen Plasma (FFP) and 47 units from Platelet Concentrate (PC) for each diverging and non-diverging method, which resulted as a total of 376 units of blood and blood components. These units of blood and blood components were selected using simple random sampling method from the recording log book of transfusion laboratory.
Data Collection Procedure
Information like unit number, types of blood and blood components, types of blood group, collection and expiry date and storage temperature were obtained from each unit of labeled blood and blood components of bags and from the recorded log book of the transfusion laboratory.
Laboratory Procedures
Each unit of whole blood and Packed Red Blood Cells (PRBCs) was mixed before sampling with hand shaking and striper and then we detached 20–25 cm segment after sealed the tubing at 5–10 cm away from the end of each blood bag’s tubing. Each detached segment was labeled with coded labeling paper. In the biological safety cabinet, each unit of Fresh Frozen Plasma (FFP) and Platelet segments were detached and decontaminated first using packed swab saturated with 70% isopropyl alcohol and waited for one minute and then with 2% tincture iodine then waited for three minutes. In the sterilized brain-heart infusion (BHI) broth (Oxoid, Basingstoke, UK) blood culture bottle, 3 mL of blood samples were drawn from each segment using sterile disposable syringe and then dispensed into 15 mL of BHI broth aseptically. The specimens were delivered to the AFCSH Microbiology laboratory incubation room for isolation, bacterial species identification and antimicrobial susceptibility testing.13
Bacterial Isolation and Identification
The inoculated BHIs were incubated at 37 °C aerobically, and then observed daily for any possible signs of bacterial growth such as pellicle formation, hemolysis, gas formation, clotting and turbidity for 7 days. After overnight incubation, the BHI bottles were mixed, then one mL blood sample was taken from the bottle with a sterile disposable syringe and subculture two drops of samples were sub cultivated on to sheep Blood Agar Plate (BAP), MacConkey Agar Plate (MAP) and Chocolate Agar Plate (CAP) after overnight incubation. Inoculated BHI bottles; that show bacterial growth at 2 to 7 days, were also sub-cultured on sheep BAP, MAP, and CAP and also again sub-cultured until we got the pure colony. The inoculated MAP was incubated aerobically but BAP and CAP were incubated with 5–10% CO2 atmosphere overnight. Whenever bacterial growth was observed on the incubated media, identification of bacterial species was done based on bacterial cultural characteristics, Gram stain and biochemical tests. The home-brew biochemical tests biochemical tests were done depending on their Gram reaction result. For Gram-positive bacteria, we used catalase, coagulase, CAMP, bile esculin, novobiocin, TSI tests and so on. We also used for Gram-negative bacteria TSI, citrate, indole, motility, urease, and oxidase. The result of biochemical referred to the chart of Gram-negative and positive bacteria to identify the species level of the bacteria. In addition, differential media like Mannitol salt agar was used to differentiate staphylococci species.14
Antibiotic Susceptibility Testing
The antibiotic susceptibility testing was performed according to Kirby-Bauer disk diffusion method on Mueller Hinton Agar plates (MHA). By comparing the bacterial cell suspension to a ready-made 0.5 McFarland standards, we were able to achieve turbidity standardization. Antibiotics were selected based on the recommendation of clinical and laboratory standards institute guideline (CLSI).15 The known volume and concentration of recommended antibiotics for Gram-positive bacteria such as amikacin (30 μg), cefoxitin (30 μg), clindamycin (2 μg), erythromycin (15 μg), penicillin (10 μg), gentamicin (10 μg), trimethoprim-sulphamethoxazole (1.25/23.75 μg), tobramycin (10 μg), ceftriaxone (30 μg), ampicillin (10 μg), chloramphenicol (30 μg) and cefotaxime (30 μg) and also antibiotics for Gram-negative bacteria like amikacin (30 μg), amoxicillin+ clavuninic acid (10/20 μg), cefepime (30 μg), ceftriaxone (30 μg), ciprofloxacin (5 μg), gentamicin (10 μg), meropenem (10 μg), piperacillin-tazobactam (10/100 μg), tobramycin (10 μg) and trimethoprim-sulphamethoxazole (1.25/23.75 μg) were (li_60) used. The zone of inhibition of those drugs was measured after 18–24 hours inculcation to the adjacent millimeter of the caliper. Interpretation of identified bacteria as susceptible, intermediate, or resistant according to the recent CLSI specified interpretive criteria.15
Data Quality Control
Using aseptic techniques and following Standard Operating Procedures (SOPs), units of blood and blood component information’s such as unit number, blood group, collection date, expiration date and types of blood and components were collected. Additionally, we used quality control strains such as Geobacillusstermophilus (ATCC 7953), Staphylococcus aureus (ATCC 25923), Staphylococcus epidermidis (ATCC 12228), Escherichia coli (ATCC 25922), Pseudomonas aeruginosa (ATCC 27853), Enterococcus faecalis (ATCC 29212), Streptococcus pyogenes (ATCC 19615), Proteus mirabilis (ATCC 35659) and Klebsiella pneumonia (ATCC 13883).
Data Analysis
Data entered and analyzed using SPSS statistical software version 20. Binary logistic regression analysis was used to see the association between the dependent and independent variables and to assess their significance level. In all cases, p-value, less than or equal to 0.05 were considered as statistically significant. Finally, the results were presented in words, percentages, graphs and tables.
Ethical Considerations
An ethical clearance with reference number SR/LS/019/18 was obtained from ethics and research committee, department of medical laboratory Sciences, School of Allied Health Sciences and College of Health Sciences of Addis Ababa University. Permission was obtained from the AFCSH administrator. Samples were coded and the confidentiality of donors’ blood was maintained throughout the study. Information was given to the AFCSH laboratory director about those blood and blood components units which showed bacterial growth to take any action.
Results
In this study, we included 376 blood samples from blood and blood products which were collected with both blood donor collection methods and delivered to AFCSH with equal proportion. Of this, blood group O with Rh-positive was the highest to be examined which accounts 137 (36.4%). The minimum and maximum storage temperatures for whole blood were 3.5 and 5 °C, PRBC 3.5 and 4.8 °C, FFP −40 and −38 °C and for platelet 23 and 25 °C. Among the different types of blood products, majority of the storage time of whole blood, PRBC, FFP and platelet were up to 1 week accounts 26 (27.7%), 1–2 week 51 (54.3%), more than six weeks 30 (31.9%) and 1–5 days 94 (100%) respectively (Table 1).
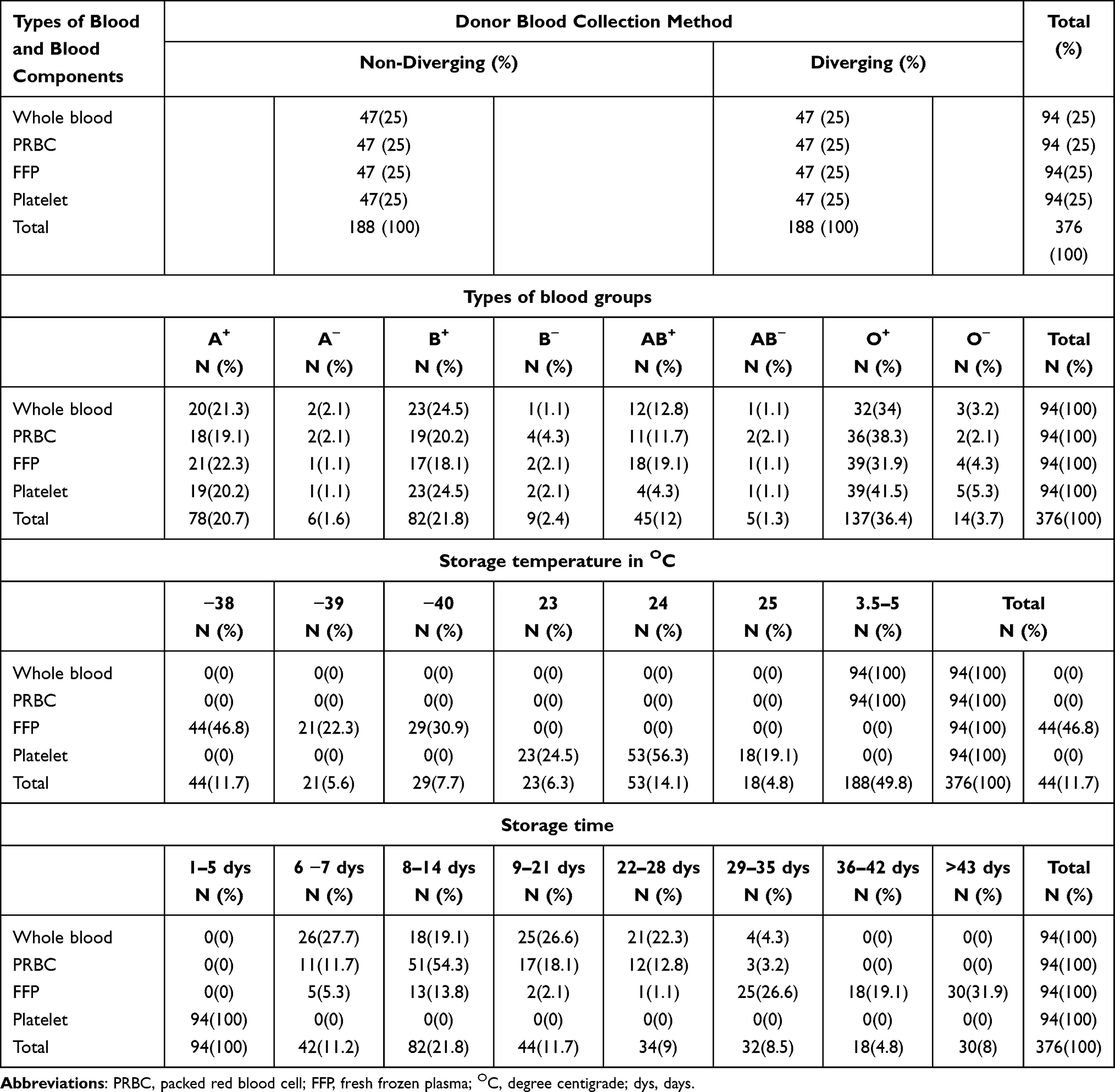 |
Table 1 Sample Characteristics of Blood and Blood Components in AFCSH Addis Ababa City, Ethiopia, 2018 |
The overall bacterial contamination among blood products was n=17 (4.5%). Of these, whole blood and PRBC took the highest to be contaminated with bacteria n=6 (35.3%). In addition, the most contaminated blood group type was O Rh-positive n=6 (35.3%). From the overall bacterial contamination, both Gram-positive and Gram negative were isolated. Of the, Gram-positive bacteria, n=14 (82.4%) took the largest number and Gram-negative bacteria accounted; n=3/ (17.6%). The most frequent isolated bacteria were Staphylococcus epidermidis; n=6 (35.3%) followed by Staphylococcus aureus; n=4/ (23.5%).
The bacterial contamination from those blood products which were collected with non-diverging; n=14 (7.4%) was higher than diverging method=3(1.6%). In addition, PRBC n=5 (2.7%) was the most bacterial contaminated one prior to whole blood n=4 (2.1%) from those collected with non-diverging. There was a statistical significant association between blood donor collection method and bacterial contamination (AOR (CI): 7.8 (1–60.1), p-value: 0.05) (Table 2).
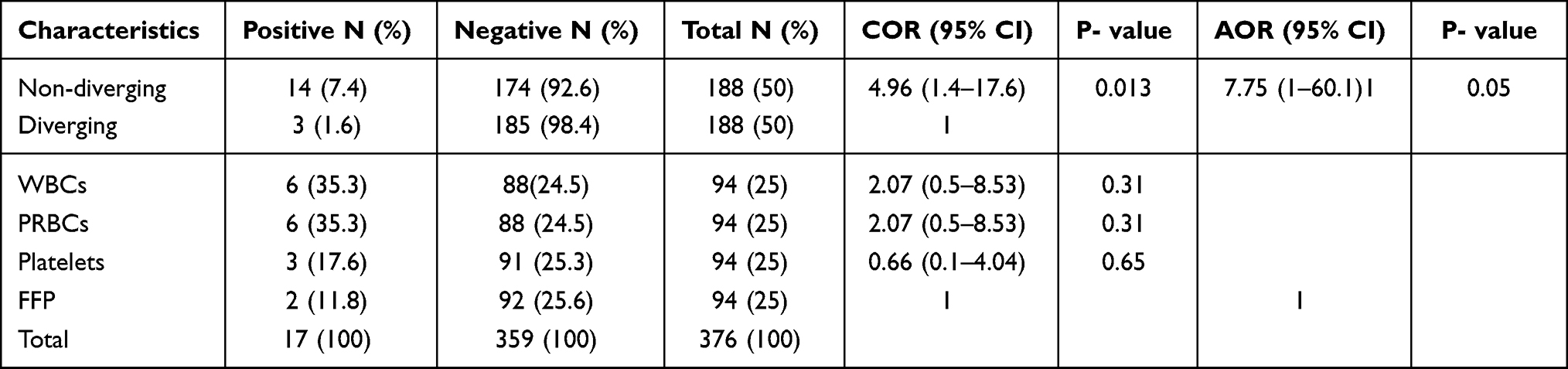 |
Table 2 Multivariable Analysis of Bacterial Contamination Among Blood and Blood Components at AFCSH, Ethiopia, 2018 |
The most frequently isolated bacterium from blood products collected with non-diverging and diverging method was Staphylococcus epidermidis (n= 4, 28.57%) and (n = 2, 66.7%) respectively.
Among gram positive bacteria such as Staphylococcus aureus, Staphylococcus epidermidis, Listeria monocytogenes and Listeria species which were isolated from those blood products collected with non-diverging method. Most isolates were sensitive to ceftriaxone (100%), ampicillin (100%), tobramycin (100%) and cefotaxime (100%) antibiotics. High resistant were observed for trimethoprim-sulphamethoxazole (27%) and erythromycin (27%) antibiotics. Similarly, Gram-negative isolates were sensitive for the antibiotics such as amoxicillin+ clavulanic acid (100%), piperacillin-tazobactam (100%), cefepime (100%), ceftriaxone (100%), tobramycin (100%), amikacin (100%), ciprofloxacin (100%) and trimethoprim-sulphamethoxazole (100%). The only isolates which showed (33.3%) resistant to gentamicin was Pseudomonas aeruginosa (Tables 3 and 4).
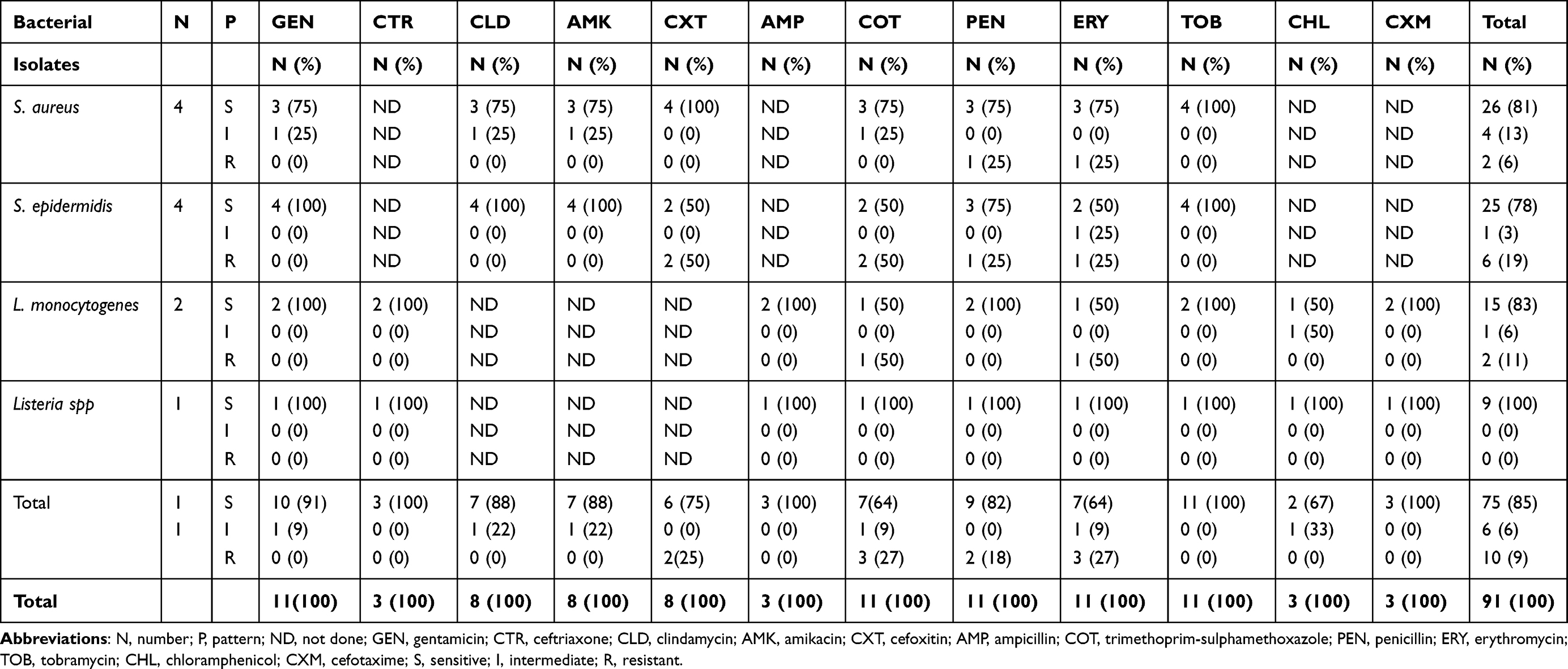 |
Table 3 Antimicrobial Susceptibility Pattern of Gram-Positive Bacteria Collected by Non-Diverging Method, 2018 |
 |
Table 4 Antimicrobial Susceptibility Pattern of Gram-Negative Bacteria Collected by Non-Diverging Method, 2018 |
Staphylococcus epidermidis and Listeria spp were isolated from blood and blood components collected with diverging blood collection method.
Among the isolated organisms, 5(29.4%) were shown to be multidrug resistant, and Staphylococcus epidermidis which accounted 3(17.6%) took the highest MDR bacteria (Table 5).
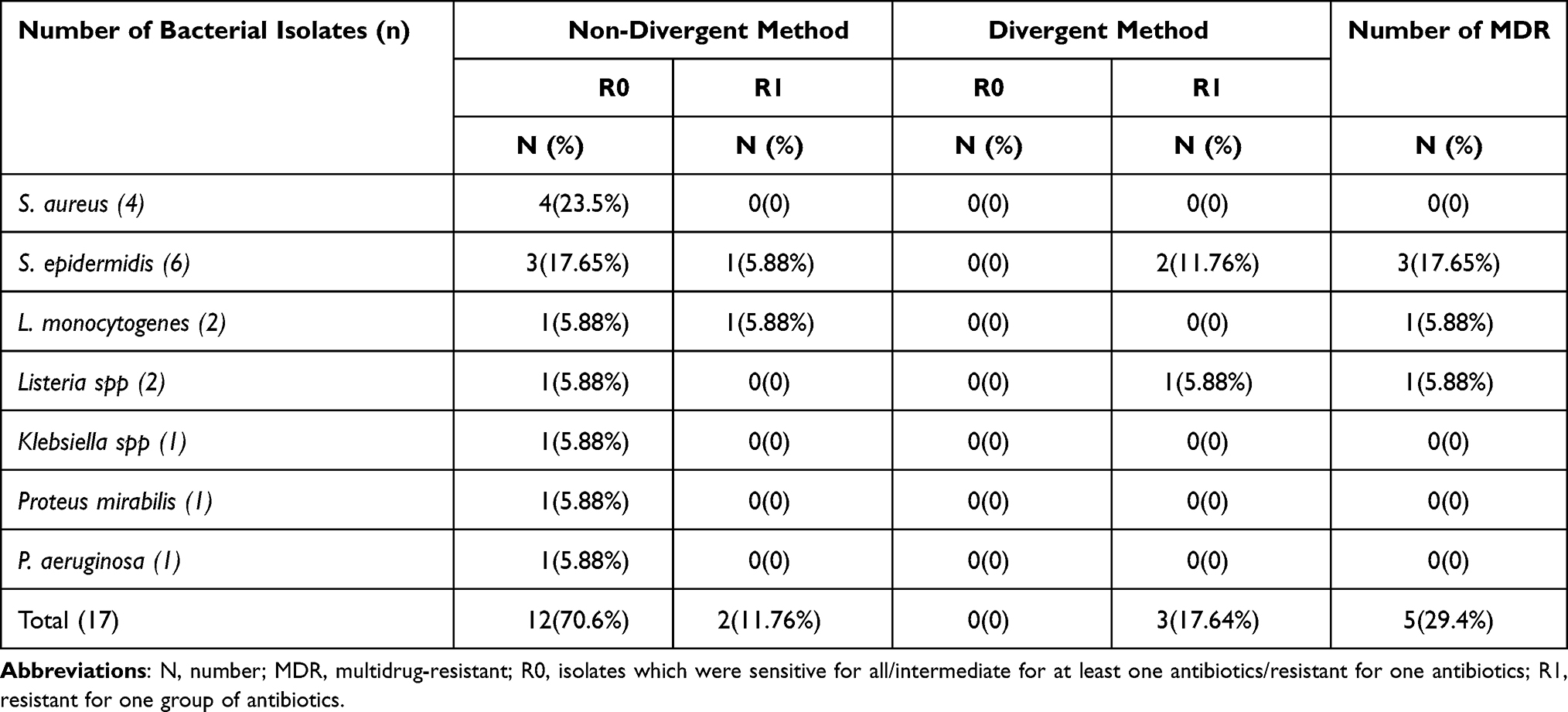 |
Table 5 Multidrug Resistant Level of Isolated Bacteria Collected by Non-Diverging and Diverging Method, 2018 |
Discussion
The awareness of bacterial contamination among blood products which are used for blood transfusion as well as their sources of contamination is imperative for setting up the preventive measure at blood transfusion centers. Moreover, it is significant to offer action and improve the blood collection practice, education and policy.
In our study, the overall prevalence of bacterial contamination among blood products was 4.5% (17/376). Blood group type O+ 35.3% (6/17) showed the most contaminated. The result was consistent from the study done in Debre Markos, Northwest Ethiopia.12
The proportion of bacterial contamination among those blood products which were collected with non-diverging donor blood collection method was 7.4% (14/188) and almost close to previous studies reported from Ghana stated as 9% (28/303)8 and that of Nigeria 8.8%, (14/162).16 The bacterial contamination of blood products collected with diverging method also was more or less similar to other finding like in Malaysia’s study, 1.7% (12 /702).17
Among the blood products, the highest bacterial contamination was observed in whole blood and PRBC. The study done in Ghana also showed that whole blood was the first blood component to be contaminated.8
The isolated bacteria in this study were both Gram-positive bacteria (S. aureus, S. epidermidis, L. monocytogenes, and Listeria spps) and Gram-negative bacteria (Klebsiellae spps, Proteus line_240 mirabilis and Pseudomonas aeruginosa). Our finding was concordant with different studies like in Nigeria16 and India.18
However, the current finding lower than studies conducted in Debre Markos, Northwest Ethiopia, 12.5% (15/120)2 and Gondar, 15.3% (21/137)11 and the study conducted in Ghana, 16.5% (16/97).13,19 This difference might be due to sample size. Our result showed high bacterial contamination than the study done in Zimbabwe, 3.1% (6/196),20 and Uganda. 3.5% (18/510).5 The reason for this discrepancy might be using only 70% alcohol disinfecting method in our situation. The proportion of bacterial contamination in the diverging method of the current study is higher than different countries; such as New Zealand which was 0.04% (2378/59,461).21 The difference may be lack of implementation of a compressive activity like proper donor screening, double disinfection, and closed processing system in our country.
The non-diverging collection method bacterial contamination was higher than diverging method one, additionally, 7.8 more likely higher to be contaminated than diverging method. Those blood products which were collected in both method share same conditions like application of single disinfection method, the absence of bacterial contamination screening and active national haemovigilance programme except changing the direction of the first 30–40 mL of blood into the diverging pouch. So, switching the first flow of blood reduced the contamination rate by 5.8%. This concept is also supported by the reviewed study done in Italy by Liumbruno et al. The purpose of diverting the first 40–50 mL of donated blood to reduce the microbes or skin fragments especially comes from donor skin entering into the collection bag.22 In addition, other study in Japan by Satake et al also maintained that the positivity rate of bacterial contamination were 36/21,786 (0.17%) and 11/21,783 (0.05%) without and with diversion method in that order.23
As opposed to the current study, a study done in Zimbabwe the finding showed the highest contaminated among blood products was platelet 10.3% (4/36) followed by PRBC 1.3% (2/149). There was no unit of whole blood was contaminated by bacteria. The difference may be they took unequal amount of from each blood products.20
Considering the drug resistance pattern, the findings of this study was concordant with a study from Nigeria and they also reported that gram-positive bacteria were sensitive for gentamicin and ceftriaxone but the majority of the antibiotics were resistant.16 The only antibiotic that showed resistant to the Pseudomonas aeruginosa was gentamicin. Majority of the antibiotics were sensitive for Klebsiella spp and Proteus mirabilis. But a study from Debremarkos indicated that all the Gram-negative organisms isolated were resistant to cotrimoxazole and susceptible to ciprofloxacin and cefoxitin.12 The level of MDR were 5 (29.4%), which was lower than study done here in Gondar, Ethiopia (66.7%).11
Conclusion
This study showed bacterial contamination in the blood and blood components was higher with non-diverging collection method. The most commonly isolated bacteria were Staphylococcus epidermidis. A considerable level of resistant bacteria and MDR organisms were observed. Therefore, blood bank should switch blood donor collection method from non-diverging to diverging method.
Abbreviations
AFCSH, Armed Forces Comprehensive Specialized Hospital; AST, Antimicrobial Susceptibility Test; BAP, Blood Agar Plate; BHI, Brain-Heart Infusion; CAP, Chocolate Agar Plate; CLSI, Clinical and Laboratory Standards Institute; CNS, Coagulase negative Staphylococci; ENDFBBS, Ethiopia National Defense forces Blood bank service; FFP, Fresh Frozen Plasma; MAP, MacConkey Agar Plate; PC, Platelet Concentrates; PRBC, Packed Red Blood Cell; TSI, Triple sugar Iron test; TTBI, Transfusion transmitted bacterial infection; TTI, Transfusion Transmitted Infection.
Data Sharing Statement
All necessary data are included here.
Ethics Approval
The study was approved and given ethical clearance number of SR/LS/019/18 by ethics and research committee of the Department of medical laboratory sciences, School of Allied Health, Sciences and College of Health Sciences of Addis Ababa University. Permission was obtained from the AFCSH administrator. Samples were coded and the confidentiality of donors’ blood was maintained throughout the study. The permission is also involved to disseminate the findings of the study through a scientific workshop and publish in reputable journals.
Acknowledgments
The authors would like to thank Armed forces Compressive Specialized Hospital Microbiology unit for providing laboratory space and facilities to conduct the experiments and its staff who had been cooperative and supportive during specimen collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that was in the conception, study design, execution, acquisition of data, analysis and interpretation or in all of these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article was submitted; and agree to be accountable for all aspects of the work.
Funding
There was no funding to conduct this study.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. American Association of Blood Banks. Transfusion medicine: highlights of transfusion medicine history; 2018. Available from: http://www.aabb.org/tm/Pages/highlights.aspx.
2. Learoyd P. The history of blood transfusion prior to the 20th century–part 2. Transfusion Med. 2012;22(6):372–376. doi:10.1111/j.1365-3148.2012.01189.x
3. Sie JN, Achila Okoth O, Issac J, et al. Seroprevalence of transfusion-transmissible infections among blood donors at National Blood Transfusion Service, Eritrea: a seven-year retrospective study. BMC Infect Dis. 2018;18:1–9.
4. Jain R, Jain P, Mahadik V, Choudhury N. Prevalence and incidence of transfusion transmitted infections among VNRBDs in Central India. Natl J Integr Res Med. 2015;6(4):82–85.
5. Aloysius GBM, Joel B, Apecu R, Yap B, Byarugaba F. Bacterial contamination of blood and blood products at Mbarara Regional Blood Bank in Rural South Western Uganda. Sci Res J. 2013;3:205–209. doi:10.4236/aid.2013.33030
6. Mcdonald CP. Interventions implemented to reduce the risk of transmission of bacteria by transfusion in the English national blood service. Transfus Med Hemother. 2011;38:255–258. doi:10.1159/000330474
7. Bihl F, Castelli D, Marincola F, Dodd Roger Y, Brander C. Transfusion transmitted infections. J Transl Med. 2007;5(25):1–44. doi:10.1186/1479-5876-5-25
8. Adjei AA, Kuma GK, Tettey Y, et al. Bacterial contamination of blood and blood components in three major blood transfusion centers, Accra, Ghana. Jpn J Infect Dis. 2009;62:265–269.
9. Norfolk D. Handbook of Transfusion Medicine.
10. Lee CC. Bacterial contamination of blood products. Hong Kong Red Cross Blood Transfusion Service, Hong Kong SAR, China. ISBT Sci Series. 2011;6:427–431. doi:10.1111/j.1751-2824.2011.01527.x
11. Wondimu H, Addis Z, Moges F, Shiferaw Y. Bacteriological safety of blood collected for transfusion at University of Gondar Hospital Blood Bank, Northwest Ethiopia. Int Scholar Res Notices. 2013;2013:7. doi:10.1155/2013/308204
12. Esmael A, Dagnew Z, Degu G. Bacterial contamination of stored blood ready for transfusion at a Referral Hospital in Ethiopia. J Clin Res Bioeth. 2014;5(2):2–5. doi:10.4172/2155-9627.1000176
13. Opoku-Okrah C, Feglo P, Amidu N, Dakorah MP. Bacterial contamination of donor blood at the Tamale Teaching Hospital, Ghana. Afr Health Sci. 2009;9(1):13–18.
14. Tadesse A, Alem M. Medical Bacteriology. The Carter Center, USA: Gondar University; 2006.
15. Clinical and Laboratory Standards Institute. Clinical and Laboratory Standards Institute Guideline. Performance Standard for Antimicrobial Susceptibility Test.
16. Bolarinwa Rahman A, Aboderin Oladipo A, Odetoyin Babatunde W, Adegunloye Aramide B. Bacterial contamination of blood and blood components in a tertiary hospital setting in Nigeria. Int J Infect Control. 2011;7:1–6. doi:10.3396/ijic.V7i1.001.11
17. Jumaah N, Joshi SR, Sandai D. Prevalence of bacterial contamination when using a diversion pouch during blood collection: a single center study in Malaysia. Malay J Med Sci. 2014;21(3):47–53.
18. Barot T, Kothari F, Dighe M, Patel S. Prevalence of bacterial contamination of stored blood at Blood Bank S.S.G. Hospital, Vadodara. Int J Res Med. 2017;5(4):
19. Boye A, Daniel D, Samuel A, James A, Mate-Siakwa P. Bacterial contamination of at-point-of transfusion blood in a Tertiary Hospital in Ghana. EC Bacteriol Virol. 2016;4:121–128.
20. Makuni N, Simango C, Mavenyengwa Rooyen T. Brief original article prevalence of bacterial contamination in blood and blood products at the National Blood Service Zimbabwe. J Infect Dev Countr. 2015;9:421–424. doi:10.3855/jidc.5428
21. Dickson M, Dinesh D. Bacterial contamination of platelet concentrate produced in New Zealand. NZ Med J. 2013;126(1374):12–21.
22. Liumbruno GM, Catalano L, Piccinini V, Pupella S, Grazzini G. Reduction of the risk of bacterial contamination of blood components through diversion of the first part of the donation of blood and blood components. Blood Transfusion = Trasfusione Del Sangue. 2009;7:86–93. doi:10.2450/2008.0026-08
23. Satake M, Mitani T, Oikawa S, et al. Frequency of bacterial contamination of platelet concentrates before and after the introduction of diversion method in Japan. Transfusion. 2009;49:2152–2157. doi:10.1111/j.1537-2995.2009.02243.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.