Back to Journals » Clinical Ophthalmology » Volume 20
Axial Length Control Using Repeated Low-Level Red Light Combined with Orthokeratology Compared with Orthokeratology Alone in Rapidly Progressing Myopic Children
Received 2 October 2025
Accepted for publication 28 December 2025
Published 13 January 2026 Volume 2026:20 571867
DOI https://doi.org/10.2147/OPTH.S571867
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Alkut Elham,1,2 Xiangjun Meng1
1Department of Ophthalmology, Affiliated Zhongshan Hospital of Dalian University, Dalian, Liaoning, People’s Republic of China; 2Dalian Medical University, Dalian, Liaoning, People’s Republic of China
Correspondence: Xiangjun Meng, Department of Ophthalmology, Affiliated Zhongshan Hospital of Dalian University, Dalian, Liaoning, People’s Republic of China, Email [email protected]
Purpose: To evaluate the efficacy and safety of combining repeated low-level red light (RLRL) therapy with orthokeratology (OK) in slowing axial elongation in children with rapid myopia progression.
Patients and Methods: This retrospective cohort included 72 children aged 8– 14 years (RLRL+OK, n=36; OK-only, n=36) meeting the rapid-progressor definition (> 0.40 mm/year axial elongation. One eye per child was randomly selected. Axial length (AL) was measured at baseline and at 3, 6, and 12 months. Inverse probability of treatment weighting (IPTW) based on age, sex, and baseline AL achieved good balance between groups. The primary outcome was the 12-month AL change, assessed using IPTW-weighted linear mixed-effects models adjusted for covariates. Prespecified subgroup analyses were stratified by age (< 10 vs ≥ 10 years). Sensitivity analyses included propensity score matching (PSM), per-protocol analysis (PP; adherence ≥ 80%), and dose–response evaluation. Safety was assessed using slit-lamp biomicroscopy and macular OCT imaging.
Results: At 12 months, the RLRL+OK group had significantly less elongation than OK-only (mean difference − 0.298 mm; 95% CI − 0.388 to − 0.209; p< 0.001), with significant group×time interactions from 3 months. Benefits were consistent across age subgroups without effect modification. Sensitivity analyses confirmed robustness: PSM (− 0.255 mm; p< 0.001) and PP (− 0.298 mm; p< 0.001). Dose–response showed each 10% higher adherence reduced elongation by − 0.148 mm (p< 0.001). No clinically significant adverse events were detected.
Conclusion: RLRL combined with OK significantly reduced axial elongation in rapid-progressing children compared with OK alone, with a clear adherence-dependent effect and reassuring short-term safety profile.
Keywords: Myopia control, Orthokeratology, Repeated low-level red light, Children and adolescents
Corrigendum for this paper has been published.
Introduction
Myopia, the most prevalent refractive error worldwide, primarily results from excessive axial elongation relative to the optical power of the cornea and lens, causing image formation anterior to the retina and blurred distance vision.1,2 However, myopia is not merely a simple optical condition; it is also associated with progressive axial elongation, scleral thinning, and an elevated risk of vision-threatening pathologies such as cataract, glaucoma, and myopic maculopathy.3,4 The condition imposes an increasing global burden, with projections suggesting that by 2050, nearly 50% of the world’s population—approximately 4.76 billion people—will be affected.5 Accordingly, effective strategies for preventing the onset and slowing the progression of myopia, particularly in children and adolescents, have become a major public health priority.
Orthokeratology (OK) lenses, introduced in the 1960s, are rigid gas-permeable contact lenses with a reverse-geometry design, intended to temporarily reshape the cornea through overnight wear. OK has become a widely accepted first-line intervention for pediatric myopia control. Meta-analyses and systematic reviews have shown that OK reduces axial elongation by approximately 40% to 45% compared with single-vision spectacle wear.6,7 In China, OK lenses were formally endorsed in the 2018 national guidelines for myopia prevention and control issued by the National Health Commission.8 However, despite their proven efficacy, a proportion of children—particularly those with rapidly progressing myopia—continue to experience axial elongation exceeding 0.3 to 0.4 mm per year.9 This variability in treatment response highlights the need for adjunctive therapies or combination strategies to optimize outcomes in high-risk individuals. In addition to monotherapy, combination approaches such as orthokeratology with low-dose (0.01%) atropine have demonstrated enhanced efficacy in slowing axial elongation compared with orthokeratology alone.10,11
Repeated low-level red light (RLRL) has recently emerged as a novel non-pharmacologic intervention for myopia control, delivering low-intensity red light (~650 nm) via direct retinal stimulation. Although the underlying mechanisms remain under investigation, RLRL is hypothesized to modulate retinal neurotransmission and enhance choroidal blood flow and thickening, thereby potentially inhibiting axial elongation.12 Clinical studies have shown that RLRL significantly reduces both SE progression and AL growth in school-aged children, with a favorable safety profile and no reported serious adverse events.13 Recent research further suggest potential synergistic effects when RLRL is combined with other interventions such as OK or multifocal defocus lenses, particularly effective in younger children or those with rapid myopia progression, supporting its potential role as an adjunctive therapy for high-risk populations.14,15 Building upon these encouraging findings, and to address the critical need for optimizing myopia control in real-world clinical settings, especially for children with suboptimal responses to monotherapy, we conducted a retrospective cohort study. This study aimed to assess the efficacy and safety of RLRL combined with OK in slowing axial elongation in myopic children compared with OK alone.
Materials and Methods
Study Design and Setting
This was a single-center, retrospective cohort study conducted at the Affiliated Zhongshan Hospital of Dalian University (Dalian, China) between January 2022 and March 2024. All participants underwent OK lens fitting and follow-up as part of routine clinical care. At baseline, all included children were already wearing OK lenses as part of their routine care, ensuring that the study compared the addition of RLRL versus continuation of OK monotherapy. Axial length (AL) and optical coherence tomography (OCT) were measured by trained technicians masked to treatment group allocation, as no external signs distinguished the two groups. Given the non-randomized design, inverse probability of treatment weighting (IPTW) and propensity score matching (PSM) were employed to control for measured confounders.
Eligibility Criteria
Inclusion Criteria
Eligible children met all of the following:
- Age 8–14 years;
- Cycloplegic spherical equivalent (SE) between –0.50 D and –5.00 D;
- Astigmatism ≤1.50 D;
- Interocular SE difference ≤1.50 D;
- Best-corrected visual acuity (BCVA) ≥0.00 logMAR;
- Central corneal thickness (CCT) >450 μm;
- Documented axial elongation >0.40 mm/year in the 12 months before baseline (applied equally to both groups to ensure comparability).
- Participants were required to be established OK lens wearers prior to enrollment.
Exclusion Criteria
Children were excluded if they had:
- Previous or concurrent myopia-control interventions other than OK (eg, atropine, defocus-incorporated or multifocal spectacles);
- Ocular or systemic disease, or prior ocular surgery, that could affect refraction or AL;
- Missing baseline data or ≥2 missed follow-up visits within the predefined ±21-day window.
To avoid inter-eye correlation, only one eye per participant was analyzed. If both eyes met all criteria, one was randomly selected using a computer-generated random number (1 = right eye, 0 = left eye). If only one eye was eligible, that eye was included. In total, 72 participants (36 per group) were included, comprising 39 right eyes and 33 left eyes.
Grouping and Interventions
At the index date (the first visit confirming rapid progression, defined as prior-year AL elongation >0.40 mm/year), adjunctive RLRL was systematically offered according to a uniform clinical pathway; treatment assignment followed an as-initiated strategy fixed at the index date (RLRL started within ≤14 days vs OK monotherapy). No participant switched treatments thereafter. Children who initiated RLRL within ≤14 days were assigned to the RLRL+OK group; those who continued monotherapy were assigned to the OK-only group. Orthokeratology lenses were fitted by certified staff in accordance with national guidelines. Most children (n=68) were fitted with DreamVision lenses (Oupu Vision, China), while a minority (n=4) used Alpha lenses (Alpha Corp., Japan). Both lens types are manufactured from high–oxygen-permeable fluorosilicone acrylate (Dk ≈160) and employ a four-zone reverse-geometry design. Average overnight wear duration was approximately 8 hours. RLRL was delivered using a tabletop device (Eyerising, Jiangsu, China; 650±10 nm; 160±20 μW). Each session lasted 3 minutes, twice daily at ≥4-hour intervals, with eyes open and fixating on the light source. The device is certified as Class 1 under IEC 60825–1:2014, conforms to ISO 13485:2016, CE-marked (Class IIa), and registered with the National Medical Products Administration (China), the Medicines and Healthcare products Regulatory Agency (UK), the Therapeutic Goods Administration (Australia), and Medsafe (New Zealand). Adherence was monitored using cloud-based logs, parental diaries, and clinic checks, and was defined as completing ≥80% of prescribed sessions.
Assessments and Outcomes
Follow-up visits were scheduled at baseline, 3, 6, and 12 months (each within a ±21-day window). At each visit, slit-lamp examination, AL measurement, OCT scan, and OK lens fit evaluation were performed. AL was measured with an optical biometer (IOLMaster 500, Carl Zeiss Meditec, Germany). Three consecutive readings were averaged at each visit. Measurements were conducted between 13:00 and 16:00 to minimize diurnal variation. The primary outcome was 12-month axial elongation of the study eye, measured from the index date. The secondary outcomes were longitudinal AL trajectories at 0, 3, 6, and 12 months, and the incidence of adverse events (AEs). Predefined AEs included conjunctival hyperemia lasting >24 hours, afterimages persisting >10 minutes on ≥2 occasions, photophobia interfering with daily activities, corneal staining, or any new scotoma/visual field abnormality. RLRL was discontinued if OCT or fundus examination revealed persistent subclinical abnormalities (eg, subtle retinal or choroidal structural changes). At each visit, macular OCT (6×6 mm cube; Dream OCT, Intalight, Shanghai, China) was performed to monitor foveal and inner retinal integrity.
Data Handling
Clinical data were extracted independently by three trained managers from electronic medical records, paper charts, and case files, and were cross-verified for completeness. To avoid inter-eye correlation, only one eye per child was included, as described above. Follow-up was nearly complete, one visit was missed at 3 months, two at 6 months, and two at 12 months (<10%). Missing visits were mostly due to scheduling conflicts or temporary withdrawal and were unrelated to treatment group. A complete-case approach was used. Linear mixed-effects (LME) models accommodated unbalanced repeated measures.
Statistical Analysis
Analyses were performed using Stata version 18.0 (StataCorp, College Station, TX, USA). A two-sided significance level of α=0.05 was applied. Propensity scores (PS) were estimated from baseline age, sex, and AL. IPTW were derived and trimmed at the 1st–99th percentiles. Balance was evaluated using standardized mean differences (adequate if |SMD|<0.25) and variance ratios, and the effective sample size (ESS) was reported. IPTW-weighted linear mixed-effects models with a subject-level random intercept were fitted, specifying time as a categorical factor (0, 3, 6, and 12 months) and fixed effects for group, time, group×time, age, sex, and baseline AL; cluster-robust standard errors were calculated with clustering by ID. Estimated marginal means (EMMs) and group differences with 95% confidence intervals (CIs) were reported. The 12-month between-group difference in axial elongation was prespecified as the primary outcome; CI half-widths were presented as a precision measure.
Sensitivity and Exploratory Analyses
Several prespecified analyses were undertaken to examine robustness. A per-protocol (PP) analysis restricted to RLRL+OK participants with adherence ≥80% was conducted, with IPTW re-estimated and the LME model repeated. Within the RLRL+OK group, dose–response analyses modeled adherence (percentage of prescribed sessions completed) as a continuous exposure; effects on 12-month axial elongation were estimated per 10% increase in adherence, adjusting for baseline covariates. Linear trend tests were prespecified, and restricted cubic splines (3 knots) were explored to assess potential non-linearity. Additionally, 1:1 nearest-neighbor PSM without replacement (caliper 0.20 SD of logit[PS]) was performed using age, sex, and baseline AL. Balance after matching was assessed by standardized mean differences (SMD <0.25 considered acceptable). In the matched cohort, 12-month axial elongation was compared between groups using linear regression with baseline covariates, applying pair-clustered robust standard errors to account for matched pairs. All results were reported as regression coefficients with 95% CIs.
Ethics
The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Zhongshan Hospital Affiliated to Dalian University (Approval No. 2021 Ethics Review Document No. 078). The study protocol was reviewed by the Institutional Review Board, which granted an exemption from additional approval due to the retrospective design and use of de-identified data. Guardians had provided written informed consent at the time of routine care, explicitly permitting the anonymized use of clinical data for research and publication. The RLRL device had prior approval for clinical use from the hospital’s Medical Device Management Committee and is registered with the National Medical Products Administration (China), the Medicines and Healthcare products Regulatory Agency (UK), the Therapeutic Goods Administration (Australia), and Medsafe (New Zealand).
Results
Participants and Baseline
Seventy-two children met the eligibility criteria and were included in the analysis (RLRL+OK, n=36; OK-only, n=36; Figure 1). The median age was 9.0 years in the RLRL+OK group and 11.0 years in the OK-only group. Baseline axial length was similar between groups (24.41 mm vs 24.23 mm). The sex distribution was balanced, with 18 boys (50.0%) in each group. In the RLRL+OK group, mean adherence to therapy was 82.7 ± 8.6% (Table 1). Follow-up completeness was high, with only 1, 2, and 2 visits missed at 3, 6, and 12 months, respectively (<10%). After IPTW, baseline covariates achieved good balance, with absolute SMDs ranging from 0.05 to 0.21 (Supplementary Table A1 and Figure A1). The participant-level ESS after weighting were 24.96 in the OK-only group and 22.91 in the RLRL+OK group (Supplementary Table A2).
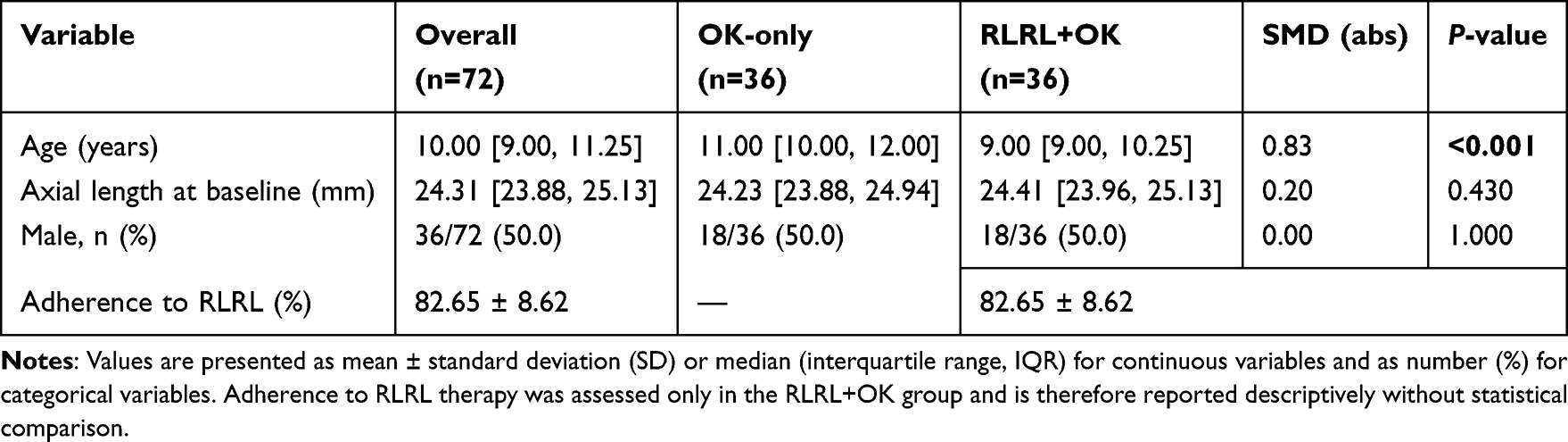 |
Table 1 Participant Demographics, Ocular Characteristics, and Treatment Adherence |
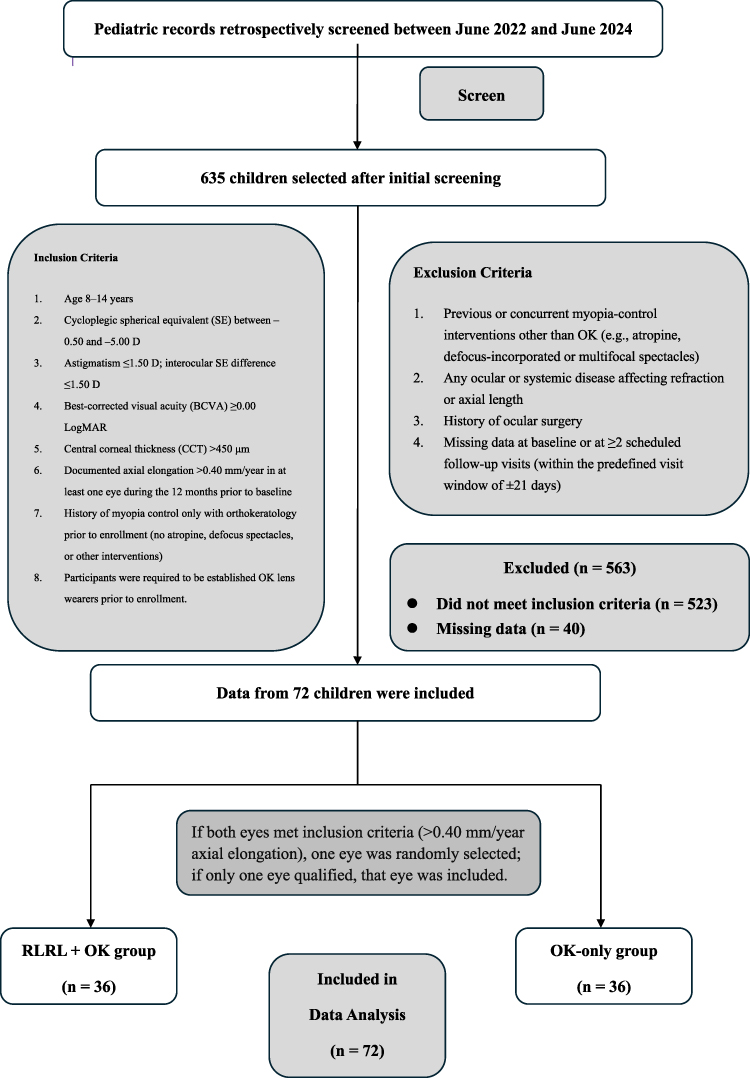 |
Figure 1 Study flow and eligibility. |
Primary Outcomes and Longitudinal Trajectories
At 12 months, the model-estimated EMMs for AL were 24.642 mm (95% CI, 24.589–24.694) in the OK-only group and 24.343 mm (95% CI, 24.274–24.412) in the RLRL+OK group, corresponding to a between-group difference in 12-month axial elongation of −0.298 mm (95% CI, −0.388 to −0.209; p<0.001), favoring RLRL+OK (Supplementary Table A3 and Table 2 and Figure 2). Model diagnostics indicated adequate fit and normally distributed residuals without influential outliers (Supplementary Figure A2).
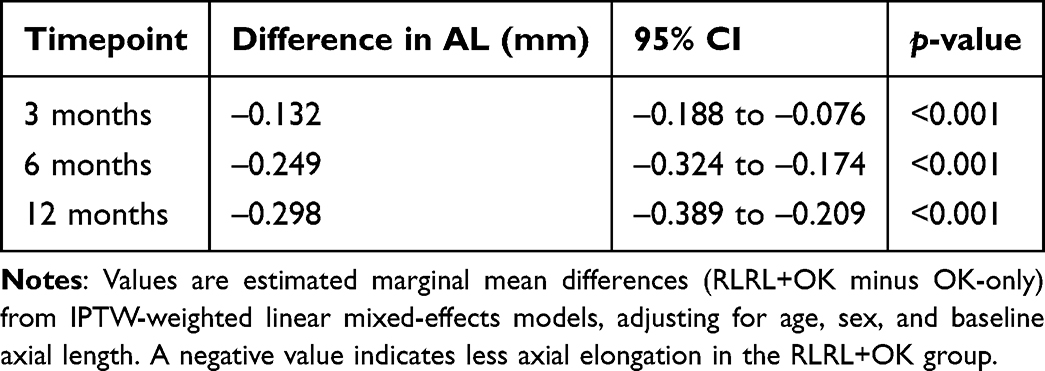 |
Table 2 IPTW-Weighted Linear Mixed-Effects Model for Axial Length Change (RLRL+OK Vs OK-Only) |
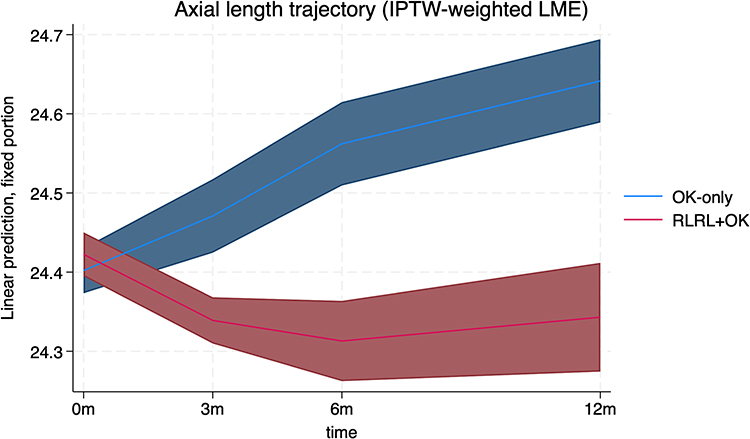 |
Figure 2 Axial length changes over 12 months. Notes: Axial length trajectory over 12 months in the IPTW-weighted LME model. Predicted means and 95% confidence intervals of axial length are shown for the RLRL+OK group (dashed line with squares) and the OK-only group (solid line with circles) at baseline, 3, 6, and 12 months. Axial elongation remained essentially stable in the RLRL+OK group, whereas the OK-only group showed progressive axial growth. |
Prespecified Age Subgroup
In the <10-year subgroup, the 12-month difference was −0.273 mm (95% CI −0.419 to −0.126); in the ≥10-year subgroup, −0.301 mm (95% CI −0.409 to −0.193). The triple interaction (group×time×age) at 12 months was not significant (p=0.81), indicating no evidence of effect modification by age (Table 3 and Figure 3).
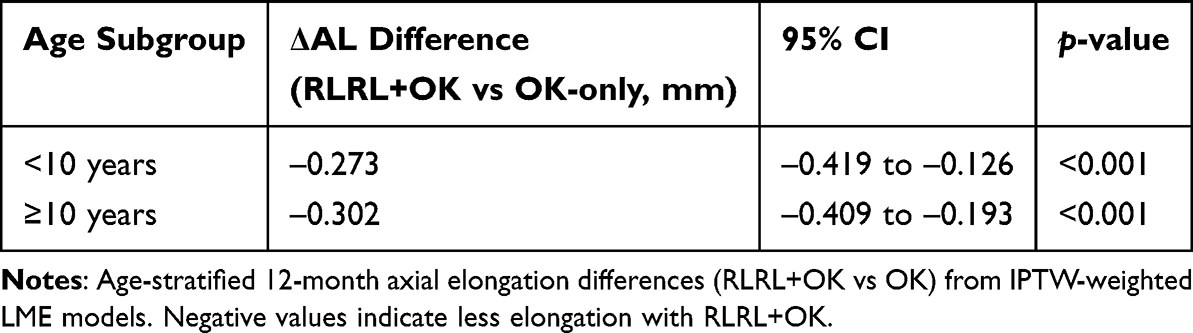 |
Table 3 Age Subgroup Analysis of Axial Elongation at 12 months |
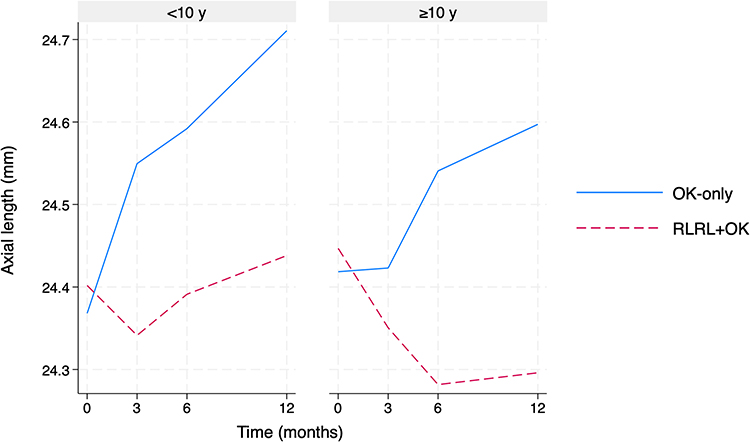 |
Figure 3 Axial length trajectories by age subgroup. Notes: Axial length trajectories by age subgroup (IPTW-weighted LME). Predicted axial length values at baseline, 3, 6, and 12 months are shown for the OK-only group (solid line, circles) and the RLRL+OK group (dashed line, squares), stratified by baseline age (<10 years vs ≥10 years). |
Sensitivity and Exploratory Analyses
In propensity score–matched analysis (1:1 nearest neighbor, no replacement; caliper 0.20 SD of logit[PS]), the 12-month axial elongation difference remained significant (−0.255 mm; 95% CI −0.344 to −0.165; p<0.001; Supplementary Table A4). In the PP analysis restricted to RLRL+OK participants with adherence ≥80%, between-group differences were −0.132 mm at 3 months, −0.249 mm at 6 months, and −0.298 mm at 12 months (all p<0.001; Supplementary Table A5). In dose–response analysis within the RLRL+OK group, higher adherence was associated with less axial elongation: each 10% increase in adherence corresponded to an additional −0.148 mm reduction at 12 months (95% CI −0.195 to −0.102; p<0.001), with consistent effects at 3 and 6 months (Supplementary Table A6).
Safety
No clinically significant adverse events occurred in the RLRL+OK group, and no participant discontinued therapy for safety reasons. In the OK-only group, four cases of mild corneal staining were detected during routine visits; all were transient and resolved with conservative management. Importantly, no RLRL-related retinal or OCT abnormalities were identified.
Discussion
This study examined whether adding RLRL to OK confers incremental control of axial elongation in children who already meet a rapid-progressor definition. In an inverse-probability–weighted longitudinal analysis, the RLRL+OK strategy was associated with ~0.30 mm less 12-month axial elongation than OK alone, with differences evident from 3 months; results were robust in prespecified propensity-score–matched and per-protocol analyses, and a clear adherence–response was observed, while OCT surveillance detected no treatment-related abnormalities. These findings align with randomized trials showing that 650-nm red light slows myopia progression and axial growth relative to conventional care, and they are concordant with emerging multicenter evidence testing the combination of RLRL and OK in clinical settings.14,16–20 In addition, a head-to-head comparison of RLRL versus OK suggests superior axial control with RLRL monotherapy in appropriately selected children, reinforcing the plausibility of added benefit when RLRL is layered onto OK.21 Differences in effect magnitude across reports likely reflect design (pragmatic cohort vs RCT), baseline risk enrichment (rapid progressors vs broader pediatric samples), and adherence intensity; the consistent direction of effect across methods strengthens confidence in the incremental value of adding RLRL to established optical strategies.14,16
Our 12-month effect (~0.29–0.30 mm) is closely aligned with a multicenter RCT among “poor responders to OK,” which reported an adjusted difference of −0.29 mm for RLRL+OK versus OK, supporting generalizability to high-risk clinic populations.14 The direction and magnitude also concord with RLRL monotherapy RCTs against single-vision spectacles and high-myopia cohorts, which consistently demonstrate clinically meaningful AL suppression and reassuring structural safety on OCT.19,20,22,23 Beyond optical comparators, network and pairwise syntheses have suggested that RLRL can perform at least comparably to low-dose atropine on axial control over 6–12 months, providing biological plausibility for the additive benefit we observed when RLRL was combined with OK.19,22 Importantly, by using OK as an active comparator and by focusing on rapid progressors while applying modern weighting/matching approaches and adherence–effect modeling, this study extends prior work that often evaluated RLRL or OK in isolation. We also note mechanistic complementarity: OK induces peripheral myopic defocus to modulate retinal signaling, whereas RLRL is hypothesized to act via photobiomodulation pathways (eg, choroidal perfusion, mitochondrial activity, scleral hypoxia), a dual-pathway rationale that may underlie the enhanced AL control seen with the combination.17,18,24,25 Consistent with the broader literature on combined strategies in pediatric myopia, evidence of synergy in other dual-modality regimens (eg, defocus-incorporated multiple segments with atropine) provides an external precedent for additivity when mechanisms are complementary.15 Although myopia control has been extensively studied, our study adds real-world evidence specifically addressing children with rapid myopia progression who were already undergoing orthokeratology treatment, a population that has been underrepresented in prior studies.
Several limitations warrant cautious interpretation. First, the single-center, retrospective, nonrandomized design limits external generalizability and leaves room for residual confounding despite balance on measured covariates with IPTW/PSM; unmeasured factors (eg, socioeconomic context, parental myopia, outdoor/near-work exposures, OK fit parameters and adherence) might have influenced treatment selection or outcomes. Second, the modest sample size (n = 72) constrains precision for subgroups and limits detection of uncommon adverse events. Nevertheless, the observed between-group difference exceeded 0.25 mm, a magnitude generally considered clinically meaningful in pediatric myopia control studies, and was detected with high statistical significance (p < 0.001), suggesting a large effect size relative to variability. Third, follow-up was 12 months in a cohort enriched for rapid progressors and predominantly using specific OK lenses, precluding assessment of long-term durability or rebound after discontinuation. We mitigated these risks by prespecifying an index date to fix exposure (limiting immortal-time bias), masking technicians for AL/OCT measurements, random selection of a single study eye to avoid inter-eye correlation, and triangulating estimates across IPTW, PSM, per-protocol, and dose–response analyses. Future multicenter RCTs—or prospectively registered target-trial emulations—with broader baseline covariate capture, larger samples powered for safety/subgroups, and extended follow-up are needed to assess durability, rebound, and long-term safety.20,22–27
To strengthen future evidence, trials should randomize at the index visit (when rapid progression is confirmed) or, where randomization is infeasible, adopt prospectively specified target-trial emulation with standardized eligibility and a predefined causal analysis plan. Baseline variables should expand beyond age/sex/AL to include cycloplegic refraction, parental myopia, socioeconomic indicators, outdoor and near-work metrics (ideally from wearables/validated logs), and OK fitting parameters; analytic robustness can be enhanced with negative-control analyses and quantitative bias assessment. Follow-up beyond 12 months with protocolized adherence capture (device logs as primary source) will enable hierarchical longitudinal modeling of treatment heterogeneity and continuous dose–response. Safety surveillance should incorporate centralized OCT/OCTA reading and standardized corneal and patient-reported outcomes; selective mechanistic substudies (eg, choroidal thickness, perfusion) may refine biological understanding. Transparent practices—public registration, prespecified SAPs, and sharing of de-identified code/tables—will facilitate reproducibility and translation,16–28 and comparative-effectiveness designs that benchmark against other combination regimens (eg, optical plus pharmacologic) may further clarify when and for whom dual-modality strategies are most effective.15,21 This work was previously posted as a preprint on Research Square (https://www.researchsquare.com/article/rs-6995321/v1).
Conclusion
In this single-center, propensity score–adjusted cohort of children with rapid myopia progression, adding RLRL to OK was associated with materially less axial elongation over 12 months than OK alone. The effect was evident from the first follow-up, persisted through 12 months, and was corroborated by prespecified sensitivity analyses (propensity score matching and per-protocol) as well as an adherence–response pattern, suggesting that treatment intensity meaningfully influences outcomes. Safety findings were reassuring in the short term: routine slit-lamp examinations and macular OCT surveillance detected no RLRL-related structural abnormalities, and only mild corneal staining events were observed, all in the OK-only group. While the retrospective, single-center, nonrandomized design and modest sample size limit causal inference and generalizability, the use of an active comparator (OK), technician masking, one-eye random selection, and modern confounding control strengthen internal validity. Clinically, these data support consideration of RLRL as an adjunct to OK for rapidly progressing children, coupled with structured adherence monitoring and continued ocular safety surveillance. Priority areas for future work include multicenter randomized or prospectively emulated target-trial designs, longer follow-up to evaluate durability and potential rebound, richer baseline covariate capture to reduce residual confounding, and implementation and economic evaluations to inform real-world adoption.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Baird PN, Saw SM, Lanca C, et al. Myopia. Nat Rev Dis Primers. 2020;6(1):99. doi:10.1038/s41572-020-00231-4
2. Morgan IG, Ohno-Matsui K, Saw SMM. Myopia. Lancet. 2012;379(9827):1739–10. doi:10.1016/S0140-6736(12)60272-4
3. Liu G, Rong H, Liu Y, et al. Effectiveness of repeated low-level red light in myopia prevention and myopia control. Br J Ophthalmol. 2024;108(9):1299–1305. doi:10.1136/bjo-2023-324260
4. Fricke TR, Holden BA, Wilson DA, et al. Global cost of correcting vision impairment from uncorrected refractive error. Bull World Health Organ. 2012;90(10):728–738. doi:10.2471/BLT.12.104034
5. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–1042. doi:10.1016/j.ophtha.2016.01.006
6. Tang K, Si J, Wang X, Lu X, Bi H. Orthokeratology for slowing myopia progression in children: a systematic review and meta-analysis of randomized controlled trials. Eye Contact Lens. 2023;49(9):404–410. doi:10.1097/ICL.0000000000001006
7. Si J-K, Tang K, Bi H-S, Guo -D-D, Guo J-G, Wang X-R. Orthokeratology for myopia control: a meta-analysis. Optom Vis Sci. 2015;92(3):252–257. doi:10.1097/OPX.0000000000000505
8. Ministry of Education of China. Notice on prevention and control of myopia in children and adolescents; 2018. Available from: http://www.moe.gov.cn/srcsite/A17/moe_943/s3285/201808/t20180830_346672.html.
9. Cho P, Cheung SW. Retardation of myopia in Orthokeratology (ROMIO) study: a 2-year randomized clinical trial. Invest Ophthalmol Vis Sci. 2012;53(11):7077–7085. doi:10.1167/iovs.12-10565
10. Tan Q, Ng AL, Choy BN, Cheng GP, Woo VC, Cho P. One-year results of 0.01% atropine with orthokeratology (AOK) study: a randomised clinical trial. Ophthalmic Physiol Opt. 2020;40(5):557–566. doi:10.1111/opo.12722
11. Wang Z, Wang P, Jiang B, Meng Y, Qie S, Yan Z. The efficacy and safety of 0.01% atropine alone or combined with orthokeratology for children with myopia: a meta-analysis. PLoS One. 2023;18(7):e0282286. doi:10.1371/journal.pone.0282286
12. Xiong R, Zhu Z, Jiang Y, et al. Longitudinal changes and predictive value of choroidal thickness for myopia control after repeated low-level red-light therapy. Ophthalmology. 2023;130(3):286–296. doi:10.1016/j.ophtha.2022.10.002
13. Zhu Q, Cao X, Zhang Y, et al. Repeated low-level red-light therapy for controlling onset and progression of myopia – a review. Int J Med Sci. 2023;20(10):1363–1376. doi:10.7150/ijms.85746
14. Xiong R, Wang W, Tang X, et al. Myopia control effect of repeated low-level red-light therapy combined with orthokeratology: a multicenter randomized controlled trial. Ophthalmology. 2024;131(11):1304–1313. doi:10.1016/j.ophtha.2024.05.015
15. Huang Z, Chen XF, He T, Tang Y, Du CX. Synergistic effects of defocus-incorporated multiple segments and atropine in slowing the progression of myopia. Sci Rep. 2022;12(1):22311. doi:10.1038/s41598-022-25599-z
16. Logan NS, Bullimore MA. Optical interventions for myopia control. Eye (Lond). 2024;38(3):455–463. doi:10.1038/s41433-023-02723-5
17. Vincent SJ, Cho P, Chan KY, et al. CLEAR – orthokeratology. Cont Lens Anterior Eye. 2021;44(2):240–269. doi:10.1016/j.clae.2021.02.003
18. Erdinest N, London N, Lavy I, et al. Peripheral defocus and myopia management: a mini-review. Korean J Ophthalmol. 2023;37(1):70–81. doi:10.3341/kjo.2022.0125
19. Tsai HR, Wang JH, Huang HK, Chen TL, Chen PW, Chiu CJ. Efficacy of atropine, orthokeratology, and combined atropine with orthokeratology for childhood myopia: a systematic review and network meta-analysis. J Formos Med Assoc. 2022;121(12):2490–2500. doi:10.1016/j.jfma.2022.05.005
20. Jiang Z, Chen S, Wang R, Ma J. Safety of and chorioretinal circulation during repeated low-level red-light therapy for myopic children. Clin Exp Ophthalmol. 2025;53(2):119–132. doi:10.1111/ceo.14462
21. Sun JR, Du ZQ, Wu GY. Efficacy comparison of repeated low-level red-light therapy and orthokeratology lenses for myopia control. Optom Vis Sci. 2024;101(11):660–665. doi:10.1097/OPX.0000000000002197
22. Schmidt DC, Hvid-Hansen A, Jacobsen N, et al. Efficacy of interventions for myopia control in children: a systematic review with network meta-analyses. Acta Ophthalmol. 2025;103:939–965. doi:10.1111/aos.17496
23. Tang J, Liao Y, Yan N, et al. Efficacy of repeated low-level red-light therapy for slowing the progression of childhood myopia: a systematic review and meta-analysis. Am J Ophthalmol. 2023;252:153–163. doi:10.1016/j.ajo.2023.03.036
24. Xiang K, Wang J, Zhu Z, et al. Changes in choroidal thickness in pre-myopic children after repeated low-level red-light therapy and their role in predicting myopia prevention and controlling myopic shift. Asia Pac J Ophthalmol. 2025;14(2):100115. doi:10.1016/j.apjo.2024.100115
25. Liao X, Yu J, Fan Y, et al. Cone density changes after repeated low-level red light treatment in children with myopia. JAMA Ophthalmol. 2025. doi:10.1001/jamaophthalmol.2025.0835
26. Liu G, Liu L, Rong H, et al. Axial shortening effects of repeated low-level red-light therapy in children with high myopia: a multicenter randomized controlled trial. Am J Ophthalmol. 2025;270:203–215. doi:10.1016/j.ajo.2024.10.011
27. Chen Y, Xiong R, Yang S, et al. Safety of repeated low-level red-light therapy for myopia: a systematic review. Asia Pac J Ophthalmol. 2024;13(6):100124. doi:10.1016/j.apjo.2024.100124
28. He X, Wang J, Zhu Z, et al. Effect of repeated low-level red light on myopia prevention among children with premyopia: a randomized clinical trial. JAMA Network Open. 2023;6(4):e239612. doi:10.1001/jamanetworkopen.2023.9612
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Long-Term Efficacy of CRT, Lucid, Euclid, and IBright Orthokeratology Lenses in Controlling Myopia Progression in Children and Adolescents: A 36-Month Retrospective Cohort Study
Xi W, Li H, Qi W, Tan T, Wang L
Clinical Ophthalmology 2025, 19:2423-2430
Published Date: 23 July 2025
The “Three-Tier Regulatory Network” of Orthokeratology in Myopia Control: Evidence Weight of Underlying Mechanisms, Controversies, and New Perspectives for Clinical Translation--A Review
Han L, He S, Dong S, Lu Y, Zhang M
Clinical Ophthalmology 2026, 20:600353
Published Date: 12 June 2026