Back to Journals » International Journal of General Medicine » Volume 19
Awareness and Understanding of Ionizing and Non-Ionizing Radiation Modalities Among Patients in Saudi Arabia
Authors Arif WM ![]()
Received 24 February 2026
Accepted for publication 6 June 2026
Published 24 June 2026 Volume 2026:19 604205
DOI https://doi.org/10.2147/IJGM.S604205
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Kenneth Adler
Wejdan M Arif
Radiological Sciences Department, College of Applied Medical Sciences, King Saud University, Riyadh, 4545, Saudi Arabia
Correspondence: Wejdan M Arif, Email [email protected]
Background: Medical diagnostic procedures involving the radiation use are important component of modern healthcare systems, enabling accurate diagnosis, staging and monitoring of many conditions or diseases. Patients’ understanding of ionizing versus non-ionizing imaging modalities, associated risks, and radiation safety is essential for informed consent and shared decision-making.
Aim: This study aims to assess patients’ awareness, knowledge, perceptions, confidence, and educational needs regarding ionizing and non-ionizing radiation used in medical imaging.
Methods: A cross-sectional questionnaire-based design was adopted in this study. Participants included patients who have undergone various medical imaging procedures, and were aged above 18 years. An online validated 28-item questionnaire was used to collect the data from 1256 adult patients. Descriptive statistics and inferential analyses, including ANOVA and t-tests, were performed with significance set at p < 0.05.
Results: Although 77.6% recognized natural ionizing radiation, 40.8% misclassified MRI as ionizing and 41.3% misclassified CT as non-ionizing. Only 34.1% identified CT as the highest-dose procedure. Mean risk awareness score was 4.13 (SD 0.78) and confidence score was 4.15 (SD 0.79). Older age, higher education, and female gender were significantly associated with greater awareness (F = 9.74, p = 0.001).
Conclusion: Despite high perceived awareness and confidence regarding ionizing radiation, significant misconceptions about imaging modalities and radiation dose still persist among patients in Saudi Arabia. This suggests the need for structured, standardized radiation-risk communication before imaging procedures to improve patient understanding and informed consent.
Keywords: ionizing radiation, medical imaging, patient awareness, radiation risk perception, patient confidence, radiation literacy
Introduction
Medical diagnostic procedures are important component of modern healthcare systems, enabling accurate diagnosis, staging and monitoring of many conditions or diseases. Diagnostic procedures, especially imaging modalities differ in the type and magnitude of radiation involved, which are categorized under ionizing and non-ionizing radiation. Non-ionizing radiation is electromagnetic radiation with insufficient photon energy (<10–33 eV) to remove electrons from atoms, causing molecular excitation rather than ionization. In medical imaging, it includes MRI (magnetic fields) and ultrasound (acoustic waves).1–4 Whereas, ionizing radiation involves removal of electrons by ionizing atoms using high-energy electromagnetic waves or subatomic particles. It is applied in various diagnostic imaging modalities such as X-ray radiography, computed tomography (CT), nuclear medicine, fluoroscopy, mammography, and radiotherapy.1–4 These procedures expose patients to radiation which involves potential stochastic risks, such as DNA damage and increased cancer incidence, with effective doses varying significantly (for example, chest X-ray at ~0.1 mSv versus CT abdomen at 10 mSv, compared to annual background or natural radiation of ~2–3 mSv).5–8 In contrast, non-ionizing radiation lacks sufficient energy for ionization and includes safer modalities like magnetic resonance imaging (MRI) and ultrasound, which rely on magnetic fields and acoustic waves, respectively.9,10
With the rising demands for healthcare, significant increase in the use of medical imaging was observed in the recent years. Radiation used for medical purposes makes up 98% of the dose from all human-made sources and 20% of the total population exposure. As of 2023, 4200 million diagnostic radiology examinations, 40 million nuclear medicine procedures, and 8.5 million radiotherapy treatments were carried out in an year,11 which is increasing at a rapid pace in the past few years. A study which included 2.5 million patients and 4.8 million CT examinations found that patients underwent a median of six CT scans per year.12 Recent studies13–15 have shown that more than 1% of patients have had a total radiation dose of more than 100 mSv over their lifetime because they have had repeated imaging tests. This is a practical threshold where stochastic cancer risks (~0.5% lifetime increase) become epidemiologically meaningful, although ICRP/IAEA recognize no safe threshold and assume proportional risk from any dose via the linear non-threshold (LNT) model.16 As a part of Vision 2030, Saudi Arabia has been rapidly promoting digital transformation of healthcare system, adopting innovative technologies and diagnostic procedures,17 given the rising demand for healthcare needs. There is a need for public to understand which modalities produce ionizing radiation, the relative doses of common imaging procedures, health risks associated with these procedures, and the trade-offs between diagnostic benefit and potential harm for promoting and facilitating informed consent and shared decision-making.18–20 Studies21–24 have found that patients often misunderstood modality specific risks, for instance, wrongly perceiving certain modalities such as MRI or ultrasound as ionizing radiation related diagnoses, and underestimating CT doses. It was observed that only 50% to 60% of the patients correctly identified ionized procedures, resulting in undue fear or lack of confidence and satisfaction that affects informed consent and ALARA (As Low As Reasonably Achievable) adherence.
Studies have shown that sociodemographic factors like education and age influencing knowledge gaps among the patients.21–24 Patients’ literacy therefore is an important aspect that need to be investigated in this context, along with their perception and needs. International studies25,26 have highlighted enduring misconceptions following educational initiatives, indicating the necessity for targeted interventions. Therefore, this study aims to assess patients’ awareness, knowledge, and perceptions of ionizing and non-ionizing radiation used in medical imaging procedures in Saudi Arabia. Accordingly, the objectives include (1) quantify modality-specific knowledge and misconceptions, (2) examine demographic determinants of awareness and educational need, and (3) identify preferred information sources.
Background
Previous research in this context has shown limited patients’ knowledge and awareness of ionizing and non-ionizing radiation used in medical imaging, with frequent misconceptions regarding modality classification and radiation dose. A recent study21 in Saudi Arabia reported only 29.7% good knowledge among 1024 patients, with 54% misclassifying MRI/ultrasound as ionizing and 62% underestimating CT doses. Another study22 has found that 67.6% patients were not aware of natural sources of ionizing radiation, 41.5% believed that chest X-rays and CT scans deliver equal radiation doses, which is incorrect, 53.1% raised concerns for radiological tests, and 58.3% believed these procedures pose health hazards. Similarly, Bastiani et al25 noted that 43% believed ultrasound ionizing, 51% overestimating mammography; and Alsubaie et al27 identified 58% CT risk misperceptions in emergency patients.
In addition to factual knowledge, perceptions of radiation risks plays an important role in shaping patient attitudes and behavior. Studies25,28 have shown that high levels of concern about radiation exposure exist among the patients, despite limited understanding of dose magnitude or long-term risk. Such high levels of concerns could lead to increased anxiety and reduced acceptance of clinically justified imaging among the patients; whereas low perceived risk could lead to complacency and limited questioning of repeated high-dose examinations.29
Among the various factors, patient confidence is one of the critical factor that has been underexplored in the previous research. Confidence refers not only to patients’ self-perceived understanding of radiation concepts but also to their ability to discuss radiation risks with healthcare providers and to trust clinical recommendations.30 It has been observed that patients often reported low confidence in their radiation knowledge and feel under prepared to engage in risk–benefit discussions, even when they express high trust in clinicians.31–33 Clear clinician communication can strongly influence patient confidence. Studies22,32 have shown that patients preferred to receive radiation-related information directly from physicians or radiologists; however, it has been observed that often the communication is brief with limited explanations, inconsistent, or absent prior to imaging procedures. Poor or inadequate communication results in decreased patient confidence and increases reliance on non-professional information sources, such as the internet or social media, which may contribute to the spread of misinformation.34–36
Demographic predictors are consistent across studies. Higher education levels and older age were linked to better modality knowledge and greater expressed need for information, whereas employment status shows weaker associations. Gender effects remain inconsistent across studies18,21,22,27,37 likely reflecting Saudi-specific factors including gender-segregated healthcare systems, preferences for same-gender clinicians, and women’s relatively lower access to digital health information sources.38 Female patients reflected higher levels of concerns and educational needs, with odds ratios of 2.1 for demanding pre-scan information; whereas male patients reflected higher awareness levels.25,31 Furthermore, low education rural females were identified with large deficits, higher anxiety levels with lower awareness levels,38 reflecting the need for stratified and targeted interventions for improving awareness.
While prior studies have identified knowledge gaps and risk perceptions,21–27 they remain largely descriptive and segregated, focusing primarily on factual recall without integrating health literacy perspectives, risk communication dynamics, or behavioral implications. Critically, there is a lack of research on how high self-perceived confidence coexists with persistent misconceptions—a potentially serious combination where overconfident patients may dismiss educational interventions or fail to engage in meaningful risk-benefit discussions.29–32 International studies25,39,40 from Europe and Australia show similar modality confusion patterns (43% ultrasound misclassification), suggesting these gaps transcend regional contexts and reflect universal challenges in patient radiation literacy. This study addresses this multi-dimensional gap by simultaneously assessing patients’ factual knowledge, perceived confidence, educational needs, and preferred communication channels within Saudi Arabia’s Vision 2030 healthcare transformation context. This integrated approach provides novel insights into how health literacy barriers and communication preferences shape patient behavior, with implications for standardized risk communication protocols applicable beyond the regional setting.
Methods
Study Settings
A cross-sectional questionnaire-based design was adopted in this study to assess patients’ knowledge, perceptions, confidence, and educational needs regarding ionizing and non-ionizing radiation used in medical imaging. The study was conducted at eight different hospitals in Saudi Arabia. Participants were recruited during outpatient appointments at eight hospitals in Saudi Arabia. After the study purpose was explained by research staff, eligible patients were provided with a QR code displayed on tablets or posters at the clinic, enabling immediate smartphone-based survey completion at their convenience within two weeks. This convenience sampling approach ensured high response rates while minimizing disruption to clinical workflows.
Participants and Sampling
The study population included adults aged 18 years and above residing in Saudi Arabia. A convenience sampling approach was adopted to recruit participants, considering demographic parameters including age, gender, and type of medical imaging received. The patients had undergone various medical imaging procedures, including CT, ultrasound, and MRI among the male and female participants, and mammography among the female participants. The minimum sample size, calculated using Cochran’s formula with a 95% confidence level and a 5% margin of error, is 385 participants. At the end of six weeks, a total of 1256 completed responses were included in the final analysis, providing adequate statistical power to examine differences across demographic groups.
Questionnaire Design
A self-administered questionnaire comprising 28 items, was developed based on previous literature21–24 and adapted to the study objectives. The questionnaire was organized into four main sections. Section A included five items capturing demographic characteristics (age group, gender, marital status, education level, and employment status). Section B consisted of two multiple-response items assessing participants’ lifetime exposure to medical imaging procedures and the frequency of repeated examinations. Section C contained 18 items evaluating knowledge and understanding of ionizing and non-ionizing radiation, including awareness of radiation sources (three items), identification of ionizing and non-ionizing imaging modalities (two multiple-response items), knowledge of radiation dose (one item), awareness of radiation-related risks (four items), patient confidence related to radiation understanding and communication (six items), and educational needs related to radiation safety (three items). Most items in Section C were measured using five-point Likert scales ranging from strongly disagree to strongly agree. Section D included three items addressing sources of information about medical imaging, preferred channels for receiving radiation-related information, and prior communication with healthcare professionals regarding radiation risks. The questionnaire was translated from English to Arabic and reviewed by two bilingual academic experts holding PhDs in health sciences with over 10 years of experience in medical research and survey development. Content validity was established through structured expert review, achieving a Content Validity Index (CVI) of 0.85 for relevance and clarity. Their feedback refined grammar, cultural appropriateness, and item clarity. A pilot study with 15 participants confirmed reliability (Cronbach’s α = 0.82)41 and comprehension ease before full deployment.
Data Collection
The survey was online for six weeks, allowing participants to complete the survey at their convenience without any influence. Clear instructions were provided at the beginning of the survey, and informed consent was obtained online before starting the survey. The average time required to complete the questionnaire was approximately 10–15 minutes.
Data Analysis
Collected data was entered into a secure, password-protected database and analyzed using SPSS software. Descriptive statistics (frequencies, percentages, means, standard deviations) were used to summarize participant demographics and response patterns. Identification accuracy was assessed by comparing participants’ responses with standard classifications of ionizing and non-ionizing imaging modalities. Correct identification scores were calculated separately for ionizing (six modalities) and non-ionizing (two modalities) procedures. For each correctly identified modality, one point was awarded. Composite scores were subsequently categorized into high and low accuracy groups for demographic comparisons. Inferential statistics were employed to examine associations between participants groups. Specifically, ANOVA analyses were conducted, with statistical significance set at p < 0.05.
Ethical Considerations
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki. The protocol was reviewed and approved by the Permanent Committee for Scientific Research Ethics at King Saud University, number (26–0097), ensuring adherence to ethical guidelines for research involving human subjects. Informed consent was obtained from all participants prior to their inclusion in the study. It was clearly stated that participation was entirely voluntary and that respondents could withdraw at any time without any consequences.
Results
A total of 1256 patients participated in the study (see Table 1), with 638 males (50.8%) and 618 females (49.2%). Majority of the participants were aged 26–35 years (n = 373, 29.7%), followed by 18–25 years (n = 276, 22.0%) and 36–45 years (n = 276, 22.0%). Majority of the participants were married (n = 676, 53.8%), while 461 were single (36.7%). Focusing on educational qualifications, majority of the participants had bachelor’s degree (n = 438, 34.9%), followed by postgraduate degree (n = 233, 18.6%), and primary education (n = 248, 19.7%). Most of the participants were employed (n = 535, 42.6%), followed by students (n = 269, 21.4%).
 |
Table 1 Participants Demographics |
Regarding exposure to radiological procedures, most of the participants were found to have undergone common imaging modalities. Ultrasound was the most frequently reported procedure (37.8%), followed by radiotherapy (35.6%), DEXA scans (35.7%), computed tomography (35.0%), fluoroscopy (35.1%), nuclear medicine scans (34.7%), magnetic resonance imaging (34.3%), radiography (X-ray) (33.8%), and mammography (32.8%). In relation to the repeated procedures or scans, one out of seven participants have undergone certain procedures more than three times in their lifetime. Highest repeated exposures were reported for DEXA scans (15.4%), ultrasound (15.2%), and radiography (15.1%), while repeated exposure to CT scans (13.8%) and nuclear medicine procedures (13.6%) was comparatively lower.
Considerable number of participants reflected the awareness that natural sources of ionizing radiation exist in daily life, with 545 participants agreeing (43.4%) and 430 strongly agreeing (34.2%), while 260 were neutral (20.7%) and only 21 disagreed (1.7%). In relation to the procedures that use ionizing radiation, computed tomography was most frequently selected (n = 774, 61.6%), followed by nuclear medicine scans (n = 770, 61.3%), ultrasound (n = 766, 61.0%), radiotherapy (n = 752, 59.9%), fluoroscopy (n = 748, 59.6%), mammography (n = 748, 59.6%), magnetic resonance imaging (n = 734, 58.4%), and radiography (X-ray) (n = 724, 57.6%). In contrast, considerable number of participants incorrectly classified ionizing modalities as non-ionizing, with fluoroscopy (n = 526, 41.9%), nuclear medicine (n = 523, 41.6%), computed tomography and mammography (each n = 519, 41.3%); and MRI (n = 512, 40.8%) being commonly misidentified.
Differences were identified across demographic groups in correctly identifying the ionizing procedures (see Table 2). Higher identification accuracy was observed among participants with diploma and postgraduate education, older age groups (> 55 years), and female participants over their counterparts, indicating that that age, gender, and educational attainment influence patients’ understanding of radiation use in medical imaging.
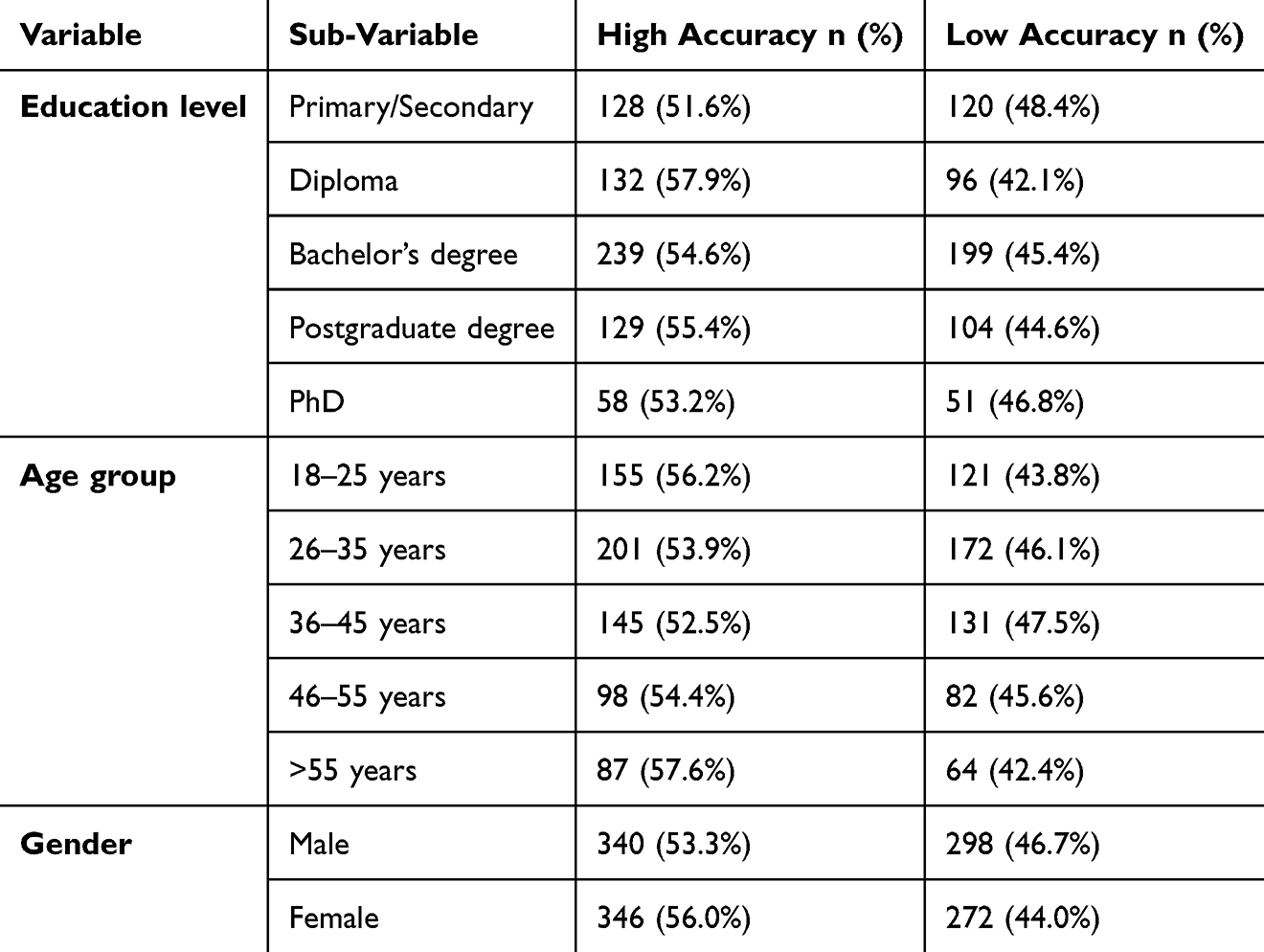 |
Table 2 Differences in Correct Identification of Ionizing Radiation Procedures by Demographic Groups |
In relation to the participants awareness of high radiation doses or intensity, computed tomography was most frequently selected (n = 428, 34.1%), followed by nuclear medicine procedures (n = 245, 19.5%) and radiography (X-ray) (n = 176, 14.0%). There are considerable number of participants who have incorrectly identified non-ionizing modalities as having the highest radiation dose, including magnetic resonance imaging (n = 166, 13.2%) and ultrasound (n = 131, 10.4%), while mammography (n = 110, 8.8%).
As shown in Table 3, high awareness of radiation-related risks was observed among the participants, with all risk items mean ratings being recorded above 4.0. Strong agreement was observed regarding children’s increased sensitivity to ionizing radiation (mean = 4.13, SD = 0.78) and the potential for health risks even at low radiation doses over time (mean = 4.14, SD = 0.78). Concern about radiation exposure from medical imaging was similarly high (mean = 4.12, SD = 0.79), indicating substantial risk perception among respondents.
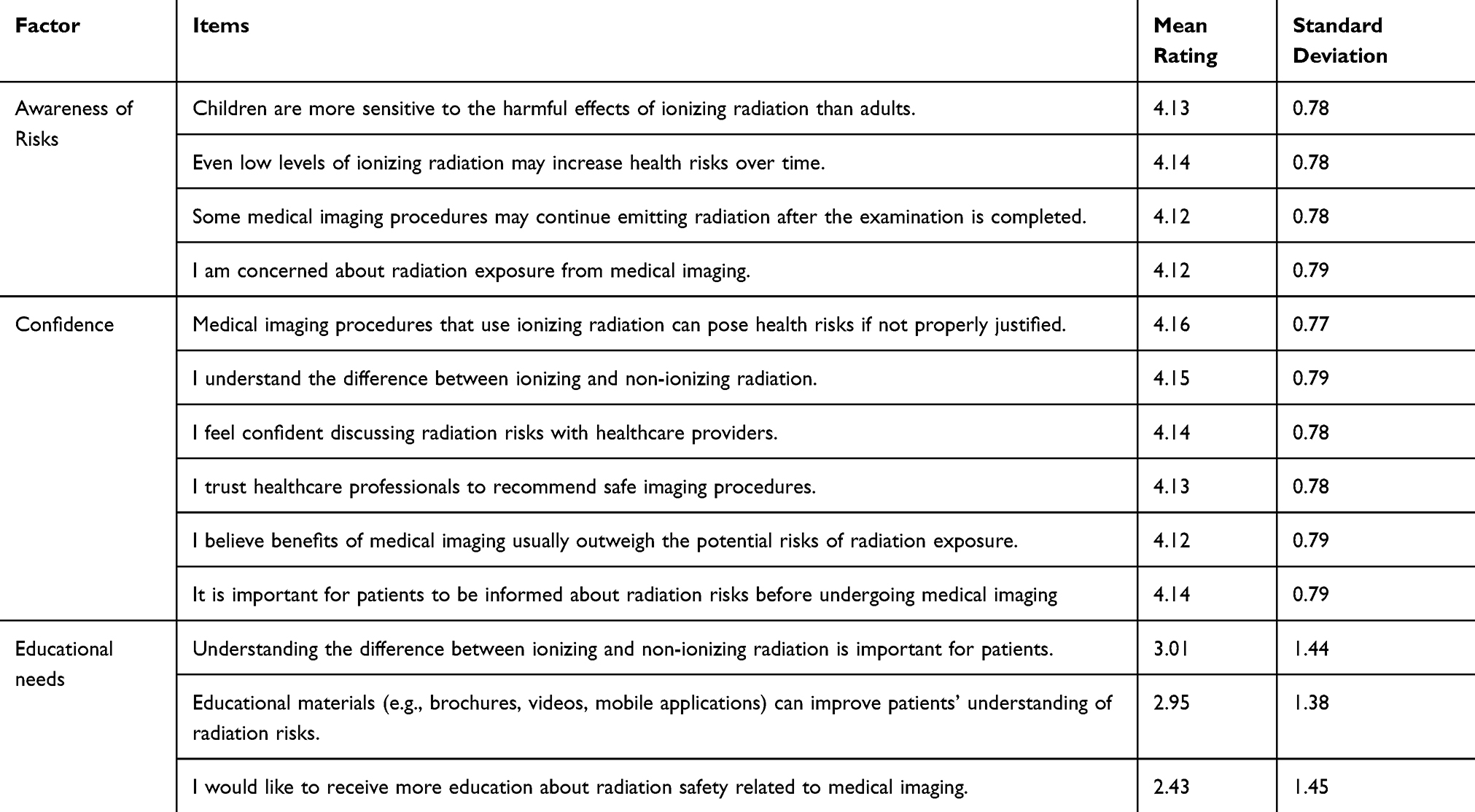 |
Table 3 Participants’ Awareness of Risks, Confidence, and Educational Needs |
High levels of patients’ confidence was observed among the participants. For instance, strong acknowledgment of the risks associated with unjustified ionizing imaging procedures (mean = 4.16, SD = 0.77) was observed among the participants. In addition, good understanding of the difference between ionizing and non-ionizing radiation (mean = 4.15, SD = 0.79) was observed. Participants expressed confidence in discussing radiation risks with healthcare providers (mean = 4.14, SD = 0.78). Trust in healthcare professionals to recommend safe imaging procedures was also high (mean = 4.13, SD = 0.79), in parallel with the belief that imaging benefits generally outweigh potential radiation risks (mean = 4.12, SD = 0.79).
Participants highlighted the importance of understanding radiation types (mean = 3.01, SD = 1.44) and agreed that educational materials could enhance patients’ understanding of radiation risks (mean = 2.95, SD = 1.38). However, despite this recognition, willingness to receive additional education about radiation safety was low (mean = 2.43, SD = 1.45), reflecting a potential gap between perceived knowledge sufficiency and openness to further learning.
Statistically significant differences in awareness of risks related to ionizing radiation were observed across age groups, gender, and education levels as shown in Table 4. Increase in awareness levels was observed in parallel with increase in age, with mean values rising from 3.98 among participants aged 18–25 years to 4.26 among those aged over 55 years with statistically significant difference (F = 9.74, p < 0.0001). Similar observation was made with respect to the education levels, as mean scores increased from 3.38 among participants with primary or secondary education to 4.87 among those holding a PhD (F = 2.38, p < 0.0001). Female participants demonstrated significantly higher awareness than males (mean = 4.18 vs. 4.07; t = 1.65, p = 0.001). In contrast, no statistically significant differences were observed across employment status categories (F = 1.24, p = 0.292), indicating comparable levels of risk awareness irrespective of occupational status.
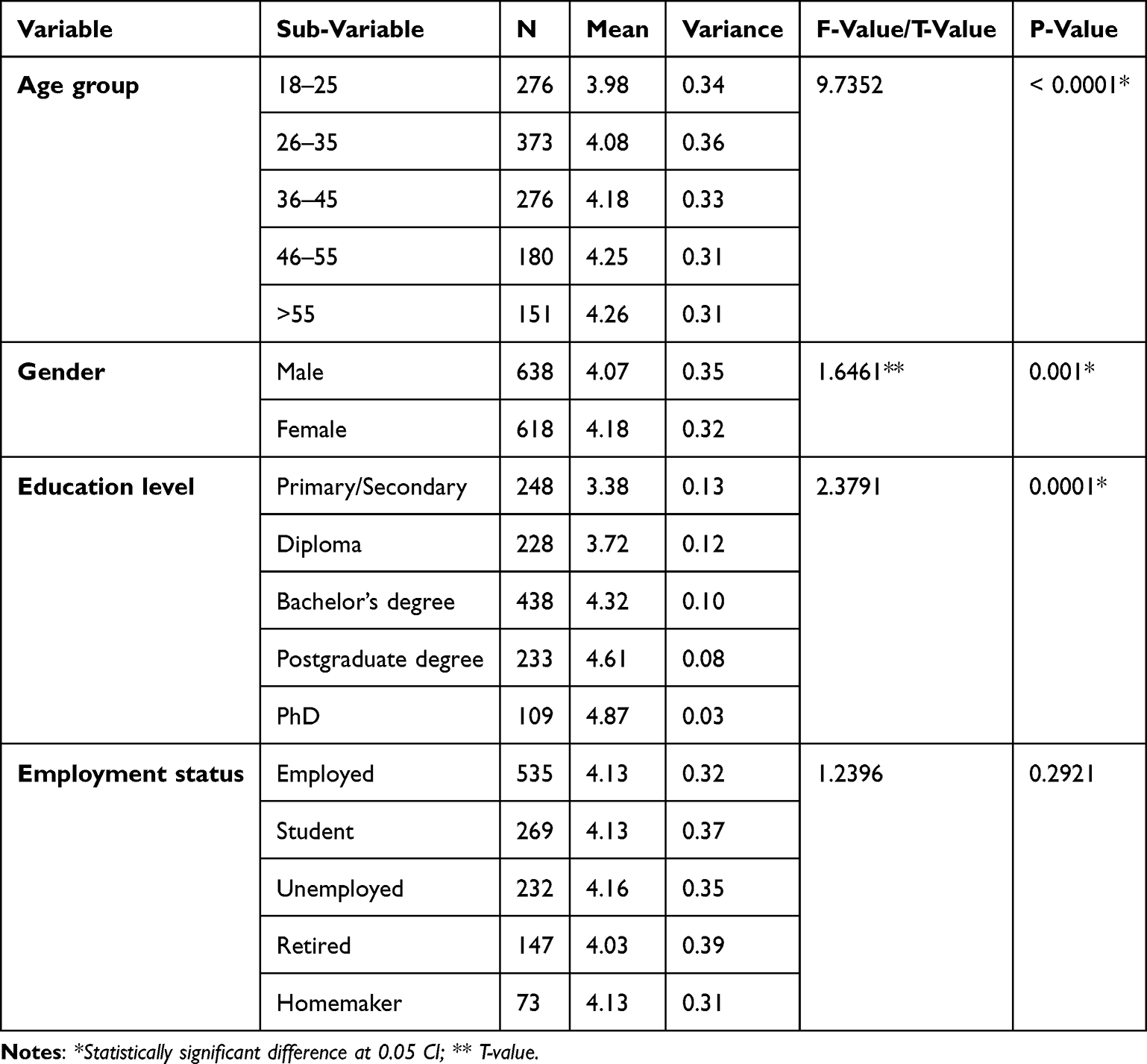 |
Table 4 Differences Among the Participants Groups in Relation to the Awareness of Risks Related to Ionizing Radiation Using |
As shown in Table 5, patients’ confidence related to ionizing radiation differed significantly across age groups, gender, and education levels. Mean confidence scores increased with increase in age, from 4.00 among participants aged 18–25 years to 4.30 among those aged over 55 years reflecting a statistically significant difference (F = 11.17, p < 0.0001) among the age groups. Female participants reflected significantly higher confidence levels than males (mean = 4.19 vs. 4.09; t = 1.65, p = 0.0005). Educational qualification was strongly associated with confidence, with mean scores rising from 3.40 among participants with primary or secondary education to 4.87 among those holding a PhD (F = 2.38, p < 0.0001). In contrast, differences in confidence across employment status categories were not statistically significant (F = 2.11, p = 0.077), indicating similar confidence levels irrespective of employment status.
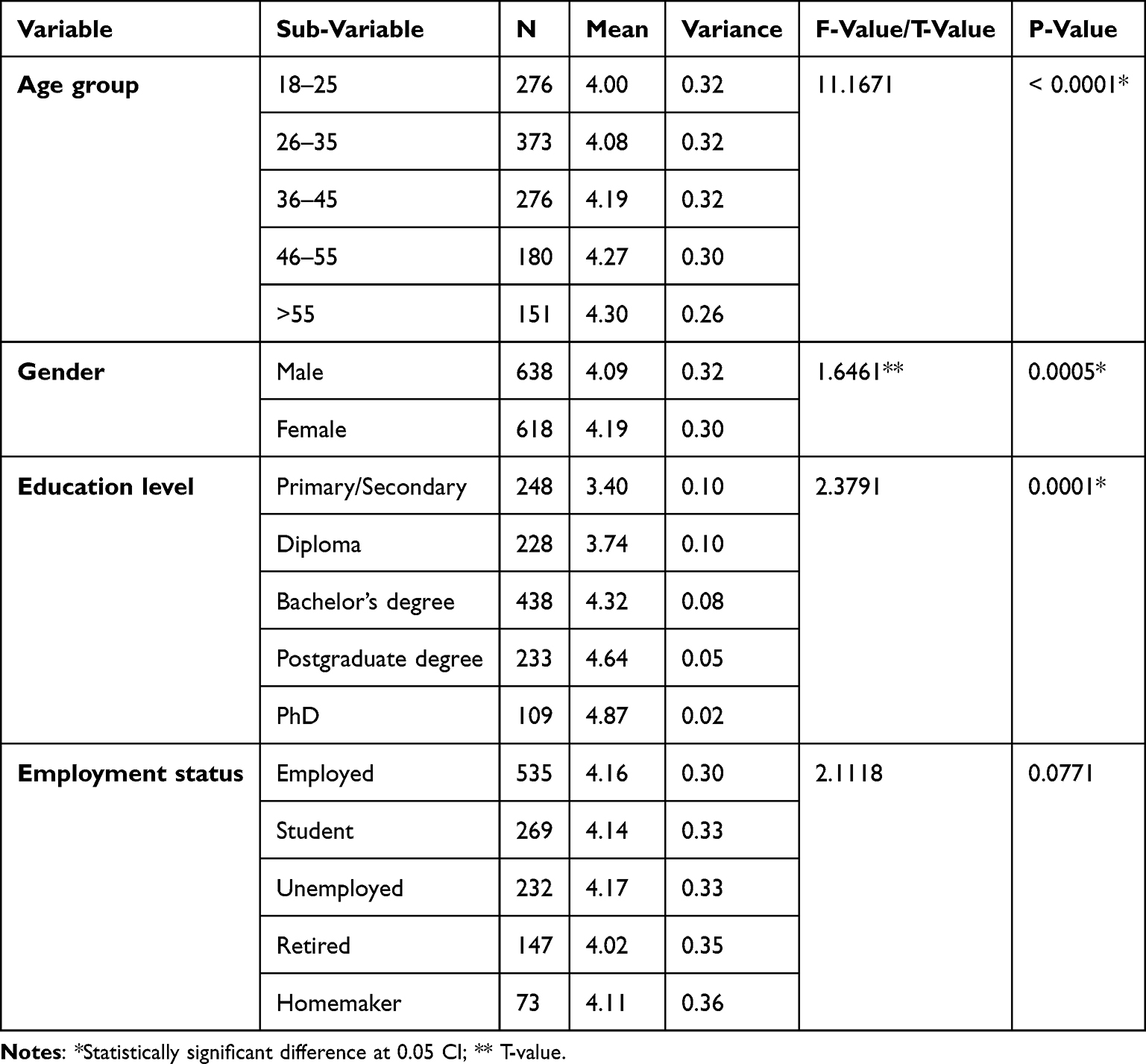 |
Table 5 Differences Among the Participants Groups in Relation to the Patients’ Confidence Related to Ionizing Radiation Using |
Statistically significant differences in educational needs (see Table 6) related to ionizing radiation were observed across age groups, gender, and education levels. Statistically significant (F = 11.76, p < 0.0001) was observed in relation to the education needs with younger patients reflecting less educational needs compared to older age group patients, as educational needs scores increased from a mean of 2.66 among participants aged 18–25 years to 2.85 among those aged over 55 years. Similar observations were made with respect to educational qualification, with mean scores rising from 2.26 among participants with primary or secondary education to 3.25 among those holding a PhD (F = 2.38, p = 0.0001). Female participants reported significantly higher educational needs than males (mean = 2.79 vs. 2.72; t = 1.96, p = 0.0008). However, differences across employment status categories were not statistically significant (F = 1.80, p = 0.126), indicating similar educational needs regardless of occupational status.
 |
Table 6 Differences Among the Participants Groups in Relation to the Educational Needs Related to Ionizing Radiation Using |
Regarding sources of information about medical imaging and radiation risks, most participants reported obtaining information from healthcare professionals (n = 484, 38.5%), followed by the internet or social media (n = 400, 31.8%). Few participants relied on television or radio (n = 133, 10.6%) or family and friends (n = 117, 9.3%), while 122 participants (9.7%) indicated that they had never received information about radiation risks. In relation to preferred sources of information, the majority reflected a preference for receiving information from physicians (n = 423, 33.7%) or radiologists (n = 370, 29.5%), followed by radiographers (n = 225, 17.9%), with fewer participants preferring public health campaigns (n = 121, 9.6%) or nurses (n = 117, 9.3%). Despite this preference for professional communication, fewer than half of the participants reported that healthcare professionals had explained radiation risks prior to an imaging procedure (n = 535, 42.6%), whereas the majority indicated that no such explanation had been provided (n = 721, 57.4%).
Discussion
This study has been conducted to comprehensively analyze patients’ knowledge, perceptions, confidence, and educational needs regarding ionizing and non-ionizing radiation used in medical imaging in Saudi Arabia. The findings reflected persistent modality-specific knowledge gaps and misconceptions, and revealed relatively high levels of perceived risk awareness and confidence. In similar to previous studies,21–25,27 a considerable number of participants misclassified imaging modalities, particularly identifying non-ionizing procedures such as MRI (40.8%) and ultrasound (38.4%) as ionizing; and ionizing modalities such as fluoroscopy (41.9%), nuclear medicine (41.6%), CT (41.3%) as non-ionizing radiation modalities; and underestimating the radiation dose associated with CT. Similar misconceptions were also found in studies conducted in other countries,25,28 indicating that such knowledge gaps are not context-specific, but reflect global deficits in public radiation literacy. Considering the rising frequency of using radiation based imaging,12–15 it is important to address such misconceptions to improve patients’ decision-making and informed consent procedures.
Despite the gaps in the knowledge, patients reflected high awareness levels in relation to radiation-related risks, including the increased sensitivity of children to ionizing radiation and the potential long-term health effects of low-dose exposure. Similar observations were made in,25,28,29 reflecting heightened concern among patients even in the presence of limited factual understanding. Such dissociation between objective knowledge and perceived risk highlights the importance of addressing both cognitive and affective components of radiation education, as excessive concern may lead to anxiety and reluctance toward clinically justified imaging modalities; and underestimation may encourage repeated exposure without questioning.29
In relation to patient confidence, which is poorly explored in previous studies, participants in this study reflected high confidence in their understanding of radiation concepts and in discussing radiation risks with healthcare providers, which contrasts with earlier findings indicating low patient confidence and passive engagement in decision-making.30–33 This discrepancy may be attributed to the growing public exposure to health information through digital platforms in Saudi Arabia or increasing trust in healthcare professionals, as a part of vision 2030 initiative of digitalization. However, one of the key concerns identified was that fewer than half of participants received explanations about radiation risks prior to imaging aligns with prior evidence of inconsistent clinician–patient communication,22,32,34 suggesting that confidence may not always be grounded in comprehensive understanding.
Demographic analyses revealed that older age, higher education, and female gender were associated with greater awareness, confidence, and educational needs, consistent with previous studies.18,21,22,25,31,37 As employment status reflected no statistically significant difference, it can be assumed that formal education and life experience play a stronger role in shaping radiation literacy than occupational status. These findings highlight the need for targeted and stratified education strategies focusing on younger and less-educated populations, who remain at greater risk of misunderstanding radiation-related information.
Current modality recognition rates (57.6–61.6%) exceed Smith et al (29.7% good knowledge, n = 1,024)42 but align with dose misperceptions reported in43 (62% CT = X-ray equivalence vs. our 65.9%) and (58% CT misconceptions).44 Higher recognition in this study likely reflects the larger sample (1,256 vs. 300–1,024) and more recent Vision 2030-era data collection. European findings40 mirror modality confusion (43% ultrasound misclassification vs. our 40.8% MRI confusion), while Australian patients demonstrated poor PET/CT recognition despite 85.6% lacking physician risk discussion—paralleling our 57.4% “no explanation” rate.39 These cross-national patterns validate universal radiation literacy deficits. Unlike single-domain studies,21–28 this investigation uniquely documents high confidence (mean 4.15) despite 40.8% modality misclassification, identifying overconfidence as a novel education barrier. The multi-dimensional approach (knowledge + confidence + needs + preferences) provides comprehensive, actionable insights absent from prior literature.
Theoretical and Practical Implications
Focusing on theoretical implications, this study extends radiation literacy research by integrating knowledge, risk perception, confidence, and educational needs within a single framework, demonstrating that confidence and perceived awareness may not always reflect accurate understanding. In relation to practical implications, the findings highlight the need for structured, clinician-led communication at the point of care and for tailored educational interventions addressing demographic disparities. Integrating radiation education into routine imaging workflows and leveraging trusted healthcare professionals may enhance informed consent, reduce anxiety, and support ALARA principles in clinical practice.
Recommendations
It is recommended that healthcare organizations should implement standardized radiation communication protocols, ensuring that patients receive clear, consistent explanations before imaging procedures. Furthermore, educational materials must be tailored to literacy level and age—such as brief brochures, infographics, or short videos, should be promoted. In addition, training programs for physicians and radiology staff should emphasize effective risk communication and shared decision-making. Public health campaigns may further support community-level awareness, particularly among younger and less-educated populations.
Study Limitations
This study employed a cross-sectional design, limiting causal inferences. Convenience sampling may restrict generalizability, particularly to rural or less digitally connected populations. Self-reported responses are subject to recall and social desirability bias. Although the questionnaire demonstrated good reliability, objective knowledge assessments were not included. Future longitudinal and mixed-methods studies are recommended to explore changes in awareness and confidence over time.
Conclusion
This study reflects that while patients in Saudi Arabia exhibit high perceived awareness and confidence regarding ionizing radiation, significant misconceptions about imaging modalities and radiation dose still persist. Among 1,256 Saudi patients, 57.6–61.6% correctly identified ionizing modalities yet 40.8% misclassified MRI as ionizing and only 34.1% recognized CT as highest-dose, confirming persistent knowledge gaps; however, patients reported high confidence (mean 4.15, SD 0.79) despite these deficits, representing the study’s most critical finding—this confidence-knowledge discrepancy constitutes a major barrier because overconfident patients (means >4.0) are less likely to seek educational materials (mean need 2.43), as older patients (>55 years), higher-educated individuals, and females showed superior awareness (p<0.001). Clinical recommendation: Implement standardized 2-minute pre-imaging risk communication protocols documenting modality type, relative dose (“CT = 100 chest X-rays”), and ALARA principles with QR-accessible infographics. Limitations include convenience sampling from tertiary centers and potential social desirability bias in self-reported confidence; future multi-center studies should validate findings across primary care settings to transform passive acceptance into informed shared decision-making.
Acknowledgment
Ongoing Research Funding program(ORF-2026-1430), King Saud University, Riyadh, Saudi Arabia.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Talapko J, Talapko D, Katalinić D, et al. Health effects of ionizing radiation on the human body. Medicina. 2024;60(4):653. doi:10.3390/medicina60040653
2. Rodrigues BV, Lopes PC, Mello-Moura AC, Flores-Fraile J, Veiga N. Literacy in the scope of radiation Protection for healthcare professionals Exposed to ionizing radiation: a Systematic review. Healthcare. 2024;12(20):2033. doi:10.3390/healthcare12202033
3. Mavrodinova S, Chernogorova Y. Insights into patient awareness and preferences in medical imaging procedures involving ionizing radiation. Polish J Med Phys Eng. 2024;30(3):108–13. doi:10.2478/pjmpe-2024-0013
4. Najjar R. Radiology’s Ionising Radiation Paradox: weighing the indispensable against the detrimental in medical imaging. Cureus. 2023;15(7):e41623. doi:10.7759/cureus.41623
5. Jahng JWS, Little MP, No HJ, Loo BW, Wu JC. Consequences of ionizing radiation exposure to the cardiovascular system. Nat Rev Cardiol. 2024;21(12):880–898. doi:10.1038/s41569-024-01056-4
6. Wassipaul C, Janata-Schwatczek K, Domanovits H, et al. Ultra-low-dose CT vs. chest X-ray in non-traumatic emergency department patients – a prospective randomised crossover cohort trial. EClinicalMedicine. 2023;65:102267. doi:10.1016/j.eclinm.2023.102267
7. Srivastava T, Chirikova E, Birk S, et al. Exposure to Ionizing Radiation and Risk of Dementia: a Systematic Review and Meta-Analysis. Radiat Res. 2023;199(5):490–505. doi:10.1667/rade-22-00153.1
8. Samaila B, Sagagi YM, Bello A, et al. Dosimetric Study on Natural Background Ionizing Radiation and Impact Assessment on Public Health: a systematic Review in Nigeria. Int J Adv Health Sci Technol. 2022;2(5). doi:10.35882/ijahst.v2i5.148
9. Taha A, Zgair IA, Hussein AA, et al. Biological Effects of Ionizing and Non-Ionizing Radiation: a Comprehensive Review of health and Environmental Impacts. Int J Design Nat Ecodyn. 2025;20(4). doi:10.18280/ijdne.200417
10. Maqbool M. An Introduction to Non-Ionizing Radiation. Bentham Science Publishers; 2023:162–179.
11. World Health Organization: WHO. Ionizing radiation and health effects. 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/ionizing-radiation-and-health-effects.
12. Rehani MM, Yang K, Melick ER, et al. Patients undergoing recurrent CT scans: assessing the magnitude. Eur Radiol. 2020;30(4):1828–1836. doi:10.1007/s00330-019-06523-y
13. Brambilla M, Vassileva J, Kuchcinska A, Rehani MM. Multinational data on cumulative radiation exposure of patients from recurrent radiological procedures: call for action. Eur Radiol. 2020;30(5):2493–2501. doi:10.1007/s00330-019-06528-7
14. Rehani MM, Hauptmann M. Estimates of the number of patients with high cumulative doses through recurrent CT exams in 35 OECD countries. Phys Med. 2020;76:173–176. doi:10.1016/j.ejmp.2020.07.014
15. International Atomic Energy Agency. Recurrent imaging. Available from: https://www.iaea.org/resources/rpop/resources/recurrent-imaging.
16. ICRP. The 2007 Recommendations of the International Commission on Radiological Protection. ICRP Publication 103. Ann. ICRP 37 (2–4). 2007. Available from: https://www.icrp.org/publication.asp?id=ICRP%20Publication%20103.
17. Suleiman AK, Ming LC. Transforming healthcare: Saudi Arabia’s vision 2030 healthcare model. J Pharmaceutical Policy Pract. 2025;18(1):2449051. doi:10.1080/20523211.2024.2449051
18. Alshihri AA, Hadadi I, Alqahtani B, et al. Assessing the Awareness of Medical Ionizing Radiation Exposure among General Public in Saudi Arabia: aseer Region. King Khalid Univ J Health Sci. 2024;9(2):150–156. doi:10.4103/kkujhs.kkujhs_23_24
19. Naderi M, Salehi F, Maleki S, Zahabi KS, Zahabi SS. The need to increase patient awareness of radiation exposure in imaging modalities: a study on the awareness and attitude of patients. J Med Imaging Radiat Sci. 2021;52(3):450–455. doi:10.1016/j.jmir.2021.05.006
20. Chen J, Zheng J, Zhang Q, Zhang J, Dai Q, Zhang D. Radiation exposure in recurrent medical imaging: identifying drivers and high-risk populations. Front Public Health. 2025;13:1626906. doi:10.3389/fpubh.2025.1626906
21. Alghamdi SA. Patients’ knowledge and perceptions of ionizing radiation from medical imaging in Saudi Arabia. J Radiat Res Appl Sci. 2025;18(3):101803. doi:10.1016/j.jrras.2025.101803
22. Alburayh AA, Alosaimi M, Alshumiesy H, et al. Assessment of Public Knowledge and Perceptions Toward Radiation Exposure Risks in Saudi Arabia: a Survey Study. Cureus. 2025;17(3):e80351. doi:10.7759/cureus.80351
23. Wedyan HH, Mohammed SA, Razan SA, Rajaa AM. Knowledge and Perception of Radiation Exposure by Patients in Diagnostic Radiology in Saudi Arabia 2024. JICRCR. 2024;22:2164–2169.
24. Alashban Y, Alghamdi SA. Patient perspectives on ionising radiation exposure from computed tomography in Saudi Arabia: a knowledge and perception study. Radiat Protect Dosimetry. 2024;200(7):687–692. doi:10.1093/rpd/ncae106
25. Bastiani L, Paolicchi F, Faggioni L, et al. Patient perceptions and knowledge of ionizing radiation from medical imaging. JAMA Netw Open. 2021;4(10):e2128561. doi:10.1001/jamanetworkopen.2021.28561
26. Memon JA, Memon ZA, Shah MS, Chandio MS, Baloch A. Examining the role of radiation risk perception in patient decision-making for diagnostic imaging procedures: insights from a multi-centre study across diverse populations. Radiography. 2025;31(5):103005. doi:10.1016/j.radi.2025.103005
27. Alsubaie FH, Abujamea AH. Knowledge and Perception of Radiation Risk From Computed Tomography Scans Among Patients Attending an Emergency Department. Cureus. 2024;16(1):e52687. doi:10.7759/cureus.52687
28. Ribeiro A, Husson O, Drey N, et al. Ionising radiation exposure from medical imaging - A review of Patient’s (un) awareness. Radiography. 2020;26(2):e25–e30. doi:10.1016/j.radi.2019.10.002
29. Smith-Bindman R, Chu PW, Firdaus HA, et al. Projected lifetime cancer risks from current computed tomography imaging. JAMA Intern Med. 2025;185(6):710. doi:10.1001/jamainternmed.2025.0505
30. Osborne C, Merchant S, Knight K, Sim J, Wright C. A phenomenological study investigating experiences of student learning using an online radiation therapy planning curriculum. Technical Innov Patient Support Radiat Oncol. 2022;24:6–12. doi:10.1016/j.tipsro.2022.08.009
31. Nyathi M, Thabane N. Evaluation of Doctor–Patient communication regarding medical examinations involving ionizing radiation: a Cross-Sectional study. Adv Public Health. 2025;2025(1). doi:10.1155/adph/5000212
32. Mellis S, Zhang Y, McAteer D. Awareness of radiation risks by medical students & referrers requesting radiological examinations in the North of Scotland: an audit. BMC Med Educ. 2024;24(1):830. doi:10.1186/s12909-024-05461-8
33. Jalal RB, Sheikh A, Khajuria A. Awareness and attitudes toward radiation risks among patients undergoing diagnostic imaging in North India: a cross-sectional study. Santosh University J Health Sci. 2025;11(1):63–67. doi:10.4103/sujhs.sujhs_26_25
34. Matković A, Ferenc T, Dimjašević L, et al. Knowledge and perceptions of ionising radiation among Croatian general practitioners: is there cause for concern? Arh Hig Rada Toksikol. 2025;76(1):24–30. doi:10.2478/aiht-2025-76-3916
35. Shubayr N, Muawwadhah M, Shami M, et al. Assessment of radiation safety culture among radiological technologists in medical imaging departments in Saudi Arabia. Radioprotection. 2024;59(1):30–35. doi:10.1051/radiopro/2023042
36. Vukani N, Lindiwe G, Bronwin VW. Radiographers’ awareness, understanding, and implementation of diagnostic reference levels in medical imaging: a scoping review. J Med Imaging Radiat Sci. 2025;56(6):102101. doi:10.1016/j.jmir.2025.102101
37. Hollada J, Speier W, Oshiro T, et al. Patients’ perceptions of radiation exposure associated with mammography. Am J Roentgenol. 2015;205(1):215–221. doi:10.2214/ajr.14.13650
38. Alzahrani HM, Alzahrani F, Aljohani H, et al. An Exploratory Analysis of Public Perspectives and Attitudes Towards Radiation in Saudi Arabia. Healthcare. 2025;13(19):2538. doi:10.3390/healthcare13192538
39. Singh N, Mohacsy A, Connell DA, Schneider ME. A snapshot of patients’ awareness of radiation dose and risks associated with medical imaging examinations at an Australian radiology clinic. Radiography. 2017;23(2):94–102. doi:10.1016/j.radi.2016.10.011. Epub 2016 Nov 17. PMID: 28390555.
40. Della Monaca S, Dini V, Grande S, et al. Assessing radiation risk perception by means of a European stakeholder survey. J Radiol Prot. 2021;41(4). doi:10.1088/1361-6498/abf75a
41. Taber KS. The Use of Cronbach’s Alpha When Developing and Reporting Research Instruments in Science Education. Res Sci Educ. 2018;48:1273–1296. doi:10.1007/s11165-016-9602-2
42. Smith SK, Petrak LM, Dhillon HM, Taylor J, Milross CG. Are radiation oncologists aware of health literacy among people with cancer treated with radiotherapy? Eur J Cancer Care. 2014;23(1):111–120. doi:10.1111/ecc.12111
43. Gavrilas L, Kotsis KT. Electromagnetic radiation: a comprehensive review of misconceptions. Eurasian J Sci Environ Educ. 2024;4(2):19–38. doi:10.30935/ejsee/15719
44. Brage K, Jensen J, Brage O, et al. Radiation awareness and occupational concerns among radiographers and students. Radiography. 2026;32(4):103356. doi:10.1016/j.radi.2026.103356
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.