Back to Journals » Patient Preference and Adherence » Volume 16
Awareness and Perception of Hospitalized Patients on Thromboembolism and Thromboprophylaxis: A Cross-Sectional Study in Sana’a-Yemen
Authors Halboup AM ![]() , Alzoubi KH
, Alzoubi KH ![]() , Mohamed Ibrahim MI
, Mohamed Ibrahim MI ![]() , Syed Sulaiman SA
, Syed Sulaiman SA ![]() , Almahbashi Y, Al-Arifi S
, Almahbashi Y, Al-Arifi S ![]() , Mohammed S
, Mohammed S ![]() , Othman G
, Othman G
Received 31 March 2022
Accepted for publication 6 July 2022
Published 11 July 2022 Volume 2022:16 Pages 1649—1661
DOI https://doi.org/10.2147/PPA.S368839
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Abdulsalam M Halboup,1 Karem H Alzoubi,2,3 Mohamed Izham Mohamed Ibrahim,4 Syed Azhar Syed Sulaiman,5 Yasmin Almahbashi,1 Shaima Al-Arifi,1 Sarah Mohammed,1 Gamil Othman1
1Department of Clinical Pharmacy and Pharmacy Practice University of Science and Technology, Sana’a, Yemen; 2Department of Pharmacy Practice and Pharmacotherapeutics, University of Sharjah, Sharjah, United Arab Emirates; 3Department of Clinical Pharmacy, Jordan University of Science and Technology, Irbid, Jordan; 4Department of Clinical Pharmacy and Practice, Qatar University, Doha, Qatar; 5Discipline of Clinical Pharmacy, Universiti Sains Malaysia, Penang, Malaysia
Correspondence: Gamil Othman, Department of Clinical Pharmacy and Pharmacy practice, University of Science and Technology, Sana’a, Yemen, Tel + 967774960247, Email [email protected]
Purpose: Patients’ awareness toward VTE and thromboprophylaxis is critical for medication adherence. This study aimed to evaluate the patient’s awareness and perception towards VTE and its prophylaxis and to assess patient’s satisfaction towards the information given by the medical staff.
Participants and Methods: A cross-sectional survey was conducted among hospitalized patients who received VTE prophylaxis in public and private hospitals in Sana’a, Yemen. Besides sociodemographic variables, participants’ awareness and perception of VTE and its prophylaxis were evaluated. Variables’ association with VTE awareness were analyzed using univariable and multivariable logistic regression using SPSS.
Results: A total of 396 of the hospitalized patients agreed to participate in the study, with 31% (n = 121) have ever heard about VTE. The multivariable logistic regression findings revealed that the participants who did not have a profession had OR = 17.182 (P < 0.001) of being unaware of VTE compared with those who had one. Participants who did not have a personal history of VTE had OR = 7.580 (P < 0.001) of being unaware of DVT/PE compared with the participants who had a personal history of VTE. Male participants had OR = 2.839 (P < 0.005) of being unaware of DVT/PE compared with female participants. Participants who were illiterate had OR = 2.832 (P < 0.022) of being unaware of DVT/PE compared with participants with a higher level of education.
Conclusion: The study revealed lack of awareness and perception of VTE and its prophylaxis among hospitalized patients in Yemen. The patients who are unaware of the disease have wrong perception about their role in DVT prophylaxis. Patient’s education must be considered in healthcare setting to improve patient’s health outcomes.
Keywords: anticoagulation, deep vein thrombosis, pulmonary embolism, patient’s knowledge, patient’s perception
Introduction
Venous thromboembolism (VTE) encompasses pulmonary embolism (PE) and deep vein thrombosis (DVT). Long-term hospitalization is frequently complicated by VTE, causing prolonged hospital stay. Globally, VTE is also the leading cause of preventable hospital death.1–4Evidence-based strategies were implemented to determine the patients at high risk for VTE, such as elderly persons and those with congestive heart failure, cancer, or patients who undergo major surgery.5 Typically, patients who are recognized to be at high risk of VTE should be provided with pharmacological prophylaxis on admission. Low dose anticoagulants, such as unfractionated heparin (5000 IU every 8–12 hours) or low-molecular weight heparin (40 mg every day or 30 mg twice a day), are the most commonly used anticoagulants prophylaxis for hospitalized medical and general surgical patients and should be continued throughout the period of VTE risk factors.6 Non-vitamin K antagonist oral anticoagulants (NOACs) are becoming more appealing for long-term VTE prophylaxis. Evidence shows that NOACs exert more clinical benefits without increase in hemorrhage in Total Hip and Knee Arthroplasty compared with traditional non-NOACs.7 Mechanical prophylaxis (eg, antiembolism stockings or intermittent pneumatic compression) can be provided to the hospitalized patients in whom pharmacological prophylaxis is contraindicated, and they as well should be extended until the patient is adequately able to walk.8
Evidence supports that all hospitalized patients should be counselled about the risk factors and consequences of VTE, the adverse effects of thromboprophylaxis medications, and the appropriate risk-reduction modalities prior to initiating thromboprophylaxis.9 Studies have shown that limited patient knowledge may negatively impact patient involvement in VTE treatment and prophylaxis.10–14 Educating the patient before medication initiation may enhance adherence, especially when the patients appreciate their medication purpose and the consequences of refusing thromboprophylaxis. A case in point, a study by Piazza et al found that a pharmacist-led individualized patient education program was associated with higher medication compliance and reduction in patient refusal. Thus, VTE has been recognized as a public health problem, and the priority of raising public knowledge of this condition is necessary to reduce mortality and morbidity.15
No studies have evaluated public awareness of thromboembolism and thromboprophylaxis in Yemen. This indicates a vital necessity to conduct this research to obtain information about the level of VTE knowledge among patients. This information will help the medical staff consider the value of educational programs for VTE patients to increase patients’ awareness. Therefore, this study aimed to assess the extent of public awareness about VTE and its prophylaxis among hospitalized patients in public and private hospitals in Sana’a, Yemen. Further, this study will also determine the awareness level of thromboembolism and thromboprophylaxis predictors.
Materials and Methods
Study Design and Location
This is a cross-sectional study where a validated questionnaire was distributed among hospitalized patients in two public hospitals (Kuwait Teaching Hospital, Aljomhori Teaching hospital) and five private hospitals (University of Science and Technology Hospital, Al-Khazan Hospital, Yemeni German Hospital, Saudi German Hospital and C-Plas Hospital) in Sanaa, the capital of Yemen. The above-mentioned hospitals were selected since they are the major teaching hospitals and cover the public and the private health sectors. The study was carried out from June to November 2020.
Ethics Approval and Consent to Participate
The protocol of this study was approved by the Ethical Committee of the Medical Research at the University of Science and Technology (Ref no: EAC/UST180). All participants were informed about the study objectives and consented to participate. This study complies with the Declaration of Helsinki, and all its amendments and revisions.
Study Population, Sample Size and Sampling Method
The number of hospital beds in both public and private sectors in Sana’a city was 2765 beds.16 Assuming a confidence level of 95%, a margin of error of 5%, and a response distribution of 50%, the minimum representative sample size was 338 based on Raosoft software (Raosoft. Inc., Seattle, USA). The sample size was increased by 22%, ie, n = 413, to account for the non-response rate. Patients were chosen by convenient sampling.
Inclusion and Exclusion Criteria
Participants who were hospitalized in the internal medicine wards and received DVT prophylactic dose of low molecular weight heparin (enoxaparin 30 mg twice daily or 40 mg once daily) or unfractionated heparin (5000 units two to three times a day) were recruited in the study. Those who were admitted to the critical care unit, emergency and those who were on the first day of their admission were excluded from the study.
Study Instrument
Previously validated questionnaires were used with slight modifications on their items.10,14 A forward translation from English to Arabic was performed. To ensure the validity of the content, the study instrument was reviewed by a multidisciplinary panel of experts: two cardiologists, one community medicine physician, and two holding a master’s in Clinical Pharmacy. The instrument of the study was piloted on a sample (n = 24) of hospitalized patients who were excluded from the final analysis of the study. In addition, the reliability of the survey was examined using Cronbach’s alpha, where the overall Cronbach’s alpha value was 0.766. The questionnaire involved twenty-nine closed-ended questions prepared to determine: patients’ sociodemographic data, including age, gender, educational level (low level is secondary school and less), smoking status, the reason for admission, comorbidities, and personal/family history of VTE or using thromboprophylaxis. In addition to more questions were incorporated to assess patients’ knowledge about the definition, clinical presentations, risk factors, underlying causes, potential complications, and prevention measures of VTE. These questions were incorporated as multiple-choice questions, and an option “I don’t know/not sure” was inserted as a last choice for each question so that the percent demonstrating the knowledge was not overestimated through guessing the correct answer. The rest of the questions assessed patients’ perception towards VTE and thromboprophylaxis, their satisfaction with thromboprophylaxis, and the information they received from health-care providers. Perception and satisfaction items were assessed using the nominal scale with “yes” or “no” questions. The patients who answered “yes” to these questions were classified as satisfied and those who answered “no” were classified as unsatisfied.
Statistical Analysis
Categorical variables, ie, the demographic characteristics, comorbidity, the reason for admission, personal and family history of DVT and PE, participants’ awareness of the correct risk factors, signs and symptoms, complications, preventive measures of DVT and PE, participants’ positive perception of VTE and satisfaction about thromboprophylaxis (indicated by a response of yes or no) were represented as frequency and percentage. Participants were classified as “aware” of VTE when they correctly answered four or more questions related to awareness of VTE including definition, causes, sign and symptoms, complications, risk factors, and preventive strategies of VTE. Those who answered less than four questions were classified as “unaware” of VTE. Univariable logistic regression was utilized to investigate the association between participants’ variables and the awareness of VTE. Variables with p value of less than 0.25 in univariable logistic regression were included in the multivariable logistic regression to create a model of variables that best predict participants’ awareness toward PE and DVT. To measure the effect of each predictor on the awareness level, odd ratios were calculated. All statistical analyses were performed using SPSS (Release 21.0; IBM Corp., Armonk, NY, USA). Statistical significance was set at p < 0.05.
Results
Of the 413 patients who received thromboprophylaxis, 396 agreed to complete the study questionnaire, comprising a response rate of 94%. Table 1 demonstrates the sociodemographic data of the study participants. Most participants were between 18- and 40-year-old (41%, n = 164), females (73%, n = 289), had no profession (74%, n = 293), had a low education level (49%, n = 194), non-smokers (70%, n = 277), and had at least one chronic disease (32%, n = 125). The main reasons for hospital admission were surgery (57%, n = 226) or medical treatment (33%, n = 129). Majority of the participants denied personal history (92%, n = 351) and/or family history (86%, n = 282) of VTE.
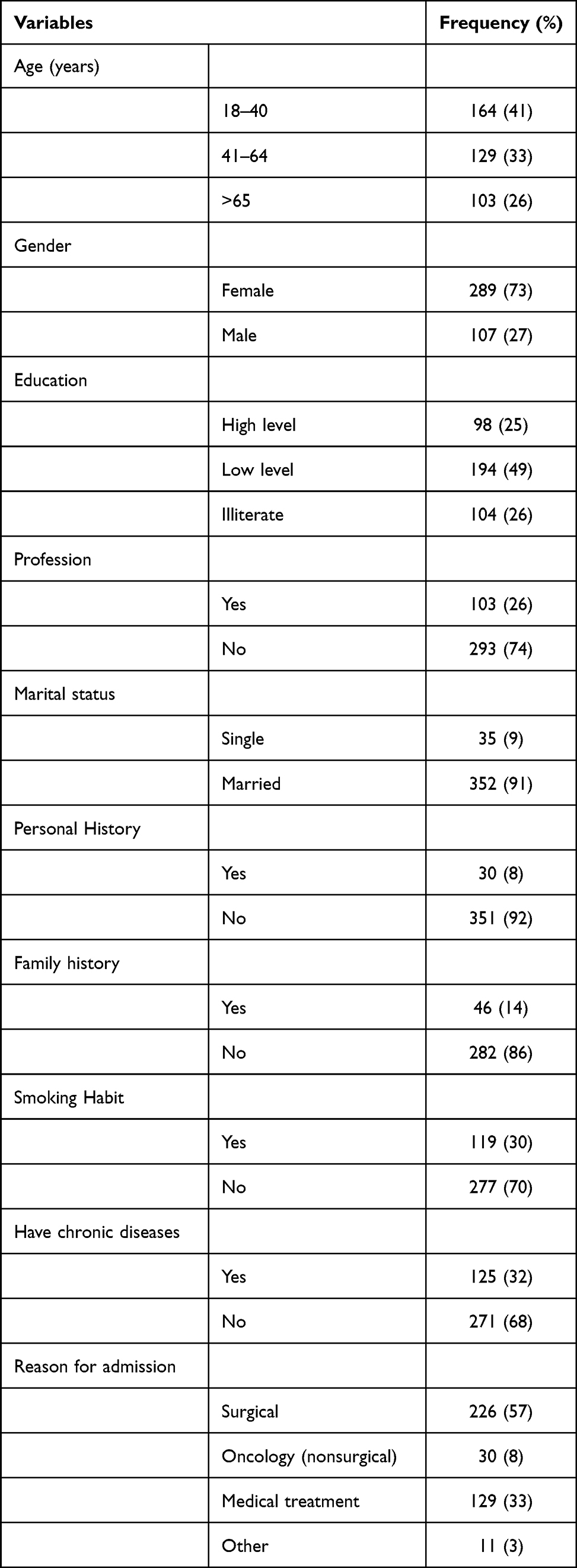 |
Table 1 Characteristic of Participants. Data are Presented as Frequency and Percentage |
As shown in Table 2, only 31% (n = 121) of the participants knew what a blood clot is. Among the participants who were interviewed, only 27 (7%) of the hospitalized patients recognized that DVT is a thrombus in the leg veins. Unilateral leg pain/tenderness (11%, n = 45), swelling (11%, n = 42), changes in the leg’s color (5%, n = 20), and warming of the leg (2%, n = 6) were properly recognized as signs/symptoms of DVT. However, 9% (n = 34) of the participants partially recognized the signs and symptoms of PE. Regarding VTE complications, proportions of 26% (n = 106) and 13% (n = 49) of the participants recognized the correct complications of DVT and PE, respectively.
 |
Table 2 Participants’ Awareness of Venous Thromboembolism. Data are Presented as Frequency and Percentage |
Regarding the risk factors of developing VTE, 27% (n = 108) of the participants recognized not moving for a long time as a risk of VTE, followed by surgery, hospital admission, cancer, and pregnancy, comprising 11% (n = 45), 8% (n = 32), 6% (n = 23), and 4% (n = 17), respectively. On the other hand, walking was correctly recognized by nearly one-third (32%, n = 127) of the participants as a VTE prevention strategy.
Perception of Participants About VTE
Most of the participants, 89% (n = 351) believed that a blood clot is a medical emergency that needs further consideration and that a clot might be prevented (66%, n = 261). Sixty percent (n = 239) of the participants believed that blood clots might cause death, and more than half (55%, n = 218) of them were aware that, if not treated appropriately, a blood clot can pass into the lungs (Table 3).
 |
Table 3 Participants’ Perception of VTE and Their Satisfaction About Thromboprophylaxis. Data are Presented as Frequency and Percentage |
Regarding thromboprophylaxis perception, most participants (67%, n = 266) believed in the safety and efficacy of thromboprophylaxis. More than two-thirds (70%, n = 276) of participants never minded receiving injectable thromboprophylaxis, and almost one-third (31%, n = 124) of them reported that the prophylactic heparin had tolerable adverse effects (Table 3).
Regarding participants’ satisfaction with thromboprophylaxis, majority the participants (69%, n = 274) were satisfied with the dose scheduling of heparin or enoxaparin, which did not interfere with their daily activities or sleep pattern. However, only 35% (n = 137) and 33% (n = 129) of the participants, respectively, were satisfied with the explanation and the information they received about VTE thromboprophylaxis.
Results of the Association Between Demographic Factors and the Awareness of VTE Using Univariable Logistic Regression
The factors that might affect participants’ awareness about VTE were subjected to a univariable logistic regression. The proportion of participants who reported unawareness of VTE was significantly higher among the participants who were not receiving enough information about VTE (OR = 7.254, P< 0.001), were unsatisfied with information provided about VTE (OR = 6.877, P< 0.001), had no personal history of VTE (OR = 5.717, P<0.001), disagreed with the time of receiving the injection (OR = 5.106, P<0.001), had no profession (OR = 4.884, P < 0.001), were not being counselled about the rationale of the use of VTE prophylaxis (OR = 4.797, P < 0.001), and those who were illiterate (OR = 3.871, P < 0.001; Table 4).
 |
Table 4 Variables Associated with Unawareness of DVT/PE Using Univariable Binary Logistic Regression |
Results of the Association Between Different Variables and VTE Awareness Using Multivariable Logistic Regression
Nine variables were included in the model of multivariable logistic regression as shown in Table 5. Participants who did not have a profession had OR = 17.182 (P < 0.001) of being unaware of DVT/PE compared with respondents who had a certain profession. Those who were illiterate had OR = 2.832 (P < 0.022) of being unaware of DVT/PE compared with those who had a higher level of education. Respondents who had no personal history of DVT/PE had a OR = 7.580 of being unaware about VTE compared with those who had a personal history of DVT/PE. Finally, male participants had OR = 2.839 (P < 0.005) of being unaware of DVT/PE compared with female.
 |
Table 5 Variables Associated with Unawareness of DVT/PE Using Multivariable Binary Logistic Regression |
Discussion
The current study’s findings indicated a lack of awareness about VTE among the majority of the hospitalized patients in both the public and the private hospitals in Sana’a, Yemen. Nearly one-third of hospitalized Yemeni patients answered questions related to the nature of blood clots correctly. Nevertheless, most patients could not recognize the signs and symptoms of DVT and PE. This might have had a consequence on self-assessment and self-reporting of possible VTE episodes. The findings of this study agree with the finding of studies conducted in other countries in the Middle East. For example, a study from Saudi Arabia by Almodaimegh et al found that only 32% and 15% of patients had awareness about DVT and PE, respectively.14 Similarly, awareness about DVT and PE among hospitalized Jordanian patients were 38% and 22%, respectively.11 Another study from Jordan conducted by Alzoubi et al, which assessed awareness of female patients who undergone cesarean section showed that there was poor knowledge about VTE among participants, particularly young females, with awareness of 46% and 18.7% about DVT and PE, respectively.17 Another study that was conducted in Saudi Arabia by Almegren et al showed low knowledge and awareness of VTE among the Saudi females who used or had been using oral contraceptive pills.18 In the current study, the participants showed a higher awareness level about DVT compared to PE. This result could be attributed to the fact that Yemeni patients were unaware that PE is considered a complication of DVT. This finding agrees with the study conducted in Jordan by Jarab et al.10 On the other hand in developed countries, a study from Canada by Saga et al found that most hospitalized patients (81.2%) had good knowledge of both DVT and PE.13 Another study from the United States by Konieczyńska et al reported that younger patients had good knowledge about VTE in general.19 In the current study, lack of awareness among participants could be attributed in part to the fact that hospitalized patients in Yemen were not educated enough about their medications and illness nor actively engaged in the management of their diseases.
This study revealed that respondents had poor knowledge about the risk factors of VTE and the necessary strategies to prevent VTE in hospitalized patients. Thus, those patients will not actively participate in DVT self-management. Epidemiological data estimate that unhealthy lifestyle risk factors, including obesity, western dietary pattern, physical inactivity, may contribute to 48% of the unprovoked VTE. Thus, improving high-risk individuals and general populations’ awareness about VTE risk factors was shown to reduce the incidence of unprovoked VTE in the whole population by 12%.20 In the current study, the most frequently reported risk factor for VTE is prolonged limited mobility. This finding shed light on the vital role of health-care providers in educating their patients about the benefits of ambulating during hospitalization. This finding is in agreement with other studies that were conducted in Jordan,10 Saudi Arabia,14,21 and Canada.13 Another study that was conducted to measure global public awareness of nine countries, including the United States, the United Kingdom, the Netherlands, Thailand, Japan, Germany, Canada, Australia, and Argentina, showed that immobility is the most recognized VTE risk factor in these countries.22 The study participants poorly recognized other risk factors of VTE, such as pregnancy, malignancy, surgery, and family history. As a result, more health education about VTE in hospitalized patients is crucial to make them active participants in VTE prophylaxis, thus, shifting VTE risk factors downward. In the line with the following studies,10,13 the finding of this study showed that walking or stretching the legs is the nonpharmacologic strategy to prevent VTE. Generally, insufficient knowledge about VTE is a common international concern, particularly for developing countries such as Yemen. A probable reason is the low education and not engaging the hospitalized patients in VTE self-management.
Improving awareness of hospitalized patients to DVT/PE is critical since such practice would have direct benefit on the patients’ health outcomes. For example, when a hospitalized patient knows that walking in the hospital corridor would have positive impact on risk reduction, he would start walking to reduce the risk instead of staying in his bed. Moreover, since the health system and insurance in Yemen is fragile due to the continuous political conflict, most patients in Yemen buy their medications from community pharmacies. This practice makes them underestimate the importance of thromboprophylaxis medication and leaving them unaware of VTE and its consequences.
The appropriate intervention to achieve high-level awareness about of VTE may be achieved by establishing patient-physician counseling session before initiating thromboprophylaxis. This practice might enhance patient’s role in VTE risk reduction and improve thromboprophylaxis adherence. Additionally, establishing VTE awareness campaign using different platforms for those at elevated risk of VTE would have positive impact on patients’ health outcome. Moreover, implementing clinical pharmacy services in both the public and the private sectors are necessary since clinical pharmacists review patients’ medications on daily basis, provide face-to-face counselling, and, thus, help in reducing drug-related problems.
Regarding the perception of participants towards VTE, the majority of participants (66%) agreed that VTE could be prevented and that untreated DVT could pass into the lungs (55%). The attitudes of the participants toward these two previous points were similar to that of the study conducted by Jarab et al10 but more than that reported by Almodaimegh et al from Saudi Arabia. Additionally, 89% of the current study participants believed that a blood clot is a medical emergency that they need to worry about it as it can lead to death, which agrees with Almodaimegh et al study.14 Similarity in the VTE perception of these previous studies might be attributed in part to the similarity of the culture among the countries where these studies were conducted.
In this study, most respondents agreed that thromboprophylaxis is safe and effective since such a drug would not be provided unless it is safe and effective. Similar findings were reported from previous studies by Almodiamegh et al and Jarab et al.10,14 Only a third of the participants reported their satisfaction with the clarification they received about the rationale of VTE prophylaxis. One-third of the patients received information and counselling about DVT/PE. These findings might justify the low awareness level of the participants about VTE, which in turn implies on the importance of providing the patients with the necessary counseling about VTE and its thromboprophylaxis. In this study, the effect of demographic factors on the awareness level of the participants was explored. Patients with a personal history or family history of VTE had significantly higher awareness levels since they were familiar with the clinical presentations of VTE. Additionally, patients who received information about VTE, or were exposed to explanations about thromboprophylaxis, had significantly higher awareness than those who did not. Moreover, participants who had a certain profession were likely to be educated, and thus they had higher awareness than those who had no profession. These groups of patients are likely to learn more about the disease and its signs and symptoms, which qualify them to adopt the risk reduction strategy of VTE.
Education also plays a significant role in the awareness level.16 The current study revealed that educated patients had significantly higher awareness levels than low education levels or illiterate ones. The current study’s findings are consistent with previous studies.10,14 Association between education level of the participants, receiving information and the awareness of the disease was also confirmed by Oh et al. Their study revealed that awareness level about stroke and its clinical presentations was higher among educated respondents, and among those who received information about the stroke via different platforms, such as websites, public education, and campaigns.23 In a randomized trial, the awareness level about VTE was significantly improved from 8% to 87% among postpartum women after implementing educational programs about VTE that were introduced by their nurses.24 On the other hand, demographic characteristics such as marital status had no significant effect on the awareness level of the participants. These results are consistent with Green and Bernhofer.25
The current study outlines the lack of awareness about VTE in hospitalized patients, which indicates the importance of enrichment and improving patients’ awareness of VTE. In a patient education program for VTE prevention in hospitalized patients by Piazza et al, it was found that pharmacist-led individualized patient education sessions were associated with higher medication adherence to clinician-ordered injectable pharmacological venous thromboembolism prophylaxis.15
This is the first study to explore hospitalized patients’ perceptions and knowledge of VTE prophylaxis in Yemen as a step forward. This study included seven private and public hospitals in Sana’a, the capital of Yemen. Moreover, the data for this study was collected via face-to-face interviews that allowed researchers to listen and realize patient’s desire to be educated about such medical issues. The current study had a limitation, as some study participants were illiterate, or their health barred them from cooperating; therefore, they were asked rather than given the survey to answer. Another potential drawback is social desirability bias on awareness and perception. Moreover, this study did not include questions related to the harm and complications of VTE prophylaxis, such as bleeding and heparin induced thrombocytopenia. One more limitation was that the pharmacological prophylaxis of VTE was commonly administered subcutaneously by health-care provider. Therefore, patients’ knowledge and attitude might not have great impact on the practices. As well, it is worth to mention that odds ratios measure used in the current study sometimes do not provide a good approximation of the relative increase in risk when the outcome is common.
Conclusion
This study shows a low awareness level toward VTE and its prophylaxis among hospitalized patients in Yemen. The study reveals that those unaware of these diseases have a wrong perception about DVT that affects their roles in VTE management. Future VTE management programs should concentrate on patients’ knowledge to improve their attitude and practice toward managing their disease. The rules for thromboprophylaxis should be clarified to patients by health care team.
Acknowledgment
The authors want to thank 6th year PharmD students Amal Alramadi, Hala althalji, and Shatha Alyousfi for helping in data collection.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Heit JA, Spencer FA, White RH. The epidemiology of venous thromboembolism. J Thromb Thrombolysis. 2016;41(1):3–14.
2. Gary E, Raskob PA, Blanco AN, et al. Thrombosis: a major contributor to the global disease burden. J Thromb Haemost. 2014;12(10):1580–1590.
3. Maynard GA, Morris TA, Jenkins IH, et al. Optimizing prevention of hospital‐acquired venous thromboembolism (VTE): prospective validation of a VTE risk assessment model. J Hosp Med. 2010;5(1):10–18.
4. Fernandez MM, Hogue S, Preblick R, Kwong WJ. Review of the cost of venous thromboembolism. Clinicoecon Outcomes Res. 2015;7:451. doi:10.2147/CEOR.S85635
5. Goldhaber SZ. Risk factors for venous thromboembolism. J Am Coll Cardiol. 2010;56(1):1–7. doi:10.1016/j.jacc.2010.01.057
6. Chisholm-Burns MA, Schwinghammer TL, Malone PM, Kolesar JM, Lee KC, Bookstaver PB. Pharmacotherapy Principles and Practice. McGraw Hill Professional; 2019.
7. Yi Y-H, Gong S, Gong T-L, Zhou L-Y, Hu C, Xu W-H. New oral anticoagulants for venous thromboembolism prophylaxis in total hip and knee arthroplasty: a systematic review and network meta-analysis. Front Pharmacol. 2022;12. doi:10.3389/fphar.2021.775126
8. Anderson JFA, Spencer FA. Risk factors for venous thromboembolism. Circulation. 2003;107(23_suppl_1):
9. Hill J, Treasure T. Reducing the risk of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to hospital: summary of the NICE guideline. Heart. 2010;96(11):879–882. doi:10.1136/hrt.2010.198275
10. Jarab AS, Al-Azzam S, Badaineh R, Mukattash TL, Bsoul R. Awareness and perception of thromboembolism and thromboprophylaxis among hospitalized patients in Jordan. Curr Clin Pharmacol. 2020;15(1):72–80. doi:10.2174/1574884714666190823162055
11. Apenteng PN, Fitzmaurice D, Litchfield I, et al. Patients’ perceptions and experiences of the prevention of hospital-acquired thrombosis: a qualitative study. BMJ open. 2016;6(12):e013839. doi:10.1136/bmjopen-2016-013839
12. Najafzadeh M, Kim S, Patterson C, et al. Patients’ perception about risks and benefits of antithrombotic treatment for the prevention of venous thromboembolism (VTE) after orthopedic surgery: a qualitative study. BMC Musculoskelet Disord. 2015;16(1):1–8. doi:10.1186/s12891-015-0777-x
13. Le Sage S, McGee M, Emed JD. Knowledge of venous thromboembolism (VTE) prevention among hospitalized patients. J Vasc Nurs. 2008;26(4):109–117. doi:10.1016/j.jvn.2008.09.005
14. Almodaimegh H, Alfehaid L, Alsuhebany N, et al. Awareness of venous thromboembolism and thromboprophylaxis among hospitalized patients: a cross-sectional study. Thromb J. 2017;15(1):1–8. doi:10.1186/s12959-017-0144-2
15. Piazza G, Nguyen TN, Morrison R, et al. Patient education program for venous thromboembolism prevention in hospitalized patients. Am J Med. 2012;125(3):258–264. doi:10.1016/j.amjmed.2011.09.012
16. Alwabr GM, Al-Mikhlafi AS, Al-Hakimi SA, Dughish MA. Determination of medical waste composition in hospitals of Sana’a city, Yemen. J Appl Sci Environ Manag. 2016;20(2):343–347.
17. Alzoubi KH, Khassawneh BY, Obeidat B, Asfoor SS, Al-azzam SI. Awareness of patients who undergo cesarean section about venous thromboembolism prophylaxis. J Vasc Nurs. 2013;31(1):15–20. doi:10.1016/j.jvn.2012.07.001
18. Almegren M, Eid AB, Alsuhaibani E, et al. Awareness about venous thromboembolism among Saudi female who use oral contraceptive pills: a descriptive cross-sectional study. Int J Med Sci Public Health. 2021;5(1). doi:10.32553/ijmsdr.v5i1.750.
19. Konieczyńska M, Sobieraj E, Bryk AH, et al. Differences in knowledge among patients with atrial fibrillation receiving non-vitamin K antagonist oral anticoagulants and vitamin K antagonists. Kardiol Pol. 2018;76(7):1089–1096. doi:10.5603/KP.a2018.0069
20. Folsom AR, Cushman M. Exploring opportunities for primary prevention of unprovoked venous thromboembolism: ready for prime time? J Am Heart Assoc. 2020;9(23):e019395. doi:10.1161/JAHA.120.019395
21. Al Bshabshe A, Mousa WF, Alshehri MS, et al. Awareness, knowledge, and attitude toward venous thromboembolism among Aseer Population, Saudi Arabia. J Family Med Prim Care. 2021;10(6):2411. doi:10.4103/jfmpc.jfmpc_2430_20
22. Wendelboe AM, McCumber M, Hylek EM, et al. Global public awareness of venous thromboembolism. J Thromb Haemost. 2015;13(8):1365–1371. doi:10.1111/jth.13031
23. Oh G-J, Moon J, Lee Y-M, et al. Public awareness of stroke and its predicting factors in Korea: a national public telephone survey, 2012 and 2014. J Korean Med Sci. 2016;31(11):1703–1710. doi:10.3346/jkms.2016.31.11.1703
24. Youness E, Hassen S, Youness H, Azer SZ. Effect of educational nursing program on reducing the incidence of venous thromboembolism among postpartum women. IOSR J Nurs Health Sci. 2016;5(4):53. doi:10.9790/1959-0504055362
25. Green J, Bernhofer EI. Effectiveness of a patient education plan on knowledge of post‐op venous thromboembolism survival skills. J Clin Nurs. 2018;27(7–8):e1485–e1493. doi:10.1111/jocn.14270
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Venous Thromboembolism Among Hospitalized Patients: Incidence and Adequacy of Thromboprophylaxis – A Retrospective Study
Ambra N, Mohammad OH, Naushad VA, Purayil NK, Mohamedali MG, Elzouki AN, Khalid MK, Illahi MN, Palol A, Barman M, Sharif M, Chalihadan S, Punnorath A, Mostafa A, Al Hariri B, Khidir TGM, Varikkodan I
Vascular Health and Risk Management 2022, 18:575-587
Published Date: 24 July 2022
Pulmonary Embolism After in vitro Fertilization and Cesarean Section: Two Case Reports and Brief Review of the Literature
Wu YY, Shan TT, Pan XT
International Journal of Women's Health 2022, 14:1489-1497
Published Date: 25 October 2022
Chemical versus Mechanical and Chemical Venous Thromboembolism Prophylaxis in Neurocritically Ill Patients: A Cohort Study
Alshaya AI, Alyahya H, Alzoman R, Faden R, Alshaya OA, Al Sulaiman K, Alanazi F, Aldekhyl S
Clinical Pharmacology: Advances and Applications 2023, 15:1-8
Published Date: 7 January 2023
Thromboprophylaxis in Patients Admitted to the Surgical Ward: Clinical Audit
Abdalla YA, Kamil AM, Mohamed SAA, Mohamed AHA, Khalifa E, Mohamed MHA, Abdelgadir EEA, Dabora M, Awoda MSEME
Vascular Health and Risk Management 2023, 19:651-656
Published Date: 22 September 2023
Therapeutic Challenge in a Case of Extensive Pulmonary Embolism with Concomitant Intracranial Haemorrhage: When Less is Really More
Tan TL, Yeoh AYZ, Munusamy RA
International Medical Case Reports Journal 2026, 19:585109
Published Date: 24 February 2026