")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Availability of Laboratory Diagnosis of Gonorrhoea and Its Meaning in Case Reporting in Shandong Province, China
Received 10 January 2023
Accepted for publication 27 March 2023
Published 31 March 2023 Volume 2023:16 Pages 783—791
DOI https://doi.org/10.2147/CCID.S402676
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Anne-Claire Fougerousse
Xinlong Chen,1 Yanling Gan,2 Dianchang Liu2
1Department of Dermatology, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, 610072, People’s Republic of China; 2Department of STI and Leprosy Prevention and Control, Shandong Provincial Hospital for Skin Diseases & Shandong Provincial Institute of Dermatology and Venereology, Shandong First Medical University & Shandong Academy of Medical Sciences, Jinan, Shandong, 250022, People’s Republic of China
Correspondence: Dianchang Liu, Tel +86 531-87298850, Email [email protected]
Background: Gonorrhea, caused by the bacterium Neisseria gonorrhoeae (NG), is a major public health concern worldwide.
Aim of the Study: The aim of this study is to understand the availability of laboratory diagnosis of gonorrhoea in Shandong province and its meaning in case reporting.
Methods: Two surveys were conducted among hospitals providing clinical services for sexually transmitted infection (STI) in Shandong Province in 2012 and 2018. The availability of laboratory tests for NG and distribution of reported gonorrhea cases were compared among different hospitals provided clinical services for STI in Shandong province. Descriptive analysis and Chi-square were used for statistical analysis.
Results: Smear, culture and PCR tests for NG were used among 301(74.69%), 123(30.52%), 43(10.67%) hospitals in 2012 and 356(74.48%), 176(36.82%) and 73(15.27%) hospitals in 2018, respectively. Significant differences were observed in the availability of smear among hospitals at different levels (X2=12.159, p=0.000) and with different affiliations (X2=4.551, p=0.033) in 2018. Significant differences were observed in the availability of culture and PCR tests among hospitals at different levels both in 2012 (X2=34.532, p=0.000; X2=7.380, p=0.007) and 2018 (X2=49.820, p=0.000; X2=21.658, p=0.000). The availability of culture and PCR tests for NG among hospitals in 2018 was higher than that in 2012 (X2=3.870, p=0.049; X2=4.050, p=0.044). More hospitals reported gonorrhea cases in 2018 than in 2012 (X2=6.768, p=0.009). A significant difference was observed in distribution of case reporting among hospitals at different levels in 2018 (X2=6.975, p=0.008) and among different types of hospital both in 2012 (X2=52.362, p=0.000) and 2018 (X2=74.478, p=0.000).
Conclusion: Poor availability of NG laboratory tests affects case reporting, and which is a crucial reason leading to underreporting of gonorrhea cases in Shandong province.
Keywords: gonorrhea, availability, laboratory tests, underreporting
Introduction
Gonorrhea, caused by the bacterium Neisseria gonorrhoeae (NG), is a major public health concern worldwide. It was estimated that 82 million new case were infected by NG worldwide in 2020.1 The 2016 global prevalence estimates in women were: gonorrhoea 0.9% and syphilis 0.5%.2 The reported incidence of gonorrhea was higher than that of syphilis.
In China, syphilis and gonorrhea belong to the second-class infectious diseases, according to the Infectious Disease Prevention Act of China.3 The incidence rates of gonorrhea were on the rise from 2011 to 2021. The annual percentage change was 2.56% for gonorrhea.4
A study found that the positive rate of syphilis and N. gonorrhoeae among women of reproductive age was 0.73% and 0.06%.5 Gonorrhea is still among the top five notifiable infectious diseases in China. The reported incidence of gonorrhea was 9.59 cases per 100,000 residents in 2018.6 Gonorrhea is still one of the major infectious diseases that should be concerned. In the absence of treatment, gonorrhea can lead to pelvic inflammatory disease, infertility and an increased risk of transmission of human immunodeficiency virus.7 Studies indicate that NG is rapidly becoming untreatable with decreased ceftriaxone and azithromycin susceptibility.8–10 Dual therapy with ceftriaxone and azithromycin is currently recommended for the treatment of gonorrhea in Thailand.11 In addition, tolerance to ceftriaxone was found in clinical samples.12 However, if the surveillance data cannot interpret the current situation of gonorrhea epidemic, misleading may be inevitable in policy making for gonorrhea prevention and control. Many factors may affect the integrity and accuracy of surveillance data. Gonorrhea may be asymptomatic in 40% of men and more than half of women.13 A survey found that 81% to 98% of individuals with chlamydia and gonorrhea infections would be undiagnosed and untreated using only symptomology.14 Case reporting of gonorrhea is largely based on laboratory diagnosis in China. Availability of laboratory tests may play a vital role in gonorrhea surveillance. In addition, the reported incidence of gonorrhea is closely related to screening programmes implemented and the development of laboratory tests techniques in medical institutions. We all know that the practice of laboratory tests for NG in hospitals are associated with case reporting, but little information on how and to what extent it effects case reporting is available in China. In addition, the spread of antimicrobial-resistant NG has led to an increasing need to improve the availability of laboratory tests in hospitals. To understand the availability of laboratory tests for NG and make out its meaning in gonorrhea case reporting, we conducted two surveys among hospitals providing STI clinical service in Shandong province in 2012 and 2018, respectively.
Materials and Methods
Study Site
The study was conducted in Shandong, the third largest economically developed province in China. A total of 1549 and 2579 hospitals had been registered by 2012 and 2018, respectively, serving for about one hundred million people in the province.15,16
Study Objects
Hospitals providing clinical services for sexually transmitted infection (STI) in Shandong province were included in this study. All hospitals with case reporting of STI in Shandong province in the past year were defined as that provided clinical service for STI.
Primary hospitals (Class I) are primary health care institutions that directly provide the community with comprehensive services of medical treatment, prevention, rehabilitation and health care. Secondary hospitals (Class II) are regional hospitals that provide medical and health services across several communities and are technical centers for regional medical prevention. Tertiary hospitals (Class III) are hospitals that provide medical and health services across regions, provinces, cities and the whole country, and are medical and preventive technology centers with comprehensive medical treatment, teaching and scientific research capabilities.
Specialized dermatological hospitals is responsible for the prevention and control of sexually transmitted diseases and skin diseases. Maternal and child health hospitals refer to hospitals that provide diagnosis and treatment for women and children. General western medicine hospitals and Chinese medicine hospitals are the most important component of delivering health care to people, but the former is dominated by western medicine, while the latter is dominated by traditional Chinese medicine. Other specialized hospitals include orthopedic specialist hospitals, ophthalmic specialist hospitals, stomatological specialist hospitals and so on.
Public hospitals are state-owned and collective-run hospitals (including government-run hospitals). Private hospitals are non-governmental hospitals.
Data Collection
We conducted two surveys in 2012 and 2018, respectively. A structured questionnaire was used in data collection. Basic information on the hospitals by levels, types, and affiliation and the types of laboratory tests for NG provided in the hospitals was collected. Trained health staff from the Chinese Centers for Diseases Control and Prevention at prefecture-level and county-level visited each hospital in their respective jurisdictions and filled in the questionnaires. The records of reported gonorrhea cases in Shandong both in 2012 and 2018 were downloaded from the China Information System for Disease Control and Prevention (CISDCP). Smear refer to Gram Stain, PCR to NAATs, and culture to agar dilution.
Data Analysis
Valid data collected were entered into Microsoft Excel for Windows (2012) and analyzed in SPSS (version 22). The percentages of hospitals providing each laboratory tests for NG and reported gonorrhea cases were analyzed and compared by levels, types, and affiliation. Descriptive analysis and Chi-square were used for statistical analysis. p values<0.05 was considered statistically significant.
Results
General Information
Among 1549 and 2579 hospitals registered in Shandong province in 2012 and 2018, clinical service for STI were available in 410 (26.47%) and 496 (19.23%) hospitals, and a total of 403 and 478 valid questionnaires were collected in the two surveys, respectively. The coverage of different hospitals provided clinical services for STI was low and had been deteriorated from 2012 to 2018, excepting among specialized dermatological hospitals and maternal and child health hospitals. (Table 1)
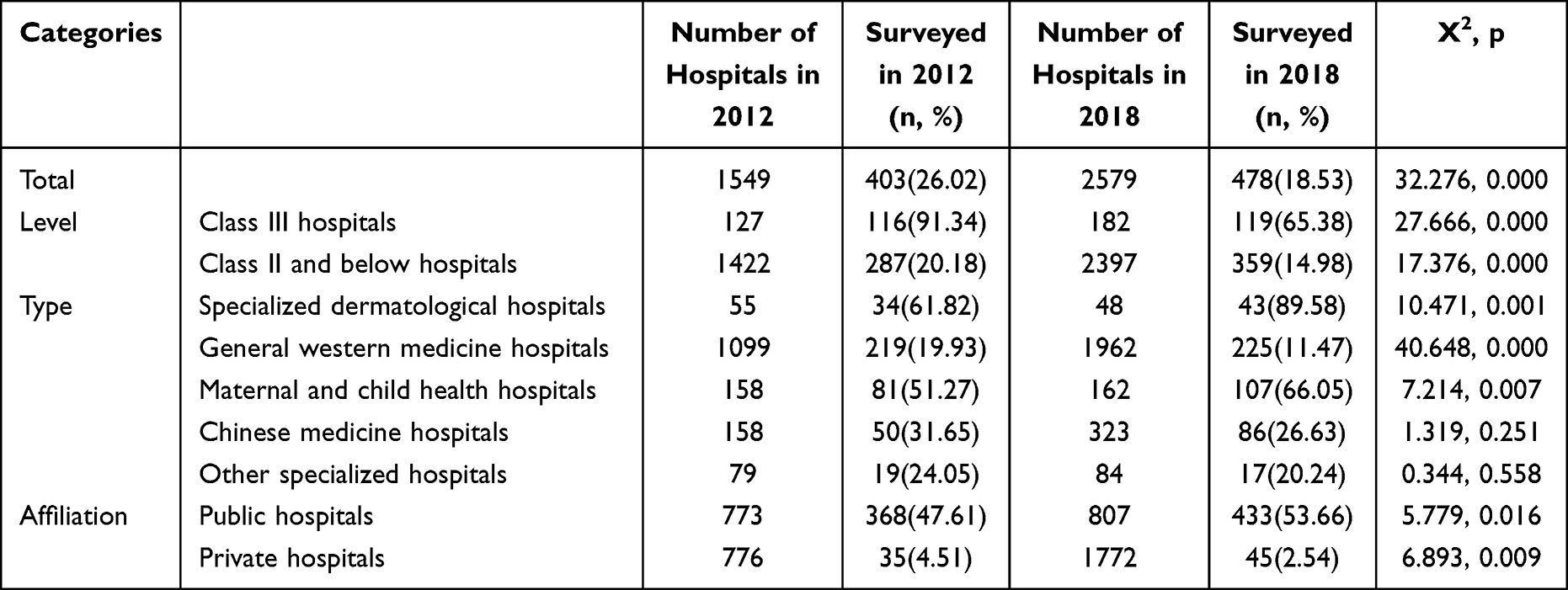 |
Table 1 Percentages of Surveyed Hospitals in Shandong |
Availability of Laboratory Tests for NG in Hospitals of Shandong Province
Smear, culture and PCR tests for NG were used among 301 (74.69%), 123 (30.52%), 43 (10.67%) hospitals in 2012 and 356 (74.48%), 176 (36.82%) and 73 (15.27%) hospitals in 2018, respectively.
Significant differences were observed in the availability of smear at different levels in 2018 (X2=12.159, p=0.000), but not in 2012. Significant differences were observed in the availability of culture and PCR tests at different levels both in 2012 (X2=34.532, p=0.000; X2=7.380, p=0.007) and 2018 (X2=49.820, p=0.000; X2=21.658, p=0.000). They were more available in class III hospitals than that in class II and below hospitals. Significant differences were observed in the availability of smear, culture and PCR tests among different types of hospital both in 2012 (X2=35.593, p=0.000; X2=27.574, p=0.000; X2=9.666, p=0.046) and 2018 (X2=92.132, p=0.000; X2=37.660, p=0.000; X2=13.310, p=0.016). Smear and culture tests were more available among specialized dermatological hospitals and general western medicine hospitals than that among other kinds of hospitals in 2012 (X2=32.450, p=0.000; X2=23.759, p=0.000) and 2018 (X2=76.587, p=0.000; X2=31.391, p=0.000). PCR test was more available among general western medicine hospitals than that among other kinds of hospitals in 2012 (X2=6.113, p=0.013) and 2018 (X2=10.365, p=0.001). Significant differences were observed in the availability of culture test among hospitals with different affiliations in 2018 (X2=4.551, p=0.033), but not in 2012. Culture test was more available in public hospitals than that in private hospitals in 2018. No significant differences were observed in the availability of smear and PCR tests among hospitals with different affiliations both in 2012 and 2018.
No significant change in the availability of smear test for NG was observed among hospitals from 2012 to 2018 (X2=0.005, p=0.942). The availability of culture test for NG among hospitals in 2018 was higher than that in 2012 (36.82% vs 30.52%, X2=3.870, p=0.049). It was significantly improved from 2012 to 2018 among general western medicine hospitals (36.99% vs 47.11%, X2=4.667, p=0.031) and public hospitals (30.71% vs 38.34%, X2=5.103, p=0.024). The availability of PCR test for NG among hospitals in 2018 was higher than that in 2012 (15.27% vs 10.67%, X2=4.050, p=0.044). It was significantly improved from 2012 to 2018 among class III hospitals (17.24% vs 28.57%, X2=4.261, p=0.039) and public hospitals (10.60% vs 15.70%, X2=4.482, p=0.034). (Table 2)
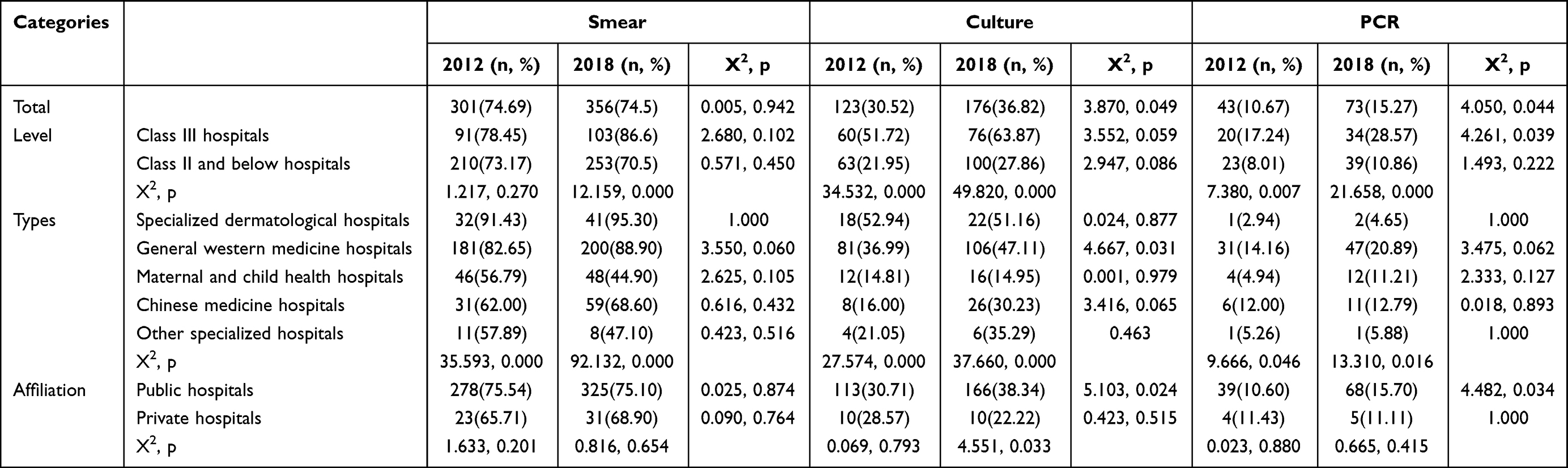 |
Table 2 Availability of NG Laboratory Tests in Hospitals of Shandong Province |
Distribution and Change of Hospitals with Gonorrhea Laboratory Tests and Cases Reporting in Shandong Province
A total of 119 (29.53%) and 188 (39.33%) hospitals reported gonorrhea cases in 2012 and 2018, respectively. A significant difference was observed in distribution of case reporting among hospitals with different level in 2018 (X2=6.975, p=0.008), but not in 2012 (X2=3.491, p=0.062). More class III hospitals reported gonorrhea cases than class II and below hospitals in 2018. A significant difference was observed in distribution of case reporting among different type of hospitals both in 2012 (X2=52.362, p=0.000) and 2018 (X2=74.478, p=0.000). More specialized dermatological hospitals reported gonorrhea cases than other hospitals in 2012 (X2=18.543, p=0.000). More specialized dermatological hospitals and general western medicine hospitals reported gonorrhea cases than other hospitals in 2018 (X2=58.654, p=0.000). No significant differences were observed in distribution of case reporting among hospitals with different affiliations both in 2012 (X2=2.826, p=0.093) and 2018 (X2=3.339, p=0.068).
More hospitals reported gonorrhea cases in 2018 than in 2012 (X2=6.768, p=0.009). Specifically, more class III hospitals, class II and below hospitals, general western medicine hospitals and public hospital reported gonorrhea cases in 2018 than in 2012 (X2=4.286, p=0.038; X2=6.086, p=0.014; X2=15.520, p=0.000; X2=8.523, p=0.004). (Table 3)
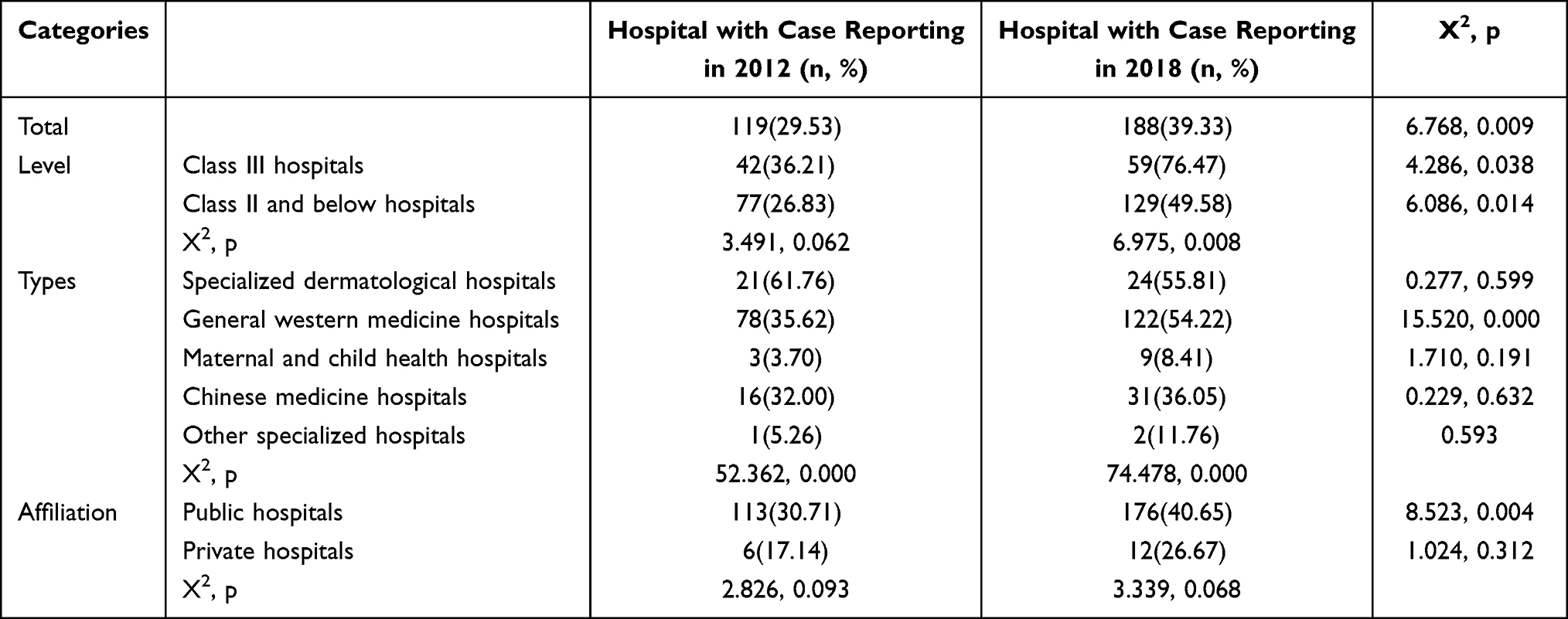 |
Table 3 Distribution and Change of Hospitals with Gonorrhea Cases Reporting in Shandong Province |
Among hospitals reported cases of gonorrhea in 2018, 95 reported female gonorrhea cases. More hospitals with culture or PCR tests available reported female cases of gonorrhea than those without (67.37% vs 32.63%; X2=7.733, p=0.005).
Discussion
In this study, we evaluated the capacity of STI clinical service in Shandong province. We found that the number of hospitals providing STI clinical service increased but the proportion decreased in the past six years. The total number of registered hospitals largely increased in the past six year, especially the number of private hospitals increased, but the proportion of providing STI clinical service was decreased. Although the proportion of specialized dermatological hospitals STI clinical service increased, their number was decreased. Public general western medicine hospitals are still playing a core role in STI clinical service in Shandong province. The proportion of hospitals providing STI clinical service was still as low as 18.53% in 2018, indicating that much room needs to be improved in availability of STI clinical service in Shandong province.
Among hospitals providing STI clinical service, the availability of laboratory tests for NG was low. Among hospitals surveyed in 2018, more than 1/4 could not provide smear test for NG, more than 3/5 could not provide culture test, and more than 5/6 could not provide PCR test. In 1990s, the reported incidence of gonorrhea was much higher than syphilis and kept increasing to its peak in 1999, then went down. A new criterion for diagnosis of gonorrhea implemented in 2007, defining gonorrhea case based on pathogenic test instead of clinical examination, and the role of laboratory tests has been emphasized since then.
Although most hospitals could provide smear test, female gonorrhea cases could not be diagnosed by smear according to the criterion for diagnosis of gonorrhea issued by the National Health Commission of China. Diagnosis of female gonorrhea cases relies on culture or PCR tests of NG. Most female cases may be underdiagnosed and underreported due to low availability of culture and PCR tests. It is recommended that all sexually active women aged 24 years or younger and older women at high risk of gonorrhea and chlamydia infection should be screened with PCR test.17 Maternal and child health hospitals should play an important role in NG screening among the female. But, the laboratory tests for NG were less available in maternal and child health hospitals than specialized dermatological hospitals and general western medicine hospitals, and no improvement was achieved in the past six years in Shandong province. Although smear test is less sensitive to women, it is still the main method for NG screening even in maternal and child health hospitals in Shandong province. More gonorrhea cases were reported in male than female as well in some countries with high availability of PCR test for NG.18,19 This would lead to an underreporting of gonorrhoea among female in Shandong province.
We confirmed that the availability of laboratory tests of NG is related to case reporting of gonorrhea. The distribution of hospitals with gonorrhea case reporting was consistent with that of hospitals where laboratory tests were available. The availability of culture and PCR tests has been improved in Class III hospitals, general western medicine hospitals and public hospitals from 2012 to 2018. Accordingly, the proportion of hospitals with case reporting increased significantly in those hospitals. Earlier study also found that the increasing number of gonorrhea cases was related to the PCR testing rate.20 Diagnosis of female gonorrhea cases relies on culture or PCR tests of NG. Insufficient of laboratory tests may lead to underdiagnosed and underreported of gonorrhea, especially for female cases, in Shandong province. In addition, more than 74% of surveyed hospitals could provide smear test for NG at least both in 2012 and 2018, however, less than 40% reported cases of gonorrhea. It indicates that availability of laboratory tests is not the exclusive factor related to case reporting. We found by interview with doctors that another factor leading to under diagnosis and under reporting of gonorrhea may be the low awareness of gonorrhea screening by clinical doctors. Many infections of NG have no symptoms and most cases may never be diagnosed without screening. In Canada, midwives, family physicians and generalist obstetricians tested 93.8%, 91.4% and 88.5% of their patients respectively.21 Low availability of NG screening may lead to underdiagnosis and underreporting of gonorrhea in China.
Many factors may affect availability and use of laboratory tests of NG. Smear test is rapid, convenient and inexpensive. The sensitivity and specificity of smear were high for symptomatic males, but low for female.22 The culture method has high sensitivity and specificity. But, it needs higher requirements with meticulous sample collection, transport and nutrient medium than other methods.23,24 PCR test offers very high sensitivity and specificity of detection, which is now the standard of diagnoses across the US and other countries.22 For rectal gonorrhea and pharyngeal gonorrhea, testing positive was more obtained by PCR than culture.25 However, higher requirements in equipment and technicians than smear and culture may restrict its wide use. From 2013 to 2015, there was an increase of some laboratories offering NG PCR test in US.26 In contrast, the availability of PCR test was still as low as 15% among hospitals providing STI clinical service in Shandong province in 2018. In a survey of 57 countries that responded, only 14 countries reported having antenatal CT or NG screening policies.27 National level policies to support routine screening for CT or NG infection to prevent adverse pregnancy and newborn outcomes are uncommon.
Some efforts are needed to improve the screening and reporting of gonorrhea in Shandong. Firstly, increase accessibility of STI clinical services by integrating the prevention and management of STI into the broader agendas of HIV, sexual and reproductive health, and other key platforms. Secondly, accelerate accessibility to innovations through the development of point-of-care (POC) testing. The overall rate of agreement and negative percentage agreement with POC were 97.8% and 100% respectively, for NG compared with NAAT methods.28 WHO also advocated the development of POC testing as a critical step within STI cascade and continuum of services. POC testing for urogenital infections might improve case-finding and infection management and is feasible in resource-poor settings.29 Integration of POC testing can mitigate the transmission and burden of STI.30 Thirdly, strengthen training of clinicians and scale up STI interventions. Lack of training for clinicians was one of the important barriers for performing STI testing.31 The testing rate increased from 7.90% to 17.86% among university campus through education.32 Finally, strengthen quality assurance of NG laboratory tests. According to a survey, only 5% of the laboratories met or surpassed the lowest quality standards defined by the WHO/AFRO-derived laboratory strengthening tool in Kampala.33
There are some limitations in the study. First, the investigation was conducted in a province of China, and generalization of the results should be cautious. Second, many other factors may affect reporting of gonorrhea incidence besides the availability of laboratory tests for NG. Third, data on gonococcal resistance were not available.
Conclusions
In conclusion, poor availability of NG laboratory tests affects case reporting and is a crucial reason leading to underreporting of gonorrhea cases in Shandong province. More efforts are needed to improve the availability of NG laboratory tests in order to effectively control of gonorrhea.
Data Sharing Statement
The data used and analyzed are available upon reasonable request by emailing [email protected].
Ethics Approval and Consent to Participate
We got an ethics approval statement from the institutional review board at the Shandong Provincial Institute of Dermatology and Venereology (20190716-KYKT-002). Meanwhile, the objects of this study were hospitals rather than human being or animals. We think that it is not applicable to provide a statement on ethics approval and consent to participate.
Acknowledgments
The authors thank the Centers for Diseases Control and Prevention at different level enrolled in this study in Shandong province. This manuscript has been released as a pre-print at Infectious Diseases.34
Funding
This work was supported by the Shandong Provincial Key R&D Plan (2018GSF118062). The funding body was not involved in the collection, analysis and interpretation of data, nor in the writing of manuscripts.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Van Gerwen OT, Muzny CA, Marrazzo JM. Sexually transmitted infections and female reproductive health. Nat Microbiol. 2022;7(8):1116–1126. doi:10.1038/s41564-022-01177-x
2. Rowley J, Vander Hoorn S, Korenromp E, et al. Chlamydia, gonorrhoea, trichomoniasis and syphilis: global prevalence and incidence estimates, 2016. Bull World Health Organ. 2019;97(8):548–562P. doi:10.2471/BLT.18.228486
3. National People’s Congress. The infectious disease prevention act (The 17th Presidential Decree of the People’s Republic of China). Available from: http://www.gov.cn/gongbao/content/2004/content_62975.
4. Zhu Z, Zhu X, Zhan Y, Gu L, Chen L, Li X. Development and comparison of predictive models for sexually transmitted diseases-AIDS, gonorrhea, and syphilis in China, 2011–2021. Front Public Health. 2022;10:966813. doi:10.3389/fpubh.2022.966813
5. Liu J, Zeng M, Yang L, et al. Prevalence of reproductive tract infections among women preparing to conceive in Chongqing, China: trends and risk factors. Reprod Health. 2022;19(1):197. doi:10.1186/s12978-022-01502-x
6. The China Disease Prevention and Control Center. Overview of the epidemic situation of statutory infectious diseases in China in 2018. Available from: http://www.nhc.gov.cn/jkj/s3578/201904/050427ff32704a5db64f4ae1f6d57c6c.shtml.
7. Marks M, Harding-Esch E. Antimicrobial resistance in gonorrhea: diagnostics to the rescue. Clin Infect Dis. 2021;73(2):304–305. doi:10.1093/cid/ciaa591
8. Somsri M, Oransathid W, Vesely B, et al. Antimicrobial susceptibility of Neisseria gonorrhoeae in adult patients seeking care at military hospitals in Thailand from 2014 to 2020. Mil Med. 2022:usab549. doi:10.1093/milmed/usab549
9. Golparian D, Kittiyaowamarn R, Paopang P, et al. Genomic surveillance and antimicrobial resistance in Neisseria gonorrhoeae isolates in Bangkok, Thailand in 2018. J Antimicrob Chemother. 2022;77(8):2171–2182. doi:10.1093/jac/dkac158
10. Lin EY, Adamson PC, Ha SM, Klausner JD, Andam CP. Reliability of genetic alterations in predicting ceftriaxone resistance in Neisseria gonorrhoeae globally. Microbiol Spectr. 2022;10(2):e0206521. doi:10.1128/spectrum.02065-21
11. Nokchan N, Wongsurawat T, Jenjaroenpun P, et al. Whole-genome sequence analysis of high-level penicillin-resistant strains and antimicrobial susceptibility of Neisseria gonorrhoeae clinical isolates from Thailand. PLoS One. 2022;17(7):e0271657. doi:10.1371/journal.pone.0271657
12. Balduck M, Laumen JGE, Abdellati S, et al. Tolerance to ceftriaxone in Neisseria gonorrhoeae: rapid Induction in WHO P reference strain and detection in clinical isolates. Antibiotics. 2022;11(11):1480. doi:10.3390/antibiotics11111480
13. Handsfield HH, Lipman TO, Harnisch JP, et al. Asymptomatic gonorrhea in men. Diagnosis, natural course, prevalence and significance. N Engl J Med. 1974;290(3):117–123. doi:10.1056/NEJM197401172900301
14. Tobin L, Guerra L, Ahouanvoeke L, et al. Is it time to use nucleic acid amplification tests for identification of persons with sexually transmitted infections? Evidence from seroprevalence and behavioral epidemiology risk surveys in men with chlamydia and gonorrhea. Pan Afr Med J. 2020;36:299. doi:10.11604/pamj.2020.36.299.20777
15. Health and Family Planning Commission of Shandong Province. 2012 Shandong province health and family planning development statistics bulletin. Available from: http://wsjkw.shandong.gov.cn/jksd/tjsj_763/zytjbg/201305/t20130530_591620.html.
16. Health and Family Planning Commission of Shandong Province. 2018 Shandong province health and family planning development statistics bulletin. Available from: http://wsjkw.shandong.gov.cn/jksd/tjsj_763/zytjbg/201908/t20190801_2335002.html.
17. Audrey T, Adam SC. Screening for gonorrhea, chlamydia, and hepatitis B. JAMA. 2016;315(12):1278–1279. doi:10.1001/jama.2016.0223
18. Choudhri Y, Miller JP, Sandhu J, et al. Gonorrhea in Canada, 2010–2015. Can Commun Dis Rep. 2018;44(2):37–42. doi:10.14745/ccdr.v44i02a01
19. Centers for Disease Control and Prevention. Sexually transmitted disease surveillance 2017. Available from: https://www.cdc.gov/std/stats17/Gonorrhea.htm.
20. Honglin W, Yumao C, Lan L. Factors associated with the raising prevalence of gonorrhea in Shenzhen in 2016. Inter J Epidemiol Infect Dis. 2019;46(4):301–305. doi:10.3760/cma.j.issn.1673-4149.2019.04.011
21. Vainder M, Kives S, Yudin MH. Screening for gonorrhea and chlamydia in pregnancy: room for improvement. J Obstet Gynaecol Can. 2019;41(9):1289–1294. doi:10.1016/j.jogc.2019.02.006
22. Centers for Disease Control and Prevention. Recommendations for the laboratory-based detection of chlamydia trachomatis and Neisseria gonorrhoeae-2014. MMWR Recomm Rep. 2014;63(2):1–19. doi:10.1186/1745-6673-9-10
23. Boiko I, Golparian D, Krynytska I, et al. High prevalence of Chlamydia trachomatis, Neisseria gonorrhoeae and particularly Trichomonas vaginalis diagnosed using US FDA-approved Aptima molecular tests and evaluation of conventional routine diagnostic tests in Ternopil, Ukraine. APMIS. 2019;127(9):627–634. doi:10.1111/apm.12975
24. Visser M, van Westreenen M, van Bergen J, van Benthem BHB. Low gonorrhoea antimicrobial resistance and culture positivity rates in general practice: a pilot study. Sex Transm Infect. 2020;96(3):220–222. doi:10.1136/sextrans-2019-054006
25. Cornelisse VJ, Chow EP, Huffam S, et al. Increased detection of pharyngeal and rectal gonorrhea in men who have sex with men after transition from culture to nucleic acid amplification testing. Sex Transm Dis. 2017;44(2):114–117. doi:10.1097/OLQ.0000000000000553
26. Davis A, Gaynor A. A comparison of US clinical laboratory chlamydia and gonorrhea testing practices before and after the 2014 centers for disease control and prevention testing recommendations. Sex Transm Dis. 2021;48(6):e73–e76. doi:10.1097/OLQ.0000000000001299
27. Medline A, Joseph Davey D, Klausner JD. Lost opportunity to save newborn lives: variable national antenatal screening policies for Neisseria gonorrhoeae and Chlamydia trachomatis. Int J STD AIDS. 2017;28(7):660–666. doi:10.1177/0956462416660483
28. Badman SG, Willie B, Narokobi R, et al. A diagnostic evaluation of a molecular assay used for testing and treating anorectal chlamydia and gonorrhoea infections at the point-of-care in Papua New Guinea. Clin Microbiol Infect. 2019;25(5):623–627. doi:10.1016/j.cmi.2018.08.001
29. Verwijs MC, Agaba SK, Sumanyi JC, et al. Targeted point-of-care testing compared with syndromic management of urogenital infections in women (WISH): a cross-sectional screening and diagnostic accuracy study. Lancet Infect Dis. 2019;6:658–669. doi:10.1016/S1473-3099(18)30724-2
30. Toskin I, Govender V, Blondeel K, et al. Call to action for health systems integration of point-of-care testing to mitigate the transmission and burden of sexually transmitted infections. Sex Transm Infect. 2020;96(1):1–6. doi:10.1136/sextrans-2019-054358
31. Ong JJ, Peng M, Zhu S, et al. Opportunities and barriers to STI testing in community health centres in China: a nationwide survey. Sex Transm Infect. 2017;93(8):566–571. doi:10.1136/sextrans-2017-053196
32. Myers A, McCaskill SP, VanRavenstein K. Improving STD screening rates on a university campus. J Community Health. 2017;42(6):1247–1254. doi:10.1007/s10900-017-0377-9
33. Elbireer AM, Jackson JB, Sendagire H, et al. The good, the bad, and the unknown: quality of clinical laboratories in Kampala, Uganda. PLoS One. 2013;8(5):e64661. doi:10.1007/s10900-017-0377-9
34. Chen X, Gan Y, Dianchang L. Availability of laboratory diagnosis of gonorrhoea and its meaning in case reporting in Shandong province, China. Res Square. 2020. doi:10.21203/rs.3.rs-35168/v1
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.