Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Automated Oxygen Delivery in Home Setting for Patients with COPD on Long-Term Oxygen Therapy – A Randomized Crossover Feasibility Trial
Authors Kofod LM, Hansen EF ![]() , Kristensen MT
, Kristensen MT ![]() , Brocki BC
, Brocki BC ![]() , Westerdahl E
, Westerdahl E ![]()
Received 12 June 2025
Accepted for publication 28 October 2025
Published 14 November 2025 Volume 2025:20 Pages 3697—3712
DOI https://doi.org/10.2147/COPD.S546748
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jill Ohar
Linette Marie Kofod,1,2 Ejvind Frausing Hansen,3 Morten Tange Kristensen,4,5 Barbara Cristina Brocki,6 Elisabeth Westerdahl7
1PMR-C, Department of Physio- and Occupational Therapy, Copenhagen University Hospital, Hvidovre, Denmark; 2School of Medical Sciences, Faculty of Medicine and Health, Örebro University, Örebro, Sweden; 3Department of Pulmonology, Copenhagen University Hospital, Hvidovre, Denmark; 4Department of Physical and Occupational Therapy, Copenhagen University Hospital, Bispebjerg-Frederiksberg, Copenhagen, Denmark; 5Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark; 6Department of Physiotherapy and Occupational Therapy, Aalborg University Hospital, Aalborg, Denmark; 7University Health Care Research Center, Faculty of Medicine and Health, Örebro University, Örebro, Sweden
Correspondence: Linette Marie Kofod, Department of Physio- and Occupational Therapy, Copenhagen University Hospital- Hvidovre, Kettegaard Allé 30, Hvidovre, 2650, Denmark, Tel +45 38621619, Email [email protected]
Rationale: Patients with COPD on long-term oxygen therapy (LTOT) have an unmet need for oxygen adjustments during sleep, rest, and activity, documented by continuous monitoring of oxygen saturation (SpO2). While emerging technology enables automated adjustments, its feasibility in home settings remains uncertain. This randomized crossover trial evaluated the feasibility and preliminary effects of continuous automated oxygen titration at home.
Methods: The intervention period involved four days of automated oxygen titration targeting a SpO2 of 90– 94% using a Bluetooth-connected electronic device and wrist pulse oximeter, forming a closed-loop system. Oxygen flow (0.9– 6.8 L/min) was continuously adjusted based on SpO2. During the control period, patients received their usual fixed dose oxygen. Feasibility was defined as time with automated titration, time within target SpO2 and patient acceptance. Additionally, health status was measured using the Clinical COPD Questionnaire (CCQ, minimal important difference 0.4).
Results: Twelve patients (8 men, mean (SD) age 72.9 (5.5) years) on LTOT with an oxygen dose of 2.0 (0.8) L/min were included. Each patient provided more than 217,000 paired SpO2 and oxygen flow data points. Oxygen flow was automatically adjusted for a median of 77 h (IQR 68.0– 84.3), covering 83% of the time. Time within target SpO2 increased from 52% (42– 63) to 86% (75– 90) during the intervention. All patients used the full available flow range. The CCQ score improved by 0.74 (0.47) points; p < 0.001.
Conclusion: Automated oxygen titration is feasible in the home setting, achieving more time with normoxia, but it required a wide flow range and continuous SpO2 monitoring. The patients reported a clinically relevant reductions in COPD symptoms measured with CCQ. The clinical importance of controlling SpO2 needs to be examined in a larger study.
Plain Language Summary: Why was the study done?
Patients with COPD who use home oxygen often need different amounts during rest, activity, or sleep. Standard oxygen therapy provides a fixed amount, which may not meet these changing needs. This study tested whether oxygen could be adjusted automatically at home to better match each patient’s needs.
What did the researchers do and find?
Twelve patients on home oxygen used a new system that adjusted the oxygen flow automatically based on their blood oxygen levels. The system used a wrist-worn monitor and aimed to keep oxygen levels within a target range (90– 94%).
The system worked well, automatically adjusting oxygen for the largest part of the time but using a wide range of oxygen flow. Time spent in the target range increased from 52% with usual therapy to 86% with the automated system. The patients reported improvements in both breathlessness and mental well-being.
What do these results mean?
Automatic oxygen adjustment at home is possible and helps patients spend more time with adequate oxygen levels. It needs continuous monitoring and flexible oxygen settings. This approach could improve comfort and quality of life for patients using home oxygen.
Keywords: automated oxygen titration, long-term oxygen therapy, closed-loop, activities of daily living, oxygen saturation, technology
Introduction
Oxygen is essential for human life. Regrettably, some patients with advanced COPD develop a reduced ability to deliver sufficient oxygen to the blood, resulting in chronic respiratory failure with the constant need of oxygen supplementation.
In acute settings, it is recommended to maintain target oxygen saturation using conservative oxygen doses in patients with acute hypoxemic respiratory failure, as this approach is associated with reduced mortality.1–3 Several studies found that electronic, closed-loop devices, which automatically adjusts oxygen in response to the saturation, were more accurate in keeping the recommended saturation compared to manual adjustments.4–8
In contrast, our understanding is limited when it comes to maintaining target saturation during daily living in the home setting. Home oxygen is prescribed based on arterial blood gas analysis to achieve a partial pressure of oxygen (PaO2) >8.0 kPa, corresponding to a peripheral oxygen saturation (SpO2) of 90% at rest.9,10 Although patients with COPD on long-term oxygen therapy (LTOT) use this prescribed fixed oxygen dose, continuous monitoring of oxygen saturation has revealed an unmet need for oxygen adjustments, depending on whether the patients are sleeping, sitting, or engaging in daily activities.11,12 These fluctuating oxygen needs lead to episodes of desaturation and hypoxemia.12–16 Clinical benefits of minimizing these episodes of hypoxemia are particularly evident during walking tests.17–19 Optimizing patients’ oxygen saturation by using the electronic devices for automated oxygen titration increased the patients’ walking capacity and alleviated dyspnea.17–19 Furthermore, improved oxygenation enhanced the patients' ability to perform activity of daily living (ADL) and reduced their perceived breathing effort during an ADL-test.20 These results suggest, that increasing time spent with normoxia may benefit patients in daily life.
Automated oxygen titration technology has entered the home setting, enabling a closed-loop system to adjust oxygen delivery in real time based on oxygen saturation measurements. It requires the patients to wear a pulse oximeter that communicates with the oxygen delivery system, which then dynamically adapts the oxygen flow to each situation. When SpO2 falls below the lower threshold, the system increases the oxygen flow, and when it rises above the upper threshold, the flow is reduced. This process is repeated continuously, creating a feedback loop between monitoring and oxygen delivery, without manual adjustments. Around-the-clock monitoring of oxygen saturation and consequently continuous adjustments of the oxygen flow in the home setting represent a new approach, and it remains unclear how, or even if, such oxygen titration could be effectively managed. The patients may face practical or technical challenges, and their acceptance of automated titration is unknown. Therefore, before conducting a larger trial, it is necessary to determine whether the intervention can be safely and reliably applied in the home setting. The aim of this randomized crossover study was to evaluate the feasibility of automated oxygen titration as response to the saturation during daily living for four days in the home of patients with COPD on LTOT. Feasibility was defined as successful time during which the patients’ oxygen was automatically titrated, the patients’ willingness toward the intervention, and clinically relevance.
Methods
Study Design
This randomized crossover feasibility trial was conducted in the homes of 12 patients with COPD on LTOT. The patients were recruited from two departments of pulmonology at Copenhagen University Hospital, Hvidovre and Copenhagen University Hospital, Bispebjerg-Frederiksberg, Denmark, from January to December 2023 in connection with a scheduled study visit.20
The study complies with the Declaration of Helsinki and was approved by The Committees on Health Research Ethics in the Capital Region of Denmark (H-22032988) and the Danish Data Protection Agency j.nr. P-2022-625. The study was registered at ClinicalTrials.gov (NCT05556187), and the reporting followed the CONSORT statement for randomized pilot and feasibility trials.
Participants
Inclusion criteria included patients with COPD and chronic respiratory failure with resting hypoxemia (PaO2 ≤7.3 kPa), who were receiving LTOT according to the international criteria for home oxygen therapy,9 had the ability to walk independently (with or without a walking aid), and were cognitively able to participate. Exclusion criteria were an exacerbation in COPD treated with either antibiotics or prednisolone within the preceding three weeks or comorbidities known to impact physical functioning. Additionally, before randomization, each patient underwent two venous blood gas tests: the first with their usual oxygen dose and the second after 20 minutes of 8 L/min of oxygen. Venous blood gases (instead of arterial blood gases) were used to minimize discomfort to the patients.21 The blood samples were analyzed for pH-value and PvCO2. The patients were excluded if they exhibited a drop in pH to <7.31 on 8 L/min of oxygen flow or an increase in the partial pressure of carbon dioxide within venous blood (PvCO2) of >1 kPa compared to their usual fixed oxygen dose.
Included patients provided written informed consent before participation.
Intervention
The Automated Oxygen Period
The intervention period consisted of four days with a continuous titration of the oxygen flow aiming at a target saturation between 90% and 94% using an electronic closed-loop device installed in the patients’ homes. If SpO2 dropped below 90% or exceeded 94% the oxygen flow was automatically adjusted according to the algorithm in the device.
The Fixed Dose Period
For the control period, the patients received their usual fixed oxygen flow for four days while monitoring and collecting data on SpO2 and heart rate.
The two periods were scheduled on comparable days to minimize significant variations in social or physical activities; however, no specific washout time was planned. In both periods, daily steps were monitored with an accelerometer, and the patients used their usual portable oxygen concentrator when being outdoors.
Study Technology and Data Capture
The Automated Oxygen Period
A closed-loop device O2matic Home Oxygen Treatment (HOT) (O2matic Ltd., Herlev, Denmark) was used for automated oxygen titration. Oxygen was supplied either by the 9 L/min Invacare Platinum 9 concentrator (Invacare Ltd. Brøndby, Denmark) or by the 10 L/min Caire NewLife Intensity concentrator (Medical Danmark Ltd., Ejby, Denmark), connected to the HOT device using a tube.
The patients wore the Nonin Wrist Pulse Oximeter (Nonin Medical, Inc., USA) with the sensor well-attached to a finger using a sensor tape, Figure 1. The pulse oximeter transmitted data on SpO2 and heart rate to the HOT device via Bluetooth. The adjustments on oxygen were done every second based on average SpO2 for the last 15s. The SpO2 target interval and a flow range was set at the beginning of the intervention, and only the investigator had access to modify these settings. A previous study identified a mean oxygen demand of 8 L/min during a walking test.18 Therefore, the aim was an oxygen flow from 0.5 to 8.0 L/min. However, the concentrators were only able to deliver a stable flow between 0.8 and 6.8 L/min. In case the patients removed the pulse oximeter (or experienced a general loss of signal) for more than two minutes the flow would return to usual flow ± 1 L/min and stay there until the signal was restored.
 |
Figure 1 Artistic presentation of the automated oxygen delivery setup. (A) Pulse oximeter, which transmits oxygen saturation data via Bluetooth to the closed-loop devise, (B) Closed-loop device, that titrates oxygen via the high-flow nasal cannula to the patient, (C) Oxygen concentrator, (D) Patient tablet, displaying the current saturation, oxygen flow and heart rate. The patient tablet also transmits information via Wi-fi to the online platform. |
Data Collection
The close-loop device transmitted raw real-time data (recordings each second of heart rate, SpO2, and oxygen flow) to an app on the patient-tablet. These data were relayed via Wi-Fi to a secure web platform (Microsoft Azure), where it could be accessed by the principal investigator. The patients could also view their real-time data on the tablet. For purpose of analysis, raw data could be extracted and downloaded from the platform as CSV files.
In case of a temporary disconnection to the patient-tablet, raw data were stored locally on the closed-loop device and transmitted once the connection was restored. After these periods, the online platform provided aggregated data files, derived from the raw recordings, which contained only summary information: total time with automated oxygen titration, and average values for SpO2, oxygen flow, and heart rate. For purpose of analysis, only the duration of automated oxygen titration was used from these aggregated files.
The Fixed Dose Period
During the fixed dose period, the patients wore the same wrist pulse oximeter as during the intervention. Since automated oxygen titration could only be administered in the patient’s home, we instructed the patients to remove the pulse oximeters when leaving the house during the control period, so that data were only collected when being indoors.
Data Collection
The data on SpO2 and heart rate were stored locally in the wrist oximeter. CSV files, used for analysis, were generated using Nonin’s nVISION Data Management Software. The batteries in the pulse oximeter needed to be changed every second day, and when removed, it resulted in a reset of date and time in the system. As a result, the collected data during the fixed dose period were untransparent, regarding the exact date and time.
Step Counts
The physical activity was monitored equally in both study periods using the SENS motion accelerometer (SENS innovation ApS, Denmark) placed with a patch above the patients’ knee. It continuously recorded movements, which were synchronized via an app to a web server. The system has been validated in hospitalized patients, showing accuracy even in older individuals taking small steps.22 Summary files containing information on steps were accessed from SENS online platform and used for analysis.
Outcome
Feasibility
The goal of this study was for patients to wear the pulse oximeter continuously during the daytime while having their oxygen adjusted automatically. We defined three key areas that needed to be fulfilled for it to be considered feasible: time when the patients were automatically titrated, patients’ willingness toward the intervention and clinical relevance. Prior to the study, we established the following criteria:
- Data were successfully transmitted from the wrist pulse oximeter to the closed-loop device and further to the cloud solution (<10% data loss),
- The patients wore the wrist pulse oximeter for more than 50% of the daytime (08:00–20:00),
- The time spent within target saturation was statistically different between arms and in favour of automated oxygen titration with a difference of at least 10%,
- The patients were at least as active with automated oxygen titration as with usual fixed oxygen therapy, measured by the activity sensor,
- The patients were safe with no serious adverse events, leading to unscheduled healthcare contacts.
Rationale for criteria 1, Titration time: Both raw and aggregated data received on the platform were proof of “the time when the patients were automatically titrated”. The 10% threshold was based on experiences from three earlier studies on automated oxygen delivery.7,18,20
Rationale for criteria 2, Patient willingness: We considered patients’ willingness to wear the wrist pulse oximeter in the daytime from 8 a.m. to 8 p.m. as essential for continuous oxygen titration.
Rationale for criteria 3 and 4, Clinical relevance: If automated oxygen titration did not improve oxygen saturation, it was deemed irrelevant. Therefore, we evaluated: differences in time spent with normoxia (SpO2 90–94%), moderate hypoxemia (SpO2 85–89%), severe hypoxemia (SpO2 < 85%) and hyperoxemia (SpO2 > 94%). Step count was monitored to ensure comparable activity levels across study periods, thereby minimizing potential confounding from differences in activity-related desaturation episodes.
Rationale for criteria 5, Patient safety: The setup was considered non-feasible if it posed notable risks to the patient, such as unscheduled contacts to the hospital due to acute-on-chronic respiratory failure.
Secondary outcome
At study start, after four days intervention, and after four days of usual care, the patients were assessed using the health status Clinical COPD Questionnaire (CCQ), 24-hour version.23 The CCQ is validated in Danish, consists of ten questions across three domains: symptoms, mental state, and functional state. Each question is scored from 0 to 6, with a higher score indicating a lower health status. A Minimal Important Difference (MID) of 0.4 is considered clinically relevant.24
The patients’ oxygen flow was compared between both study periods.
Variables
We included the following variables to describe the characteristics and clinical profile of the patients: age, gender, body mass index (BMI), pulmonary function and duration of LTOT, all of which were extracted from the patients’ medical records. Additionally, the patients were asked about their perceived dyspnea at rest, measured using the Borg CR10 dyspnea scale, their marital status, need for a walking aid, and frequency of engaging in activities outside their home. The patients also completed the modified Medical Research Council Dyspnea Scale (mMRC) and the COPD Assessment Test (CAT).
Randomization and Blinding
The patients were randomized after inclusion to either the automated oxygen period followed by the fixed dose period, or vice versa. The randomization list was computer-generated and compiled for each patient in REDCap electronic data capture tools (REDCap Consortium, Nashville, US) hosted at Capital Region of Denmark.
Neither the patients nor the investigator were blinded.
Statistical Considerations
Due to the feasibility design of the present study, a formal sample size calculation was not performed. In a non-feasibility design, CCQ could be a primary outcome, which would require 42 patients to detect a MID of 0.4 with a standard deviation of 0.9. For the purpose of this feasibility study, we selected a sample of 12 patients, as we considered this number sufficient to assess feasibility. Furthermore, this sample size provided an adequate basis for evaluating variations in SpO2 intervals and generating preliminary insights into the CCQ outcome.
For the analysis on the patients’ SpO2 and oxygen use in this study, only raw data extracted from CSV files were used. In the evaluation of Criteria 1, however, both raw and aggregated data were applied to obtain a more complete estimate of the ‘titration time’.
Continuous variables were examined for normality. Those meeting normality assumptions were analyzed with a paired t-test and presented as mean (standard deviation (SD)). For not normally distributed variables, the Wilcoxon signed-rank test was used, with data presented as median with interquartile range (IQR). CCQ was tested in a two-way ANOVA with treatment, period and an interaction term between treatment and period as explanatory variables to account for carryover effect bias. IBM SPSS Statistics for Windows, ver. 29.01 was used for all statistical analyses. GraphPad Prism version 10.1.2 for Windows was used to create the figures.
Results
Thirty-two patients were screened for eligibility, of whom 13 met the inclusion criteria and consented to participate, Figure 2. One patient was subsequently excluded after venous blood gas analysis revealed a PCO2 of 11.3 kPa and a pH decrease from 7.30 to 7.28 following 20 minutes with 8 L/min oxygen. Accordingly, 12 patients (four women and eight men) with a mean (SD) home oxygen dose of 2.0 (0.7) L/min were randomized, Table 1. All patients completed the study.
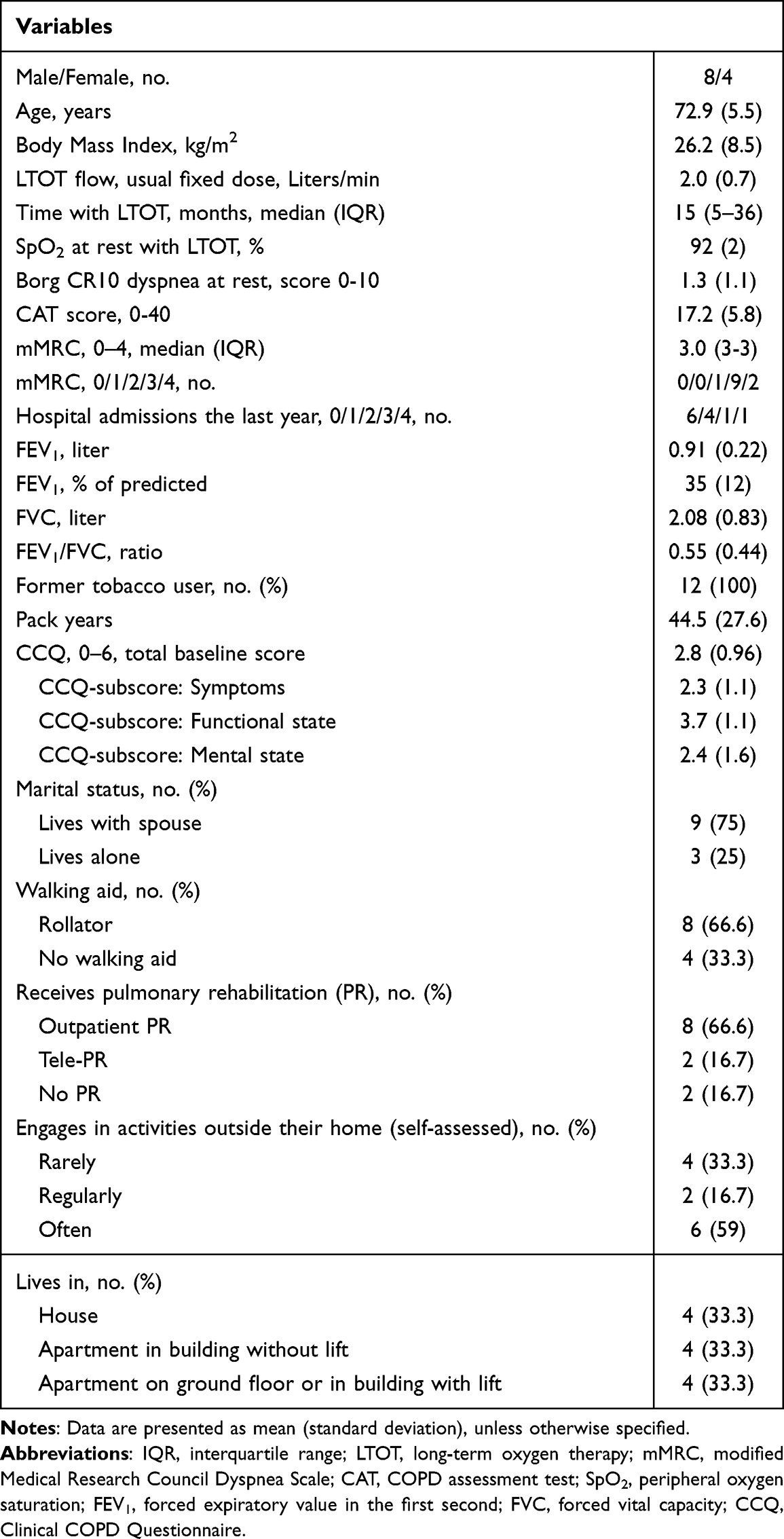 |
Table 1 Characteristics and Clinical Profile of the Study Patients with COPD on LTOT, n=12 |
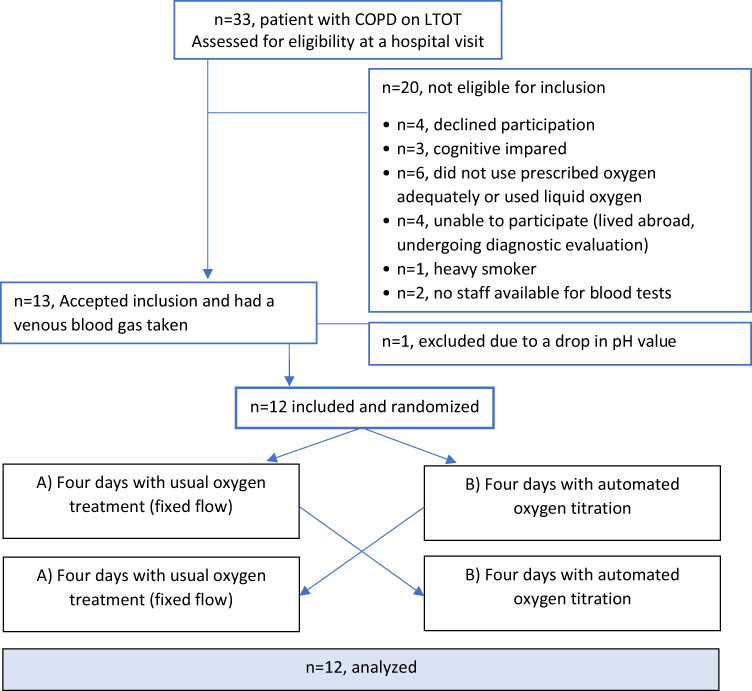 |
Figure 2 Flow diagram of inclusion of patients. |
Feasibility
During the four days of automated oxygen intervention, the equipment was installed for a median duration of 96 h (IQR 94.7–96.0). Detailed raw data were received for each patient for 69.5 h (53.3–82.8), providing more than 217,000 paired data points on SpO2 and oxygen flow per patient during the automated oxygen period, Table 2.
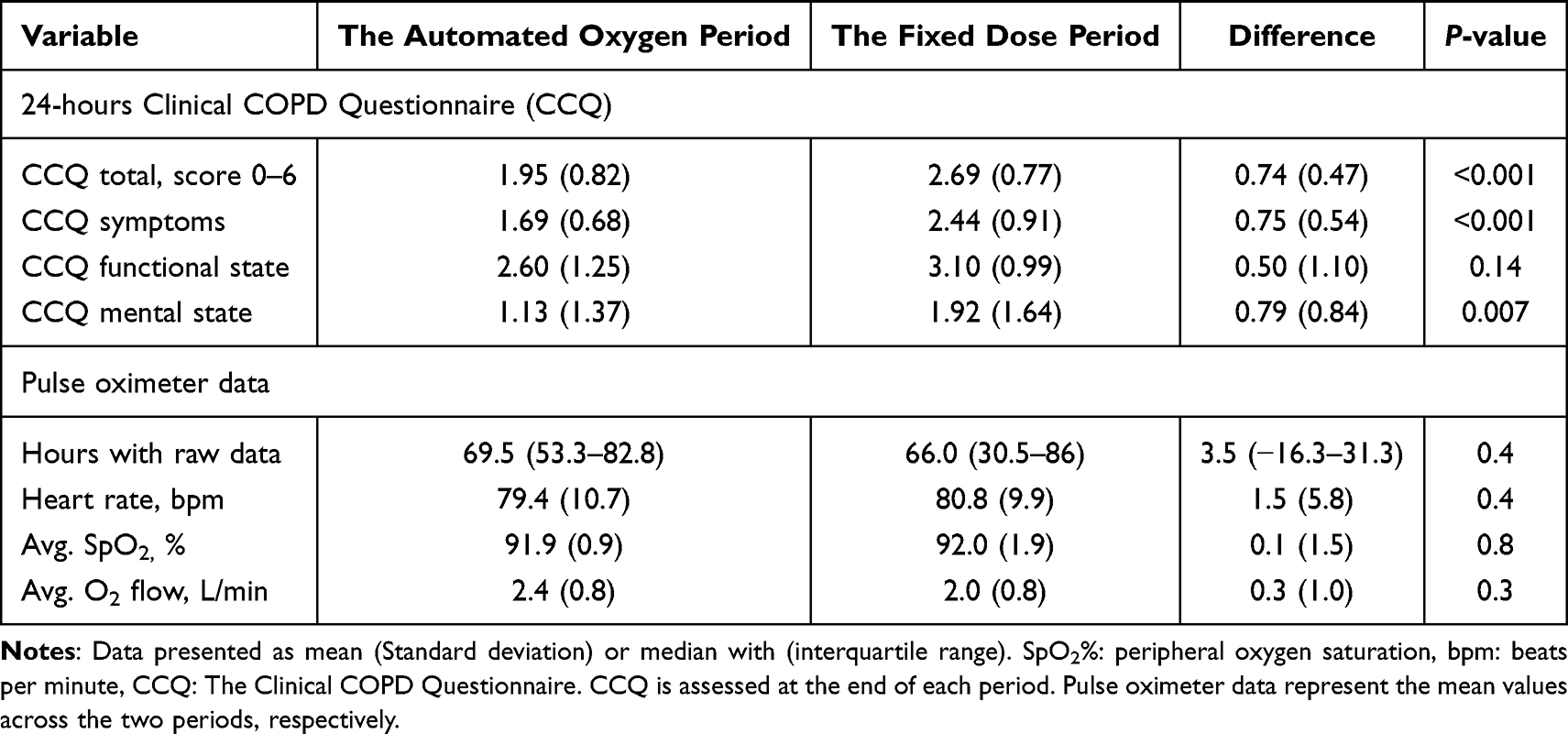 |
Table 2 Patient Reported Outcome and Physiological Parameters, n=12 |
Criteria 1, Titration time: Raw and aggregated data showed that the patients’ oxygen flow was automatically titrated for 77 h (68.0–84.3), corresponding to 83% (74–88) of the possible time. The remaining 17% reflected periods when patients left their homes, removed the pulse oximeter for showering or battery changes, or experienced unintentional signal loss and disconnection.
Criteria 2, Patient willingness: Raw data were received for 35.5 h (26.3–42.5) for each patient in the daytime period, constituting 75% (64–88) of the time. Of the 12 patients, 11 patients wore the pulse oximeter for at least 50% of the time in the automated oxygen period.
Criteria 3, Clinical relevance: Time spent with SpO2 of 90–94% differed significantly between periods: 52% (42–63) with fixed oxygen flow versus 86% (75–90) with automated titration, p = 0.002. Correspondingly, significant differences in favor of the automated oxygen intervention were also observed in time spent with moderate hypoxemia, p = 0.003, severe hypoxemia p = 0.004, and hyperoxemia p = 0.01, as illustrated in Figure 3.
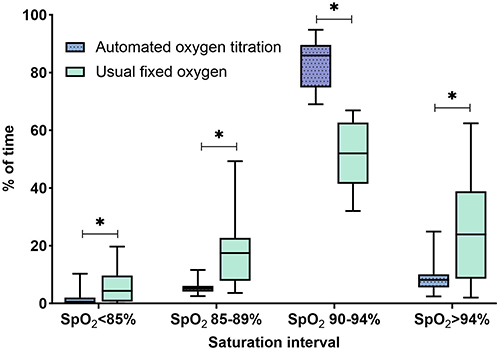 |
Figure 3 Percentage of time spent within oxygen saturation (SpO2) intervals. Boxplot illustrating median, interquartile range, minimum and maximum time spent in the various intervals. X-axis: Four predefined oxygen saturations intervals. Y-axis: Percentage of time over a total period of four full days. Statistics: Wilcoxon signed-rang test, *p ≤ 0.01. |
Criteria 4, Clinical relevance: The patients took 2,297 (1,519–3,106) steps daily in the fixed dose period and 2,366 (1,236–3,703) steps during the automated oxygen period, with no significant difference between periods, p = 0.7.
Criteria 5, Patient safety: Unintended events were observed during the intervention, none which required hospitalization or unscheduled healthcare visits. Some events triggered system alarms, primarily due to insufficient oxygen supply, see Table 3. The patients expressed annoyance with the noise from the concentrator, the bulkiness of the pulse oximeter, and the frequent use of batteries.
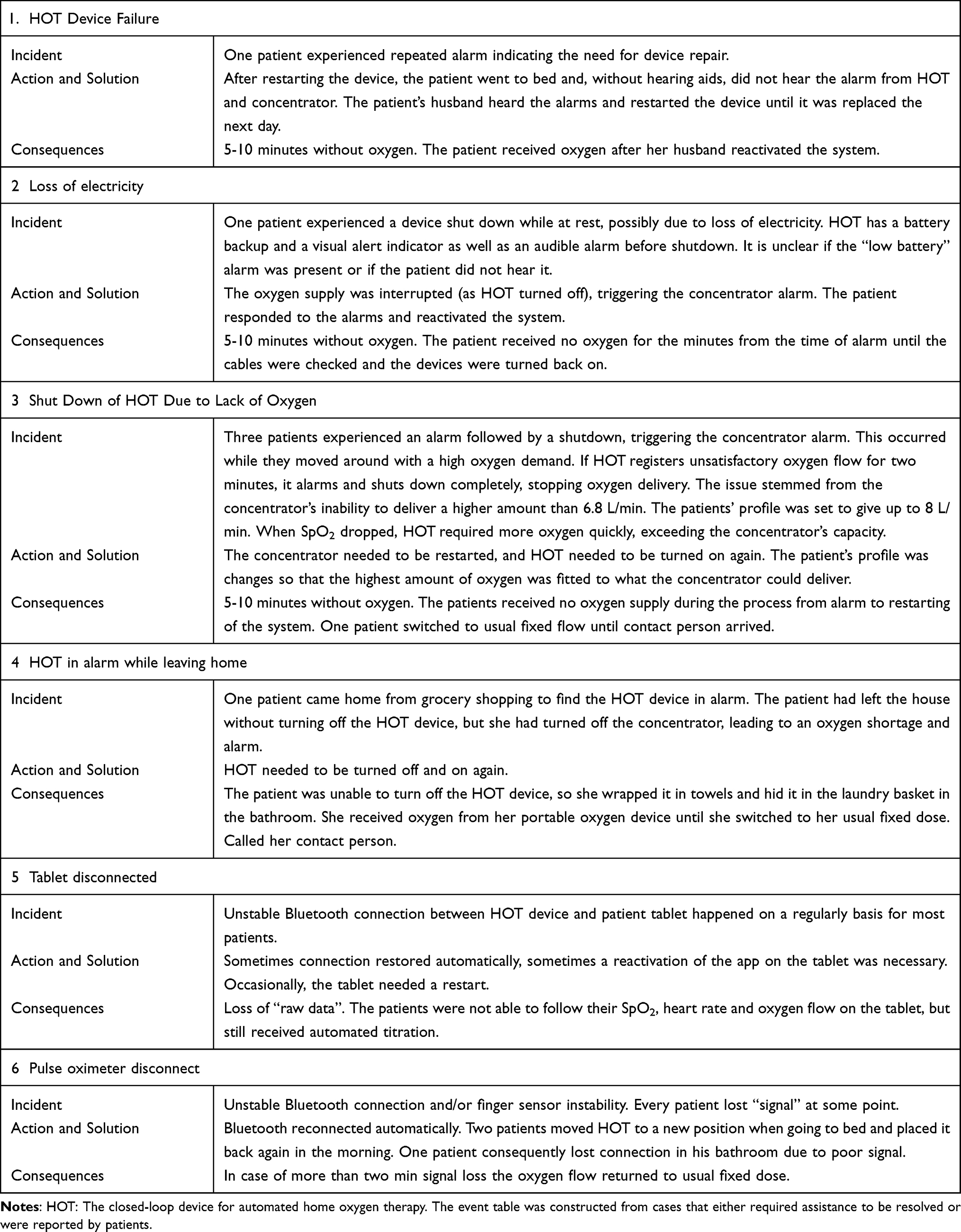 |
Table 3 Outlining Of Incidents During The Automated Oxygen Period |
Secondary Outcome
The total score in the CCQ improved significantly by a mean of 0.74 (0.47) points favoring the automated oxygen intervention, p < 0.001, Table 2. Eleven of the twelve patients met or exceeded the MID of 0.4, with individual changes presented in Figure 4.
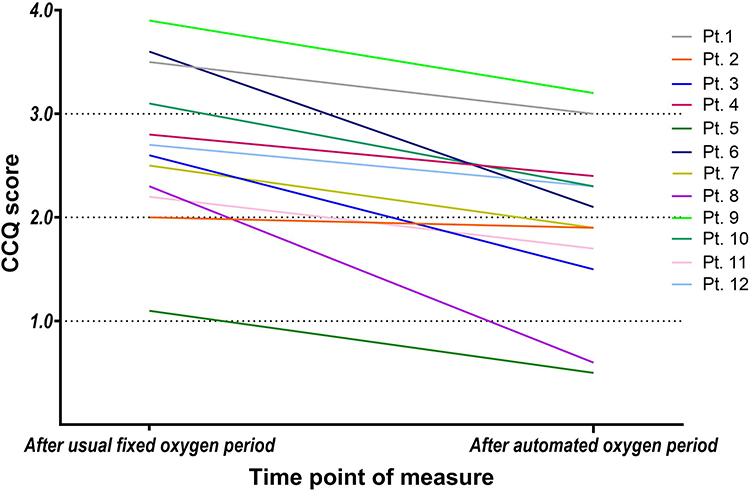 |
Figure 4 Individual scores in the CCQ. Individual 24-hour Clinical COPD Questionnaire (CCQ) scores, with higher scores indicating poorer health status. Measurements were taken after the period of usual fixed oxygen dosing and after the period of automated oxygen titration. Each line represents an individual patient. Eleven of the 12 patients showed an improvement in CCQ score of at least the minimal important difference (0.4). |
No difference in mean oxygen flow between periods was observed, p > 0.3, Table 2. However, all 12 patients used the full range of possible oxygen flow during the automated oxygen period. During 34 (18)% of the measured time, the patients’ oxygen flow was titrated up compared to their usual fixed oxygen dose, and in 38 (27)% of the time it was decreased, Figure 5.
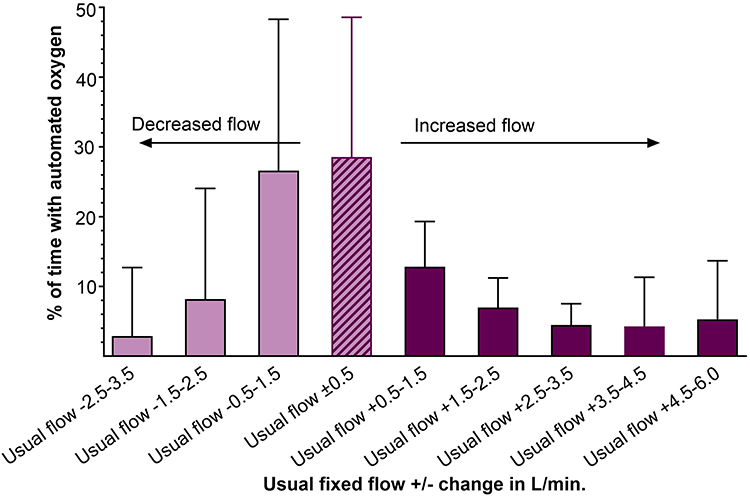 |
Figure 5 Various oxygen flow used during the automated oxygen period. The percentage of the time the patients spent using various oxygen flows during automated titration, expressed as changes in 1 L/min intervals from their usual fixed flow ±0.5 L/min. The striped bar represents the 29% (20) of the time, where the patients received their usual oxygen flow. The light purple bars indicate the percentage of time patients experienced decreased oxygen flow compared to their usual flow, while the dark purple bars represent the time in which the oxygen flow was increased. |
The test for carryover-effect showed neither significant difference in CCQ total score between the two periods nor significance of an interaction term between treatment and the period.
Discussion
We found that continuous automated oxygen titration in the homes of patients with COPD on LTOT was both feasible and well tolerated, with high patient compliance. For more than 80% of the day, the patients’ oxygen flow was titrated based on their saturation, resulting in a significant improvement in oxygenation at home compared to using their fixed dose. Furthermore, the patients reported a lower symptom burden, as measured by the CCQ, indicating a more positive perception of health status when oxygen saturation was improved.
Feasibility, Titration Time and Patient Acceptance
Our feasibility criteria were necessarily pragmatic, as no prior experience existed with continuous automated oxygen titration in this setting. One reasoning in defining the criteria, was that if the patients removed the wrist pulse oximeter for more than half of the day (criteria 2), this would indicate such limited engagement with titration that continuous automated adjustment would be of little value. The 10% threshold (in criteria 1) was intended to represent unintended loss of data; however, we soon realized that we could not distinguish between unintended data loss and deliberate (voluntary) removal of the oximeter. We also predefined the daytime as the relevant observation period since we expected patients to remove the oximeter at night. In practice, however, patients were highly motivated to keep their saturation within target, and all 12 participants wore the oximeter continuously, day and night. As a result, we obtained substantially more data than anticipated: 83% of the total four-(24h)-day study period. Importantly, the remaining 17% of missing data included both unintentional loss (criteria 1) and voluntary removal (criteria 2). Thus, taken together, data completeness clearly exceeded our predefined feasibility criteria and confirmed that technical performance and patient adherence were better than expected.
Target Saturation and Oxygen Flow
Notably, the patients were within the target range only about half of the time (52%) while using their prescribed oxygen dose at home. Given that the prescribed dose is intended to ensure adequate oxygenation, this highlights a substantial gap between intended and actual treatment effect. The mean oxygen flow and mean saturation levels were nearly identical across both study periods, but the patients’ fluctuating oxygen needs throughout the day, required full use of the device’s flow capacity. In 71% of the time where the patients used automated oxygen delivery, their oxygen flow was automatically adjusted to a different rate than their usual fixed dose. Not only did the oxygen flow increase with up to additional 5 L/min in the automated period but more than 33% of the time, the patients’ oxygen flow was reduced compared to their usual fixed dose. This highlights the fluctuating oxygen needs at an individual level for each patient. This variability in oxygen flow corresponded to the significant improvements in the time spent within the target saturation increasing from 52% to 86% of the day and thereby fulfilling feasibility criteria 3.
Fluctuating oxygen needs and time spent with hypoxemia have also been observed during walking, as well as in more home-related settings, such as during an ADL test.17–20 In a study in ADL context, the mean oxygen flow increased from 1.6 to 5.2 L/min, while the time spent with severe hypoxemia (SpO2 < 85%) decreased by 30% to 17%.20 These improvements in oxygen saturation led to enhanced performance and reduced experiences of dyspnea.
As mentioned, the patients spent approximately 22% of the day with SpO2 below 90% while using their usual fixed oxygen flow. This is slightly different from a study by Sliwinski et al, in which patients spent 30% of the day with hypoxemia.12 Patients are typically more active when being outdoors; thus, probably also more frequently experiencing hypoxemia, and this could explain the differences in time spent with hypoxemia between the present study and Sliwinski’s, where patients also were monitored while outdoors.
Sliwinski did not report how long patients maintained a saturation above 94%. However, Zhu et al argued that oxygen flow rates should be reduced during rest, as patients’ oxygen saturation were often too high.11 In the present study, we found that patients with usual oxygen dose spent 24% of their time with saturation above the target range while at home. This corresponds to six hours per day with hyperoxemia, during which the patients could use a lower oxygen flow or, depending on the degree of respiratory failure, take a break from the nasal cannula. In line with this, Ekström et al recently found that patients could pause oxygen therapy for up to nine hours per day without any consequences on mortality or hospitalization.25 However, they did not monitor for how long time the patients were well treated without hypoxemia.25 The NOTT and MRC studies from the 1980s established that reducing hypoxemia at rest by increasing PaO2 above 8 kPa reduces mortality.26,27 Oxygen use for 24 hours was found to be more beneficial than 12 hours, and 15 hours was better than no oxygen at all. However, it remains unclear whether the critical factor is the overall duration of oxygen therapy or the time spent with effective oxygen therapy (PaO2 > 8 kPa).
Health Status and Daily Step Counts
Health status, evaluated using the CCQ, could potentially detect improvements in patients’ ability to move with less dyspnea and participate in more social activities. In our 12-patient feasibility study, the CCQ overall score significantly favored the automated oxygen period, with a difference of 0.74 point, which is almost the double of the 0.4 MID established for the CCQ in this population. Both the symptoms and mental state domains of the CCQ showed significant improvement, supporting the hypothesis that optimized oxygenation can alleviate dyspnea, as also observed during walking and in ADL. Patients with advanced COPD often report a markedly impaired health-related quality of life (HRQoL),28,29 particularly those receiving long-term oxygen therapy (LTOT).30 Interventions that enhance oxygen delivery have shown meaningful clinical benefits in this patient group. High-flow nasal cannula (HFNC) therapy has been shown to stabilize SpO2 more effectively than usual oxygen therapy with fewer episodes of desaturation, which has led to reductions in exacerbation rates, hospital admissions, and improvements in subjective symptom scores.31–33 In line with this, Sandau et al reported that automated oxygen titration enhanced patients’ sense of safety during acute exacerbations,34 which, together with the improved health status observed in our study and findings from HFNC research, supports the notion that optimized and individualized oxygen delivery contributes positively to patient-perceived outcomes.
The patients in the present study were generally inactive with approximately 2,300 steps per day with no difference between periods, which aligns with what is previously reported for this severely ill group (2,400 to 3,800 steps per day).35 Our criteria 4 for feasibility related to physical activity (no difference between periods) was met. The study was not powered to find any difference in step counts and given the short, indoor-only intervention and the difficulty of changing habits we did not expect to find a difference between periods.
An essential factor in evaluating feasibility before considering a larger trial or implementation is the patients’ attitude toward the intervention. This includes the perceived burden of the technology and how well it aligns with what patients find personally meaningful and effective. Patients’ experiences are reported in a separate paper, gathered through qualitative interviews with the involved patients in the present study.36
Equipment Challenges
The proper solution for maintaining a target saturation emerged with the introduction of automated closed-loop devices for home use. Effective automated oxygen administration (based on continuous saturation monitoring during daytime and automatic oxygen adjustments) depends on optimization of all system components. This includes the closed-loop device, the pulse oximeter, and the oxygen concentrator, as well as reliable Wi-Fi and coordination between these elements. A well-designed nasal cannula capable of delivering flows above 5 L/min without causing discomfort to the patient is also preferable. Early in the study, it became apparent that the concentrators were unable to sustain an 8 L/min flow, leading us to lower the maximum flow for consistent performance. Furthermore, the standard concentrator, typically used for flow rates higher than 5 L/min, was notably noisy and the reason for the patients’ primary complaints. The pulse oximeter was by many found to be uncomfortable for constant wear and too demanding in battery use.
Adding an electronic device to the patient’s oxygen therapy system increases the risk of unintended events and system alarms. Some of these alarms are appropriate as they alert to an undesirable situation such as low oxygen flow. Acting on alarms under current conditions requires that the patients have both auditory and visual awareness, along with sufficient cognitive capacity to respond adequately to alarms or, at a minimum, switch to their standard treatment if needed. As shown in Table 3, some minor events, including system alarms, were observed. None resulted in patient harm, thereby fulfilling feasibility criteria 5 regarding patient safety.
Strength and Limitation
A key strength of the present study is the home setting, where patients behaved as they typically would, without the need for round-the-clock support. They engaged in their usual daily activities and moved around with their normal level of physical activity. This provided valuable insight into how automated oxygen titration might function in real-world conditions and its potential impact on patients’ daily lives. We believe, the data we received were reflective of real-life scenarios.
Another strength is the extensive amount of data collected for each patient. We collected data over two four-day periods, providing a detailed overview of time spent in different SpO2 intervals with and without the automated oxygen delivery. The same wrist pulse oximeter ensured consistent saturation measurements during both periods.
A central limitation of this study is the non-blinded design, which may have influenced patient-reported outcomes such as the CCQ. Although patients reported clinically relevant improvements with increased time in normoxia, the small sample size and lack of blinding mean these findings should be interpreted as indicative rather than conclusive. The mental state domain of the CCQ addresses anxiety and worries about disease progression. As highlighted in the previous qualitative work, patients strongly associate desaturation with dyspnea and distress, and simply knowing that oxygen titration was being automated may have alleviated anxiety and improved self-reported well-being, independent of physiological effects. Nevertheless, whether perceived or real, such reductions themselves can be meaningful for the patients. In addition, the option for patients to directly contact the investigator in case of problems may have provided a reassuring effect, potentially amplifying the sense of safety across both study arms. Furthermore, the short intervention period may have increased patients’ willingness to tolerate the noise from the oxygen concentrator and wearing the wrist pulse oximeter. Both aspects were among the most frequent issues criticized by the patients, and over longer durations they may lead to fatigue and reduce the feasibility of the intervention in routine practice, underscoring a pressing need for better oxygen delivery technology.
A large, long-term trial is needed to confirm the preliminary positive effects on health status, including outcomes such as hospitalization and mortality. Such a study should also rigorously address cost-effectiveness, providing a clearer basis for future clinical and economic decision-making.
Conclusion
In the home setting, it was feasible to increase the time that patients with stable COPD on long-term oxygen therapy spent within target saturation from 52% to 86% of the day using automated oxygen titration. This improvement in oxygen saturation appeared to be associated with better patient-perceived health status, reflecting reduced symptom and cognitive burden, such as dyspnea and worries in daily life. These findings need to be confirmed in a larger RCT with a longer follow-up period. Despite promising advances in digital technologies for home oxygen therapy, the need for technical equipment updates and further development still remains.
Data Sharing Statement
Due to Danish national legislation (Data Protection Act §10 and the Data Disclosure Proclamation Act), public deposition of raw data is not permitted. Pseudonymized data can only be shared following approval by the Danish Data Protection Agency and, in compliance with Capital Region data governance. Researchers interested in accessing the data may contact the corresponding author to discuss the procedure. However, any official request for access must be approved by the Danish Data Protection Agency; the authors cannot grant access independently.
Acknowledgment
A special thank you to Ida Heefelt for her support and assistance with blood gases. Thanks to O2matic Ltd. for adjusting the equipment to align with our study requirements and for consistently incorporating feedback from both our study team and the patients. During the preparation of this work, the first author used ChatGPT in the writing process in order to improve the readability of the manuscript. After using this tool/service, the authors reviewed and edited the content as needed and take full responsibility for the content of the published article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was funded by Innovation Fund Denmark grant nr. 8056-00054B, Swedish Respiratory Society (SMLF) and The Association of Danish Physiotherapists Research Fund.
Disclosure
This paper is based on the thesis of Linette Marie Kofod. It has been published on the institutional website of Örebro University, Sweden, https://www.diva-portal.org/-smash/record.jsf?pid=diva2:1955394. The authors original manuscript has been uploaded as a preprint on medRxiv: https://www.medrxiv.org/content/10.1101/2025.01.23.25320958v1. One of the investigators (Ejvind Frausing Hansen) is a co-inventor of the closed-loop device and holds shares in O2matic Ltd. Neither the company nor the funders had influence on the protocol, the data analysis, or the writing of the scientific paper. The authors report no other conflicts of interest in this work.
References
1. Austin MA, Wills KE, Blizzard L, Walters EH, Wood-Baker R. Effect of high flow oxygen on mortality in chronic obstructive pulmonary disease patients in prehospital setting: randomised controlled trial. BMJ. 2010;341(oct18 2):c5462. doi:10.1136/bmj.c5462
2. Chu DK, Kim LH, Young PJ, et al. Mortality and morbidity in acutely ill adults treated with liberal versus conservative oxygen therapy (IOTA): a systematic review and meta-analysis. Lancet. 2018;391(10131):1693–1705.
3. O’Driscoll BR, Howard LS, Earis J, Mak V, British Thoracic Society Emergency Oxygen Guideline Group, BTS Emergency Oxygen Guideline Development Group. BTS guideline for oxygen use in adults in healthcare and emergency settings. Thorax. 2017;72(Suppl 1):ii1–ii90. doi:10.1136/thoraxjnl-2016-209729
4. L’Her E, Dias P, Gouillou M, et al. Automatic versus manual oxygen administration in the emergency department. Eur Resp J. 2017;50(1):1602552
5. Harper J, Kearns N, Bird G, et al. Automatic versus manual oxygen titration using a novel nasal high-flow device in medical inpatients with an acute illness: a randomised controlled trial. BMJ Open Respir Res. 2021;8(1):e000843. doi:10.1136/bmjresp-2020-000843
6. Lellouche F, Bouchard PA, Roberge M, et al. Automated oxygen titration and weaning with FreeO2 in patients with acute exacerbation of COPD: a pilot randomized trial. Int J Chron Obstruct Pulmon Dis. 2016;11:1983–1990. doi:10.2147/COPD.S112820
7. Sandau C, Hansen EF, Ringbæk TJ, et al. Automated oxygen administration alleviates dyspnea in patients admitted with acute exacerbation of COPD: a randomized controlled trial. Int J Chron Obstruct Pulmon Dis. 2023; 18:599–614.
8. Hansen EF, Hove JD, Bech CS, Jensen JS, Kallemose T, Vestbo J. Automated oxygen control with O2matic((R)) during admission with exacerbation of COPD. Int J Chron Obstruct Pulmon Dis. 2018;13:3997–4003.
9. Hardinge M, Annandale J, Bourne S, et al. British thoracic society guidelines for home oxygen use in adults. Thorax. 2015;70(1):1. doi:10.1136/thoraxjnl-2015-206865
10. Jacobs SS, Krishnan JA, Lederer DJ, et al. Home oxygen therapy for adults with chronic lung disease. an official American thoracic society clinical practice guideline. Am J Respir Crit Care Med. 2020;202(10):e121–e141. doi:10.1164/rccm.202009-3608ST
11. Zhu Z, Barnette RK, Fussell KM, Michael Rodriguez R, Canonico A, Light RW. Continuous oxygen monitoring--a better way to prescribe long-term oxygen therapy. Respir Med. 2005;99(11):1386–1392. doi:10.1016/j.rmed.2005.03.010
12. Sliwiński P, Lagosz M, Górecka D, Zieliński J. The adequacy of oxygenation in COPD patients undergoing long-term oxygen therapy assessed by pulse oximetry at home. Eur Respir J. 1994;7(2):274–278. doi:10.1183/09031936.94.07020274
13. Decker MJ, Arnold JL, Haney D, Masny J, Strohl KP. Extended monitoring of oxygen saturation in chronic lung disease. Chest. 1992;102(4):1075–1079. doi:10.1378/chest.102.4.1075
14. Sant’Anna T, Donária L, Hernandes NA, et al. Oxygen desaturation in daily life and during a laboratory-based protocol of activities of daily living in COPD: is there relationship? Lung. 2018;196(1):19–26. doi:10.1007/s00408-017-0068-4
15. Soguel Schenkel N, Burdet L, de Muralt B, Fitting JW. Oxygen saturation during daily activities in chronic obstructive pulmonary disease. Eur Respir J. 1996;9(12):2584–2589. doi:10.1183/09031936.96.09122584
16. Plywaczewski R, Sliwinski P, Nowinski A, Kaminski D, Zieliński J. Incidence of nocturnal desaturation while breathing oxygen in COPD patients undergoing long-term oxygen therapy. Chest. 2000;117(3):679–683. doi:10.1378/chest.117.3.679
17. Schneeberger T, Jarosch I, Leitl D, et al. Automatic oxygen titration versus constant oxygen flow rates during walking in COPD: a randomised controlled, double-blind, crossover trial. Thorax. 2023;78(4):326–334. doi:10.1136/thoraxjnl-2020-216509
18. Kofod LM, Westerdahl E, Kristensen MT, Brocki BC, Ringbæk T, Hansen EF. Effect of automated oxygen titration during walking on dyspnea and endurance in chronic hypoxemic patients with COPD: a randomized crossover trial. J Clin Med. 2021;10(21):4820. doi:10.3390/jcm10214820
19. Vivodtzev I, L’Her E, Vottero G, et al. Automated O(2) titration improves exercise capacity in patients with hypercapnic chronic obstructive pulmonary disease: a randomised controlled cross-over trial. Thorax. 2019;74(3):298–301. doi:10.1136/thoraxjnl-2018-211967
20. Kofod LM, Hansen EF, Brocki BC, Kristensen MT, Roberts NB, Westerdahl E. Optimised oxygenation improves functional capacity during daily activities in patients with COPD on long-term oxygen therapy: a randomised crossover trial. Thorax. 2025; 2025:thorax–221883.
21. Byrne AL, Bennett M, Chatterji R, Symons R, Pace NL, Thomas PS. Peripheral venous and arterial blood gas analysis in adults: are they comparable? A systematic review and meta-analysis. Respirology. 2014;19(2):168–175. doi:10.1111/resp.12225
22. Pedersen BS, Kristensen MT, Josefsen CO, Lykkegaard KL, Jønsson LR, Pedersen MM. Validation of two activity monitors in slow and fast walking hospitalized patients. Rehabil Res Pract. 2022;2022:9230081. doi:10.1155/2022/9230081
23. van der Molen T, Willemse BW, Schokker S, ten Hacken NH, Postma DS, Juniper EF. Development, validity and responsiveness of the clinical COPD questionnaire. Health Qual Life Outcomes. 2003;1(1):13. doi:10.1186/1477-7525-1-13
24. Kon SS, Dilaver D, Mittal M, et al. The clinical COPD questionnaire: response to pulmonary rehabilitation and minimal clinically important difference. Thorax. 2014;69(9):793–798. doi:10.1136/thoraxjnl-2013-204119
25. Ekström M, Andersson A, Papadopoulos S, et al. Long-term oxygen therapy for 24 or 15 hours per day in severe hypoxemia. N Engl J Med. 2024;391(11):977–988. doi:10.1056/NEJMoa2402638
26. Nocturnal Oxygen Therapy Trial Group. Continuous or nocturnal oxygen therapy in hypoxemic chronic obstructive lung disease: a clinical trial. Ann Intern Med. 1980;93(3):391–398. doi:10.7326/0003-4819-93-3-391
27. Party MW. Long term domiciliary oxygen therapy in chronic hypoxic cor pulmonale complicating chronic bronchitis and emphysema. Report of the medical research council working party. Lancet. 1981;1(8222):681–686.
28. Habraken JM, ter Riet G, Gore JM, et al. Health-related quality of life in end-stage COPD and lung cancer patients. J Pain Symptom Manage. 2009;37(6):973–981. doi:10.1016/j.jpainsymman.2008.07.010
29. Ståhl E, Lindberg A, Jansson S, et al. Health-related quality of life is related to COPD disease severity. Health Qual Life Outcomes. 2005;3(1):56. doi:10.1186/1477-7525-3-56
30. Cani KC, Matte DL, Silva IJ, Gulart AA, Karloh M, Mayer AF. Impact of home oxygen therapy on the level of physical activities in daily life in subjects with COPD. Respir Care. 2019;64(11):1392–1400. doi:10.4187/respcare.06206
31. Theunisse C, de Graaf NTC, Braam AWE, et al. The effects of home high-flow nasal cannula oxygen therapy on clinical outcomes in patients with severe COPD and frequent exacerbations. J Clin Med. 2025;14(3):868. doi:10.3390/jcm14030868
32. Storgaard LH, Hockey H, Laursen BS, Weinreich UM. Long-term effects of oxygen-enriched high-flow nasal cannula treatment in COPD patients with chronic hypoxemic respiratory failure. Int J Chron Obstruct Pulmon Dis. 2018;13:1195–1205. doi:10.2147/COPD.S159666
33. Nagata K, Horie T, Chohnabayashi N, et al. Home high-flow nasal cannula oxygen therapy for stable hypercapnic COPD: a randomized clinical trial. Am J Respir Crit Care Med. 2022;206(11):1326–1335. doi:10.1164/rccm.202201-0199OC
34. Sandau C, Poulsen I, Nørholm V, et al. Patients’ perspective on automated oxygen administration during hospitalization for acute exacerbation of chronic obstructive pulmonary disease: a qualitative study nested in a randomized controlled trial. COPD. 2022;19(1):345–352. doi:10.1080/15412555.2022.2141620
35. Saunders T, Campbell N, Jason T, et al. Objectively measured steps/day in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. J Phys Act Health. 2016;13(11):1275–1283. doi:10.1123/jpah.2016-0087
36. Kofod LM, Laursen LB, Westerdahl E, et al. The experience of automated home oxygen therapy for patients with COPD - A qualitative study. COPD. 2025;22(1):2477243. doi:10.1080/15412555.2025.2477243
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.