Back to Journals » ClinicoEconomics and Outcomes Research » Volume 16
Automated Drugs Dispensing Systems in Hospitals: a Health Technology Assessment (HTA) Study Across Six European Countries
Authors Foglia E ![]() , Asperti F, Antonacci G, Jani YH, Garagiola E, Bellavia D, Ferrario L
, Asperti F, Antonacci G, Jani YH, Garagiola E, Bellavia D, Ferrario L ![]()
Received 27 May 2024
Accepted for publication 16 August 2024
Published 20 September 2024 Volume 2024:16 Pages 679—696
DOI https://doi.org/10.2147/CEOR.S468417
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Dean Smith
Emanuela Foglia,1 Federica Asperti,1 Grazia Antonacci,2,3 Yogini H Jani,4 Elisabetta Garagiola,1 Daniele Bellavia,1 Lucrezia Ferrario1
1LIUC - University Cattaneo, Healthcare Datascience LAB, Castellanza, Varese, 21053, Italy; 2Department of Primary Care and Public Health, Imperial College London, National Institute of Health Research (NIHR) Applied Research Collaboration (ARC) Northwest London, London, UK; 3Business School, Centre for Health Economics and Policy Innovation (CHEPI), Imperial College London, London, UK; 4Centre for Medicines Optimisation Research and Education, University College London Hospitals NHS Foundation Trust, London, UK
Correspondence: Elisabetta Garagiola, Healthcare Datascience Laboratory - HD LAB, LIUC-Università Cattaneo, Corso G. Matteotti, 22, Castellanza, VA, 21053, Italy, Tel +39.0331.572.467, Email [email protected]
Background: Automated Drug Dispensing (ADD) systems are considered to be strategic hospital assets used to reduce errors and enhance economic and organizational sustainability. With regards to efficacy and safety, the literature evidence demonstrates the incremental benefits of centralised or decentralised systems compared to manual dispensing. Analyses about organisational and economic sustainability are still lacking and the present study aims to perform a Health Technology Assessment (HTA), producing multidimensional evidence on the use of ADD systems within hospitals.
Methods: In 2023, a comprehensive HTA draws insights from healthcare professionals across six European nations: Italy, France, Germany, the Netherlands, the United Kingdom, and Belgium. This appraisal juxtaposed four drug dispensing scenarios: manual methods, centralized ADD systems, decentralized ADD systems, and integrated solutions employing cutting-edge technologies in both central pharmacies and wards. The study deployed an Activity-Based Costing approach that was combined with a cost-effectiveness and Budget Impact Analysis to evaluate economic impacts. Qualitative questionnaires were implemented to assess ethical, legal, organizational, safety, and efficacy aspects.
Results: From a multidimensional perspective, healthcare professionals acknowledged ADD manifold advantages of ADD systems. From an organizational perspective and within a 12-month timeframe, transitioning to automation may face initial challenges that are attributed to potential resistance from professionals and significant investments. However, 36 months past its adoption, automation’s superiority over manual methods was recognized. Economically, savings burgeoned from +17.9% in UK to +26.6% in Belgian hospitals that adopted integrated systems in comparison to traditional manual approaches.
Conclusion: Compared to traditional methods, implementing ADD systems could improve the logistic management of drug in the hospital setting, thereby enhancing safety and efficacy, streamlining the healthcare professionals’ workflow, and bolstering financial stability.
Keywords: automated drug dispensing systems, HTA, economic impact, drug logistic management, efficiency
Introduction
As healthcare systems cope with ongoing challenges, medications logistics emerged as a strategic asset for hospitals. Medication logistics especially ensures service quality, minimizes errors, and bolsters both economic and organizational sustainability, especially important in this era of downsizing and limiting of healthcare personnel.1 Automated Drug Dispensing (ADD) systems, which are recognized as potentially enhancing medication safety as well as the medication, the process and the workforce efficiency,2–4 utilize digital technologies and information technologies to store, package, and dispense medications. They have been linked to fewer medication errors, heightened administration accuracy, and a more efficient pharmacy workflow,5–7 especially when paired with electronic prescribing systems.8 However, ADD systems can be expensive, potentially straining hospital budgets. Additionally, there’s an ongoing debate about their real-world effectiveness in enhancing workflow and reducing medication errors:9 different results might be underlined if considering different organisational or national contexts.4
Scholarly literature that compares the various ADD systems illuminates the incremental benefits between the manual dispensing methods and centralised or decentralised systems.7 Primarily, studies have underscored the automation’s impact on effectiveness10–12 and safety,4,13 particularly concerning the lessening of medication errors and adverse drug events.6 However, some evidence14 identified only modest benefits from decentralized automated dispensing in diminishing medication errors, emphasizing the pressing need for more holistic research focused on cost-effectiveness and economic implications. Indeed, a rigorous assessment of these systems’ influence on hospital efficiency, juxtaposed with their effectiveness and safety, is of utmost importance. In addition, the integration of ADD systems could offer advantages across several organizational levels, potentially leading to significant economic benefits.
However, the merits and limitations of these technologies have only been partially explored by the academic literature and the evidence produced is of average quality and has only poor possibilities for the generalization of the results achieved. Furthermore, key stakeholders and decision-makers—such as clinicians, pharmacists, and policymakers—have not fully acknowledged their implications,15 revealing a considerable knowledge deficit. While there exists evidence and reviews affirming the safety and efficacy of ADD systems,16 a comparison of centralized and decentralized methods within a fully integrated medication management system is conspicuously absent. In this view, it’s imperative to adopt a comprehensive perspective, encompassing a wide array of factors associated with the uptake and application of such technologies. A thorough multi-dimensional assessment, that may highlight the economic and organizational feasibility of innovative drug logistics systems and touch upon the organizational, legal, equity, social, and safety consequences has yet to be undertaken. Specifically, there’s a need to delineate the viewpoints of all stakeholders who are typically engaged in the decision-making processes concerning the deployment of ADD systems. The design of specific studies that can overcome the actual knowledge gap concerning the real-life generalizability of ADD system safety, efficiency, and effectiveness,17 could provide more precise and complete information related to the impact of these technologies on hospital performance to effectively support the decision-making process. This approach could pave the way to increase the breadth and depth of technological performance, enriching quantitative data with qualitative perceptions.18
It is essential to delineate the intrinsic value of drug dispensing technologies and their prospective implications for healthcare institutions.19 By integrating this value into the decision-making paradigm, policymakers could appraise beyond mere technical dimensions, thereby gaining insights into organizational, ethical, accessibility, and societal concerns (breadth), with different points of views (depth).20
To generate comprehensive evidence regarding the utilization of ADD technologies within the hospital environment, this study will employ a Health Technology Assessment (HTA) multi-dimensional approach.21 It aims to offer pertinent insights for a broad spectrum of stakeholders, including national and regional institutions, decision-makers concerned with the inception of innovative technologies, end-users, and tender overseers, among others. In this context, considering the importance of automated solutions within the fields of healthcare operations management, the incorporation of comparative effectiveness research alongside HTA analysis could substantially bolster the adoption of these innovative technologies, paving new avenues for patient care that prioritize safety and timely response to healthcare demands.22
The primary aim of this research is to delineate the implications associated with the integration of ADD technologies, encapsulating both organizational and economic facets. This is to furnish both qualitative and quantitative data on the advantages of these solutions in hospitals across six European nations: Italy, Germany, the Netherlands, Belgium, the United Kingdom (UK), and France. Attaining such an ambitious goal, anchored in an HTA framework, is pivotal in addressing the policy queries here proposed:
- “In terms of HTA’s characteristic domains, what could be the principal benefits of adopting ADD systems with varying degrees of integration between the Central Pharmacy and respective wards, that can also provide generalizability and a local adaptation of the derived results?”
- “How does this compare to traditional manual dispensing methods, taking into account not just the hospital’s perspective on economic and organizational sustainability, but also the perceptions of healthcare professionals actively using these systems, while addressing the lack of robust evidence in the literature?”
Materials and Methods
Study Design
A mixed method approach was defined to answer the research questions, combining both qualitative and quantitative data and analyses. By triangulating different data sets and evidence derived both from the literature and from real practice,23,24 several perspectives were explored and the understanding of a such complex issues and phenomena was enhanced.
An HTA was undertaken in 2023 from a hospital-centric viewpoint as an evaluation tool to carefully define the potential impacts of ADD systems on different dimensions of interest (breadth). The assessment focused on comparing four scenarios, delineated based on the extant literature, regarding the integration of automation within hospital settings and the innovative technologies currently available in the market.
- Scenario 1: this scenario pertains to manual drug management and dispensing, both within the Central Pharmacy and the wards.5
- Scenario 2: this scenario involves the use of centralized pharmacy automated dispensing systems catering to inpatient needs, and occasionally, outpatient demands.25
- Scenario 3: this scenario encompasses decentralized systems that incorporate the various automated technologies, such as dispensing cabinets situated within wards, which are enhanced with medication traceability, thereby aiding nurses in their dispensing tasks.26
- Scenario 4: this scenario results from the integration of the technologies of Scenarios 2 and 3, culminating in a integrated automated system.27
Given the multifaceted and interdisciplinary essence of HTA, the aforementioned Scenarios underwent evaluation from multiple perspectives, as recommended by the AdHopHTA Model:28 i) technological use, ii) safety, iii) efficacy and effectiveness, iv) economic and financial impact, v) organizational dimension, and vi) strategic and political aspects. The assessment leverages on a mixed method approach, and, in adherence also to the principle of research elements triangulation,29 the methodology applied in this study encompassed a systematic literature review (to determine efficacy, safety and efficiency parameters), qualitative methods (integrating healthcare professionals’ perception, gathered via a dedicated questionnaire) and the employment of health economics’ instruments. The latter discerns the economic and organizational sustainability of ADD systems, with data inputs garnered from the relevant literature.3,4,13
Ethical approval for the study was obtained by the Carlo Cattaneo – LIUC University Ethical Committee (protocol number #R05-23, dated February 24th, 2023).
Qualitative Questionnaire
A convenience sample30 was considered for the analysis. Preliminary desk research was conducted to identify the characteristics of the reference hospitals and to find an adequate sample of potential healthcare professionals to be involved in the study. The invitations were sent via email, trying to have more than one professional per hospital invited to join the qualitative study, aiming at avoiding the common method bias.31 The inclusion criteria in the selection of healthcare professionals were: i) working in hospitals of different dimensions (small, medium and large), ii) various professional profile (pharmacists, decision makers, nurses and biomedical technicians/engineers), iii) professional working in at least one of six European countries (Italy, Germany, France, Netherlands, UK and Belgium).
Healthcare professionals were invited to participate in this study between March 2023 and July 2023.
The panel of expert healthcare professionals was convened to gather insights and perceptions that would shape a qualitative understanding of the potential impacts of automated solutions.
Utilizing validated qualitative questionnaires, various HTA domains were probed. These questionnaires incorporated items derived from the EUnetHTA Core Model concerns,32 extensively used in the literature.33 Further tailored integrations and modifications were made to suit the distinct nature of the automated technologies under examination. The primary items employed to appraise each dimension were many:
- Safety: evaluated based on i) adverse events or harms due to dispensing errors; ii) management of expired drugs and iii) general patient’s safety.
- Efficacy: probed concerning i) medication administration errors; ii) outpatients dispensing errors and iii) dispensing errors if combined with additional technologies, such as electronic prescribing.
- Equity aspect: examined factors such as i) patients’ clinical pathway efficiency (measured as the reduction in follow-ups or in the clinical pathway timing) and ii) general accessibility to healthcare services.
- Social and ethical impact: assessed benefits related to i) perceived quality of life and satisfaction; ii) trust between clinicians/nurses and patients.
- Legal impact: included considerations of i) adherence to local policies and European/National regulations; ii) legal controversies in the drug dispensing processes; iii) theft of drugs and other materials from hospital stocks.
- Organisational impact: covered aspects like i) additional people; ii) training courses; iii) learning time and impact on professionals’ workflow; iv) overall drug purchasing time; v) stock and inventory management; vi) impact of different wards’ connection; vii) impact on the relationship between healthcare workers; viii) impact on healthcare professionals’ organisational well-being and satisfaction, considering both the short-term (12 months) and long-term (36 months) time horizon.
Respondents were asked to provide comparative feedback on the aforementioned scenarios, using an evaluative scale that spanned from −3 (detrimental impact) to +3 (beneficial impact).34 The questionnaire used for this purpose is appended as Supplementary Material.
Beyond capturing qualitative perspectives, the questionnaire was engineered to collect quantitative data, particularly concerning organizational and economic variables. Metrics like hospital size, bed count, allocated resources (both technical and human) for the Central Pharmacy and wards, volume of drug packages processed, expired drugs, logistic activity durations, and manual dispensing times were recorded.
To uphold data privacy and confidentiality, participants were entrusted with self-completing the questionnaire using the Lime Survey platform, which is able to guarantee the anonymity of the respondents. Before completing the survey, participants were asked to consent to data processing, study adherence and participation: a written informed consent was collected before the compilation of the survey. Participants who wanted to proceed filling the survey, should subscribe it. They were also provided information about data management, processing methods and the research objective. Gathered data was catalogued into a standardized MS Excel format and was later merged to create a consolidated database in MS Excel. Subsequent analysis employed descriptive statistics via SPSS Version 27.0, probing statistically significant deviations (p-value < 0.05) across scenarios, countries, and professional capacities using the ANOVA test to verify generalizability and robustness of the results.
Economic and Organizational Analysis
To examine the economic dimension of this study, three distinct health economics methodologies were applied,35–37 all centred on the perspective of the hospital within a 12-month time frame.
Activity-Based Costing Analysis (ABC)
An Activity-Based Costing analysis (ABC) was performed32 to determine the total cost of logistics processes for drugs management within the six countries. The analysis incorporated different cost drivers: i) time that healthcare professionals dedicate to pharmaceutical logistics activities; ii) waste related to expired drugs; iii) administration errors; iv) stock-outs occurring in the drug management.
The analyses were based on some initial assumptions: i. the costs related to drug management and delivery within the hospital facilities were included; ii. procurement costs and inbound logistics costs, for which any changes among the different Scenarios did not occur, were considered as fixed costs; iii. costs related to the acquisition and implementation of automated dispensing systems for the Central Pharmacy, the wards or both, were considered as the initial investments.
The allocation basis considered was the number of inpatients being treated by a medium-size hospital (with the initial hypothesis of a hospital’s bed saturation rate equal to 85%), in the European landscape.
The hourly labour costs required to analyse healthcare professionals’ costs related to the drug management process for the six countries involved in the study, were obtained by reviewing the respective National Collective Labour Agreements in place in 202338 and by stratifying the healthcare professionals, as based on their professional roles (pharmacists, nurses, and technicians) (Table 1). The healthcare professionals involved in logistics activities who were considered for the economic analysis were technicians and pharmacists for the activities performed in the Central Pharmacy and nurses for drug management activities in the wards.
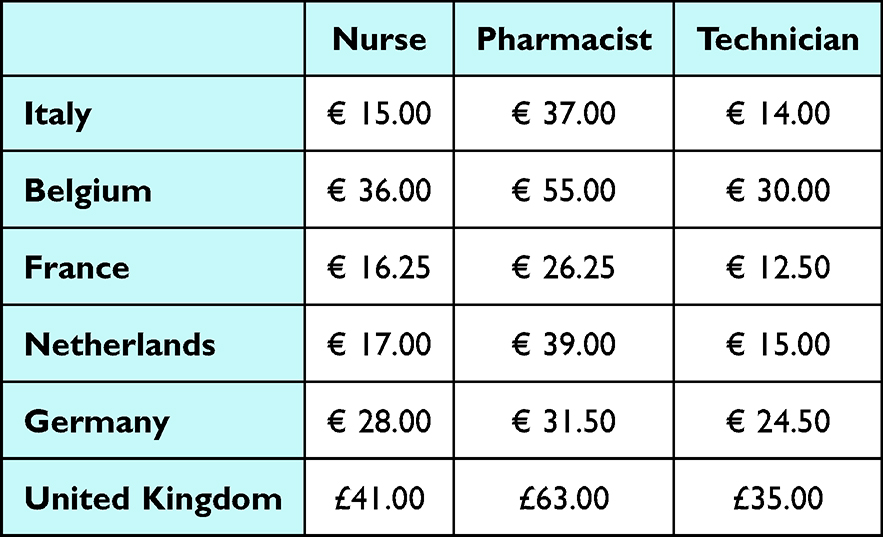 |
Table 1 Hourly Labour Costs for All the European Countries |
Expired drugs and related economic evaluation, useful to determine the waste costs, were estimated based on the surplus medications data declared by the experts involved in the qualitative data retrieval. The occurrence rate related to expired drugs (0.50% for the manual dispensing Scenario and 0.30% for the Scenario 2, 3 and 4) was derived from data collected and reported by the King’s College Hospital.10
Table 2 presents the calculations used to perform the ABC for each cost driver, both for the Central Pharmacy and the wards, to derive the total cost of drug management, associated with each Scenario. Then, to define the process costs, the total costs were divided by the number of inpatients.
 |
Table 2 Activity-Based Costing Analysis’ Calculations |
Cost-Effectiveness Analysis (CEA)
Subsequent to determining the process costs, a Cost-Effectiveness Analysis (CEA) was executed.36 This aimed to discern which Scenario of the four under assessment would offer the best trade-off between incurred process costs and efficacy realized for each country included in the study, particularly with regards to the potential of ADD technologies to mitigate dispensing errors both within the Central Pharmacy and in the wards, assuming that a threshold value could not be defined as a reference for all the six countries, which would vary according to the size of the hospital and the healthcare services provided.
Dispensing error rates were sourced searching in the literature10–12 (Table 3), identifying two different rates to guarantee the adaptability to the specific practices in each country: one pertinent to the UK context10 and another characterised by an high level of robustness,16 which was applicable to the remaining five European countries.11,12
 |
Table 3 Dispensing Errors Rates, derived from the Literature |
The UK-specific rate was adopted due to the presence of a nationally focused study and considering that the English context represents differential characteristics in terms of the adoption and implementation of automated solutions in comparison with the other European countries.10 Furthermore, feedback from participating healthcare professionals indicated a steeper learning curve associated with automation in the UK when juxtaposed with the other European nations.
These dispensing error rates were subsequently applied to the volume of packages managed in each national context. This volume was deduced from the average values provided by the respective participating hospitals for each nation.
Consequently, the CEA, in terms of Cost-Effectiveness Value, was derived by computing the ratio between the process costs, as elucidated by the ABC analysis, and the aforementioned effectiveness rates adjusted by the volume of packages managed.
Budget Impact Analysis (BIA)
A BIA35,39 was developed to assess the hospitals’ financial sustainability and viability associated with the introduction of automated dispensing technologies. The primary objective was to estimate and project the economic impact related to the adoption and diffusion of new technologies into a healthcare system constrained by limited resources.
The BIA spanned a 36-month time horizon and was predicated on a representative medium-sized hospital encompassing 1209 beds, a Central Pharmacy, and an array of six departments.
The BIA design was dependent on the following information:
- The number of medications packages managed per day by the Central Pharmacy and the wards, being equal to 1864 and 169 per wards, respectively. This was ascertained from the aggregate data collected.
- The economic evaluation related to the drug management process, both in the Central Pharmacy and in the wards (as calculated at the point i) of the economic evaluation, related to the ABC analysis, carried out per Country of reference).
- The analysis also included the initial investment that must be covered by hospitals to install automated drug management systems, sourcing this expenditure from the mean market valuation of extant technologies.
- A total technological replacement rate was defined considering the possibility to shift completely from one Scenario to another.
The BIA analysis did not include the economic valorisation of the potential healthcare professionals’ labour hours released from logistics activities and reallocated to other activities. This aspect was valorised only as an organisational advantage for the healthcare facilities, as explained in the following methodological paragraph.
Organisational Impact
The aforementioned hypotheses were also implemented to perform the organisational analysis, aimed at quantifying the healthcare professionals time saving, segmented by their specific roles (technicians, pharmacists, and nurses) and respective national affiliations.
Quantitative data, collected during the questionnaire administration, were used to estimate key variable required for the organizational analysis, such as the dispensing times (evaluating minimum and maximum values, observed by professionals for the baseline scenario, also to conduct a scenario analysis) essential to perform the drug’s dispensing. This analysis aimed at identifying the potential efficiencies attainable upon embracing automated modalities.
For each country, the average volumes of drugs handled in one year declared, were used as the basis of allocation to determine the time savings derived from the implementation of ADD systems.
Scenario Analysis
A scenario analysis was carried out (adopting a comparative approach between the four different degrees of automation) observing the different results in case of various hospital size and specific beds saturation rates.
The three scenarios related to the hospital size consider a small size (584 drug packages moved per day in the central pharmacy and 53 drug packages moved every day in each ward), a medium size (1864 drug packages moved per day in the central pharmacy and 169 drug packages moved every day in each ward) and a large size (2336 drug packages moved per day in the central pharmacy and 212 drug packages moved every day in each ward) hospital.
The stratification of the results concerning the hospital’s bed saturation rate was analysed to assess potential economic variations, starting with a hospital’s bed saturation rate equal to 85% and then setting the range of this parameter from 80% to 99%.
Results
The Sample of the Healthcare Professionals
Of the 200 healthcare professionals invited to the study, a total of 129 respondents across six countries (Belgium, France, Germany, Italy, the Netherlands, and the UK) answered all the questions, yielding a response rate of 65%, which is considered acceptable according to the literature.40 The respondent professionals were firstly classified according to their nationality: 19.4% Belgian, 15.5% French, 32.6% Italian, 12.4% German, 16.3% English and 3.9% Dutch.
Respondents were analysed depending on their current use of automation (59.7% automation users and 40.3% potential automation users) and their professional role (35.6% pharmacists, 31.0% nurses, 19.4% other professionals, ie, biomedical engineers and IT specialists - and 14.0% decision makers).
Defining the Perceptions of the Healthcare Professionals
Table 4 depicts the healthcare professionals’ perceptions, comparing the four investigated scenarios.
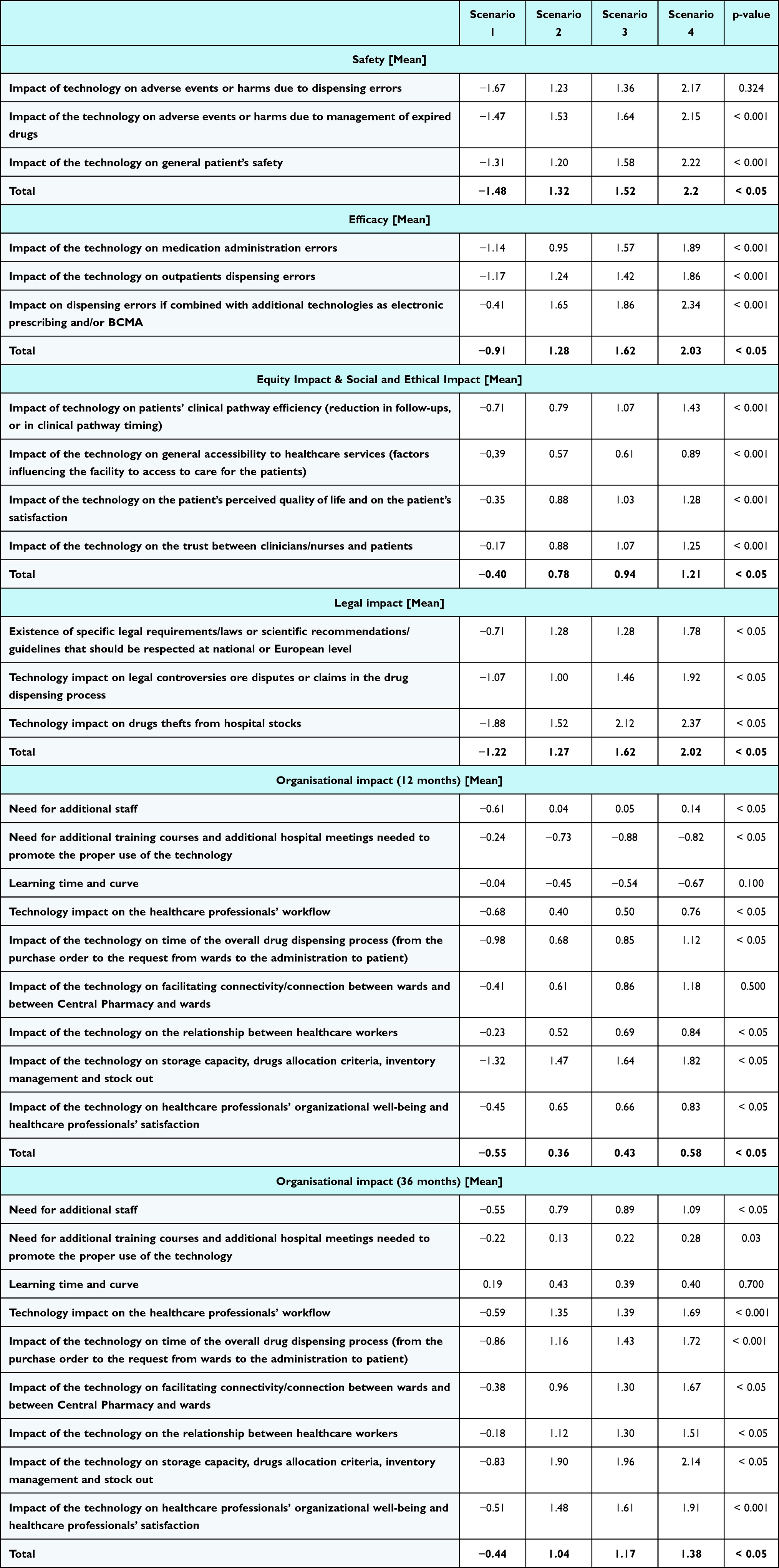 |
Table 4 Results for the Qualitative Domains, on a Scale Between −3 and +3 [Mean] |
Respondents reported that Scenario 4 allowed them to achieve better performance in terms of safety. Specifically, this scenario was associated with a marked decrease in adverse events resulting from dispensing errors or the management of expired drugs (+2.17 and +2.15 for the Scenario 4 versus −1.67 and −1.47 for the Scenario 1, p-value = 0.324 and p-value < 0.001). When analyzed on a country-specific basis, French and Dutch biomedical engineers and IT specialists provided the highest evaluations for the value of automation in terms of patient safety (respectively, +2.00 and +2.33, for the Scenario 4, p-value < 0.05). Conversely, Italian and Belgian professionals exhibited a more pronounced interest in the impact associated with the management of expired medications.
Data reveal that participants perceive that the integration of automated solutions and electronic prescribing (Scenario 4) could positively impact the effectiveness dimension with a statistically significant difference among Scenarios (−0.41, +1.65, +1.86, +2.34, respectively for Scenario 1, 2, 3 and 4, with a p-value < 0.001, comparing all the Scenarios). Among the surveyed groups, decision makers were the ones that most recognised the value of automated solutions (Scenarios 2, 3 and 4) in augmenting efficacy. Respondents from Germany and Italy, in particular, allocated superior ratings to the potential of automated technologies (Scenarios 2.3 and 4) to reduce dose error occurrence and MAE (Mean Absolute Error) compared to other countries (respectively +1.64 and +1.66 for Germany and Italy, +1.28 for Belgium, +0.87 for Netherlands, +1.36 for France, +1.23 for the UK, p-value < 0.05).
Considering the social aspects, automated solutions were seen to significantly bolster the quality of the patient journey (+0.67, +0.90, +1.37, respectively for Scenario 2, 3 and 4, p-value < 0.001). This was attributed to a reduction in error rates and an augmented trust between patients and healthcare professionals (+0.81, +0.95, +1.27, respectively for Scenario 2, 3 and 4, p-value < 0.001). Moreover, there was a consensus that automation has the potential to streamline the patient’s clinical pathway by curtailing inefficiencies and redundant follow-ups.
Differently from the other professional groups, nurses did not recognise the value of automation in terms of equity, social and ethical impact. Furthermore, English IT specialists recognised the value of automation in enhancing the patients’ clinical pathway (+2.50, for the Scenario 4) and in terms of trust between healthcare professionals and patients (+3.00, for the Scenario 4). Dutch biomedical engineers gave positive high score (+2.67, for the Scenario 4) to the impact of automation on the patient’s perceived quality of life (related to a different dispensing error risk occurrence) and on the patient’s satisfaction.
Considering the legal domain, respondents recognised the importance of automation in reducing thefts from hospital stock, especially in the wards (−1.88, +1.52, +2.12, +2.37, respectively for Scenario 1, 2, 3 and 4, p-value < 0.05). Respondents reported that automated technologies could also be useful to identify responsibilities in case of legal controversies in the drug dispensing process, especially from the decision makers perspectives (−1.07, +1.00, +1.46, +1.92, with a p-value < 0.05, respectively for Scenario 1, 2, 3 and 4). This aspect was valued by all the European decision makers involved in the study.
All the organisational aspects investigated with the HTA questionnaire presented statistically significant differences among scenarios (p-value < 0.05). Overall perceptions reported by respondents from the different countries reveal that automation could help hospitals improving the stock management processes, free up storage capacity and set up and implement drug allocation criteria (−1.32, +1.47, +1.64, +1.82, respectively for Scenario 1, 2, 3 and 4, p-value < 0.05). Participants also gave good scores to the potential of automated solutions, whether implemented with either a centralized or decentralized approach, to facilitate the connection between wards (+0.55, +0.86, +1.21, respectively for Scenarios 2, 3 and 4) and improve the collaboration between different healthcare professionals (+0.42, +0.57, +0.76, respectively for Scenarios 2, 3 and 4). When considering all three possibilities (centralised, decentralised and integrated approach), for France, Belgium, the Netherlands, and United Kingdom, the impact of automation was deemed to be better by users compared to non-users. German respondents appreciated the positive impact in terms of relationship between healthcare workers (+1.56, for the Scenario 4) and in terms of connection among wards, and between Central Pharmacy and wards (+1.63, for the Scenario 4), giving higher scores in comparison with the ones attributed to the healthcare professionals from other countries.
Economic Evaluation
The integration of automated technologies within both the Central Pharmacy and wards (as depicted in Scenario 4) may result in reduced process costs relative to alternative scenarios. This cost-effectiveness can be attributed to a decline in errors, a diminished count of expired drugs, and more efficient utilization of human resources. As delineated in Table 5, automated logistical solutions can yield considerable cost savings in drug administration and management, evidencing a cost reduction of over 37% when contrasting Scenario 4 with Scenario 1.
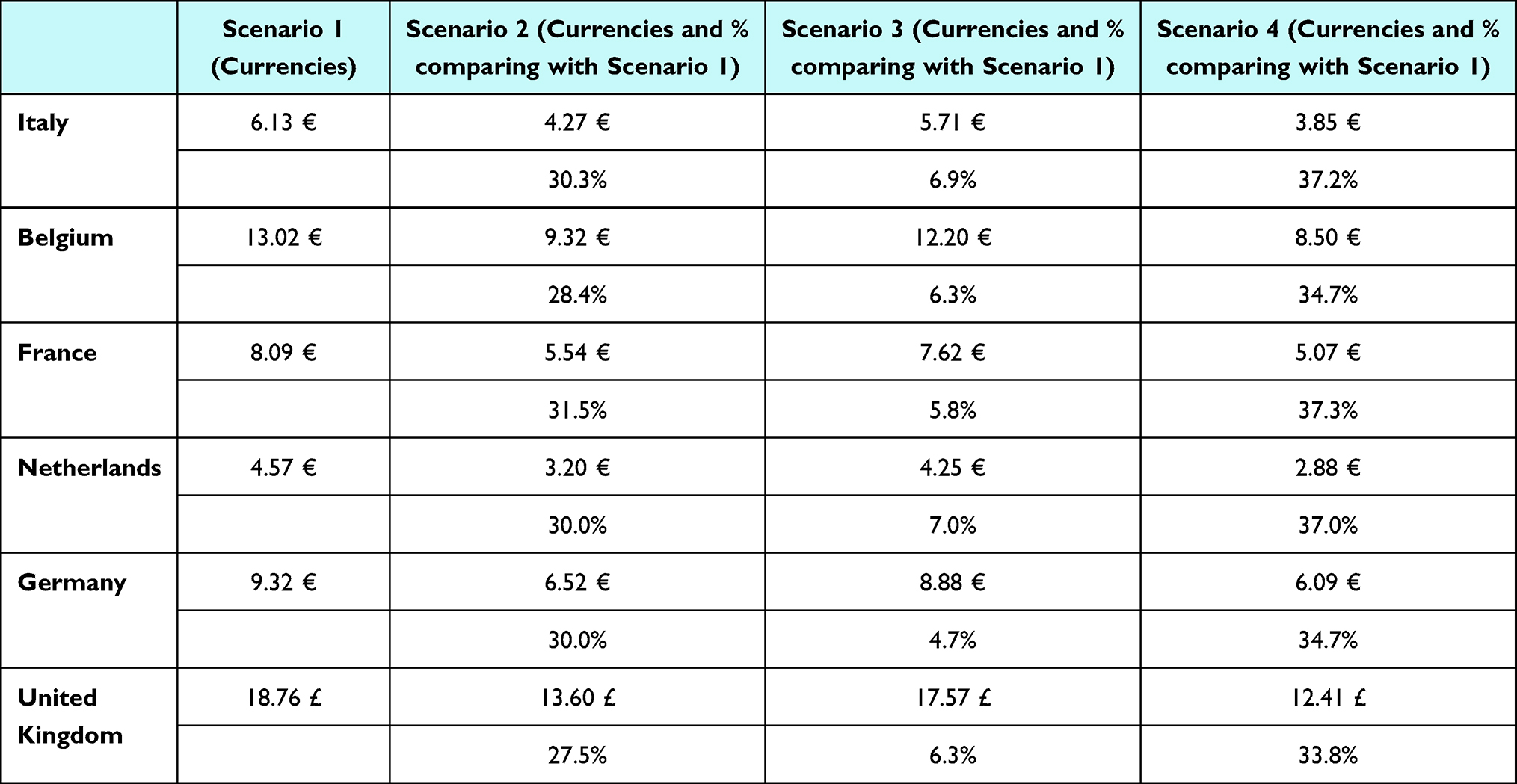 |
Table 5 Results from the ABC Analysis, Comparing All the Scenarios for All the Six Countries |
Human resource-associated expenditures witnessed a 30% improvement across all participating countries. This financial amelioration was primarily driven by the reduced number of healthcare professionals engaged in the drug management process following the introduction of automated dispensing systems.
Varying the parameter related to the bed saturation rate, the results are comparable among the six analysed countries, showing an average percentage variation equal to 19%, taking into consideration the process’s economic valorisation for Scenario 4. Considering the different sizes of a hospital, the Table below (Table 6) represents the variations occurring in the economic evaluation of the dispensing activities and process. For Scenario 4, increasing the hospital’s dimensions, there emerges an increase in the cost per in-patient, with a variation between +11.72% (for the English hospitals) and +33.09% (for the French ones).
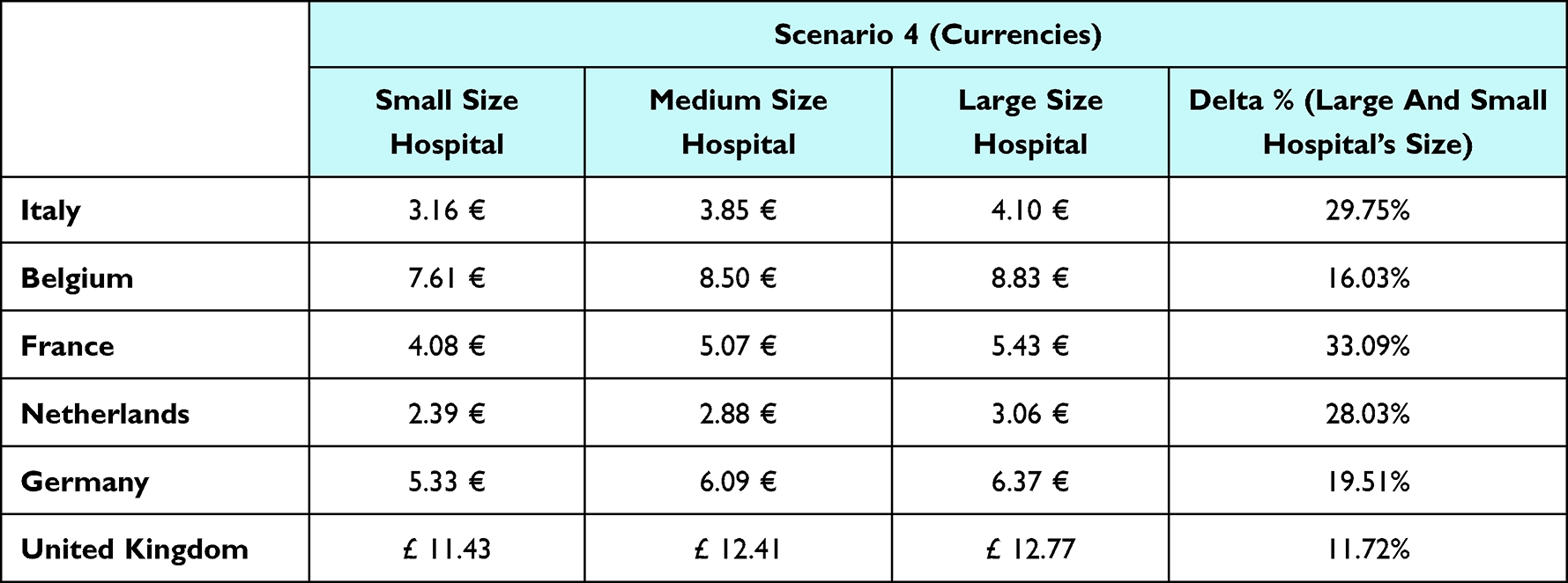 |
Table 6 Results from the Scenario 4’s ABC Analysis, Comparing a Small, a Medium and a Large Hospital |
Table 7 illustrates that the synergy of automated technologies within both the Central Pharmacy and wards (as presented in Scenario 4) emerges as the most advantageous solution for hospitals from a cost-effectiveness standpoint. Indeed, Scenario 4 has the potential to enhance the entire medication management process by delivering superior outcomes, particularly in the reduction of drug administration error rates.
 |
Table 7 Results from the Cost-Effectiveness Analysis (CEA), Comparing All the Scenarios [Currencies from Table 5 /Dispensing Errors’ Rates Derived from the Literature and Adjusted Considering the Total Number of Packages Moved] |
Over a three-year span, the integration of automated technologies in both the Central Pharmacy and wards (as indicated in Scenario 4) consistently yielded the most significant savings across all countries annually. This not only ensures but also buttresses the financial equilibrium of healthcare institutions that opt for the implementation of automated drug dispensing systems.
As elucidated in Table 8, the automation of drug management could culminate in total savings ranging from €259,757.39 (within the French context) to €588,253.17 (in the framework of the Belgian healthcare facilities).
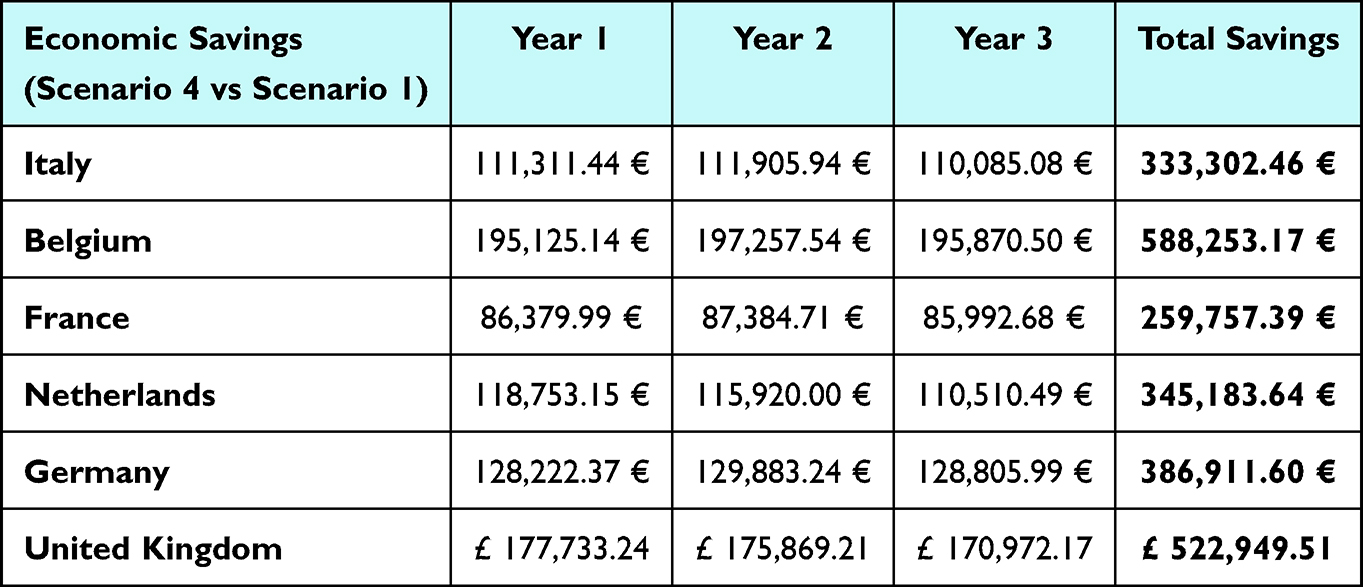 |
Table 8 Savings for Each Year, Comparing Scenario 4 with the Scenario 1, and the Total Savings |
Even considering the initial investment in the analysis, the assessment underscored the economic and financial benefits leaning towards the innovative solutions, epitomizing a significant cost reduction. By juxtaposing the cumulative savings over the three-year span and analysing the total savings for each scenario, Table 9 reports the proportional range of savings.
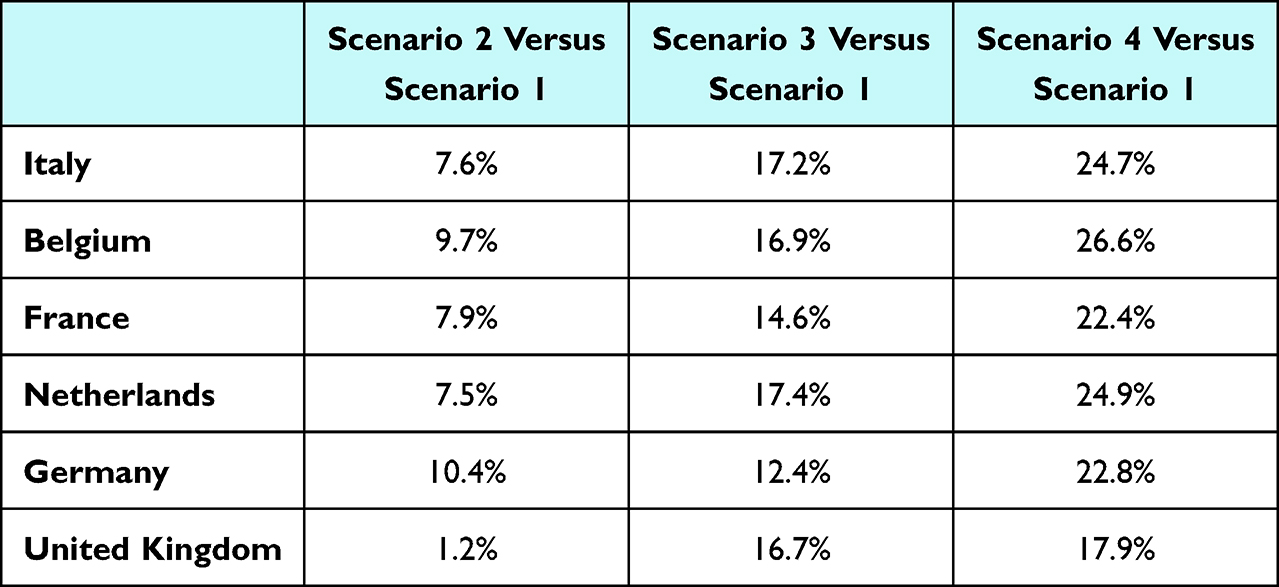 |
Table 9 Results from the Budget Impact Analysis, Comparing the Total Savings Obtained in the Three-Years’ Time Horizon in All the Scenarios with the Scenario 1 (%) |
The following table (Table 10) reports the total savings achieved for each country, comparing Scenario 4 and Scenario 1, with a reference time horizon of three years, and the percentage variations resulting from the sensitivity analysis. By increasing the hospital’s size, significant economic savings could be reached in the three years after the implementation of automated solutions, with the most important results in France (+85.2%) and Italy (+58.3%).
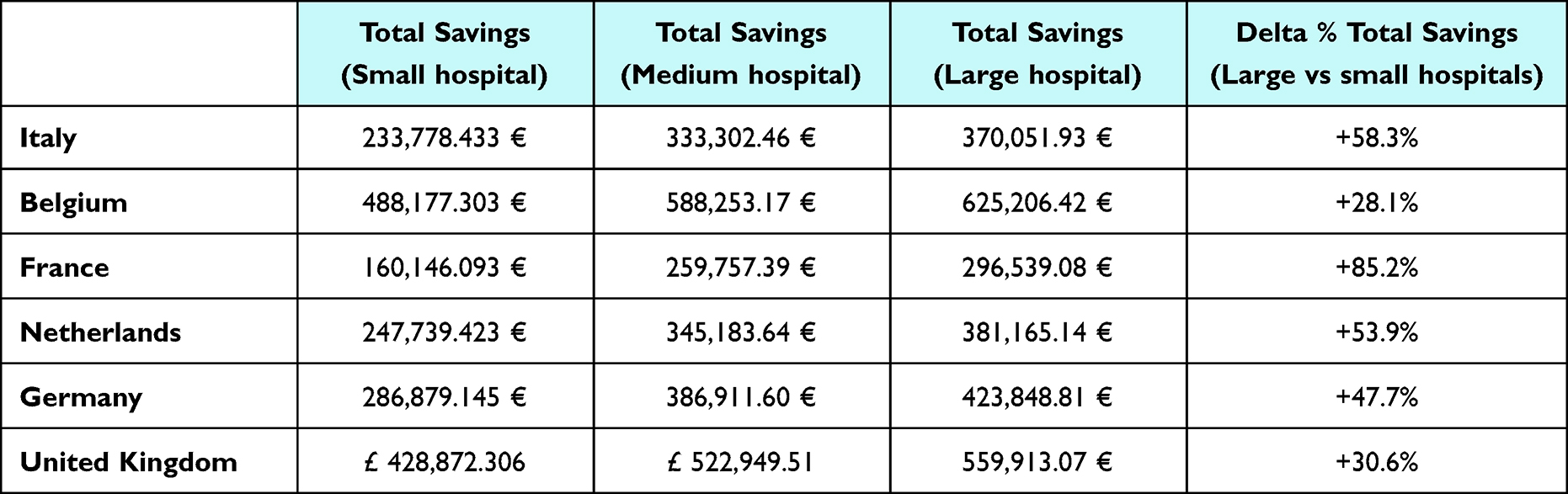 |
Table 10 Total Savings Reached in Three Years, Comparing Scenario 4 with the Scenario 1, Resulting from the Sensitivity Analysis |
Organizational Evaluation
From an organizational perspective, Table 11 presents the annual cumulative hours required to execute all the activities within the drug management process, broken down by the specific country.
 |
Table 11 Organisational Analysis, Presenting the Total Hours per Year Dedicated to Pharmaceutical Logistics Activities and the Savings Occurring in Each Scenario in Comparison with the Scenario 1 |
Under Scenario 4, the integration of automated systems in both the Central Pharmacy and wards culminates in the most pronounced reduction in hours that healthcare professionals allocate to drug dispensing activities. Belgian hospitals stand to realize the maximum of these savings, with a potential reduction of 33,435 hours annually.
Discussion
Summary of Key Findings and Interpretation
The HTA approach has been proven instrumental in evaluating diverse aspects related to the use of automated dispensing technologies, including economic, organisational, legal, equity, and social impacts.41 This study bridges a pivotal knowledge void and fosters a heightened consciousness around automated solutions and the related multidimensional impacts, considering that previous evidence was shown to be mostly related only to the safety profile of electronic prescription system42 and alert systems integrated within the pharmacy information.43
To overcome the traditional one-dimensional approach used by previous authors for the evaluation of computerised and automated solutions,44 the proposed integration of economic and organizational empirical evidence and the collection of healthcare professionals’ perceptions enrich available knowledge around the complex decision-making processes and the need to adapt the results considering different local perspectives and priorities. This multifaceted approach transcends traditional national-centric paradigms,13,45 and shows itself to be suitable as required by the new EU HTA regulation, particularly focusing on the non-clinical domains, and the related need for adaptation within the local contexts.46 Consequently, it facilitates a holistic evaluation of the inherent merits and potential pitfalls of automated dispensing solutions, shifting the lens beyond mere clinical advantages and outcomes.47
This study corroborated previous evidence suggesting that the adoption of automated technologies within the hospital setting could significantly bolster drug management performance,48,49 fulfilling high-volume prescriptions safely and efficiently. Findings show that potential and actual benefits resulting from the implementation of innovative logistics technologies were acknowledged across the three scenarios featuring automated solutions in all examined domains.
From an economic perspective, Scenario 4 demonstrated the most substantial savings over a 36-month period: this also mirrors the effectiveness perception in line with the findings presented by some authors.50 Beyond the cost analysis of the drug management process, the derived cost-effectiveness values for all examined Scenarios provide decision-makers with a framework to discern interventions offering optimal value for investment. Despite the benefits highlighted in existing literature4,51 suggests that changes in the work routine following the introduction of ADD technologies could be managed by organising regular meetings with the professionals involved in the drug management and dispensing process. This sentiment resonated in our findings, where professionals underscored the necessity of systematic meetings and training sessions, amounting to a peak of 14 hours in the Belgian context. Such routine institutional dialogues were deemed pivotal across all national contexts surveyed, with a particularly high frequency noted among UK healthcare professionals. These meetings serve as conduits to disseminate insights, amplify cognizance of automated solutions, and recalibrate human resources strategies during the early phases of deployment.51
Shifting the focus to the perceptions of healthcare professionals, Scenario 4 registered the highest value across all evaluated dimensions, spanning safety (+2.2), efficacy (+2.3) and legal aspects (+2.02). Furthermore, the findings revealed a wide range of viewpoints due to the use of a panel of experts with different professional backgrounds. For instance, executive-level personnel and hospital administrators directed their attention differently as compared to end-users like technicians or pharmacists. The former cohort was primarily concerned with deciphering implementation costs and required investments, placing premium emphasis on both the economic impact and organizational implications linked to the embrace of automated solutions. Conversely, the latter group exhibited greater interest in the nuanced technical performance of the dispensing automation within the ambit of hospital logistical operations.
Study Contributions
Many are the possible contributions of this study, spanning both theoretical constructs and practical applications, especially from management and organizational standpoints. Academically, the findings underscore the pressing necessity for robust effectiveness data across the diverse technologies and scenarios examined, as well as the availability of evidence being useful to understand the level of local adaptation and the variability of the results according to the territorial contexts of reference, and the hospitals dimensions. Practically, they elucidate for practitioners and hospital managers the rationale behind the adoption of specific technologies and the subsequent evolution of drug management paradigms, in the light of specific contextual factors or local peculiarities. Moreover, these insights could guide the delineation of judicious investment strategies within the hospital and clinical practice settings, tailored for the deployment of ADD systems in both centralized and decentralized scenarios.
Of significant note is the emphasis on healthcare professionals’ perceptions. These perceptions can pave the way for discerning the factors that might either facilitate or hinder the seamless adoption and utilization of ADD systems. A qualitative examination of ADD systems can shed light on the lived experiences and viewpoints of healthcare services providers. Such understanding is invaluable, as it not only informs strategies that optimize technology utilization and enhance patient safety and outcomes but also offers insights into the professional landscape. Additionally, a deeper comprehension of professionals’ perceptions could empower hospital executives and leadership to craft optimal training modules and continuous support mechanisms during the transformative phase of technology adoption.
The principal strength of this study is anchored in its utilization of real-world data drawn from hospitals across six different European countries, complemented by the engagement of a panel of healthcare professionals. Such an approach ensures that the derived results are pertinent and generalizable across the participating European nations, spanning qualitative assessment as well as economic and organizational evaluations, thus overcoming the evidence gaps present in the extant literature.
Limitations
The methodologies employed to bolster economic and organizational sustainability are adaptable to other hospitals embracing similar technologies. One merely needs to adjust the input parameters—such as the number of beds, technicians, pharmacists, and moved packages—to resonate with the specific contextual data on hand. This fact could represent a limitation of the study. Another limitation could be the sample size: in certain countries, the more restricted respondent pool might have nuanced the outcomes. In addition, a more balanced sample between the different healthcare professional roles should be encouraged. Additionally, the study overlooked the delineation of drivers that might amplify the propensity to employ automated dispensing solutions. Therefore, a deeper dive into the organizational repercussions of automation within the hospital environment is warranted, especially considering the technological acceptability from the vantage point of end users. Exploring external factors, such as nationality or professional background, might illuminate their influence on automation acceptability and the ensuing intention to use.
Moreover, another limitation of the study could be mentioned in the sensitivity analysis. As previously described, only a scenario analysis was performed, varying the results only considering the characteristics of the hospitals in the countries involved; in particular, the number of beds of the healthcare facilities and the bed saturation rates were used to define the robustness of the results achieved.
Conclusions
This study pioneers an effort to quantify the comprehensive implications associated with the deployment of automated drug dispensing systems in the hospital environment, transcending the traditional boundaries of safety and efficacy discussions. The evaluated technologies have showcased potential in enhancing workflow efficiency, curtailing healthcare expenditures, reducing manual tasks, and optimizing resources allocation.
Nonetheless, the analysis also underscored several challenges, chief among them being the imperative for robust staff training. Additionally, the initial outlay and subsequent maintenance costs of these systems must be judiciously balanced against their projected long-term benefits and potential cost savings. In this context, the delineated HTA approach, underpinned by the integration of literature evidence and insights drawn from healthcare professionals via qualitative methods, can significantly inform decisions related to the adoption of automated drug dispensing technologies across various organizational levels.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Ethics Statement
The study was approved by Research Ethics Committee of University Carlo Cattaneo - LIUC (protocol number #R05-23, dated February 24th, 2023).
Acknowledgments
The authors would like to thank the healthcare professionals involved in the data collection.
Funding
YJ is funded by the National Institute for Health and Care Research Applied Research Collaboration Northwest London. The views expressed in this publication are those of the authors and not necessarily those of the National Institute for Health Research or the Department of Health and Social Care. EG, EF, FA, GA, DB, LF were funded by BD, being supported with research grants or fee for educational activities, but this article was conceived, written and internally reviewed, independently.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lasater KB, Aiken LH, Sloane DM, et al. Chronic hospital nurse understaffing meets COVID-19: an observational study. BMJ Qual Saf. 2021;30(8):639–647. doi:10.1136/bmjqs-2020-011512
2. Beard RJ, Smith P. Integrated electronic prescribing and robotic dispensing: a case study. Springerplus. 2013;2(1):295. doi:10.1186/2193-1801-2-295
3. Berdot S, Savoldelli V, Zaugg V, et al. Return on investment after implementation of a centralised automated storage system in a hospital pharmacy. J Pharm Pharmacol. 2016;4:526–532.
4. Franklin BD, O’Grady K, Voncina L, Popoola J, Jacklin A. An evaluation of two automated dispensing machines in UK hospital pharmacy. Int J Pharm Pract. 2008; 16(1):47–53.
5. Anacleto TA, Perini E, Rosa MB, et al. Medication errors and drug-dispensing systems in a hospital pharmacy. Clinics. 2005;60(4):325–332. doi:10.1590/S1807-59322005000400011
6. Ahtiainen HK, Kallio MM, Airaksinen M, Holmström AR. Safety, time and cost evaluation of automated and semi-automated drug distribution systems in hospitals: a systematic review. Eur J Hosp Pharm. 2020;27(5):253–262. doi:10.1136/ejhpharm-2018-001791
7. Batson S, Mitchell SA, Lau D, et al. Automated compounding technology and workflow solutions for the preparation of chemotherapy: a systematic review. Eur J Hosp Pharm. 2020;27(6):330–336. doi:10.1136/ejhpharm-2019-001948
8. Hernandez F, Majoul E, Montes-Palacios C, et al. An observational study of the impact of a computerized physician order entry system on the rate of medication errors in an orthopaedic surgery unit. PLoS One. 2015;10(7):e0134101. doi:10.1371/journal.pone.0134101
9. Pazour JA, Meller RD. A multiple-drawer medication layout problem in automated dispensing cabinets. Health Care Manag Sci. 2012;15(4):339–354. doi:10.1007/s10729-012-9197-8
10. Brinklow NA. A report assessing the impact of an Automated Dispensing System (ADS) at Kings College Hospital NHS Trust 2016.
11. Borel JM, Rascati KL. Effected of an automated, nursing unit-based drug-dispensing device on medication errors. AM J Health-Syst Pharm. 1995;52(17):1878–1879. doi:10.1093/ajhp/52.17.1875
12. Berdot S, Korb-Savoldelli V, Jaccoulet E, et al. Centralised automated-dispensing system in a French teaching hospital: return on investment and quality improvement. Int J Qual Health Care. 2019;31(3):219–224. doi:10.1093/intqhc/mzy152
13. Cousein E, Mareville J, Lerooy A, et al. Effect of automated drug distribution systems on medication error rates in a short-stay geriatric unit. J Eval Clin Pract. 2014;20(5):678–684. doi:10.1111/jep.12202
14. Tsao NW, Lo C, Babich M, et al. Decentralized automated dispensing devices: systematic review of clinical and economic impacts in hospitals. Canadian J Hosp Pharm. 2014;67(2):138–148. doi:10.4212/cjhp.v67i2.1343
15. Holdsworth MT, Fichtl RE, Behta M, et al. Overcoming resistance to pharmacy automation: a case study of implementing medication carousels in a hospital pharmacy. Am J Health Syst Pharm. 2008;65(1):65. doi:10.2146/ajhp070087
16. Garagiola E, Foglia E, Asperti F, et al. Automated drugs dispensing systems in hospital pharmacies and wards: a systematic literature review. Biomed J Sci Tech Res. 2023;53(5):2023. BJSTR. MS.ID.008454.
17. Moroshek JG. Improving outpatient primary medication adherence with physician guided, automated dispensing. Clinicoecon Outcomes Res. 2017;9:59–63. doi:10.2147/CEOR.S114416
18. Patel PC, Van der Have RP. Enhancing innovation performance through exploiting complementarity in search breadth and depth. Front Entrepreneurship Res. 2010;30(9):1.
19. Wiffen P. Value or cost: looking for the wider perspective. Eur J Hosp Pharm. 2017;24(2):73. doi:10.1136/ejhpharm-2017-001213
20. Moorthy S, Polley DE. Technological knowledge breadth and depth: performance impacts. J Knowledge Manag. 2010;14(3):359–377. doi:10.1108/13673271011050102
21. Banta D, Jonsson E. History of HTA: introduction. Int J Tech Assess Health Care. 2009;25(S1):1–6. doi:10.1017/S0266462309090321
22. Drummond M, Barbieri M, Cook J, et al. Transferability of economic evaluations across jurisdictions: ISPOR good research practices task force report. Value Health. 2009;12(4):409–418. doi:10.1111/j.1524-4733.2008.00489.x
23. Creswell J, Plano Clark V. Designing and Conducting Mixed Methods Research. Thousand Oaks, CA: Sage; 2007.
24. Johnson BR, Onwuegbuzie AJ, Turner LA. Toward a definition of mixed methods research. J Mixed Methods Res. 2007;1(2):112–133. doi:10.1177/1558689806298224
25. Acheampong F, Anto BP, Koffuor GA. Medication safety strategies in hospitals–a systematic review. Int J Risk Safety Med. 2014;26(3):117–131. doi:10.3233/JRS-140623
26. Hawkins B. ASHP guidelines on the safe use of automated dispensing devices. Am J Health Syst Pharm. 2010;67:483–490.
27. Gray JP, Ludwig B, Temple J, et al. Comparison of a hybrid medication distribution system to simulated decentralised distribution models. Am J Health Syst Pharm. 2013;70(15):1322–1335. doi:10.2146/ajhp120512
28. Sampietro-Colom L, Lach K, Escolar Haro I, et al. THE AdHopHTA HANDBOOK. 2015;222.
29. Olsen WK, Haralambos M, Holborn M, Ed.. Triangulation in Social Research: Qualitative and Quantitative Methods Can Really Be Mixed. In Developments in Sociology Causeway Press Ltd; 2004.
30. Rahi S. Research design and methods: a systematic review of research paradigms, sampling issues and instruments development. Int J Economics Manag Sci. 2017;6(2):1–5. doi:10.4172/2162-6359.1000403
31. Kock F, Adiyukh Berbekova AGA, Assaf AG. Understanding and managing the threat of common method bias: detection, prevention and control. Tourism Manage. 2021;86(104330):ISSN0261–5177. doi:10.1016/j.tourman.2021.104330
32. EUNetHTA. The HTA Core Model, Version 3.0. Available online: https://www.eunethta.eu/wp-content/uploads/2018/03/HTACoreModel3.0-1.pdf.
33. Vanni F, Foglia E, Pennestrì F, Ferrario L, Banfi G. Introducing enhanced recovery after surgery in a high-volume orthopaedic hospital: a health technology assessment. BMC Health Serv Res. 2020;20(1):1–15. doi:10.1186/s12913-020-05634-3
34. Mitton C, Dionne F, Damji R, Campbell D, Bryan S. Difficult decisions in times of constraint: criteria based resource allocation in the Vancouver Coastal Health Authority. BMC Health Serv Res. 2011;11(1):169. doi:10.1186/1472-6963-11-169
35. Cooper R, Kaplan RS. Activity-based systems: measuring the costs of resource usage. Accounting Horizons. 1992;September:1–13.
36. Russell LB, Gold MR, Siegel JE, Daniels N, Weinstein MC. The role of cost-effectiveness analysis in health and medicine. JAMA. 1996;276(14):1172–1177. doi:10.1001/jama.1996.03540140060028
37. Mauskopf JA, Sullivan SD, Annemans L, et al. Principles of good practice for budget impact analysis: report of the ISPOR task force on good research practices--budget impact analysis. Value Health. 2007;10(5):336–347. doi:10.1111/j.1524-4733.2007.00187.x
38. Job Pricing Observatory. JP Salary. Outlook; 2023.
39. Sullivan SD, Mauskopf JA, Augustovski F, et al. Budget impact analysis-principles of good practice: report of the ISPOR 2012 budget impact analysis good practice II task force. Value Health. 2014;17(1):5–14. doi:10.1016/j.jval.2013.08.2291
40. Johnson TP, Owens L Survey response rate reporting in the professional literature. In:
41. Drummond MF, Schwartz JS, Jönsson B, et al. Key principles for the improved conduct of health technology assessments for resource allocation decisions. Int J Technol Assess Health Care. 2008;24(3):244–258. doi:10.1017/S0266462308080343 discussion 362-8.
42. Jeffries M, Keers RN, Belither H, et al. Understanding the implementation, impact and sustainable use of an electronic pharmacy referral service at hospital discharge: a qualitative evaluation from a sociotechnical perspective. PLoS One. 2021;16(12):e0261153. doi:10.1371/journal.pone.0261153
43. Campmans Z, Van Rhijn A, Dull RM, Santen-Reestman J, Taxis K, Borgsteede SD. Preventing dispensing errors by alerting for drug confusions in the pharmacy information system—A survey of users. PLoS One. 2018;13(5):e0197469. doi:10.1371/journal.pone.0197469
44. Bano T, Haq N, Nasim A, et al. Evaluation of medication errors in patients with kidney diseases in Quetta, Pakistan. PLoS One. 2023;18(8):e0289148. doi:10.1371/journal.pone.0289148
45. Vermeulen KM, van Doormaal JE, Zaal RJ, et al. Cost-effectiveness of an electronic medication ordering system (CPOE/CDSS) in hospitalised patients. Int J Med Inform. 2014;83(8):572–580. doi:10.1016/j.ijmedinf.2014.05.003
46. Regulation (EU). 2021/2282 of the European Parliament and of the Council of 15 December 2021 on health technology assessment and amending Directive 2011/24/EU [2021] OJ L 458/1; 2021. Available from: https://eur-lex.europa.eu/eli/reg/2021/2282/oj.
47. Schvvarz HO, Brodowy BA. Implementation and evaluation of an automated dispensing system. Am J Health Syst Pharm. 1995;52(8):823–828. doi:10.1093/ajhp/52.8.823
48. Jessurun JG, Hunfeld NGM, Van Rosmalen J, et al. Effect of automated unit dose dispensing with barcode scanning on medication administration errors: an uncontrolled before-and-after study. Int J Qual Health Care. 2011;33(4): mzab142.
49. Berdot S, Gillaizeau F, Caruba T, et al. Drug administration errors in hospital inpatients: a systematic review. PLoS One. 2013;8(6):e68856. doi:10.1371/journal.pone.0068856
50. Risør BW, Lisby M, Sørensen J. Cost-effectiveness analysis of an automated medication system implemented in a Danish hospital setting. Value Health. 2017;20(7):886–893.
51. Pedersen CA, Schneider PJ, Scheckelhoff DJ. ASHP national survey of pharmacy practice in hospital settings: dispensing and administration—2014. Am J Health Syst Pharm. 2015;72(13):1119–1137. doi:10.2146/ajhp150032
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.