")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 17
Autologous Nanofat Injection Combined with Fractional CO2 Laser in the Treatment of Atrophic Acne Scars
Authors Rageh MA , Ibrahim SMA , Abdallah N, Tawfik AA
Received 8 January 2024
Accepted for publication 16 March 2024
Published 20 March 2024 Volume 2024:17 Pages 697—705
DOI https://doi.org/10.2147/CCID.S454514
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Rungsima Wanitphakdeedecha
Mahmoud A Rageh,1 Shady Mahmoud Attia Ibrahim,1 Noha Abdallah,2 Abeer Attia Tawfik2
1Department of Dermatology, Faculty of Medicine, Al-Azhar University, Cairo, Egypt; 2Department of Medical Applications of Laser, National Institute of Laser Enhanced Sciences, Cairo University, Giza, Egypt
Correspondence: Mahmoud A Rageh, Department of Dermatology, Faculty of Medicine, Al-Azhar University, Al-Darrasah, Cairo, 11633, Egypt, Email [email protected]
Background: Atrophic acne scarring is a widely prevalent condition and one of the most distressing complications of acne vulgaris. Numerous options with variable outcomes are available for the treatment of acne scarring. Laser is considered a first‐line therapy for acne scars, and recently there has been a growing interest in using stem cells and their derivatives for treating acne scars. In addition, combined therapeutic modalities often achieve more satisfactory results than a single treatment.
Objective: We tried to evaluate the role of nanofat and fractional CO2 laser as a combined treatment approach for atrophic acne scarring.
Methods: Twenty-five patients with atrophic acne scarring were enrolled. They received a single session of intradermal nanofat injection, at different points 1 cm apart, for acne scars. Two weeks later, they were treated with three sessions of fractional CO2 laser at monthly intervals. Patients were evaluated three months after the last session using the quantitative Goodman and Baron scoring system. Pain, side effects, and patients’ satisfaction were also evaluated.
Results: There were two males and 23 females with a mean age of 25.96 years. Their skin type ranged between Fitzpatrick skin type III, IV, and V. Boxcar scars were the most common scar type in 13 patients (52%). After treatment, there was a significant reduction (p < 0.05) in the quantitative Goodman and Baron scores. The improvement was more evident in rolling scars. Seven patients reported significant improvement, and 12 reported marked improvement.
Conclusion: This study showed that combining nanofat and fractional CO2 laser is a safe and effective treatment modality for atrophic acne scars.
Keywords: acne scars, fractional laser, fat grafting, nanofat
Introduction
Acne vulgaris is a pleomorphic disorder of the pilosebaceous unit. It is the eighth most common disease globally, affecting over 0.5 billion people, and has a prevalence of over 90% in the adolescent community.1 Acne pathogenesis is attributed to four key factors: excess sebum production, hyperproliferation of Cutibacterium acnes bacteria, hyperkeratinization of the pilosebaceous follicles, and inflammatory mechanisms.2
Inflammatory acne lesions may result in permanent scars, the severity of which may depend on delays in acne treatment.3 Atrophic scarring represents about 75% of acne scars and is subdivided into icepick, rolling, and boxcar scars.4
Acne scars has been found to adversely affect the social life, self-esteem, and body image of affected individuals, and is often co-morbid with psychological disorders including depression and anxiety.5
Currently, there is no standard treatment for atrophic acne scars. Various treatment approaches have been used to improve the appearance of acne scars, with varying degrees of success.6 Traditional treatment methods include skin abrasion, chemical peeling, scarring drill excision, tissue filling, microneedling, scarring drill elevation, thread lifting, and photodynamic therapy, while emerging therapies such as mesenchymal stem cells (MSCs) and their derivatives are also available.7
Laser is a first‐line therapy for acne scars. Fractional CO2 laser improves the appearance of skin by removing portions of the epidermis and dermis as well as heating microthermal zones extending from the epidermis to the mid- or deep dermis. Parts of the epidermis and dermis are replaced by wound-healing responses after the injury, replacing the damaged tissue with healthy, new foci of the epidermis and dermis.8,9 However, the ensuing downtime, the potential for protracted erythema, and, occasionally, hyperpigmentation constrain fractional CO2 laser.10 Therefore, through expediting tissue regeneration and wound healing, an adjuvant use of other modalities, such as nanofat, may provide synergistic advantages and reduce side effects.11
In recent years, many studies have also used stem cells and their derivatives for treating acne scars, among which MSCs and their derivatives are the most commonly used.7 Nanofat was first described by Tonnard et al in 2013. Its capacity for regeneration is primarily attributable to the abundant adipose tissue-derived stem cells (ADSCs) and stromal vascular fraction (SVF) cells that promote blood vessel formation and the secretion of growth factors that impede fibrosis and inflammation, speed up wound healing, and improve skin texture.12,13
Since most monotherapeutic approaches for acne scars provide insufficient effects, tailored combined therapy utilizing multiple treatments is necessary. As a result, the aim of this study was to assess the safety and efficacy of nanofat as an adjuvant therapy to fractional CO2 laser for atrophic acne scars.
Materials and Methods
This study included 25 patients with atrophic acne scars. The study was done in accordance with the Declaration of Helsinki after approval of the ethical committee (Approval No. Der-Med.22.Research.0000216). All patients signed informed consent before the procedures.
All patients in this study were subjected to complete history taking, thorough general and dermatological examinations, and routine laboratory investigations. Acne scars were graded through Goodman and Baron’s quantitative global grading system.14
Exclusion criteria included: Age <18 or >40 years, isotretinoin therapy or other treatment procedures for acne scars within six months prior to the study, patients with hematological or autoimmune diseases, keloid formation tendency, pregnancy, and lactation.
Treatment Protocol
All patients received a single session of nanofat injection for acne scars. Two weeks later, they were treated with three sessions of fractional CO2 laser at monthly intervals. The final evaluation was done three months after the last session.
Nanofat Preparation and Injection
Fat was harvested mainly from the abdomen, followed by the thighs. Infiltration of Klein’s15 tumescent anesthesia was done followed by fat aspiration using a Sorensen cannula (Tulip Medical Inc., San Diego, CA) mounted on a 10-mL Luer-Lock syringe. Centrifugation of the harvested fat at 3000 rpm for three minutes was performed to filter the fat from residual blood and tumescent fluid.
Nanofat preparation was done using 2.4, 1.4, and 1.2 mm Luer-to-Luer Tulip connectors via 30 mechanical passes between two syringes through each connector, respectively, followed by a single pass through 400 µm filter within Tulip NanoTransfer device. Nanofat was then transferred to sterile 28 G syringes for injection.
In a single session, about two mL of nanofat was injected intradermally at different points 1 cm apart till a yellowish discoloration of the skin appeared.
Laser Treatment
Local anesthetic cream was applied for one hour. Then, the scars were treated with one pass of fractional CO2 laser (SmartXide Punto, Deka, Florence, Italy) using the following parameters: 15 W power, 800 µm spacing, 600 µs dwell time, and stack two.
Postprocedural Care
Following fat harvesting, all patients were prescribed oral antibiotic for one week. After the procedures, the treated sites were covered by ice packs. Prolonged sun exposure was avoided, and sunscreen was applied daily till the end of the follow-up period.
Outcome Assessment
The therapeutic outcome was assessed three months after the last treatment session based on the quantitative Goodman and Baron system scores. To minimize potential bias, the assessment was made by two non-treating dermatologists.
Side Effects
Patients were asked to categorize the laser session-associated pain as mild, moderate, or severe. The subjective downtime (caused by redness, swelling, pigmentation, or crust) following each laser treatment was also documented.
In addition, side effects related to fat harvesting (such as bruising, pigmentation, or infection) were assessed one week after the session and at the final evaluation. Pain associated with fat harvesting and injection was also evaluated using a numerical 0 to 10 scale (0 = no pain, 1–4 = mild pain, 5–7 = moderate pain, and 8–10 = severe pain.16
Patient Satisfaction
Three months after the last treatment session, the authors used a quartile scale (slight improvement <25%, moderate improvement 25%-49%, significant improvement 50%-74%, and marked improvement ≥75%) and asked the patients to evaluate their improvement.
Statistical Analysis
The Statistical Program for Social Science (SPSS) version 25 was used to examine the data. A proper analysis was done for every variable, depending on the collected data type.
Results
The study comprised 25 patients with atrophic acne scars, 23 (92%) females and two (8%) males (14 had Fitzpatrick skin type III, nine had type IV, and two had type V). They ranged in age from 19 to 36 years (25.96 ± 4.85 years). The scars’ duration ranged from three to 17 years (7.16 ± 3.86 years). Boxcar scars were the most common scar type in 13 patients (52%), followed by rolling scars in nine (36%) and icepick scars in three (12%) (Table 1).
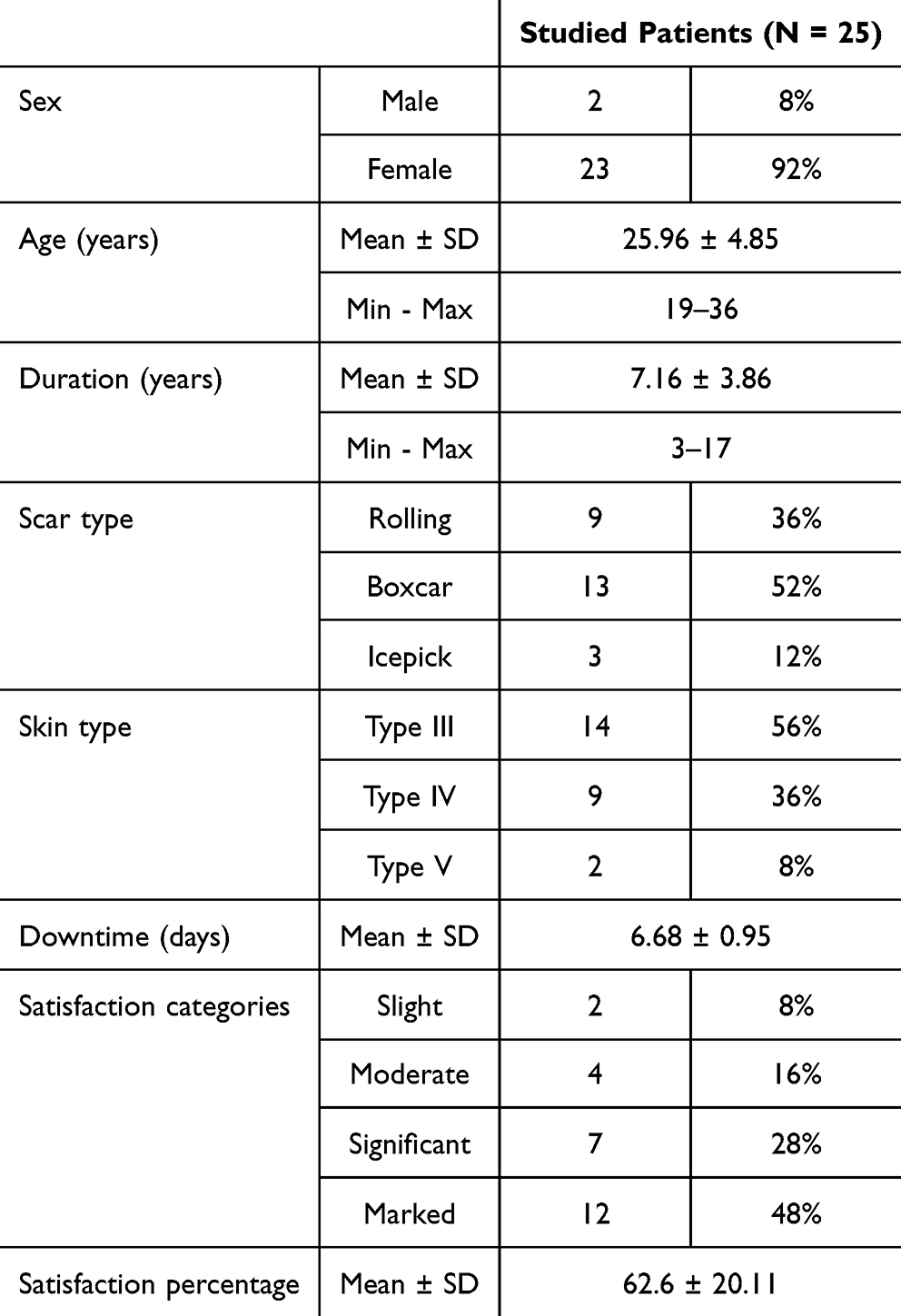 |
Table 1 Description of Clinical Data, Reported Downtime, and Satisfaction Categories in All Studied Patients |
All patients reported mild pain during the laser sessions. Erythema, edema, and crust formation were reported by all patients, which faded away within 6.68 ± 0.95 days after the session (Table 1). No hyperpigmentation at the treated sites was reported in any case.
As regards patient satisfaction, two patients (8%) reported slight improvement, four (16%) reported moderate improvement, seven (28%) reported significant improvement, and 12 (48%) reported marked improvement (Table 1).
After treatment, there was a statistically significant reduction (p <0.05) in the quantitative Goodman and Baron scores (Table 2 and Figures 1–3). Using Pearson coefficient, there was a positive correlation between the age and duration of acne scars and the Goodman scores, indicating that the scars were more severe at older ages and for more extended periods.
 |
Table 2 Comparison between the Scores before and after Treatment on the Quantitative Goodman and Baron Scale |
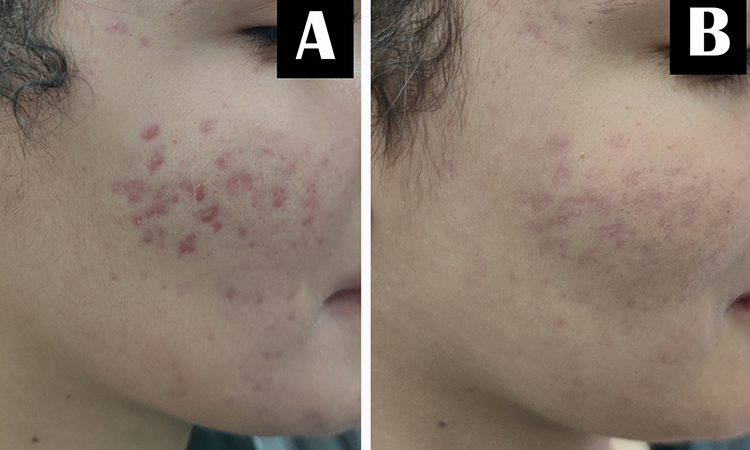 |
Figure 1 A 24-year-old female patient with atrophic acne scars. (A) Before treatment. (B) Marked improvement after treatment with fractional CO2 laser and nanofat injection. |
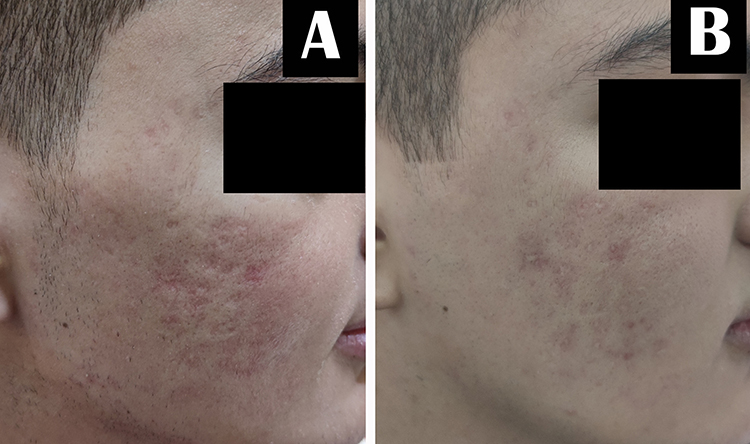 |
Figure 2 A 20-year-old male patient with atrophic acne scars. (A) Before treatment. (B) Significant improvement after treatment with fractional CO2 laser and nanofat injection. |
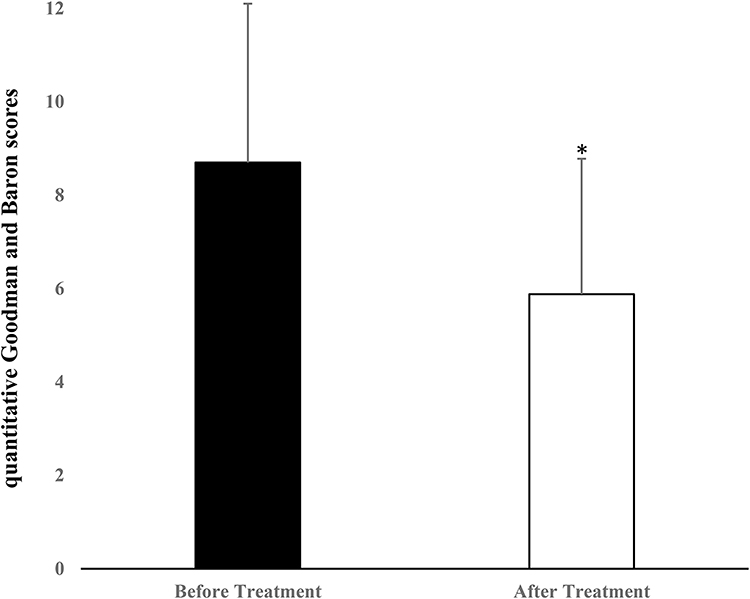 |
Figure 3 Difference between quantitative Goodman and Baron scores before and after treatment (*Denotes p-value <0.05 which is considered statistically significant). |
The quantitative Goodman and Baron scores revealed that rolling scars improved the most, followed by boxcar and icepick scars (Table 3).
 |
Table 3 Description of the Studied Scores Regarding the Atrophic Scar Type |
Regarding complications related to the fat harvesting site, there were complications in ten patients (40%). There was bruising in five patients (20%), erythema in three (12%), edema in one (4%), and hyperpigmentation in one (4%).
Regarding pain scores related to fat harvesting and nanofat injection, the mean pain score in all studied patients was 3.44 ± 1.96, with a minimum score of 0 and a maximum score of eight. There were 17 patients (68%) with mild pain, five patients (20%) with moderate pain, and one patient (4%) with severe pain, while there were two patients (8%) with no pain.
Discussion
Given the prevalence of acne scarring and the dearth of effective clinical solutions, treating acne scarring continues to be a novel area of research. Developing therapeutic approaches that can be both efficient and safe continues to be a key achievement in cosmetic dermatology.17
Acne scarring is caused by altered wound healing responses to pilosebaceous unit inflammation. Prolonged inflammation leads to dermal damage, mainly in the form of collagen loss, and this subsequently causes persistent skin texture alterations and atrophic scarring.18,19 Acne scars can have a significant impact not only on patients’ aesthetic appearance but also on their emotional well-being as well as their quality of life.20
This study shows that fractional CO2 laser combined with the injection of nanofat enhanced the clinical improvement of acne scars. Only one session of nanofat injection was performed to assess the maximum benefits gained through the minimum number of sessions. In addition, although liposuction is a relatively simple and safe procedure for harvesting adipose tissues, some patients may still consider it an invasive surgical intervention. Nanofat was injected two weeks before laser sessions to allow nanofat to settle within the targeted scars, avoid being degraded by the thermal laser energy, and subsequently augment tissue regeneration stimulated by laser. After treatment, the quantitative Goodman and Baron scores showed a statistically significant improvement.
Utilizing thermal energy delivered by monochromatic light, laser resurfacing enables dermal fibroblasts to replenish depleted collagen and elastin.19 The fractional CO2 laser combines CO2 ablation with fractional photothermolysis, and its efficacy in treating acne scars has been proven.20,21 However, there is a chance of unfavorable results and associated complications in many cases.22
Fang et al23 in their study demonstrated that three treatment sessions over three months with fractional CO2 laser improved atrophic acne scars in 82 patients with Fitzpatrick skin types III–IV. However, adverse events secondary to laser resurfacing, including erythema for a period <3 months (in 80.49% of patients), prolonged erythema >3 months (19.51%), hyperpigmentation for <3 months (41.46%), persistent hyperpigmentation >3 months (31.71%), hypopigmentation (1.22%), acne flare-up (9.76%), and post-laser scar (2.44%) were recorded. Several other researchers have shown that combination therapies can outperform single laser treatments.
Nanofat contains multiple biologically active substances that can improve skin quality and tissue regeneration, such as platelet-derived growth factor, transforming growth factor-β, and epithelial growth factor.24,25 Nanofat has also been associated with accelerated healing after fractional CO2 laser, attributed to its high concentration of regenerative and anti-inflammatory growth factors.11 ADSCs enhance collagen synthesis and promote fibroblast proliferation and migration.26,27 Moreover, ADSCs preserve the integrity of the epidermal barrier through increasing ceramide synthesis.28
Gu et al29 conducted a prospective case series to study the efficacy of nanofat in atrophied scars. They recruited 20 patients with 25 atrophic facial scars, where two were due to acne. A significantly improved overall Patient and Observer Scar Assessment Scale was found at the end of their follow-up.
The authors, in a former study, recruited 35 patients and compared the advantages of fractional CO2 laser combined with nanofat versus fractional CO2 laser combined with PRP for treating acne scars. The evaluation was done subjectively using Goodman score and objectively using Antera camera. A statistically significant improvement was found after using both modalities. However, a single session of nanofat injection showed at least comparable results to 3 sessions of PRP in terms of improvement of acne scars.30
In a prospective split-face trial by Abou Eitta et al,31 10 patients with acne scars received a single injection of ADSCs to one side of the face, while the other side was treated by three sessions of fractional CO2 laser. After three months of therapy, there was no significant difference between the two treatment modalities, concluding that one injection of ADSCs was shown to be as effective as three sessions of fractional CO2 laser.
Azzam et al32 compared fractional CO2 laser treatment to autologous fat in 20 patients with acne scars. Sixty percent of patients significantly improved when treated with autologous fat compared with 20% treated with fractional CO2 laser.
Our results are similar to the split-face study done by Kwon et al11 They treated 25 patients with three fractional CO2 laser sessions. After laser treatment, one side of the face was treated with the adipose exosomes gel, and the other was treated with a control gel. Treatment with adipose exosomes led to much more improvement and less incidence of adverse effects than the control sides, concluding that using ADSCs combined with laser skin resurfacing technologies might improve the outcome of treating acne scars.
Limitations of this study include the small sample size, the short follow-up period, the unequal ratio of male and female study participants, and the lack of comparison with other treatment modalities. Additional studies across a larger population with longer durations of follow-up, using objective evaluation methods, and the addition of comparison groups with CO2 laser alone and/or nanofat injection alone are needed.
Conclusions
In summary, this study shows that atrophic acne scars significantly improved with the combined nanofat injection and fractional CO2 laser therapy. In terms of efficacy and safety, co-treatment with these approaches may synergistically affect both aesthetic appearance and psychological health of patients with minimal complications and good patient compliance.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study was done in accordance with the Declaration of Helsinki after approval of the ethical committee of the Faculty of Medicine, Al-Azhar University (Approval No. Der-Med.22.Research.0000216). All patients signed informed consent before the procedures.
Consent for Publication
All patients signed informed consent for publication of this research and any accompanying images.
Acknowledgments
We thank the patients who participated in this study.
Author Contributions
All authors made a significant contribution to this study, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Manfredini M, Sticchi A, Lippolis N, et al. Characterization of acne-prone skin with reflectance confocal microscopy and optical coherence tomography and modifications induced by topical treatment and probiotic supplementation. J Clin Med. 2023;12(14):4787. doi:10.3390/jcm12144787
2. Baldwin H, Tan J. Effects of diet on acne and its response to treatment. Am J Clin Dermatol. 2021;22(1):55–65. doi:10.1007/s40257-020-00542-y
3. Fabbrocini G, Fardella N, Monfrecola A, Proietti I, Innocenzi D. Acne scarring treatment using skin needling. Clin Exp Dermatol. 2009;34(8):874–879. doi:10.1111/j.1365-2230.2009.03291.x
4. Kravvas G, Al-Niaimi F. A systematic review of treatments for acne scarring. Part 1: non-energy-based techniques. Scars Burn Heal. 2017;3:2059513117695312. doi:10.1177/2059513117695312
5. Heng AHS, Chew FT. Systematic review of the epidemiology of acne vulgaris. Sci Rep. 2020;10(1):5754. doi:10.1038/s41598-020-62715-3
6. Ismail SA, Khella NAH, Abou-Taleb DAE. Which is more effective in atrophic acne scars treatment microneedling alone or platelet rich plasma alone or combined both therapeutic modalities? Dermatol Ther. 2022;35(12):e15925. doi:10.1111/dth.15925
7. Lin M, Ma Y, Liu Z, Ruan H, Yuan B. Modern techniques in addressing facial acne scars: a thorough analysis. Skin Res Technol. 2024;30(2):e13573. doi:10.1111/srt.13573
8. Kauvar ANB, Warycha MA. Wrinkles and Acne Scars: fractional Ablative Lasers. In: Raulin C, Karsai S, editors. Laser and IPL Technology in Dermatology and Aesthetic Medicine.
9. Omi T, Numano K. The role of the CO2 Laser and Fractional CO2 laser in dermatology. Laser Ther. 2014;23(1):49–60. doi:10.5978/islsm.14-RE-01
10. Husain Z, Alster TS. The role of lasers and intense pulsed light technology in dermatology. Clin Cosmet Invest Dermatol. 2016;9:29–40. doi:10.2147/CCID.S69106
11. Kwon HH, Yang SH, Lee J, et al. Combination treatment with human adipose tissue stem cell-derived exosomes and fractional CO2 laser for acne scars: a 12-week prospective, double-blind, randomized, split-face study. Acta Derm Venereol. 2020;100(18):adv00310. doi:10.2340/00015555-3666
12. Tonnard P, Verpaele A, Peeters G, Hamdi M, Cornelissen M, Declercq H. Nanofat grafting: basic research and clinical applications. Plast Reconstr Surg. 2013;132(4):1017–1026. doi:10.1097/PRS.0b013e31829fe1b0
13. Rageh MA, El-Khalawany M, Ibrahim SMA. Autologous nanofat injection in treatment of scars: a clinico-histopathological study. J Cosmet Dermatol. 2021;20(10):3198–3204. doi:10.1111/jocd.14363
14. Goodman GJ, Baron JA. Postacne scarring--a quantitative global scarring grading system. J Cosmet Dermatol. 2006;5(1):48–52. doi:10.1111/j.1473-2165.2006.00222.x
15. Klein JA. Tumescent technique for local anesthesia. West J Med. 1996;164:517.
16. Johnson C. Measuring pain. visual analog scale versus numeric pain scale: what is the difference? J Chiropr Med. 2005;4(1):43–44. doi:10.1016/S0899-3467(07)60112-8
17. Tam C, Khong J, Tam K, Vasilev R, Wu W, Hazany S. A comprehensive review of non-energy-based treatments for atrophic acne scarring. Clin Cosmet Invest Dermatol. 2022;15:455–469. doi:10.2147/CCID.S350040
18. Connolly D, Vu HL, Mariwalla K, Saedi N. Acne scarring-pathogenesis, evaluation, and treatment options. J Clin Aesthet Dermatol. 2017;10(9):12–23.
19. Bhargava S, Cunha PR, Lee J, Kroumpouzos G. Acne scarring management: systematic review and evaluation of the evidence. Am J Clin Dermatol. 2018;19(4):459–477. doi:10.1007/s40257-018-0358-5
20. Chang HC, Sung CW, Lin MH. Efficacy of autologous platelet-rich plasma combined with ablative fractional carbon dioxide laser for acne scars: a systematic review and meta-analysis. Aesthet Surg J. 2019;39(7):NP279–NP287. doi:10.1093/asj/sjz048
21. Xu Y, Deng Y. Ablative fractional CO2 Laser for facial atrophic acne scars. Facial Plast Surg. 2018;34(2):205–219. doi:10.1055/s-0037-1606096
22. Park GH, Rhee Do Y, Moon HR, et al. Effect of an epidermal growth factor-containing cream on postinflammatory hyperpigmentation after Q-switched 532-nm neodymium-doped yttrium aluminum garnet laser treatment. Dermatol Surg. 2015;41(4):131–135. doi:10.1097/DSS.0000000000000197
23. Fang F, Yang H, Liu X, et al. Treatment of acne scars with fractional carbon dioxide laser in Asians: a retrospective study to search for predicting factors associated with efficacy. Lasers Med Sci. 2022;37(6):2623–2627. doi:10.1007/s10103-022-03528-w
24. Maisel-Campbell AL, Ismail A, Reynolds KA, et al. A systematic review of the safety and effectiveness of platelet-rich plasma (PRP) for skin aging. Arch Dermatol Res. 2020;312(5):301–315. doi:10.1007/s00403-019-01999-6
25. Jeyaraman M, Muthu S, Sharma S, Ganta C, Ranjan R, Jha SK. Nanofat: a therapeutic paradigm in regenerative medicine. World J Stem Cells. 2021;13(11):1733–1746. doi:10.4252/wjsc.v13.i11.1733
26. Kim WS, Park BS, Sung JH, et al. Wound healing effect of adipose-derived stem cells: a critical role of secretory factors on human dermal fibroblasts. J Dermatol Sci. 2007;48(1):15–24. doi:10.1016/j.jdermsci.2007.05.018
27. Wang L, Hu L, Zhou X, et al. Exosomes secreted by human adipose mesenchymal stem cells promote scarless cutaneous repair by regulating extracellular matrix remodelling. Sci Rep. 2017;7(1):13321. doi:10.1038/s41598-017-12919-x
28. Shin KO, Ha DH, Kim JO, et al. Exosomes from human adipose tissue-derived mesenchymal stem cells promote epidermal barrier repair by inducing de novo synthesis of ceramides in atopic dermatitis. Cells. 2020;9(3):680. doi:10.3390/cells9030680
29. Gu Z, Li Y, Li H. Use of condensed nanofat combined with fat grafts to treat atrophic scars. JAMA Facial Plast Surg. 2018;20(2):128–135. doi:10.1001/jamafacial.2017.1329
30. Rageh MA, Tawfik AA, Abdallah N, Ibrahim SMA. Fractional CO2 laser combined with autologous nanofat injection versus fractional CO2 laser combined with platelet-rich plasma in the treatment of atrophic acne scars: a split-face comparative study with optical skin imaging. Dermatol Surg. 2024;50(1):75–80. doi:10.1097/DSS.0000000000003968
31. Abou Eitta RS, Ismail AA, Abdelmaksoud RA, Ghezlan NA, Mehanna RA. Evaluation of autologous adipose-derived stem cells vs. fractional carbon dioxide laser in the treatment of post acne scars: a split-face study. Int J Dermatol. 2019;58(10):1212–1222. doi:10.1111/ijd.14567
32. Azzam OA, Atta AT, Sobhi RM, Mostafa PI. Fractional CO(2) laser treatment vs autologous fat transfer in the treatment of acne scars: a comparative study. J Drugs Dermatol. 2013;12(1):e7–e13.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.